 Zoltán Vokó1,2*†
Zoltán Vokó1,2*† Zoltán Kiss3†
Zoltán Kiss3† György Surján4,5Orsolya Surján6Zsófia Barcza7István Wittmann3
György Surján4,5Orsolya Surján6Zsófia Barcza7István Wittmann3 Gergő Attila Molnár3Dávid Nagy1,2
Gergő Attila Molnár3Dávid Nagy1,2 Veronika Müller8Krisztina Bogos9
Veronika Müller8Krisztina Bogos9 Péter Nagy10,11,12
Péter Nagy10,11,12 István Kenessey10,13András Wéber10,14Lőrinc Polivka8Mihály Pálosi15
István Kenessey10,13András Wéber10,14Lőrinc Polivka8Mihály Pálosi15 János Szlávik16
János Szlávik16 György Rokszin3,17Cecília Müller18Zoltán Szekanecz19‡Miklós Kásler4‡
György Rokszin3,17Cecília Müller18Zoltán Szekanecz19‡Miklós Kásler4‡- 1Center for Health Technology Assessment, Semmelweis University, Budapest, Hungary
- 2Syreon Research Institute, Budapest, Hungary
- 3Second Department of Medicine and Nephrology-Diabetes Center, University of Pécs Medical School, Pécs, Hungary
- 4Ministry of Human Resources, Budapest, Hungary
- 5Institute of Digital Health Sciences, Semmelweis University, Budapest, Hungary
- 6Department of Deputy Chief Medical Officer II., National Public Health Center, Budapest, Hungary
- 7Syntesia Medical Communications Ltd., Budapest, Hungary
- 8Department of Pulmonology, Semmelweis University, Budapest, Hungary
- 9Department of Pulmonology, National Korányi Institute of Pulmonology, Budapest, Hungary
- 10Department of Molecular Immunology and Toxicology and the National Tumor Biology Laboratory, National Institute of Oncology, Budapest, Hungary
- 11Department of Anatomy and Histology, Laboratory of Redox Biology, University of Veterinary Medicine, Budapest, Hungary
- 12Institute of Oncochemistry, University of Debrecen, Debrecen, Hungary
- 13Department of Pathology, Forensic and Insurance Medicine, Semmelweis University, Budapest, Hungary
- 14Cancer Surveillance Branch, International Agency for Research on Cancer, Lyon, France
- 15National Health Insurance Fund, Budapest, Hungary
- 16Department of Infectology South-Pest Hospital Centre – National Institute for Infectology and Haematology, Budapest, Hungary
- 17RxTarget Ltd., Szolnok, Hungary
- 18Department of Chief Medical Officer, National Public Health Center, Budapest, Hungary
- 19Department of Rheumatology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
Background: In late 2021, the pandemic wave was dominated by the Delta SARS-CoV-2 variant in Hungary. Booster vaccines were offered for the vulnerable population starting from August 2021.
Methods: The nationwide HUN-VE 3 study examined the effectiveness and durability of primary immunization and single booster vaccinations in the prevention of SARS-CoV-2 infection, Covid-19 related hospitalization and mortality during the Delta wave, compared to an unvaccinated control population without prior SARS-CoV-2 infection.
Results: The study population included 8,087,988 individuals who were 18–100 years old at the beginning of the pandemic. During the Delta wave, after adjusting for age, sex, calendar day, and chronic diseases, vaccine effectiveness (VE) of primary vaccination against registered SARS-CoV-2 infection was between 11% to 77% and 18% to 79% 14–120 days after primary immunization in the 16–64 and 65–100 years age cohort respectively, while it decreased to close to zero in the younger age group and around 40% or somewhat less in the elderly after 6 months for almost all vaccine types. In the population aged 65–100 years, we found high, 88.1%–92.5% adjusted effectiveness against Covid-19 infection after the Pfizer-BioNTech, and 92.2%–95.6% after the Moderna booster dose, while Sinopharm and Janssen booster doses provided 26.5%–75.3% and 72.9%–100.0% adjusted VE, respectively. Adjusted VE against Covid-19 related hospitalization was high within 14–120 days for Pfizer-BioNTech: 76.6%, Moderna: 83.8%, Sputnik-V: 78.3%, AstraZeneca: 73.8%, while modest for Sinopharm: 45.7% and Janssen: 26.4%. The waning of protection against Covid-19 related hospitalization was modest and booster vaccination with mRNA vaccines or the Janssen vaccine increased adjusted VE up to almost 100%, while the Sinopharm booster dose proved to be less effective. VE against Covid-19 related death after primary immunization was high or moderate: for Pfizer-BioNTech: 81.5%, Moderna: 93.2%, Sputnik-V: 100.0%, AstraZeneca: 84.8%, Sinopharm: 58.6%, Janssen: 53.3%). VE against this outcome also showed a moderate decline over time, while booster vaccine types restored effectiveness up to almost 100%, except for the Sinopharm booster.
Conclusions: The HUN-VE 3 study demonstrated waning VE with all vaccine types for all examined outcomes during the Delta wave and confirmed the outstanding benefit of booster vaccination with the mRNA or Janssen vaccines, and this is the first study to provide clear and comparable effectiveness results for six different vaccine types after primary immunization against severe during the Delta pandemic wave.
Introduction
In Hungary, six different SARS-CoV-2 vaccines were approved in the first half of 2021, and five of them were investigated and showed high or very high short-term effectiveness against SARS-CoV-2 infection (Alpha variant) and Covid-19 related mortality in the nationwide HUN-VE 1 study (1). In the second half of 2021, a growing number of studies started reporting a waning effectiveness for vaccines over time, especially against the new, more infectious Delta variant and to less extent against Covid-19 related death (B.1.617.2) (2–6). To maintain protection against emerging new waves and variants, several European countries including Hungary started offering booster vaccine doses in summer 2021 (7, 8). The benefit of booster vaccination has been demonstrated by a number of recent studies (6–8). On August 1, 2021, the Hungarian government introduced the option of a booster dose with one of six vaccine types at least 4 months after primary immunization, particularly for the vulnerable population such as people aged 60 years or older and those having chronic illnesses (9).
The aim of our study was to estimate the effectiveness of six different vaccine types as well as their combinations as primary or booster vaccines against SARS-CoV-2 infection, Covid-19 related hospitalization and death during the Delta pandemic wave between September 2021 and December 2021 in Hungary. We also aimed to evaluate the durability of protection offered by vaccine combinations to provide guidance for countries where multiple vaccine types are available.
Methods
The study population included Hungarian residents aged 18 to 100 years who were registered in the Hungarian-COVID-19 Registry based on the National Public Health Center (NPHC) and National Health Insurance Fund Manager (NHIFM) database on March 4, 2020, when the first case of Covid-19 infection was detected in Hungary. Exclusion criteria included any inconsistencies in data such as a person receiving two different vaccine types for primary immunization, missing information on the type of the second vaccine dose, first vaccination administered before the first potential date of administration, fewer than 14 days between the first and second doses, a date of diagnosis before the first case was officially reported, or a date of death preceding the date of first vaccination. Fewer than 1,000 cases were excluded for reasons other than age outside the predefined range.
Cases of SARS-CoV-2 infection were reported on a daily basis using a centralized system via the National Public Health Center (NPHC). The report is based on (i) Covid-19-related symptoms identified by hospital physicians and general practitioners, (ii) positive nucleic acid amplification test reported by microbiological laboratories. Cases identified by symptoms were confirmed by PCR or antigen test included in the EC rapid test list (10). Covid-19 related hospitalization was defined as hospitalization with a positive PCR or antigen test within 5 days before or 20 days after admission to hospital. Covid-19 related mortality was defined as death during SARS-CoV-2 positivity, regardless of whether death was the direct consequence of Covid-19 infection or other underlying causes. Patients with confirmed SARS-CoV-2 infection who died without previously declared recovery and another clear cause of death were classified as Covid-19 related deaths. The definition was based on WHO recommendations and defined by the healthcare government (11).
Individuals were classified as primary vaccinated if at least 14 days had passed since the administration of the second dose of the BNT162b2 (Pfizer-BioNTech), HB02 (Sinopharm), Gam-COVID-Vac (Sputnik-V), AZD1222 (AstraZeneca), or mRNA-1273 (Moderna) vaccines, or the first dose of Ad26.COV2.S (Janssen). At any time point during the study period, the unvaccinated, control population included individuals who had not received any dose of any Covid-19 vaccine type beforehand.
Vaccine effectiveness (VE) was defined as 1 minus the incidence rate ratio of the outcome in question. Vaccine combinations administered to at least 3,000 people by December 31, 2021 or with at least 300 cases from the start of the pandemic until December 31, 2021 in Hungary were included in the analysis. Vaccine combinations were further broken down into subcategories according to the time elapsed since their administration. These subcategories were defined as 14–120, 121–180, 181–240, or more than 240 days. For booster vaccinations, only the 14–120 days category was established, because there were very few individuals during the Delta wave who had received their booster vaccination more than 120 days earlier.
All Hungarian residents aged 18–100 years who were registered in the NHIFM on March 4, 2020 were considered unvaccinated and uninfected persons apart from the first identified cases of Covid-19 infection. For each day afterwards until the end of the study period, we calculated the number of individuals at risk for different groups by age, sex, history of certain chronic diseases and vaccination, taking into account the types of vaccines and the time elapsed since their administration (intervention). Individuals who died were removed from the study base. The numbers of new registered infections, COVID-19 related hospitalizations, and deaths were registered for each day according to intervention, and individuals experiencing an outcome were removed from the study population of the respective analysis. Person-days for each intervention group were calculated by adding up the number of persons in each group for each day.
Age was categorized as 18–24, 25–34, 35–44, 45–54, 55–64, 65–74, 75–84, and 85–100 years. The presence of chronic diseases was identified based on in- and outpatient health service utilization and prescription data from the NHIFM between January 1, 2013 and March 3, 2021. The following chronic conditions were considered: cardiovascular diseases (myocardial infarction, angina, chronic heart failure, peripheral vascular disease, and stroke), diabetes mellitus (type 1 and type 2), immunosuppression (immunosuppressive therapy and transplantation), chronic pulmonary diseases (asthma and chronic obstructive pulmonary diseases), neoplasms, and chronic kidney diseases. The definitions of chronic diseases are presented in Supplementary Table 1.
Incidence rates (number of outcomes divided by person-time of observation) together with their exact 95% confidence intervals (CIs) were calculated for the period between September 13, 2021 and December 31, 2021 (Delta wave). Rate ratios with their exact confidence intervals were obtained considering unvaccinated as the reference category, using STATA (version 16.1).
Mixed effect negative binomial regression model was used to derive adjusted incidence rate ratios (IRRs) with 95% CIs for each outcome adjusted for age, sex, history of different chronic diseases, and calendar day (modelled as a random effect), which is better suited for over-dispersed count data than the traditional Poisson regression. The model is a random intercept model, which allows for different incidence rates in the reference category (i.e., unvaccinated) each day, but assumes fixed effect of the intervention categories. Separate models were fitted to estimate age group specific effects (i.e., 18–64 years and 65–100 years).
The study was approved by the Central Ethical Committee of Hungary (OGYÉI/10296-1/2022 and IV/1722- 1/2022/EKU).
Results
The study population included 8,087,988 individuals (18-64 years: n=6,193,552, 65-100 years: n=1,894,436) at the beginning of the pandemic.
In the age group of 16–64 years, the crude incidence rate of SARS-CoV-2 infection was 67.6 per 100,000 person-days in the unvaccinated cohort during the Delta wave. In the primary vaccination cohorts, crude incidence rates varied between 5.2 and 38.3 per 100,000 person-days after 14–120 days of the second vaccine dose (Supplementary Table 2). Crude incidence rates of infection progressively increased 120–180, 181–240 and >240 days after the second vaccine dose for each vaccine type, even exceeding crude incidence rates of the unvaccinated population 6 months after primary vaccination. On the other hand, after booster vaccination with the Pfizer-BioNTech, Moderna or Janssen vaccines, crude incidence rates fell below 20 per 100,000 person-days, regardless of the type of vaccines used for primary immunization except for the Sputnik-V, Sputnik-V, Janssen combination. On the other hand, booster vaccination with the Sinopharm vaccine resulted in crude incidence rates of 25.2–61.2 per 100,000 person-days, depending on the type of the primary vaccination (Supplementary Table 2).
Similar results were seen in the 65–100 years age cohort: lower crude incidence rates of SARS-CoV-2 infection 14–120 days after primary vaccination for each vaccine type compared to the unvaccinated cohort (54.8 per 100,000 person-days), increasing infection rates after 4 months, and very low rates (<10 per 100,000 person-days) after booster vaccination with mRNA vaccines, regardless of primary vaccine types (Supplementary Table 3).
Higher effectiveness and slightly less waning of protection were found against Covid-19 related hospitalization and death in both age groups. However, both hospitalization and mortality rates were close to respective rates in the unvaccinated cohort 240 days after the second vaccine dose for most vaccine types, while booster vaccination led to relevant decreases in the incidence rates of these outcomes (Supplementary Tables 4-7).
After adjusting for age, sex, chronic diseases, and calendar day, vaccine effectiveness of primary vaccination against SARS-CoV-2 infection varied between 10.9% and 76.9% 14–120 days after the second dose in the 16–64 years age cohort (Figure 1A), and between 17.8% and 79.1% in the 65–100 years age cohort (Figure 2A). Adjusted vaccine effectiveness decreased to close to zero in the younger age group and around 40% or somewhat less in the elderly after 6 months for almost all vaccine types. In the population aged 65–100 years, we found high, 88.1%–92.5% adjusted effectiveness against Covid-19 infection after the Pfizer-BioNTech booster dose, and 92.2%–95.6% adjusted effectiveness after the Moderna booster during the first 4 months after booster immunization. The Sinopharm and Janssen boosters provided 26.5%–75.3% and 72.9%–100.00% adjusted effectiveness, respectively, depending on primary immunization type (Figures 1A, 2A and Supplementary Table 3).
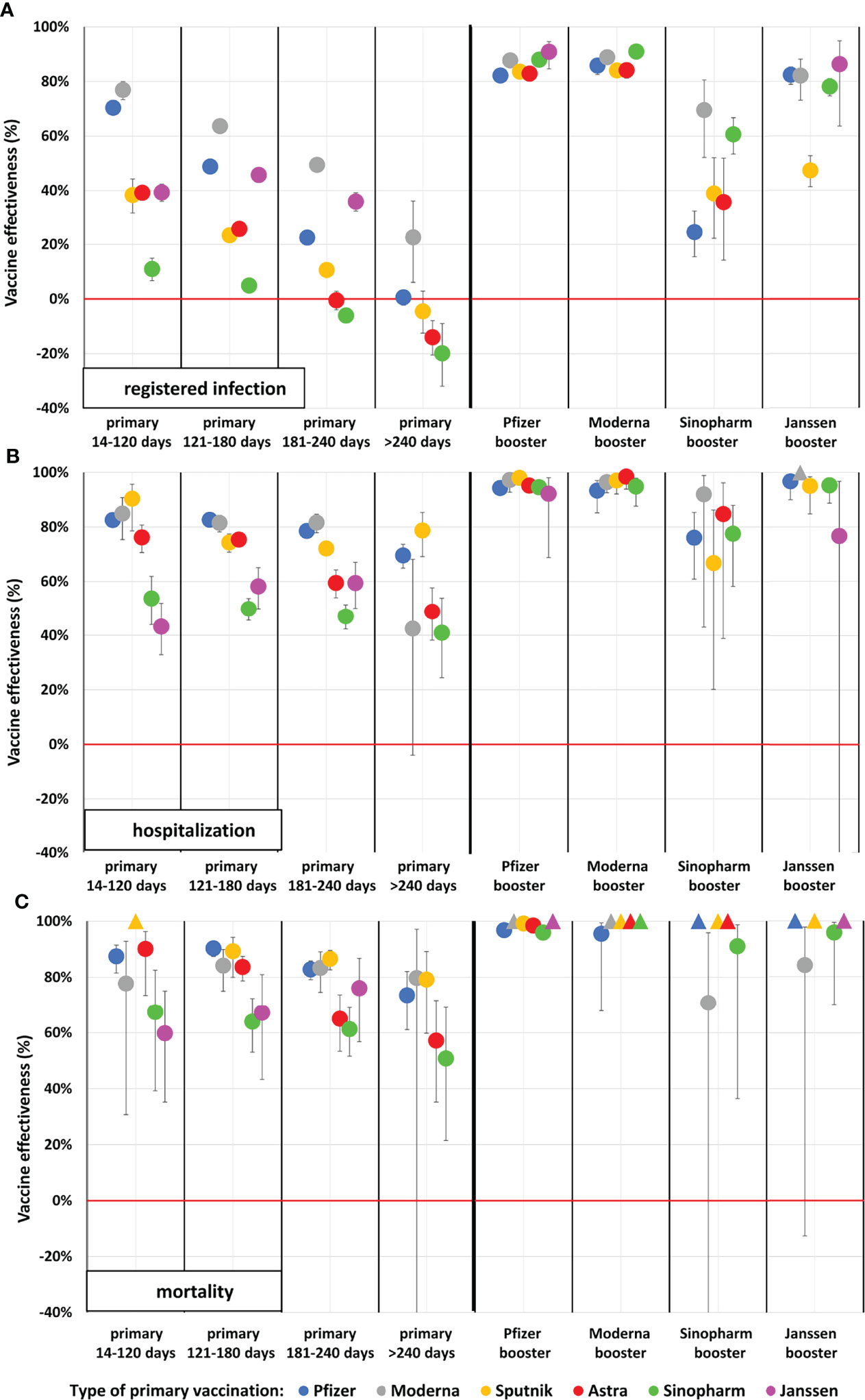
Figure 1 Adjusted vaccine effectiveness against registered SARS-CoV-2 infection, Covid-19 related hospitalization and death during the Delta wave in the Hungarian population aged 16–64 years. (Data points marked with triangles at value 100% indicate vaccine combination categories where no outcome occurred. In these categories, the person-time of observation is very limited). (A) Registered infection, (B) Hospitalization, (C) Mortality.
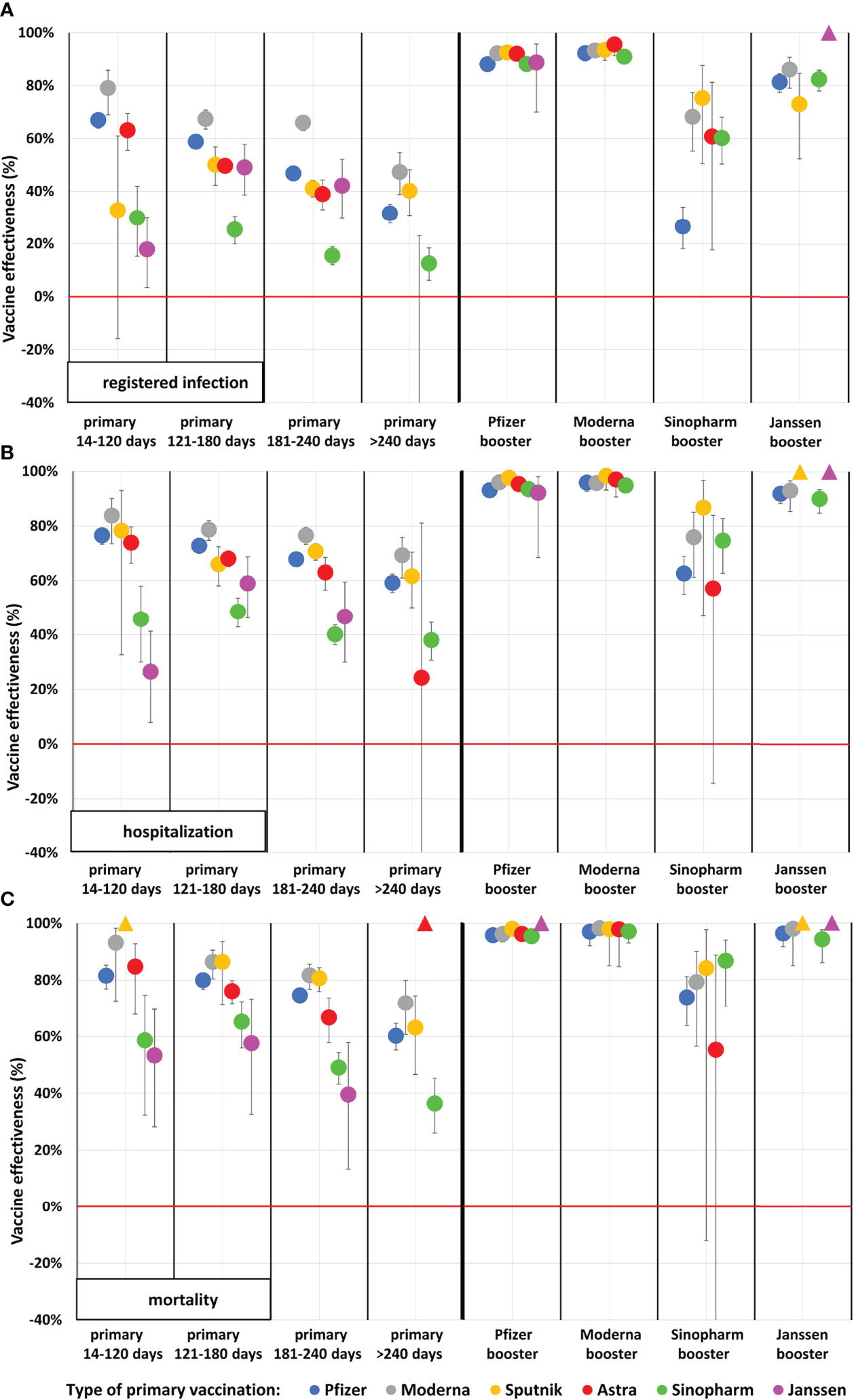
Figure 2 Adjusted vaccine effectiveness against registered SARS-CoV-2 infection, Covid-19 related hospitalization and death during the Delta wave in the Hungarian population aged 65–100 years. (Data points marked with triangles at value 100% indicate vaccine combination categories where no outcome occurred. In these categories, the person-time of observation is very limited). (A) Registered infection, (B) Hospitalization, (C) Mortality.
In the primary immunized population aged 65–100 years, adjusted vaccine effectiveness against Covid-19 related hospitalization was 76.6% with the Pfizer-BioNTech, 83.8% with the Moderna, 78.3% with the Sputnik-V, 73.8% with the AstraZeneca, 45.7% with the Sinopharm, and 26.4% with the Janssen vaccine within 14–120 days after the second dose (Figure 2B and Supplementary Table 5). The waning of protection against Covid-19 related hospitalization was much less pronounced than against SARS-CoV-2 infection. Nevertheless, after more than 240 days, primary Pfizer-BioNTech, Moderna, Sputnik-V, and Sinopharm vaccinations had lost around 20% of their effectiveness in relative terms against Covid-19 related hospitalization. Booster vaccination with mRNA vaccines or the Janssen vaccine increased adjusted effectiveness up to almost 100% (92.1% to 97.6% for Pfizer-BioNTech booster, 94.8% to 98.3% for Moderna booster and 90.00% to 100.00% for Janssen booster doses) irrespective of the vaccine type used for primary immunization, while the Sinopharm booster dose proved to be less effective in this regard (57.1% to 86.7%) (Figure 2B and Supplementary Table 5).
In individuals aged 65–100 years, vaccine effectiveness against Covid-19 related death after primary immunization was high or moderate (Pfizer-BioNTech: 81.5%, Moderna: 93.2%, Sputnik-V: 100.0%, AstraZeneca: 84.8%, Sinopharm: 58.6%, Janssen: 53.3%). Vaccine effectiveness decreased to 60.2% for the Pfizer-BioNTech, 71.9% for the Moderna, 63.0% for the Sputnik-V, and 36.4% for the Sinopharm vaccines by >240 days after the completion of primary immunization. All types of booster vaccines restored effectiveness up to almost 100% (95.8% to 100.00% for the Pfizer-BioNTech booster, 97.0% to 98.2% for the Moderna booster and 94.2% to 100.00% for the Janssen booster depending on prior vaccine types), except for the Sinopharm booster (55.3% after 2 doses of AstraZeneca to 86.8% after 2 doses of Sinopharm) (Figure 2C and Supplementary Table 7).
In the age group of 18–64 years, vaccine effectiveness against Covid-19 related death was somewhat higher than in the 65–100 years age group. Similarly to the older population, the Sinopharm and Janssen vaccines showed lower effectiveness compared to other vaccine types. The patterns of waning were very similar in the two age groups, with slightly less waning in terms of Covid-19 related hospitalization and mortality (Figure 1 and Supplementary Table 6).
Discussion
We found lower vaccine effectiveness against the Delta variant (B.1.617.2) within the first 4 months after primary immunization compared to effectiveness rates reported by the HUN-VE 1 study for spring 2021 against the Alpha variant (B.1.1.7) (1), although the results are not directly comparable. The lower effectiveness of globally available vaccine types against the Delta variant compared to Alpha has been widely reported (12–16). Our study is among the first to report effectiveness data for the Sinopharm, Sputnik-V, and Janssen vaccines against the Delta variant, showing a lower benefit for Janssen and Sinopharm compared to other vaccine types.
Most vaccine types provided sustained protection and high effectiveness against Covid-19 related death and hospitalization even after only two doses, which is in line with previous publications (17, 18). A recent prospective study from the United States reported similar, 85% effectiveness of mRNA vaccines against Covid-19 related hospitalization among patients infected with the Delta or Alpha SARS-CoV-2 variant after two doses (17). In a study conducted in the United Arab Emirates (UAE), the Sinopharm and Pfizer-BioNTech vaccines provided 95% and 98% effectiveness against Covid-19 related hospitalization in patients infected with the Delta variant, respectively (19). We found high protection against mortality of Pfizer-BioNTech, Moderna, Sputnik-V, and AstraZeneca vaccines but lower than 60% effectiveness for the Janssen and Sinopharm vaccines during the Delta wave in these age groups.
Waning effectiveness was observed for all outcomes, mostly for protection against SARS-CoV-2 infection, especially 6 months after primary immunization. The waning of vaccine effectiveness after primary immunization is widely discussed (20, 21), and in most cases it is attributed to the time-dependent decrease of neutralizing response against the SARS-CoV-2 virus. However, most studies have reported maintained and only slightly decreased protection against severe outcomes (4–6, 22).
There have been very few comparative studies on Sinopharm and other vaccines. The Pfizer vaccine was found to be superior to Sinopharm with respect to post-vaccination quantitative antibody titers (23). Similarly, the Sputnik V vaccine was also more immunogenic compared to Sinopharm (24). Regarding the Omicron variant, both Sinopharm and Janssen yielded significantly lower neutralizing activities compared to Pfizer and Moderna (25), and, this may explain that in our study, these vaccines showed a steeper decrease in efficacy over time.
Improved protection against all Covid-19 related outcomes with booster vaccines compared to primary immunization has been demonstrated by a number of studies (6–8). In a recently published preprint of HUN-VE 2 study from Hungary, booster vaccination provided 96% vaccine effectiveness against SARS-CoV-2 related death as an overall result in comparison to those, having only primary immunization during the Delta wave, where these VE was only 73% (26). Another study from Israel was among the first to report a 93% lower risk of Covid-19 related hospitalization and an 81% lower risk of Covid-19 related death among patients who had received three doses of the Pfizer-BioNTech vaccine compared to those who had received only two doses at least 5 months earlier (7). Later, another Israeli study confirmed the mid-term benefit of booster vaccination with the Pfizer-BioNTech vaccine in the older population (50 years or older), with an adjusted hazard ratio of 0.10 for Covid-19 related death after the third dose vs. primary immunization (8). In a phase 1/2 clinical trial, adults who had received the Pfizer-BioNTech, Janssen, or Moderna vaccine at least 12 weeks prior to enrolment had a 4.2 to 76-fold increase in neutralizing activity against a D614G pseudovirus, and a 4.6 to 56-fold increase in binding antibody titers with all vaccine combinations. Homologous booster doses resulted in a 4.2 to 20-fold increase in neutralizing antibody titers, while heterologous boosters increased titers 6.2 to 76-fold (9). The benefit of booster doses was later confirmed by the VISION Network providing vaccine effectiveness data against Covid-19-associated emergency department and urgent care encounters or hospitalizations during the Delta and Omicron waves (27). In a robust cohort study from the United Kingdom (U.K.), booster vaccination with mRNA vaccines provided 85% to 95% relative effectiveness against symptomatic Covid-19 infection and 97% to 99% absolute effectiveness against hospitalization in all age groups during the Delta wave, irrespective of the primary course, with no sign of waning for up to 10 weeks (28). In line with these observations, our study also demonstrated very high effectiveness against infection with the Delta variant for mRNA booster vaccines during the first 4 months irrespective of the type of the primary immunization, and very high, almost 100% effectiveness against Covid-19 related hospitalization and death. Our results harmonized and partially explained by a recently published Hungarian study, where administering a third dose of BNT162b2 (Pfizer-BioNTech) vaccine following two doses of Sinopharm vaccines provided a significantly enhance both humoral and T cell-mediated immune response, and its effectiveness was comparable to three doses of BNT162b2 vaccines (29).
On the other hand, our study showed less improvement in adjusted vaccine effectiveness after the Sinopharm booster against SARS-CoV-2 infection and Covid-19 related hospitalization and death both in younger and older age groups. Limited data are available on the benefit of the Sinopharm vaccine as a booster option. Two Chinese study demonstrated the safety and high immunogenicity of a third, homologous Sinopharm vaccination among healthy adults (30, 31). To our knowledge, this is the first on the effectiveness of the Sinopharm booster against SARS-CoV-2 infection and Covid-19 related hospitalization and death, particularly in comparison with mRNA vaccine boosters.
Although few people received Janssen booster vaccine, we were still able to examine its effectiveness. It proved to be highly effective against SARS-CoV-2 infection as well as against Covid-19 related hospitalization and death, with similar protection to mRNA boosters irrespective of the type of the primary vaccination. Because only few people received AstraZeneca or Sputnik-V boosters in our study, we were not able to assess the effectiveness of these combinations.
The strengths of our study include its nationwide nature inclusion of six different vaccines as primary or booster immunization, the robust number of more than 6 million vaccinated individuals, the 4 different time frames for the evaluation of waning effectiveness after primary vaccination, the 3 different outcomes, and the adjustment for the history of chronic diseases.
However, despite adjustments for age, sex, calendar day, and chronic diseases, further important covariates such as medications or socio-economic status were not included in the analysis. The latter could be related to differences in the likelihood of seeking SARS-CoV-2 testing, chance of detection, uptake of vaccines, prognosis of Covid-19, thus may also have resulted in residual confounding. Furthermore, the diagnosis of SARS-CoV-2 infection could also be established based on clinical symptoms, which might have resulted in differential misclassification, somewhat overestimating vaccine efficacy because physicians might have been less likely to diagnose Covid-19 in vaccinated individuals. On the other hand, misclassification might have biased the results in the other direction (i.e., underestimation of vaccine efficacy), as well, regarding the first infection as outcome, as the proportion of unregistered cases were likely to be higher among the unvaccinated population due to the higher incidence among them. Because of the issue of unregistered cases, we did not censor patients with registered infection in the analysis of the risk of hospitalization and death. As the proportion of individuals with natural immunity were likely to be higher in the unvaccinated population, our estimates can be considered conservative in respect of hospitalization and death. Importantly, vaccine effectiveness was demonstrated when the Delta SARS-CoV-2 variant (B.1.617.2) was the dominant strain in Hungary, therefore, the results do not represent the effectiveness of investigated vaccines against the Omicron variant (B.1.1.529) or against new, upcoming variants.
In conclusion, the nationwide HUN-VE 3 study provides a comprehensive overview of the durability and effectiveness of SARS-CoV-2 vaccines against infection, Covid-19 related hospitalization and mortality with six different vaccine types used for primary immunization and booster doses after primary immunization with various vaccine types. We found significantly waning vaccine effectiveness after primary immunization with each vaccine type, especially against SARS-CoV-2 infection and to a lesser degree against severe Covid-19 related outcomes. On the other hand, our study demonstrates the outstanding benefit of mRNA and Janssen booster vaccines against all Covid-19 related outcomes, irrespective of previously administered vaccine types.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by The study was approved by the Central Ethical Committee of Hungary (OGYÉI/10296-1/2022 and IV/1722- 1/2022/EKU). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
ZV: Conceptualization, Methodology, Formal analysis, Validation and Writing – Review & Editing. ZK and IW: Conceptualization, Methodology, Investigation, Visualization and Writing – Original Draft. LP Conceptualization, Methodology, Formal analysis, Validation, Data curation. GS, PN, IK, AW: Conceptualization, Methodology, Validation, Review & Editing. DN: Conceptualization, Methodology, Formal analysis. OS, VM, ZS, JS: Conceptualization, Review & Editing; MK, CM: Conceptualization, Methodology, Investigation and Supervision; ZB: Writing – Original Draft. GM: Validation, Project Administration. All authors contributed to the article and approved the submitted version.
Funding
The Center for Health Technology Assessment of the Semmelweis University participated in the project on a contractual basis made with the Ministry of Human Resources of Hungary and received funding. Zsófia Barcza of Syntesia Medical Communications Ltd. received payment for medical writing support from the National Public Health Center of Hungary.
Conflict of Interest
Author ZB was employed by company Syntesia Medical Communications Ltd. ZB of Syntesia Medical Communications Ltd. received payment for medical writing support from the National Public Health Center of Hungary. ZK is employed by MSD Pharma Hungary Ltd., too. However, this provides no relevant conflict of interest for the current research. At the time the study was performed, MK served as the minister of human resources. The ministry includes the secretariat for health.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Richárd Kiss for the initial data curation and dataset validation.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.919408/full#supplementary-material
Supplementary Table 1 | Description of different comorbidities in HUN-VE 3 study
Supplementary Table 2 | Incidence rates, crude and adjusted effectiveness rates of vaccine combinations against registered SARS-CoV-2 infection during the Delta wave in the 18–64-year-old Hungarian population.
Supplementary Table 3 | Incidence rates, crude and adjusted effectiveness rates of vaccine combinations against registered SARS-CoV-2 infection during the Delta wave in the 65–100-year-old Hungarian population.
Supplementary Table 4 | Incidence rates, crude and adjusted effectiveness rates of vaccine combinations against Covid-19 related hospitalization during the Delta wave in the 18–64-year-old Hungarian population.
Supplementary Table 5 | Incidence rates, crude and adjusted effectiveness rates of vaccine combinations against Covid-19 related hospitalization during the Delta wave in the 65–100-year-old Hungarian population.
Supplementary Table 6 | Incidence rates, crude and adjusted effectiveness rates of vaccine combinations against Covid-19 related mortality during the Delta wave in the 18–64-year-old Hungarian population.
Supplementary Table 7 | Incidence rates, crude and adjusted effectiveness rates of vaccine combinations against Covid-19 related mortality during the Delta wave in the 65–100-year-old Hungarian population.
References
1. Vokó Z, Kiss Z, Surján G, Surján O, Barcza Z, Pályi B, et al. Nationwide Effectiveness of Five SARS-CoV-2 Vaccines in Hungary-The HUN-VE Study. Clin Microbiol Infect (2022) 28(3):398–404. doi: 10.1016/j.cmi.2021.11.011
2. Tartof SY, Slezak JM, Fischer H, Hong V, Ackerson BK, Ranasinghe ON, et al. Effectiveness of mRNA BNT162b2 COVID-19 Vaccine Up to 6 Months in a Large Integrated Health System in the USA: A Retrospective Cohort Study. Lancet (2021) 398(10309):1407–16 doi: 10.1016/S0140-6736(21)02183-8.
3. Chemaitelly H, Tang P, Hasan MR, AlMukdad S, Yassine HM, Benslimane FM, et al. Waning of BNT162b2 Vaccine Protection Against SARS-CoV-2 Infection in Qatar. New Engl J Med (2021) 385(24):e83 doi: 10.1056/NEJMoa2114114.
4. Goldberg Y, Mandel M, Bar-On YM, Bodenheimer O, Freedman L, Haas EJ, et al. Waning Immunity After the BNT162b2 Vaccine in Israel. New Engl J Med (2021) 385(24):e85 doi: 10.1056/NEJMoa2114228.
5. Cohn BA, Cirillo PM, Murphy CC, Krigbaum NY, Wallace AW. SARS-CoV-2 Vaccine Protection and Deaths Among US Veterans During 2021. Science (2022) 375(6578):331–6 doi: 10.1126/science.abm0620.
6. Hansen CH, Schelde AB, Moustsen-Helm IR, Emborg HD, Krause TG, Mølbak K, et al. Vaccine Effectiveness Against SARS-CoV-2 Infection With the Omicron or Delta Variants Following a Two-Dose or Booster BNT162b2 or mRNA-1273 Vaccination Series: A Danish Cohort Study. medRxiv (2021), 12.20.21267966. doi: 10.1101/2021.12.20.21267966
7. Barda N, Dagan N, Cohen C, Hernán MA, Lipsitch M, Kohane IS, et al. Effectiveness of a Third Dose of the BNT162b2 mRNA COVID-19 Vaccine for Preventing Severe Outcomes in Israel: An Observational Study. Lancet (2021) 398(10316):2093–100 doi: 10.1016/S0140-6736(21)02249-2.
8. Arbel R, Hammerman A, Sergienko R, Friger M, Peretz A, Netzer D, et al. BNT162b2 Vaccine Booster and Mortality Due to Covid-19. New Engl J Med (2021) 385(26):2413–20 doi: 10.1056/NEJMoa2115624.
9. Koronavirus.gov.hu site – official site of Hungarian Government. . Available at: https://koronavirus.gov.hu/cikkek/magyarorszag-az-elso-ahol-mar-harmadik-oltasra-lehet-idopontot-foglalni.
10. European Commission Directorate-General For Health And Food Safety. EU Health Preparedness: A Common List of COVID-19 Rapid Antigen Tests and a Common Standardised Set of Data to be Included in COVID-19 Test Result Certificates . Available at: https://ec.europa.eu/health/sites/default/files/preparedness_response/docs/covid-19_rat_common-list_en.pdf (Accessed 3 October 2021).
11. World Health Organization. International Guidelines for Certification and Classification (Coding) of COVID-19 as Cause of Death (2020). Available at: www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf (Accessed 19 August 2021).
12. Puranik A, Lenehan PJ, Silvert E, Niesen M, Corchado-Garcia J, O'Horo JC, et al. Comparison of Two Highly-Effective mRNA Vaccines for COVID-19 During Periods of Alpha and Delta Variant Prevalence. MedRxiv Preprint Server Health Sci (2021) 2021.08.06.21261707. doi: 10.1101/2021.08.06.21261707
13. Hayawi K, Shahriar S, Serhani MA, Alashwal H, Masud MM. Vaccine Versus Variants (3vs): Are the COVID-19 Vaccines Effective Against the Variants? A Systematic Review. Vaccines (2021) 9(11):1305. doi: 10.3390/vaccines9111305
14. Kislaya I, Rodrigues EF, Borges V, Gomes JP, Sousa C, Almeida JP, et al. Comparative Effectiveness of Coronavirus Vaccine in Preventing Breakthrough Infections Among Vaccinated Persons Infected With Delta and Alpha Variants. Emerg Infect Dis (2022) 28(2):331–7. doi: 10.3201/eid2802.211789
15. Lopez Bernal J, Andrews N, Gower C, Gallagher E, Simmons R, Thelwall S, et al. Effectiveness of Covid-19 Vaccines Against the B.1.617.2 (Delta) Variant. New Engl J Med (2021) 385(7):585–94. doi: 10.1056/NEJMoa2108891
16. Sheikh A, McMenamin J, Taylor B, Robertson C, Public Health Scotland and the EAVE II Collaborators. SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet (2021) 397(10293):2461–2. doi: 10.1016/S0140-6736(21)01358-1
17. Lauring AS, Tenforde MW, Chappell JD, Gaglani M, Ginde AA, McNeal T, et al. Clinical Severity of, and Effectiveness of mRNA Vaccines Against, Covid-19 From Omicron, Delta, and Alpha SARS-CoV-2 Variants in the United States: Prospective Observational Study. BMJ (Clin Res ed) (2022) 376:e069761. doi: 10.1136/bmj-2021-069761
18. Fiolet T, Kherabi Y, MacDonald CJ, Ghosn J, Peiffer-Smadja N. Comparing COVID-19 Vaccines for Their Characteristics, Efficacy and Effectiveness Against SARS-CoV-2 and Variants of Concern: A Narrative Review. Clin Microbiol Infect (2022) 28(2):202–21. doi: 10.1016/j.cmi.2021.10.005
19. Mousa M, Albreiki M, Alshehhi F, AlShamsi S, Marzouqi NA, Alawadi T, et al. Similar Effectiveness of the Inactivated Vaccine BBIBP-CorV (Sinopharm) and the mRNA Vaccine BNT162b2 (Pfizer-BioNTech) Against COVID-19 Related Hospitalizations During the Delta Outbreak in the United Arab Emirates. J Travel Med (2022), taac036. doi: 10.1093/jtm/taac036
20. Levine-Tiefenbrun M, Yelin I, Alapi H, Katz R, Herzel E, Kuint J, et al. Viral Loads of Delta-Variant SARS-CoV-2 Breakthrough Infections After Vaccination and Booster With BNT162b2. Nat Med (2021) 27(12):2108–10. doi: 10.1038/s41591-021-01575-4
21. Pouwels KB, Pritchard E, Matthews PC, Stoesser N, Eyre DW, Vihta KD, et al. Effect of Delta Variant on Viral Burden and Vaccine Effectiveness Against New SARS-CoV-2 Infections in the UK. Nat Med (2021) 27(12):2127–35. doi: 10.1038/s41591-021-01548-7
22. Tang P, Hasan MR, Chemaitelly H, Yassine HM, Benslimane FM, Al Khatib HA, et al. BNT162b2 and mRNA-1273 COVID-19 Vaccine Effectiveness Against the SARS-CoV-2 Delta Variant in Qatar. Nat Med (2021) 27(12):2136–43. doi: 10.1038/s41591-021-01583-4
23. Alqassieh R, Suleiman A, Abu-Halaweh S, Santarisi A, Shatnawi O, Shdaifat L, et al. Pfizer-BioNTech and Sinopharm: A Comparative Study on Post-Vaccination Antibody Titers. Vaccines (2021) 9(11):1223. doi: 10.3390/vaccines9111223
24. Stoma I, Korsak K, Voropaev E, Osipkina O, Kovalev A. Comparative Study of Immunogenicity and Safety of Gam-COVID-Vac and Sinopharm BBIBP-CorV Vaccines in Belarus. medRxiv (2022), 02.05.22270499. doi: 10.1101/2022.02.05.22270499
25. Cameroni E, Saliba C, Bowen JE, Rosen LE, Culap K, Pinto D, et al. Broadly Neutralizing Antibodies Overcome SARS-CoV-2 Omicron Antigenic Shift. bioRxiv (2021), 12.12.472269. doi: 10.1101/2021.12.12.472269
26. Kiss Z, Wittmann I, Polivka L, Surján GY, Surján O, Barcza ZS, et al. Nationwide Effectiveness of First and Second SARS-CoV2 Booster Vaccines During the Delta and Omicron Pandemic Waves in Hungary (HUN-VE 2 Study). Front Immunol (2022) 13:905585. doi: 10.3389/fimmu.2022.905585
27. Ferdinands JM, Rao S, Dixon BE, Mitchell PK, DeSilva MB, Irving SA, et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance — VISION Network, 10 States, August 2021–January 2022. MMWR Morb Mortal Wkly Rep (2022) 71:255–63. doi: 10.15585/mmwr.mm7107e2externalicon
28. Andrews N, Stowe J, Kirsebom F, Toffa S, Sachdeva R, Gower C, et al. Effectiveness of COVID-19 Booster Vaccines Against COVID-19-Related Symptoms, Hospitalization and Death in England. Nat Med (2022) 28(4): 831–837 doi: 10.1038/s41591-022-01699-1
29. Matula Z, Gönczi M, Bekő G, Kádár B, Ajzner É., Uher F, et al. Antibody and T Cell Responses Against SARS-CoV-2 Elicited by the Third Dose of BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) Vaccines Using a Homologous or Heterologous Booster Vaccination Strategy. Vaccines (2022) 10:539. doi: 10.3390/vaccines10040539
30. Ai J, Zhang Y, Zhang H, Zhang Q, Fu Z, Lin K, et al. Safety and Immunogenicity of a Third-Dose Homologous BBIBP-CorV Boosting Vaccination: Interim Results From a Prospective Open-Label Study. Emerg Microbes Infect (2022) 11(1):639–47. doi: 10.1080/22221751.2022.2025746
Keywords: booster vaccine, delta variant, vaccine effectiveness, sinopharm, sputnik-V, janssen, Covid-19
Citation: Vokó Z, Kiss Z, Surján G, Surján O, Barcza Z, Wittmann I, Molnár GA, Nagy D, Müller V, Bogos K, Nagy P, Kenessey I, Wéber A, Polivka L, Pálosi M, Szlávik J, Rokszin G, Müller C, Szekanecz Z and Kásler M (2022) Effectiveness and Waning of Protection With Different SARS-CoV-2 Primary and Booster Vaccines During the Delta Pandemic Wave in 2021 in Hungary (HUN-VE 3 Study). Front. Immunol. 13:919408. doi: 10.3389/fimmu.2022.919408
Received: 13 April 2022; Accepted: 15 June 2022;
Published: 22 July 2022.
Edited by:
Rong Hai, University of California, Riverside, United StatesReviewed by:
Linfeng Gao, University of California, Irvine, United StatesVijay Tripathi, Sam Higginbottom University of Agriculture, Technology and Sciences, India
Copyright © 2022 Vokó, Kiss, Surján, Surján, Barcza, Wittmann, Molnár, Nagy, Müller, Bogos, Nagy, Kenessey, Wéber, Polivka, Pálosi, Szlávik, Rokszin, Müller, Szekanecz and Kásler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoltán Vokó, dm9rby56b2x0YW5Ac2VtbWVsd2Vpcy11bml2Lmh1
†These authors have contributed equally to this work
‡These authors share last authorship