 Dominika Ambrożej1,2
Dominika Ambrożej1,2 Heidi Makrinioti3
Heidi Makrinioti3 Abigail Whitehouse4
Abigail Whitehouse4 Nikolas Papadopoulos5,6
Nikolas Papadopoulos5,6 Marek Ruszczyński7Aleksander Adamiec1,2
Marek Ruszczyński7Aleksander Adamiec1,2 Jose A. Castro-Rodriguez8Khalid Alansari9,10,11Tuomas Jartti12,13,14
Jose A. Castro-Rodriguez8Khalid Alansari9,10,11Tuomas Jartti12,13,14 Wojciech Feleszko1*
Wojciech Feleszko1*- 1Department of Pediatric Pneumonology and Allergy, Medical University of Warsaw, Warsaw, Poland
- 2Doctoral School, Medical University of Warsaw, Warsaw, Poland
- 3Harvard T.H. Chan School of Public Health, Boston, MA, United States
- 4Centre for Genomics and Child Health, Queen Mary University of London, London, United Kingdom
- 5Division of Infection, Immunity and Respiratory Medicine, University of Manchester, Manchester, United Kingdom
- 6Allergy Department, 2nd Pediatric Clinic, University of Athens, Athens, Greece
- 7Department of Pediatrics, Medical University of Warsaw, Warsaw, Poland
- 8Department of Pediatric Pulmonology and Cardiology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
- 9Department of Pediatric Emergency Medicine, Sidra Medicine, Doha, Qatar
- 10Clinical Pediatrics, Qatar University College of Medicine, Doha, Qatar
- 11Clinical Pediatrics, Weill Cornell Medical College- Qatar, Doha, Qatar
- 12Department of Pediatrics, Turku University Hospital and University of Turku, Turku, Finland
- 13PEDEGO Research Unit, Medical Research Center, University of Oulu, Oulu, Finland
- 14Department of Pediatrics and Adolescent Medicine, Oulu University Hospital, Oulu, Finland
It has become clear that severe bronchiolitis is a heterogeneous disease; even so, current bronchiolitis management guidelines rely on the one-size-fits-all approach regarding achieving both short-term and chronic outcomes. It has been speculated that the use of molecular markers could guide more effective pharmacological management and achieve the prevention of chronic respiratory sequelae. Existing data suggest that asthma-like treatment (systemic corticosteroids and beta2-agonists) in infants with rhinovirus-induced bronchiolitis is associated with improved short-term and chronic outcomes, but robust data is still lacking. We performed a systematic search of PubMed, Embase, Web of Science, and the Cochrane’s Library to identify eligible randomized controlled trials to determine the efficacy of a personalized, virus-dependent application of systemic corticosteroids in children with severe bronchiolitis. Twelve studies with heterogeneous methodology were included. The analysis of the available results comparing the respiratory syncytial virus (RSV)-positive and RSV-negative children did not reveal significant differences in the associatons between systemic corticosteroid use in acute episode and duration of hospitalization (short-term outcome). However, this systematic review identified a trend of the positive association between the use of systematic corticosteroids and duration of hospitalization in RSV-negative infants hospitalized with the first episode of bronchiolitis (two studies). This evidence is not conclusive. Taken together, we suggest the design for future studies to assess the respiratory virus type in guiding predictive enrichment approaches in infants presenting with the first episode of bronchiolitis.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42020173686
Introduction
It is believed that the first severe episode of wheezing, or severe bronchiolitis, may be the first sign of developing asthma; therefore, immunological methods for its early detection are being sought to implement efficient management early (1, 2). In addition, mechanistic studies have shown that viral respiratory infections can contribute to type 2 inflammation (3, 4). The restriction to access to airway samples in infants has complicated the investigation of host immune responses to respiratory viruses, limiting our understanding of these processes and, thus, impacting the appropriate choice of therapeutic strategies that can benefit children presenting with the first episode of bronchiolitis.
The current conservative bronchiolitis management relies on the one-size-fits-all approach regardless of short-term and chronic outcomes. However, the common clinical practice based on the use of systemic corticosteroids in bronchiolitis has not been supported by any systematic review. Thus, systemic corticosteroids are not recommended as the first-line treatment in any international guidelines for managing bronchiolitis and mainstream bronchiolitis care is solely supportive (5–9).
On the other hand, increasing evidence demonstrates that bronchiolitis is a heterogeneous disease and that a viral trigger may be one of the key exposures and part of the underlying pathobiology, very important in identifying endotypes (2, 10, 11). Although the clinical features of bronchiolitis attributed to different viruses are usually indistinguishable, the recently recognized bronchiolitis profiles are associated with various risks for recurrent wheeze and asthma, some differences in disease severity, and, potentially, different therapeutic responses to systemic corticosteroids (10–13). For example, it has been shown that human rhinovirus (HRV)-associated bronchiolitis can result in shorter hospitalization times than bronchiolitis caused by the respiratory syncytial virus (RSV); however, the evidence around associations between virus type and severity is still unclear (14, 15). While most children hospitalized due to bronchiolitis have an uneventful course, it should be remembered that approximately 2-6% require admission to pediatric intensive care units and invasive mechanical ventilation, or even occasionally be fatal (16–18).
Likewise, current studies evaluated the efficacy of systemic corticosteroid therapy in severe bronchiolitis (19–21). In evaluating these studies, one should remember that the sample size was not homogeneous. Therefore, other confounding factors, such as respiratory virus type or peripheral blood eosinophilia or parental history of asthma/allergy, were not evaluated. Furthermore, the effectiveness of the systemic corticosteroids may not depend on the virus type per se but potentially on the eosinophilic airway inflammation, which is often present in atopic children and/or accompanied by a HRV-induced respiratory infection (22, 23).
Recognition of the variability of bronchiolitis, coupled with the failure to identify effective therapies, has provided incentives to establish a precision medicine approach in bronchiolitis management (24). Precision medicine refers to the customization of diagnostic and therapeutic processes based on the unique features of an individual patient (25, 26), and this concept is called the “concept of enrichment” (27). Prognostic enrichment reflects the selection of patients more prone to a disease-related event, such as mortality. Meanwhile, predictive enrichment refers to selecting patients more likely to respond to therapy based on the biological mechanism.
Currently, no clear evidence suggests using respiratory virus testing as a guide for systemic corticosteroids in the first episode of severe bronchiolitis. Therefore, we aimed to systematically revise the literature on whether the respiratory virus type can guide predictive enrichment approaches in the first episode of bronchiolitis.
Methods
Search strategy
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (28) and was registered in the National Institute for Health Research’s PROSPERO (CRD42020173686).
Four bibliographic databases were searched (PubMed, Web of Science, Embase, and Cochrane’s Library) from inception to September 23, 2019. Additionally, the updated search was conducted closer to submission (January 04, 2022). The search term (*steroid* OR *predniso* OR dexamethasone) AND (wheez* OR bronchiolitis) was followed using a Boolean methodology. All extracted citations were imported into EndNote® reference manager (Version X8, Clarivate Analytics, 2016). After removing the duplicates, two reviewers (DA and HM) working independently screened the retrieved titles and abstracts.
Subsequently, all potentially relevant publications were assessed in full text. At each stage, uncertainty about the eligibility of studies for the review was resolved through discussion and through obtaining consensus by other reviewers (AW, NP, WF, TJ), if necessary.
Eligibility criteria
Main eligibility criteria included publication in English language, randomized controlled trial design (RCTs), age group under two years old, the clinical presentation with the first episode of bronchiolitis or wheezing episode at the hospital setting (emergency department (ED) and/or ward), intervention with the administration of systemic corticosteroids, that assessed viral etiology of the illness.
Exclusion criteria included duplicate publications, non-human studies, RCTs that did not involve management at the ED or admission to the paediatric ward, RCTs including children presenting with confirmed one viral agent (e.g., only RSV-positive cases), RCTs including children who received inhaled corticosteroids as the trial intervention, study protocols, editorials or review papers, and conference abstracts.
Actions were taken to contact corresponding authors when additional clarification and further data were required.
Our primary outcomes were viral-dependent short-term outcomes, such as change in the baseline clinical severity scores (i.e., the Respiratory Distress Assessment Instrument, RDAI), need for oxygen therapy, hospitalization rate in the ED studies, and length of hospitalization in the inpatient studies. The secondary outcomes of our review included viral-dependent long-term outcomes (two months or longer after the study enrollment) such as re-admission to medical center due to respiratory symptoms or initiation of regular controller medication for asthma symptoms.
Study extraction and synthesis
Data were extracted from each included study for the following parameters: (a) study origin, (b) participant details, (c) diagnostic intervention(s) and the type of systemic corticosteroids used, (d) administered control, (e) short-term and long-term outcomes, (f) details on results assessed per viral etiology, (g) overall risk of bias assessment, and (h) potential confounding factor(s).
Given the small number of studies utilizing similar methodology and describing virus detection data, meta‐analysis was not possible, and consequently, a narrative synthesis method was used.
Risk of bias assessment
Two independent reviewers (DA, HM) assessed the risk of bias in each of the included studies without being blinded to the authors or journal. A revised Cochrane risk-of-bias tool for randomized trials was used (RoB 2) (29). Encountered discrepancies were resolved through a discussion of all the reviewers. The RoB 2 tool is structured into five bias domains, which enables to judge the randomization process, deviations from intended interventions, any missing outcome data, measurement of the outcome, selection of the reported result.
The judgments for each domain were to choose between “low risk of bias”, “some concerns”, or “high risk of bias”. In conclusion, the overall bias was determined by reflecting the individual marks. The graphical summary of the risk of bias assessment was performed using the robvis online tool (30).
Results
Description of the studies
Following the systematic search, 6831 records were obtained, including 5947 unique citations. The PRISMA flow chart is shown in Figure 1. The screening of titles and abstracts excluded 5788 articles, rendering 159 to full-text assessment. Finally, twelve studies fulfilling the inclusion criteria for systemic application of corticosteroids in the first episode (corticosteroid-naïve) of bronchiolitis and details on the performed viral detection were included (n=1931, see Table 1) (31–41, 43). The included studies were conducted in different parts of the world – three studies in Europe (Ireland, Finland) (33, 38, 43), one study in South America (Paraguay) (41), six in North America (USA, Canada) (31, 34, 36, 37, 39, 40), and two in Asia (32, 35). Two of the studies were multicenter (39, 40).
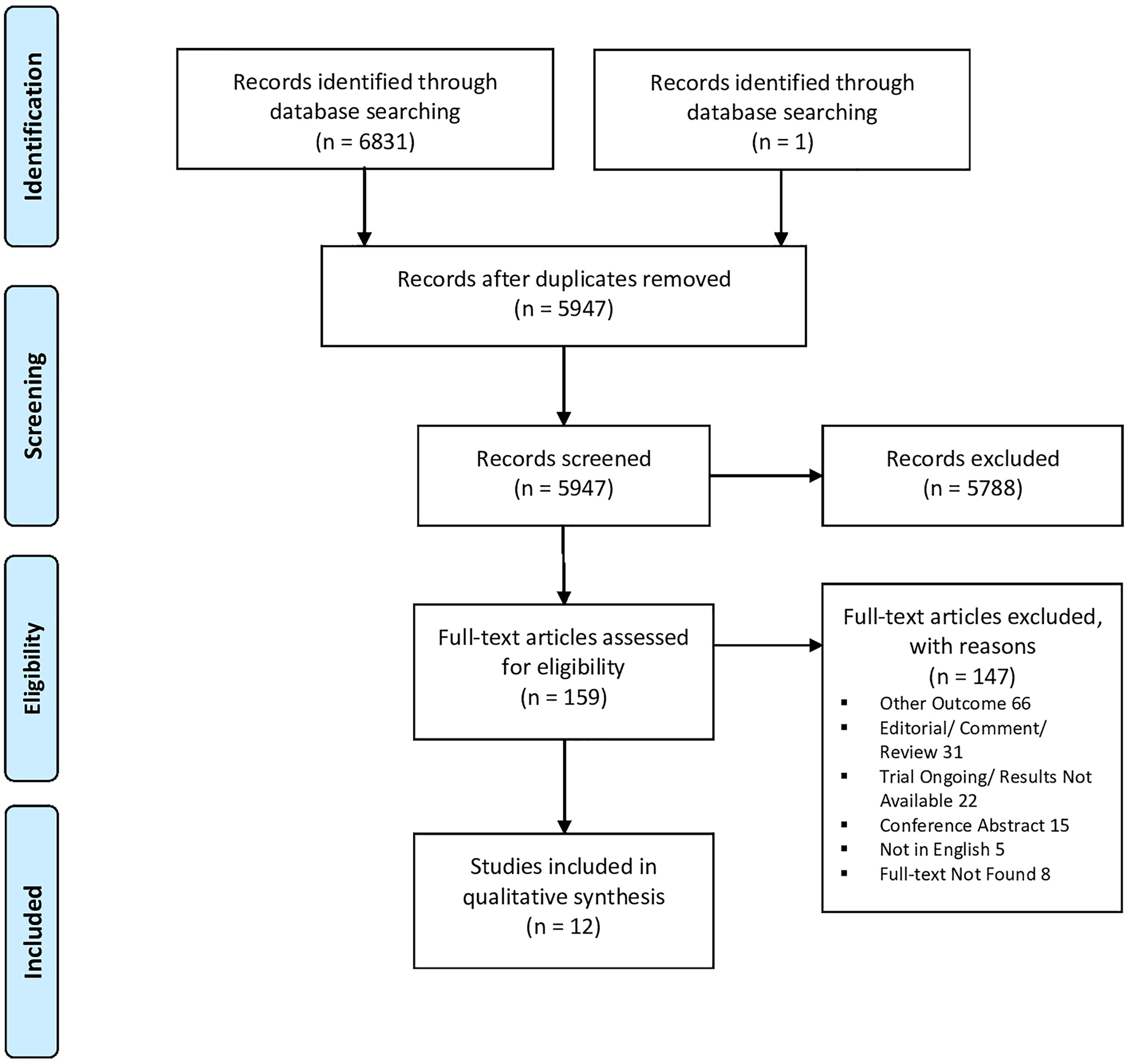
Figure 1 Prisma flow diagram of the study.
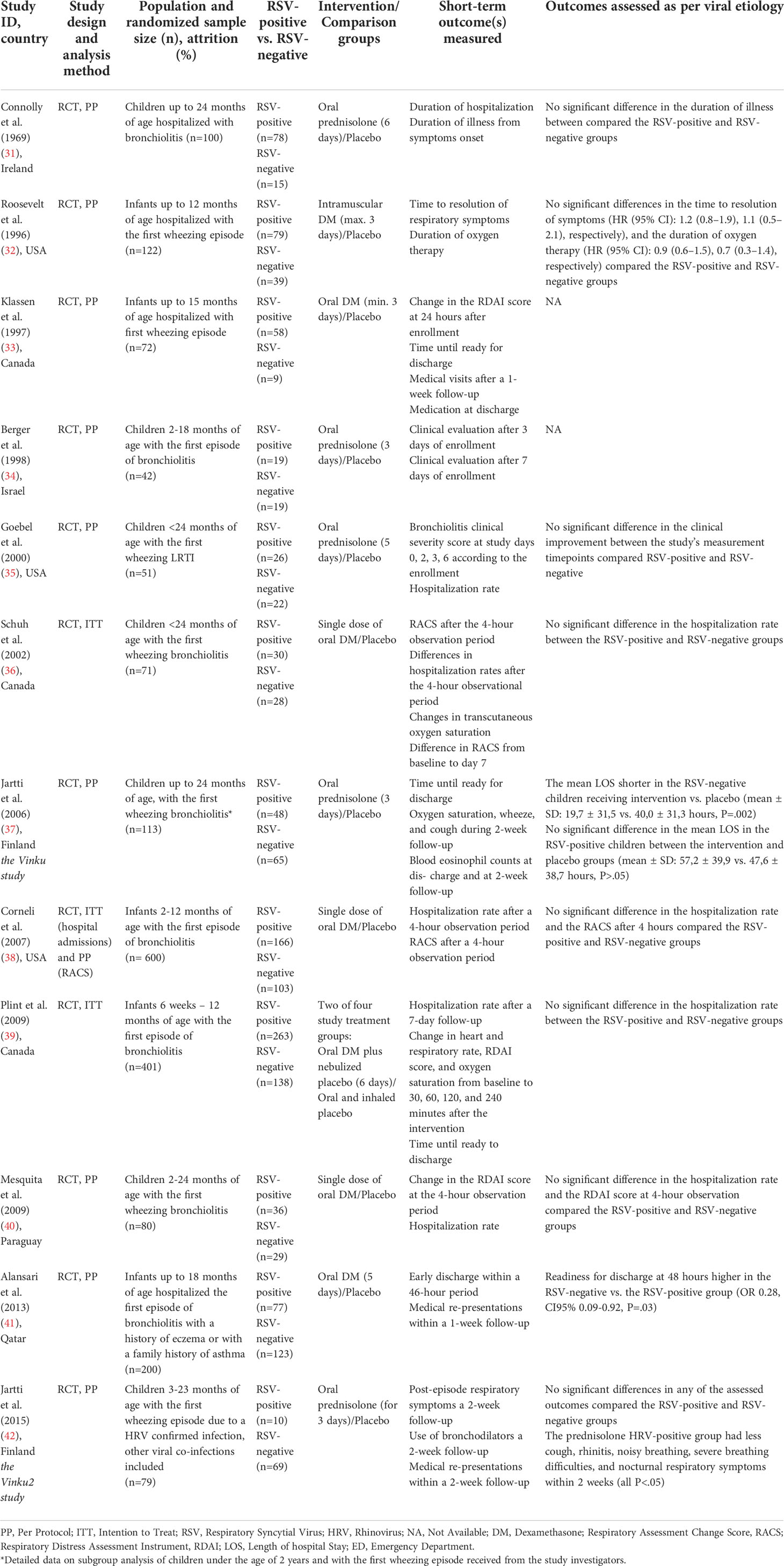
Table 1 Characteristics of the included studies in the magnitude of short-term outcome assessment.
Among the included studies, the overall risk of bias was considered low (33–38) in six, or only with some concerns in three of them (31, 32, 41) (Figure 2). However, one of the studies were judged as with a high risk of bias (43). Their methodological concerns included poor data availability on randomization and blinding process, deviations from the intended intervention, potentially missing outcome data, and some discrepancies in reporting results. Notably, most of the papers presented the results according to the per-protocol analysis (31–36, 38, 41, 43), which might have led to the increased bias. The attempt was made to perform the quantitative synthesis of the short-term effectiveness of corticosteroids in the first episode of bronchiolitis compared between RSV-positive and RSV-negative groups; however, we encountered a significant heterogeneity that heterogeneity (I2>75%) that any potential subgroup analysis could not have avoided.
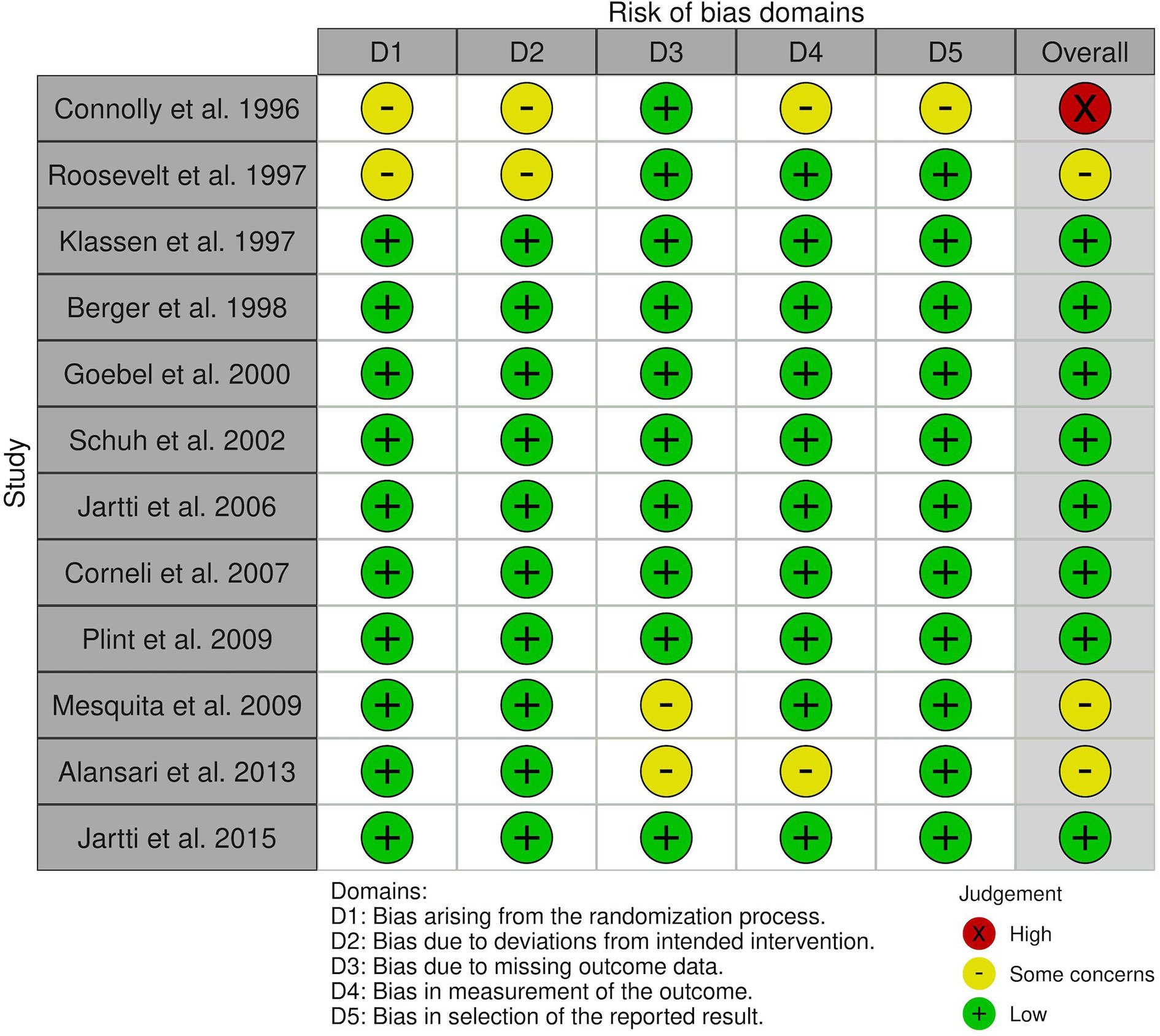
Figure 2 Summary of risk of bias assessment of the eligible studies.
Population
The age of eligible participants differed between the included studies. Three studies, all based in the USA, recruited infants up to 12 months of age (31, 39, 40). The remaining studies included children up to 15 (34), 18 (32, 35) or 24 (33, 36, 37, 41, 43) months of age. One of the RCTs initially analyzed children under the age of 3 years; however, according to predefined inclusion criteria, we decided to selectively assess only the patients under the age of 2 years (38). All studies included patients with wheezing as one of the compulsory criteria apart from one (32), in which crackles or wheezing were needed on inspection. Six studies were conducted in the ED units and the pediatrics wards (35–37, 39–41), while six of the studies recruited solely hospitalized children (31–34, 38, 43).
Viral detection
Most of the identified studies performed viral detection tests only on the presence of RSV (31, 32, 34–37, 39, 40). The other additionally detected viruses included HRV, bocavirus (33, 38), influenza virus (33, 38, 41, 43), parainfluenza virus (33, 38, 43), and adenovirus (33, 38, 41, 43). Moreover, the viral detection techniques varied across the studies, i.e., virus isolation, serology testing, rapid immunoassay method of nasopharyngeal swabs, and PCR tests. Two out of twelve studies did not provide the results with an adjustment to the performed viral testing (34, 35).
Interventions
The systemic corticosteroids were administered orally in all the included studies, apart from one in which intramuscular injections were used (31) (Table 1). Prednisolone served as the intervention drug in five studies (33, 35, 36, 38, 43), while dexamethasone was used in the remaining seven (31, 32, 34, 37, 39–41). Usually, prednisolone was given orally at 2 mg/kg/day (33, 35, 36, 38), while in one study decreasing dosages starting from 15 mg to 2,5 mg were administered (43). Furthermore, the heterogeneity across the duration of the interventions was noticed. A single dose of corticosteroids was administered in three studies (37, 39, 41). The 3-day intervention course was introduced in five RCTs (31, 33–35, 38). The 5-, 6-, or 7-day treatment with corticosteroids was tested in four studies (32, 36, 40, 43).
Short-term outcomes of corticosteroid treatment in severe bronchiolitis per viral etiology
Only two studies showed significant differences in the short-term efficacy of systemic corticosteroids compared between RSV-positive and RSV-negative groups (n=313) (32, 38).
In one of these studies, the mean duration of hospitalization of neither RSV-positive nor HRV-positive patients administered corticosteroids varied from the ones receiving a placebo (mean ± SD [hours]: 57,2 ± 39,9 vs. 47,6 ± 38,7 for RSV-positive and 14,6 ± 32,5 vs. 19,5 ± 31,9 for HRV-positive, both P>.05) (38). However, in the RSV-negative group, oral prednisolone almost by one day shortened the mean length of hospital stay compared to the placebo group (mean ± SD [hours]: 19,7 ± 31,5 vs. 40,0 ± 31,3, P=.002). Furthermore, the mean hospitalization time significantly differed between RSV-positive and HRV-positive children in the intervention group (mean ± SD [hours]: 57,2 ± 39,9 vs. 19,7 ± 31,5, P=.002) (38).
In the second study, oral dexamethasone’s efficacy, regarded as the readiness rate for discharge at 48 hours, was higher in the RSV-negative group than in the RSV-positive group (OR 0.28, CI95% 0.09-0.92, P=.03) (32).
Four studies reported no difference in the hospital admission rate after the initial visit to ED between RSV-positive and RSV-negative children who were administered systemic corticosteroids (37, 39–41).
Chronic outcomes of corticosteroid treatment in severe bronchiolitis per viral etiology
The long-term follow-up – herein defined as two-month or more extended time – was evaluated only in three studies (33, 35, 38). The prevalence of respiratory symptoms during the two-year follow-up by Berger et al. (35) was not reported according to the RSV infection status. Solely Jartti et al. reassessed their participants two (38) and 12 months (33) after their studies’ enrollment. Although in their report, the number of wheezing episodes and initiation of regular controller medication for asthma symptoms within 12 months was not significantly reduced in the HRV-positive intervention group, in HRV(+) children less risk of physician-confirmed recurrence within 2 and 12 months was shown in the prednisolone group compared with placebo (both P<.05) (33). Moreover, they observed fewer new wheezing episodes during the 12-month follow-up in the corticosteroid-treated group compared with the placebo (P=.04) (33).
Discussion
Although this systematic review failed to provide evidence in favor of the use of systemic corticosteroids in children with severe bronchiolitis, it has identified a trend of the positive association between the use of systematic corticosteroids and duration of hospitalization in RSV-negative infants in hospitalized bronchiolitis (32, 38).
The scarcity of expected effect may be attributed: (i) to the considerable diversity in methodology among the analyzed studies, (ii) under-reporting the full panel of respiratory viruses in study subjects, (iii) baseline inflammatory endotype of the child rather than only the viral agent, and (iv) that most studies focused on RSV etiology. Only two studies from the same study center reported the details on HRV detection – the second most common cause of bronchiolitis in infants above six months old. These studies showed oral prednisolone as an effective modality in managing the first HRV-induced wheezing episode. This effectiveness was defined as clinical improvement (no escalation to non-invasive ventilation) and reduced relapses during the first months of follow-up (33, 38). Therefore, our analysis highlights the lack of predictive enrichment strategies in trials investigating corticosteroid treatment in bronchiolitis, which is in line with a recent meta-analysis by Elliott et al. (6).
On the other hand, the strengths of this study are in the identification of the existing evidence gaps, in the innovative view on the corticosteroid’s treatment in bronchiolitis, including focusing on both the first episode and its viral etiology, and efforts made to contact the authors to address the missing data. Also, there were attempts to synthesize the results quantitatively with subgroup analyses; however, the significant heterogeneity could not have been omitted.
We attempted to make the results of this systematic review as clinically relevant as possible. Hence, we dichotomized the data into RSV and non-RSV (another respiratory virus) data to accommodate the current clinical practice protocols that do not include mandatory testing for all respiratory viruses. Moreover, many confounding factors across the studies undermined the synthesis of the available data. The performed viral testing was obsolete, including viral isolation and serology tests (43). In some studies, most patients were RSV-positive (34, 43), or a noticeable proportion of participants did not undergo viral detection. A considerable loss to follow-up was found to be another confounder (35, 36, 41). Regarding the two Finnish studies, there was a delay in initiating the study’s drug administration due to the completion of HRV detection in the second study (33) compared to the first one (38) (45 vs. 0 h, respectively).
RSV remains the leading cause of severe bronchiolitis and, proportion-wise is the most prominent risk factor for future asthma development (42). The possible lack of action of systemic corticosteroids in RSV bronchiolitis may result from at least two reasons: firstly, several studies have shown that RSV can inhibit the immunosuppressive activity of corticosteroids via the glucocorticoid receptor (44). Secondly, dexamethasone was shown to have a favorable inhibitory impact on RSV-driven mucus production yet prevent immune responses that limit RSV infection in vitro and in vivo (45). On the other hand, one may expect a beneficial effect of systemic corticosteroid therapy in HRV-induced bronchiolitis due to the well-known Th2-skewing, a typical feature for atopic children infected with the HRV-C virus (46). Also, over the last decade, several cohort studies have associated an early life HRV infection with recurrent wheeze and asthma in the following years (11, 47–49).
Recent evolution in high-throughput sequencing technology offers an opportunity for personalized guidance in pharmacological management and assessing long-term respiratory sequelae in infants with bronchiolitis (11, 50, 51). A relatively small number of epidemiologic studies have investigated associations between biological (e.g., viral etiology, proteins), genetic and environmental factors in infants with bronchiolitis. Even fewer intervention studies in bronchiolitis incorporated a predictive enrichment approach using an interplay of such factors in their methodology.
In 2020-2021, we witnessed an unprecedented revolution in respiratory virus testing on a mass scale. A wide distribution of the mass PCR testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections has contributed to the increased use of the multiplex technique for other respiratory viruses (52). Therefore one cannot exclude the notion that in the coming years, studies evaluating a panel of respiratory viruses will provide more evidence around the role of HRV as a potential biomarker for the use of selected medications, including corticosteroids, during the first episode of bronchiolitis (53).
According to our recent meta-analysis on the association between infant bronchiolitis and recurrent wheeze, it has been shown that HRV-bronchiolitis children were more likely to develop recurrent wheeze (OR 4.11) and asthma (OR 2.72) than RSV-bronchiolitis group (P <0.01) (54). Furthermore, it has been proposed that the impact of rhinoviral infection may be species-specific. Of three species (A, B, and C), HRV-C-induced bronchiolitis has been linked to the highest risk for preschool wheeze and asthma in children (10). Thus, future studies evaluating the treatment efficacy according to virus subtypes are eagerly anticipated.
We are aware of several limitations of our review. The heterogeneity of the severity of assessed bronchiolitis episode introduced interventions, pre-specified outcomes, and follow-up time of analyzed studies makes our results less precise. Even though the search strategy was inclusive, within the initially identified studies recruiting only first wheezing bronchiolitis, viral tests were rarely performed and mainly focused on RSV etiology. Hence, the number of finally included studies was sparse.
Severe bronchiolitis remains a heterogeneous disease ideally suited for a precision medicine approach. This systematic review shows that there is currently insufficient data to recommend using systemic corticosteroids for short-term beneficial effects in treating the first episode of bronchiolitis. Nevertheless, an identified trend of the positive association between the use of systematic corticosteroids and shorter duration of hospitalization in RSV-negative infants hospitalized with the first episode of bronchiolitis should be further elucidated.
In conclusion, our study points out the need to identify groups of infants who would benefit from systemic corticosteroid treatment. A precise definition of the group of patients who benefit from a treatment is associated with decreased use of non-specific treatment. Therefore, this approach could ultimately result in decreased overall usage of systemic corticosteroids in bronchiolitis. Predictive enrichment approaches are guided by integration multi-omic data on HRV infection status (with its subtyping). Ongoing research in this area should focus on elucidating the complex interactions between pathogenetic factors in viral bronchiolitis with the aim to increase effectiveness and prevent the development of chronic outcomes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
DA, HM, WF, TJ, and AW contributed to the study design. DA and HM performed the systematic search, analyzed the data, and wrote the manuscript. WF, AW, NP, TJ reviewed the first draft of the manuscript, gave directions around the table and the figure design, and worked on the editing of manuscript to help reach the final version. All authors contributed to the article and approved the submitted version.
Funding
The Sigrid Juselius Foundation, Helsinki, Finland (D. Ambrożej and T. Jartti).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jartti T, Smits HH, Bønnelykke K, Bircan O, Elenius V, Konradsen JR, et al. Bronchiolitis needs a revisit: Distinguishing between virus entities and their treatments. Allergy. (2019) 74(1):40–52. doi: 10.1111/all.13624
2. Achten NB, van Rossum AMC, Bacharier LB, Fitzpatrick AM, Hartert TV. Long-term respiratory consequences of early-life respiratory viral infections: A pragmatic approach to fundamental questions. J Allergy Clin Immunol Pract (2021) 10:664–670. doi: 10.1016/j.jaip.2021.12.005
3. Cheung DS, Ehlenbach SJ, Kitchens RT, Riley DA, Thomas LL, Holtzman MJ, et al. Cutting edge: CD49d+ neutrophils induce FcepsilonRI expression on lung dendritic cells in a mouse model of postviral asthma. J Immunol (2010) 185(9):4983–7. doi: 10.4049/jimmunol.1002456
4. Cheung DS, Sigua JA, Simpson PM, Yan K, Hussain S-RA, Santoro JL, et al. Cysteinyl leukotriene receptor 1 expression identifies a subset of neutrophils during the antiviral response that contributes to postviral atopic airway disease. J Allergy Clin Immunol (2018) 142(4):1206–1217.e5. doi: 10.1016/j.jaci.2017.11.026
5. National Institute for Health and Care ExcellenceBronchiolitis: Diagnosis and management of bronchiolitis in children. In: NICE. (2015). (London: National Institute for Health and Care Excellence) 1–301
6. Elliott SA, Gaudet LA, Fernandes RM, Vandermeer B, Freedman SB, Johnson DW, et al. Comparative efficacy of bronchiolitis interventions in acute care: A network meta-analysis. Pediatrics (2021) 147(5). doi: 10.1542/peds.2020-040816
7. Castro-Rodriguez JA, Rodriguez-Martinez CE, Sossa-Briceño MP. Principal findings of systematic reviews for the management of acute bronchiolitis in children. Paediatr Respir Rev (2015) 16(4):267–75. doi: 10.1016/j.prrv.2014.11.004
8. O’Brien S, Borland ML, Cotterell E, Armstrong D, Babl F, Bauert P, et al. Australasian Bronchiolitis guideline. J Paediatr Child Health (2019) 55(1):42–53. doi: 10.1111/jpc.14104
9. Kirolos A, Manti S, Blacow R, Tse G, Wilson T, Lister M, et al. A systematic review of clinical practice guidelines for the diagnosis and management of bronchiolitis. J Infect Dis (2020) 222(Supplement_7):S672–9. doi: 10.1093/infdis/jiz240
10. Raita Y, Camargo CA, Bochkov YA, Celedón JC, Gern JE, Mansbach JM, et al. Integrated-omics endotyping of infants with rhinovirus bronchiolitis and risk of childhood asthma. J Allergy Clin Immunol (2021) 147(6):2108–17. doi: 10.1016/j.jaci.2020.11.002
11. Dumas O, Hasegawa K, Mansbach JM, Sullivan AF, Piedra PA, Camargo CA. Severe bronchiolitis profiles and risk of recurrent wheeze by age 3 years. J Allergy Clin Immunol (2019) 143(4):1371–9. doi: 10.1016/j.jaci.2018.08.043
12. Dumas O, Erkkola R, Bergroth E, Hasegawa K, Mansbach JM, Piedra PA, et al. Severe bronchiolitis profiles and risk of asthma development in Finnish children. Allergy Clin Immunol (2021) 149:1281–1285.e1. doi: 10.1016/j.jaci.2021.08.035
13. Kothalawala DM, Murray CS, Simpson A, Custovic A, Tapper WJ, Arshad SH, et al. Development of childhood asthma prediction models using machine learning approaches. Clin Transl Allergy (2021) 11(9):e12076. doi: 10.1002/clt2.12076
14. Mansbach JM, Piedra PA, Teach SJ, Sullivan AF, Forgey T, Clark S, et al. Prospective multicenter study of viral etiology and hospital length of stay in children with severe bronchiolitis. Arch Pediatr Adolesc Med (2012) 166(8):700–6. doi: 10.1001/archpediatrics.2011.1669
15. Papadopoulos NG, Moustaki M, Tsolia M, Bossios A, Astra E, Prezerakou A, et al. Association of rhinovirus infection with increased disease severity in acute bronchiolitis. Am J Respir Crit Care Med (2002) 165(9):1285–9. doi: 10.1164/rccm.200112-118BC
16. Ghazaly M, Nadel S. Characteristics of children admitted to intensive care with acute bronchiolitis. Eur J Pediatr (2018) 177(6):913–20. doi: 10.1007/s00431-018-3138-6
17. Hall CB, Weinberg GA, Blumkin AK, Edwards KM, Staat MA, Schultz AF, et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics. (2013) 132(2):e341–8. doi: 10.1542/peds.2013-0303
18. Hasegawa K, Tsugawa Y, Brown DFM, Mansbach JM, Camargo CA. Trends in bronchiolitis hospitalizations in the united states, 2000-2009. Pediatrics. (2013) 132(1):28–36. doi: 10.1542/peds.2012-3877
19. Foster SJ, Cooper MN, Oosterhof S, Borland ML. Oral prednisolone in preschool children with virus-associated wheeze: a prospective, randomised, double-blind, placebo-controlled trial. Lancet Respir Med (2018) 6(2):97–106. doi: 10.1016/S2213-2600(18)30008-0
20. Zahirul Hasan K, Abid Hossain Mollah M, Monir Hossain M, Zahangir Alam M, Shahidul Islam Bhuiyan A NM, Faruk Ahmed M, et al. Efficacy of prednisolone in recovery from acute bronchiolitis: Study in a tertiary care hospital, Dhaka, Bangladesh. Am J Pediatr (2021) 7(2):85. doi: 10.11648/j.ajp.20210702.19
21. Baig M, Anwaar O, Hussain M, Zahid S, Mehmood M, Saleem S. Efficacy of prednisolone in bronchiolitis with and without family history of atopy. J Pak Med Assoc (2019) 0):1. doi: 10.5455/JPMA.296296
22. Jackson DJ, Gern JE. Rhinovirus infections and their roles in asthma: Etiology and exacerbations. J Allergy Clin Immunol Pract (2022) 10: 673–681. doi: 10.1016/j.jaip.2022.01.006.
23. Leino A, Lukkarinen M, Turunen R, Vuorinen T, Söderlund-Venermo M, Vahlberg T, et al. Pulmonary function and bronchial reactivity 4 years after the first virus-induced wheezing. Allergy. (2019) 74(3):518–26. doi: 10.1111/all.13593
24. Makrinioti H, Camargo CA, Jartti T, Hasegawa K. Toward precision epidemiology in bronchiolitis. Chest. (2022): 162:744–746. doi: 10.1016/j.chest.2022.06.003
25. Wong HR. Intensive care medicine in 2050: precision medicine. Intensive Care Med (2017) 43(10):1507–9. doi: 10.1007/s00134-017-4727-y
26. Collins FS, Varmus H. A new initiative on precision medicine. N Engl J Med (2015) 372(9):793–5. doi: 10.1056/NEJMp1500523
27. Stanski NL, Wong HR. Prognostic and predictive enrichment in sepsis. Nat Rev Nephrol. (2020) 16(1):20–31. doi: 10.1038/s41581-019-0199-3
28. Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PloS Med (2009) 6(7):e1000097. doi: 10.1016/j.ijsu.2010.02.007
29. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
30. McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): An r package and shiny web app for visualizing risk-of-bias assessments. Res Synth Methods (2020) 12:55–61. doi: 10.1002/jrsm.1411
31. Roosevelt G, Sheehan K, Grupp-Phelan J, Tanz RR, Listernick R. Dexamethasone in bronchiolitis: a randomised controlled trial. Lancet (London England). (1996) 348(9023):292–5. doi: 10.1016/S0140-6736(96)02285-4
32. Alansari K, Sakran M, Davidson BL, Ibrahim K, Alrefai M, Zakaria I. Oral dexamethasone for bronchiolitis: A randomized trial. Pediatrics. (2013) 132(4):e810–6. doi: 10.1542/peds.2012-3746
33. Jartti T, Nieminen R, Vuorinen T, Lehtinen P, Vahlberg T, Gern J, et al. Short- and long-term efficacy of prednisolone for first acute rhinovirus-induced wheezing episode. J Allergy Clin Immunol (2015) 135(3):691–8.e9. doi: 10.1016/j.jaci.2014.07.001
34. Klassen TP, Sutcliffe T, Watters LK, Wells GA, Allen UD, Li MM. Dexamethasone in salbutamol-treated inpatients with acute bronchiolitis: A randomized, controlled trial. J Pediatr (1997) 130(2):191–6. doi: 10.1016/S0022-3476(97)70342-1
35. Berger I, Argaman Z, Schwartz SB, Segal E, Kiderman A, Branski D, et al. Efficacy of corticosteroids in acute bronchiolitis: Short-term and long-term follow-up. Pediatr Pulmonol. (1998) 26(3):162–6. doi: 10.1002/(SICI)1099-0496(199809)26:3<162::AID-PPUL2>3.0.CO;2-N
36. Goebel J, Estrada B, Quinonez J, Nagji N, Sanford D, Boerth RC. Prednisolone plus albuterol versus albuterol alone in mild to moderate bronchiolitis. Clin Pediatr (Phila). (2000) 39(4):213–20. doi: 10.1177/000992280003900404
37. Schuh S, Coates AL, Binnie R, Allin T, Goia C, Corey M, et al. Efficacy of oral dexamethasone in outpatients with acute bronchiolitis. J Pediatr (2002) 140(1):27–32. doi: 10.1067/mpd.2002.120271
38. Jartti T, Lehtinen P, Vanto T, Hartiala J, Vuorinen T, Makela MJ, et al. Evaluation of the efficacy of prednisolone in early wheezing induced by rhinovirus or respiratory syncytial virus. Pediatr Infect Dis J (2006) 25(6):482–8. doi: 10.1097/01.inf.0000215226.69696.0c
39. Corneli HM, Zorc JJ, Mahajan P, Majahan P, Shaw KN, Holubkov R, et al. A multicenter, randomized, controlled trial of dexamethasone for bronchiolitis. N Engl J Med (2007) 357(4):331–9. doi: 10.1056/NEJMoa071255
40. Plint AC, Johnson DW, Patel H, Wiebe N, Correll R, Brant R, et al. Epinephrine and dexamethasone in children with bronchiolitis. N Engl J Med (2009) 360(20):2079–89. doi: 10.1056/NEJMoa0900544
41. Mesquita M, Castro-Rodríguez JA, Heinichen L, Fariña E, Iramain R. Single oral dose of dexamethasone in outpatients with bronchiolitis: A placebo controlled trial. Allergol Immunopathol (Madr). (2009) 37(2):63–7. doi: 10.1016/S0301-0546(09)71106-1
42. Törmänen S, Lauhkonen E, Riikonen R, Koponen P, Huhtala H, Helminen M, et al. Risk factors for asthma after infant bronchiolitis. Allergy. (2018) 73(4):916–22. doi: 10.1111/all.13347
43. Connolly JH, Field CM, Glasgow JF, Slattery CM, MacLynn DM. A double blind trial of prednisolone in epidemic bronchiolitis due to respiratory syncytial virus. Acta Paediatr Scand (1969) 58(2):116–20. doi: 10.1111/j.1651-2227.1969.tb04693.x
44. Sedeyn K, Schepens B, Saelens X. Respiratory syncytial virus nonstructural proteins 1 and 2: Exceptional disrupters of innate immune responses. PloS Pathog (2019) 15(10):e1007984. doi: 10.1371/journal.ppat.1007984
45. McAllister CS, Ansaldi D, Growcott EJ, Zhong Y, Quackenbush D, Wolff KC, et al. Dexamethasone inhibits respiratory syncytial virus-driven mucus production while increasing viral replication without altering antiviral interferon signaling. Virology. (2020) 540:195–206. doi: 10.1016/j.virol.2019.10.007
46. Rajput C, Han M, Ishikawa T, Lei J, Goldsmith AM, Jazaeri S, et al. Rhinovirus c infection induces type 2 innate lymphoid cell expansion and eosinophilic airway inflammation. Front Immunol (2021) 12:1401. doi: 10.3389/fimmu.2021.649520
47. Midulla F, Nicolai A, Ferrara M, Gentile F, Pierangeli A, Bonci E, et al. Recurrent wheezing 36 months after bronchiolitis is associated with rhinovirus infections and blood eosinophilia. Acta Paediatr (2014) 103(10):1094–9. doi: 10.1111/apa.12720
48. Makrinioti H, Maggina P, Lakoumentas J, Xepapadaki P, Taka S, Megremis S, et al. Recurrent wheeze exacerbations following acute bronchiolitis–a machine learning approach. Front Allergy (2021) 2:76. doi: 10.3389/falgy.2021.728389
49. Lemanske RF, Jackson DJ, Gangnon RE, Evans MD, Li Z, Shult PA, et al. Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol (2005) 116(3):571–7. doi: 10.1016/j.jaci.2005.06.024
50. Fujiogi M, Dumas O, Hasegawa K, Jartti T, Camargo CA. Identifying and predicting severe bronchiolitis profiles at high risk for developing asthma: Analysis of three prospective cohorts. eClinicalMedicine. (2022) 43:101257. doi: 10.1016/j.eclinm.2021.101257
51. Fujiogi M, Zhu Z, Raita Y, Ooka T, Celedon JC, Freishtat R, et al. Nasopharyngeal lipidomic endotypes of infants with bronchiolitis and risk of childhood asthma: A multicentre prospective study. Thorax (2022) 77:1059–1069. doi: 10.1136/thorax-2022-219016
52. Maataoui N, Chemali L, Patrier J, Tran Dinh A, Le Fèvre L, Lortat-Jacob B, et al. Impact of rapid multiplex PCR on management of antibiotic therapy in COVID-19-positive patients hospitalized in intensive care unit. Eur J Clin Microbiol Infect Dis (2021) 40(10):2227–34. doi: 10.1007/s10096-021-04213-6
53. Rosenthal LA, Avila PC, Heymann PW, Martin RJ, Miller EK, Papadopoulos NG, et al. Viral respiratory tract infections and asthma: The course ahead. J Allergy Clin Immunol (2010) 125(6):1212–7. doi: 10.1016/j.jaci.2010.04.002
54. Makrinioti H, Hasegawa K, Lakoumentas J, Xepapadaki P, Tsolia M, Castro-Rodriguez JA, et al. The role of respiratory syncytial virus- and rhinovirus-induced bronchiolitis in recurrent wheeze and asthma–a systematic review and meta-analysis. Pediatr Allergy Immunol (2022) 00:1–12. doi: 10.1111/pai.13741
Keywords: precision medicine, infant, bronchiolitis, viruses, corticosteroids, asthma, rhinovirus
Citation: Ambrożej D, Makrinioti H, Whitehouse A, Papadopoulos N, Ruszczyński M, Adamiec A, Castro-Rodriguez JA, Alansari K, Jartti T and Feleszko W (2022) Respiratory virus type to guide predictive enrichment approaches in the management of the first episode of bronchiolitis: A systematic review. Front. Immunol. 13:1017325. doi: 10.3389/fimmu.2022.1017325
Received: 11 August 2022; Accepted: 17 October 2022;
Published: 27 October 2022.
Edited by:
Susetta Finotto, University Hospital Erlangen, GermanyCopyright © 2022 Ambrożej, Makrinioti, Whitehouse, Papadopoulos, Ruszczyński, Adamiec, Castro-Rodriguez, Alansari, Jartti and Feleszko. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wojciech Feleszko, d29qY2llY2guZmVsZXN6a29Ad3VtLmVkdS5wbA==