 Stephen A. Rawlings1†
Stephen A. Rawlings1† Sven Heldt2,3†
Sven Heldt2,3† Juergen Prattes3
Juergen Prattes3 Susanne Eigl2
Susanne Eigl2 Jeffrey D. Jenks4Holger Flick2Jasmin Rabensteiner5Florian Prüller5Albert Wölfler6Peter Neumeister6Heimo Strohmaier7
Jeffrey D. Jenks4Holger Flick2Jasmin Rabensteiner5Florian Prüller5Albert Wölfler6Peter Neumeister6Heimo Strohmaier7 Robert Krause3,8
Robert Krause3,8 Martin Hoenigl1,2,3*
Martin Hoenigl1,2,3*- 1Division of Infectious Diseases, Department of Medicine, University of California, San Diego, San Diego, CA, United States
- 2Division of Pulmonology, Medical University of Graz, Graz, Austria
- 3Section of Infectious Diseases and Tropical Medicine, Medical University of Graz, Graz, Austria
- 4Department of Medicine, University of California, San Diego, San Diego, CA, United States
- 5Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University of Graz, Graz, Austria
- 6Division of Hematology, Medical University of Graz, Graz, Austria
- 7Center for Medical Research, Medical University of Graz, Graz, Austria
- 8BioTechMed-Graz, Graz, Austria
Background: Molds and other pathogens induce elevated levels of several cytokines, including interleukin (IL)-6 and IL-8. The objective of this study was to investigate the prognostic value of IL-6 and IL-8 as well as fungal biomarkers in blood and bronchoalveolar lavage fluid (BAL) for overall survival in patients with underlying hematological malignancies and suspected mold infection.
Methods: This cohort study included 106 prospectively enrolled adult cases undergoing bronchoscopy. Blood samples were collected within 24 h of BAL sampling and, in a subset of 62 patients, serial blood samples were collected up until 4 days after bronchoscopy. IL-6, IL-8, and other cytokines as well as galactomannan (GM) and β-D-glucan (BDG) were assayed in blood and BAL fluid and associations with overall mortality were assessed at the end of the study using receiver operating characteristic (ROC) curve analysis.
Results: Both blood IL-8 (AUC 0.731) and blood IL-6 (AUC 0.699) as well as BAL IL-6 (AUC 0.763) and BAL IL-8 (AUC 0.700) levels at the time of bronchoscopy were predictors of 30-day all-cause mortality. Increasing blood IL-6 levels between bronchoscopy and day four after bronchoscopy were significantly associated with higher 90-day mortality, with similar findings for increasing IL-8 levels. In ROC analysis the difference of blood IL-8 levels between 4 days after bronchoscopy and the day of bronchoscopy had an AUC of 0.829 (95%CI 0.71–0.95; p < 0.001) for predicting 90-day mortality.
Conclusions: Elevated levels of IL-6 and IL-8 in blood or BAL fluid at the time of bronchoscopy, and rising levels in blood 4 days following bronchoscopy were predictive of mortality in these patients with underlying hematological malignancy who underwent bronchoscopy for suspected mold infection.
Introduction
Patients with hematologic malignancies are immunocompromised with increased rates of hospital admissions and, in particular, admissions to the intensive care unit (ICU) (1). Factors that increase the risk of admission to the ICU include pneumonia caused by invasive mold infections (IMI) or other pathogens (2). IMI, including invasive aspergillosis (IA), are associated with high morbidity and mortality among patients with underlying hematological malignancies (3–7). Prognosticating survival in patients at risk for IMI remains difficult (8), although prompt identification of those most at risk for severe complications and death and early initiation of antifungal or other anti-infective therapy could lead to better outcomes (9).
Aspergillus spp. have been shown to induce T-helper cell subsets resulting in elevated levels of several cytokines (10, 11) and recent studies have indicated—after adjusting for multiple covariates also associated with higher cytokine levels—that particularly Interleukin (IL)-8 and IL-6 may show promise as diagnostic markers (12, 13). Our own work suggests that elevated levels of IL-8 in patients presenting with suspected pulmonary infection have excellent specificity (>90%) for detecting IMI (14), however whether these cytokines may also predict overall mortality and whether serial measurement of this cytokines may increase their prognostic potential remains unknown.
The objective of this analysis was to determine the potential of variations in IL-6 and IL-8, as well as established fungal biomarkers, to predict overall mortality in patients with underlying hematological malignancies and suspicion of pulmonary mold infection in a setting that uses mold-active prophylaxis.
Materials and Methods
This prospective cohort study comprised paired routine serum and BAL samples obtained on the same day from cases with underlying hematological malignancies who underwent routine bronchoscopy due to suspicion of pulmonary mold infections. The decision was based on suspicious or non-specific radiological findings in chest computed tomography, with or without clinical laboratory findings including fungal biomarker levels. Investigators had no influence on clinical interventions (e.g., bronchoscopy) and treatment of the enrolled patients. The diagnostic potential of several biomarkers and cytokines measured in same day BAL and blood samples obtained as part of this cohort study for diagnosing IMI has been previously published (13, 14). However, the present analysis focuses on the overall prognostic potential of several cytokines and biomarkers in clinical outcomes of IMI. Approximately halfway through the study, the protocol was modified to include permission to use routinely-collected surplus plasma samples stored in the hospital laboratory for 4 days following collection. These longitudinal samples have not previously been published.
IA and IMI were graded in accordance with the revised criteria by the European Organization for Research and Treatment of Cancer Invasive Fungal Infections Cooperative Group (EORTC) and the Mycoses Study Group of the National Institute of Allergy and Infectious Disease (MSG) (15).
Study Cohort
Participants undergoing bronchoscopy were prospectively enrolled at the Medical University of Graz, Graz, Austria, between April 2014 and July 2017. Key inclusion criteria were (i) adult patients with (ii) underlying hematological malignancy who were (iii) at risk for IMI according to the attending clinicians discretion (e.g., febrile neutropenia, induction chemotherapy for acute myeloid leukemia, allogeneic stem cell transplantation), had (iv) a BAL sample obtained due to clinical suspicion of pulmonary infection, and (v) an order of fungal biomarkers from BAL [i.e., galactomannan (GM) and in a subset also panfungal or Mucorales specific polymerase chain reaction]. All patients who met inclusion criteria between April 2014 and July 2017 and signed an informed consent were included in the cohort. After informed consent was obtained, serum and whole blood samples were collected within 24 h of bronchoscopy. In the last 62 patients enrolled in the study, serial daily plasma samples were also obtained from blood samples drawn as part of routine clinical care from 4 days before bronchoscopy until 4 days after bronchoscopy. Because Investigators had no influence on blood sample drawn besides the same-day samples, sample size varied between 2 and 9 plasma samples per case. These were stored at 4°C for up to 4 days before processing for storage at −70°C and analysis.
Biomarker Testing
Conventional culture as well as BAL and serum GM concentrations (Platelia enzyme immunoassay; Bio-Rad Laboratories, Vienna, Austria) were prospectively determined in clinical routine at the Medical University of Graz. Given that the vast majority of patients received mold-active antifungals at the time of bronchoscopy, cut-offs of 0.5 GM optical density index (ODI) where used for serum and BAL, following previous evidence that the 0.5 ODI cutoff is preferable in patients on mold-active antifungals (16).
β-D-glucan (BDG) testing was performed in part prospectively and in part retrospectively at the Medical University of Graz, using the commercially available Fungitell® assay (Cape Cod Diagnostics, Falmouth, MA, USA) with an adopted protocol suitable for use on a routine BCS XP® coagulation analyzer, as described previously (17). BDG testing was only performed in serum samples, as BAL BDG testing yields very low specificity due to non-pathogenic Candida colonization in the lungs and high BDG values (18–20). For serum BDG we used the recommended cut-off of ≥ 80 pg/mL to define positivity.
All blood (i.e., serum and plasma) and BAL isolates used in this study were frozen to −70°C after processing and stored for batched analysis. IL-6 and IL-8 concentrations were determined in serum, plasma, and BAL samples at the Center for Medical Research of the Medical University of Graz, Austria, between 09/2016 and 10/2017 with a personalized ProcartaPlex® immunoassay (eBioscience, Vienna, Austria) as previously described (13).
Investigators measuring biomarkers and cytokine levels were blinded toward clinical and demographic information of the patients.
Assessing Mortality
All patients enrolled in the study were followed clinically on initial admission and their medical records were reviewed after discharge. Autopsies were not routinely performed or requested as part of the study and therefore the absolute rate of autopsies on patients in the study was very low—likely reflecting the low cultural predilection for autopsy in the study country.
Our study was conducted in accordance with the Declaration of Helsinki, 2013, Good Clinical Practice. The study protocol was approved by the local ethics committee, Medical University Graz, Austria (EC-numbers 25-221 and 23-343), and registered at ClinicalTrials.gov (Identifier: NCT02058316 and NCT01576653). Informed consent was obtained from all study participants. Statistical analysis was performed using SPSS, version 25 (SPSS Inc., Chicago, IL, USA). For continuous data, including cytokine levels, receiver operating characteristic (ROC) curves analyses were performed and area under the curve (AUC) values are presented including 95% confidence intervals (95% CI) for the 30-, 90-, and 180-day overall mortality outcomes (p-values were not corrected for multiple comparisons). Optimal cut-offs for cytokines discriminating in patients who died within 30 days vs. those who survived were calculated using the Youden's index. Two-sided p-value < 0.05 was taken as cut-off for statistical significance.
Results
Study Cohort
In total, 122 participants undergoing bronchoscopy were prospectively enrolled between April 2014 and July 2017. A total of 16 cases had to be excluded due to the following reasons: (i) same day blood samples (i.e., collected within 24-h) were not available (n = 13); (ii) BAL volume after routine testing was insufficient for further diagnostic work up within the study protocol (n = 2); (iii) hematological malignancy was suspected but not confirmed because of mortality within days of admission (n = 1). After exclusion of these 16 cases, 106 patients remained in the final analysis. Patients' characteristics are displayed in Table 1. Mortality was 16% (17/106) at 30 days, 27.4% (29/106) at 90 days, and 42.5% (45/106) at 180 days after study enrollment and bronchoscopy. In those with mold infections, 30-day mortality was 36% for probable/proven IA, 16% for possible IA and 13% for those without evidence for IA (for all probable/possible/no IMI 33, 12, and 13%, respectively).
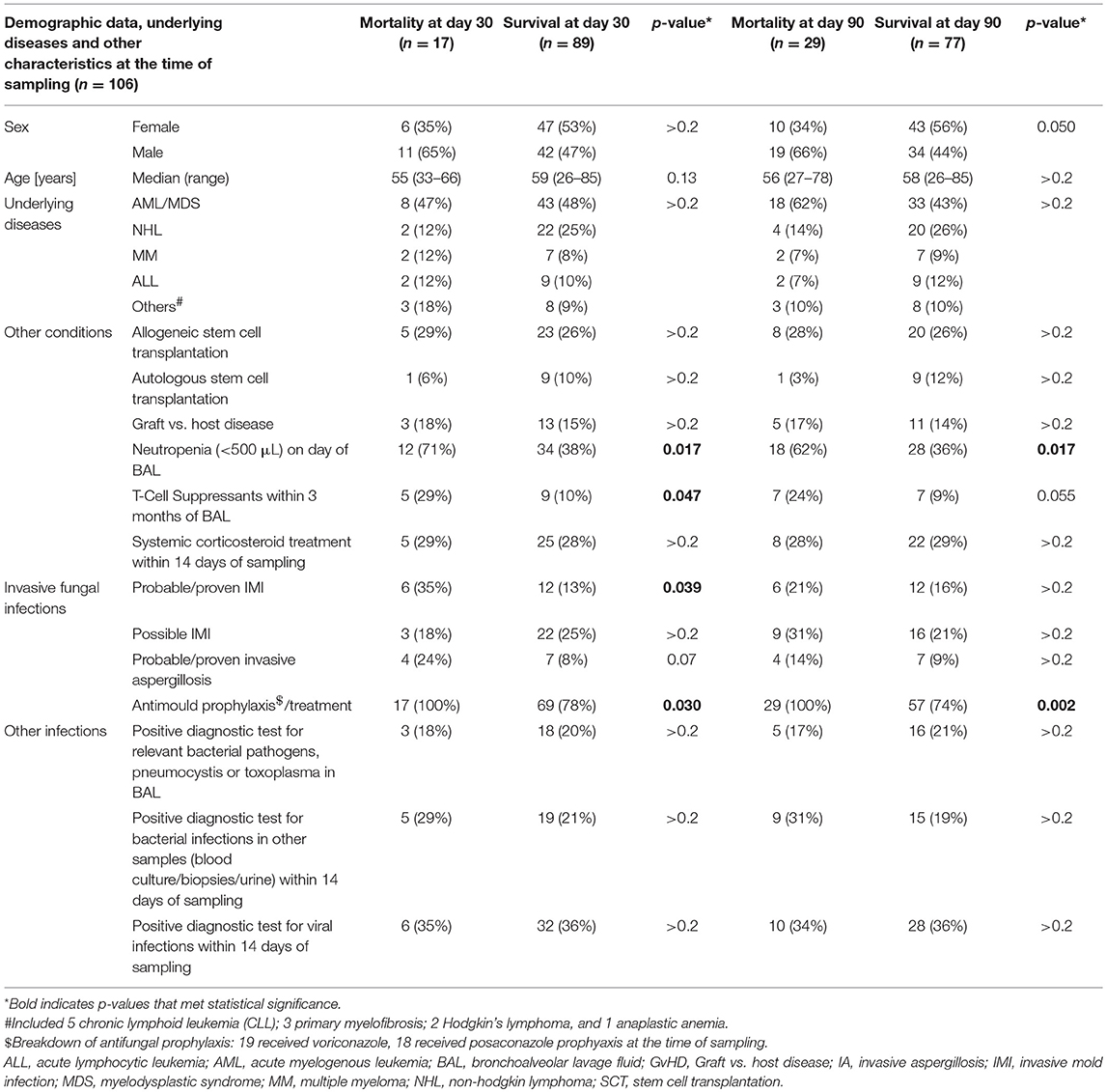
Table 1. Demographic data, underlying diseases, and infections in cases who died within 30 and 90 days after bronchoscopy vs. those who survived.
Overall patients who died within 30 days were more frequently neutropenic at the time of bronchoscopy, had more frequently received T-cell suppressants, had more frequently probable or proven IMI and had received more frequently mold active prophylaxis or treatment at the time of bronchoscopy (Table 1). Of the 17 cases who died within 30 days of bronchoscopy (median 14 days after bronchoscopy, range 1–30 days), autopsy was performed in four cases, revealing progression of acute myeloid leukemia as cause of death in two cases, while cause of death was infectious (organized viral pneumonia, multi organ failure) in the other two cases. Of the other 13 cases who did not undergo autopsy, five had probable IMI, two possible IMI, two viral pneumonias, and each one bacterial pneumonia or systemic bacterial infection. Neutropenia and receipt of mold-active antifungals were also more frequent in those who died within 90 days, in fact every single patient who died within 90 days had received a mold-active antifungal at the time of bronchoscopy while this was 74% of patients who survived to day 90 (p = 0.002).
Prognostic Potential of Blood and BAL Cytokines at the Time of Bronchoscopy
In ROC curve analysis, serum IL-8 was a significant predictor of 30-day overall mortality, followed by serum IL-6, while serum GM and serum BDG were not significant predictors (Table 2). In BAL IL-6 and IL-8 were significant predictors of overall 30-day mortality, while GM was not (Table 2). Both serum IL-8 and serum IL-6 as well as BAL IL-6 were also significant predictors of 90- and 180-day cumulative overall mortality, although AUCs were lower when compared to 30-day mortality, and significance driven mostly by the predictive potential for 30-day mortality (Table 2). When focusing only on participants who died within 30- and 90-days, or between 90- and 180-days, AUCs were highest for serum IL-8 (AUC 0.578 and 0.592, respectively), followed by serum IL-6 (AUC 0.564 for both; all p > 0.2). Boxplots of serum and BAL IL-8 and IL-6 levels in those who died and those who survived are displayed in Figure 1. For prediction of 30-day mortality, optimal cut-offs were serum IL-8 > 13.93 pg/mL (82.4% sensitivity, 61.8% specificity), serum IL-6 > 165 pg/mL (52.9% sensitivity, 87.6% specificity), BAL IL-8 > 1,111 pg/mL (64.7% sensitivity, 69.7% specificity), and BAL IL-6 > 43.95 pg/mL (100% sensitivity, 46.1% specificity).
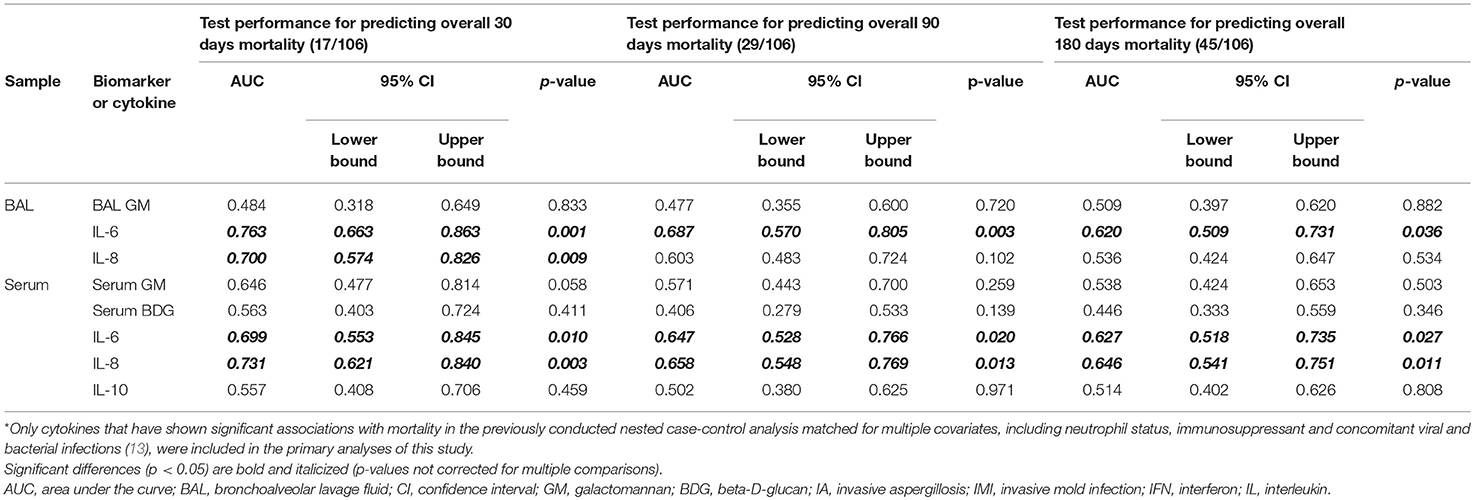
Table 2. Performance of cytokine levels*, Galactomannan (GM) and Beta-D-glucan (BDG) in serum and bronchoalveolar fluid (BAL) for differentiating cases who died within 30, 90, and 180 days of bronchoscopy vs. those who survived.
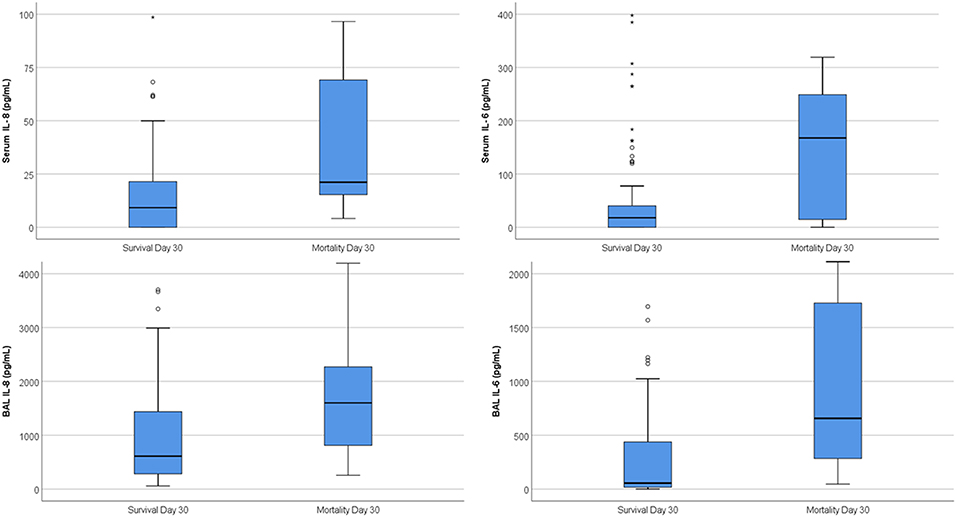
Figure 1. Boxplots of same-day serum and BAL cytokines in those who survived day 30 and those who died. On the boxplot shown here, outliers are identified by different markers. “Out” values (small circle) and “far out” or as SPSS calls them “Extreme values” (marked with a star). SPSS uses a step of 1.5×IQR (Interquartile range).
Sub-analyses for 30-day mortality found that (i) among those with possible, probable or proven IMI serum IL-8 (AUC 0.650), BAL IL8 (AUC 0.693), and BAL IL6 (AUC 0.631) had prognostic potential, while serum-IL-6 did not; (ii) among those with bacterial infections, serum IL-8 (AUC 0.685), BAL IL-8 (AUC 0.756), and BAL IL-6 (AUC 0.685) had prognostic potential, while serum IL-6 did not; (iii) among those with viral infections, only BAL levels of IL-8 (AUC 0.734) and IL-6 (AUC 0.677) had prognostic potential, while serum levels did not; (iv) among those with neutropenia at the time of bronchoscopy, serum levels of IL-6 (AUC 0.691) and IL-8 (AUC 0.642) had some prognostic potential while BAL levels had not; in contrast, BAL IL-8 (AUC 0.920) and BAL IL-6 (AUC 0.862) had very strong prognostic potential among non-neutropenic patients; (v) among those on corticosteroids, BAL IL-6 (AUC 0.831) and BAL IL-8 (AUC 0.728) levels had stronger prognostic potential than serum levels; and (vi) among female patients serum IL-8 (AUC 0.862), serum IL-6 (AUC 0.771), BAL IL-8 (AUC 0.812), and BAL IL-6 (AUC 0.801) had all strong prognostic potential.
Kinetics of Blood IL-6 and IL-8 Before and After Bronchoscopy
In a subset of 62 participants, serial blood samples were obtained from 4 days preceding to 4 days following bronchoscopy (this particular subset had 30-day mortality of 14%, 90-day mortality of 28%, and 180-day mortality of 50%). Kinetics of serum IL-8 and IL-6 levels stratified by categories of overall mortality are displayed in Figures 2, 3 (23 samples tested for Day −4, 42 samples for Day −3, 46 samples for Day −2; 53 samples for Day −1; 62 samples for Day 0; 48 samples for Day +1; 52 samples for Day +2; 46 samples for Day +3; 49 samples for Day +4).
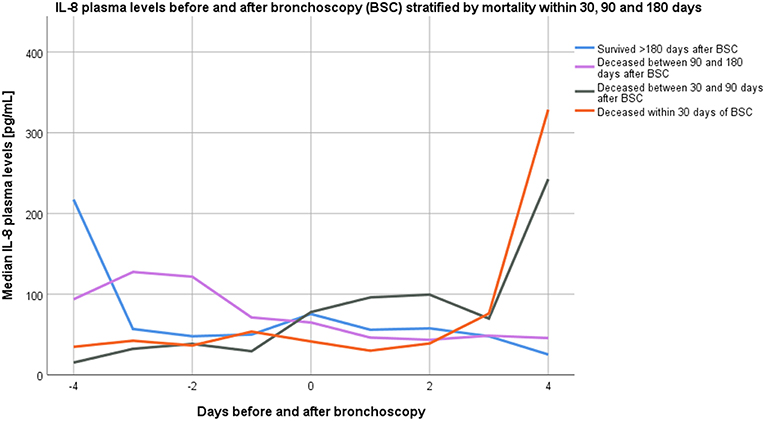
Figure 2. Kinetics of median interleukin-8 plasma levels from 4 days before until 4 days after bronchoscopy stratified by overall mortality categories.
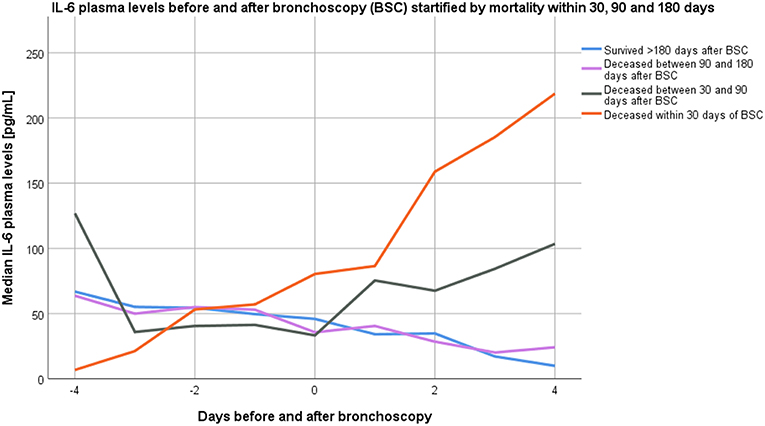
Figure 3. Kinetics of median interleukin-6 plasma levels from 4 days before until 4 days after bronchoscopy stratified by overall mortality categories.
Between the day of bronchoscopy and 4 days following bronchoscopy (samples available from 49 participants on both time points), blood IL-6 levels increased in 14/49 (29%) participants, while blood IL-8 levels increased in 19/49 (39%) of participants. Increasing IL-6 levels at day four were significantly associated with higher 90-day mortality rates [7/13 (54%) died vs. 7/36 (19%) with stable or decreasing levels; p = 0.031], with similar findings for increasing IL-8 levels 4 days following bronchoscopy [9/18 (50%) died vs. 5/31 (16%); p = 0.020]. In ROC analysis, the difference of IL-8 levels between 4 days following bronchoscopy and the day of bronchoscopy had an AUC of 0.829 (95%CI 0.71–0.95; p < 0.001) for predicting 90-day mortality (AUC for IL-6 0.686; 95%CI 0.499–0.872; p = 0.044). AUC for IL-8 difference to predict 30-day mortality was 0.771 (95%CI 0.578–0.963; p = 0.023) and for 180-day mortality 0.680 (95%CI 0.529–0.831; p = 0.031); while differences in IL-6 levels were not significant predictors for 30- and 180-day mortality.
Discussion
We evaluated prognostic potential of IL-6, IL-8, and several fungal biomarkers for overall mortality in a high-risk cohort of hematological malignancy patients (>80% of cases had received mold-active antifungals at the time of sampling) undergoing bronchoscopy for suspected pulmonary mold infection. Two major findings are evident. First, elevated levels of IL-6 or IL-8 in blood or BAL fluid at the time of bronchoscopy was associated with increased 30-day overall mortality. Second, increasing blood levels of IL-8 within the 4 days following bronchoscopy were highly predictive of overall 30- and 90-day mortality.
From prior studies, it is understood that cytokines are centrally involved in protective immunity against Aspergillus spp. and other molds (13, 21) and may therefore be used as an early biomarker for risk stratification regarding IA associated mortality (22). In the early stages of invasive aspergillosis (IA), conidia are killed by local alveolar macrophage and IL-8, also known as neutrophil chemotactic factor, is produced by these macrophages as well as neighboring epithelial cells as an important chemoattractant for neutrophils (11, 21). The mechanism of IL-8 increase during IA has also been studied in vitro where an up-regulation of gene transcription by Aspergillus fumigatus proteases was shown to cause increased release of IL-8 (as well as IL-6, which plays an important role in T cell recruitment) by A549 pulmonary epithelial cells and primary epithelial cells (16). Other studies have shown that in vitro opsonization of Aspergillus fumigatus conidia with H-ficolin, L-ficolin (17), and M-ficolin (which play essential roles in pathogen recognition and complement activation through the lectin pathway) potentiate IL-8 secretion of A549 lung epithelial cells (12, 18, 19). In line, we have previously shown that significantly better diagnostic performances were observed for serum IL-8 and also serum IL-6 when compared to established blood biomarkers (14).
It is worth noting that a number of other conditions/irritants lead to increased levels of IL-6 and IL-8 in both blood and lung environments. Studies have shown increased levels of IL-6 and IL-8 in patients with tobacco smoke exposure and/or chronic obstructive pulmonary disease (20), asthma (23), and influenza infection (24), suggesting these are relatively non-specific cytokines involved in responses to myriad insults that may be visited upon the lungs. These other conditions, including bacterial infections, may have boosted the prognostic potential of these cytokines in our high-risk cohort where IMI was suspected but only confirmed in a subset of cases, as shown in results of our sub-analyses where cytokines were also predictive of overall mortality in those with bacterial and viral infection. As a limitation, prognostic potential of these cytokines may not be limited to patients with confirmed IMI, but may extend to patients with suspected IMI who subsequently are found to have other infections such as bacterial pneumonia. This may, however, also be considered a strength as it would allow for the use of these cytokines more broadly for treatment stratification in hematological malignancy patients with suspected pulmonary infection. While the clinical value of single measurements of cytokines may be more limited (the optimal cut-off for serum IL-8 yielded 82.4% sensitivity but only 61.8% specificity), serial measurements of these cytokines may be more promising. Overall, studies and clinical trials with larger sample sizes are needed to evaluate the prognostic potential of serial measurements of these cytokines for various subgroups of patients.
Limitations
Overall, fungal infections are rare in patients receiving anti-mold prophylaxis, with a prevalence of 2–3% (25, 26), and therefore multicenter studies are needed to confirm our findings in larger cohorts. To avoid bias introduced by multiple comparisons and confounding factors, we also had to rely on results from smaller, nested matched case-control analysis for identification of cytokines that were evaluated in the primary analyses of this cohort study. Case-control pairs in this nested analysis were matched for multiple covariates that may affect cytokine levels (27).
Additionally, autopsies were performed only in a very small subset of deceased patients and it is therefore likely that the 90- and 180-day mortality causes were not directly related to the initial reason for bronchoscopy (e.g., suspected pulmonary infection). It is still interesting that elevated levels of cytokines had predictive value for mortality so far ahead, suggesting there may be a component of specific immune dysregulation related to these cytokines playing a role in mortality in patients with underlying hematologic malignancies.
Conclusion
In conclusion, high blood and BAL IL-8 and IL-6 levels at the time of bronchoscopy and, in particular, increasing cytokine levels over time were predictive of mortality in a cohort of patients with underlying hematologic malignancies presenting with concern for pulmonary infection. These findings suggest it could be possible to create a treatment algorithm incorporating measurement of these cytokines at admission and throughout initial treatment for the purpose of identifying patients who warrant more aggressive treatment (e.g., combination treatment) (28, 29) when IMI is suspected in at-risk individuals.
Data Availability
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical University Graz, Austria (EC-numbers 25-221 and 23-343). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SR, MH, JP, SE, JJ, and SH designed the study and drafted the manuscript. Data were analyzed by MH and SH. Samples were collected by SH, SE, JR, HF, AW, PN, and FP. Samples were analyzed by HS, RK, FP, JR, SH, SE, and JP. The manuscript was critically revised and important intellectual content provided by RK, HS, HF, JR, FP, PN, and AW. The final version for publication was approved by all authors. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This work was supported by funds of the Gilead Investigator Initiated Study IN-AT-131-1939, and also the Gilead Investigator Initiated Study ISR-NL-18-10601 and the Oesterreichische Nationalbank (Anniversary Fund, project number 15346). This work has also partly been carried out with the K1 COMET Competence Center CBmed, which was funded by the Federal Ministry of Transport, Innovation and Technology (BMVIT); the Federal Ministry of Science, Research and Economy (BMWFW); Land Steiermark (Department 12, Business and Innovation); the Styrian Business Promotion Agency (SFG); and the Vienna Business Agency. The COMET program is executed by the FFG (The Austrian Research Promotion Agency, project number 844609), and has been partially supported by grants from the National Institutes of Health (MH113477). The funders had no role in study design, data collection, analysis, interpretation, decision to publish, in the writing of the manuscript, and in the decision to submit the manuscript for publication.
Conflict of Interest Statement
JP received consulting fees from Gilead. AW received speaker honoraria from Merck. RK received research grants from Merck and served on the speakers' bureau of Pfizer, Gilead, Astellas, Basilea, Merck, and Angelini. MH received research grants from Gilead.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors acknowledge the support of Jennifer Ober and Sabrina Obersteiner in sample processing and testing, as well as the team of the Clinical Institute of Medical and Chemical Laboratory Diagnostics in providing routinely collected samples and performing routine, GM and BDG testing.
References
1. Bird GT, Farquhar-Smith P, Wigmore T, Potter M, Gruber PC. Outcomes and prognostic factors in patients with haematological malignancy admitted to a specialist cancer intensive care unit: a 5 yr study. Br J Anaesth. (2012) 108:452–9. doi: 10.1093/bja/aer449
2. Halpern AB, Culakova E, Walter RB, Lyman GH. Association of risk factors, mortality, and care costs of adults with acute myeloid leukemia with admission to the intensive care unit. JAMA Oncol. (2017) 3:374–81. doi: 10.1001/jamaoncol.2016.4858
3. Kontoyiannis DP, Marr KA, Park BJ, Alexander BD, Anaissie EJ, Walsh TJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001-2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin Infect Dis. (2010) 50:1091–100. doi: 10.1086/651263
4. Prattes J, Lackner M, Eigl S, Reischies F, Raggam RB, Koidl C, et al. Diagnostic accuracy of the aspergillus-specific bronchoalveolar lavage lateral-flow assay in haematological malignancy patients. Mycoses. (2015) 58:461–9. doi: 10.1111/myc.12343
5. Jenks JD, Mehta SR, Taplitz R, Aslam S, Reed SL, Hoenigl M. Point-of-care diagnosis of invasive aspergillosis in non-neutropenic patients: aspergillus galactomannan lateral flow assay versus aspergillus-specific lateral flow device test in bronchoalveolar lavage. Mycoses. (2018) 62:230–6. doi: 10.1111/myc.12881
6. Jenks JD, Mehta SR, Taplitz R, Law N, Reed SL, Hoenigl M. Bronchoalveolar lavage aspergillus galactomannan lateral flow assay versus aspergillus-specific lateral flow device test for diagnosis of invasive pulmonary aspergillosis in patients with hematological malignancies. J Infect. (2018) 78:249–59. doi: 10.1016/j.jinf.2018.10.014
7. Jenks JD, Reed SL, Seidel D, Koehler P, Cornely OA, Mehta SR, et al. Rare mould infections caused by Mucorales, Lomentospora prolificans and Fusarium, in San Diego, CA: the role of antifungal combination therapy. Int J Antimicrob Agents. (2018) 52:706–12. doi: 10.1016/j.ijantimicag.2018.08.005
8. Cornish M, Butler MB, Green RS. Predictors of poor outcomes in critically Ill adults with hematologic malignancy. Can Respir J. (2016) 2016:9431385. doi: 10.1155/2016/9431385
9. Scorzoni L, de Paula ESAC, Marcos CM, Assato PA, de Melo WC, de Oliveira HC, et al. Antifungal therapy: new advances in the understanding and treatment of mycosis. Front Microbiol. (2017) 8:36. doi: 10.3389/fmicb.2017.00036
10. Garcia-Vidal C, Viasus D, Carratala J. Pathogenesis of invasive fungal infections. Curr Opin Infect Dis. (2013) 26:270–6. doi: 10.1097/QCO.0b013e32835fb920
11. Camargo JF, Husain S. Immune correlates of protection in human invasive aspergillosis. Clin Infect Dis. (2014) 59:569–77. doi: 10.1093/cid/ciu337
12. Goncalves SM, Lagrou K, Rodrigues CS, Campos CF, Bernal-Martinez L, Rodrigues F, et al. Evaluation of bronchoalveolar lavage fluid cytokines as biomarkers for invasive pulmonary aspergillosis in at-risk patients. Front Microbiol. (2017) 8:2362. doi: 10.3389/fmicb.2017.02362
13. Heldt S, Eigl S, Prattes J, Flick H, Rabensteiner J, Pruller F, et al. Levels of interleukin (IL)-6 and IL-8 are elevated in serum and bronchoalveolar lavage fluid of haematological patients with invasive pulmonary aspergillosis. Mycoses. (2017) 60:818–25. doi: 10.1111/myc.12679
14. Heldt S, Prattes J, Eigl S, Spiess B, Flick H, Rabensteiner J, et al. Diagnosis of invasive aspergillosis in hematological malignancy patients: performance of cytokines, Asp LFD, and Aspergillus PCR in same day blood and bronchoalveolar lavage samples. J Infect. (2018) 77:235–41. doi: 10.1016/j.jinf.2018.05.001
15. De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. (2008) 46:1813–21. doi: 10.1086/588660
16. Borger P, Koeter GH, Timmerman JA, Vellenga E, Tomee JF, Kauffman HF. Proteases from Aspergillus fumigatus induce interleukin (IL)-6 and IL-8 production in airway epithelial cell lines by transcriptional mechanisms. J Infect Dis. (1999) 180:1267–74. doi: 10.1086/315027
17. Bidula S, Sexton DW, Abdolrasouli A, Shah A, Reed A, Armstrong-James D, et al. The serum opsonin L-ficolin is detected in lungs of human transplant recipients following fungal infections and modulates inflammation and killing of Aspergillus fumigatus. J Infect Dis. (2015) 212:234–46. doi: 10.1093/infdis/jiv027
18. Ghufran MS, Ghosh K, Kanade SR. A fucose specific lectin from Aspergillus flavus induced interleukin-8 expression is mediated by mitogen activated protein kinase p38. Med Mycol. (2017) 55:323–33. doi: 10.1093/mmy/myw066
19. Houser J, Komarek J, Kostlanova N, Cioci G, Varrot A, Kerr SC, et al. A soluble fucose-specific lectin from Aspergillus fumigatus conidia–structure, specificity and possible role in fungal pathogenicity. PLoS ONE. (2013) 8:e83077. doi: 10.1371/journal.pone.0083077
20. Grubek-Jaworska H, Paplinska M, Hermanowicz-Salamon J, Bialek-Gosk K, Dabrowska M, Grabczak E, et al. IL-6 and IL-13 in induced sputum of COPD and asthma patients: correlation with respiratory tests. Respiration. (2012) 84:101–7. doi: 10.1159/000334900
21. Winn RM, Gil-Lamaignere C, Roilides E, Simitsopoulou M, Lyman CA, Maloukou A, et al. Selective effects of interleukin (IL)-15 on antifungal activity and IL-8 release by polymorphonuclear leukocytes in response to hyphae of Aspergillus species. J Infect Dis. (2003) 188:585–90. doi: 10.1086/377099
22. Chai LYA, Netea MG, Teerenstra S, Earnest A, Vonk AG, Schlamm HT, et al. Early proinflammatory cytokines and C-reactive protein trends as predictors of outcome in invasive aspergillosis. J Infect Dis. (2010) 202:1454–62. doi: 10.1086/656527
23. Gibson PG, Simpson JL, Saltos N. Heterogeneity of airway inflammation in persistent asthma: evidence of neutrophilic inflammation and increased sputum interleukin-8. Chest. (2001) 119:1329–36. doi: 10.1378/chest.119.5.1329
24. Short KR, Kroeze E, Fouchier RAM, Kuiken T. Pathogenesis of influenza-induced acute respiratory distress syndrome. Lancet Infect Dis. (2014) 14:57–69. doi: 10.1016/S1473-3099(13)70286-X
25. Cornely OA, Maertens J, Winston DJ, Perfect J, Ullmann AJ, Walsh TJ, et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N Engl J Med. (2007) 356:348–59. doi: 10.1056/NEJMoa061094
26. Duarte RF, Sanchez-Ortega I, Cuesta I, Arnan M, Patino B, Fernandez de Sevilla A, et al. Serum galactomannan-based early detection of invasive aspergillosis in hematology patients receiving effective antimold prophylaxis. Clin Infect Dis. (2014) 59:1696–702. doi: 10.1093/cid/ciu673
27. Pruller F, Wagner J, Raggam RB, Hoenigl M, Kessler HH, Truschnig-Wilders M, et al. Automation of serum (1–>3)-beta-D-glucan testing allows reliable and rapid discrimination of patients with and without candidemia. Med Mycol. (2014) 52:455–61. doi: 10.1093/mmy/myu023
28. Marr KA, Schlamm HT, Herbrecht R, Rottinghaus ST, Bow EJ, Cornely OA, et al. Combination antifungal therapy for invasive aspergillosis: a randomized trial. Ann Intern Med. (2015) 162:81–9. doi: 10.7326/M13-2508
Keywords: hematologic malignancy, invasive mold infection, interleukin-6, interleukin-8, prognosis
Citation: Rawlings SA, Heldt S, Prattes J, Eigl S, Jenks JD, Flick H, Rabensteiner J, Prüller F, Wölfler A, Neumeister P, Strohmaier H, Krause R and Hoenigl M (2019) Using Interleukin 6 and 8 in Blood and Bronchoalveolar Lavage Fluid to Predict Survival in Hematological Malignancy Patients With Suspected Pulmonary Mold Infection. Front. Immunol. 10:1798. doi: 10.3389/fimmu.2019.01798
Received: 21 May 2019; Accepted: 17 July 2019;
Published: 02 August 2019.
Edited by:
Agostinho Carvalho, University of Minho, PortugalReviewed by:
Norman Nausch, Heinrich Heine University of Düsseldorf, GermanyCharalampos Antachopoulos, Aristotle University of Thessaloniki, Greece
Copyright © 2019 Rawlings, Heldt, Prattes, Eigl, Jenks, Flick, Rabensteiner, Prüller, Wölfler, Neumeister, Strohmaier, Krause and Hoenigl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Hoenigl, bWhvZW5pZ2xAdWNzZC5lZHU=
†These authors have contributed equally to this work as share first authorship