 Zhiliang Jia1
Zhiliang Jia1 Dristhi Ragoonanan1
Dristhi Ragoonanan1 Kris Michael Mahadeo1
Kris Michael Mahadeo1 Jonathan Gill1
Jonathan Gill1 Richard Gorlick1
Richard Gorlick1 Elizabeth Shpal2
Elizabeth Shpal2 Shulin Li1*
Shulin Li1*- 1Department of Pediatric Research, University of Texas MD Anderson Cancer Center, Houston, TX, United States
- 2Department of Stem Cell Transplantation and Cellular Therapy, University of Texas MD Anderson Cancer Center, Houston, TX, United States
Interleukin 12 (IL-12) is a naturally occurring cytokine that plays a key role in inducing antitumor immune responses, including induction of antitumor immune memory. Currently, no IL-12-based therapeutic products have been approved for clinical application because of its toxicities. On the basis of this review of clinical trials using primarily wild-type IL-12 and different delivery methods, we conclude that the safe utilization of IL-12 is highly dependent on the tumor-specific localization of IL-12 post administration. In this regard, we have developed a cell membrane-anchored and tumor-targeted IL-12-T (attIL12-T) cell product for avoiding toxicity from both IL-12 and T cells-induced cytokine release syndrome in peripheral tissues. A phase I trial using this product which seeks to avoid systemic toxicity and boost antitumor efficacy is on the horizon. Of note, this product also boosts the impact of CAR-T or TCR-T cell efficacy against solid tumors, providing an alternative approach to utilize CAR-T to overcome tumor resistance.
IL-12 biology
Human interleukin 12 (IL-12) is a proinflammatory cytokine that is produced by dendritic cells (DCs) and activated phagocytes. It is a disulfide-bonded heterodimeric cytokine. Human IL-12 gene was cloned from an Epstein–Barr virus–transformed cell line. IL-12 activates natural killer (NK) cells, induces interferon gamma (IFNγ) production, and is pivotal to the process of regulating the transition from innate to adaptive immunity (1, 2). In addition to NK cells, IL-12 acts directly on other types of lymphocytes, including natural killer T cells and CD8+ T cells, to promote proliferation and enhance their cytotoxicity (3). Because it activates these lymphocytes, IL-12 is considered a potent anticancer agent that enhances differentiation of T-helper 1 (Th1) and promotes T cell-mediated cytolysis of cancer cells (4) (5). IL-12 can also directly stimulate DCs to produce additional IL-12 and promote antigen presentation (6). Clinical trials that delivered wild-type recombinant human IL-12 (rhIL-12) or the human IL-12 gene to cancer patients began toward the end of the last century (7, 8). IL-12 has also been used to treat HIV and hepatitis virus infections (9–11). Our goal in this review is to analyze and compare the toxicity and safety results of clinical trials of IL-12 delivered via different routes and various forms (i.e., protein, gene, cells) to identify a safe way for IL-12 to be used clinically. A secondary goal is to discuss tumor-targeted delivery of IL-12, as accumulating evidence shows that tumor-targeted delivery of IL-12 is critical to triggering the antigen spreading associated with long-term tumor eradication.
Toxicity of human IL-12 therapy
IL-12-armed T cell therapy was found to stimulate a significant antitumor response that induced regression of tumors established in preclinical mouse models (12, 13). However, the early clinical trials that used systemic administration of rhIL-12 were disappointing because of observed toxicities produced by high production of proinflammatory cytokine (7, 8, 14, 15). The most common adverse events reported in these clinical trials were fever and flu-like symptoms. Other common toxicities included fatigue, nausea, vomiting, diarrhea, and headache. Hepatic toxicities were also frequently observed, including elevated alanine transaminase (ALT) and aspartate transaminase (AST). The most frequently experienced hematologic adverse events were leukopenia, anemia, neutropenia, and thrombocytopenia (16).
The most commonly reported hematologic toxicities of recombinant IL-12 (rIL-12) protein therapy are neutropenia and thrombocytopenia (17). In multiple trials, rhIL-12 treatment significantly affected leukocytes (7). In one trial, after the initial administration of rhIL-12, it was observed that in all the major lymphocyte subsets patients developed transient and profound lymphopenia (18). In other trials, it was observed that the absolute peripheral blood lymphocyte counts fell dramatically within 4 hours after administration of rhIL-12; these low levels persisted for the first 24 hours after treatment, though a gradual increase was observed thereafter, with levels returning to normal at 168 hours (19, 20). Unlike a single or initial rhIL-12 treatment, subsequent rhIL-12 administrations were followed by significant increases in patients’ peripheral blood lymphocyte counts (21). A dose-dependent increase of T cells, B cells, and NK cells was also observed in vivo in lymphoma and myeloma patients receiving rhIL-12 therapy after peripheral blood autologous stem cell transplantation (22).
These toxicities are at least partially caused by the induction of toxic cytokines. One study showed that in 21 cancer patients, administration of rhIL-12 once a week increased the expression of IFNγ, even at very low doses (15). In addition to IFNγ, increased expression of several other cytokines, including tumor necrosis factor alpha (TNFα) and IP-10, has been noted (14, 15). In a phase I trial that was to determine both the optimal biological dose and safety of IL-12 given together with trastuzumab, patients with metastatic human epidermal growth factor receptor 2 (HER2)-positive nonhematological malignancies were administered trastuzumab on day 1 of each weekly cycle. At the beginning of week 3, rhIL-12 protein was injected intravenously on days 2 and 5. Elevated serum levels of macrophage inflammatory protein-1α, TNFα, IP-10, and monokines induced by IFNγ were observed in the patients who had a clinical response or stabilized disease (23). In another trial in patients with HER2-positive malignancies, it was found that activation of extracellular signal-regulated kinase in peripheral blood mononuclear cells and levels of IFNγ and several other chemokines (MIP-1α, IL-8, RANTES, IP-10, and MIG) increased in patients who experienced a clinical benefit including complete response, partial response, or stable disease. But these increases were not observed in patients with progressive disease (21).
In the trial referenced above of rhIL-12 in 21 cancer patients, besides IFNγ, TNFα, and IP-10, several other cytokines, including monokine induced by interferon-gamma (MIG), IL-10, and IL-4, were found to be increased in peripheral blood mononuclear cells even when IL-12 was given at very low doses (30 ng/kg) (15). In the trial of rhIL-12 in patients with ovarian cancer or peritoneal cancer, 3-fold or greater increases of IFNγ, TNFα, IL-10, IL-8, and vascular endothelial growth factor (VEGF) in the peritoneal fluid were observed post-rhIL-12 administration. IP-10 levels were increased in 5 of 5 patients (14). On the basis of cytokine response profile examinations, it was suggested that either NK or T cells could mediate IL-12’s effects (14). Experimental results showed that IL-12 induced a greater than 2-fold increase of IFNγ in 16 patients and of the mRNA expression of TNFα in peripheral whole blood in 13 of 21 patients (15). Though the presence of cytokines is beneficial to the antitumor response, a decrease in IFNγ concentration was associated with the nonexistence of toxicity from IL-12 (15, 24). These results suggested that IL-12-mediated cytokine release contributed substantially to its toxicity in clinical trials; among the induced cytokines, IFNγ, IP-10, and TNFα were the major players (25–28).
Route dependence in IL-12 therapy-associated toxicity
Despite its toxicities, trials have demonstrated benefits of IL-12-based therapies depending on the route of delivery. In a clinical trial that included 42 patients, 32 with non-Hodgkin lymphoma and 10 with Hodgkin lymphoma, rhIL-12 was administered intravenously (n = 11) or subcutaneously (n = 31) (29). Most toxicities were grade 1 or 2, but grade 3 hepatic toxicity (reversible) was also reported in 3 patients, who required dose reduction. It was also reported that the response rates altered according to IL-12 administration route. Among patients who received intravenous IL-12, 40% had a partial or complete response, while only 7% of patients who received subcutaneous IL-12 had a partial or complete response. These results clearly demonstrated that at doses with similar toxicity profiles, intravenous delivery of IL-12 produced a better response rate than subcutaneous delivery.
To avoid cytokine toxicity following systemic (i.e., intravenous, subcutaneous) delivery of the IL-12 protein, intratumoral delivery of the IL-12 gene has been investigated. In a trial whose results were published in 2007, DNA encoding an IL-12 plasmid was injected into metastatic lesions between 0.5 and 2.5 cm in diameter) cutaneous or subcutaneously (30). The tumors were treated with either 3 or 6 intratumoral injections. Significant decrease in the treated lesion’s size was observed in 5 of the 12 patients. The lack of toxicity from this intratumoral treatment was associated with a lack of detection of IL-12 in serum. No greater than grade 1 local toxicity was observed from any patient in this trial, and only 2 patients were reported to have grade 1 local toxic effects. In other studies, intratumoral delivery of IL-12 with viral vectors, plasmid vectors, DCs, and CAR-Ts all showed no toxicities or only mild ones (31–36).
Intramuscular or intratumoral electroporation delivery of IL-12 has been reported in several clinical trials. There was a phase I trial reported in 2008, 24 patients that had metastatic melanoma received intratumoral IL-12 plasmid via electroporation on days 1, day 5, and day 8 during a single 39-day cycle. Minimal systemic toxicity was observed. Posttreatment examination showed notable tumor necrosis and lymphocytic infiltrate. Thus, intratumoral IL-12 DNA administration via electroporation is not only safe but also efficacious against melanoma (37). While IL-12 DNA was combined with other reagent and delivered intramuscular, no significant difference of adverse events was observed with or without IL-12 (26). The toxicity and efficacy findings of clinical trials using IL-12 wild-type protein, gene, and armed cells are summarized in Tables 1–3, respectively.
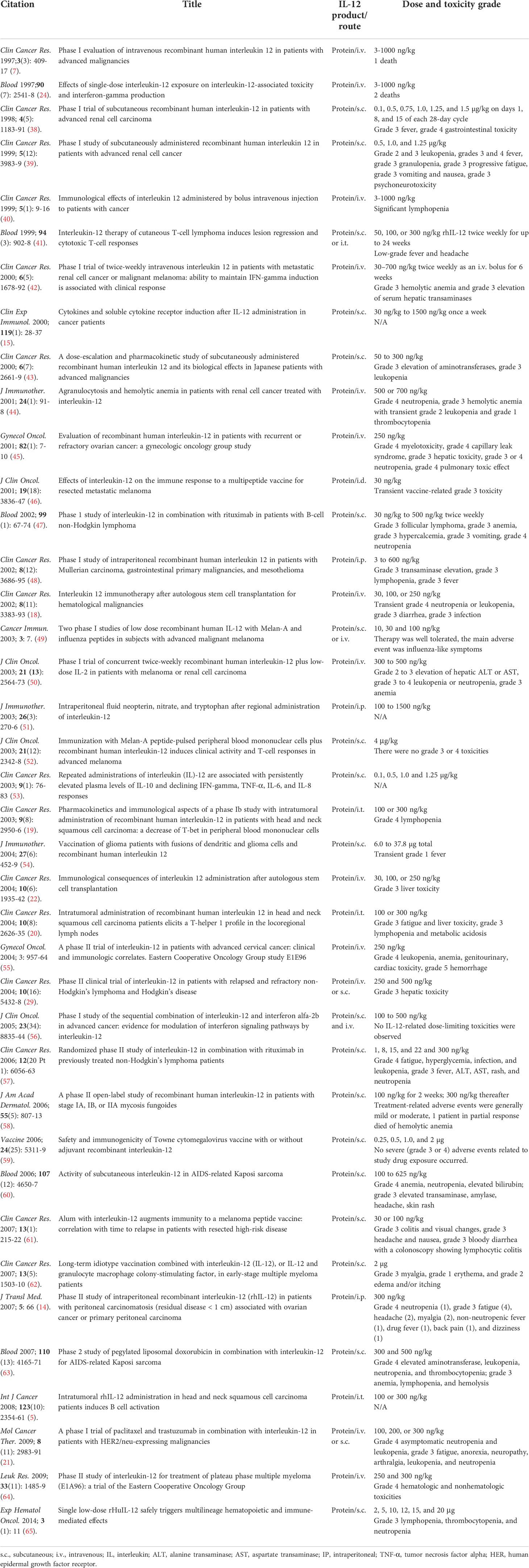
Table 1 Summary of human clinical trials of wild-type IL-12 protein therapy.
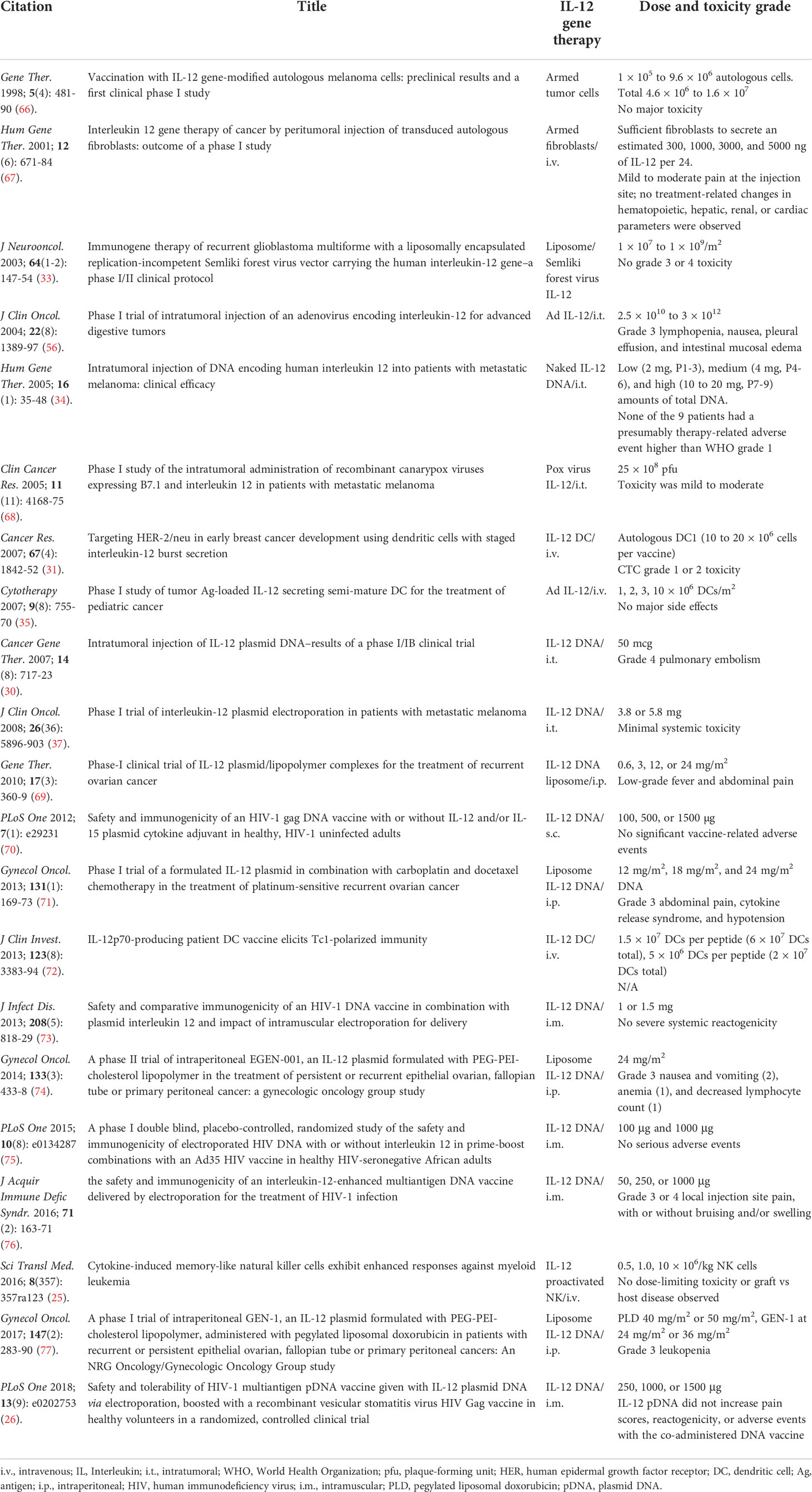
Table 2 Summary of human clinical trials of IL-12 gene therapy.

Table 3 Summary of clinical trials of targeted IL-12 therapy.
Tumor-targeted IL-12–armed antibodies in clinical trials
IL-12 can be covalently linked with monoclonal antibodies to create IL-12-armed antibodies. This design combines the high specificity against target antigen of monoclonal antibodies with the antitumor effects of IL-12, resulting in “armed” monoclonal antibodies that deliver IL-12 to tumor cells that have enriched levels of the target antigen. Such IL-12 delivery targeting a specific antigen minimizes IL-12 exposure in normal tissues and results in less toxicity and a better therapeutic index.
AS1409 is an IL-12-armed antibody in which humanized antibody BC1 is covalently linked to IL-12. It is constructed to deliver IL-12 to tumor-associated vasculature. Humanized antibody BC1 targets the ED-B variant of fibronectin. In a phase I clinical trial, 11 patients with melanoma and 2 with renal cell carcinoma received AS1409 at doses of 15 and 25 μg/kg (78). Most of the observed adverse events were grade 2 or lower. These adverse events included chills, pyrexia, vomiting, fatigue, transient liver function abnormalities, and headache. No dose-limiting toxicities were observed at 15 μg/kg weekly. However, 3 patients had dose-limiting toxicities at the 25 μg/kg dose level. One patient had grade 3 fatigue, and 2 patients had grade 3 transaminase elevation, which resolved after study drug discontinuation. At the 25 μg/kg dose, dose-limiting transaminase elevation and grade 3 fatigue were observed. Of the 11 patients, anemia of grade 3 to 4 was observed in 5 and lymphopenia in 7.
Another IL-12-armed antibody IL12-L19 is being investigated. It targets the splicing variant extra domain B of fibronectin. But there is no toxicity data available from this clinic trial (NCT04471987) yet (81, 82).
Tumor-targeted tumor-infiltrating lymphocytes or CAR-T cells armed with IL-12 in clinical trials
Tumor-infiltrating lymphocytes (TILs) isolated from tumor specimens have been shown to have highly specific cytolytic activity against their autologous tumors, and this activity inspired the development of TIL immunotherapy at the end of the last century (83–85). In 2015, Zhang et al. reported a clinical trial of IL-12 delivered via TILs (79). The trial enrolled 33 patients with metastatic melanoma. Patients were treated with autologous TILs in escalating doses. The TILs were transduced with nuclear factor of activated T cells (NFAT.IL12) promoter driving an IL-12 single-chain gene. Only 1 of the 17 patients who received 0.001 to 0.1 × 109 NFAT.IL12–transduced TILs had an objective response. But among patients who received doses between 0.3 and 3 × 109 cells, 10 of 16 experienced clinical responses. No immediate complications were observed after first cell infusion in all patients. Following that toxicity could be observed. High IL-12 and IFNγ serum levels were observed in patients treated with high cell doses, as were clinical adverse events such as high fever, liver dysfunction, and sporadic severe hemodynamic instability. Increased serum ALT and AST were observed in all cohorts, and the incidence grew higher at higher TIL doses. Fever was observed in all patients. The high IL-12 and IFNγ levels in the serum were life threatening. Some patients were transferred to the intensive care unit for management of these events. Grade 3 adverse events were observed in 16 patients, and grade 4 adverse events were observed in 4 patients. This was the first-in-human trial of autologous TILs that carried an inducible IL-12 gene. It was highlighted that cell doses were 10- to 100-fold lower than the conventional TILs. However, multiple and high-grade toxicities were observed in most patients, and these adverse events were attributable to the secreted IL-12.
Though the IL-12-armed TILs produced toxicity, IL-12-armed CAR-T cell therapy seemed to cause limited toxicity. In a phase I clinical trial of IL-12 delivered via mucin 1 (MUC1)-targeting CAR-T cells reported in 2016 by You et al., only mild toxic effects were observed (36). In the study, 2 anti-(MUC1) CAR-T cell lines were constructed. One CAR-T cell line, named SM3-CAR, had an SM3 single-chain variable fragment sequence that target MUC1. The other CAR-T cell line, named pSM3-CAR, contained an SM3 single-chain variable fragment sequence that was modified to have higher binding affinity to MUC1. Only the first CAR-T cells, SM3-CAR co-expressed IL-12. These 2 types of CAR-T cells were injected intratumorally into 2 independent metastatic lesions of the only patient enrolled. Adverse events included mild headache, muscle pain, nasal congestion, and mild abdominal bloating discomfort. All adverse effects resolved by day 12 post intratumoral administration. Analysis of the patient’s blood indicated some abnormalities, such as elevated eosinophil ratio and counts and glucose levels, which suggested an inflammatory response or acute response. The results indicating a serum cytokine response were positive, and the reported side effects of the MUC1-targeting CAR-T cell strategy were very mild.
There is a clinical trial (NCT03932565) that is being investigated. Nectin4/FAP (fibroblast activation protein) targeting CAR-T cells that express IL7 and CCL19, or IL12 were created to treat malignant solid tumors. But there is no toxicity data available from this clinic trial yet.
Exploration of future safe IL-12 clinical studies
Based on published preclinical studies, we can easily predict that multiple tumor-targeted IL-12 therapies will be evaluated in clinical trials. This approach will also solve the thorny issue of intratumoral delivery for inaccessible metastatic tumors. Both tumor-targeted IL-12 protein and gene/cell therapies will be seen in clinical trials in the near future.
One tumor-targeted IL-12 protein therapy, NHS-tethered IL-12, is particularly noteworthy. Two IL-12 heterodimeric molecules were combined with NHS76 antibody to produce a fusion protein, NHS-IL12 immuno-cytokine. Mechanism studies have proven that IL-12 could be targeted to areas with tumor necrosis by the NHS76 antibody through binding histones to free DNA fragments found in these regions. This targeting mechanism resulted in promoted antitumor activity (80). In the phase I clinical trial, NHS-IL12 were administered subcutaneously to 59 patients with metastatic solid tumors. Of these participants, 22 were enrolled in a single ascending-dose cohort and 37 in an every-4-week multiple ascending-dose cohort. Five patients were reported to have durable stable disease. But no tumor responses were observed. Flu-like symptoms, increased ALT/AST, and decreased circulating lymphocyte count were the most frequently observed treatment-related adverse events. Among all treatment-related grade 3 adverse events, only hyperhidrosis was symptomatic. All others were transient.
Regarding tumor-targeted IL-12 gene therapy, there was design to delivers non-secreting IL-12 with tumor-targeted oncolytic adenovirus (Ad-TD-nsIL12) to tumor cells. The design was tested in Syrian hamster models of pancreatic cancer to examine its therapeutic and toxic effects (86). Surprisingly, no toxic side effects were observed after intraperitoneal delivery of Ad-TD-nsIL12 to orthotopic pancreatic tumors model. The peritoneal disseminated pancreatic tumors were cured. and animal survival was significantly enhanced. After intraperitoneal administration of Ad-TDnsIL12 (1 × 109) into hamsters that had peritoneally disseminated SHPC6 pancreatic tumors, liver function was examined by assessing AST, ALT, and ALP levels in the serum on days 1, 3, and 5. All 3 enzymes were found to remain at levels equivalent to those in the PBS-treated control animals. Serum levels of IL-12 remained constant at all the time points examined, as expected.
Another novel tumor-targeted IL-12 gene is a tumor cell surface vimentin-targeted IL-12 (ttIL12). Combined with resection of the primary tumor, ttIL12 transformed tumors immune profile to INFγ HiCD8HiFOXP3LowCD33Low (87). The immune profile transformation inhibited metastasis and increased survival in both mouse tumor model and patient-derived xenograft tumor mouse models. Mice treated with wild-type IL-12 and surgery had shorter overall survival than the control plasmid DNA treatment group. This significant difference was believed to be the result of IL-12 toxicity. However, IL-12 toxicity was not observed in the ttIL12-treated mice.
Despite the success of tumor targeted IL-12 gene therapy in preclinical models, the success of this therapy in clinical trials is questionable because a therapeutic level of IL-12 must accumulate at the tumor site. Such therapeutic levels were achieved in the previously described trial by Zhang et al. using TIL-armed IL-12 therapy (79). However, that trial demonstrated that cytokines secreted by TILs can also induce toxicity when the number of T cells is high. It seems that avoiding IL-12 secretion before T cells accumulate in tumors will be the key to reduce the toxicity. This hypothesis (concept) provided the foundation for our creation of attIL12-T cell therapy, in which IL-12 is anchored to T cells via including a transmembrane domain in the C-terminal of ttIL12 (WO2018068008A1) (27).
This hypothesis (concept) has been validated by a recent publication by Zhang et al., in which the authors found that anchoring IL-12 on T cells avoided IL-12 secretion and the associated systemic toxicity (28). This membrane-anchored IL-12 (aIL12) strategy also increased antitumor efficacy, lowered levels of circulating IL-12 and IFNγ, and did not cause body weight loss in patient-derived xenograft models. NFAT-inducible promoter driven aIL12 expression coordinated the expression of aIL12 and T cell activation. These aIL12-T cells were tested in an OT-1 TCR transgenic murine tumor model. Experimental results showed that aIL12 expression induced by NFAT improved the treatment outcome, but no detectable IL-12 or weight loss was observed. It was then tested in a human tumor xenograft mouse model. The aIL12 expression induced by NFAT enhanced antitumor responses through human T cells that co-expressed tumor-specific engineered TCRs. In both mouse models, this NFAT-inducible IL-12 expression construct did not yield detectable IL-12 in serum.
Both ttIL12- and aIL12-T cells reduced toxic cytokine induction in peripheral tissues. This feature is important because CAR-T cells induce severe cytokine release syndrome in 50% of treated patients (88–90), and this percentage could be reduced by attIL12 modification of these T cells. Supporting this hypothesis, attIL12-modified CAR-T cells or TCR-T cells constrained the production of IL12-induced cytokines in tumors and significantly inhibited cytokine release syndrome-associated cytokines in peripheral tissues of both immune deficient human tumor-bearing mice and immune competent mouse tumor-bearing mice (27).
Conclusion
The above review includes different types of IL-12 clinical studies using rhIL-12 protein, IL-12-modified cells, and IL-12 genes delivered via physical, chemical, or viral vectors. All these approaches have improved safety, but none of them have eliminated the toxic cytokine release in peripheral tissue associated toxicity. To avoid this clinical side effect, we have invented attIL12-T cell therapy, and others have explored NFAT-inducible IL-12 therapy using mouse models. However, these products, attIL12-modified TILs, TCR-T cells, and CAR-T cells, have yet to be evaluated in the clinical setting. The success of such trials would further boost the enthusiasm for T cell therapy. Of note, attIL12-T cells also boosted T cell penetration and induced antigen spreading, and these bundled features may boost the firepower of currently explored CAR-T cell therapies while reducing the risk of adverse effects.
Author contributions
ZJ draft the manuscript and conducted the literature search. SL revised and prepared the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Funding support: NIH/NCI, R01 CA120985.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ALT, alanine transaminase; AST, aspartate transaminase; att (cell membrane-anchored and tumor-targeted; IL-12, interleukin 12; CAR, chimeric antigen receptor; DC, dendritic cell; IFNγ, interferon gamma; IL-12, interleukin 12; NK, natural killer; rh, recombinant human; TCR, T cell receptor; CRS, cytokine release syndrome.
References
1. Kobayashi M, Fitz L, Ryan M, Hewick RM, Clark SC, Chan S, et al. Identification and purification of natural killer cell stimulatory factor (NKSF), a cytokine with multiple biologic effects on human lymphocytes. J Exp Med (1989) 170(3):827–45. doi: 10.1084/jem.170.3.827
2. Stern AS, Podlaski FJ, Hulmes JD, Pan YC, Quinn PM, Wolitzky AG, et al. Purification to homogeneity and partial characterization of cytotoxic lymphocyte maturation factor from human b-lymphoblastoid cells. Proc Natl Acad Sci USA (1990) 87(17):6808–12. doi: 10.1073/pnas.87.17.6808
3. Aste-Amezaga M, D’Andrea A, Kubin M, Trinchieri G. Cooperation of natural killer cell stimulatory factor/interleukin-12 with other stimuli in the induction of cytokines and cytotoxic cell-associated molecules in human T and NK cells. Cell Immunol (1994) 156(2):480–92. doi: 10.1006/cimm.1994.1192
4. Nguyen HM, Guz-Montgomery K, Saha D. Oncolytic virus encoding a master pro-inflammatory cytokine interleukin 12 in cancer immunotherapy. Cells (2020) 9(2):400–26. doi: 10.3390/cells9020400
5. van Herpen CM, van der Voort R, van der Laak JA, Klasen IS, de Graaf AO, van Kempen LC, et al. Intratumoral rhIL-12 administration in head and neck squamous cell carcinoma patients induces b cell activation. Int J Cancer (2008) 123(10):2354–61. doi: 10.1002/ijc.23756
6. Grohmann U, Belladonna ML, Bianchi R, Orabona C, Ayroldi E, Fioretti MC, et al. IL-12 acts directly on DC to promote nuclear localization of NF-kappaB and primes DC for IL-12 production. Immunity (1998) 9(3):315–23. doi: 10.1016/S1074-7613(00)80614-7
7. Atkins MB, Robertson MJ, Gordon M, Lotze MT, DeCoste M, DuBois JS, et al. Phase I evaluation of intravenous recombinant human interleukin 12 in patients with advanced malignancies. Clin Cancer Res (1997) 3(3):409–17.
8. Cohen J. IL-12 deaths: explanation and a puzzle. Science (1995) 270(5238):908. doi: 10.1126/science.270.5238.908.a
9. Zeuzem S, Carreno V. Interleukin-12 in the treatment of chronic hepatitis b and c. Antiviral Res (2001) 52(2):181–8. doi: 10.1016/S0166-3542(01)00183-8
10. Rigopoulou EI, Suri D, Chokshi S, Mullerova I, Rice S, Tedder RS, et al. Lamivudine plus interleukin-12 combination therapy in chronic hepatitis b: antiviral and immunological activity. Hepatol (Baltimore Md) (2005) 42(5):1028–36. doi: 10.1002/hep.20888
11. Li SS, Kochar NK, Elizaga M, Hay CM, Wilson GJ, Cohen KW, et al. DNA Priming increases frequency of T-cell responses to a vesicular stomatitis virus HIV vaccine with specific enhancement of CD8(+) T-cell responses by interleukin-12 plasmid DNA. Clin Vaccine immunol: CVI (2017) 24(11):e00263-17. doi: 10.1128/CVI.00263-17
12. Kerkar SP, Muranski P, Kaiser A, Boni A, Sanchez-Perez L, Yu Z, et al. Tumor-specific CD8+ T cells expressing interleukin-12 eradicate established cancers in lymphodepleted hosts. Cancer Res (2010) 70(17):6725–34. doi: 10.1158/0008-5472.CAN-10-0735
13. Zhang L, Kerkar SP, Yu Z, Zheng Z, Yang S, Restifo NP, et al. Improving adoptive T cell therapy by targeting and controlling IL-12 expression to the tumor environment. Mol Ther (2011) 19(4):751–9. doi: 10.1038/mt.2010.313
14. Lenzi R, Edwards R, June C, Seiden MV, Garcia ME, Rosenblum M, et al. Phase II study of intraperitoneal recombinant interleukin-12 (rhIL-12) in patients with peritoneal carcinomatosis (residual disease < 1 cm) associated with ovarian cancer or primary peritoneal carcinoma. J Trans Med (2007) 5:66. doi: 10.1186/1479-5876-5-66
15. Haicheur N, Escudier B, Dorval T, Negrier S, De Mulder PH, Dupuy JM, et al. Cytokines and soluble cytokine receptor induction after IL-12 administration in cancer patients. Clin Exp Immunol (2000) 119(1):28–37. doi: 10.1046/j.1365-2249.2000.01112.x
16. Lu X. Impact of IL-12 in cancer. Curr Cancer Drug Targets (2017) 17(8):682–97. doi: 10.2174/1568009617666170427102729
17. Lasek W, Zagozdzon R, Jakobisiak M. Interleukin 12: still a promising candidate for tumor immunotherapy? Cancer immunol immunother: CII (2014) 63(5):419–35. doi: 10.1007/s00262-014-1523-1
18. Robertson MJ, Pelloso D, Abonour R, Hromas RA, Nelson RP Jr., Wood L, et al. Interleukin 12 immunotherapy after autologous stem cell transplantation for hematological malignancies. Clin Cancer Res (2002) 8(11):3383–93.
19. Van Herpen CM, Huijbens R, Looman M, De Vries J, Marres H, Van De Ven J, et al. Pharmacokinetics and immunological aspects of a phase ib study with intratumoral administration of recombinant human interleukin-12 in patients with head and neck squamous cell carcinoma: a decrease of T-bet in peripheral blood mononuclear cells. Clin Cancer Res (2003) 9(8):2950–6.
20. van Herpen CM, Looman M, Zonneveld M, Scharenborg N, de Wilde PC, van de Locht L, et al. Intratumoral administration of recombinant human interleukin 12 in head and neck squamous cell carcinoma patients elicits a T-helper 1 profile in the locoregional lymph nodes. Clin Cancer Res (2004) 10(8):2626–35. doi: 10.1158/1078-0432.CCR-03-0304
21. Bekaii-Saab TS, Roda JM, Guenterberg KD, Ramaswamy B, Young DC, Ferketich AK, et al. A phase I trial of paclitaxel and trastuzumab in combination with interleukin-12 in patients with HER2/neu-expressing malignancies. Mol Cancer Ther (2009) 8(11):2983–91. doi: 10.1158/1535-7163.MCT-09-0820
22. Pelloso D, Cyran K, Timmons L, Williams BT, Robertson MJ. Immunological consequences of interleukin 12 administration after autologous stem cell transplantation. Clin Cancer Res (2004) 10(6):1935–42. doi: 10.1158/1078-0432.CCR-03-1156
23. Parihar R, Nadella P, Lewis A, Jensen R, De Hoff C, Dierksheide JE, et al. A phase I study of interleukin 12 with trastuzumab in patients with human epidermal growth factor receptor-2-overexpressing malignancies: analysis of sustained interferon gamma production in a subset of patients. Clin Cancer Res (2004) 10(15):5027–37. doi: 10.1158/1078-0432.CCR-04-0265
24. Leonard JP, Sherman ML, Fisher GL, Buchanan LJ, Larsen G, Atkins MB, et al. Effects of single-dose interleukin-12 exposure on interleukin-12-associated toxicity and interferon-gamma production. Blood (1997) 90(7):2541–8.
25. Romee R, Rosario M, Berrien-Elliott MM, Wagner JA, Jewell BA, Schappe T, et al. Cytokine-induced memory-like natural killer cells exhibit enhanced responses against myeloid leukemia. Sci Transl Med (2016) 8(357):357ra123. doi: 10.1126/scitranslmed.aaf2341
26. Elizaga ML, Li SS, Kochar NK, Wilson GJ, Allen MA, Tieu HVN, et al. Safety and tolerability of HIV-1 multiantigen pDNA vaccine given with IL-12 plasmid DNA via electroporation, boosted with a recombinant vesicular stomatitis virus HIV gag vaccine in healthy volunteers in a randomized, controlled clinical trial. PloS One (2018) 13(9):e0202753. doi: 10.1371/journal.pone.0202753
27. Hu J, Yang Q, Zhang W, Du H, Chen Y, Zhao Q, et al. Cell membrane-anchored and tumor-targeted IL-12 (attIL12)-T cell therapy for eliminating large and heterogeneous solid tumors. J Immunother Cancer (2022) 10(1):e003633. doi: 10.1136/jitc-2021-003633
28. Zhang L, Davies JS, Serna C, Yu Z, Restifo NP, Rosenberg SA, et al. Enhanced efficacy and limited systemic cytokine exposure with membrane-anchored interleukin-12 T-cell therapy in murine tumor models. J Immunother Cancer (2020) 8(1):e000210. doi: 10.1136/jitc-2019-000210
29. Younes A, Pro B, Robertson MJ, Flinn IW, Romaguera JE, Hagemeister F, et al. Phase II clinical trial of interleukin-12 in patients with relapsed and refractory non-hodgkin’s lymphoma and hodgkin’s disease. Clin Cancer Res (2004) 10(16):5432–8. doi: 10.1158/1078-0432.CCR-04-0540
30. Mahvi DM, Henry MB, Albertini MR, Weber S, Meredith K, Schalch H, et al. Intratumoral injection of IL-12 plasmid DNA–results of a phase I/IB clinical trial. Cancer Gene Ther (2007) 14(8):717–23. doi: 10.1038/sj.cgt.7701064
31. Czerniecki BJ, Koski GK, Koldovsky U, Xu S, Cohen PA, Mick R, et al. Targeting HER-2/neu in early breast cancer development using dendritic cells with staged interleukin-12 burst secretion. Cancer Res (2007) 67(4):1842–52. doi: 10.1158/0008-5472.CAN-06-4038
32. Triozzi PL, Allen KO, Carlisle RR, Craig M, LoBuglio AF, Conry RM. Phase I study of the intratumoral administration of recombinant canarypox viruses expressing B7.1 and interleukin 12 in patients with metastatic melanoma. Clin Cancer Res (2005) 11(11):4168–75. doi: 10.1158/1078-0432.ccr-04-2283
33. Ren H, Boulikas T, Lundstrom K, Soling A, Warnke PC, Rainov NG. Immunogene therapy of recurrent glioblastoma multiforme with a liposomally encapsulated replication-incompetent semliki forest virus vector carrying the human interleukin-12 gene–a phase I/II clinical protocol. J Neuro-Oncol (2003) 64(1-2):147–54. doi: 10.1007/BF02700029
34. Heinzerling L, Burg G, Dummer R, Maier T, Oberholzer PA, Schultz J, et al. Intratumoral injection of DNA encoding human interleukin 12 into patients with metastatic melanoma: clinical efficacy. Hum Gene Ther (2005) 16(1):35–48. doi: 10.1089/hum.2005.16.35
35. Dohnal AM, Witt V, Hugel H, Holter W, Gadner H, Felzmann T. Phase I study of tumor Ag-loaded IL-12 secreting semi-mature DC for the treatment of pediatric cancer. Cytotherapy (2007) 9(8):755–70. doi: 10.1080/14653240701589221
36. You F, Jiang L, Zhang B, Lu Q, Zhou Q, Liao X, et al. Phase 1 clinical trial demonstrated that MUC1 positive metastatic seminal vesicle cancer can be effectively eradicated by modified anti-MUC1 chimeric antigen receptor transduced T cells. Sci China Life Sci (2016) 59(4):386–97. doi: 10.1007/s11427-016-5024-7
37. Daud AI, DeConti RC, Andrews S, Urbas P, Riker AI, Sondak VK, et al. Phase I trial of interleukin-12 plasmid electroporation in patients with metastatic melanoma. J Clin Oncol (2008) 26(36):5896–903. doi: 10.1200/JCO.2007.15.6794
38. Motzer RJ, Rakhit A, Schwartz LH, Olencki T, Malone TM, Sandstrom K, et al. Phase I trial of subcutaneous recombinant human interleukin-12 in patients with advanced renal cell carcinoma. Clin Cancer Res (1998) 4(5):1183–91.
39. Portielje JE, Kruit WH, Schuler M, Beck J, Lamers CH, Stoter G, et al. Phase I study of subcutaneously administered recombinant human interleukin 12 in patients with advanced renal cell cancer. Clin Cancer Res (1999) 5(12):3983–9.
40. Robertson MJ, Cameron C, Atkins MB, Gordon MS, Lotze MT, Sherman ML, et al. Immunological effects of interleukin 12 administered by bolus intravenous injection to patients with cancer. Clin Cancer Res (1999) 5(1):9–16.
41. Rook AH, Wood GS, Yoo EK, Elenitsas R, Kao DM, Sherman ML, et al. Interleukin-12 therapy of cutaneous T-cell lymphoma induces lesion regression and cytotoxic T-cell responses. Blood (1999) 94(3):902–8. doi: 10.1182/blood.V94.3.902.415k23_902_908
42. Gollob JA, Mier JW, Veenstra K, McDermott DF, Clancy D, Clancy M, et al. Phase I trial of twice-weekly intravenous interleukin 12 in patients with metastatic renal cell cancer or malignant melanoma: ability to maintain IFN-gamma induction is associated with clinical response. Clin Cancer Res (2000) 6(5):1678–92.
43. Ohno R, Yamaguchi Y, Toge T, Kinouchi T, Kotake T, Shibata M, et al. A dose-escalation and pharmacokinetic study of subcutaneously administered recombinant human interleukin 12 and its biological effects in Japanese patients with advanced malignancies. Clin Cancer Res (2000) 6(7):2661–9.
44. Gollob JA, Veenstra KG, Mier JW, Atkins MB. Agranulocytosis and hemolytic anemia in patients with renal cell cancer treated with interleukin-12. J immunother (Hagerstown Md: 1997) (2001) 24(1):91–8. doi: 10.1097/00002371-200101000-00011
45. Hurteau JA, Blessing JA, DeCesare SL, Creasman WT. Evaluation of recombinant human interleukin-12 in patients with recurrent or refractory ovarian cancer: a gynecologic oncology group study. Gynecol Oncol (2001) 82(1):7–10. doi: 10.1006/gyno.2001.6255
46. Lee P, Wang F, Kuniyoshi J, Rubio V, Stuges T, Groshen S, et al. Effects of interleukin-12 on the immune response to a multipeptide vaccine for resected metastatic melanoma. J Clin Oncol (2001) 19(18):3836–47. doi: 10.1200/JCO.2001.19.18.3836
47. Ansell SM, Witzig TE, Kurtin PJ, Sloan JA, Jelinek DF, Howell KG, et al. Phase 1 study of interleukin-12 in combination with rituximab in patients with b-cell non-Hodgkin lymphoma. Blood (2002) 99(1):67–74. doi: 10.1182/blood.V99.1.67
48. Lenzi R, Rosenblum M, Verschraegen C, Kudelka AP, Kavanagh JJ, Hicks ME, et al. Phase I study of intraperitoneal recombinant human interleukin 12 in patients with mullerian carcinoma, gastrointestinal primary malignancies, and mesothelioma. Clin Cancer Res (2002) 8(12):3686–95.
49. Cebon J, Jager E, Shackleton MJ, Gibbs P, Davis ID, Hopkins W, et al. Two phase I studies of low dose recombinant human IL-12 with melan-a and influenza peptides in subjects with advanced malignant melanoma. Cancer Immun (2003) 3:7.
50. Gollob JA, Veenstra KG, Parker RA, Mier JW, McDermott DF, Clancy D, et al. Phase I trial of concurrent twice-weekly recombinant human interleukin-12 plus low-dose IL-2 in patients with melanoma or renal cell carcinoma. J Clin Oncol (2003) 21(13):2564–73. doi: 10.1200/JCO.2003.12.119
51. Melichar B, Lenzi R, Rosenblum M, Kudelka AP, Kavanagh JJ, Melicharova K, et al. Intraperitoneal fluid neopterin, nitrate, and tryptophan after regional administration of interleukin-12. J Immunother (Hagerstown Md: 1997). (2003) 26(3):270–6. doi: 10.1097/00002371-200305000-00010
52. Peterson AC, Harlin H, Gajewski TF. Immunization with melan-a peptide-pulsed peripheral blood mononuclear cells plus recombinant human interleukin-12 induces clinical activity and T-cell responses in advanced melanoma. J Clin Oncol (2003) 21(12):2342–8. doi: 10.1200/JCO.2003.12.144
53. Portielje JE, Lamers CH, Kruit WH, Sparreboom A, Bolhuis RL, Stoter G, et al. Repeated administrations of interleukin (IL)-12 are associated with persistently elevated plasma levels of IL-10 and declining IFN-gamma, tumor necrosis factor-alpha, IL-6, and IL-8 responses. Clin Cancer Res (2003) 9(1):76–83.
54. Kikuchi T, Akasaki Y, Abe T, Fukuda T, Saotome H, Ryan JL, et al. Vaccination of glioma patients with fusions of dendritic and glioma cells and recombinant human interleukin 12. J Immunother (Hagerstown Md: 1997) (2004) 27(6):452–9. doi: 10.1097/00002371-200411000-00005
55. Wadler S, Levy D, Frederickson HL, Falkson CI, Wang Y, Weller E, et al. A phase II trial of interleukin-12 in patients with advanced cervical cancer: clinical and immunologic correlates. Eastern cooperative oncology group study E1E96. Gynecol Oncol (2004) 92(3):957–64. doi: 10.1016/j.ygyno.2003.12.022
56. Eisenbeis CF, Lesinski GB, Anghelina M, Parihar R, Valentino D, Liu J, et al. Phase I study of the sequential combination of interleukin-12 and interferon alfa-2b in advanced cancer: evidence for modulation of interferon signaling pathways by interleukin-12. J Clin Oncol (2005) 23(34):8835–44. doi: 10.1200/JCO.2005.02.1691
57. Ansell SM, Geyer SM, Maurer MJ, Kurtin PJ, Micallef IN, Stella P, et al. Randomized phase II study of interleukin-12 in combination with rituximab in previously treated non-hodgkin’s lymphoma patients. Clin Cancer Res (2006) 12(20 Pt 1):6056–63. doi: 10.1158/1078-0432.CCR-06-1245
58. Duvic M, Sherman ML, Wood GS, Kuzel TM, Olsen E, Foss F, et al. A phase II open-label study of recombinant human interleukin-12 in patients with stage IA, IB, or IIA mycosis fungoides. J Am Acad Dermatol (2006) 55(5):807–13. doi: 10.1016/j.jaad.2006.06.038
59. Jacobson MA, Sinclair E, Bredt B, Agrillo L, Black D, Epling CL, et al. Safety and immunogenicity of towne cytomegalovirus vaccine with or without adjuvant recombinant interleukin-12. Vaccine (2006) 24(25):5311–9. doi: 10.1016/j.vaccine.2006.04.017
60. Little RF, Pluda JM, Wyvill KM, Rodriguez-Chavez IR, Tosato G, Catanzaro AT, et al. Activity of subcutaneous interleukin-12 in AIDS-related kaposi sarcoma. Blood (2006) 107(12):4650–7. doi: 10.1182/blood-2005-11-4455
61. Hamid O, Solomon JC, Scotland R, Garcia M, Sian S, Ye W, et al. Alum with interleukin-12 augments immunity to a melanoma peptide vaccine: Correlation with time to relapse in patients with resected high-risk disease. Clin Cancer Res (2007) 13(1):215–22. doi: 10.1158/1078-0432.CCR-06-1450
62. Hansson L, Abdalla AO, Moshfegh A, Choudhury A, Rabbani H, Nilsson B, et al. Long-term idiotype vaccination combined with interleukin-12 (IL-12), or IL-12 and granulocyte macrophage colony-stimulating factor, in early-stage multiple myeloma patients. Clin Cancer Res (2007) 13(5):1503–10. doi: 10.1158/1078-0432.CCR-06-1603
63. Little RF, Aleman K, Kumar P, Wyvill KM, Pluda JM, Read-Connole E, et al. Phase 2 study of pegylated liposomal doxorubicin in combination with interleukin-12 for AIDS-related kaposi sarcoma. Blood (2007) 110(13):4165–71. doi: 10.1182/blood-2007-06-097568
64. Lacy MQ, Jacobus S, Blood EA, Kay NE, Rajkumar SV, Greipp PR. Phase II study of interleukin-12 for treatment of plateau phase multiple myeloma (E1A96): A trial of the Eastern cooperative oncology group. Leukemia Res (2009) 33(11):1485–9. doi: 10.1016/j.leukres.2009.01.020
65. Gokhale MS, Vainstein V, Tom J, Thomas S, Lawrence CE, Gluzman-Poltorak Z, et al. Single low-dose rHuIL-12 safely triggers multilineage hematopoietic and immune-mediated effects. Exp Hematol Oncol (2014) 3(1):11. doi: 10.1186/2162-3619-3-11
66. Sun Y, Jurgovsky K, Moller P, Alijagic S, Dorbic T, Georgieva J, et al. Vaccination with IL-12 gene-modified autologous melanoma cells: preclinical results and a first clinical phase I study. Gene Ther (1998) 5(4):481–90. doi: 10.1038/sj.gt.3300619
67. Kang WK, Park C, Yoon HL, Kim WS, Yoon SS, Lee MH, et al. Interleukin 12 gene therapy of cancer by peritumoral injection of transduced autologous fibroblasts: outcome of a phase I study. Hum Gene Ther (2001) 12(6):671–84. doi: 10.1089/104303401300057388
68. Sangro B, Mazzolini G, Ruiz J, Herraiz M, Quiroga J, Herrero I, et al. Phase I trial of intratumoral injection of an adenovirus encoding interleukin-12 for advanced digestive tumors. J Clin Oncol (2004) 22(8):1389–97. doi: 10.1200/JCO.2004.04.059
69. Anwer K, Barnes MN, Fewell J, Lewis DH, Alvarez RD. Phase-I clinical trial of IL-12 plasmid/lipopolymer complexes for the treatment of recurrent ovarian cancer. Gene Ther (2010) 17(3):360–9. doi: 10.1038/gt.2009.159
70. Kalams SA, Parker S, Jin X, Elizaga M, Metch B, Wang M, et al. Safety and immunogenicity of an HIV-1 gag DNA vaccine with or without IL-12 and/or IL-15 plasmid cytokine adjuvant in healthy, HIV-1 uninfected adults. PloS One (2012) 7(1):e29231. doi: 10.1371/journal.pone.0029231
71. Anwer K, Kelly FJ, Chu C, Fewell JG, Lewis D, Alvarez RD. Phase I trial of a formulated IL-12 plasmid in combination with carboplatin and docetaxel chemotherapy in the treatment of platinum-sensitive recurrent ovarian cancer. Gynecol Oncol (2013) 131(1):169–73. doi: 10.1016/j.ygyno.2013.07.081
72. Carreno BM, Becker-Hapak M, Huang A, Chan M, Alyasiry A, Lie WR, et al. IL-12p70-producing patient DC vaccine elicits Tc1-polarized immunity. J Clin Invest (2013) 123(8):3383–94. doi: 10.1172/JCI68395
73. Kalams SA, Parker SD, Elizaga M, Metch B, Edupuganti S, Hural J, et al. Safety and comparative immunogenicity of an HIV-1 DNA vaccine in combination with plasmid interleukin 12 and impact of intramuscular electroporation for delivery. J Infect Dis (2013) 208(5):818–29. doi: 10.1093/infdis/jit236
74. Alvarez RD, Sill MW, Davidson SA, Muller CY, Bender DP, DeBernardo RL, et al. A phase II trial of intraperitoneal EGEN-001, an IL-12 plasmid formulated with PEG-PEI-cholesterol lipopolymer in the treatment of persistent or recurrent epithelial ovarian, fallopian tube or primary peritoneal cancer: a gynecologic oncology group study. Gynecol Oncol (2014) 133(3):433–8. doi: 10.1016/j.ygyno.2014.03.571
75. Mpendo J, Mutua G, Nyombayire J, Ingabire R, Nanvubya A, Anzala O, et al. A phase I double blind, placebo-controlled, randomized study of the safety and immunogenicity of electroporated HIV DNA with or without interleukin 12 in prime-boost combinations with an Ad35 HIV vaccine in healthy HIV-seronegative African adults. PloS One (2015) 10(8):e0134287. doi: 10.1371/journal.pone.0134287
76. Jacobson JM, Zheng L, Wilson CC, Tebas P, Matining RM, Egan MA, et al. The safety and immunogenicity of an interleukin-12-Enhanced multiantigen DNA vaccine delivered by electroporation for the treatment of HIV-1 infection. J Acquir Immune defic Syndr (1999) (2016) 71(2):163–71. doi: 10.1097/QAI.0000000000000830
77. Thaker PH, Brady WE, Lankes HA, Odunsi K, Bradley WH, Moore KN, et al. A phase I trial of intraperitoneal GEN-1, an IL-12 plasmid formulated with PEG-PEI-cholesterol lipopolymer, administered with pegylated liposomal doxorubicin in patients with recurrent or persistent epithelial ovarian, fallopian tube or primary peritoneal cancers: An NRG Oncology/Gynecologic oncology group study. Gynecol Oncol (2017) 147(2):283–90. doi: 10.1016/j.ygyno.2017.08.001
78. Rudman SM, Jameson MB, McKeage MJ, Savage P, Jodrell DI, Harries M, et al. A phase 1 study of AS1409, a novel antibody-cytokine fusion protein, in patients with malignant melanoma or renal cell carcinoma. Clin Cancer Res (2011) 17(7):1998–2005. doi: 10.1158/1078-0432.CCR-10-2490
79. Zhang L, Morgan RA, Beane JD, Zheng Z, Dudley ME, Kassim SH, et al. Tumor-infiltrating lymphocytes genetically engineered with an inducible gene encoding interleukin-12 for the immunotherapy of metastatic melanoma. Clin Cancer Res (2015) 21(10):2278–88. doi: 10.1158/1078-0432.CCR-14-2085
80. Strauss J, Heery CR, Kim JW, Jochems C, Donahue RN, Montgomery AS, et al. First-in-Human phase I trial of a tumor-targeted cytokine (NHS-IL12) in subjects with metastatic solid tumors. Clin Cancer Res (2019) 25(1):99–109. doi: 10.1158/1078-0432.CCR-18-1512
81. Ziffels B, Stringhini M, Probst P, Fugmann T, Sturm T, Neri D. Antibody-based delivery of cytokine payloads to carbonic anhydrase IX leads to cancer cures in immunocompetent tumor-bearing mice. Mol Cancer Ther (2019) 18(9):1544–54. doi: 10.1158/1535-7163.MCT-18-1301
82. Ongaro T, Matasci M, Cazzamalli S, Gouyou B, De Luca R, Neri D, et al. A novel anti-cancer L19-interleukin-12 fusion protein with an optimized peptide linker efficiently localizes in vivo at the site of tumors. J Biotechnol (2019) 291:17–25. doi: 10.1016/j.jbiotec.2018.12.004
83. Topalian SL, Muul LM, Solomon D, Rosenberg SA. Expansion of human tumor infiltrating lymphocytes for use in immunotherapy trials. J Immunol Methods (1987) 102(1):127–41. doi: 10.1016/S0022-1759(87)80018-2
84. Rosenberg SA, Packard BS, Aebersold PM, Solomon D, Topalian SL, Toy ST, et al. Use of tumor-infiltrating lymphocytes and interleukin-2 in the immunotherapy of patients with metastatic melanoma. A preliminary Rep N Engl J Med (1988) 319(25):1676–80. doi: 10.1056/NEJM198812223192527
85. Kradin RL, Kurnick JT, Lazarus DS, Preffer FI, Dubinett SM, Pinto CE, et al. Tumour-infiltrating lymphocytes and interleukin-2 in treatment of advanced cancer. Lancet (London England) (1989) 1(8638):577–80. doi: 10.1016/S0140-6736(89)91609-7
86. Wang P, Li X, Wang J, Gao D, Li Y, Li H, et al. Re-designing interleukin-12 to enhance its safety and potential as an anti-tumor immunotherapeutic agent. Nat Commun (2017) 8(1):1395. doi: 10.1038/s41467-017-01385-8
87. Zhao Q, Hu J, Mitra A, Cutrera J, Zhang W, Zhang Z, et al. Tumor-targeted IL-12 combined with tumor resection yields a survival-favorable immune profile. J Immunother Cancer (2019) 7(1):154. doi: 10.1186/s40425-019-0631-z
88. Jensen MC, Popplewell L, Cooper LJ, DiGiusto D, Kalos M, Ostberg JR, et al. Antitransgene rejection responses contribute to attenuated persistence of adoptively transferred CD20/CD19-specific chimeric antigen receptor redirected T cells in humans. Biol Blood marrow Transplant (2010) 16(9):1245–56. doi: 10.1016/j.bbmt.2010.03.014
89. Wang M, Munoz J, Goy A, Locke FL, Jacobson CA, Hill BT, et al. KTE-X19 CAR T-cell therapy in relapsed or refractory mantle-cell lymphoma. N Engl J Med (2020) 382(14):1331–42. doi: 10.1056/NEJMoa1914347
Keywords: IL-12, clinical trial, CRS, cytokines, T cells
Citation: Jia Z, Ragoonanan D, Mahadeo KM, Gill J, Gorlick R, Shpal E and Li S (2022) IL12 immune therapy clinical trial review: Novel strategies for avoiding CRS-associated cytokines. Front. Immunol. 13:952231. doi: 10.3389/fimmu.2022.952231
Received: 24 May 2022; Accepted: 29 August 2022;
Published: 20 September 2022.
Edited by:
Giulio Fracasso, University of Verona, ItalyReviewed by:
Khue Nguyen, North Carolina State University, United StatesXue-Feng Bai, The Ohio State University, United States
Copyright © 2022 Jia, Ragoonanan, Mahadeo, Gill, Gorlick, Shpal and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shulin Li, c2xpNEBtZGFuZGVyc29uLm9yZw==