 Jose Ramón Vidal-Castiñeira1
Jose Ramón Vidal-Castiñeira1 Viviana Corte-Iglesias1Lucia Sobrino-Diaz2
Viviana Corte-Iglesias1Lucia Sobrino-Diaz2 Sonia Pérez-Fernández3Santiago Melón4
Sonia Pérez-Fernández3Santiago Melón4 Carlos López-Larrea1,5*Carmen Díaz-Corte2
Carlos López-Larrea1,5*Carmen Díaz-Corte2- 1Translational Immunology Laboratory, Health Research Institute of the Principality of Asturias, Hospital Universitario Central de Asturias, Oviedo, Spain
- 2Nephrology Service, Hospital Universitario Central de Asturias, Oviedo, Spain
- 3Department of Statistics and Operational Research and Mathematics Didactics, Universidad de Oviedo, Oviedo, Spain
- 4Microbiology Service, Hospital Universitario Central de Asturias, Oviedo, Spain
- 5Immunology Service, Hospital Universitario Central de Asturias, Oviedo, Spain
Background: Dialysis is the first procedure to partially replace renal function in end-stage renal diseases, despite several adverse side effects, such as infections. The primary aim of this study was to evaluate the levels of immune CMV-specific CD8+ T cells in a representative cohort of pre-transplant patients receiving hemodialysis (HD) or peritoneal dialysis (PD). The secondary aim was to monitor the CMV-specific CD8+ T cells in kidney transplant recipients undergoing different types of dialysis during the first year following their transplant.
Methods: Sixty-nine patients were enrolled and examined with respect to the type of dialysis they received. HLA class I dextramers for CMV were used to determine the quantity of CMV-specific CD8+ T cells. The CMV DNA viral load was also determined. Forty-two of the patients enrolled in the study underwent solid organ transplantation and were analyzed during their first year post-transplantation.
Results: Patients receiving HD had fewer CMV-specific CD8+ T cells than those in PD (p < 0.05). We also observed that patients in PD had more CMV-specific CD8+ T cells during the follow-up period than those in HD (p < 0.05), independently of the CMV DNA. Finally, PD patients had a higher frequency of CD8+ Effector-Memory RA T cells (TEMRA) and a lower frequency of central memory T cells (TCM) than did HD patients.
Conclusions: These results indicate the better status of CMV-specific T cell immunity in PD patients. The use of CMV T cell dextramers would be advantageous for monitoring the CD8+ T-specific response, enabling the use of prophylactic treatment to be optimized.
Introduction
Patients in end-stage renal diseases experience disturbances of the immune system and are highly susceptible to infections arising from dialysis. The frequency of mortality of patients in dialysis is higher than in the general population, especially in patients in hemodialysis (HD) compared with those in peritoneal dialysis (PD) (1, 2). The risk of infections in these patients increases following kidney transplantation, especially during the first 12 months, because of the initial immunosuppression, which makes the recipient susceptible to serious infections such as human cytomegalovirus (CMV) (3). Primary infection or reactivation with CMV may cause a viremia and can lead to severe CMV disease with organ involvement (4). The clinical manifestations of human CMV infection include CMV syndrome (viremia and neutropenia), graft infection, predisposition to opportunistic infections, post-transplant lymphoproliferative disorders (generally with Epstein–Barr virus [EBV]), and chronic effects, including accelerated vasculopathy (5).
Two main strategies are used to prevent CMV infection after kidney organ transplantation (6). The first is prophylaxis of viral infections using antiviral drugs; the second strategy is preemptive therapy for organ recipients who develop evidence of CMV infection during routine screening (7). These strategies have brought about significant reductions of CMV infection and CMV-related mortality (8) but, on the other hand, they have led to a higher risk of developing anti-CMV drug resistance, a higher cost of antiviral medication, and a greater risk of side effects, with many patients being over-treated (9).
Customarily, CMV-DNA copy number has been used to identify viral reactivation (10), but the cellular immunity mediated by T lymphocytes is more relevant for controlling CMV infection (11). Immunity to CMV depends on the provision of adequate help from CMV-specific CD4+ T cells that enable production of neutralizing antibodies by CMV-specific B-cells/plasma blasts, and effective cytotoxic CD8+ T cell (CTL) responses (12). Many studies have reported the relationship between post-transplant functional impairment of CD8+ T cells immunity and failure to suppress CMV replication after kidney transplantation (8, 13), but little is known about the influence of the type of dialysis on CMV-specific CD8+ T cell status. Most of them have focused on evaluating functional immune responses (14, 15).
The aim of this study was to analyze the impact of the type of dialysis on the frequency of CMV-specific CD8+ T cells in pre- and post-transplant patients. Our overall purpose was to redefine therapeutic strategies for selected groups of immunosuppressed patients.
Methods
Study Population
A cohort of 69 unrelated Caucasian patients on the waiting list for a kidney transplant in the Nephrology Service of the Hospital Universitario Central de Asturias (HUCA), Oviedo, Spain, were included in the study between February 2016 and February 2017 (Table 1). They were recruited when they were called for organ transplantation. Forty-two of these patients (61.9% males) received a kidney transplant and were followed up for 1 year. Comprehensive clinical and analytical data of these patients were collected in order to analyze the evolution of the CMV-CD8+ specific T cells.
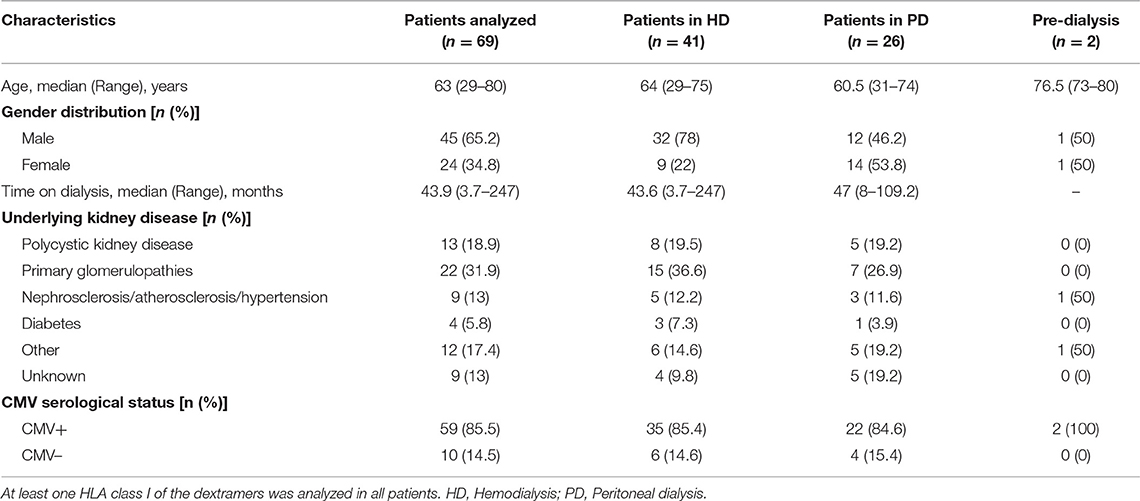
Table 1. Baseline clinical characteristics of the patient groups.
Blood samples were extracted in a blood collection tube with EDTA at different times (pre-transplant, and 15, 30, 45, 60, 90, 120, 150, 180, 210, 240, 270, 300, and 360 days post-transplant).
This study was carried out in accordance with the recommendations of the Regional Ethics Committee of Clinical Research of the Principado de Asturias. All the subjects gave their written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics Committee of our hospital.
CMV Viral Load Determination
CMV viral serostatus of the patients was determined as part of current routine clinical practice in the Microbiology Service (HUCA) using the Liaison CMV IgG II assays (DiaSorin, Saluggia, Italy). In-house real-time PCR was used to quantify CMV DNA in accordance with general regulatory guidelines concerning CMV viral load monitoring. A blood sample was extracted in a blood collection tube with EDTA, and the viral DNA was isolated from peripheral blood mononuclear cells (PBMCs). The viral β-glycoprotein and the human APOB gene as a control were amplified and hybridized with fluorescent-labeled probes in an RT-PCR based on TaqMan Genotyping Assays (Applied Biosystems, Foster City, CA, USA). The viral load in copies of CMV DNA per mL was determined, from which the International Units (IU) per mL were then calculated. The CMV DNA data of the patients were collected at the same post-transplant times as for the CMV-specific CD8+ T cell determination.
Flow Cytometry Analysis
The Dextramer CMV kit (Immudex, Copenhagen, Denmark) was used according to the manufacturer's instructions to quantify the CMV-specific CD8+ T cells. The CMV-MHC class I dextramers used, which covered most HLA specificities, were A:0101, A:0201, A:0301, A:2402, B:0702, B:0801, and B:3501. Samples were acquired using a Gallios flow cytometer (Beckman Coulter, Pasadena, CA, USA) and analyzed using Kaluza Analysis software (Beckman Coulter, Pasadena, CA, USA). A whole-blood control for lymphocyte subset enumeration was used in all sessions (BDTM Multi-Check control, BD Biosciences, San Jose, CA, USA). Absolute CD8+ T cells number and percentage were calculated using Trucount Tubes (BD Biosciences, San Jose, CA, USA).
For CD8+ T cell phenotyping, whole-EDTA anticoagulate was obtained by venipuncture. Peripheral blood mononuclear cells were obtained by Ficoll–Paque density-gradient centrifugation and directly analyzed. Naïve (CCR7+CD45RA+), central memory (CM) (CCR7+CD45RA–), effector memory (EM) (CCR7–CD45RA−), and effector memory RA (EMRA) (CCR7–CD45RA+) CD8+ T cells were assessed by flow cytometry using the following antibodies: CD3 (PerCP; BD Biosciences, San Jose, CA, USA), CD8 (FITC; BD Biosciences, San Jose, CA, USA), CD45RA (ECD; Beckman Coulter, Pasadena, CA, USA), and CCR7 (APC; BioLegend, San Diego, CA, USA).
ELISpot Assay for IFN-γ Detection of CMV-Specific T Cells
CMV-specific T cell activity was determined by measuring IFN-γ upon stimulation of PBMCs in 43 patients. The PBMCs were isolated from 5 mL of citrate blood using a standard Ficoll–Paque density gradient and resuspended in RPMI 1640 medium containing 2 ×10−3M l-glutamine and Hepes, supplemented with 10% FCS (ICN Flow, Costa Mesa, CA, USA) and antibiotics. For the ELISpot assay, 3 ×105 PBMCs per well were placed in triplicate wells of a 96-well filter plate (Millipore, Billerica, MA, USA) that was coated with anti-IFN-γ Ab (BD Biosciences, San Jose, CA, USA). These cells were stimulated with CMV-pp65 (PM-PP65-1; JPT, Berlin, Germany) and with 1 μg/mL anti-PMA (Sigma-Aldrich, St. Louis, MO, USA) as a positive control, and incubated for 24 h at 37°C. Negative controls were also included using PBMCs plus medium and DMSO. Plates were incubated for 2h at room temperature with 100 μL (1 μL/mL) biotinylated detection IFN-γ antibody to detect IFN-γ captured by the plate-bound Ab. Subsequently, plates were incubated with streptavidin (1 μg/mL) for 2 h at room temperature. As a final step, spots were developed by adding 200 μL of 3-amino-9-ethylcarbazole (BD Biosciences, San Jose, CA, USA) in acetate buffer supplemented with H2O2 30% for 3–5 min. Resulting spots were counted using a computer-assisted ELISpot reader (AID Autoimmun Diagnostika GmbH, Strassberg, Germany). Positive ELISpot signals were defined as those containing at least 25 spot-forming units per well.
Statistical Analysis
A descriptive statistical analysis of the variables was done separately for pre-transplant and post-transplant patients who received HD or PD. The continuous numerical variables were not normally distributed, so they were summarized as their median and range. Absolute and relative frequencies are displayed for qualitative variables. In order to test the difference between dialysis groups, the non-parametric Wilcoxon rank-sum test was used for continuous measures, while Fisher's exact test was considered for qualitative variables.
Multiple linear and logistic regression models were fitted as a multivariate study of the simultaneous statistical associations among several of the variables studied. Model terms were chosen in a backwards-stepwise manner, considering the Akaike information criterion (AIC), and the parameter estimates with 95% confidence intervals and associated probabilities were reported for the final model. The distribution of those measurements showing statistically significant differences between groups was displayed using boxplots. Statistical significance was concluded for values of p < 0.05 in all analyses. Data were analyzed within the R statistical environment (version 3.6.0).
Results
Analysis of Patients on the Waiting List
Patients were classified according to the type of dialysis they were receiving (n = 69; Table 1): 59.4% of them were in HD and 37.7% were in PD. The two other patients (2.9%) were included on the waiting list for kidney transplant in pre-dialysis because of the clinical recommendation of the nephrologists. The number of CMV-specific CD8+ T cells in the pre-transplant state was studied with respect to the patients' dialysis type. We found no significant differences between the dialysis groups in the total number of CD8+ T cells. However, there were statistically significant differences between them with respect to the proportions of patients who were serologically CMV+ (p = 0.03; Figure 1A). Among these CMV+ patients, we observed that those in HD had fewer CMV-specific CD8+ T cells than those receiving PD (median: HD vs. PD, 1.92 vs. 7.11, p = 0.012; Figure 1B).
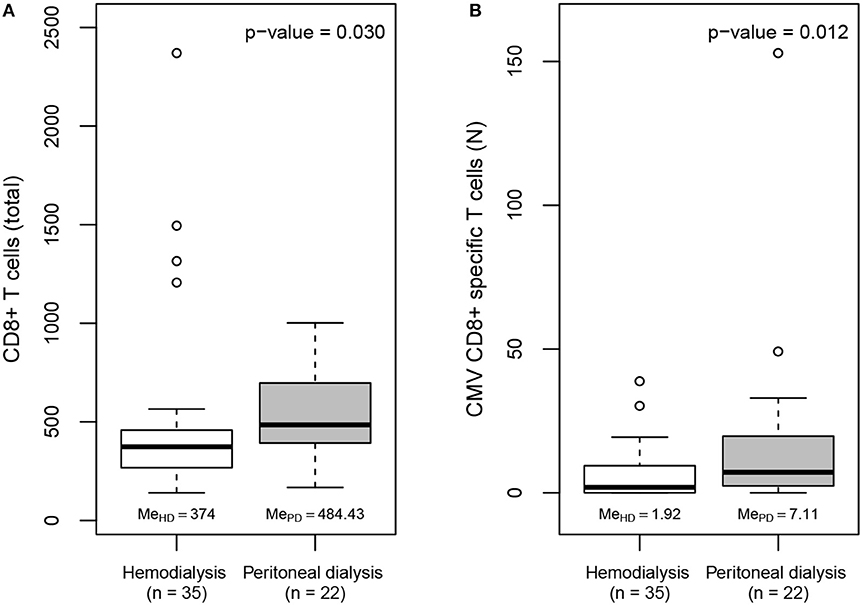
Figure 1. (A) Boxplots of the total frequency of CD8+ T cells in CMV seropositive patients on the kidney transplant waiting list by dialysis group. (B) Boxplots of the total frequency of CMV-specific CD8+ T cells in CMV seropositive patients on the kidney transplant waiting list by dialysis group.
Multivariate linear regression models were derived with the log-transformed frequency of CMV-specific CD8+ T cells as the response variable, and the type of dialysis and variables related to anti-CMV immunity (age, time on dialysis, serological CMV status and absolute frequency of CD8+ T cells) as regressors in the initial model. The final stepwise regression model shows that the type of dialysis (p < 0.01) and serological CMV status (p < 0.005) were significantly related to the frequency of anti-CMV CD8+ T cells (Table 2).
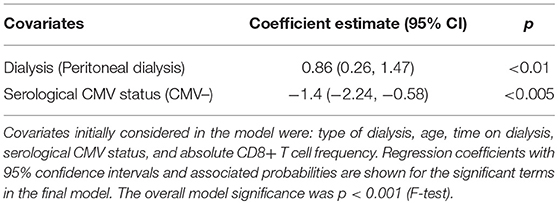
Table 2. Multiple linear regression model to explain variation in CMV-specific CD8+ T cell frequency.
In relation to the CD8+ T cells subsets, we found that patients in PD tended to have a higher porcentage of CD8+ TEMRA cells (median [range]: PD vs. HD, 48.3 [13–67] vs. 29.9 [17–72]) and a lower frequency of TCM cells than patients in HD (median [range]: HD vs. PD, 16.3 [6.2–31] vs. 7.8 [3.1–27]), but the magnitude of the difference was not sufficiently great to be statistically significant in the small sample of patients analyzed. Finally, in order to determine the immune responsiveness of these specific T cells we analyzed the levels of pre-transplant IFN-γ using a CMV ELISpot assay. Patients in HD exhibited preformed CMV-specific T cells directed to CMV-pp65 in 73.9% of the cases analyzed (17/23 of the patients, median frequency of spots/3 ×105 PBMCs [range], 77 [3–233]) compared with those in PD, 85% of whom (17/20, median frequency of spots/3 ×105 PBMCs [range], 94 [7–334]) showed preformed CMV-specific T cells directed to CMV-pp65. These differences were not significant.
In conclusion, we observed that the frequency of CMV-specific CD8+ T cells was higher in patients in PD than in those on HD. These patients also had a better cellular immune status against CMV than those in HD.
Analysis of Transplant Patients
We followed up those patients who had undergone solid organ transplantation (n = 42) for 1 year. Of the 42 patients, 19 experienced CMV reactivation (>100 IU/mL) within 360 days post-transplantation (Table 3), and five appeared to have no CMV-specific CD8+ T cells during the follow-up period after transplantation. Three of these five recipients were seronegative for CMV just before the kidney transplant but received a CMV-seropositive transplant. The other 37 patients were positive for CMV-specific CD8+ T cells on one or more occasion.
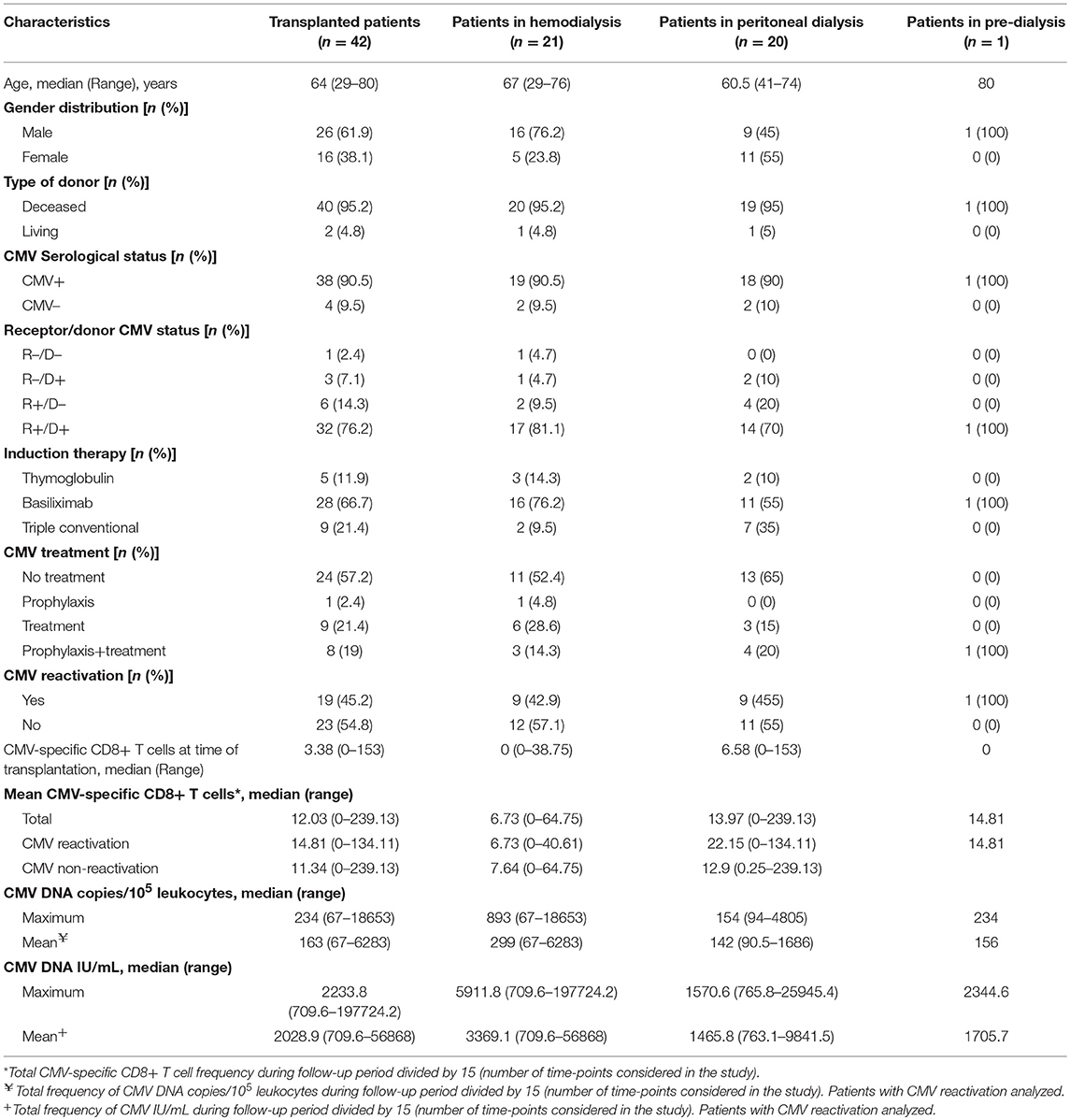
Table 3. Characteristics of transplanted patients by dialysis type.
The frequency of CMV-specific CD8+ T cells at the time of transplantation was higher in patients in PD compared with those in HD (PD vs. HD, median, 6.58 vs. 0, p = 0.026)—a similar finding to that noted in pre-transplanted patients. Furthermore, during the follow-up period, patients who were receiving PD had significantly more CMV-specific CD8+ T cells than did those in HD (PD vs. HD, median, 13.97 vs. 6.73, p = 0.015). The differences were greatest after 90 days, but frequencies had equalized by 360 days. Considering the patients with respect to the CMV reactivation, the CMV-specific CD8+ T cells frequency at the times studied showed that values for PD patients were more variable, but generally higher, than those patients in HD in both patient groups (Table 3, Figures 2A,B).
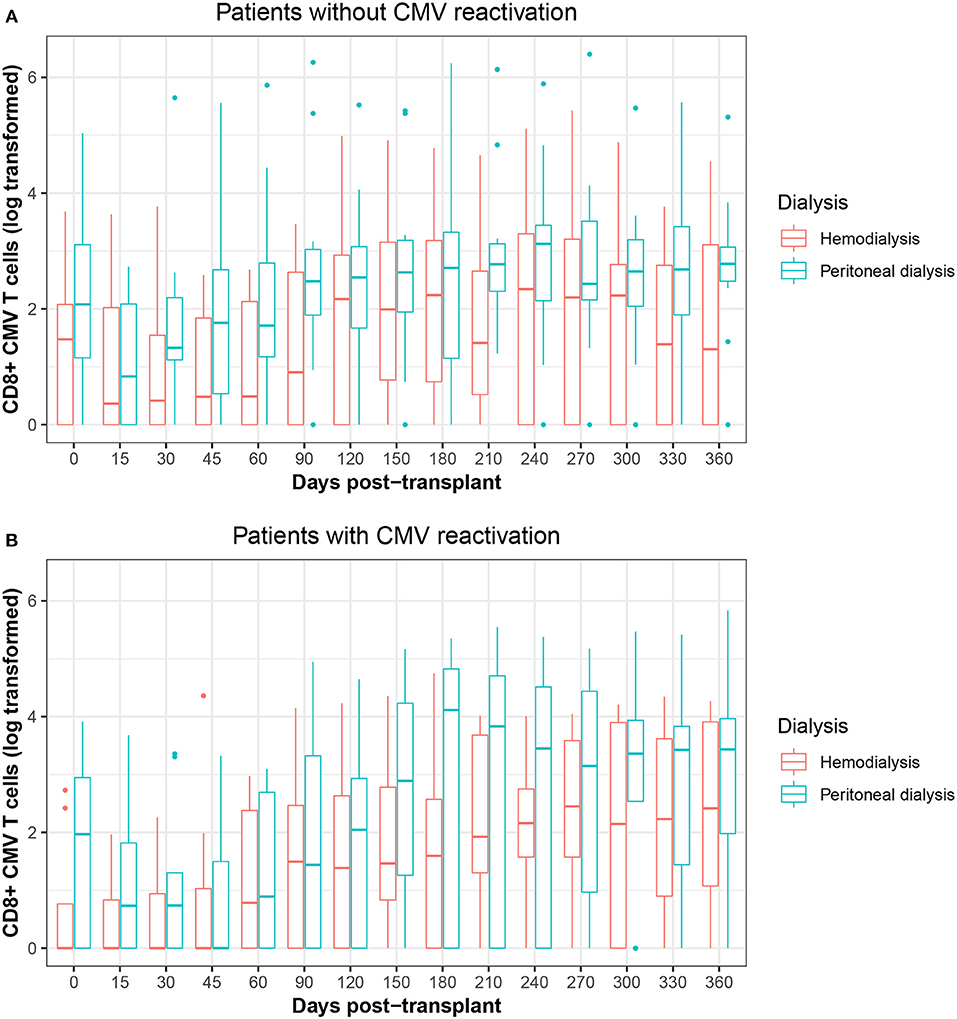
Figure 2. (A) Boxplots of the frequency of CMV-specific CD8+ T cells during the follow-up period classified by dialysis type in CMV non-reactivation patients. (B) Boxplots of the frequency of CMV-specific CD8+ T cells during the follow-up period classified by dialysis type in CMV reactivation patients.
On the other hand, we found no statistically significant correlation between the frequency of CMV-specific CD8+ T cells and the amount of CMV DNA, although 36.8% (7 of 19) of the patients who experienced CMV reactivation and needed antiviral treatment were from the group who had received HD, compared with 26.2% (5 of 19) of the patients who had received PD. There were fewer than 5 CMV-specific CD8+ T cells/μl in this group at the beginning of the CMV reactivation. In contrast, 5 of 19 patients who underwent CMV reactivation did not receive antiviral prophylaxis or treatment. These patients (2 HD and 3 PD patients) had a high frequency of >20 CMV-specific CD8+ T cells/μl during follow-up.
Finally, other clinical parameters related to CMV reactivation, such as the CMV serostatus of the donors and recipients, the immunosuppressor levels and receipt of induction therapy were analyzed, but did not reveal any differences in the frequency of CMV-specific CD8+ T cells. A multivariate analysis including the type of dialysis, age, time on dialysis, serological CMV status, and total frequency of CD8+ T cells was performed, but none of the variables proved to be significantly associated with the increase in frequency of anti-CMV CD8+ T cells, possibly due to the low number of patients analyzed.
In summary, the frequency of CMV-specific CD8+ T cells increased in both groups of patients by 90 days, possibly due to the reduction in immunosuppression levels and the end of CMV prophylaxis. We also observed that patients in PD had better cellular immune status than those in HD.
Discussion
CMV has a negative consequence for patients and allograft outcomes after kidney transplantation. CMV-specific CD8+ T cells are thought to be crucial to the control of CMV replication in the early phase after kidney transplantation (16). The frequency of CMV-specific CD8+ T cells has so far been little studied with regard to the risk of post-prophylaxis CMV infection, irrespective of the pre-transplant serological status. One study reported a strong positive correlation between the levels of CMV-specific CD4+ T cells and the frequency of infectious episodes in lung- but not kidney-transplant recipients, depending on the immunosuppression regimen employed (17). Moreover, Gordon et al. recently reported a correlation between the persistence of CMV and antiviral T cell immunity, whereby there was a different distribution of CMV-specific CD8+ T cells in several tissues (18).
The aim of this study was to monitor the frequency of CMV CD8+ specific T cells by using the dextramer technology in pre- and post-kidney transplant patients. We found more CMV-specific CD8+ T cells in patients in PD than in those receiving HD, and noted that this status was maintained throughout the 1-year follow-up after kidney transplantation, irrespective of patients' CMV serological status. Thus, protective anti-CMV cellular immunity may exist in these patients, unlike those receiving HD, indicating that patients in PD treatment were better able to resolve CMV reactivation. During the post-transplant follow-up, the presence of CMV-specific CD8+ T cells was not sufficient to prevent viral reactivation (CMV viremia) in most patients. Associated risk factors and a greater susceptibility to immunosuppressors led to the decline in the frequency of CMV-specific CD8+ T cells. This is insufficient during the initial months to provide further protection from CMV replication, and valganciclovir prophylaxis is necessary, at least for the first 3 months, in patients with risk factors such as D+/R– transplants. On the other hand, some patients with a high frequency of CMV-specific CD8+ T cells, most of whom are patients in PD, are able to control the viremia themselves without the need for antiviral treatment. Nevertheless, this variation between patients suggests that CMV-specific T cell monitoring could provide a means of risk stratification in addition to CMV serostatus.
The type of dialysis is known to have a range of effects on the immune response (19). Mild monocytosis and lymphopenia are more prevalent in patients receiving HD compared with those in PD, and these could be responsible for the higher rate of acute rejection episodes in the early stages following renal transplantation in patients in HD (20). Moreover, patients in HD are more prone to infections and to an inadequate response to vaccinations (21), and severe lymphopenia has been shown to be a predictor of mortality in these patients (19). Recently, a CD19+ B-cell lymphopenia was observed in HD patients, leading the authors to conclude that it could be a biomarker of cardiovascular complication-related mortality (22). In contrast, patients in PD were less likely to suffer chronic inflammations (23).
CMV infection generally leads to substantial and long-lasting changes in circulating T cells. In particular, those of the highly differentiated TEMRA (Effector Memory RA) cells subset are expanded in the CD8+ T cell population (24). Recently, Ferreira et al. have shown that organ transplant recipients who were unable to control CMV viremia had higher frequencies of TEMRA cells with low activation and differentiation markers compared with those with increased activation markers in TCM and TEMRA cells subsets and who were able to control their viremia (25). In this preliminary study, we observed differences in the CD8+ T cells subsets between patients in PD and HD, but the magnitude was not large enough to be statistically significant in the small sample of patients analyzed. Nevertheless, the description of the status of these CD8+ T cells subsets including other markers could help us understand how dialysis affects the maintenance of an adequate pool of the CMV-specific CD8+ T lymphocytes that are required to ensure immunity against CMV infection in the post-transplant context. In the near future, we will study more patients in order to verify our current results. As part of this work, we will analyze activation and differentiation markers in these CD8+ T cell subpopulations.
The determination of cellular immunity to assess risk before kidney transplantation by analyzing patients on the waiting list who are receiving dialysis, and the analysis of immune responsiveness using ELISpot, are powerful methods for evaluating CMV antiviral prophylaxis therapy. Further studies are needed to identify the variables associated with the risk of CMV reactivation, to characterize these CMV-specific T cells phenotypically, and to establish a cut-off for pre-transplant CMV-specific CD8+ T cells in order to be able to categorize patients.
Data Availability
The raw data supporting the conclusions of this manuscript will be made available on request to the corresponding author.
Ethics Statement
This study was carried out in accordance with the recommendations of the Regional Ethics Committee of Clinical Research of Principado de Asturias, with written informed consent from all subjects. The study was carried out in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics committee of our hospital.
Author Contributions
JV-C, CD-C, and CL-L: concept and design. JV-C, VC-I, LS-D, and SM: experiments and procedures. JV-C, VC-I, CD-C, and CL-L: writing of article. SP-F: statistical analysis. LS-D, SM, and CD-C: patients selection.
Funding
This work was supported by the Plan Nacional de I+D+I 2013-2016 ISCIII (Spanish Institute of Health Carlos III; grant numbers PI16/01318 and PI17/01244); Gobierno del Principado de Asturias, PCTI-Plan de Ciencia, Tecnología e Innovación 2013–2017, (grant number IDI/2018/144); FEDER Funding Program of the European Union; and the Red Española de Investigación Renal (REDinREN, grant numbers RD16/0009/0020 and RD16/0009/0021). SP-F was supported by Severo Ochoa grant BP16118 (Gobierno del Principado de Asturias).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. McDonald SP, Marshall MR, Johnson DW, Polkinghorne KR. Relationship between dialysis modality and mortality. J Am Soc Nephrol. (2009) 20:155–63. doi: 10.1681/ASN.2007111188
2. Lukowsky LR, Mehrotra R, Kheifets L, Arah OA, Nissenson AR, Kalantar-Zadeh K. Comparing mortality of peritoneal and hemodialysis patients in the first 2 years of dialysis therapy: a marginal structural model analysis. Clin J Am Soc Nephrol. (2013) 8:619–28. doi: 10.2215/CJN.04810512
3. Humar A, Michaels M, AST ID Working Group on Infectious Disease Monitoring. American Society of Transplantation recommendations for screening, monitoring and reporting of infectious complications in immunosuppression trials in recipients of organ transplantation. Am J Transplant. (2006) 6:262–74. doi: 10.1111/j.1600-6143.2005.01207.x
4. Crough T, Khanna R. Immunobiology of human cytomegalovirus: from bench to bedside. Clin Microbiol Rev. (2009) 22:76–98. doi: 10.1128/CMR.00034-08
5. Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med. (2007) 357:2601–14. doi: 10.1056/NEJMra064928
6. Kaminski H, Fishman JA. The cell biology of cytomegalovirus: implications for transplantation. Am J Transplant. (2016) 16:2254–69. doi: 10.1111/ajt.13791
7. Humar A, Lebranchu Y, Vincenti F, Blumberg EA, Punch JD, Limaye AP, et al. The efficacy and safety of 200 days valganciclovir cytomegalovirus prophylaxis in high-risk kidney transplant recipients. Am J Transplant. (2010) 10:1228–37. doi: 10.1111/j.1600-6143.2010.03074.x
8. Mattes FM, Vargas A, Kopycinski J, Hainsworth EG, Sweny P, Nebbia G, et al. Functional impairment of cytomegalovirus specific CD8 T cells predicts high-level replication after renal transplantation. Am J Transplant. (2008) 8:990–9. doi: 10.1111/j.1600-6143.2008.02191.x
9. Razonable RR. Drug-resistant cytomegalovirus: clinical implications of specific mutations. Curr Opin Organ Transplant. (2018) 23:388–94. doi: 10.1097/MOT.0000000000000541
10. Eshraghi H, HekmatR. Which CMV viral load threshold should be defined as CMV infection in kidney transplant patients? Transplant Proc. (2015) 47:1136–9. doi: 10.1016/j.transproceed.2014.11.066
11. Cantisan S, Rodelo-Haad C, Paez-Vega A, Nieto A, Vaquero JM, Poyato A, et al. Factors related to the development of CMV-specific CD8+ T cell response in CMV-seropositive solid organ transplant candidates. Am J Transplant. (2015) 15:715–22. doi: 10.1111/ajt.13012
12. Klenerman P, Oxenius A. T cell responses to cytomegalovirus. Nat Rev Immunol. (2016) 16:367–77. doi: 10.1038/nri.2016.38
13. Engstrand M, Lidehall AK, Totterman TH, Herrman B, Eriksson BM, Korsgren O. Cellular responses to cytomegalovirus in immunosuppressed patients: circulating CD8+ T cells recognizing CMVpp65 are present but display functional impairment. Clin Exp Immunol. (2003) 132:96–104. doi: 10.1046/j.1365-2249.2003.02098.x
14. Cantisan S, Lara R, Montejo M, Redel J, Rodriguez-Benot A, Gutierrez-Aroca J, et al. Pretransplant interferon-γ secretion by CMV-specific CD8+ T cells informs the risk of CMV replication after transplantation. Am J Transplant. (2013) 13:738–45. doi: 10.1111/ajt.12049
15. Yang R, Xia T, Xu G, Li Z, Ying Z, Xu X. Human cytomegalovirus specific CD8(+) T lymphocytes display interferon-gamma secretion impairment in kidney transplant recipients with pp65 antigenemia. Transplant Proc. (2008) 40:3500–4. doi: 10.1016/j.transproceed.2008.03.176
16. Schachtner T, Stein M, Reinke P. CMV-specific T cell monitoring offers superior risk stratification of CMV-seronegative kidney transplant recipients of a CMV-seropositive donor. Transplantation. (2017) 101:e315–25. doi: 10.1097/TP.0000000000001825
17. Sester U, Gartner BC, Wilkens H, Schwaab B, Wossner R, Kindermann I, et al. Differences in CMV-specific T-cell levels and long-term susceptibility to CMV infection after kidney, heart and lung transplantation. Am J Transplant. (2005) 5:1483–9. doi: 10.1111/j.1600-6143.2005.00871.x
18. Gordon CL, Miron M, Thome JJ, Matsuoka N, Weiner J, Rak MA, et al. Tissue reservoirs of antiviral T cell immunity in persistent human CMV infection. J Exp Med. (2017) 214:651–67. doi: 10.1084/jem.20160758
19. Reddan DN, Klassen PS, Szczech LA, Coladonato JA, O'Shea S, Owen WF Jr, et al. White blood cells as a novel mortality predictor in haemodialysis patients. Nephrol Dial Transplant. (2003) 18:1167–73. doi: 10.1093/ndt/gfg066
20. Satoh S, Tsuchiya N, Sato K, Ohtani H, Komatsuda A, Habuchi T, et al. Influence of pretransplant dialysis modality on the change of lymphocyte subset populations and acute rejection rates after renal transplantation. Int J Urol. (2004) 11:825–30. doi: 10.1111/j.1442-2042.2004.00915.x
21. Eleftheriadis T, Antoniadi G, Liakopoulos V, Kartsios C, Stefanidis I. Disturbances of acquired immunity in hemodialysis patients. Semin Dial. (2007) 20:440–51. doi: 10.1111/j.1525-139X.2007.00283.x
22. Molina M, Allende LM, Ramos LE, Gutierrez E, Pleguezuelo DE, Hernandez ER, et al. CD19(+) B-cells, a new biomarker of mortality in hemodialysis patients. Front Immunol. (2018) 9:1221. doi: 10.3389/fimmu.2018.01221
23. Cai K, Luo Q, Zhu B, Han L, Wu D, Dai Z, et al. Neutrophil-lymphocyte ratio is associated with arterial stiffness in patients with peritoneal dialysis. BMC Nephrol. (2016) 17:191. doi: 10.1186/s12882-016-0394-4
24. Solana R, Tarazona R, Aiello AE, Akbar AN, Appay V, BeswickM, et al. CMV and immunosenescence: from basics to clinics. Immun Ageing. (2012) 9:23. doi: 10.1186/1742-4933-9-23
Keywords: CMV, hemodialysis, peritoneal dialysis, CMV-specific CD8+ T cells, dextramers
Citation: Vidal-Castiñeira JR, Corte-Iglesias V, Sobrino-Diaz L, Pérez-Fernández S, Melón S, López-Larrea C and Díaz-Corte C (2019) Effect of Type of Dialysis on CMV-Specific CD8+ T Cells in Kidney Transplant Candidates. Front. Immunol. 10:1680. doi: 10.3389/fimmu.2019.01680
Received: 15 April 2019; Accepted: 04 July 2019;
Published: 19 July 2019.
Edited by:
Aurore Saudemont, GlaxoSmithKline, United KingdomReviewed by:
David Navarro, Clinical University Hospital Valencia, SpainCorinna La Rosa, City of Hope National Medical Center, United States
Copyright © 2019 Vidal-Castiñeira, Corte-Iglesias, Sobrino-Diaz, Pérez-Fernández, Melón, López-Larrea and Díaz-Corte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos López-Larrea, aW5tdW5vQGhjYS5lcw==