 Bahaa Abu-Raya1
Bahaa Abu-Raya1 Kirsten Maertens2Kathryn M. Edwards3Saad B. Omer4Janet A. Englund5
Kirsten Maertens2Kathryn M. Edwards3Saad B. Omer4Janet A. Englund5 Katie L. Flanagan6,7,8Matthew D. Snape9Gayatri Amirthalingam10Elke Leuridan2Pierre Van Damme2Vana Papaevangelou11Odile Launay12
Katie L. Flanagan6,7,8Matthew D. Snape9Gayatri Amirthalingam10Elke Leuridan2Pierre Van Damme2Vana Papaevangelou11Odile Launay12 Ron Dagan13Magda Campins14Anna Franca Cavaliere15Tiziana Frusca16
Ron Dagan13Magda Campins14Anna Franca Cavaliere15Tiziana Frusca16 Sofia Guidi15Miguel O'Ryan17
Sofia Guidi15Miguel O'Ryan17 Ulrich Heininger18Tina Tan19
Ulrich Heininger18Tina Tan19 Ahmed R. Alsuwaidi20
Ahmed R. Alsuwaidi20 Marco. A. Safadi21Luz M. Vilca22
Marco. A. Safadi21Luz M. Vilca22 Nasamon Wanlapakorn23
Nasamon Wanlapakorn23 Shabir A. Madhi24,25Michelle L. Giles26Roman Prymula27Shamez Ladhani10
Shabir A. Madhi24,25Michelle L. Giles26Roman Prymula27Shamez Ladhani10 Federico Martinón-Torres28Litjen Tan29Lessandra Michelin30
Federico Martinón-Torres28Litjen Tan29Lessandra Michelin30 Giovanni Scambia15
Giovanni Scambia15 Nicola Principi31and
Nicola Principi31and  Susanna Esposito32* on behalf of World Association of Infectious Diseases and Immunological Disorders (WAidid) and the Vaccine Study Group of the European Society of Clinical Microbiology and Infectious Diseases (EVASG)
Susanna Esposito32* on behalf of World Association of Infectious Diseases and Immunological Disorders (WAidid) and the Vaccine Study Group of the European Society of Clinical Microbiology and Infectious Diseases (EVASG)- 1Department of Pediatrics, University of British Columbia, Vancouver, BC, Canada
- 2Faculty of Medicine and Health Sciences, Centre for the Evaluation of Vaccination, Vaccine and Infectious Diseases Institute, University of Antwerp, Antwerp, Belgium
- 3Division of Pediatric Infectious Diseases, Department of Pediatrics, Vanderbilt University School of Medicine, Nashville, TN, United States
- 4Department of Internal Medicine (Infectious Diseases), Department of Epidemiology of Microbial Diseases, Yale School of Medicine, Yale School of Public Health, New Haven, CT, United States
- 5Department of Pediatrics, Seattle Children's Research Institute, University of Washington, Seattle, WA, United States
- 6Faculty of Health Sciences, School of Medicine, University of Tasmania, Launceston, TAS, Australia
- 7School of Health and Biomedical Science, RMIT University, Melbourne, VIC, Australia
- 8Department of Immunology and Pathology, Monash University, Melbourne, VIC, Australia
- 9Oxford Vaccine Group, Department of Paediatrics, University of Oxford, Oxford, United Kingdom
- 10Immunisation and Countermeasures Division, National Infection Service, Public Health England, London, United Kingdom
- 11Third Department of Pediatrics, University Hospital ATTIKON, National and Kapodistrian University of Athens, Athens, Greece
- 12Université de Paris, Inserm, CIC 1417, F-CRIN I REIVAC, Assistance Publique-Hôpitaux de Paris, Paris, France
- 13The Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel
- 14Preventive Medicine and Epidemiology Department, Hospital Universitario Vall d'Hebron, Barcelona, Spain
- 15Dipartimento Scienze della Salute della Donna e del Bambino e di Sanità Pubblica, Fondazione Policlinico Universitario “A. Gemelli” IRCCS-Università Cattolica del Sacro Cuore, Rome, Italy
- 16Department of Medicine and Surgery, Obstetrics and Gynaecology Unit, University of Parma, Parma, Italy
- 17Microbiology and Mycology Program, Faculty of Medicine, Institute of Biomedical Sciences and Associate Researcher, Millennium Institute of Immunology and Immunotherapy, University of Chile, Santiago, Chile
- 18Pediatric Infectious Diseases, University of Basel Children's Hospital, Basel, Switzerland
- 19Division of Pediatric Infectious Diseases, Department of Pediatrics, Northwestern University Feinberg School of Medicine, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States
- 20Department of Pediatrics, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
- 21Department of Pediatrics, Santa Casa de São Paulo School of Medical Sciences, São Paulo, Brazil
- 22Unit of Obstetrics and Gynecology, Buzzi Hospital - ASST Fatebenefratelli Sacco, University of Milan, Milan, Italy
- 23Center of Excellence in Clinical Virology, Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
- 24Department of Science and Technology/National Research Foundation: Vaccine Preventable Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- 25Medical Research Council: Respiratory and Meningeal Pathogens Research Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- 26Department of Obstetrics and Gynaecology, Monash University, Melbourne, VIC, Australia
- 27School of Medicine Hradec Kralove, Institute of Social Medicine, Charles University Prague, Prague, Czechia
- 28Translational Pediatrics and Infectious Diseases, Pediatrics Department, Hospital Clínico Universitario de Santiago de Compostela, University of Santiago, Santiago de Compostela, Spain
- 29Immunization Action Coalition, St. Paul, MN, United States
- 30Infectious Diseases and Vaccinology Division, Health Sciences Post Graduation Program, University of Caxias Do Sul, Caxias Do Sul, Brazil
- 31Università degli Studi di Milano, Milan, Italy
- 32Department of Medicine and Surgery, Pediatric Clinic, Pietro Barilla Children's Hospital, University of Parma, Parma, Italy
Immunization during pregnancy has been recommended in an increasing number of countries. The aim of this strategy is to protect pregnant women and infants from severe infectious disease, morbidity and mortality and is currently limited to tetanus, inactivated influenza, and pertussis-containing vaccines. There have been recent advancements in the development of vaccines designed primarily for use in pregnant women (respiratory syncytial virus and group B Streptococcus vaccines). Although there is increasing evidence to support vaccination in pregnancy, important gaps in knowledge still exist and need to be addressed by future studies. This collaborative consensus paper provides a review of the current literature on immunization during pregnancy and highlights the gaps in knowledge and a consensus of priorities for future research initiatives, in order to optimize protection for both the mother and the infant.
Introduction
Vaccination of pregnant women induces a vaccine-specific immune response in the mothers and the transfer of vaccine-specific antibodies via the placenta and breastmilk to directly protect the infant during the first months of life from the targeted pathogens (1, 2). The potential of maternal immunization in protecting young infants was made evident by tetanus vaccination during pregnancy contributing to the reduction in incidence of neonatal tetanus (3). This has also become evident by the decrease in the incidence of severe pertussis disease in young infants in countries that have implemented pertussis immunization programs in pregnancy (4–7).
During the last decade, an increasing number of countries have included vaccines for pregnant women in their national vaccination programs. Vaccination with tetanus-containing vaccines in pregnancy has been recommended for years in most low and middle -income countries (LMICs) (3), and pertussis and influenza vaccination programs for pregnant women have been more recently recommended in a number of high-income countries (HICs) and LMICs (Figure 1) (8, 9). Moreover, the prevention of respiratory syncytial virus (RSV) and group B Streptococcus (GBS) infections in infants through maternal vaccination has become a priority and a target for potential new vaccine candidates in trials and development (10–12).
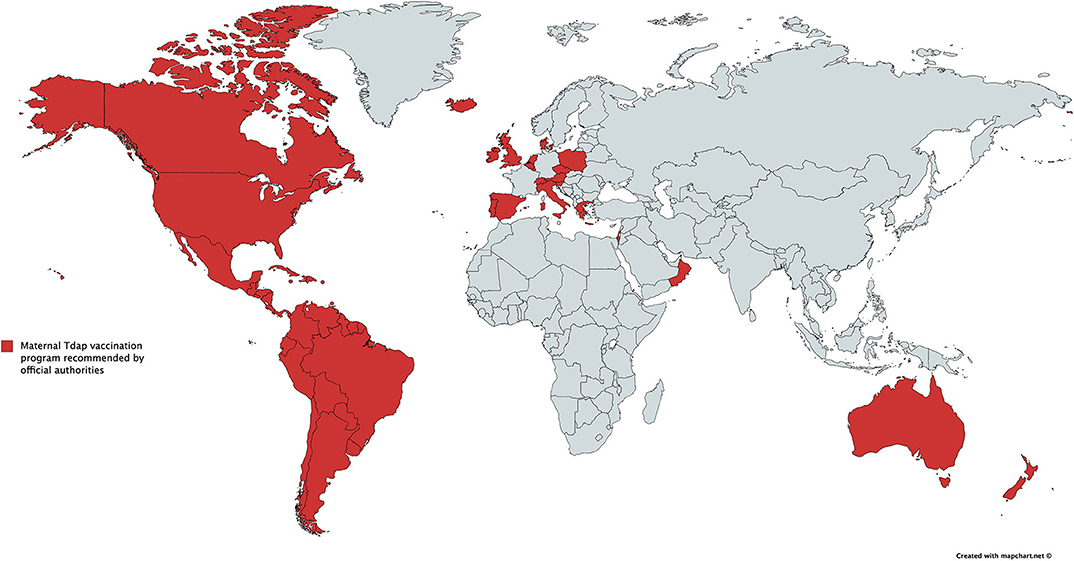
Figure 1. Countries with recommendations for immunization against pertussis in pregnancy by official authorities (for South America, pertussis immunization during pregnancy is recommended by The Pan American Health Organization). This figure was inspired by G. Amirthalingham and K. Maertens and created by K. Maertens.
To optimize the protection offered to mothers and infants by maternal immunization, several factors that can affect this strategy must be better understood (Figure 2). The goal of this consensus paper written by experts in infectious diseases, vaccination and maternal immunization from different world regions is to summarize current evidence in the field of immunization during pregnancy and to highlight the knowledge gaps and prioritize future research strategies in order to optimize protection for the mother, fetus and the infant.
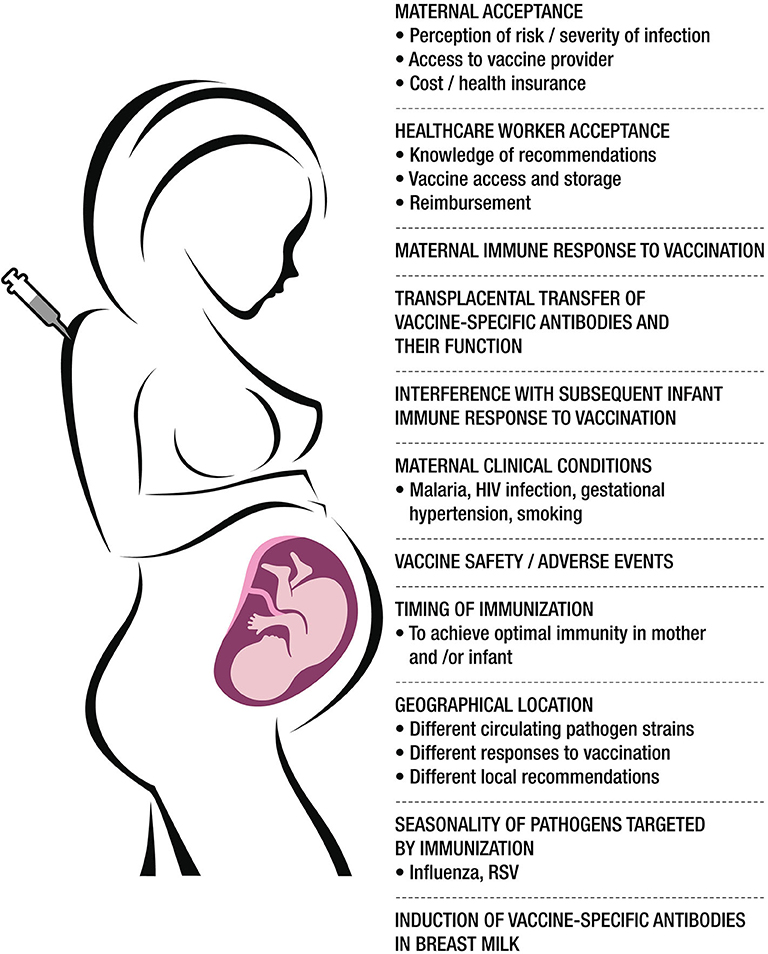
Figure 2. A summary of the major factors affecting vaccination in pregnancy. Created by Claudio Rosa.
Study Design
The main aim of this consensus paper is to discuss current knowledge regarding immunization during pregnancy and highlight the gaps that need to be addressed to ensure the highest protection for both the mother and their infants. References were identified through searches of PubMed for human studies published in English using the terms “immunization” or “vaccination” or “tetanus” or “tetanus disease” or “tetanus vaccine” or “pertussis” or “Tdap” or “pertussis immunization” or “pertussis vaccination” or “pertussis vaccine” or “Tdap vaccine” or “Tdap immunization” or “influenza” or “influenza vaccines” or “influenza immunization” or “maternal influenza vaccination” or “influenza vaccines in pregnancy” or “RSV” or “respiratory syncytial virus” or “GBS” or “GBS vaccine” or “Group B streptococcus” and “pregnancy.” Articles resulting from these searches and relevant references cited in those articles were reviewed. References were also provided by authors. Outcomes assessed were safety, immunogenicity, efficacy, and effectiveness of immunization during pregnancy against tetanus, pertussis, influenza, RSV, and GBS diseases. After the initial review, a meeting was held in Italy to discuss the current literature and knowledge gaps. A consensus on the content was reached after multiple rounds of revision among the authors.
Ethics in Vaccine Trials During Pregnancy
Maternal immunization, and the use of medication in pregnancy in general, have been a focus of ethical deliberations for decades. Until recently, the ethical prevailing approach for immunization during pregnancy was based on the precautionary principle, which limits introduction of new intervention whose ultimate effects are uncertain. This precautionary principle-centered approach, combined with risk aversion among legal departments of vaccine manufacturers, led to exclusion of pregnant women from most vaccine trials for decades, leading to gaps in evidence of vaccine safety and efficacy among pregnant women. With an increasing focus on maternal immunization, there has been reconsideration of relevant ethical paradigms resulting in several recent developments in this area.
First, a report of the U.S. National Vaccine Advisory Committee's Working Group on Maternal Immunization recommended that “Relevant regulations, statutes, and policies…should be modified to indicate that pregnant women are not a vulnerable population for the purposes of ethical review” (13). This recommendation and concurrent policy action led to a change in the U.S. Code of Federal Regulations which had previously classified pregnant women as being inherently vulnerable to coercion (14). Second, recognizing that conventional paradigms often treated the risks and benefits of maternal immunization to mothers and infants as independent entities, a maternal interest-based paradigm was proposed by Chamberlain et al. (15). This paradigm recognizes the legitimacy of maternal interests in protecting their infants and the legitimacy of her taking measures that benefit only the fetus/newborn even if such measures do not have direct benefits for the mother herself. The third major development was creation of the Pregnancy Research Ethics for Vaccines, Epidemics, and New Technologies (PREVENT) working group. This multidisciplinary, international team of 17 experts developed a roadmap for inclusion of the interests of pregnant women in the development and deployment of vaccines (16). The underlying goal of these recommendations was to ensure that pregnant women's inclusion in vaccine trials is the default position and that any exclusions need to be justified rather than justifications being needed for inclusion of pregnant women.
Globally, a progress has also been made in the prioritization of immunization in pregnancy and the inclusion of pregnant women in vaccine trials. The WHO Strategic Advisory Group of Experts on Immunization (SAGE) recommended in 2012 that pregnant women should be highly prioritized for influenza vaccination in countries that consider initiating or expanding of seasonal influenza vaccine programs (17). In 2015, SAGE further emphasized the importance of the platform of immunization in pregnancy, as well the need to strengthen the delivery of vaccines administered during pregnancy (18).
These and other developments in ethical considerations for maternal immunization are likely to result in a more conducive environment for maternal immunization research and deployment. However, there are a few areas that require further deliberations (Table 1).
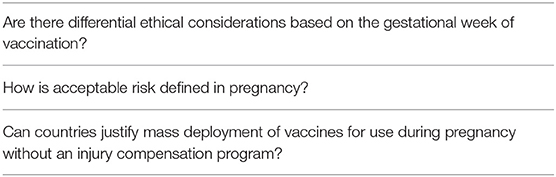
Table 1. Ethics areas related to immunization during pregnancy that require further deliberations.
Safety of Immunization During Pregnancy
Safety of vaccines administered during pregnancy needs to be evaluated for both the mother and her newborn, and is an important consideration for the mothers' willingness to receive a vaccine during pregnancy. There is a significant bulk of evidence to support the safety of immunization with tetanus toxoids (TT), the longest standing vaccine that is recommended during pregnancy. There is also an increasing body of evidence to support the safety of pertussis and influenza immunization during pregnancy (see below specific sections). However, continuous assessment and reporting of adverse events after immunization during pregnancy remains important, especially for relatively newly introduced maternal vaccines (e.g., pertussis), as it informs about rare events that might follow immunization. In addition, assessment of baseline pregnancy outcomes in unvaccinated women in different world regions and settings will help in establishing baselines to assess safety outcomes against.
Furthermore, there is significant heterogeneity and lack of consensus on adverse event reporting in maternal immunization studies. This is a challenge for comparing and pooling data from different studies. In an attempt to overcome this weakness, WHO and the Brighton Collaboration worked together to provide written guidance on how to conduct safety studies in the field of maternal immunization (19). The initiative termed the Global Alignment of Immunization Safety Assessment in Pregnancy (GAIA) project worked on standardizing the assessment of safety of vaccines in pregnancy with specific focus on LMICs (20). Specifically, this initiative proposed systematic data collection, specific case definitions of key obstetric and neonatal health outcomes, ontology of key terms and a map of pertinent disease codes. More recently, case definition and guidelines for data collection, analysis and presentation has been proposed for neonatal seizures, neurodevelopmental delay, chorioamnionitis and post-partum endometritis and infection by the GAIA and Brighton collaboration working groups (21–24). Future studies assessing safety of immunization during pregnancy should use the proposed terms and definitions. In addition, currently available data on safety of vaccination in pregnancy is derived from vaccines that were initially licensed in non-pregnant populations. Future vaccine trials will likely assess vaccines intended to be licensed primarily for use in pregnant women. This further emphasizes the need to standardize reporting of safety outcomes in maternal immunization trials. Thus, we recommend following the GAIA and Brighton collaboration guidelines for assessment and reporting of safety outcomes in maternal immunization trials.
Key Factors That Influence Immunogenicity and Efficacy/Effectiveness of Immunization During Pregnancy
Immune Responses of Pregnant Women to Vaccination
The immune system of a pregnant woman is adapted to allow for the survival of the semi-allogeneic fetus. Serum estradiol levels increase up to 500-fold during normal pregnancy (25), and the interplay between sex hormones and the maternal immune system in pregnancy is complex (Table 2). These changes might lead to the assumption that there are differences in immune responses to vaccines between healthy pregnant and non-pregnant women potentially leading to a lower immune response in pregnant women. However, studies comparing immunogenicity of vaccines in pregnant and non-pregnant women have generally not demonstrated decreased antibody responses in pregnant women. This has been the case for TT (40) and for the pertussis antigens in the combined tetanus, diphtheria, and acellular pertussis vaccine (Tdap) (41). However, results for influenza vaccines have been less consistent. Some studies carried out with influenza vaccines, including both the pandemic H1N1/2009 (pH1N1/2009) monovalent inactivated vaccine (MIV) and seasonal trivalent inactivated vaccine (TIV) preparations, show similar hemagglutination inhibition (HAI) seroconversion rates and antibody titers in pregnant and non-pregnant women (42–44). Other studies showed lower seroconversion rates and lower HAI geometric mean titers after vaccination of pregnant women when compared to non-pregnant women (45–47).
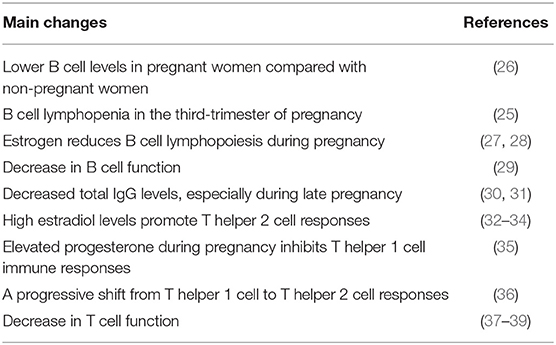
Table 2. Key changes in maternal adaptive immune system during pregnancy.
The effect of maternal immunization on cellular immunity has been less studied limiting conclusions. Proliferative and interferon-γ responses to the Bordetella pertussis (B. pertussis) antigens pertussis toxin (PT) 1 month after receipt of Tdap vaccine were not significantly different in pregnant and non-pregnant women and were comparable in both after 1 year (41). A small study showed that Natural killer cell and T-cell responses to inactivated influenza vaccination (IIV) were higher in a pregnant women compared to non-pregnant women (48).
Trans-placental Transfer of Maternal Antibodies
Immunoglobulin G (IgG) is the dominant immunoglobulin isotype that crosses the placenta and contributes to maternally derived passive immunity during early infancy. In healthy pregnant women, IgG transfer across the placenta begins toward the end of the first trimester of pregnancy and increases as pregnancy progresses. IgG concentrations in the fetus are 5–10% of the maternal levels at 17–22 weeks gestation, 50% at weeks 28–32, and usually exceed maternal levels by 20–30% at term (49–52). The transplacental transfer of IgG is mediated by the neonatal Fc receptors (FcRn), localized in the syncytiotrophoblast that covers the villous tree of the placenta (53). FcRn regulates IgG transplacental transfer through binding to its constant domain and actively transport IgG into the fetal circulation. Several factors appear to affect the transfer of IgG across the placenta. IgG subclasses have differential efficiency of transfer across the placenta, defined as the antibody levels in the newborn divided by antibody levels in the mother. Based on studies from the 1990s, IgG1 is the subclass transferred with the highest efficiency, achieving higher levels in cord compared with the maternal blood, and this subclass is induced by vaccines containing protein antigens (54). IgG2 is transferred with the least efficiency, achieving lower cord than maternal blood levels, and is the dominant antibody induced by vaccines containing polysaccharide antigens (53, 55–58). Transfer of antibodies across the placenta can also be influenced by several clinical conditions in the mother and some of these health conditions are more prevalent in certain parts of the world. For instance, cord IgG levels were lower in infants from women with human immunodeficiency virus (HIV) infection (59), malaria infection (60), and hypergammaglobulinemia (61), compared with infants from women without those conditions, and these conditions are more prevalent in LMICs. In addition, the potential effect of toxoplasma and tuberculosis infection on the transfer of maternal antibodies has not been investigated. Furthermore, other maternal conditions, that have not yet been investigated, might also affect the structure of the placenta (e.g., gestational hypertension, gestational diabetes, smoking) and the transfer of maternal antibodies.
Timing of Immunization
A number of factors should be considered when determining the ideal timing of vaccination in pregnancy including time-dependent safety when administered at different time points in gestation, time-dependent efficiency of transplacental transfer of vaccine-induced antibodies, interference with infants' immune response to vaccination and clinical efficacy/effectiveness (62, 63). Furthermore, the optimal timing of maternal immunization varies depending on who is the target for protection and when maximal protection is desired in the mother and/or the fetus/infant (62). For example, pregnancy is a well-known risk factor for severe influenza, being most severe during the third trimester of pregnancy (64, 65). Therefore, to maximize the protection for the mother, it is best to administer the influenza vaccine early in pregnancy and ideally prior to the peak of influenza seasonal activity. If the primary goal is to protect the infant, as for pertussis, the vaccine should be administered during a time period in gestation to provide optimal trans-placental transfer of antibodies, in order to ensure maximal protection against pertussis disease in early infancy (66). The risk for premature labor should also be considered as this population is at an increased risk for severe infections, such as pertussis and might not benefit from maternal vaccination if it happens late in gestation (67–69).
Based on the literature review and consultation among authors, a consensus on priorities for future research related to factors affecting immunization during pregnancy was reached (Table 3).
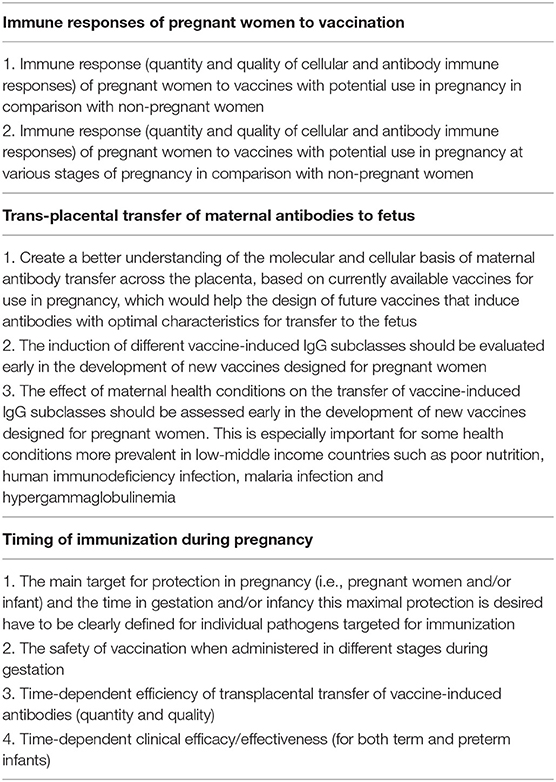
Table 3. Consensus on priorities for future research related to factors that influence the immunogenicity and efficacy/effectiveness of immunization during pregnancy.
Vaccines Currently Recommended for Pregnant Women
Vaccines currently recommended and used are aimed to protect against tetanus, pertussis and influenza diseases. Different vaccine formulations and dosages exist for use in pregnant women in selected countries in Europe, North America, South America, and Asia (Table 4).
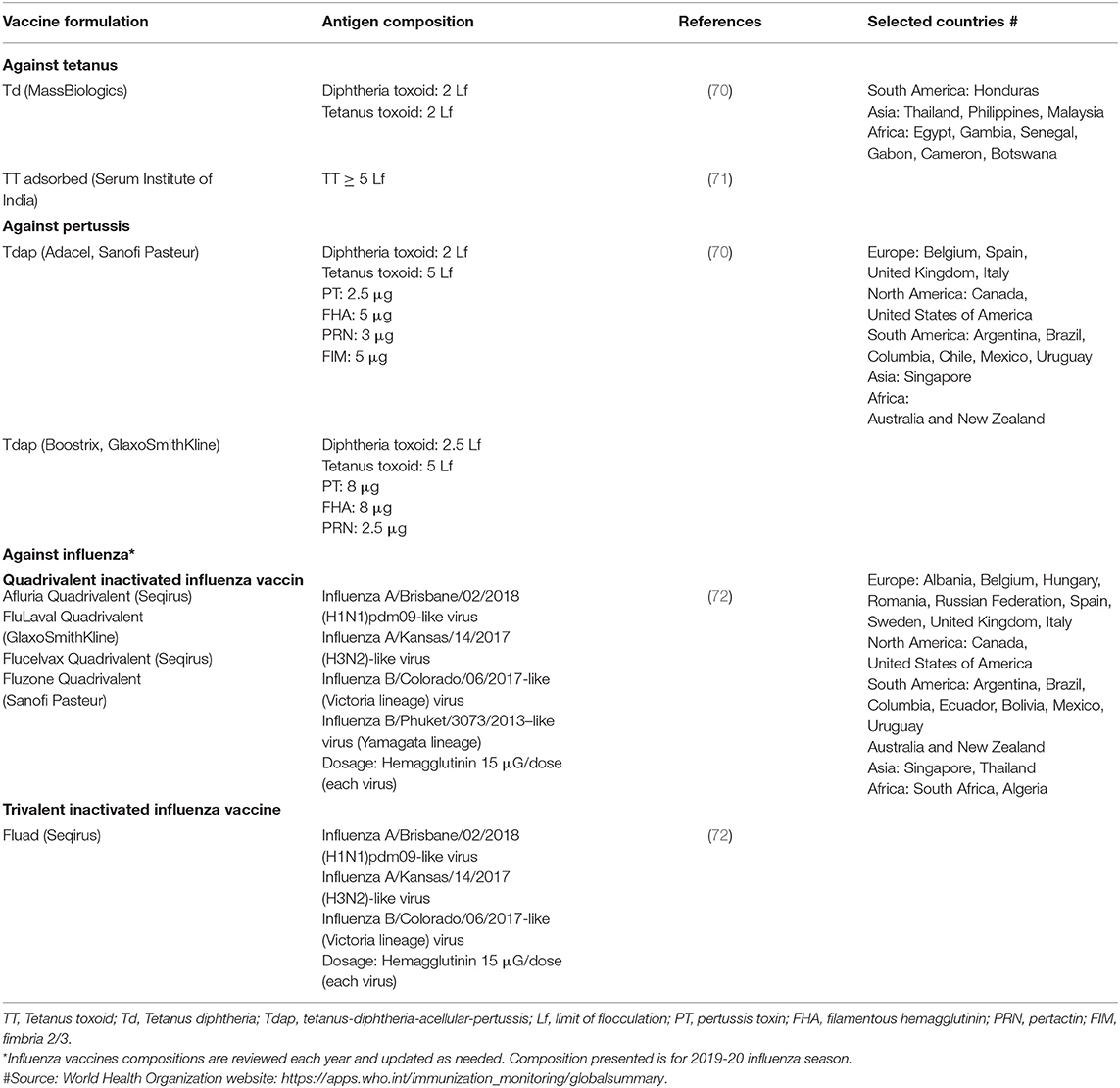
Table 4. Formulations and dosages of common vaccines to protect against pertussis, and tetanus disease for use in pregnant women in selected countries in Europe, North America, South America, and Asia.
Vaccines Against Tetanus
The World Health Organization (WHO) recommends that if a pregnant woman has never received a tetanus-toxoid -containing vaccine (TT-CV) (e.g., Diphtheria-Tetanus-Pertussis [DTP], Diphtheria-Tetanus [DT], Tetanus-diphtheria [Td], TT) or her vaccination status is unknown, she should receive two TT (or Td) vaccine doses 4 weeks apart during pregnancy, with the second dose given at least 2 weeks before delivery. Based on WHO recommendations, five total doses are likely needed for protection throughout the childbearing years so a third dose is given 6 months after the second dose, and two additional doses are recommended to be given during the next 2 years or during two subsequent pregnancies (73). For women who have received 1–4 TT-CV doses prior to their pregnancy, one TT-CV dose is recommended during each subsequent pregnancy to a total of five doses. However, this vaccination schedule and policy has never been formally evaluated in clinical trials.
Safety
Several studies have demonstrated TT-CVs to be safe in pregnancy (74–76). As the current pertussis-containing vaccines administered in pregnancy are part of multicomponent formulations that include TT, safety assessments of pertussis-containing vaccines in pregnancy also provide information on the safety of the TT component (see below discussion under pertussis vaccines) (77). Safety was demonstrated even when the most recent TT-CV was administered within 2 years prior to vaccination in pregnancy (76).
Immunogenicity
Several studies have shown that following maternal immunization with TT-CVs, anti-TT IgG is actively transferred across the placenta, leading to protective levels in the infant (77–80). Vaccination with TT induces IgG1 (54, 81), which are efficiently transferred across the placenta. Approximately 80% of maternal antibodies remain present in infants 1 month after delivery; thus, protection is maintained until a primary vaccination course is commenced and is maximal during the most vulnerable period when umbilical infections may occur (82).
If a Tdap vaccine in pregnancy is being considered to replace a single dose of TT vaccine in some settings, in order to provide dual coverage for pertussis and tetanus disease, it is important to assess the immunogenicity of Tdap in inducing anti-TT IgG compared with TT or Td formulations. In a small study from Vietnam, vaccination with Tdap in pregnancy resulted in higher cord anti-TT IgG levels compared with vaccination with TT, however, this difference did not persist at 2 months of age (83). These results are reassuring that replacing TT with Tdap is not expected to result in inferior immunogenicity against tetanus.
Effectiveness
Both maternal and neonatal tetanus were very common in most developing countries even into the 1980's. In 1989, the WHO called for the elimination of maternal and neonatal tetanus by the end of the century. At that time, 59 countries reported maternal and neonatal tetanus. As part of the MNTE program, and along with safer birth techniques and effective immunization strategies in children and adults, more than 150 million women were vaccinated against tetanus during pregnancy. Altogether, these practices contributed to the elimination of maternal and neonatal tetanus in 45/59 countries as of the end of 2018 (84, 85). However, 14 countries, mainly in Africa, still have residual maternal and neonatal tetanus, highlighting that additional efforts are required to extend maternal immunization, immunization of children and adolescents, and other hygienic measures aimed at improved cord-care. The WHOs most updated goal is to achieve maternal and neonatal tetanus elimination by 2020 which will be difficult to achieve (85).
Based on the literature review and consultation among authors, a consensus on priorities for future research related to immunization against tetanus during pregnancy was reached (Table 5).
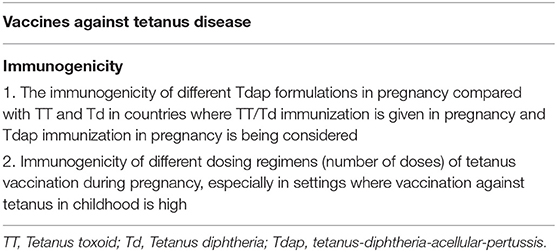
Table 5. Consensus on priorities for future research related to vaccination against tetanus during pregnancy.
Vaccines Against Pertussis
Safety
Data on tolerability and safety of pertussis immunization during pregnancy are reassuring (86). This has been demonstrated with different Tdap vaccine formulations regardless of the number of pertussis antigens included in the vaccines (77, 87–96). Specifically, no increased risk for the development of severe maternal adverse events (e.g., postpartum endometritis, preterm delivery, and preterm premature rupture of membranes) or fetal and neonatal outcomes (e.g., low birth weight, very low birth weight, small for gestational age, birth defects, and need for neonatal intensive care unit admission) has been reported. However, a small increased risk of chorioamnionitis among Tdap-vaccinated women (relative risk [RR] 1.19, 95% CI, 1.13 to 1.26) was documented in one study (89). In another study using the Vaccine Adverse Event Reporting System database, the majority of these women with chorioamnionitis had at least one risk factor for this complication (97). In addition, there was limited supportive evidence for a chorioamnionitis diagnosis on chart review and the risk of preterm birth (a concern after chorioamnionitis) was not higher among Tdap recipients. Therefore, the association between this complication and vaccination during pregnancy has been debated. However, a recent study reported a small increase of chorioamnionitis in pregnant women who received Tdap vaccine during pregnancy with a RR of 1.11 (95% CI: 1.07–1.15); but the absolute risk was still quite low, at 2.8% (98). Ongoing studies are currently evaluating the potential association between Tdap vaccination during pregnancy and chorioamnionitis. In view of the recommendation to vaccinate against pertussis during each pregnancy, it has been shown that repeated Tdap vaccinations in consecutive pregnancies are well-tolerated (76).
Immunogenicity
Vaccination against pertussis in pregnancy has been achieved using Tdap formulations that include mostly three or five B. pertussis antigens. Antibodies against all B. pertussis antigens included in the Tdap vaccine have been shown to reach peak levels at the end of the second week after Tdap administration in non-pregnant women of childbearing age, and this peak is followed by a rapid decline (99). In pregnant women, studies have shown a significant increase in B. pertussis-specific antibody levels 1 month after Tdap vaccination, also with a significant decline, within the first year after maternal vaccination (41, 100, 101). Thus, the persistence of antibodies after a single dose of Tdap vaccine in pregnancy is short and does not probably ensure infant protection during consecutive pregnancies. Therefore, vaccination is currently recommended in every pregnancy.
Vaccination with B. pertussis antigens induces mainly IgG1 antibodies (102, 103) which are actively across the placenta to the newborn resulting in higher antibody levels in the term newborn than in the mother (77, 80, 104).
Pertussis toxin is a major virulence factor of B. pertussis and is potentially responsible for both local and systemic responses (105). Administration of humanized neutralizing anti-PT monoclonal antibodies have been shown to abolish disease manifestations in mice and non-human primates (106). Maternal immunization with a monocomponent PT vaccine protected newborn baboons against pertussis following respiratory challenge with B. pertussis (107). In human, low anti-PT IgG levels have been associated with high susceptibility to pertussis (108). However, antibody levels that confer protection against human pertussis disease have not been defined. In addition, the number and type of B. pertussis antigens are required for pregnant women in order to provide clinical protection to the infant has not been clearly established.
Timing
A study conducted in Thailand showed that vaccination earlier in pregnancy was associated with higher B. pertussis-specific cord antibody levels (109). Furthermore, three other studies found that vaccination during the early third trimester of pregnancy is associated with higher cord anti-B. pertussis-specific IgG levels than immunization during late third trimester (110–112). In addition, one study showed that anti-PT and anti-FHA IgG levels were higher in cord blood of mothers vaccinated between 13 and 25 weeks gestation compared to those immunized after 25 weeks gestation (113). This was also observed in preterm infants (114). In addition, avidity of cord anti-PT IgG was higher when mothers were vaccinated in the early third trimester compared with late third trimester (115, 116), although this finding was not observed in a third study (117). Therefore, more data are needed to address this controversy, including also data from vaccination at earlier time points in pregnancy. Moreover, because the role of antibody levels and avidity in protection against pertussis is not conclusive to date, interpretation of the above studies requires caution.
Effectiveness
Effectiveness of maternal immunization for prevention of pertussis in young infants has been well-studied. In England, vaccine effectiveness was 91% in the reduction of laboratory-confirmed cases in infants <3 months of age (6), and 93% in prevention of laboratory-confirmed cases in infants <8 weeks of age (118). In the US, effectiveness among infants <8 weeks of life ranged between 85 and 91% (7, 119, 120). In addition, disease was significantly less severe among infants from vaccinated mothers (119). In Spain, a case-control study reported VE to be 90% against laboratory-confirmed pertussis infection in infants <3 months of age (121), while in Australia it was 69% in infants <3 month of age (122). In Brazil, vaccine effectiveness was reported to be 82.6% for the prevention of clinical pertussis in infants <2 months of age, confirming the success of the maternal pertussis immunization strategy also in middle-income countries (123).
Based on the literature review and consultation among authors, a consensus on priorities for future research related to immunization against pertussis during pregnancy was reached (Table 6).
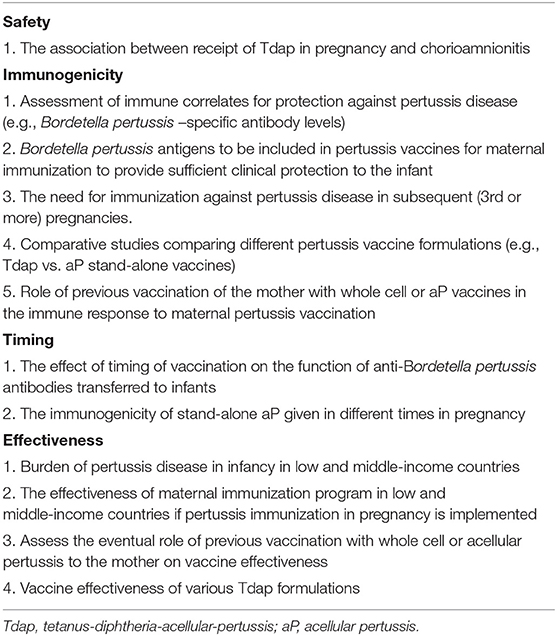
Table 6. Consensus on priorities for future research related to vaccination against pertussis disease during pregnancy.
Vaccines Against Influenza
Safety
There is an extensive body of evidence in the literature from both HICs and LMICs that confirm the safety of maternal influenza vaccination (124–129) [reviewed in (130)]. During the H1N1 influenza pandemic, data from Sweden and Argentina found that both AS03-adjuvanted and MF59-adjuvanted -H1N1 influenza vaccines were not associated with increased risk for low-birth weight or preterm birth or low Apgar score (131, 132). A meta-analysis including studies using both adjuvanted and non-adjuvanted influenza vaccines found lower estimates of still birth after maternal influenza vaccination and no association with an increased risk of spontaneous abortion (133). However, a small case-control study in the US over two influenza seasons (2010–11, 2011–12) found an increased risk of early spontaneous abortion in a group of women who had received influenza vaccination in the first trimester of pregnancy, although cases had other risk factors for spontaneous abortion (older age, pervious history of spontaneous abortion, smoking); thus the causal relationship between influenza vaccination and this complication has been questioned (134). To further support the safety of influenza vaccination in pregnancy, three Bill & Melinda Gates Foundation funded studies from South Africa (135), Mali (136), and Nepal (137), and recent studies and systematic reviews found that maternal influenza vaccination was not associated with an increased risk of fetal death, spontaneous abortion, or congenital malformations (138–141).
Furthermore, concomitant or sequential vaccination with Tdap and influenza vaccines has also been shown to be safe and not associated with differences in medically attended acute events in pregnant women or adverse birth outcomes (142).
Immunogenicity
Influenza vaccination preferentially induces IgG1 subclass antibodies (143), and studies have shown increased levels of influenza-specific hemagglutinin antibodies in neonates born to women given a monovalent (pH1N1/09) or seasonal TIV during pregnancy, suggesting efficient transplacental transfer of influenza-specific antibodies (144–146). Importantly, seroconversion rates were lower after administration of TIV in women living with HIV than in women without HIV, and hemagglutination-inhibiting antibodies (HIA) titers were lower in HIV-exposed infants (146).
The kinetics of influenza antibody decline in the infant vary according to the influenza virus and the levels of transferred antibodies, and thus the duration of protection is not precisely defined. Some data indicate that maternally-derived HIA against seasonal influenza viruses have a half-life of approximately 45 days in infants after maternal vaccination and that these antibodies decline to levels similar to those detected in infants born to unvaccinated women by 16 weeks of age (147, 148). This is consistent with higher protection from laboratory-confirmed influenza disease among infants of vaccinated mothers during the first 2–3 months of age (135, 136).
In another study, children born to mothers vaccinated with an adjuvanted pH1N1 vaccine had antibody levels that remained elevated above the correlate of protection for adults (HIA titer > 1:40) up to 5 months (149). However, the interpretation of influenza immunogenicity studies are complicated as the correlate of protection against infection in infants has not yet been established and is likely to be different and higher than the correlate of protection used for adults (150). This is an area of controversy, where more research is needed to define the correlate(s) of protection against influenza disease in infants, which is important as currently available pediatric influenza vaccines are recommended in certain settings from 6 months of age onwards.
Timing
The optimal timing for maternal influenza immunization has not been established, and recommendations (e.g., CDC, ECDC, WHO) allow administration at any time during pregnancy (17, 151, 152). Importantly, since influenza is a seasonal disease (except in tropical regions, where influenza disease may occur throughout the year) and the goal of vaccination also serves to protect the mother, the actual determination of timing may depend on factors other than optimizing antibody transfer to the infant. Jackson et al. reported lower antibody levels at birth in infants of mothers vaccinated earlier during pregnancy (144). On the other hand, Sperling et al. did not find a significant association between the gestational age at vaccination and the seroconversion rates following influenza vaccination in pregnant women. However, maternal seroconversion rates were slightly lower in women immunized in the first trimester than in those given the vaccine in the late third trimester (153). In another study, a higher level of transplacental transfer of antibodies was associated with a longer interval between vaccination and delivery in pregnant women vaccinated against influenza after 20 weeks gestation (146). Blanchard-Rohner et al. showed that receipt of influenza vaccine at least 2 weeks before delivery increased umbilical cord HIA titers and seroprotection rates in newborns (154). Finally, Katz et al. found no significant differences in influenza HIA titers in cord sera of women vaccinated early (17–25 weeks gestation) or later (26–34 weeks gestation) in randomized trials during pregnancy (155).
Efficacy
Influenza can be a severe disease for pregnant women, neonates and young infants. The severity of infection increases as pregnancy advances, with the greatest maternal risk occurring during the third trimester of pregnancy (156, 157). Young infants on the other hand, have been shown to experience the highest rates of influenza-related hospitalization (158) and death (159) among children with influenza infection.
Multiple studies have shown that administration of an IIV during pregnancy reduces the risk of influenza in pregnant woman by ~35–50% (135, 160–162). The efficacy of maternal influenza vaccination against laboratory-confirmed influenza in infants below 6 months of age also varies in different trials conducted at different geographic sites. Efficacy has been 63% (95% CI, 5–85) in Bangladesh (162), 49% (95% CI, 12–70) in South Africa (135), 33% (95% CI, 4–54) in Mali (136), and 30% (95% CI, 5–48) in Nepal (137). Efficacy against laboratory-confirmed influenza in infant was higher in the first 2–3 months of life and in the range of 70–80% in 2 RCTs from South Africa and Mali (135, 136). Observational studies carried out in the USA (163, 164) and England (165), reported reductions of laboratory-confirmed influenza in children born to vaccinated mothers ranged from 41 to 71%. A recent meta-analysis reported that maternal influenza vaccination reduced the risk of laboratory-confirmed influenza infection in infants by 48% (95% CI, 33–59) (166). In addition, maternal influenza vaccination was associated with a reduction in all-cause severe pneumonia in infants. An analysis of three Bill & Melinda Gates foundation -funded clinical trials conducted in Nepal, Mali and South Africa including 10,002 mothers and 9801 live-born eligible infants concluded that the pooled incidence rate of severe pneumonia up to 6 months of age was 20% lower in infants born to women vaccinated with IIV compared with infants born to women unvaccinated in pregnancy (incidence rate ratio [IRR]: 0.80; 95% CI: 0.66–0.99) (167). However, it should be noted that few of these cases had influenza identified despite testing suggesting that influenza vaccination during pregnancy might have benefits beyond the prevention of classical influenza disease.
The efficacy of IIV in pregnancy in the prevention of maternal and infant influenza disease varies depending on the setting as well as the match of the vaccine utilized to circulating influenza strains. The majority of efficacy data are derived from studies performed in LMICs when compared to HICs. While influenza disease is seasonal in countries with temperate climates (e.g., Europe, North America), there is no seasonal pattern in tropical countries.
Altogether, current data on safety, immunogenicity, and efficacy of maternal IIV vaccination, for the pregnant women and their infants has resulted in pregnancy as a potential indication in the vaccine label by the European Medicines Agency as of July, 2019 (168). In Australia, categorization of influenza vaccines given during pregnancy has changed to category A (no proven harmful effects) (169). Other individual countries will have their own considerations.
Based on the literature review and consultation among authors, a consensus on priorities for future research realted to immunization against influenza during pregnancy was reached (Table 7).
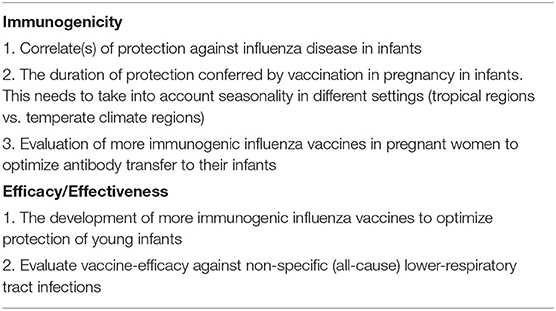
Table 7. Consensus on priorities for future research related to vaccination against influenza disease during pregnancy.
Impact of Maternal Immunization on Infants' Immune Responses to Immunization
High levels of vaccine-induced maternally-derived antibodies have the potential to reduce the infants' humoral immune responses by inhibiting antibody generation after the infant's own vaccination, leading to lower antibody levels/titers later on in the infant (170, 171). This phenomenon is called “interference” or “blunting” and has been described for the same vaccine antigens used by mother and infant, as well as for conjugated vaccines administered in infancy (172). Data from the 1990s showed that the administration of Haemophilus influenzae type b (Hib) polysaccharide or Hib conjugated vaccines in pregnant women was associated with mild inhibition of infants' immune responses to Hib conjugated vaccines (173). Differences in antibody responses in infants born to vaccinated compared with unvaccinated mothers were minimized following the booster dose. An analysis of the genetic repertoire of the light chain of antibodies to the polysaccharide vaccine demonstrated no differences between infants born to immunized women compared with non-immunized women (174). There was no evidence of inhibition of “priming” of the infants' immune system to Hib in these studies.
Tetanus-Containing Vaccines
Most data on the impact on TT-CVs in infancy are derived from studies that used Tdap formulations in pregnancy and measured anti-TT IgG levels after infant vaccination. These studies found inconsistent results. Some showed significantly lower anti-TT levels after primary immunization in infants born to Tdap-vaccinated women compared to infants from unvaccinated women whilst other studies showed equal or even significantly higher anti-TT levels in infants born to Tdap-vaccinated women compared to infants from unvaccinated women (77, 80, 175–177). However, this inhibition found in some studies did not result in a reduction of the percentage of infants with seroprotective anti-TT antibody levels.
The effect of different TT-CV formulations used in pregnancy (Tdap vs. TT/Td) on immune responses to tetanus-containing vaccines in infancy is of importance in countries where a replacement of the existing tetanus vaccination program by a Tdap vaccination program is being considered. A small study in Vietnam reported higher anti-TT levels after primary immunization with tetanus-containing vaccines in infants born to Tdap-vaccinated pregnant women compared to infants born to TT-vaccinated pregnant women (83). A study from Canada found no difference in anti-TT levels after primary and booster immunization in infants born to Tdap-vaccinated pregnant women when compared to Td-vaccinated pregnant women (104). These data suggest that Tdap, when compared to TT or Td in pregnancy, is not associated with lower anti-TT IgG levels after primary and booster immunization with tetanus-containing vaccines in infancy. However, in order to provide a definite conclusion, formal studies should be conducted with the aim to address this question as the primary outcome.
Several vaccines are conjugated to TT as a carrier protein (e.g., Hib vaccines, meningococcal vaccines) and thus vaccine-induced immune responses to these vaccines in infant born to Tdap-vaccinated pregnant women might also be affected. Hib anti-polyribosylribitol phosphate (PRP) levels were higher after primary immunization with Hib TT-conjugated vaccine in infants born to Tdap-vaccinated pregnant women when compared to infants of unvaccinated mothers (175, 178).
One study found no differences between anti-Men C antibody levels after primary immunization with meningococcal C TT-conjugated vaccine in infant born to Tdap-vaccinated when compared to unvaccinated pregnant women (178). More studies are needed to investigate the potential effect of tetanus-containing vaccines administered in pregnancy on infants' immune response to vaccines conjugated to TT.
Pertussis Vaccines
Studies have shown that Tdap immunization in pregnancy is associated with decreases in humoral immune responses to infants' immunization with acellular pertussis (aP) containing vaccines. Several studies describe significantly lower anti-PT IgG levels in infants born to Tdap-vaccinated pregnant women after the completion of primary immunization, while results were less consistent after booster immunization (77, 80, 83, 104, 175–177). Results from these studies showed also interference to other pertussis antigens (FHA, pertactin, fimbria 2/3) after primary immunization while results were inconsistent after booster immunization.
Most studies investigating the potential modification of infants' immune responses to aP vaccines have been performed in HICs, with the exception of one study from Vietnam (83, 177). It is important to note that the degree of reduction in immune responses to wP infant vaccines might be different than to immunization with aP infant vaccines. The use of wP vaccines but not aP vaccines was associated with a substantial reduction in the subsequent infant antibody response to PT in infants born to mothers with high levels of maternally-derived anti-PT antibodies (179). In another study, there was no correlation between low anti- B. pertussis antibody levels at delivery in infants born to unvaccinated women and their anti-B. pertussis antibody levels after wP vaccination (180).
A recent study reported that Thai infants born to unvaccinated mothers and subsequently vaccinated with wP vaccines, had higher anti-B. pertussis-specific antibody levels after primary and booster vaccination than infants born to women vaccinated with Tdap during pregnancy and vaccinated with wP vaccines (181). In addition, infants born to women vaccinated with Tdap in pregnancy and vaccinated with wP vaccines had lower anti- B. pertussis-specific antibody levels after vaccination when compared with infants born to vaccinated mothers and vaccinated with aP vaccines (181).
Altogether, these results indicate that infants born to Tdap-vaccinated mothers might be at increased risk for pertussis later in life. However, surveillance data from the US and UK did not demonstrate any increase in the number of pertussis cases later in infancy after the introduction of the maternal immunization program suggesting a possible lack of clinical significance of this interference (6). Interpretation of interference to wP immunization is more challenging in LMICS compared with HICs due to the lack of comprehensive surveillance systems in some countries (182).
Because vaccines against pertussis that are currently used in pregnancy also contain dT, interference might also be extended to diphtheria-containing vaccines administered in infancy. Data on this respect have been inconsistent, with some studies reporting significantly lower anti-diphtheria toxin antibody levels in infants born to Tdap-vaccinated women when compared to infants born to unvaccinated women, while other studies did not report this effect (77, 80, 83, 104, 175–177). It is also important to note that Tdap immunization in pregnancy, likely due to anti-DT antibodies, is associated with lower anti-pneumococcal capsular polysaccharide levels after immunization with pneumococcal vaccines (PCVs) conjugated to a non-toxic diphtheria toxin mutant (CRM197), although, this did not result in lower seropotection levels for most serotypes (175, 183). Surveillance will be key to assess whether this interference has any impact on pneumococcal disease burden.
If long-term surveillance data would indicate that interference is clinically significant, strategies to mitigate the effect of interference will need to be evaluated. Timing of vaccination in pregnancy is an important modifiable variable and should be investigated. Delaying primary infant vaccination is another approach and has been recently implemented in The Netherlands in infants born to Tdap-vaccinated mothers. In addition, stand-alone pertussis vaccines (without TT, dT) should be investigated in clinical trials (184) as these vaccines might lessen the concern of interference to TT and DT components and vaccines conjugated to those proteins as carrier proteins.
Influenza Vaccines
Data on the potential impact of maternal influenza immunization on the immune response of infants to their immunization against influenza are scarce as influenza vaccines are administered in infants older than 6 months, when most maternally-derived antibodies already have waned from infant's circulation. Earlier studies performed to assess immunogenicity of influenza vaccination in infants younger than 6 months old found that post vaccination seroprotection rates (titer ≥ 1:40) were higher in infants who received IIV at 6 months of age when compared to infants who received vaccination during 6–12 weeks of age (185). Another prospective, open-label study in which 2 doses of a TIV were administered to healthy infants aged 3–5 months found a 4-fold increase in antibody titers to be significantly more common in children who were seronegative (pre-vaccination titers <1:8) at enrollment than in those with pre-vaccination titers ≥1:8 (186).
Mechanism of Interference
Mechanism of interference between maternally-derived antibodies and infant's immune responses to subsequent immunizations has not been fully explored (187). Some proposed mechanisms include inhibition of B cell response to vaccine antigens through epitope masking by maternal antibodies (172) and neutralization of vaccine antigens (187, 188). Inhibition of B cell activation through crosslinking of FcγRIIB to the B-cell receptor on B cells has also been proposed. Specifically, vaccine antigen–antibody complexes cross-link the B-cell receptor (which recognizes the variable region of the antibody) with the Fcγ receptor IIB (which recognizes the constant region of the antibody), thus inhibiting antigen specific B-cell activation (189). Furthermore, vaccine antigen-antibody complexes removal by macrophages has been suggested although no evidence has been provided to support this hypothesis. Using influenza vaccination in pregnancy as a model, it was recently shown in mice that maternal antibodies do not prevent activation of B cells or the formation of the germinal center. However, maternal antibodies reduced the number of B cells that differentiate to plasma cells and memory B cells (190). Whether these results apply to human infants and other antigens needs to be determined. Finally, while B cell responses are inhibited in the presence of maternal antibodies, scarce data support that T cell responses are detected in the presence of maternal antibodies (191).
Impact of Maternal Immunization on the Neonatal Immune System
The impact of maternal vaccination on the fetal/neonatal immune system, beyond the trans-placental transfer of IgG, has not been well-studied. In utero priming of the fetal immune system after vaccination against influenza in pregnancy has been reported. IgM antibodies against influenza vaccine antigens were detected in nearly 40% of cord blood specimens of newborns born to women vaccinated with IIV in pregnancy (192). As IgM antibodies do not cross the placenta, these antibodies are of fetal origin. In addition, using MHC tetramers, HA-specific CD4+ T cells were also detected in cord blood, further supporting the “in utero priming hypothesis” after maternal immunization (192). Additional studies are needed to further assess the possibility of priming of fetal immune system to B. pertussis antigens after immunization in pregnancy.
Based on the literature review and consultation among authors, a consensus on priorities for future research related to the effect of immunization during pregnancy on infants' immune responses was reached (Table 8).
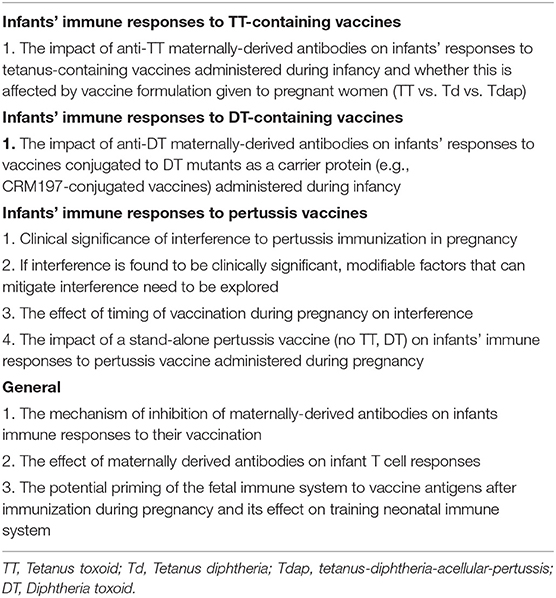
Table 8. Consensus on priorities for future research related to the impact of maternal immunization on in-utero immune system and infants' immune responses to immunization.
Future Vaccines for Immunization During Pregnancy
In addition to tetanus containing, pertussis containing and influenza vaccines currently used in pregnancy, multiple novel GBS and RSV candidate vaccines are under development for use in pregnant women (193). Infection with other pathogens (e.g., dengue virus, Zika virus) during pregnancy is associated with a significant risk of adverse fetal outcome (194–196), and thus vaccines developed with the goal to prevent these congenital infections might prove to be an important preventative strategy. However, these not part of this consensus paper and are reviewed elsewhere (197, 198).
Group B Streptococcus Vaccines
GBS colonization in pregnant women is associated with an increased risk of premature birth, birth asphyxia, stillbirths, and invasive GBS disease in newborns during the first week of life (early-onset disease, EOD). Newborns of mothers colonized with GBS are at higher risk of developing meningitis and sepsis (199). Although intrapartum antibiotic prophylaxis is effective in preventing GBS EOD, it is not effective in preventing late onset disease (LOD, >7–90 days of age) and it might be associated with dysregulation of the infants' gastro-intestinal microbiome (200). Importantly, identification and treatment of colonized mothers can be difficult and expensive, particularly in LMICs, where the incidence of neonatal invasive GBS disease is higher compared to HICs (201). Development of GBS vaccines for immunization in pregnancy and its use in LMICs has been identified as a priority by the WHO (202).
Vaccines based on the capsular polysaccharide of the most common GBS strains conjugated to a carrier protein (e.g., TT or a non-toxic mutant of diphtheria toxin) are the most studied candidate vaccines (203). A recent systematic review of clinical trials evaluating candidate GBS vaccines concluded that these candidate GBS vaccines are safe and well-tolerated in pregnant women and non-pregnant adults, may reduce vaginal colonization and induce antibody titers against the GBS strains included in the vaccine at a significantly higher level than that detected in unvaccinated controls (203). Moreover, antibodies induced by GBS vaccines showed high longevity and were able to promote GBS opsonophagocytosis in vitro (203).
Several challenges for the development of GBS vaccines for maternal immunization remain unsolved. There are only 10 known GBS serotypes, of which 6 are associated with 98% of all described strains that cause invasive disease and even a trivalent vaccine (Ia, Ib, and III) would provide coverage for 80% of all global invasive disease cases (204). The prevalence of different GBS serotypes may vary in different countries, however, the most common serotypes (Ia, Ib, II, III, IV, and V) are dominant globally, with only Asia reporting a slightly higher proportion of cases due to one additional serotype (VII) (205). The distribution of serotypes responsible for early and late -onset GBS disease also varies, with the most common serotypes being III and Ia (206). Correlates of protection for the different GBS serotypes against the various clinical conditions associated with the pathogen (i.e., colonization, maternal and infant disease) are not precisely defined (207), and these correlates may vary by serotype (207). Furthermore, transplacental transfer of antibodies might be affected by the characteristics of the vaccine (conjugated vs. unconjugated), the carrier protein used for conjugation, and the presence of underlying diseases in the mother which can reduce transfer, such as HIV infection (208).
Phase 1b/2 clinical trials have shown that vaccination of pregnant women with a trivalent GBS vaccine (serotype III, Ia, and Ib conjugated to CRM197) induces anti-GBS antibodies that are transferred to the newborn at delivery (208–210). Other phase 1/2 clinical trials are currently evaluating multi-serotype vaccines, including a hexavalent vaccine (serotypes Ia, Ib, II, III, IV, V) that cover 98% of strains associated with invasive GBS disease in both a non-pregnant population (NCT03170609) and in pregnant women (NCT03765073).
Finally, the clinical effectiveness of GBS vaccines in pregnant women and neonates has not been determined. Considering the relatively low incidence of invasive GBS disease, especially in HICs, the pathway of licensure of a GBS vaccine targeted at pregnant women with the main objective of protection of their infants against early and late-onset invasive GBS disease is likely to require an alternate approach than conventional efficacy trials. This would include demonstrating the safety of the vaccine in pregnant women (~3,000–4,500 participants), and benchmarking their immune responses to a serological endpoint associated with reduced risk for invasive GBS disease. Studies are currently underway in LMICs and HICs, which are investigating the association of maternal-derived serotype-specific IgG (using a standardized assay) and threshold associated with 80–90% risk reduction for invasive GBS disease.
As current GBS vaccines that are under development are conjugated to TT or the DT mutant CRM197, it will be important to investigate whether these vaccines given to pregnant women may result in interference to infant vaccines conjugated to these carrier proteins and given in infancy (e.g., PCV, Hib, and Meningococcal vaccines). Current evidence suggests that CRM197-conjugated GBS vaccine administered in pregnancy did not affect infants' immune responses to PCVs (211).
Respiratory Syncytial Virus
RSV is the most common cause of severe lower respiratory tract infections (LRTIs) in young children worldwide with a disproportionate high burden of disease in LMICs (e.g., higher case-fatality rate) (212). Preterm infants and infants with underlying severe chronic heart or lung disease are at higher risk of severe RSV infection, leading to hospitalization and death. A monoclonal antibody directed against the RSV fusion (F) protein has been administered to high-risk populations to prevent RSV-related morbidity in infants in high-income countries (213, 214). However, this strategy is highly expensive and its effectiveness varies ranging between 48 and 96% in the prevention of RSV-related hospitalization in high-risk children (215, 216). In addition, overall more healthy children are infected with RSV each year than high-risk children. A novel prolonged half-life anti-RSV monoclonal antibody may prove to be more effective in preventing RSV disease in infancy (217).
Recently, several new vaccines, including live-attenuated, gene-based vector vaccines, and particle-based vaccines, have been developed and found to be safe and well-tolerated in the non-pregnant population (11, 193). Hence, as most of the cases of severe RSV infection occur in the first 3 months of life, it is unlikely that infants' immunization can provide sufficient and timely protection. Therefore, maternal immunization is considered as a suitable strategy for prevention of RSV disease in young infants (11, 218).
Studies on RSV-F protein in pregnant women have shown that these vaccines are safe and immunogenic in pregnant women (219, 220). The use of these RSV vaccines in healthy pregnant women is further supported by evidence that maternal RSV neutralizing antibodies are efficiently transferred from the mother to the newborn, with levels at delivery that are similar or higher in the cord blood compared with the maternal blood at delivery (219, 220). However, the association between higher cord RSV neutralizing antibody levels and the reduction of risk for RSV LRTI in the infant is not clear, and no definitive correlates of protection have been defined so far (221–223). Vaccines containing the RSV-F protein in pregnant women have shown that these vaccines are safe and immunogenic in pregnant women (219, 220).
A phase 3, randomized, placebo controlled trial including 4,636 pregnant women has been conducted in 11 countries with a RSV-F nanoparticle alum-adjuvanted vaccine showed that protection against RSV LRTI hospitalization was noted (44.4% vaccine efficacy, 95%CI: 19.6 to 61.5), but the primary study endpoint (per protocol analysis) for reduction of medically-significant RSV LRTI (39% vaccine efficacy; 97.5% CI: −1 to 63.7) was not met (albeit the 95% CI been 5.3 to 61.2) (224). This is the largest study so far to evaluate a vaccine primarily designed for use in pregnant women.
Multiple factors could have affected the outcomes measured in this first immunization study of a RSV vaccine in pregnancy. Pregnant women were vaccinated during 28–36 weeks gestation, and efficiency of transfer of anti-RSV antibodies were found to be higher in women vaccinated <30 weeks GA compared with women vaccinated ≥30 weeks GA. In addition, vaccine efficacy varied in different settings, being higher in middle-income countries (compared with HICs). Mathematical modeling can help predict women and infants who are expected to benefit the most from RSV vaccines. This could be achieved by defining women who are expected to deliver in RSV season and the preferred timing of vaccination to optimize protection in those infants. Ideal timing of vaccination could be predicted based on the kinetics of antibody response in mothers, the efficiency of antibody transfer and their estimated half-life, and duration of infants' exposure to seasonal RSV.
Based on the literature review and consultation among authors, a consensus on priorities for future research related to immunization during pregnancy against GBS and RSV was reached (Table 9).
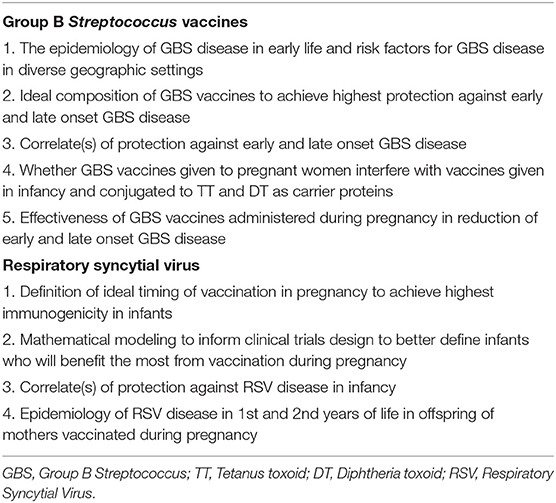
Table 9. Consensus on priorities for future research related to vaccines against respiratory syncytial virus and Group B Streptococcus diseases during pregnancy.
Induction of Vaccine-Specific Immunity in Breastmilk
There is a paucity of information on the induction of antibodies in breastmilk following vaccination in pregnancy (225). Anti-B. pertussis secretory immunoglobulin A (sIgA) antibodies were detected in colostrum and in breast milk up to 8 weeks after delivery from women vaccinated with Tdap during pregnancy (226, 227). However, the clinical significance of these elevated B. pertussis-specific antibody concentrations in breastmilk has not been studied. A study from Bangladesh showed that vaccination with TIV in pregnancy induced influenza-specific sIgA levels in breastmilk for at least 6 months postpartum. In addition, breastfeeding was associated with a decrease in episodes of respiratory illness with fever in infants born to mothers vaccinated against influenza during pregnancy (228). A study from South Africa found that breastmilk sIgA against GBS was associated with lower risk for GBS LOD in young infants (229). In a study from Nepal, breastmilk RSV IgG levels, but not IgA levels, were lower in mothers of infants with RSV acute respiratory infection (230). While these studies report potential association between breastfeeding and reduction in disease risk, the casual relationship has not been confirmed.
Based on the literature review and consultation among authors, a consensus on priorities for future research related to the effect of immunization during pregnancy on the induction of vaccine-specific immunity in breast milk was reached (Table 10).
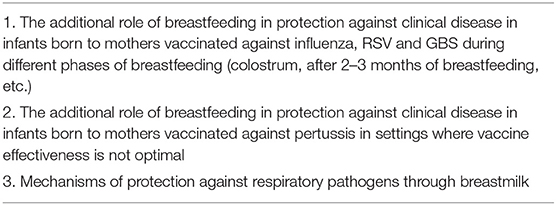
Table 10. Consensus on priorities for future research related to induction of vaccine-specific immunity in breast milk.
Acceptance and Strategies for Increasing Uptake of Vaccines
The acceptance and coverage of immunization against tetanus during pregnancy in LMICs have been historically high (231). Despite recommendations by multiple health authorities worldwide, maternal immunization with influenza and pertussis vaccines has not been as widely accepted by healthcare workers or the general public, including pregnant women (232). Coverage remains suboptimal in many countries where recommendations for maternal immunization with influenza and pertussis vaccines have been in place for several years. In the US, influenza and pertussis vaccines have been recommended for all pregnant women since 2004 (233) and 2011 (234), respectively. However, during the 2017–2018 influenza season, only 49.1% of pregnant women received the influenza vaccine during the peak influenza season (235). During the same months, maternal Tdap uptake was only slightly higher (54.4%). Finally, the receipt of both vaccines was documented in only 32.8% of pregnant women (235). In the UK, where pertussis vaccine has been offered to all pregnant women since October 1, 2012, coverage during the period from April to June 2018 was 68.2% (236). In the European Union, although 90% of countries recommend vaccination against influenza for pregnant women, coverage was generally low in 2014–2015, with half of the countries reporting uptake of <10% (237). In France, during the 2015–16 season vaccine coverage was only 7.4% (238). In Switzerland influenza and pertussis immunizations in pregnancy have been recommended since 2009 and 2013, respectively. Yet, in a study performed in women who gave birth between 2013 and 2017, only five (3%) of 172 mothers had received both pertussis and influenza vaccines during pregnancy, 15 (9%) only against pertussis and 12 (7%) only against influenza (239).
Several factors can explain the poor compliance with the official recommendations. A recent literature review documented 25 individual patient-level and 24 healthcare provider-level barriers to maternal immunization uptake (240). Among the patient-identified barriers, concerns regarding safety for the mother or the newborn were very common and were cited in 6.4–71% and 2.9–77.0% of studies, respectively. Other vaccine and disease-related factors included concerns about vaccine efficacy, the belief that the disease was not sufficiently severe to require prevention, and the idea that healthy people did not need immunization. Moreover, several structural and logistical barriers were identified. Lack of insurance coverage, limited access or transportation, and the difficulty of finding a provider for vaccine administration were reported. Finally, social, psychological factors, and insufficient knowledge were listed repeatedly. Among the provider-level barriers, poor knowledge of the recommendations for immunization of pregnant women, financial concerns (inadequate reimbursement, payment, and/or complexity of billing), and inability to order, obtain and store vaccines. Globally, the lack of knowledge of vaccine recommendations seems to be the most important barrier for both health care workers (HCWs) (241–246) and pregnant women (247–252). HCWs in contact with pregnant women frequently have little experience in vaccines and therefore do not offer vaccinations to pregnant women (239, 253).
To overcome barriers to maternal immunization, both provider-focused and mother-focused interventions have been suggested, with a significant improvement in vaccine uptake has been evidenced in several cases (253). Suggested provider-focused interventions were notifying the provider of the vaccination status of pregnant women, establishing standing orders authorizing nursing staff to administer the vaccines without a medical consultation, giving provider feedback by reporting the vaccination rates of other institutions, and providing education to improve the knowledge and attitudes of HCWs toward vaccination in pregnancy. However, education of HCWs alone is probably ineffective if parental vaccine hesitancy is not addressed simultaneously.
Multiple educational efforts involving all HCWs who deliver care to pregnant women and the pregnant women themselves can yield positive results (254). This observation seems to have been confirmed by a study by Chamberlain et al., who showed that when obstetricians and women became familiar with the recommendation to promote and receive the influenza vaccine during pregnancy, the percentage of women who refused to be vaccinated declined from 88.9% in 2004 to 64.2% in 2011 (254). To overcome barriers in pregnant women, studies were planned to disseminate education and promotion of materials specifically for pregnant women by mass media campaigns via the internet, posters and leaflets, lectures and workshops, and personalized reminders and recall system (254). Integrating maternal immunization into routine obstetric care, with vaccine availability within the obstetrical setting, appears to be the best method of improving maternal immunization as well as subsequent childhood vaccine uptake (255).
Based on the literature review and consultation among authors, a consensus on priorities for future research related to acceptance and uptake of vaccines administered during pregnancy was reached (Table 11).
Table 11. Consensus on priorities for future research related to acceptance and strategies for increasing uptake of vaccines administered during pregnancy.
Conclusions
Pregnant women, their newborns and young infants are vulnerable to serious and potentially fatal infections. The new WHO goals aim to increase rates of live births and improve antenatal care for pregnant women (256), and vaccination in pregnancy is one strategy to improve health of pregnant women and their offspring. Safe and effective vaccines are already available against some diseases (tetanus, pertussis and influenza) for use during pregnancy, and these vaccines have the potential to prevent significant infectious disease morbidity and mortality in both the mothers and their offspring. In addition, new vaccines (e.g., RSV, GBS) are currently under development and are being tested in clinical trials, to be licensed and used in pregnant women. Following literature review and a consultation amongst experts in the fields of infectious diseases, vaccination and immunization during pregnancy, several gaps in knowledge and priorities for research were identified and are proposed (Tables 3–11). Addressing these priorities in future research has the potential to increase our understanding in different aspects of immunization during pregnancy and optimize protection for both the mother and the infant.
Author Contributions
SE proposed the project, coordinated the study group, and wrote the first draft of the manuscript. BA-R wrote the first draft of the consensus statements and revised the initial draft of the manuscript. SO wrote the first draft of the ethics section. KM produced Figure 1. BA-R, KM, KE, SO, JE, MDS, GA, EL, PD, VP, OL, RD, MC, AC, KF, TF, SG, LV, MO'R, UH, NP, AA, MAS, NW, SM, MG, RP, SL, LM, FM-T, and SE reviewed and edited the manuscript, provided comments, suggested references, and substantially contributed to the content of the manuscript. BA-R, KM, KE, SO, JE, MDS, GA, EL, PD, VP, OL, RD, MC, AC, KF, TF, SG, LV, MO'R, UH, NP, AA, MAS, NW, SM, MG, RP, SL, LM, FM-T, and SE approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This Consensus was supported by a Grant from the World Association of Infectious Diseases and Immunological Disorders (Waidid_2019_03).
Conflict of Interest
SE: Research support from GSK, Sanofi, and Vifor. Speaker's fees from GSK, Pfizer, Novartis, Sanofi Pasteur, and MSD in the past 3 years. BA-R is supported by the Canadian Health and Research Institute Vanier Canada scholarship. KM is the beneficiary of a postdoctoral mandate fellowship from the FWO (Fund for Scientific Research-Flanders; FWO12R5819N). JE: Research support to my institution from Novavax, GlaxoSmithKline, Merck, Novavax, Chimerix; consultant for Sanofi Pasteur and Meissa. Have received both honoraria from both companies mentioned. MDS is currently, or has previously been, a Chief or Principal investigator on vaccine trials funded by vaccine manufacturers including GSK< MCM, Sanofi-Pasteur, Novartis Vaccines, Pfizer, Novavax, and Medimmune. These studies are conducted on behalf of the GSK, Novartis, Sanofi Pasteur MSD, and Novavax, University of Oxford and MDS receives no personal payment for this work. LV has received speaker's fees from GSK, Pfizer, Novartis, Sanofi Pasteur, and MSD. GlaxoSmithKline in the past 3 years. MO'R: Funding for clinical trials on Rotavirus Vaccines (GlaxoSmithKline up to 2008), Meningococcal b vaccines (GSK and Novartis up to 2017), RSV (Medimmue up to 2018), Pneumococcal vaccines (Merck to date). Funding for epidemiology/impact of disease studies: Enteric virus impact studies (Takeda vaccines to date), Vaccination acceptance study (Sanofi Pasteur to date). Travel support to present study results received; No speakers fees nor honorariums perceived. MAS has received grants to support research projects and consultancy fee from GSK, Pfizer, MSD, Seqirus, and Sanofi Pasteur. KF has served on the vaccine advisory boards for Sanofi-Pasteur and Seqiris in the past 3 years and received honoraria for attending meetings and speaker fees. SM; Institution received grant support in relation to studies on GBS and RSV including from BMGF, Pfizer, GSK, Minervax, and Novavax. No personal fees received from any of these sources, expect advisory honorarium from BMGF. FM-T has received honoraria from GSK, Pfizer, Sanofi Pasteur, Merck Sharp & Dohme, Seqirus, and Janssen for taking part in advisory boards and expert meetings, and for acting as speaker in congresses outside the scope of the submitted work. FM-T has also acted as principal investigator in RCTs of the above-mentioned companies as well as Ablynx, Regeneron, Roche, Abbot, Novavax, and Medimmune, with honoraria paid to his institution. FM-T research activities received support from the Instituto de Salud Carlos III (Proyecto de Investigación en Salud, Acción Estratégica en Salud): project ReSVinext ISCIII/PI16/01569/Cofinanciado FEDER and project Enterogen (ISCIII/PI19/01090). LM has received speaker's fees from GSK, Pfizer, Novartis, Sanofi Pasteur and MSD. RD has received grants/research support from Pfizer and Merck Sharp & Dohme; has been a scientific consultant for MeMed, Merck Sharp & Dohme, and Pfizer and a speaker for Pfizer. MC has received honoraria from GSK, Pfizer, Sanofi Pasteur, Merck Sharp & Dohme and Seqirus for taking part in advisory boards and expert meetings, and for acting as speaker in congresses outside the scope of the submitted work. MC has also been the principal investigator in RCTs of GSK, Sanofi Pasteur, and Novavax with honoraria paid to his institution. PD is (principal) investigator of vaccine trials for a large number of vaccine manufacturers (GSK Vaccines, Janssen Vaccines, Pfizer, Osyvax, Merck, Sanofi, and MSD) and institutions (Bill & Melinda Gates Foundation, EU-IMI, and FWO) for which the university of Antwerp obtains grants. UH is a member of the Global Pertussis Initiative (supported by Sanofi Pasteur, USA) and the Collaboration of European Experts on Pertussis Awareness Generation, CEEPAG (supported by Sanofi, France).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank Claudio Rosa for the design of Figure 2.
References
1. Esposito S, Bosis S, Morlacchi L, Baggi E, Sabatini C, Principi N. Can infants be protected by means of maternal vaccination? Clin Microbiol Infect. (2012) 18:85–92. doi: 10.1111/j.1469-0691.2012.03936.x
2. Marchant A, Sadarangani M, Garand M, Dauby N, Verhasselt V, Pereira L, et al. Maternal immunisation: collaborating with mother nature. Lancet Infect Dis. (2017) 17:e197–208. doi: 10.1016/S1473-3099(17)30229-3
3. Thwaites CL, Beeching NJ, Newton CR. Maternal and neonatal tetanus. Lancet. (2015) 385:362–70. doi: 10.1016/S0140-6736(14)60236-1
4. Campbell H, Gupta S, Dolan GP, Kapadia SJ, Kumar Singh A, Andrews N, Amirthalingam G. Review of vaccination in pregnancy to prevent pertussis in early infancy. J Med Microbiol. (2018) 67:1426–56. doi: 10.1099/jmm.0.000829
5. Esposito S, Stefanelli P, Fry NK, Fedele G, He Q, Paterson P, et al. Pertussis prevention: reasons for resurgence, and differences in the current acellular pertussis vaccines. Front Immunol. (2019) 10:1344. doi: 10.3389/fimmu.2019.01344
6. Amirthalingam G, Andrews N, Campbell H, Ribeiro S, Kara E, Donegan K, et al. Effectiveness of maternal pertussis vaccination in England: an observational study. Lancet. (2014) 384:1521–8. doi: 10.1016/S0140-6736(14)60686-3
7. Baxter R, Bartlett J, Fireman B, Lewis E, Klein NP. Effectiveness of vaccination during pregnancy to prevent infant pertussis. Pediatrics. (2017) 139:e20164091. doi: 10.1542/peds.2016-4091
8. Abu Raya B, Edwards KM, Scheifele DW, Halperin SA. Pertussis and influenza immunisation during pregnancy: a landscape review. Lancet Infect Dis. (2017) 17:e209–22. doi: 10.1016/S1473-3099(17)30190-1
10. Heath PT, Culley FJ, Jones CE, Kampmann B, Le Doare K, Nunes MC, et al. Group B streptococcus and respiratory syncytial virus immunisation during pregnancy: a landscape analysis. Lancet Infect Dis. (2017) 17:e223–34. doi: 10.1016/S1473-3099(17)30232-3
11. Esposito S, Pietro GD. Respiratory syncytial virus vaccines: an update on those in the immediate pipeline. Fut Microbiol. (2016) 11:1479–90. doi: 10.2217/fmb-2016-0106
12. A Roadmap for Advancing RSV Maternal Immunization. (2018) Available online at: https://path.azureedge.net/media/documents/PATH-AMIRoadmap_01.16.19_web.pdf. accessed December 4th, 2019.
13. Overcoming barriers and identifying opportunities for developing maternal immunizations: recommendations from the National Vaccine Advisory Committee. Public Health Rep. (2017) 132:271–84. doi: 10.1177/0033354917698118
14. Beigi RH, Omer SB, Thompson KM. Key steps forward for maternal immunization: policy making in action. Vaccine. (2018) 36:1521–3. doi: 10.1016/j.vaccine.2018.02.041
15. Chamberlain AT, Lavery JV, White A, Omer SB. Ethics of maternal vaccination. Science. (2017) 358:452–3. doi: 10.1126/science.aao4219
16. Pregnant Women and Vaccines Against Emerging Epidemic Threats. Ethics Guidance for Preparedness, Research and Response. The Prevent Working Group. Available online at: https://static1.squarespace.com/static/574503059f72665be88193e9/t/5c0823f36d2a73e7a091098b/1544037364415/PREVENT-ES.pdf (accessed January 28, 2020).
17. Vaccines against influenza WHO position paper – November 2012. Wkly Epidemiol Rec. (2012) 87:461–76. Available online at: https://www.who.int/wer/2012/wer8747.pdf
18. Meeting of the Strategic Advisory Group of Experts on immunization, April 2015: conclusions and recommendations. Wkly Epidemiol Rec. (2015) 90:261–78. Available online at: https://www.who.int/wer/2015/wer9022.pdf?ua=1
19. Munoz FM, Eckert LO, Katz MA, Lambach P, Ortiz JR, Bauwens J, et al. Key terms for the assessment of the safety of vaccines in pregnancy: results of a global consultative process to initiate harmonization of adverse event definitions. Vaccine. (2015) 33:6441–52. doi: 10.1016/j.vaccine.2015.07.112
20. Bonhoeffer J, Kochhar S, Hirschfeld S, Heath PT, Jones CE, Bauwens J, et al. Global alignment of immunization safety assessment in pregnancy - the GAIA project. Vaccine. (2016) 34:5993–7. doi: 10.1016/j.vaccine.2016.07.006
21. Rouse CE, Eckert LO, Muñoz FM, Stringer JSA, Kochhar S, Bartlett L, et al. Postpartum endometritis and infection following incomplete or complete abortion: case definition & guidelines for data collection, analysis, presentation of maternal immunization safety data. Vaccine. (2019) 37:7585–95. doi: 10.1016/j.vaccine.2019.09.101
22. Pellegrin S, Munoz FM, Padula M, Heath PT, Meller L, Top K, et al. Neonatal seizures: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. (2019) 37:7596–609. doi: 10.1016/j.vaccine.2019.05.031
23. Kachikis A, Eckert LO, Walker C, Bardají A, Varricchio F, Lipkind HS, et al. Chorioamnionitis: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. (2019) 37:7610–22. doi: 10.1016/j.vaccine.2019.05.030
24. Villagomez AN, Muñoz FM, Peterson RL, Colbert AM, Gladstone M, MacDonald B, et al. Neurodevelopmental delay: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. (2019) 37:7623–41. doi: 10.1016/j.vaccine.2019.05.027
25. Pazos M, Sperling RS, Moran TM, Kraus TA. The influence of pregnancy on systemic immunity. Immunol Res. (2012) 54:254–61. doi: 10.1007/s12026-012-8303-9
26. Lima J, Martins C, Leandro MJ, Nunes G, Sousa MJ, Branco JC, et al. Characterization of B cells in healthy pregnant women from late pregnancy to post-partum: a prospective observational study. BMC Pregn Childbirth. (2016) 16:139. doi: 10.1186/s12884-016-0927-7
27. Medina KL, Smithson G, Kincade PW. Suppression of B lymphopoiesis during normal pregnancy. J Exp Med. (1993) 178:1507–15. doi: 10.1084/jem.178.5.1507
28. Medina KL, Kincade PW. Pregnancy-related steroids are potential negative regulators of B lymphopoiesis. Proc Natl Acad Sci USA. (1994) 91:5382–6. doi: 10.1073/pnas.91.12.5382
29. Birkeland SA, Kristoffersen K. Lymphocyte transformation with mitogens and antigens during normal human pregnancy: a longitudinal study. Scand J Immunol. (1980) 11:321–5. doi: 10.1111/j.1365-3083.1980.tb00240.x
30. Lima J, Cambridge G, Vilas-Boas A, Martins C, Borrego LM, Leandro M. Serum markers of B-cell activation in pregnancy during late gestation, delivery, and the postpartum period. Am J Reprod Immunol. (2019) 81:e13090. doi: 10.1111/aji.13090
31. Larsson A, Palm M, Hansson LO, Basu S, Axelsson O. Reference values for alpha1-acid glycoprotein, alpha1-antitrypsin, albumin, haptoglobin, C-reactive protein, IgA, IgG and IgM during pregnancy. Acta Obstet Gynecol Scand. (2008) 87:1084–8. doi: 10.1080/00016340802428146
32. Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. (2014) 370:2211–18. doi: 10.1056/NEJMra1213566
33. Wegmann TG, Lin H, Guilbert L, Mosmann TR. Bidirectional cytokine interactions in the maternal-fetal relationship: is successful pregnancy a TH2 phenomenon? Immunol Today. (1993) 14:353–6. doi: 10.1016/0167-5699(93)90235-D
34. Saito S. Cytokine network at the feto-maternal interface. J Reprod Immunol. (2000) 47:87–103. doi: 10.1016/S0165-0378(00)00060-7
35. Piccinni MP, Giudizi MG, Biagiotti R, Beloni L, Giannarini L, Sampognaro S, et al. Progesterone favors the development of human T helper cells producing Th2-type cytokines and promotes both IL-4 production and membrane CD30 expression in established Th1 cell clones. J Immunol. (1995) 155:128–33.
36. Raghupathy R, Makhseed M, Azizieh F, Omu A, Gupta M, Farhat R. Cytokine production by maternal lymphocytes during normal human pregnancy and in unexplained recurrent spontaneous abortion. Hum Reprod. (2000) 15:713–18. doi: 10.1093/humrep/15.3.713
37. Glassman AB, Bennett CE, Christopher JB, Self S. Immunity during pregnancy: lymphocyte subpopulations and mitogen responsiveness. Ann Clin Lab Sci. (1985) 15:357–62.
38. Fujisaki S, Mori N, Sasaki T, Maeyama M. Cell-mediated immunity in human pregnancy: changes in lymphocyte reactivity during pregnancy and postpartum. Microbiol Immunol. (1979) 23:899–907. doi: 10.1111/j.1348-0421.1979.tb02823.x
39. Marzi M, Vigano A, Trabattoni D, Villa ML, Salvaggio A, Clerici E, et al. Characterization of type 1 and type 2 cytokine production profile in physiologic and pathologic human pregnancy. Clin Exp Immunol. (1996) 106:127–33. doi: 10.1046/j.1365-2249.1996.d01-809.x
40. Brabin BJ, Nagel J, Hagenaars AM, Ruitenberg E, van Tilborgh AM. The influence of malaria and gestation on the immune response to one and two doses of adsorbed tetanus toxoid in pregnancy. Bull World Health Organ. (1984) 62:919–30.
41. Huygen K, Caboré RN, Maertens K, Van Damme P, Leuridan E. Humoral and cell mediated immune responses to a pertussis containing vaccine in pregnant and nonpregnant women. Vaccine. (2015) 33:4117–23. doi: 10.1016/j.vaccine.2015.06.108
42. Hulka JF. Effectiveness of polyvalent influenza vaccine in pregnancy. Report of a controlled study during an outbreak of Asian influenza. Obstet Gynecol. (1964) 23:830–7.
43. Murray DL, Imagawa DT, Okada DM, St. Geme JW. Antibody response to monovalent A/New Jersey/8/76 influenza vaccine in pregnant women. J Clin Microbiol. (1979) 10:184–7. doi: 10.1128/JCM.10.2.184-187.1979
44. Tsatsaris V, Capitant C, Schmitz T, Chazallon C, Bulifon S, Riethmuller D, et al. Maternal immune response and neonatal seroprotection from a single dose of a monovalent nonadjuvanted 2009 influenza A(H1N1) vaccine: a single-group trial. Ann Intern Med. (2011) 155:733–41. doi: 10.7326/0003-4819-155-11-201112060-00005
45. Schlaudecker EP, Ambroggio L, McNeal MM, Finkelman FD, Way SS. Declining responsiveness to influenza vaccination with progression of human pregnancy. Vaccine. (2018) 36:4734–41. doi: 10.1016/j.vaccine.2018.05.117
46. Bischoff AL, Folsgaard NV, Carson CG, Stokholm J, Pedersen L, Holmberg M, et al. Altered response to A(H1N1)pnd09 vaccination in pregnant women: a single blinded randomized controlled trial. PLoS ONE. (2013) 8: e56700. doi: 10.1371/journal.pone.0056700
47. Schlaudecker EP, McNeal MM, Dodd CN, Ranz JB, Steinhoff MC. Pregnancy modifies the antibody response to trivalent influenza immunization. J Infect Dis. (2012) 206:1670–3. doi: 10.1093/infdis/jis592
48. Kay AW, Fukuyama J, Aziz N, Dekker CL, Mackey S, Swan GE, et al. Enhanced natural killer-cell and T-cell responses to influenza A virus during pregnancy. Proc Natl Acad Sci USA. (2014) 111:14506–11. doi: 10.1073/pnas.1416569111
49. Simister NE. Placental transport of immunoglobulin G. Vaccine. (2003) 21:3365–9. doi: 10.1016/S0264-410X(03)00334-7
50. Saji F, Samejima Y, Kamiura S, Koyama M. Dynamics of immunoglobulins at the feto-maternal interface. Rev Reprod. (1999) 4:81–9. doi: 10.1530/ror.0.0040081
51. Malek A, Sager R, Kuhn P, Nicolaides KH, Schneider H. Evolution of maternofetal transport of immunoglobulins during human pregnancy. Am J Reprod Immunol. (1996) 36:248–55. doi: 10.1111/j.1600-0897.1996.tb00172.x
52. Kohler PF, Farr RS. Elevation of cord over maternal IgG immunoglobulin: evidence for an active placental IgG transport. Nature. (1966) 210:1070–71. doi: 10.1038/2101070a0
53. Palmeira P, Quinello C, Silveira-Lessa AL, Zago CA, Carneiro-Sampaio M. IgG placental transfer in healthy and pathological pregnancies. Clin Dev Immunol. (2012) 2012:985646. doi: 10.1155/2012/985646
54. Schauer U, Stemberg F, Rieger CH, Büttner W, Borte M, Schubert S, et al. Levels of antibodies specific to tetanus toxoid, Haemophilus influenzae type b, and pneumococcal capsular polysaccharide in healthy children and adults. Clin Diagn Lab Immunol. (2003) 10:202–7. doi: 10.1128/CDLI.10.2.202-207.2003
55. Malek A, Sager R, Schneider H. Maternal-fetal transport of immunoglobulin G and its subclasses during the third trimester of human pregnancy. Am J Reprod Immunol. (1994) 32:8–14. doi: 10.1111/j.1600-0897.1994.tb00873.x
56. Garty BZ, Ludomirsky A, Danon YL, Peter JB, Douglas SD. Placental transfer of immunoglobulin G subclasses. Clin Diagn Lab Immunol. (1994) 1:667–9. doi: 10.1128/CDLI.1.6.667-669.1994
57. Vidarsson G, Dekkers G, Rispens T. IgG subclasses and allotypes: from structure to effector functions. Front Immunol. (2014) 5:520. doi: 10.3389/fimmu.2014.00520
58. Costa-Carvalho BT, Vieria HM, Dimantas RB, Arslanian C, Naspitz CK, Solé D, et al. Transfer of IgG subclasses across placenta in term and preterm newborns. Braz J Med Biol Res. (1996) 29:201–4.
59. Abu-Raya B, Kollmann TR, Marchant A, MacGillivray DM. The immune system of HIV-exposed uninfected infants. Front Immunol. (2016) 7:383. doi: 10.3389/fimmu.2016.00383
60. Dechavanne C, Cottrell G, Garcia A, Migot-Nabias F. Placental malaria: decreased transfer of maternal antibodies directed to Plasmodium falciparum and Impact on the incidence of febrile infections in infants. PLoS ONE. (2015) 10:e0145464. doi: 10.1371/journal.pone.0145464
61. Okoko BJ, Wesumperuma LH, Ota MO, Pinder M, Banya W, Gomez SF, et al. The influence of placental malaria infection and maternal hypergammaglobulinemia on transplacental transfer of antibodies and IgG subclasses in a rural West African population. J Infect Dis. (2001) 184:627–32. doi: 10.1086/322808
62. Abu-Raya B, Edwards KM. Optimizing the timing of vaccine administration during pregnancy. JAMA. (2019) 321:935–6. doi: 10.1001/jama.2019.0703
63. Abu Raya B, Srugo I, Bamberger E. Optimal timing of immunization against pertussis during pregnancy. Clin Infect Dis. (2016) 63:143–4. doi: 10.1093/cid/ciw233
64. Louie JK, Acosta M, Jamieson DJ, Honein MA, the California Pandemic (H1N1) Working Group. Severe 2009 H1N1 influenza in pregnant and postpartum women in California. N Engl J Med. (2010) 362:27–35. doi: 10.1056/NEJMoa0910444
65. Principi N, Esposito S. Severe influenza in children: incidence and risk factors. Expert Rev Anti Infect Ther. (2016) 14:961–8. doi: 10.1080/14787210.2016.1227701
66. Principi N, Esposito S. Influenza vaccine use to protect healthy children: a debated topic. Vaccine. (2018) 36:5391–6. doi: 10.1016/j.vaccine.2017.09.016
67. Abu-Raya B, Bettinger JA, Vanderkooi OG, Vaudry W, Halperin SA, Sadarangani M, et al. Burden of children hospitalized with pertussis in canada in the acellular pertussis vaccine era, 1999–2015. J Pediatr Infect Dis Soc. (2018) 9:118–27. doi: 10.1093/jpids/piy128
68. Abu-Raya B, Giles ML. Extending antenatal pertussis immunization to second trimester or at-birth pertussis immunization of premature infants? JAMA Pediatr. (2019) 173:294–5. doi: 10.1001/jamapediatrics.2018.5139
69. Riise Ø, Laake I, Vestrheim D, Flem E, Moster D, Riise Bergsaker MA, et al. Risk of pertussis in relation to degree of prematurity in children less than 2 years of age. Pediatr Infect Dis J. (2017) 36:e151–6. doi: 10.1097/INF.0000000000001545
70. Centers for Disease Control and Prevention. Vaccines and Preventable Diseases. Available online at: https://www.cdc.gov/vaccines/vpd/dtap-tdap-td/hcp/about-vaccine.html (accessed May 3, 2020).
71. Tetanus Toxoid Vaccine Adsorbed. Available online at: https://www.seruminstitute.com/product_diphtheriatetanus_texoid.php (accessed May 3, 2020).
72. Centers for Disease Control and Prevention. Influenza (flu) Available online at: https://www.cdc.gov/flu/professionals/acip/summary/summary-recommendations.htm - anchor-star (accessed May 4, 2020).
73. World Health Organization. WHO Recommendation on Tetanus Toxoid Vaccination for Pregnant Women. (2018) Available online at: https://extranet.who.int/rhl/topics/preconception-pregnancy-childbirth-and-postpartum-care/antenatal-care/who-recommendation-tetanus-toxoid-vaccination-pregnant-women (accessed December 15, 2018).
74. Stanfield JP, Gall D, Bracken PM. Single-dose antenatal tetanus immunisation. Lancet. (1973) 1:215–19. doi: 10.1016/S0140-6736(73)90062-7
75. Silveira CM, Cáceres VM, Dutra MG, Lopes-Camelo J, Castilla EE. Safety of tetanus toxoid in pregnant women: a hospital-based case-control study of congenital anomalies. Bull World Health Organ. (1995) 73:605–8.
76. Sukumaran L, McCarthy NL, Kharbanda EO, McNeil MM, Naleway AL, Klein NP, et al. Association of Tdap vaccination with acute events and adverse birth outcomes among pregnant women with prior tetanus-containing immunizations. JAMA. (2015) 314:1581–7. doi: 10.1001/jama.2015.12790
77. Munoz FM, Bond NH, Maccato M, Pinell P, Hammill HA, Swamy GK, et al. Safety and immunogenicity of tetanus diphtheria and acellular pertussis (Tdap) immunization during pregnancy in mothers and infants: a randomized clinical trial. JAMA. (2014) 311:1760–9. doi: 10.1001/jama.2014.3633
78. Cumberland P, Shulman CE, Maple PA, Bulmer JN, Dorman EK, Kawuondo K, et al. Maternal HIV infection and placental malaria reduce transplacental antibody transfer and tetanus antibody levels in newborns in Kenya. J Infect Dis. (2007) 196:550–7. doi: 10.1086/519845
79. Hood N, Chan MC, Maxwell SM, Familusi JB, Hart CA. Placental transfer of tetanus toxoid antibodies in Nigerian mothers. Ann Trop Paediatr. (1994) 14:179–82. doi: 10.1080/02724936.1994.11747714
80. Maertens K, Caboré RN, Huygen K, Hens N, Van Damme P, Leuridan E. Pertussis vaccination during pregnancy in Belgium: results of a prospective controlled cohort study. Vaccine. (2016) 34:142–50. doi: 10.1016/j.vaccine.2015.10.100
81. Kim JS, Kim SJ, Shin KJ, Hwang PH, Cho SC. Changes of tetanus specific IgG, IgM and IgG subclasses after DPT vaccination. Yonsei Med J. (1989) 30:158–63. doi: 10.3349/ymj.1989.30.2.158
82. World Health Organization. The Immunological Basis for Immunization Series: Module 3: Tetanus. World Health Organization (2018). Available online at: http://www.who.int/iris/handle/10665/275340 (accessed July 1, 2019).
83. Hoang HT, Leuridan E, Maertens K, Nguyen TD, Hens N, Vu NH, et al. Pertussis vaccination during pregnancy in Vietnam: results of a randomized controlled trial Pertussis vaccination during pregnancy. Vaccine. (2016) 34:151–9. doi: 10.1016/j.vaccine.2015.10.098
84. UNICEF. Elimination of Maternal and Neonatal Tetanus. Available at: https://www.unicef.org/health/index_43509.html (accessed December 15, 2018).
85. World Health Organization. Protecting All Against Tetanus. Available online at: https://www.who.int/immunization/diseases/tetanus/Protecting_All_Against_Tetanus_final_draftV4_23Jan_web.pdf?ua=1 (accessed November 24, 2019).
86. Vygen-Bonnet S, Hellenbrand W, Garbe E, von Kries R, Bogdan C, Heininger U, et al. Safety and effectiveness of acellular pertussis vaccination during pregnancy: a systematic review. BMC Infect Dis. (2020) 20:136. doi: 10.1186/s12879-020-4824-3
87. Donegan K, King B, Bryan P. Safety of pertussis vaccination in pregnant women in UK: observational study. BMJ. (2014) 349:g4219. doi: 10.1136/bmj.g4219
88. Kharbanda EO, Vazquez-Benitez G, Lipkind HS, Klein NP, Cheetham TC, Naleway A, et al. Evaluation of the association of maternal pertussis vaccination with obstetric events and birth outcomes. JAMA. (2014) 312:1897–904. doi: 10.1001/jama.2014.14825
89. Kharbanda EO, Vazquez-Benitez G, Lipkind HS, Klein NP, Cheetham TC, Naleway AL, et al. Maternal Tdap vaccination: coverage and acute safety outcomes in the vaccine safety datalink, 2007–2013. Vaccine. (2016) 34:968–73. doi: 10.1016/j.vaccine.2015.12.046
90. Morgan JL, Baggari SR, McIntire DD, Sheffield JS. Pregnancy outcomes after antepartum tetanus, diphtheria, and acellular pertussis vaccination. Obstet Gynecol. (2015) 125:1433–8. doi: 10.1097/AOG.0000000000000862
91. Shakib JH, Korgenski K, Sheng X, Varner MW, Pavia AT, Byington CL. Tetanus, diphtheria, acellular pertussis vaccine during pregnancy: pregnancy and infant health outcomes. J Pediatr. (2013) 163:1422–6.e1421-4. doi: 10.1016/j.jpeds.2013.06.021
92. Walls T, Graham P, Petousis-Harris H, Hill L, Austin N. Infant outcomes after exposure to Tdap vaccine in pregnancy: an observational study. BMJ Open. (2016) 6:e009536. doi: 10.1136/bmjopen-2015-009536
93. Villarreal Perez JZ, Aranda JMR, de la O, Cavazos M, Zamudio Osuna MJ, Dávila JM, Elizondo MRB, et al. Randomized clinical trial of the safety and immunogenicity of the Tdap vaccine in pregnant Mexican women. Human Vaccines Immunother. (2017) 13:128–35. doi: 10.1080/21645515.2016.1232786
94. Berenson AB, Hirth JM, Rahman M, Laz TH, Rupp RE, Sarpong KO. Maternal and infant outcomes among women vaccinated against pertussis during pregnancy. Hum Vaccin Immunother. (2016) 12:1965–71. doi: 10.1080/21645515.2016.1157241
95. DeSilva M, Vazquez-Benitez G, Nordin JD, Lipkind HS, Romitti PA, DeStefano F, et al. Tdap vaccination during pregnancy and microcephaly and other structural birth defects in offspring. JAMA. (2016) 316:1823–5. doi: 10.1001/jama.2016.14432
96. D'Heilly C, Switzer C, Macina D. Safety of maternal immunization against pertussis: a systematic review. Infect Dis Ther. (2019) 8:543–68. doi: 10.1007/s40121-019-00265-6
97. Datwani H, Moro PL, Harrington T, Broder KR. Chorioamnionitis following vaccination in the Vaccine Adverse Event Reporting System. Vaccine. (2015) 33:3110–13. doi: 10.1016/j.vaccine.2015.04.097
98. Layton JB, Butler AM, Li D, Boggess KA, Weber DJ, McGrath LJ, et al. Prenatal Tdap immunization and risk of maternal and newborn adverse events. Vaccine. (2017) 35:4072–8. doi: 10.1016/j.vaccine.2017.06.071
99. Halperin BA, Morris A, Mackinnon-Cameron D, Mutch J, Langley JM, McNeil SA, et al. Kinetics of the antibody response to tetanus-diphtheria-acellular pertussis vaccine in women of childbearing age and postpartum women. Clin Infect Dis. (2011) 53:885–92. doi: 10.1093/cid/cir538
100. Abu Raya B, Srugo I, Kessel A, Peterman M, Vaknin A, Bamberger E. The decline of pertussis-specific antibodies after tetanus, diphtheria, and acellular pertussis immunization in late pregnancy. J Infect Dis. (2015) 212:1869–73. doi: 10.1093/infdis/jiv324
101. Maertens K, Tran TMP, Hens N, Van Damme P, Leuridan E. Effect of Prepregnancy pertussis vaccination in young infants. J Infect Dis. (2017) 215:1855–61. doi: 10.1093/infdis/jix176
102. Giammanco A, Taormina S, Chiarini A, Dardanoni G, Stefanelli P, Salmaso S, et al. Analogous IgG subclass response to pertussis toxin in vaccinated children, healthy or affected by whooping cough. Vaccine. (2003) 21:1924–31. doi: 10.1016/S0264-410X(02)00823-X
103. Hendrikx LH, Schure RM, Oztürk K, de Rond LG, de Greeff SC, Sanders EA, et al. Different IgG-subclass distributions after whole-cell and acellular pertussis infant primary vaccinations in healthy and pertussis infected children. Vaccine. (2011) 29:6874–80. doi: 10.1016/j.vaccine.2011.07.055
104. Halperin SA, Langley JM, Ye LD, Elsherif M, Allen VM, Smith B, et al. A Randomized controlled trial of the safety and immunogenicity of tetanus, diphtheria, acellular pertussis vaccine immunization during pregnancy and subsequent infant immune response. Clin Infect Dis. (2018) 67:1063–71. doi: 10.1093/cid/ciy244
105. Scanlon K, Skerry C, Carbonetti N. Association of pertussis toxin with severe pertussis disease. Toxins. (2019) 11:373. doi: 10.3390/toxins11070373
106. Nguyen AW, Wagner EK, Laber JR, Goodfield LL, Smallridge WE, Harvill ET, et al. A cocktail of humanized anti-pertussis toxin antibodies limits disease in murine and baboon models of whooping cough. Sci Transl Med. (2015) 7:316ra195. doi: 10.1126/scitranslmed.aad0966
107. Kapil P, Papin JF, Wolf RF, Zimmerman LI, Wagner LD, Merkel TJ. Maternal vaccination with a monocomponent pertussis toxoid vaccine is sufficient to protect infants in a baboon model of whooping cough. J Infect Dis. (2018) 217:1231–6. doi: 10.1093/infdis/jiy022
108. Storsaeter J, Hallander HO, Gustafsson L, Olin P. Low levels of antipertussis antibodies plus lack of history of pertussis correlate with susceptibility after household exposure to Bordetella pertussis. Vaccine. (2003) 21:3542–9. doi: 10.1016/S0264-410X(03)00407-9
109. Wanlapakorn N, Maertens K, Chaithongwongwatthana S, Srimuan D, Suratannon N, Vongpunsawad S, et al. Assessing the reactogenicity of Tdap vaccine administered during pregnancy and antibodies to Bordetella pertussis antigens in maternal and cord sera of Thai women. Vaccine. (2018) 36:1453–9. doi: 10.1016/j.vaccine.2018.01.059
110. Abu Raya B, Srugo I, Kessel A, Peterman M, Bader D, Gonen R, et al. The effect of timing of maternal tetanus, diphtheria, and acellular pertussis (Tdap) immunization during pregnancy on newborn pertussis antibody levels - a prospective study. Vaccine. (2014) 32:5787–93. doi: 10.1016/j.vaccine.2014.08.038
111. Naidu MA, Muljadi R, Davies-Tuck ML, Wallace EM, Giles ML. The optimal gestation for pertussis vaccination during pregnancy: a prospective cohort study. Am J Obstet Gynecol. (2016) 215:237.e231-6. doi: 10.1016/j.ajog.2016.03.002
112. Healy CM, Rench MA, Swaim LS, Smith EO, Sangi-Haghpeykar H, Mathis MH, et al. Association between third-trimester tdap immunization and neonatal pertussis antibody concentration. JAMA. (2018) 320:1464–70. doi: 10.1001/jama.2018.14298
113. Eberhardt CS, Blanchard-Rohner G, Lemaitre B, Boukrid M, Combescure C, Othenin-Girard V, et al. Maternal immunization earlier in pregnancy maximizes antibody transfer and expected infant seropositivity against pertussis. Clin Infect Dis. (2016) 62:829–36. doi: 10.1093/cid/ciw027
114. Eberhardt CS, Blanchard-Rohner G, Lemaître B, Combescure C, Othenin-Girard V, Chilin A, et al. Pertussis antibody transfer to preterm neonates after second- versus third-trimester maternal immunization. Clin Infect Dis. (2017) 64:1129–32. doi: 10.1093/cid/cix046
115. Abu Raya B, Bamberger E, Almog M, Peri R, Srugo I, Kessel A. Immunization of pregnant women against pertussis: the effect of timing on antibody avidity. Vaccine. (2015) 33:1948–52. doi: 10.1016/j.vaccine.2015.02.059
116. Abu-Raya B, Giles ML, Kollmann TR, Sadarangani M. The effect of timing of tetanus-diphtheria-acellular pertussis vaccine administration in pregnancy on the avidity of pertussis antibodies. Front Immunol. (2019) 10:2423. doi: 10.3389/fimmu.2019.02423
117. Maertens K, Hoang THT, Caboré RN, Leuridan E. Avidity of maternal pertussis antibodies after vaccination during pregnancy. Vaccine. (2015) 33:5489. doi: 10.1016/j.vaccine.2015.05.075
118. Dabrera G, Amirthalingam G, Andrews N, Campbell H, Ribeiro S, Kara E, et al. A case-control study to estimate the effectiveness of maternal pertussis vaccination in protecting newborn infants in England and Wales, 2012–2013. Clin Infect Dis. (2015) 60:333–7. doi: 10.1093/cid/ciu821
119. Winter K, Cherry JD, Harriman K. Effectiveness of prenatal tetanus, diphtheria, and acellular pertussis vaccination on pertussis severity in infants. Clin Infect Dis. (2017) 64:9–14. doi: 10.1093/cid/ciw633
120. Winter K, Nickell S, Powell M, Harriman K. Effectiveness of prenatal versus postpartum tetanus, diphtheria, and acellular pertussis vaccination in preventing infant pertussis. Clin Infect Dis. (2017) 64:3–8. doi: 10.1093/cid/ciw634
121. Bellido-Blasco J, Guiral-Rodrigo S, Míguez-Santiyán A, Salazar-Cifre A, González-Morán F. A case-control study to assess the effectiveness of pertussis vaccination during pregnancy on newborns, Valencian community, Spain, 1 March 2015 to 29 February 2016. Euro Surveill. (2017) 22:30545. doi: 10.2807/1560-7917.ES.2017.22.22.30545
122. Saul N, Wang K, Bag S, Baldwin H, Alexander K, Chandra M, et al. Effectiveness of maternal pertussis vaccination in preventing infection and disease in infants: the NSW Public Health Network case-control study. Vaccine. (2018) 36:1887–92. doi: 10.1016/j.vaccine.2018.02.047
123. Fernandes EG, Sato APS, Vaz-de-Lima LRA, Rodrigues M, Leite D, de Brito CA, et al. The effectiveness of maternal pertussis vaccination in protecting newborn infants in Brazil: a case-control study. Vaccine. (2019) 37:5481–4. doi: 10.1016/j.vaccine.2019.03.049
124. Trotta F, Da Cas R, Spila Alegiani S, Gramegna M, Venegoni M, Zocchetti C, et al. Evaluation of safety of A/H1N1 pandemic vaccination during pregnancy: cohort study. BMJ. (2014) 348:g3361. doi: 10.1136/bmj.g3361
125. Nordin JD, Kharbanda EO, Vazquez Benitez G, Lipkind H, Vellozzi C, Destefano F, et al. Maternal influenza vaccine and risks for preterm or small for gestational age birth. J Pediatr. (2014) 164:1051–7.e1052. doi: 10.1016/j.jpeds.2014.01.037
126. Chambers CD, Johnson D, Xu R, Luo Y, Louik C, Mitchell AA, et al. Risks and safety of pandemic H1N1 influenza vaccine in pregnancy: birth defects, spontaneous abortion, preterm delivery, and small for gestational age infants. Vaccine. (2013) 31:5026–32. doi: 10.1016/j.vaccine.2013.08.097
127. Richards JL, Hansen C, Bredfeldt C, Bednarczyk RA, Steinhoff MC, Adjaye-Gbewonyo D, et al. Neonatal outcomes after antenatal influenza immunization during the 2009 H1N1 influenza pandemic: impact on preterm birth, birth weight, and small for gestational age birth. Clin Infect Dis. (2013) 56:1216–22. doi: 10.1093/cid/cit045
128. Omer SB, Goodman D, Steinhoff MC, Rochat R, Klugman KP, Stoll BJ, et al. Maternal influenza immunization and reduced likelihood of prematurity and small for gestational age births: a retrospective cohort study. PLoS Med. (2011) 8:e1000441. doi: 10.1371/journal.pmed.1000441
129. Vesikari T, Virta M, Heinonen S, Eymin C, Lavis N, Chabanon AL, et al. Immunogenicity and safety of a quadrivalent inactivated influenza vaccine in pregnant women: a randomized, observer-blind trial. Hum Vaccin Immunother. (2019) 16:623–9. doi: 10.1080/21645515.2019.1667202
130. Ortiz JR, Englund JA, Neuzil KM. Influenza vaccine for pregnant women in resource-constrained countries: a review of the evidence to inform policy decisions. Vaccine. (2011) 29:4439–52. doi: 10.1016/j.vaccine.2011.04.048
131. Ludvigsson JF, Zugna D, Cnattingius S, Richiardi L, Ekbom A, Örtqvist Å, et al. Influenza H1N1 vaccination and adverse pregnancy outcome. Eur J Epidemiol. (2013) 28:579–88. doi: 10.1007/s10654-013-9813-z
132. Rubinstein F, Micone P, Bonotti A, Wainer V, Schwarcz A, Augustovski F, et al. Influenza A/H1N1 MF59 adjuvanted vaccine in pregnant women and adverse perinatal outcomes: multicentre study. BMJ. (2013) 346:f393. doi: 10.1136/bmj.f393
133. Bratton KN, Wardle MT, Orenstein WA, Omer SB. Maternal influenza immunization and birth outcomes of stillbirth and spontaneous abortion: a systematic review and meta-analysis. Clin Infect Dis. (2015) 60:e11–19. doi: 10.1093/cid/ciu915
134. Donahue JG, Kieke BA, King JP, DeStefano F, Mascola MA, Irving SA, et al. Association of spontaneous abortion with receipt of inactivated influenza vaccine containing H1N1pdm09 in 2010–11 and 2011–12. Vaccine. (2017) 35:5314–22. doi: 10.1016/j.vaccine.2017.06.069
135. Madhi SA, Cutland CL, Kuwanda L, Weinberg A, Hugo A, Jones S, et al. Influenza vaccination of pregnant women and protection of their infants. N Engl J Med. (2014) 371:918–31. doi: 10.1056/NEJMoa1401480
136. Tapia MD, Sow SO, Tamboura B, Tégueté I, Pasetti MF, Kodio M, et al. Maternal immunisation with trivalent inactivated influenza vaccine for prevention of influenza in infants in Mali: a prospective, active-controlled, observer-blind, randomised phase 4 trial. Lancet Infect Dis. (2016) 16:1026–35. doi: 10.1016/S1473-3099(16)30054-8
137. Steinhoff MC, Katz J, Englund JA, Khatry SK, Shrestha L, Kuypers J, et al. Year-round influenza immunisation during pregnancy in Nepal: a phase 4, randomised, placebo-controlled trial. Lancet Infect Dis. (2017) 17:981–9. doi: 10.1016/S1473-3099(17)30252-9
138. McMillan M, Porritt K, Kralik D, Costi L, Marshall H. Influenza vaccination during pregnancy: a systematic review of fetal death, spontaneous abortion, and congenital malformation safety outcomes. Vaccine. (2015) 33:2108–17. doi: 10.1016/j.vaccine.2015.02.068
139. Giles ML, Krishnaswamy S, Macartney K, Cheng A. The safety of inactivated influenza vaccines in pregnancy for birth outcomes: a systematic review. Hum Vaccin Immunother. (2019) 15:687–99. doi: 10.1080/21645515.2018.1540807
140. Ohfuji S, Deguchi M, Tachibana D, Koyama M, Takagi T, Yoshioka T, et al. Safety of influenza vaccination on adverse birth outcomes among pregnant women: a prospective cohort study in Japan. Int J Infect Dis. (2020) 93:68–76. doi: 10.1016/j.ijid.2020.01.033
141. Donahue JG, Kieke BA, King JP, Mascola MA, Shimabukuro TT, DeStefano F, et al. Inactivated influenza vaccine and spontaneous abortion in the Vaccine Safety Datalink in 2012–13:2013–14, and 2014–15. Vaccine. (2019) 37:6673–81. doi: 10.1016/j.vaccine.2019.09.035
142. Sukumaran L, McCarthy NL, Kharbanda EO, Weintraub ES, Vazquez-Benitez G, McNeil MM, et al. Safety of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis and influenza vaccinations in pregnancy. Obstetr Gynecol. (2015) 126:1069–74. doi: 10.1097/AOG.0000000000001066
143. Frasca D, Diaz A, Romero M, Mendez NV, Landin AM, Blomberg BB. Effects of age on H1N1-specific serum IgG1 and IgG3 levels evaluated during the 2011–2012 influenza vaccine season. Immun Ageing. (2013) 10:14. doi: 10.1186/1742-4933-10-14
144. Jackson LA, Patel SM, Swamy GK, Frey SE, Creech CB, Munoz FM, et al. Immunogenicity of an inactivated monovalent 2009 H1N1 influenza vaccine in pregnant women. J Infect Dis. (2011) 204:854–63. doi: 10.1093/infdis/jir440
145. Horner I, Nanan R, Liu A. Influenza vaccination of pregnant women and protection of their infants. N Engl J Med. (2014) 371:2340. doi: 10.1056/NEJMc1412050
146. Nunes MC, Cutland CL, Dighero B, Bate J, Jones S, Hugo A, et al. Kinetics of hemagglutination-inhibiting antibodies following maternal influenza vaccination among mothers with and those without HIV infection and their infants. J Infect Dis. (2015) 212:1976–87. doi: 10.1093/infdis/jiv339
147. Principi N, Senatore L, Esposito S. Protection of young children from influenza through universal vaccination. Hum Vaccin Immunother. (2015) 11:2350–8. doi: 10.1080/21645515.2015.1055428
148. Nunes MC, Cutland CL, Jones S, Hugo A, Madimabe R, Simoes EA, et al. Duration of infant protection against influenza illness conferred by maternal immunization: secondary analysis of a randomized clinical trial. JAMA Pediatr. (2016) 170:840–7. doi: 10.1001/jamapediatrics.2016.0921
149. Zuccotti G, Pogliani L, Pariani E, Amendola A, Zanetti A. Transplacental antibody transfer following maternal immunization with a pandemic 2009 influenza A(H1N1) MF59-adjuvanted vaccine. JAMA. (2010) 304:2360–1. doi: 10.1001/jama.2010.1729
150. Black S, Nicolay U, Vesikari T, Knuf M, Del Giudice G, Della Cioppa G, et al. Hemagglutination inhibition antibody titers as a correlate of protection for inactivated influenza vaccines in children. Pediatr Infect Dis J. (2011) 30:1081–5. doi: 10.1097/INF.0b013e3182367662
151. Grohskopf LA, Alyanak E, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: recommendations of the advisory committee on immunization practices - United States, 2019–20 Influenza Season. MMWR Recomm Rep. (2019) 68:1–21. doi: 10.15585/mmwr.rr6803a1
152. European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States – Overview of Vaccine Recommendations for 2017–2018 and Vaccination Coverage Rates for 2015–2016 and 2016–2017 Influenza Seasons. Stockholm: ECDC (2018). Available online at: https://ecdc.europa.eu/sites/portal/files/documents/seasonal-influenza-antiviral-use-2018.pdf (accessed November 24, 2019).
153. Sperling RS, Engel SM, Wallenstein S, Kraus TA, Garrido J, Singh T, et al. Immunogenicity of trivalent inactivated influenza vaccination received during pregnancy or postpartum. Obstet Gynecol. (2012) 119:631–9. doi: 10.1097/AOG.0b013e318244ed20
154. Blanchard-Rohner G, Meier S, Bel M, Combescure C, Othenin-Girard V, Swali RAB, et al. Influenza vaccination given at least 2 weeks before delivery to pregnant women facilitates transmission of seroprotective influenza-specific antibodies to the newborn. Pediatr Infect Dis J. (2013) 32:1374–80. doi: 10.1097/01.inf.0000437066.40840.c4
155. Katz J, Englund JA, Steinhoff MC, Khatry SK, Shrestha L, Kuypers J, et al. Impact of timing of influenza vaccination in pregnancy on transplacental antibody transfer, influenza incidence, and birth outcomes: a randomized trial in rural Nepal. Clin Infect Dis. (2018) 67:334–40. doi: 10.1093/cid/ciy090
156. Dodds L, McNeil SA, Fell DB, Allen VM, Coombs A, Scott J, et al. Impact of influenza exposure on rates of hospital admissions and physician visits because of respiratory illness among pregnant women. CMAJ. (2007) 176:463–8. doi: 10.1503/cmaj.061435
157. Vilca LM, Verma A, Bonati M, Campins M. Impact of influenza on outpatient visits and hospitalizations among pregnant women in Catalonia, Spain. J Infect. (2018) 77:553–60. doi: 10.1016/j.jinf.2018.06.015
158. Poehling KA, Edwards KM, Weinberg GA, Szilagyi P, Staat MA, Iwane MK, et al. The underrecognized burden of influenza in young children. N Engl J Med. (2006) 355:31–40. doi: 10.1056/NEJMoa054869
159. Bhat N, Wright JG, Broder KR, Murray EL, Greenberg ME, Glover MJ, et al. Influenza-associated deaths among children in the United States, 2003–2004. N Engl J Med. (2005) 353:2559–67. doi: 10.1056/NEJMoa051721
160. Thompson MG, Li DK, Shifflett P, Sokolow LZ, Ferber JR, Kurosky S, et al. Effectiveness of seasonal trivalent influenza vaccine for preventing influenza virus illness among pregnant women: a population-based case-control study during the 2010–2011 and 2011–2012 influenza seasons. Clin Infect Dis. (2014) 58:449–57. doi: 10.1093/cid/cit750
161. Omer SB, Richards JL, Madhi SA, Tapia MD, Steinhoff MC, Aqil AR, et al. Three randomized trials of maternal influenza immunization in Mali, Nepal, and South Africa: methods and expectations. Vaccine. (2015) 33:3801–12. doi: 10.1016/j.vaccine.2015.05.077
162. Zaman K, Roy E, Arifeen SE, Rahman M, Raqib R, Wilson E, et al. Effectiveness of maternal influenza immunization in mothers and infants. N Engl J Med. (2008) 359:1555–64. doi: 10.1056/NEJMoa0708630
163. Shakib JH, Korgenski K, Presson AP, Sheng X, Varner MW, Pavia AT, et al. Influenza in infants born to women vaccinated during pregnancy. Pediatrics. (2016) 137:e20152360. doi: 10.1542/peds.2015-2360
164. Eick AA, Uyeki TM, Klimov A, Hall H, Reid R, Santosham M, et al. Maternal influenza vaccination and effect on influenza virus infection in young infants. Arch Pediatr Adolesc Med. (2011) 165:104–11. doi: 10.1001/archpediatrics.2010.192
165. Dabrera G, Zhao H, Andrews N, Begum F, Green H, Ellis J, et al. Effectiveness of seasonal influenza vaccination during pregnancy in preventing influenza infection in infants, England, 2013/14. Euro Surveill. (2014) 19:20959. doi: 10.2807/1560-7917.ES2014.19.45.20959
166. Nunes MC, Madhi SA. Influenza vaccination during pregnancy for prevention of influenza confirmed illness in the infants: a systematic review and meta-analysis. Hum Vaccin Immunother. (2018) 14:758–66. doi: 10.1080/21645515.2017.1345385
167. Omer SB, Clark DR, Aqil AR, Tapia MD, Nunes MC, Kozuki N, et al. Maternal Influenza immunization and prevention of severe clinical pneumonia in young infants: analysis of randomized controlled trials conducted in Nepal, Mali and South Africa. Pediatr Infect Dis J. (2018) 37:436–40. doi: 10.1097/INF.0000000000001914
168. European Medicines Agency. Quadrivalent Influenza Vaccine (Split virion, inactivated) (2020). Available online at: https://www.medicines.org.uk/emc/product/666/smpc (accessed February 17, 2020).
169. Giles ML, Cheng AC. Regulatory agencies have a role to play in maintaining consumer confidence in vaccine safety for pregnant women. Hum Vaccines Immunother. (2020). doi: 10.1080/21645515.2020.1718976. [Epub ahead of print].
170. Jones C, Pollock L, Barnett SM, Battersby A, Kampmann B. The relationship between concentration of specific antibody at birth and subsequent response to primary immunization. Vaccine. (2014) 32:996–1002. doi: 10.1016/j.vaccine.2013.11.104
171. Van Savage J, Decker MD, Edwards KM, Sell SH, Karzon DT. Natural history of pertussis antibody in the infant and effect on vaccine response. J Infect Dis. (1990) 161:487–92. doi: 10.1093/infdis/161.3.487
172. Niewiesk S. Maternal antibodies: clinical significance, mechanism of interference with immune responses, and possible vaccination strategies. Front Immunol. (2014) 5:446. doi: 10.3389/fimmu.2014.00446
173. Englund JA, Glezen WP, Thompson C, Anwaruddin R, Turner CS, Siber GR. Haemophilus influenzae type b-specific antibody in infants after maternal immunization. Pediatr Infect Dis J. (1997) 16:1122–30. doi: 10.1097/00006454-199712000-00005
174. Nahm MH, Glezen P, Englund J. The influence of maternal immunization on light chain response to Haemophilus influenzae type b vaccine. Vaccine. (2003) 21:3393–7. doi: 10.1016/S0264-410X(03)00340-2
175. Ladhani SN, Andrews NJ, Southern J, Jones CE, Amirthalingam G, Waight PA, et al. Antibody responses after primary immunization in infants born to women receiving a pertussis-containing vaccine during pregnancy: single arm observational study with a historical comparator. Clin Infect Dis. (2015) 61:1637–44. doi: 10.1093/cid/civ695
176. Maertens K, Cabore RN, Huygen K, Vermeiren S, Hens N, Van Damme P, et al. Pertussis vaccination during pregnancy in Belgium: follow-up of infants until 1 month after the fourth infant pertussis vaccination at 15 months of age. Vaccine. (2016) 34:3613–19. doi: 10.1016/j.vaccine.2016.04.066
177. Maertens K, Hoang TT, Nguyen TD, Cabore RN, Duong TH, Huygen K, et al. The effect of maternal pertussis immunization on infant vaccine responses to a booster pertussis-containing vaccine in Vietnam. Clin Infect Dis. (2016) 63:S197–204. doi: 10.1093/cid/ciw551
178. Zimmermann P, Perrett KP, Messina NL, Donath S, Ritz N, van der Klis FRM, et al. The effect of maternal immunisation during pregnancy on infant vaccine responses. EClin Med. (2019) 13:21–30. doi: 10.1016/j.eclinm.2019.06.010
179. Englund JA, Anderson EL, Reed GF, Decker MD, Edwards KM, Pichichero ME, et al. The effect of maternal antibody on the serologic response and the incidence of adverse reactions after primary immunization with acellular and whole-cell pertussis vaccines combined with diphtheria and tetanus toxoids. Pediatrics. (1995) 96:580–4.
180. Ibrahim R, Ali SA, Kazi AM, Rizvi A, Guterman LB, Bednarczyk RA, et al. Impact of maternally derived pertussis antibody titers on infant whole-cell pertussis vaccine response in a low income setting. Vaccine. (2018) 36:7048–53. doi: 10.1016/j.vaccine.2018.09.045
181. Wanlapakorn N, Maertens K, Vongpunsawad S, Peunpa J, Tran TMP, Hens N, et al. Quantity and quality of antibodies after acellular versus whole cell pertussis vaccines in infants born to mothers who received Tdap during pregnancy: a randomised trial. Clin Infect Dis. (2019). doi: 10.1093/cid/ciz778. [Epub ahead of print].
182. Abu Raya, B, Edwards KM. Interference with pertussis vaccination in infants after maternal pertussis vaccination. Pediatrics. (in press).
183. Maertens K, Burbidge P, van Damme P, Goldblatt D, Leuridan E. Pneumococcal immune response in infants whose mothers received tdap vaccination during pregnancy. Pediatr Infect Dis J. (2017) 36:1186–92. doi: 10.1097/INF.0000000000001601
184. Heininger U. Is there a need for a stand-alone acellular pertussis vaccine? Pediatr Infect Dis J. (2018) 37:359–60. doi: 10.1097/INF.0000000000001767
185. Walter EB, Englund JA, Blatter M, Nyberg J, Ruben FL, Decker MD. Trivalent inactivated influenza virus vaccine given to two-month-old children: An off-season pilot study. Pediatr Infect Dis J. (2009) 28:1099–104. doi: 10.1097/INF.0b013e3181b0c0ca
186. Halasa NB, Gerber MA, Chen Q, Wright PF, Edwards KM. Safety and immunogenicity of trivalent inactivated influenza vaccine in infants. J Infect Dis. (2008) 197:1448–54. doi: 10.1086/587643
187. Siegrist CA. Mechanisms by which maternal antibodies influence infant vaccine responses: review of hypotheses and definition of main determinants. Vaccine. (2003) 21:3406–12. doi: 10.1016/S0264-410X(03)00342-6
188. Naniche D. Human immunology of measles virus infection. Curr Top Microbiol Immunol. (2009) 330:151–71. doi: 10.1007/978-3-540-70617-5_8
189. Kim D, Huey D, Oglesbee M, Niewiesk S. Insights into the regulatory mechanism controlling the inhibition of vaccine-induced seroconversion by maternal antibodies. Blood. (2011) 117:6143–51. doi: 10.1182/blood-2010-11-320317
190. Vono M, Eberhardt CS, Auderset F, Mastelic-Gavillet B, Lemeille S, Christensen D, et al. Maternal antibodies inhibit neonatal and infant responses to vaccination by shaping the early-life B cell repertoire within germinal centers. Cell Rep. (2019) 28:1773–84.e1775. doi: 10.1016/j.celrep.2019.07.047
191. Orije MRP, Maertens K, Corbière V, Wanlapakorn N, Van Damme P, Leuridan E, et al. The effect of maternal antibodies on the cellular immune response after infant vaccination: a review. Vaccine. (2020) 38:20–28. doi: 10.1016/j.vaccine.2019.10.025
192. Rastogi D, Wang C, Mao X, Lendor C, Rothman PB, Miller RL. Antigen-specific immune responses to influenza vaccine in utero. J Clin Invest. (2007) 117:1637–46. doi: 10.1172/JCI29466
193. Esposito S, Principi N. Strategies to develop vaccines of pediatric interest. Expert Rev Vaccines. (2017) 16:175–86. doi: 10.1080/14760584.2017.1237875
194. Charlier C, Beaudoin MC, Couderc T, Lortholary O, Lecuit M. Arboviruses and pregnancy: maternal, fetal, and neonatal effects. Lancet Child Adolesc Health. (2017) 1:134–46. doi: 10.1016/S2352-4642(17)30021-4
195. Carles G, Peiffer H, Talarmin A. Effects of dengue fever during pregnancy in French Guiana. Clin Infect Dis. (1999) 28:637–40. doi: 10.1086/515144
196. Kleber de Oliveira W, Cortez-Escalante J, De Oliveira WT, do Carmo GM, Henriques CM, et al. Increase in reported prevalence of microcephaly in infants born to women living in areas with confirmed zika virus transmission during the first trimester of pregnancy - Brazil, 2015. MMWR Morb Mortal Wkly Rep. (2016) 65:242–7. doi: 10.15585/mmwr.mm6509e2
197. Abbink P, Stephenson KE, Barouch DH. Zika virus vaccines. Nat Rev Microbiol. (2018) 16:594–600. doi: 10.1038/s41579-018-0039-7
198. Thisyakorn U, Thisyakorn C. Latest developments and future directions in dengue vaccines. Ther Adv Vaccines. (2014) 2:3–9. doi: 10.1177/2051013613507862
199. Phares CR, Lynfield R, Farley MM, Mohle-Boetani J, Harrison LH, Petit S, et al. Epidemiology of invasive group B streptococcal disease in the United States, 1999–2005. JAMA. (2008) 299:2056–65. doi: 10.1001/jama.299.17.2056
200. Tapiainen T, Koivusaari P, Brinkac L, Lorenzi HA, Salo J, Renko M, et al. Impact of intrapartum and postnatal antibiotics on the gut microbiome and emergence of antimicrobial resistance in infants. Sci Rep. (2019) 9:10635. doi: 10.1038/s41598-019-46964-5
201. Di Renzo GC, Melin P, Berardi A, Blennow M, Carbonell-Estrany X, Donzelli GP, et al. Intrapartum GBS screening and antibiotic prophylaxis: a European consensus conference. J Matern Fetal Neonatal Med. (2015) 28:766–82. doi: 10.3109/14767058.2014.934804
202. Seale AC, Baker CJ, Berkley JA, Madhi SA, Ordi J, Saha SK, et al. Vaccines for maternal immunization against Group B Streptococcus disease: WHO perspectives on case ascertainment and case definitions. Vaccine. (2019) 37:4877–85. doi: 10.1016/j.vaccine.2019.07.012
203. Dzanibe S, Madhi SA. Systematic review of the clinical development of group B streptococcus serotype-specific capsular polysaccharide-based vaccines. Expert Rev Vaccines. (2018) 17:635–51. doi: 10.1080/14760584.2018.1496021
204. Madrid L, Seale AC, Kohli-Lynch M, Edmond KM, Lawn JE, Heath PT, et al. Infant Group B streptococcal disease incidence and serotypes worldwide: systematic review and meta-analyses. Clin Infect Dis. (2017) 65:S160–72. doi: 10.1093/cid/cix656
205. Shabayek S, Spellerberg B. Group B Streptococcal Colonization, Molecular Characteristics, and Epidemiology. Front Microbiol. (2018) 9:437. doi: 10.3389/fmicb.2018.00437
206. Song JY, Lim JH, Lim S, Yong Z, Seo HS. Progress toward a group B streptococcal vaccine. Hum Vaccin Immunother. (2018) 14:2669–81. doi: 10.1080/21645515.2018.1493326
207. Le Doare K, Kampmann B, Vekemans J, Heath PT, Goldblatt D, Nahm MH, et al. Serocorrelates of protection against infant group B streptococcus disease. Lancet Infect Dis. (2019) 19:e162–71. doi: 10.1016/S1473-3099(18)30659-5
208. Heyderman RS, Madhi SA, French N, Cutland C, Ngwira B, Kayambo D, et al. Group B streptococcus vaccination in pregnant women with or without HIV in Africa: a non-randomised phase 2, open-label, multicentre trial. Lancet Infect Dis. (2016) 16:546–55. doi: 10.1016/S1473-3099(15)00484-3
209. Fabbrini M, Rigat F, Tuscano G, Chiarot E, Donders G, Devlieger R, et al. Functional activity of maternal and cord antibodies elicited by an investigational group B Streptococcus trivalent glycoconjugate vaccine in pregnant women. J Infect. (2018) 76:449–56. doi: 10.1016/j.jinf.2018.01.006
210. Madhi SA, Cutland CL, Jose L, Koen A, Govender N, Wittke F, et al. Safety and immunogenicity of an investigational maternal trivalent group B streptococcus vaccine in healthy women and their infants: a randomised phase 1b/2 trial. Lancet Infect Dis. (2016) 16:923–34. doi: 10.1016/S1473-3099(16)00152-3
211. Madhi SA, Koen A, Cutland CL, Jose L, Govender N, Wittke F, et al. Antibody kinetics and response to routine vaccinations in infants born to women who received an investigational trivalent group B streptococcus polysaccharide CRM197-conjugate vaccine during pregnancy. Clin Infect Dis. (2017) 65:1897–904. doi: 10.1093/cid/cix666
212. Shi T, McAllister DA, O'Brien KL, Simoes EAF, Madhi SA, Gessner BD, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. (2017) 390:946–58. doi: 10.1016/S0140-6736(17)30938-8
213. Baraldi E, Lanari M, Manzoni P, Rossi GA, Vandini S, Rimini A, et al. Inter-society consensus document on treatment and prevention of bronchiolitis in newborns and infants. Ital J Pediatr. (2014) 40:65. doi: 10.1186/1824-7288-40-65
214. Borchers AT, Chang C, Gershwin ME, Gershwin LJ. Respiratory syncytial virus–a comprehensive review. Clin Rev Allergy Immunol. (2013) 45:331–79. doi: 10.1007/s12016-013-8368-9
215. Resch B. Product review on the monoclonal antibody palivizumab for prevention of respiratory syncytial virus infection. Hum Vaccin Immunother. (2017) 13:2138–49. doi: 10.1080/21645515.2017.1337614
216. Wegzyn C, Toh LK, Notario G, Biguenet S, Unnebrink K, Park C, et al. Safety and effectiveness of palivizumab in children at high risk of serious disease due to respiratory syncytial virus infection: a systematic review. Infect Dis Ther. (2014) 3:133–58. doi: 10.1007/s40121-014-0046-6
217. Robbie GJ, Criste R, Dall'acqua WF, Jensen K, Patel NK, Losonsky GA, et al. A novel investigational Fc-modified humanized monoclonal antibody, motavizumab-YTE, has an extended half-life in healthy adults. Antimicrob Agents Chemother. (2013) 57:6147–53. doi: 10.1128/AAC.01285-13
218. Gerretsen HE, Sande CJ. Development of respiratory syncytial virus (RSV) vaccines for infants. J Infect. (2017) 74(Suppl. 1):S143–6. doi: 10.1016/S0163-4453(17)30205-0
219. August A, Glenn GM, Kpamegan E, Hickman SP, Jani D, Lu H, et al. A Phase 2 randomized, observer-blind, placebo-controlled, dose-ranging trial of aluminum-adjuvanted respiratory syncytial virus F particle vaccine formulations in healthy women of childbearing age. Vaccine. (2017) 35:3749–59. doi: 10.1016/j.vaccine.2017.05.045
220. Munoz FM, Swamy GK, Hickman SP, Agrawal S, Piedra PA, Glenn GM, et al. Safety and immunogenicity of a respiratory syncytial virus fusion (F) protein nanoparticle vaccine in healthy third-trimester pregnant women and their infants. J Infect Dis. (2019) 220:1802–15. doi: 10.1093/infdis/jiz390
221. Chu HY, Tielsch J, Katz J, Magaret AS, Khatry S, LeClerq SC, et al. Transplacental transfer of maternal respiratory syncytial virus (RSV) antibody and protection against RSV disease in infants in rural Nepal. J Clin Virol. (2017) 95:90–95. doi: 10.1016/j.jcv.2017.08.017
222. Glezen WP, Paredes A, Allison JE, Taber LH, Frank AL. Risk of respiratory syncytial virus infection for infants from low-income families in relationship to age, sex, ethnic group, and maternal antibody level. J Pediatr. (1981) 98:708–15. doi: 10.1016/S0022-3476(81)80829-3
223. Nyiro JU, Sande CJ, Mutunga M, Kiyuka PK, Munywoki PK, Scott JA, et al. Absence of association between cord specific antibody levels and severe Respiratory Syncytial Virus (RSV) disease in early infants: a case control study from coastal Kenya. PLoS ONE. (2016) 11:e0166706. doi: 10.1371/journal.pone.0166706
224. Muñoz F, Madhi S, Swamy GK, Heath PT, Vrbicky K, Glenn G, et al. Phase 3 PREPARE study: efficacy and safety of an RSV vaccine administered to pregnant women for the prevention of RSV lower respiratory tract infection in infants. In: 37 Annual Meeting of the European Society for Pediatric Infectious Diseases. Ljubljana (2019).
225. Maertens K, De Schutter S, Braeckman T, Baerts L, Van Damme P, De Meester I, et al. Breastfeeding after maternal immunisation during pregnancy: providing immunological protection to the newborn: a review. Vaccine. (2014) 32:1786–92. doi: 10.1016/j.vaccine.2014.01.083
226. Abu Raya B, Srugo I, Kessel A, Peterman M, Bader D, Peri R, et al. The induction of breast milk pertussis specific antibodies following gestational tetanus-diphtheria-acellular pertussis vaccination. Vaccine. (2014) 32:5632–7. doi: 10.1016/j.vaccine.2014.08.006
227. De Schutter S, Maertens K, Baerts L, De Meester I, Van Damme P, Leuridan E. Quantification of vaccine-induced antipertussis toxin secretory IgA antibodies in breast milk: comparison of different vaccination strategies in women. Pediatr Infect Dis J. (2015) 34:e149–52. doi: 10.1097/INF.0000000000000675
228. Schlaudecker EP, Steinhoff MC, Omer SB, McNeal MM, Roy E, Arifeen SE, et al. IgA and neutralizing antibodies to influenza a virus in human milk: a randomized trial of antenatal influenza immunization. PLoS ONE. (2013) 8:e70867. doi: 10.1371/journal.pone.0070867
229. Dangor Z, Khan M, Kwatra G, Izu A, Nakwa F, Ramdin T, et al. The association between breastmilk group B Streptococcal capsular antibody levels and late-onset disease in young infants. Clin Infect Dis. (2019) 70: 1110–14. doi: 10.1093/cid/ciz360
230. Mazur NI, Horsley NM, Englund JA, Nederend M, Magaret A, Kumar A, et al. Breast milk prefusion F immunoglobulin G as a correlate of protection against respiratory syncytial virus acute respiratory illness. J Infect Dis. (2019) 219:59–67. doi: 10.1093/infdis/jiy477
231. World Health Organization. Maternal and Neonatal Tetanus Elimination by 2005: Strategies for Achieving and Maintaining Elimination. Geneva: WHO (2000). Available online at: https://apps.who.int/iris/bitstream/handle/10665/69618/WHO_V-B_02.09_eng.pdf?sequence=1&isAllowed=y (accessed December 15, 2018).
232. Esposito S, Tremolati E, Bellasio M, Chiarelli G, Marchisio P, Tiso B, et al. Attitudes and knowledge regarding influenza vaccination among hospital health workers caring for women and children. Vaccine. (2007) 25:5283–9. doi: 10.1016/j.vaccine.2007.05.011
233. Mak TK, Mangtani P, Leese J, Watson JM, Pfeifer D. Influenza vaccination in pregnancy: current evidence and selected national policies. Lancet Infect Dis. (2008) 8:44–52. doi: 10.1016/S1473-3099(07)70311-0
234. Centers for Disease Control and Prevention (CDC). Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months — Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. (2011) 60:1424–6.
235. Kahn KE, Black CL, Ding H, Williams WW, Lu PJ, Fiebelkorn AP, et al. Influenza and Tdap vaccination coverage among pregnant women - United States, April 2018. MMWR Morb Mortal Wkly Rep. (2018) 67:1055–9. doi: 10.15585/mmwr.mm6738a3
236. Public Health England. Pertussis Vaccination Programme for Pregnant Women Update: Vaccine Coverage in England, April to June 2018. Health Protection Report, Vol. 12.
237. World Health Organizaion. WHO Europe/ECDC joint statement: Low Uptake of Seasonal Influenza Vaccination in Europe May Jeopardize Capacity to Protect People in Next Pandemic. Available online at: https://www.euro.who.int/en/media-centre/sections/press-releases/2018/who-europeecdc-joint-statement-low-uptake-of-seasonal-influenza-vaccination-in-europe-may-jeopardize-capacity-to-protect-people-in-next-pandemic (accessed December 15, 2018).
238. Descamps A, Launay O, Bonnet C, Blondel B. Seasonal influenza vaccine uptake and vaccine refusal among pregnant women in France: results from a national survey. Hum Vaccin Immunother. (2019) 16:1093–100. doi: 10.1080/21645515.2019.1688035
239. Erb ML, Erlanger TE, Heininger U. Child-parent immunization survey: how well are national immunization recommendations accepted by the target groups? Vaccine X. (2019) 1:100013. doi: 10.1016/j.jvacx.2019.100013
240. Lutz CS, Carr W, Cohn A, Rodriguez L. Understanding barriers and predictors of maternal immunization: identifying gaps through an exploratory literature review. Vaccine. (2018) 36:7445–55. doi: 10.1016/j.vaccine.2018.10.046
241. Shavell VI, Moniz MH, Gonik B, Beigi RH. Influenza immunization in pregnancy: overcoming patient and health care provider barriers. Am J Obstet Gynecol. (2012) 207:S67–74. doi: 10.1016/j.ajog.2012.06.077
242. Broughton DE, Beigi RH, Switzer GE, Raker CA, Anderson BL. Obstetric health care workers' attitudes and beliefs regarding influenza vaccination in pregnancy. Obstet Gynecol. (2009) 114:981–7. doi: 10.1097/AOG.0b013e3181bd89c2
243. Leddy MA, Anderson BL, Power ML, Gall S, Gonik B, Schulkin J. Changes in and current status of obstetrician-gynecologists' knowledge, attitudes, practice regarding immunization. Obstet Gynecol Surv. (2009) 64:823–9. doi: 10.1097/OGX.0b013e3181c4bbb7
244. Power ML, Leddy MA, Anderson BL, Gall SA, Gonik B, Schulkin J. Obstetrician-gynecologists' practices and perceived knowledge regarding immunization. Am J Prev Med. (2009) 37:231–4. doi: 10.1016/j.amepre.2009.05.019
245. Vilca LM, Martínez C, Burballa M, Campins M. Maternal care providers' barriers regarding influenza and pertussis vaccination during pregnancy in Catalonia, Spain. Matern Child Health J. (2018) 22:1016–24. doi: 10.1007/s10995-018-2481-6
246. Beigi RH, Fortner KB, Munoz FM, Roberts J, Gordon JL, Han HH, et al. Maternal immunization: opportunities for scientific advancement. Clin Infect Dis. (2014) 59(Suppl. 7):S408–14. doi: 10.1093/cid/ciu708
247. Frew PM, Kriss JL, Chamberlain AT, Malik F, Chung Y, Cortés M, et al. A randomized trial of maternal influenza immunization decision-making: a test of persuasive messaging models. Hum Vaccin Immunother. (2016) 12:1989–96. doi: 10.1080/21645515.2016.1199309
248. Goodman K, Mossad SB, Taksler GB, Emery J, Schramm S, Rothberg MB. Impact of video education on influenza vaccination in pregnancy. J Reprod Med. (2015) 60:471–9.
249. Kriss JL, Frew PM, Cortes M, Malik FA, Chamberlain AT, Seib K, et al. Evaluation of two vaccine education interventions to improve pertussis vaccination among pregnant African American women: a randomized controlled trial. Vaccine. (2017) 35:1551–8. doi: 10.1016/j.vaccine.2017.01.037
250. Meharry PM, Cusson RM, Stiller R, Vázquez M. Maternal influenza vaccination: evaluation of a patient-centered pamphlet designed to increase uptake in pregnancy. Matern Child Health J. (2014) 18:1205–14. doi: 10.1007/s10995-013-1352-4
251. Panda B, Stiller R, Panda A. Influenza vaccination during pregnancy and factors for lacking compliance with current CDC guidelines. J Matern Fetal Neonatal Med. (2011) 24:402–6. doi: 10.3109/14767058.2010.497882
252. Ledent E, Gabutti G, de Bekker-Grob EW, Alcázar Zambrano JL, Campins Martí M, Del Hierro Gurruchaga MT, et al. Attributes influencing parental decision-making to receive the Tdap vaccine to reduce the risk of pertussis transmission to their newborn - outcome of a cross-sectional conjoint experiment in Spain and Italy. Hum Vaccin Immunother. (2019) 15:1080–91. doi: 10.1080/21645515.2019.1571890
253. Vilca LM, Esposito S. The crucial role of maternal care providers as vaccinators for pregnant women. Vaccine. (2018) 36:5379–84. doi: 10.1016/j.vaccine.2017.08.017
254. Chamberlain AT, Berkelman RL, Ault KA, Rosenberg ES, Orenstein WA, Omer SB. Trends in reasons for non-receipt of influenza vaccination during pregnancy in Georgia, 2004–2011. Vaccine. (2016) 34:1597–603. doi: 10.1016/j.vaccine.2016.01.058
255. Danchin MH, Costa-Pinto J, Attwell K, Willaby H, Wiley K, Hoq M, et al. Vaccine decision-making begins in pregnancy: correlation between vaccine concerns, intentions and maternal vaccination with subsequent childhood vaccine uptake. Vaccine. (2018) 36:6473–9. doi: 10.1016/j.vaccine.2017.08.003
Keywords: group B Streptococcus vaccines, influenza, maternal immunization, pertussis, pregnant women, respiratory syncytial virus, tetanus
Citation: Abu-Raya B, Maertens K, Edwards KM, Omer SB, Englund JA, Flanagan KL, Snape MD, Amirthalingam G, Leuridan E, Damme PV, Papaevangelou V, Launay O, Dagan R, Campins M, Cavaliere AF, Frusca T, Guidi S, O'Ryan M, Heininger U, Tan T, Alsuwaidi AR, Safadi MA, Vilca LM, Wanlapakorn N, Madhi SA, Giles ML, Prymula R, Ladhani S, Martinón-Torres F, Tan L, Michelin L, Scambia G, Principi N and Esposito S (2020) Global Perspectives on Immunization During Pregnancy and Priorities for Future Research and Development: An International Consensus Statement. Front. Immunol. 11:1282. doi: 10.3389/fimmu.2020.01282
Received: 12 March 2020; Accepted: 20 May 2020;
Published: 24 June 2020.
Edited by:
Fabio Bagnoli, GlaxoSmithKline, ItalyReviewed by:
Thorsten Demberg, Marker Therapeutics, United StatesSelidji Todagbe Agnandji, Centre de Recherche Médicales de Lambaréné, Gabon
Copyright © 2020 Abu-Raya, Maertens, Edwards, Omer, Englund, Flanagan, Snape, Amirthalingam, Leuridan, Damme, Papaevangelou, Launay, Dagan, Campins, Cavaliere, Frusca, Guidi, O'Ryan, Heininger, Tan, Alsuwaidi, Safadi, Vilca, Wanlapakorn, Madhi, Giles, Prymula, Ladhani, Martinón-Torres, Tan, Michelin, Scambia, Principi and Esposito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanna Esposito, c3VzYW5uYW1hcmlhcm9iZXJ0YS5lc3Bvc2l0b0B1bmlwci5pdA==