 Iñigo Romon
Iñigo Romon Soledad Gonzalez-Barrera2
Soledad Gonzalez-Barrera2- 1Transfusion Section, Hematology Department, University Hospital “Marques de Valdecilla”, Santander, Spain
- 2Home Hospitalization Department, University Hospital “Marques de Valdecilla” - Instituto de Investigación Valdecilla (IDIVAL), Santander, Spain
- 3Transfusion Service, Toledo University Hospital, Toledo, Spain
- 4Hematology Department, University Hospital “Marques de Valdecilla” - IDIVAL, Santander, Spain
Hematopoietic stem cell transplantation and cell therapies like CAR-T are costly, complex therapeutic procedures. Outpatient models, including at-home transplantation, have been developed, resulting in similar survival results, reduced costs, and increased patient satisfaction. The complexity and safety of the process can be addressed with various emerging technologies (artificial intelligence, wearable sensors, point-of-care analytical devices, drones, virtual assistants) that allow continuous patient monitoring and improved decision-making processes. Patients, caregivers, and staff can also benefit from improved training with simulation or virtual reality. However, many technical, operational, and above all, ethical concerns need to be addressed. Finally, outpatient or at-home hematopoietic transplantation or CAR-T therapy creates a different, integrated operative system that must be planned, designed, and carefully adapted to the patient’s characteristics and distance from the hospital. Patients, clinicians, and their clinical environments can benefit from technically improved at-home transplantation.
1 Introduction
Medicine strives to find the best place of care for patients, which can be defined as one that achieves the best clinical outcomes with minimal disruption for the patient, at a manageable cost (1, 2).
With the number of hematopoietic stem cell transplantations (HSCTs) increasing, due to the number of conditions treated and the incorporation of low and middle-income countries into the HSCT field, rising costs, staffing difficulties and hospital capacity shortages must be addressed. The Worldwide Network for Blood and Marrow Transplantation identified the major cost drivers as patient characteristics, laboratory and radiology, drugs, supportive care, quality management and staff training, and graft procurement (3).
Outpatient (OP) and at-home management, were adopted early during the inception of hematological therapies, including HSCT (4).
The advent of CAR-T platforms with an increased range of indications and more limited toxicity, together with the physician’s experience and confidence, has increased interest in early patient discharge while maintaining close patient monitoring (5).
Social trends, cost constraints, and the impact of COVID-19 (6) support the shift from inpatient (IP) care to more acceptable modalities, like home care for HSCT or CAR-T cell therapies (2).
However, safety concerns for outpatient modalities will always be extremely important until HSCT and cell therapy procedures cause less aggressive effects on the patient’s health.
Fortunately, emerging technological developments (i.e., wearable devices, artificial intelligence (AI), facial recognition) provide important opportunities to increase safety while reducing costs. This mini-review discusses HSCT and CAR-T as models for clinical out-of-hospital management and takes a prospective view of technologies that can help maximize clinical efficacy, contain costs, and enhance patients´ well-being.
2 Outpatient and at-home HSCT
In 1997, Jagannath reported 91 multiple myeloma autologous HSCT (auto-HSCTs) followed on an OP basis (7).
In the OP setting, patients receive the conditioning regimen and HSCT infusion at an outpatient clinic or the hospital, and are then discharged and followed up in an ambulatory day clinic.
Nowadays, several reports on the management of HSCTs on an OP basis have been published, but systematization and research are still lacking (8). Even the definition of OP setting can be controversial since several modalities exist, from OP to full at-home management (9).
Holbro (10) reported 91 auto-HSCTs in myeloma patients managed entirely at an OP clinic where 84% had to be readmitted during the first 100 days, mostly for febrile neutropenia. No patient died or required ICU care. Savings of nearly 20,000 Canadian dollars per patient were calculated compared with IP HSCT.
McDiarmid (11) retrospectively analyzed infections in 178 allogeneic (allo-HSCT) and 508 autologous OP HSCTs from 1,045 consecutive allo- and auto-HSCTs. The infection incidence was significantly lower in both OP auto- and allo- cohorts compared to IP setting. The 100-day non-relapse mortality (NRM) was significantly lower for OP allo-HSCT than for IP allo-HSCT. They concluded that OP allo- and auto-HSCT had comparable short-term outcomes and complications to IP HSCT.
Granot (12) retrospectively reported 1,037 OP allo-HSCT, and noted that 47% of OP patients were never hospitalized as well as having a lower 5-year risk of NRM than IP HSCT (13% OP vs. 23% IP, p<0.001). OPs evaluated the experience favorably. Shingal (13) reported 856 OP allo-HSCT (a third of whom were never hospitalized) with a median decreased stay of 6 days but no report on long-term results was made.
A Mexican group found that performing OP allo- and auto- HSCTs, with simplified stem cell conservation or conditioning regimens, amongst other measures, could be a solution for countries needing less resource-intense modalities (14, 15).
In the at-home model, patients equally receive the conditioning regimen and stem cell infusion at the hospital or outpatient clinic, spending the aplastic phase at home, where they are cared for by a healthcare team and only returned to hospital if severe complications appear.
A group in Barcelona (16, 17) performed 50 auto-HSCT at home, suggesting nearly 50% cost reduction with great patient satisfaction. Gonzalez-Barrera (18) reported 84 at-home auto- HSCTs with a median at-home stay of 17 days, 86% experienced neutropenic fever, 44% presented grade 3-4 mucositis, and 26% received parenteral nutrition. Hospital readmission occurred in 12% of patients, usually for sepsis, and lasted a median of 9 days, with no transplant-related mortality (TRM). The Durham group analyzed both auto- and allo-HSCTs, finding similar results and good preservation of quality of life for at-home HSCTs (19) compared to IP controls.
Svahn (20) analyzed at-home allo-HSCTs finding significantly reduced TRM (13% at-home vs. 44% IP controls), with improved four-year survival (63% at-home vs. 44% IP controls). They suggested that this advantage could be due to better oral nutrition, resulting in the reduced probability of acute graft-versus-host disease (GvHD) and bacteriemia (21). Pediatric at-home allo-HSCTs has also been performed with favorable results (22, 23). Jenkelowitz reported great caregiver satisfaction for at-home HSCT (24)
Gonzalez (8) summarized 29 auto- and allo-HSCT studies, finding evidence of improved health outcomes, quality of life, and at-home/OP models vs IP effectiveness. Overall survival rates comparing both models were similar for both autologous and allogeneic patients. They also found that OP and at-home HSCT were safe, perhaps more than conventional modalities. They estimated a shorter average stay with the OP/at-home models, being 55% and 19% shorter than the IP model for auto- and allo-HSCTs, respectively, which could ease hospital bed shortages and waiting times. The average cost reduction over the IP-HSCT model was 33.42% and 19.27% for auto- and allo-HSCTs, respectively (Appendix 1 and 2 update a published summary of the studies on allo -HSCT and their results).
As Gonzalez has indicated (8), the high-quality research in the field that is needed for evaluation and benchmarking is lacking. Research should include clinical trials with uniform defining criteria for the different HSCT care models, uniform cost analyses, and assessment of personal experiences and quality of life of staff and patients involved. Finally, the different HSCT modalities should be registered in the different HSCT databases.
3 Outpatient CAR-T therapies
In the OP CAR-T model, lymphodepletion, and CAR-T infusion are administered at an OP clinic, with patients staying at home and followed up at fixed intervals at the OP clinic, and admitted to hospital preemptively, or to monitor or treat adverse events (25, 26).
Several authors have reviewed the challenges and requirements for OP CAR-T (5, 27–29).
Borogovac (26) reported 21 patients treated at a CAR-T unit designed for the OP setting. Seventy-one percent were admitted after discharge to treat adverse effects and stayed a median of 8 days, but none needed ER or ICU care. None died. Similar experiences were reported by McGann (25) with 40 patients. Cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) had a similar incidence as with IPs (25, 26). Table 1 summarizes these findings.
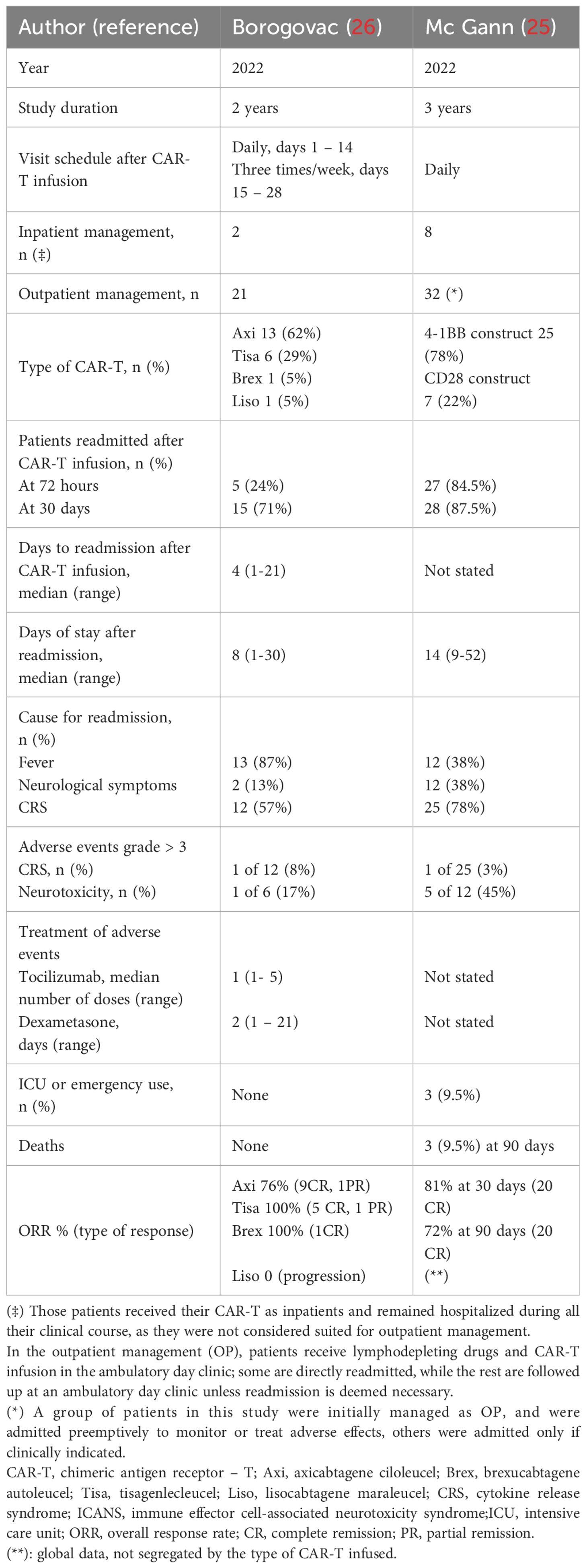
Table 1 Reported experiences of CAR-T outpatient management in daily practice.
Paludo (30) reported 123 OP CAR-T patients managed with a remote patient monitoring program (RPM), to monitor vital data and neurological symptoms (31). Sixteen percent could be completely managed in the OP setting, with a median stay of 8 days for those who were hospitalized to treat post CAR-T adverse effects, with 6% needing ICU. Most patients (83%) were satisfied with their RPM. Dwivedy (32)Shao (33) and Bachier (34) reported similar experiences. Appendix 3 summarizes these reports.
4 At-home and outpatient procedures: practical considerations
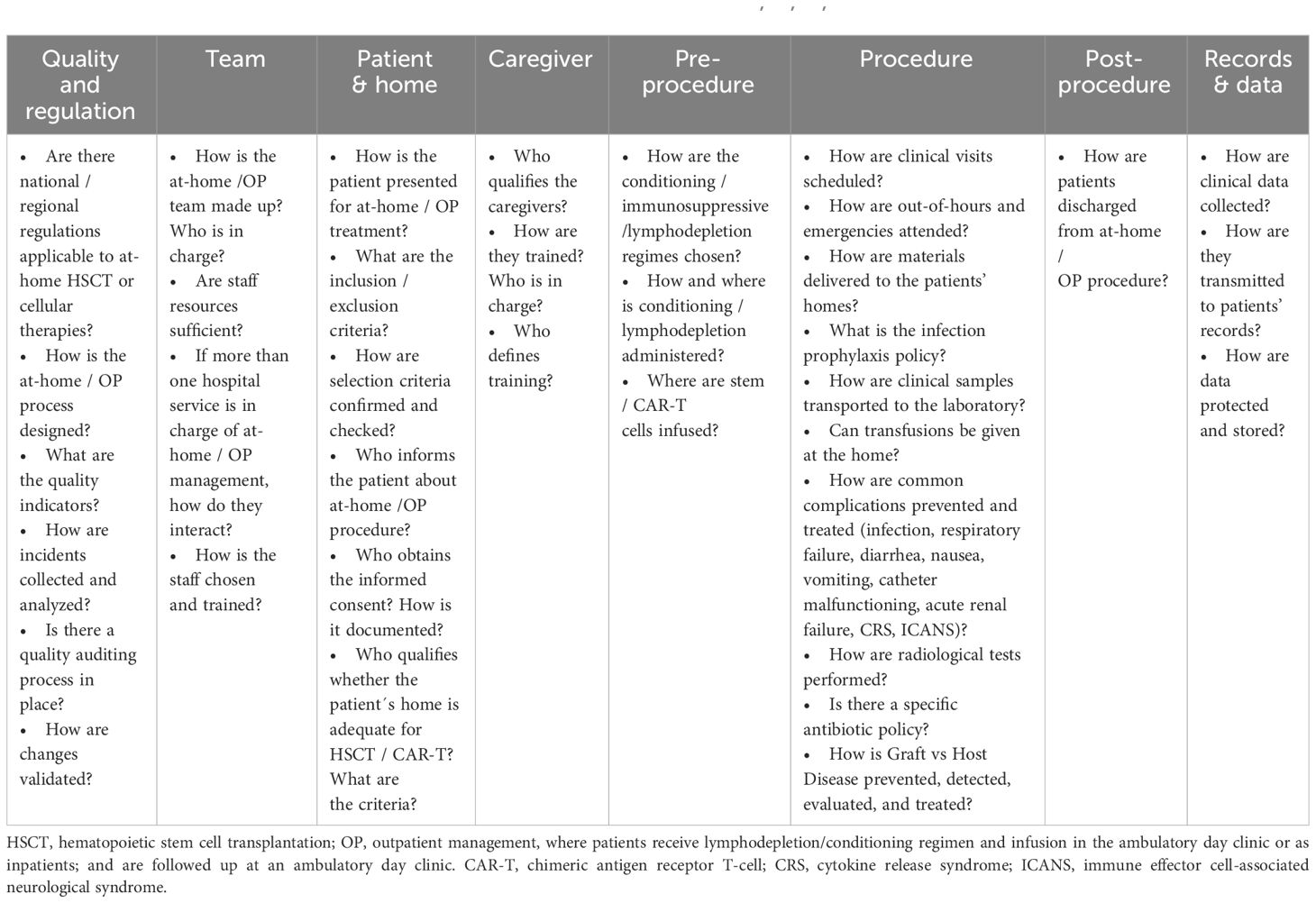
At-home/OP HSCT is a well-recognized management platform (9). Borogobac (26) defined the key components of an OP CAR-T model: create a multidisciplinary team, train nursing staff, educate community providers, increase patient knowledge and support, acquire physical space for CAR-T operations, adhere to standardized procedures and processes, review procedures, outcomes and finances. Similar considerations were made by an expert panel of the American Society of Transplantation and Cellular Therapy (28)
At-home/OP programs should define patient eligibility criteria, patient and caregiver information, and training. Appendix 4 summarizes and updates prior published provisional patient acceptance criteria for at-home/OP HSCT and CAR-T therapy programs.
A well-trained staff with on-call nurses and physicians to attend routine or emergency calls as well as an antibiotic policy adapted to the at-home/OP context and efficient transport for diagnostic samples are needed. Both routine and emergency operational scenarios must be assessed (8, 9).
Allo-HSCT presents a higher incidence of infections, including aspergillosis, and adverse events like GvHD or acute renal failure (20, 35), which should be detected and managed during the early stages. Common complications of HSCT [fever, mucositis (36, 37), GvHD, capillary leak syndrome, bleeding, diarrhea, nutrition (21)], or CAR-T (CRS, ICANS) should have defined prevention and treatment strategies, which must be planned and trained for. Decreased physical performance should be addressed with a specialized exercise program (38, 39).
Interventions (i.e., fluid therapy, transfusions, antibiotics, catheter care) should be designed to minimize clinical team visits, considering the distance of patients’ homes from the hospital. For example, the use of continuous infusion pumps (40) or self-administration could be contemplated (41). For OP CAR-T, special protocols for the early use (even while at home) of tocilizumab or dexamethasone in the treatment of complications should be implemented.
Table 2 summarizes critical issues when implementing an at-home HSCT/OP CAR-T program.
5 Frontiers for at-home HSCT and CAR-T: improving patient safety and quality of care
Emerging technologies provide means for improved patient safety monitoring, which is of special concern for at-home/OP HSCT and CAR-T therapy programs. Remarkably, many can potentially feed data to patients’ records and form networks with AI, resulting in early warning systems and better patient records, creating a continuous care ecosystem.
a. Staff and caregiver training: at-home/OP HSCT and CAR-T programs require specific and timely training for both caregivers and health staff.
i. Clinical simulation (CS) is based on creating situations replicating common daily clinical problems with mannequins or actors which allows for ‘real life’ learning. Feedback and debriefing are provided by the supervisors (42). Simulation has been used successfully to train nurses and caregivers, resulting in improved learning performances, with training verification of the learning quality (43).
ii. Virtual reality (VR) is a real-world computer simulation that produces immersive images where the user communicates with the computer via an interface. VR, less expensive than simulation, has been used to improve caregiver and staff training in different contexts. This can result not only in improved skill uptake but also in stress reduction for caregivers (44, 45).
b. Patient electronics:
i. Facial recognition technologies (FRT): Cheng showed that oxygen saturation can be measured by remote photoplethysmography using a general-purpose camera (46). Due to its sensitivity, FRT can be more sensitive than clinician judgment, creating early warning systems and enabling improved clinical decision-making.
ii. Point of care tests (POC):
1. POC tests can reduce decision times and costs, waiving the time and complexity of sample or patient transport.
2. Glucose, coagulation, and urinary tests can be performed at home, often with one drop of blood or urine. Portable, miniaturized devices and nanotechnologies can perform leukocyte count or blood grouping (47–49).
3. Furthermore, implantable cytomimetic nanomaterials can detect bacteria in saliva, forewarning the introduction of a new, less invasive generation of clinical samples (50)
iii. Wearables and remote follow-up:
1. Patients can wear several sensor-carrying devices (hearing aids, smart clothes and watches, optical displays, subcutaneous sensors, electronic footwear, etc.) (51, 52). The sensors transmit data via different communication means (smartphones, Wi-Fi, routers, 5G networks…) to the healthcare team (51), giving more detailed patient supervision.
2. Those sensors can detect early deviations in patient health data (i.e., temperature, oxygen saturation, pH, lactate, respiratory rate, blood pressure, etc.), report accidents or guide behavioral therapy and rehabilitation, which is particularly useful for supervising physical activity during the HSCT process (53).
3. Medication delivery through wearable devices coupled with a skin sensor is commonplace for diabetes (54). The use of subcutaneous micro-needles could be particularly useful for drugs with a narrow therapeutic margin, like immunosuppressors (53).
4. In conclusion, wearables show great promise in providing a continuous flow of patient data and potentially delivering medication. Low-priced wearables could allow healthcare delivery, particularly to resource-strapped areas. However, many problems need to be resolved in technical (security, connectivity, precision, battery life, etc.), regulatory (privacy, clinical trials, data use), and clinical aspects (patient, caregiver, and staff training, data interpretation) before widespread use can be implemented. Recently, Hurtado (55) found that usability was considered acceptable and vital signs (heart rate, oxygen saturation, etc.) measured via a scanwatch had medium/high adherence, while temperature recorded via manual intervention had lower compliance. Recordings of quality-of-life assessment decreased during the study, and it was concluded that adding wearable devices to a telehealth clinical platform could potentially be synergistic for HSCT and CAR-T patient monitoring. Non-complete platform automation and the absence of a dedicated telemedicine team still represent major limitations, particularly for older patients and those with low digital education.
iv. Drones: unmanned vehicles (drones) are flying devices used for automated transport. Ground drones also exist.
1. Drones have been used to carry heavy weights, including blood for transfusion (56). They can fly at high speeds, sometimes faster than ambulances (57), being unaffected by bad traffic, and in this way reduce response times in routine and emergency settings.
2. Drones could deliver clinical materials (needles, syringes, tubing…), blood components, or drugs to patients’ homes or return samples to the hospital.
3. Many hurdles, like cost, user-friendly design, weight capacity or airspace control over cities, material traceability, accident liability, etc. remain.
v. Virtual assistants (VA) or AI virtual assistants are embodied or disembodied conversational agents that allow patients to ask questions, receive information, and report their clinical evolution to a technical system in a natural language.
1. With the rise of AI, VA are gaining ground as an aid in daily clinical information tasks. VA has been used to support home care for patients (58). VA has also been used with cancer patients (59).
2. Generally, patients and caregivers accept VA, which can both reassure them and increase medication compliance. Therefore, VA could be a valuable resource by supporting clinical teams with upfront patient evaluation and information during their daily work.
3. However, validation studies are still pending, and patient participation is critical when designing and implementing such services (59).
c. Artificial intelligence:
i. AI encompasses several technologies, from performing algorithms to neural networks that mimic the human brain and allow computer systems to emulate human intelligence and “learn” as they gather data (60), without the need for programming.
ii. AI can be used to support decision-making processes in HSCT, and refine predictive models of hematological diseases (61), potentially improving patient stratification. AI has been used in the HSCT context (62) to predict survival (63) or GvHD after HSCT (64). AI has the potential to help select the suitable drugs and doses (65) or support transfusion decisions (66, 67).
iii. During the HSCT/CAR-T process, AI can also be used in early warning systems, coupled with sensors or image devices. For example, AI coupled with FRT can detect patients’ vasovagal reactions (68).
iv. Many regulatory issues still need to be overcome, and a profound understanding of data analysis is required (60), with possible bias, ethical, and privacy issues to be solved before widespread uptake.
d. As technical advances improve communications and patient care, which in turn facilitate the implementation of at-home OP treatments; more diverse, patient- and process- centered organizational models will become necessary.
6 Conclusions: “brave new world”:
a. The feasibility of at-home HSCT is well established, and, in some instances, it could improve patient outcomes (infections, GvHD, survival), with reduced mortality (8, 16, 18, 20, 22). Outpatient management has been considered the future of CAR-T (5), with several dozens of patients already managed this way. However, those are usually single-center reports, so further research, including prospective comparative trials, is required to prove the advantages of at-home/OP management over IP treatment, in clinical and economic terms.
b. Safety and clinical efficacy are critical for at-home/OP HSCT and CAR-T operations. Clinicians must establish policies addressing the specific adverse events, adapted to the constraints of at-home/OP HSCT and CAR-T. An anticipatory approach must be taken, given the possible difficulties in managing patients outside the hospital setting. To this end, emerging technologies can create an improved ecosystem for HSCT/CAR-T.
i. Before HSCT/CAR-T:
1. AI applications can help physicians improve diagnostic accuracy, patient stratification, patient selection and the tailoring of conditioning regimens and prophylactic strategies.
2. Patients, caregivers, and clinical staff can be trained with VR or CS, with a more intense schedule, adapted to the requirements of at-home/OP HSCT and CAR-T programs.
ii. During HSCT/CAR-T:
1. VAs can collect information from patients and caregivers, supporting the work of clinical care teams.
2. Wearable sensors, coupled with AI platforms, enable constant patient supervision, resulting in early warning systems for adverse events (i.e., septic shock, hypoxemia).
3. Drones or POC devices allow simpler, faster care delivery.
4. Altogether, this allows for a more flexible working schedule for clinical care teams.
c. Technical support holds significant promise for at-home/OP HSCT and CAR-T programs. Gatwood proposed telemedicine and wearables as requirements for OP CAR-T management (5). However, even if high sensitivity and specificity levels are demonstrated, many issues linger: patient and caregiver acceptability, data safekeeping, training, regulation, etc.
i. Ethical concerns (i.e., privacy vs. continued surveillance) will have to be overcome via clinical trials.
ii. Clinical teams will have to validate the devices that provide the most significant information and learn the real value of the data received and adjust responses accordingly (e.g., physicians would have to learn to react to continuous oxygen saturation variations).
d. Staff education and training for routine and emergency responses must be an integral part of at-home/OP programs. Several barriers including psychological and personal factors, training opportunities or connectivity, as well as facilitators for the incorporation of digital technologies by healthcare staff should be addressed to implement real change (69).
e. Finally, at-home/OP HSCT and CAR-T therapies could result in improved clinical results and satisfaction rates for patients and staff over conventional hospitalization. Now is the time for further research. However, we should never forget that the ultimate objective of outpatient or at-home HCST and CAR-T programs is patient’s well-being (5), and not economics. The lessons learned in this demanding context could be expanded to the standard IP environment.
Author contributions
IR: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. SG: Investigation, Writing – review & editing. CC: Conceptualization, Investigation, Writing – review & editing. EO: Investigation, Writing – review & editing. IS: Conceptualization, Investigation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank Jonathan McFarland for his invaluable help with the English version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1366962/full#supplementary-material
References
1. Gonzalez-Huelgas R, Barba R, Corbella X, García-Alegría J, Herranz MT, Vallejo I, et al. El hospital del FUTURO (2021). Available online at: https://www.fesemi.org/publicaciones/hospital-del-futuro (Accessed 2021 Apr 11).
2. Szer J. Is there no place like home for an allogeneic stem cell transplant? Bone Marrow Transplant. (2020) 55:855–6. doi: 10.1038/s41409-020-0828-2
3. Aljurf M, Weisdorf D, Hashmi S, Nassar A, Gluckman E, Mohty M, et al. Worldwide network for blood and marrow transplantation recommendations for establishing a hematopoietic stem cell transplantation program in countries with limited resources, part II: clinical, technical, and socioeconomic considerations. Vol. 25. Biol Blood Marrow Transplant. (2019) 25(12):2330–7. doi: 10.1016/j.bbmt.2019.04.012
4. Lippert M, Semmens S, Tacey L, Rent T, Defoe K, Bucsis M, et al. The hospital at home program: No place like home. Curr Oncol. (2017) 24:23–7. doi: 10.3747/co.24.3326
5. Gatwood KS, Dholaria BR, Lucena M, Baer B, Savani BN, Oluwole OO. Chimeric antigen receptor T-cell therapy: Challenges and framework of outpatient administration. EJHaem. (2022) 3:54–60. doi: 10.1002/jha2.333
6. Martínez-Roca A, Rodríguez-Lobato LG, Ballestar N, Gallego C, Fernández-Avilés F. Personalized at-home autologous hematopoietic stem cell transplantation during the SARS-CoV-2 outbreak. Leuk Res. (2021) 106:106589. doi: 10.1016/j.leukres.2021.106589
7. Jagannath S, Vesole DH, Zhang M, Desikan KR, Copeland N, Jagannath M, et al. Feasibility and cost-effectiveness of outpatient autotransplants in multiple myeloma. Bone Marrow Transplant. (1997) 20:6. doi: 10.1038/sj.bmt.1700900
8. González MJ, Urizar E, Urtaran-Laresgoiti M, Nuño-Solinís R, Lázaro-Pérez E, Vázquez L, et al. Hospital and outpatient models for Hematopoietic Stem Cell Transplantation: A systematic review of comparative studies for health outcomes, experience of care and costs. PloS One. (2021) 16:1–15. doi: 10.1371/journal.pone.0254135
9. Fernandez - Avilés F, Gutiérrez - García G. t-home HSCT. In: Carreras E, Dofour C, Mothy M, Kröger N, editors. Hematopoietic stem cell transplantation and cellular therapies the EBMT handbook, 7 th. Spinger, Cham, Switherland (2019). p. 467–71.
10. Holbro A, Ahmad I, Cohen S, Roy J, Lachance S, Chagnon M, et al. Safety and cost-effectiveness of outpatient autologous stem cell transplantation in patients with multiple myeloma. Biol Blood Marrow Transplantation. (2013) 19:547–51. doi: 10.1016/j.bbmt.2012.12.006
11. McDiarmid SD, Hutton B, Atkins H, Bence-Bruckler I, Bredeson C, Sabri E, et al. Performing allogeneic and autologous hematopoietic SCT in the outpatient setting: Effects on infectious complications and early transplant outcomes. Bone Marrow Transplant. (2010) 45:1220–6. doi: 10.1038/bmt.2009.330
12. Granot N, Storer BE, Cooper JP, Flowers ME, Sandmaier BM, Storb R. Allogeneic hematopoietic cell transplantation in the outpatient setting. Biol Blood Marrow Transplantation. (2019) 25:2152–9. doi: 10.1016/j.bbmt.2019.06.025
13. Singhal S, Saadeh SS, Durani U, Kansagra A, Alkhateeb HB, Shah MV, et al. Allogeneic hematopoietic stem cell transplantation in the outpatient setting: the mayo clinic experience. Transplant Cell Ther. (2023) 29(3):183.e1–6. doi: 10.1016/j.jtct.2022.12.016
14. Ruiz-Argüelles GJ, Seber A, Ruiz-Delgado GJ. Conducting hematopoietic stem cell transplantation in low and middle income countries. Hematol (United Kingdom). (2022) 27:809–12. doi: 10.1080/16078454.2022.2105513
15. Abigail Montes-Robles M, Manuel Gallardo-Pérez M, Hernández-Flores EJ, de Lourdes Pastelín-Martínez M, Sánchez-Bonilla D, Robles-Nasta M, et al. In persons with CIDP, auto-HSCT can be conducted fully on an outpatient basis and induces significant clinical responses: A prospective study in a single center. Transpl Immunol. (2023) 81:101944. doi: 10.1016/j.trim.2023.101944
16. Rives S, Carreras E, Rovira M, Montoto S, Urbano-Ispizua Á, Martínez C, et al. Trasplante autogénico de progenitores hemopoyéticos en régimen ambulatorio: Análisis de viabilidad en el Hospital Clínic de Barcelona. Med Clin (Barc). (1999) 113(6):201–4.
17. Fernández-Avilés F, Carreras E, Urbano-Ispizua A, Rovira M, Martínez C, Gaya A, et al. Case-control comparison of at-home to total hospital care for autologous stem-cell transplantation for hematologic Malignancies. J Clin Oncol. (2006) 24:4855–61. doi: 10.1200/JCO.2006.06.4238
18. González-Barrera S, Martín-Sánchez G, Parra-Jordán JJ, Fernández-Luis S, Calvo JA, Lobeira R, et al. Feasibility of a hospital-at-home program for autologous hematopoietic stem cell transplantation. Transplant Cell Ther. (2023) 29(2):111.e1–7. doi: 10.1016/j.jtct.2022.11.018
19. Sung AD, Giri VK, Tang H, Nichols KR, Lew MV, Bohannon L, et al. Home-based hematopoietic cell transplantation in the United States. Transplant Cell Ther. (2022) 28:207.e1–8. doi: 10.1016/j.jtct.2022.01.015
20. Svahn BM, Ringdén O, Remberger M. Long-term follow-up of patients treated at home during the pancytopenic phase after allogeneic haematopoietic stem cell transplantation. Bone Marrow Transplant. (2005) 36:511–6. doi: 10.1038/sj.bmt.1705096
21. Svahn BM, Remberger M, Heijbel M, Martell E, Wikström M, Eriksson B, et al. Case-control comparison of at-home and hospital care for allogeneic hematopoietic stem-cell transplantation: The role of oral nutrition. Transplantation. (2008) 85:1000–7. doi: 10.1097/TP.0b013e31816a3267
22. Ringdén O, Remberger M, Törlén J, Engström M, Fjaertoft G, Mattsson J, et al. Home care during neutropenia after allogeneic hematopoietic stem cell transplantation in children and adolescents is safe and may be more advantageous than isolation in hospital. Pediatr Transplant. (2014) 18:398–404. doi: 10.1111/petr.12262
23. Bergkvist K, Larsen J, Johansson UB, Mattsson J, Svahn BM. Hospital care or home care after allogeneic hematopoietic stem cell transplantation – Patients’ experiences of care and support(2013) (Accessed 2023 Sep 21). doi: 10.1016/j.ejon.2012.12.004
24. Jenkelowitz J, Garzon MG, Lynch K, Shuk E, Feindler E, Landau H, et al. Exploring the caregiver’s experience in an innovative homebound hematopoietic stem cell transplantation program. Palliat Support Care. (2021) 19:397–404. doi: 10.1017/S1478951520000954
25. McGann M, Davis JA, Gaffney KJ, Smith D, Edwards K, Hess BT, et al. Real-world experience and optimization of outpatient chimeric antigen receptor T cell therapy. Transplant Cell Ther. (2022) 28:583–5. doi: 10.1016/j.jtct.2022.06.021
26. Borogovac A, Keruakous A, Bycko M, Holter Chakrabarty J, Ibrahimi S, Khawandanah M, et al. Safety and feasibility of outpatient chimeric antigen receptor (CAR) T-cell therapy: experience from a tertiary care center. Vol. 57 Bone Marrow Transplantation. Springer Nature;. (2022) 57(6):1025–7. doi: 10.1038/s41409-022-01664-z
27. Alexander M, Culos K, Roddy J, Shaw JR, Bachmeier C, Shigle TL, et al. Chimeric antigen receptor T cell therapy: A comprehensive review of clinical efficacy, toxicity, and best practices for outpatient administration. Transplant Cell Ther. (2021) 27:558–70. doi: 10.1016/j.jtct.2021.01.014
28. Oluwole OO, Dholaria B, Knight TE, Jain T, Locke FL, Ramsdell L, et al. Chimeric antigen receptor T-cell therapy in the outpatient setting: an expert panel opinion from the american society for transplantation and cellular therapy. Transplant Cell Ther. (2023) 10(2):131–42. doi: 10.1016/j.jtct.2023.11.008
29. Myers GD, Verneris MR, Goy A, Maziarz RT. Perspectives on outpatient administration of CAR-T cell therapy in aggressive B-cell lymphoma and acute lymphoblastic leukemia. Vol. 9. J Immunother Cancer. (2021) 9(4):e002056. doi: 10.1136/jitc-2020-002056
30. Paludo J, Bansal R, Hathcock M, Pritchett JC, De Menezes Silva Corraes A, Oyarzabal BA, et al. Healthcare utilization outcomes of outpatient CAR-T cell therapy with remote patient monitoring program. Blood. (2023) 142:5075–5. doi: 10.1182/blood-2023-187834
31. Bansal R, Paludo J, Hathcock MA, Spychalla MT, Khurana A, Hampel PJ, et al. Outpatient practice pattern for recently approved CAR-T in patients with lymphoma and multiple myeloma. Blood. (2022) 140:2399–401. doi: 10.1182/blood-2022-167187
32. Dwivedy Nasta S, Namoglu EC, Hughes ME, Chong EA, Svoboda J, Ballard HJ, et al. Hospitalization patterns with commercial CAR T-cell therapy: A single institution experience. Blood. (2019) 134:3240–0. doi: 10.1182/blood-2019-130650
33. Shao YF, Modi D, Kin A, Alavi A, Ayash L, Ratanatharathorn V, et al. Feasibility of outpatient CAR T cell therapy: experience of a single institution. Blood. (2021) Supplement 1):4828–8. doi: 10.1182/blood-2021-146283
34. Bachier CR, Palomba ML, Abramson JS, Andreadis C, Sehgal A, Godwin J, et al. Outpatient treatment with lisocabtagene maraleucel (liso-cel) in 3 ongoing clinical studies in relapsed/refractory (R/R) large B cell non-hodgkin lymphoma (NHL), including second-line transplant noneligible (TNE) patients: transcend NHL 001, outreach, and PILOT. Biol Blood Marrow Transplantation. (2020) 26:S25–6. doi: 10.1016/j.bbmt.2019.12.093
35. Gutiérrez-García G, Rovira M, Arab N, Gallego C, Sánchez J, Ángeles Álvarez M, et al. A reproducible and safe at-home allogeneic haematopoietic cell transplant program: first experience in Central and Southern Europe. Bone Marrow Transplant. (2020) 55:965–73. doi: 10.1038/s41409-019-0768-x
36. Rodríguez-Lobato LG, Martínez-Roca A, Moreno DF, Gutiérrez-García G, Suárez-Lledó M, Rovira M, et al. Impact of intensifying primary antibiotic prophylaxis in at-home autologous stem cell transplantation program for lymphoma patients(2020) (Accessed 2023 Aug 25). doi: 10.1080/10428194.2020.1742901
37. Martínez-Cibrian N, Magnano L, Gutiérrez-García G, Andrade X, Correa JG, Suárez-Lledó M, et al. At-home autologous stem cell transplantation in multiple myeloma with and without G-CSF administration: a comparative study(2016) (Accessed 2023 Aug 25).
38. Abo S, Ritchie D, Denehy L, Panek-Hudson Y, Irving L, Granger CL. A hospital and home-based exercise program to address functional decline in people following allogeneic stem cell transplantation(2018) (Accessed 2023 Aug 25).
39. Yildiz Kabak V, Goker H, Duger T. Effects of partly supervised and home-based exercise program in patients undergoing hematopoietic stem cell transplantation: a case-control study. Supportive Care Cancer. (2020) 28:5851–60. doi: 10.1007/s00520-020-05432-x
40. García-Queiruga M, Feal Cortizas B, Lamelo Alfonsín F, Pertega Diaz S, Martín-Herranz I. Continuous infusion of antibiotics using elastomeric pumps in the hospital at home setting. Rev Esp Quimioter. (2021) 34(3):200–6. doi: 10.37201/req/122.2020
41. Tonna A, Anthony G, Tonna I, Paudyal V, Forbes-Mckay K, Laing R, et al. Home self-administration of intravenous antibiotics as part of an outpatient parenteral antibiotic therapy service: A qualitative study of the perspectives of patients who do not self-administer. Vol. 9. BMJ Open. (2019) 9(1):e027475. doi: 10.1136/bmjopen-2018-027475
42. Kim J, Park JH, Shin S. Effectiveness of simulation-based nursing eucation depending on fidelity: A meta analysis. BMC Med Educ. (2016) 16:152. doi: 10.1186/s12909-016-0672-7
43. Saleem M, Khan Z. Healthcare Simulation: An effective way of learning in health care. Pak J Med Sci. (2023) 39(4):1185–90. doi: 10.12669/pjms.39.4.7145
44. Pottle J. Virtual reality and the transformation of medical education. Future Healthc J. (2019) 6:181–6. doi: 10.7861/fhj.2019-0036
45. Samadbeik M, Yaaghobi D, Bastani PV, Abhari S, Rezaee R, Garavand A. The applica-tions of virtual reality tech-nology in medical groups teaching. J Adv Med Educ Prof. (2018) 6(3):123–9.
46. Cheng JC, Pan TS, Hsiao WC, Lin WH, Liu YL, Su TJ, et al. Using contactless facial image recognition technology to detect blood oxygen saturation. Bioengineering. (2023) 10:1–15. doi: 10.3390/bioengineering10050524
47. Zhang W, Li Y, Chen B, Zhang Y, Du Z, Xiang F, et al. Fully integrated point-of-care blood cell count using multi-frame morphology analysis. Biosens Bioelectron [Internet]. (2023) 223:115012. doi: 10.1016/j.bios.2022.115012
48. Kim P, Ong E, Li KH, Yoon YJ, Ng SH, Puttachat K. Low-cost, disposable microfluidics device for blood plasma extraction using continuously alternating paramagnetic and diamagnetic capture modes. Biomicrofluidics. (2016) 10:024110. doi: 10.1063/1.4944587
49. Karimi S, Mehrdel P, Farré-Lladós J, Casals-Terré J. A passive portabl microfluidic blood-plasma separator for simultaneous determination of direct and indirect ABO/Rh blood typing. Lab Chip. (2019) 19:3249–60. doi: 10.1039/C9LC00690G
50. Ho D, Fung AO, Montemagno CD. Engineering novel diagnostic modalities and implantabl cytomimetic nanomaterials for next-generation medicine. Biol Blood Marrow Transplant. (2006) 12:92–9. doi: 10.1016/j.bbmt.2005.09.013
51. Yetisen AK, Martinez-Hurtado JL, Ünal B, Khademhosseini A, Butt H. Wearables in medicine. Advanced Materials. (2018) 30:2449–9. doi: 10.1002/adma.201706910
52. Dunn J, Runge R, Snyder M. Wearables and the medical revolution. Per Med. (2018) 15:429–48. doi: 10.2217/pme-2018-0044
53. Lee MA, Song MK, Bessette H, Roberts Davis M, Tyner TE, Reid A. Use of wearables for monitoring cardiometabolic health: A systematic review. Int J Med Inform. (2023) 179:105218. doi: 10.1016/j.ijmedinf.2023.105218
54. Hughes MS, Addala A, Buckingham B, riend SH, Ginsburg GS, Picard RW, et al. Digital technology for diabetes. New Engl J Med. (2023) 389:2076–86. doi: 10.1056/NEJMra2215899
55. Hurtado L, Gonzalez Concepcion M, Flix-Valle A, Ruiz-Romeo M, Gonzalez-Rodriguez S, Peña M, et al. Telemedicine-enabled care and wearable technologies in hematopoietic cell transplantation and CAR T-cell therapy patients: A prospective pilot study (TEL-HEMATO study). JMIR Formative Research. (2024), 55918. doi: 10.2196/preprints.55918
56. Ling G, Draghic N. Aerial drones for blood delivery. Transfusion. (2019) 59:1608–11. doi: 10.1111/trf.15195
57. Konert A, Smereka J, Szarpak L. The use of drones in emergency medicine: practical and legal aspects. Emerg Med Int. (2019) 2019:1–5. doi: 10.1155/2019/3589792
58. Corbett CF, Combs EM, Wright PJ, Owens OL, Stringfellow I, Nguyen T, et al. Virtual home assistant use and perceptions of usefulness by older adults and support person dyads. Int J Environ Res Public Health. (2021) 18:1–13. doi: 10.3390/ijerph18031113
59. van Bussel MJP, Odekerken–Schröder GJ, Ou C, Swart RR, Jacobs MJG. Analyzing the determinants to accept a virtual assistant and use cases among cancer patients: a mixed methods study. BMC Health Serv Res. (2022) 22(1):890. doi: 10.1186/s12913-022-08189-7
60. Secinaro S, Calandra D, Secinaro A, Muthurangu V, Biancone P. The role of artificial intelligence in healthcare : a structured literature review. BMC Med Inform Decis Mak. (2021) 21(1):1–23. doi: 10.1186/s12911-021-01488-9
61. Muhsen IN, Elhassan T, Hashmi SK. Artificial Intelligence approaches in hematopoietic cell transplant: A review of the current status and future directions. Turk J Haematol. (2018) 35(3):152–7. doi: 10.4274/tjh
62. Gupta V, Braun TM, Chowdhury M, Tewari M, Choi SW. A systematic review of machine learning techniques in hematopoietic stem cell transplantation (HSCT). Sensors. (2020) 20:6100. doi: 10.3390/s20216100
63. Shourabizadeh H, Aleman DM, Rousseau LM, Law AD, Viswabandya A, Michelis FV. Machine learning for the prediction of survival post-allogeneic hematopoietic cell transplantation: A single-center experience. Acta Haematol [Internet]. (2023), 1–12. doi: 10.1159/000533665
64. Jo T, Arai Y, Kanda J, Kondo T, Ikegame K, Uchida N, et al. A convolutional neural network-based model that predicts acute graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Commun Med. (2023) 3:1–11. doi: 10.1038/s43856-023-00299-5
65. Ho D, Quake SR, McCabe ERB, Chng WJ, Chow EK, Ding X, et al. Enabling technologies for personalized and precision medicine. Trends Biotechnol. (2020) 38:497–518. doi: 10.1016/j.tibtech.2019.12.021
66. Engelke M, Schmidt CS, Baldini G, Parmar V, Hosch R, Borys K, et al. Optimizing platelet transfusion through a personalized deep learning risk assessment system for demand management. Blood. (2023) 142:2315–26. doi: 10.1182/blood.2023021172
67. Maynard S, Farrington J, Alimam S, Evans H, Li K, Wong WK, et al. Machine learning in transfusion medicine: A scoping review. Transfusion. (2024) 64:162–84. doi: 10.1111/trf.17582
68. Rudokaite J, Ong LLS, Janssen MP, Postma E, Huis in ’t Veld E. Predicting vasovagal reactions to a virtual blood donation using facial image analysis. Transfusion. (2022) 62:838–47. doi: 10.1111/trf.16832
Keywords: stem cell transplantation, hospital at-home, outpatient, safety, training, drones, wearables, artificial intelligence
Citation: Romon I, Gonzalez-Barrera S, Coello de Portugal C, Ocio E and Sampedro I (2024) Brave new world: expanding home care in stem cell transplantation and advanced therapies with new technologies. Front. Immunol. 15:1366962. doi: 10.3389/fimmu.2024.1366962
Received: 07 January 2024; Accepted: 12 April 2024;
Published: 26 April 2024.
Edited by:
Marta Garcia-Recio, Hospital Clinic of Barcelona, SpainReviewed by:
Alberto Mussetti, Catalan Institute of Oncology, SpainCopyright © 2024 Romon, Gonzalez-Barrera, Coello de Portugal, Ocio and Sampedro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iñigo Romón, am9zZWluaWdvLnJvbW9uQHNjc2FsdWQuZXM=