 Maria Inmaculada Dominguez-Mozo1
Maria Inmaculada Dominguez-Mozo1 Victoria Galán2
Victoria Galán2 Lluís Ramió-Torrentà3Ana Quiroga4
Lluís Ramió-Torrentà3Ana Quiroga4 E. Quintana5
E. Quintana5 Luisa María Villar6
Luisa María Villar6 Lucienne Costa-Frossard7
Lucienne Costa-Frossard7 José Ignacio Fernández-Velasco6
José Ignacio Fernández-Velasco6 Noelia Villarrubia6
Noelia Villarrubia6 María Angel Garcia-Martinez1
María Angel Garcia-Martinez1 Rafael Arroyo8
Rafael Arroyo8 Roberto Alvarez-Lafuente1*
Roberto Alvarez-Lafuente1*- 1Grupo de Investigación de Factores Ambientales en Enfermedades Degenerativas, Instituto de Investigación Sanitaria del Hospital Clínico San Carlos (IdISSC), Red de Enfermedades Inflamatorias (REI), Madrid, Spain
- 2Servicio de Neurología, Hospital Universitario de Toledo, Toledo, Spain
- 3Neuroimmunology and Multiple Sclerosis Unit, Girona Biomedical Research Institute (IDIBGI), Doctor Josep Trueta University Hospital and Santa Caterina Hospital, Department of Medical Sciences, University of Girona, Red de Enfermedades Inflamatorias (REI), Girona, Spain
- 4Neuroimmunology and Multiple Sclerosis Unit (UNIEM), Girona Biomedical Research Institute (IDIBGI), Red de Enfermedades Inflamatorias (REI), Girona, Spain
- 5Girona Neuroimmunology and Multiple Sclerosis Unit (UNIEM), Girona Biomedical Research Institute (IDIBGI), Department of Medical Sciences, University of Girona, Girona, Spain
- 6Servicio de Inmunología, Hospital Universitario Ramón y Cajal, Red de Enfermedades Inflamatorias (REI), Madrid, Spain
- 7Servicio de Neurología, Hospital Universitario Ramón y Cajal, Red de Enfermedades Inflamatorias (REI), Madrid, Spain
- 8Departamento de Neurología, Hospital Universitario Quironsalud Madrid, Red Española de Esclerosis Múltiple (REEM), Madrid, Spain
Background: Although fingolimod, a sphingosine 1-phosphate receptor agonist, has shown to be an effective treatment reducing relapse rate and also slowing down the disability progression in relapsing-remitting multiple sclerosis (RRMS) patients, it is important to quickly identify those suboptimal responders.
Objective: The main objective was to assess different clinical, radiological, genetic and environmental factors as possible early predictors of response in MS patients treated with fingolimod for 24 months. The secondary objective was to analyze the possible contribution of the environmental factors analyzed to the progression and activity of the disease along the 2-years of follow-up.
Methods: A retrospective study with 151 patients diagnosed with MS, under fingolimod treatment for 24 months, with serum samples at initiation and six months later, and with clinical and radiological data at initiation and 24 months later, were included in the study. Clinical and radiological variables were collected to establish NEDA-3 (no evidence of disease activity: patients without relapses, disability progression and new T2 lesions or Gd+ lesions) and EDA (evidence of disease activity: patients with relapses and/or progression and/or new T2 lesions or gadolinium-positive [Gd+] lesions) conditions. Human leukocyte antigen II (HLA-II), EBNA-1 IgG and VCA IgG from Epstein-Barr virus (EBV) and antibody titers against Human herpesvirus 6A/B (HHV-6A/B) were also analyzed.
Results: A total of 151 MS patients fulfilled the inclusion criteria: 27.8% was NEDA-3 (37.5% among those previously treated with high efficacy therapies >24 months). The following early predictors were statistically significantly associated with NEDA-3 condition: sex (male; p=0.002), age at baseline (older; p=0.009), relapses 2-years before fingolimod initiation ≤1 (p=0.010), and absence of Gd+ lesions at baseline (p=0.006). Regarding the possible contribution of the environmental factors included in the study to the activity or the progression of the disease, we only found that EBNA-1 IgG titers decreased in 20.0% of PIRA (progression independent from relapse activity) patients vs. 73.3% of RAW (relapse-associated worsening) patients (p=0.006; O.R. = 11.0).
Conclusion: MS patients that are male, older, and with a low clinical and radiological activity at fingolimod initiation have a greater probability to reach NEDA-3 condition after two years with this therapy. An intriguing association of EBV with the progression of the disease has also been described, but it should be further study in a larger cohort to confirm these results.
1 Introduction
Fingolimod is a sphingosine 1-phosphate (S1P) receptor agonist that significantly reduces disease activity in relapsing-remitting multiple sclerosis (RRMS) patients (1). This oral immune‐modulatory treatment embodies and degrades the sphingosine‐1‐phosphate (S1P) receptor on leukocytes, inhibiting the egress of lymphocytes from lymph nodes. Therefore, this therapy is able to reduce the migration of potential inflammatory cells to the central nervous system; as a consequence, patients under fingolimod treatment present peripheral blood lymphopenia due to the redistribution of leukocytes (2). Although the U.S. Food and Drug Administration (FDA) approved this treatment for RRMS patients, its use in Europe was restricted to highly active RRMS patients or as escalation after failure to first‐line disease modifying therapies (DMT) (3). In the FREEDOMS I study, the 70.4% of MS patients treated with the 0.5mg dose, was free of relapses after 24 months of follow-up (1); these results were very similar to those of the FREEDOMS II performed later: 71.5% (4). Regarding real-world studies, results are similar to those obtained in the clinical trials or even better when the percentage of relapse-free patients is analyzed, after two years of fingolimod treatment: 81.9% of 286 Turkish MS patients (5), 77.4% of 78 Italian MS patients (6), 74.6% of 167 Spanish MS patients (7). Therefore, although fingolimod has shown to be an effective treatment reducing relapse rate and also slowing down the disability progression, it is important to quickly identify those suboptimal responders.
With this aim, we performed a retrospective study analyzing different clinical, radiological, genetic and environmental factors as possible early predictors of response in MS patients treated with fingolimod along 24 months. Some clinical factors have been previously related to fingolimod response as early predictors (8, 9). Regarding genetic factors, they have been searched before in relation to the response to the different DMTs in MS. Pharmacogenomic studies have shown that the human leukocyte antigen (HLA) could help to better identify appropriated candidates to each treatment (10, 11), although in other occasions not (12, 13). In fact, a recent paper published in pediatric and adolescent MS patients treated with fingolimod identified different haplotypes that showed a trend towards a more favorable clinical course (14). Finally, viruses have been proposed as possible biomarkers of response to different DMTs (15, 16). Viruses like Human herpesvirus 6 (HHV-6) or Epstein-Barr virus (EBV) have been proposed to be actively involved in processes like the activity (17) or the progression of the disease (18, 19), and therefore, modifications in their antibody levels or in their viral load along the treatment could be identified in relation with these processes. The main objective of this study was to assess all of them, in the same cohort of MS patients treated with fingolimod, in relation to the clinical and radiological response comparing NEDA-3 (no evidence of disease activity: patients without relapses, disability progression and new T2 lesions or Gd+ lesions) and EDA (evidence of disease activity: patients with relapses and/or progression and/or new T2 lesions or Gd+ lesions) patients. The secondary objective was to analyze the possible contribution of the environmental factors analyzed to the progression and activity of the disease along the 2-years of follow-up. Furthermore, in the last years, different S1P receptor agonists have been approved for the treatment of MS patients (20–22). Thus, the results obtained with fingolimod could be of interest for them, since they largely share the same mechanism of action.
2 Methods
2.1 Design
This is a retrospective study with the following inclusion criteria: 1) MS patients diagnosed by Poser, 2010 or 2017 McDonald criteria (23–25); 2) under fingolimod treatment for 24 months; 3) with serum samples collected within a month before starting fingolimod treatment and six months after the first dose; 4) with the following clinical and radiological data at initiation and 24 months later: Expanded disability status scale (EDSS) score, number of relapses, T2 lesions and gadolinium-positive (Gd+) lesions at initiation, and one and two years later.
2.2 Patients
Patients were recruited from the following hospitals: Hospital Clínico San Carlos (Madrid), Hospital Universitario Doctor Josep Trueta (Gerona) and Hospital Universitario Ramón y Cajal (Madrid). The clinical and radiological data were collected by neurologists and radiologists belonging to the Multiple Sclerosis Units of these hospitals.
2.3 Ethics statement
This study was approved by the local Ethic Committee of the Hospital Clínico San Carlos (Comité Ético de Investigación Clínica del Hospital Clínico San Carlos). All the patients recruited received and signed a written informed consent. All experiments were performed in accordance with relevant guidelines and regulations.
2.4 Response criteria
According to the pre-treatment EDSS score, we defined the progression as the following increases after 24 months of fingolimod treatment: 1) EDSS=0: ≥1.5 points; 2) EDSS ≥1 and ≤5: ≥1 point; 3) EDSS ≥5.5: ≥0.5 points. We also analyzed two different variables related to the progression: RAW (relapse-associated worsening: patients with progression and with at least one relapse during the two years of follow-up under fingolimod treatment) and PIRA (progression independent from relapse activity: patients with progression and without relapses during the two years of follow-up under fingolimod treatment). Although they are non-mutually exclusive drivers for long-term disability, we considered PIRA and RAW as two competing outcomes (26). Relapses were defined as a worsening of neurological impairment or an appearance of a new symptom or abnormality attributable to MS; they lasted at least 24 hours and they were preceded by stability period of at least 1 month. Regarding magnetic resonance imaging (MRI), it was performed one month prior fingolimod treatment onset and 1 and 2 years after starting this therapy in 1.5T scanners; a previous published protocol was followed (27). The sequences collected for this study were; axial fluid-attenuated inversion recovery (FLAIR) T2, axial proton density T2-weighted imaging, axial T2-weighted imaging, and T1-weighted imaging with gadolinium (Gd) enhancement. With previous definitions, these were the response criteria: clinical response (absence of disability progression and relapses), NEDA-3 (no evidence of disease activity: patients without relapses, disability progression and new T2 lesions or Gd+ lesions), and EDA (evidence of disease activity: patients with relapses and/or progression and/or new T2 lesions or Gd+ lesions).
2.5 Researched variables
The following variables were analyzed: 1) Clinical: sex, age at recruitment, age at disease onset, disease duration, number of relapses two years before the recruitment, EDSS score at treatment initiation and previous treatments. Therapies were classified as: moderate efficacy treatments (MET: beta-interferon, glatiramer acetate, dimethyl fumarate and teriflunomide) and high efficacy treatments (HET: natalizumab, mitoxantrone, azathioprine) 2) Radiological: T2 and Gd+ lesions at recruitment and after one and two years of fingolimod treatment. 3) Genetic: HLA-II. 4) Viral: antibody responses to EBV (EBNA-1 IgG and VCA IgG) and HHV-6 IgG and IgM antibody titers at fingolimod initiation; based on previous published results of our group we also analyzed the change in the antibody titers between the baseline and the six month sample (15, 17).
2.6 DNA extraction
DNA spin column technique of QIAamp DNA Blood Mini Kit (QIAGEN. Hilden. Germany) was used to isolate total DNA from 0.2 ml of blood, following the manufacturer’s instructions.
2.7 HLA genotyping
The genotyping of the alleles belonging to HLA class II (DR, DQA and DQB) was carried out using the rSSO-PCR technique (sequence-specific oligonucleotide reverse PCR). LABType™ One Lambda kits (Thermo Fisher Scientific, Waltham, MA, USA) were used following the manufacturer’s instructions. The detection was carried out on a FLEXMAP 3D™ device (Luminex Corporation, Austin, TX, USA), whose detection is based on Luminex™ technology.
2.8 ELISA
Commercial tests for the detection of EBNA-1 and VCA IgG (Trinity Biotech, USA) and HHV-6A/B IgG and IgM (Vidia, Ltd., Czech Republic) were used in an automated ELISA processing system (DS2, Dynex Technologies, USA), following the manufacturer’s instructions. Results were expressed in artificial units (AU): index value * 10 (index value = sample absorbance/cut-off value) (15, 17). Each sample was analyzed in duplicate for each test. Doubtful samples (between 9 and 11 AU) were tested again; they were considered negative samples if they remained under 11 AU at the new analysis.
2.9 Statistical analysis
To test differences in categorical variables we used the chi-square or two-tailed Fisher’s exact test. To analyze differences in continuous variables the Kruskall-Wallis test or the Wilcoxon rank-sum test were used. Association between clinical, radiological, genetic and environmental factors as possible early predictors and clinical outcomes (activity and/or progression of the disease), alone or in combination (NEDA-3/EDA) was studied with a non-parametric test (U Mann-Whitney). Bonferroni correction was performed when multiple comparisons were made. P-values <0.05 were considered as statistically significant. All statistical analysis were performed using Statistical Package for Social Sciences, version 15.0 (IBM SPSS, Inc, Chicago, IL, USA).
3 Results
3.1 Patients recruited for the study and demographic characteristics of the population study
A total of 151 MS patients fulfilled all the inclusion criteria of the study. Their characteristics are shown in Table 1.

Table 1 Demographical characteristics of the patients included in the study at the onset of fingolimod treatment.
3.2 Clinical and radiological response after two years of fingolimod treatment
The 34.4% (52/151) of MS patients suffered relapses after two years of fingolimod treatment vs. 67.5% (102/151) two years prior to fingolimod onset (49% of reduction). The 19.9% (30/151) of MS patients experienced progression according to the progression criteria above mentioned: 50% of them were PIRA (15/30) and 50% were RAW (15/30). Regarding the MRI studies, the 38.4% (58/151) of patients had new T2 lesions after 24-months of fingolimod treatment; the 21.2% (32/151) had Gd+ lesions at 12-month and/or 24-month MRI. According to our response criteria, the 55% (83/151) could be considered as clinical responders and the 27.8% (42/151) as NEDA-3 after two years of fingolimod treatment.
3.3 Early clinical and radiological variables
When we compared MS patients with NEDA-3 vs. those with EDA, the following early predictors were statistical significantly associated with NEDA-3 condition (Figure 1): sex (male; p=0.002), age at baseline (older; p=0.009), relapses 2-years before fingolimod initiation ≤1 (p=0.010), and absence of Gd+ lesions at baseline (p=0.006). Thus, the 71.4% of those MS patients with these four early predictors were NEDA-3 vs. the 6.7% among those MS patients without any of them. Since most of the MS patients had been previously treated (Table 1), we analyzed their possible relation with the number of relapses two years before and with the number of Gd+ lesions at fingolimod initiation. We found statistically significant differences when we compared MS patients treated with MET and HET for more than 24 months (Table 2): a higher proportion of MS patients previously treated with HET had ≤1 relapses 2-years before (p=0.003; O.R. = 5.3) and no Gd+ lesions (p=<0.0001; O.R. = 12.3) at fingolimod initiation. However, when we analyzed the effect of MET and HET treatments prior to fingolimod initiation on NEDA-3 condition, we did not find any statistically significant difference (Table 3).
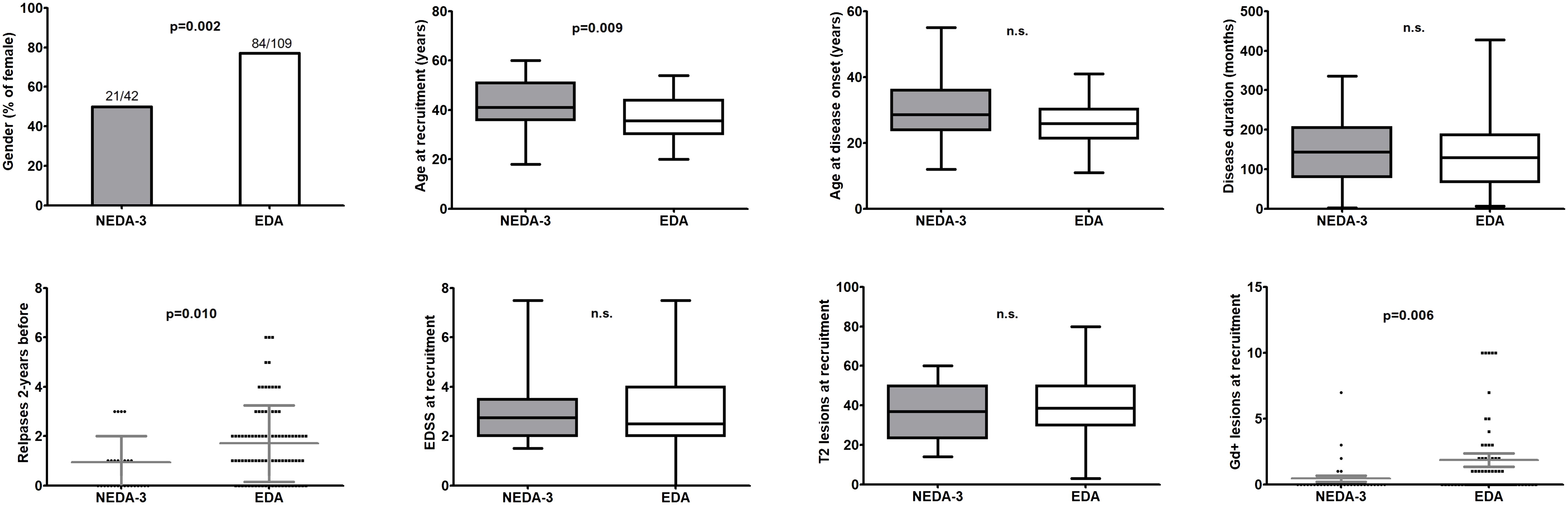
Figure 1 Comparison of clinical and radiological variables between NEDA-3 and EDA patients at recruitment (p values were calculated from Chi-square test/Fisher’s exact test for categorical variables and with the Kruskall-Wallis test for the continuous variables). Lines inside the graphs shows the mean value. (GraphPad Prism 5.0) n.s., not significant.
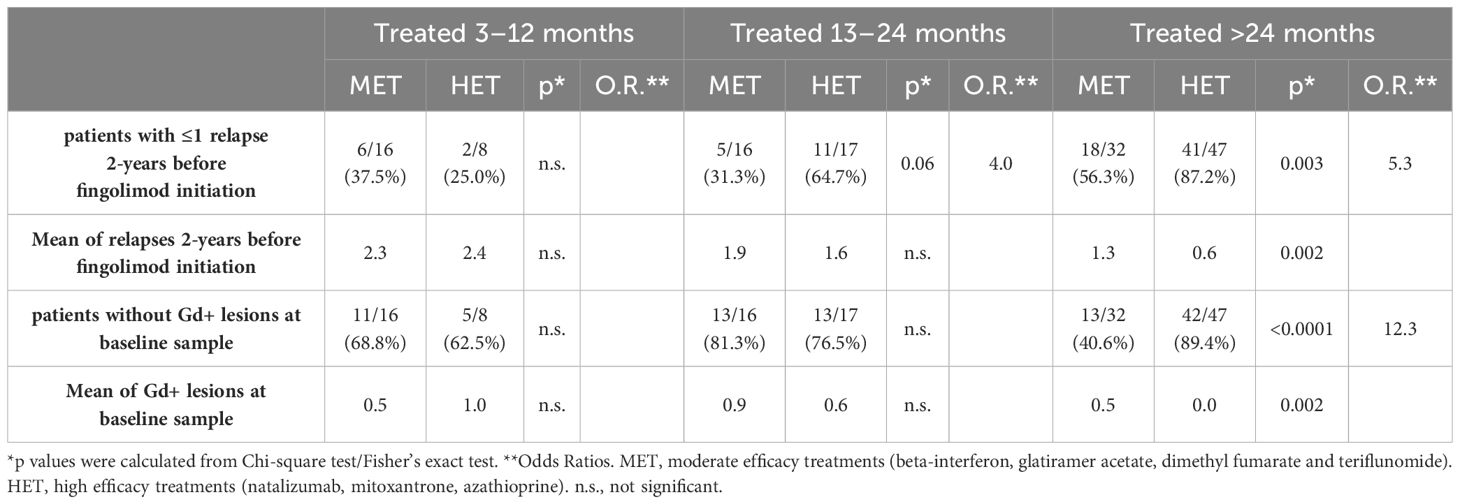
Table 2 Effect of previous treatments on the number of relapses two-years before fingolimod initiation and on the number of Gd+ lesions at baseline samples.
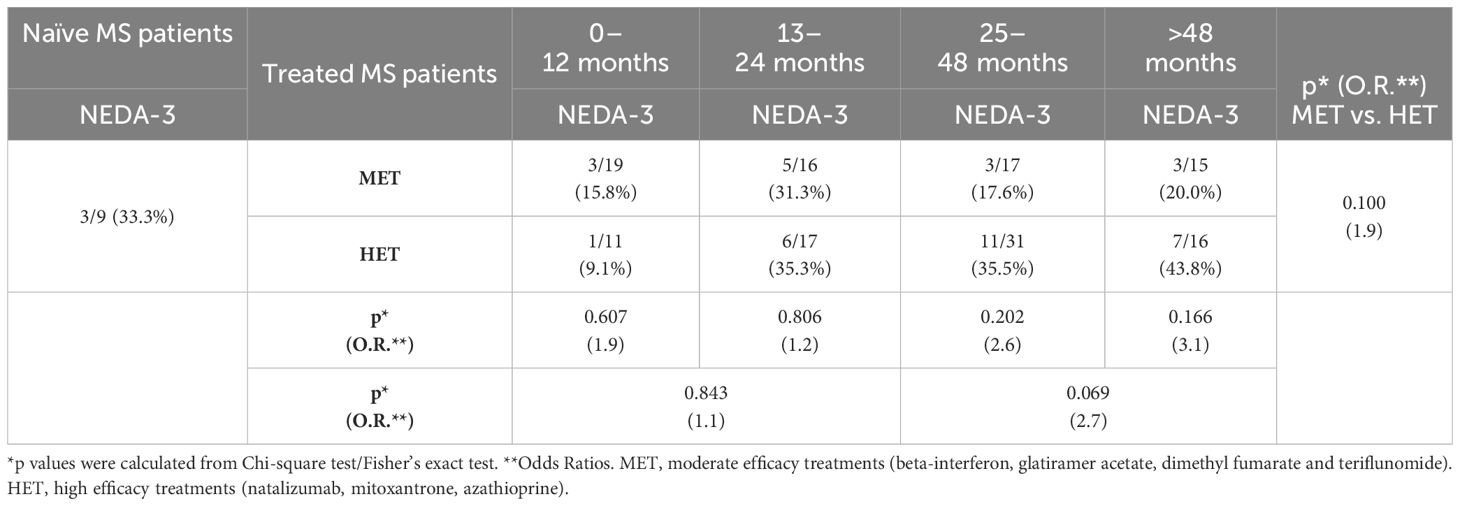
Table 3 Effect of previous treatments on NEDA-3 condition.
3.4 HLA-II as early biomarker of response
After Bonferroni correction, we only found statistically significant associations for DR4 carriers: most of them were clinical responders (p=0.008; O.R. = 3.4) and none of them progressed after two-years of follow-up (p=0.006; O.R. = 15.9). However, the statistical significance was not reached when analyzing the NEDA-3 condition (p=0.09; O.R. = 2.6).
3.5 Viral serologies and the response to fingolimod treatment
We did not find statistically significant associations for EBNA-1 IgG, VCA IgG or HHV-6 IgG and IgM titers at baseline with NEDA-3 condition (see Figure 2A). The change in the antibody titers between the baseline and the six month sample was not associated either (Figure 2B); we did not consider variations ≤4.8% (our inter-assay coefficient of variation). Finally we also analyzed the possible association of the baseline antibody titers and the antibody titers variation between the baseline sample and the six month sample with the progression (yes vs. no, and PIRA vs. RAW) and with the activity of the disease (with relapses vs. without relapses, and with Gd+ lesions vs. without Gd+ lesions), after 2-years of follow-up with fingolimod treatment. Again, we did not consider variations ≤4.8% (our inter-assay coefficient of variation). After Bonferroni correction for multiple comparisons, we only found one statistically significant association when we compared PIRA and RAW patients: we found that EBNA-1 IgG titers decreased in 3/15 (20.0%) PIRA patients after two-years of fingolimod therapy vs. 11/15 (73.3%) RAW patients (p=0.006; O.R. = 11.0) (Figure 3).
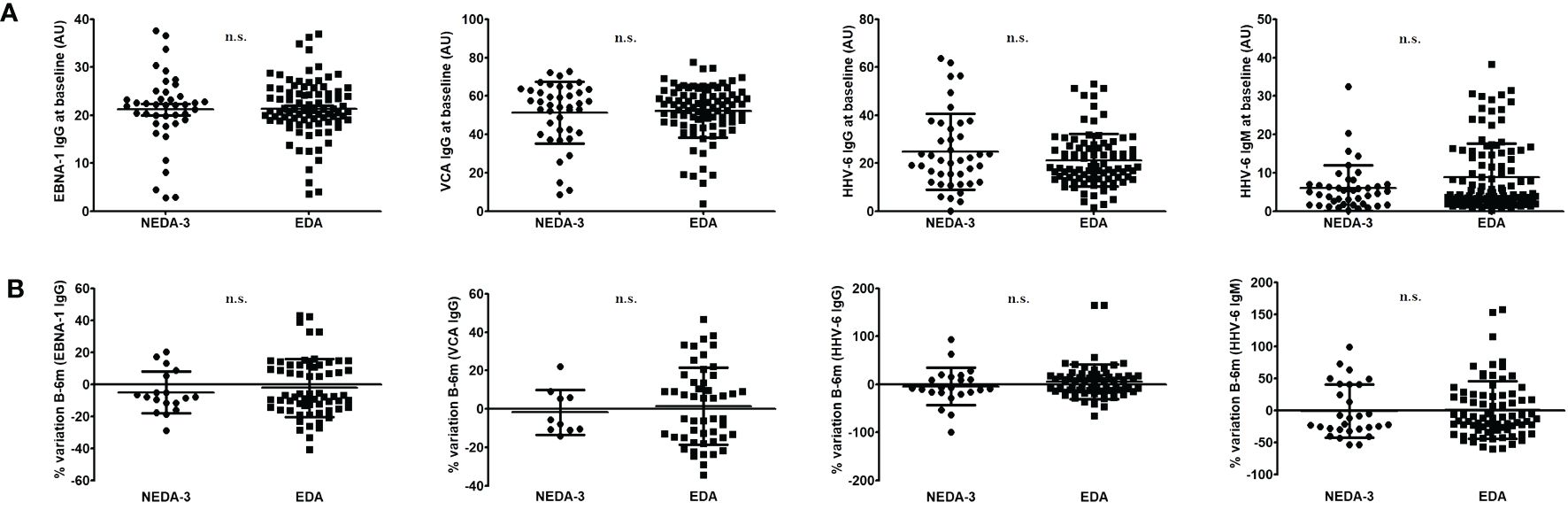
Figure 2 (A). EBNA-1 IgG, VCA IgG or HHV-6 IgG and IgM titers at baseline in NEDA-3 and EDA patients. (B) Variation in the antibody titers between NEDA-3 and EDA patients (we did not consider variations ≤4.8%, our inter-assay coefficient of variation). Significations with the two-tailed t-test are shown (n.s., not significant). Lines inside the graphs shows the mean value plus the standard deviation. (GraphPad Prism 5.0).
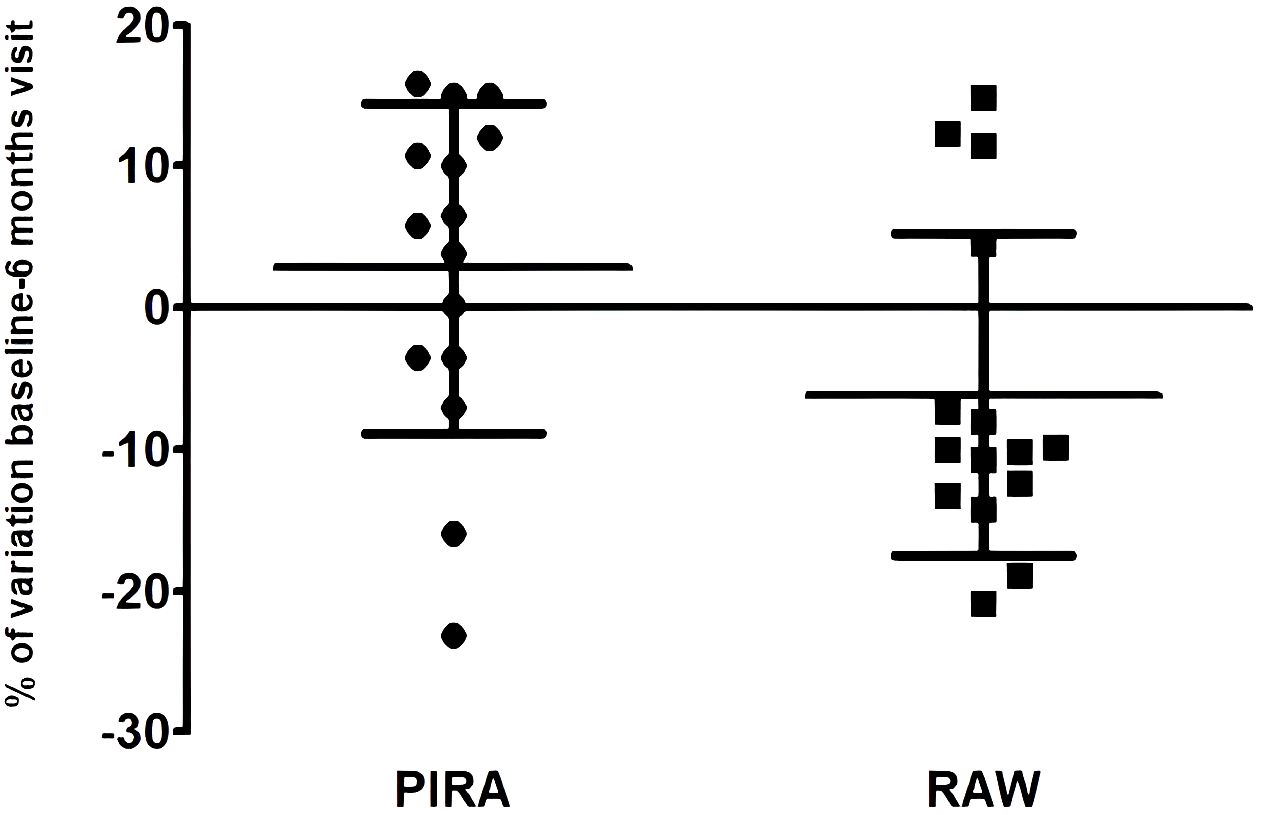
Figure 3 EBNA-1 IgG variation between the baseline sample and the six month sample in PIRA and RAW patients. Mean values plus standard deviation (GraphPad Prism 5.0).
4 Discussion
Identifying early predictors of response in MS is essential for improving patient outcomes, optimizing treatment strategies, and advancing our understanding of the disease. It holds the potential to transform MS care by enabling personalized, timely, and effective interventions, ultimately benefiting both patients and the healthcare system as a whole. With this purpose, we analyzed different clinical, radiological, genetic and serological variables to search for early predictors of NEDA-3 condition after two-years of treatment with fingolimod.
Patients recruited for this multicenter study showed a lower proportion of NEDA-3 condition compared to most of the studies performed in real-world: 56.6% (28), 44% (29), 48.3% (8), 44% (30), but similar to other real-world studies, 22% (31), and post-hoc analyses of randomized clinical trials, 29.5% (32), and 31.0% (33). The variability in NEDA-3 proportion could be explained by the heterogeneity of MS patients included in the different real-world studies. In our cohort, only 9/151 (6.0%) were treatment naïve, and previous studies published a higher proportion of NEDA-3 condition in treatment naïve patients treated with fingolimod (28). Regarding the other patients of our study, 67/151 (44.3%) were treated with MET (median: 25.0 months; range: 1–192 months) and 75/151 (49.7%) were treated with HET (median: 32.0 months; range: 1–92 months). As it has been previously described (28), previous DMTs influence the NEDA-3 proportion of MS patients treated with fingolimod. In our study, although a clear effect of previous treatments was described on the number of relapses and Gd+ lesions prior fingolimod initiation (Table 2), no statistically significant differences were found in relation to the NEDA-3 condition (Table 3). However, trends were found when we compared MET vs. HET, and also when we compared MS patients treated with MET and HET for more than two years, showing that not only prior treatments but also their duration may influence the subsequent clinical response to fingolimod.
In our study, the following early predictors were statistically significant associated with NEDA-3 condition: sex (male), age at baseline (older), relapses 2-years before fingolimod initiation ≤1, and absence of Gd+ lesions at baseline. The last three have been yet previously reported as early predictors of fingolimod treatment (8), together with lower EDSS score at baseline (9). However, previous studies have not found significant differences in treatment response between males and females taking fingolimod. In our cohort, 21/46 (45.7%) males were NEDA-3 vs. 21/105 (20.0%) females. No differences in previous treatments were found between males and females, and we did not find any difference for the other three variables between them either. Further studies will be needed to find a possible explanation.
Regarding the genetic variables analyzed, we found that DR4 carriers were better clinical responders and none of them progressed after two-years of follow-up. There is only one previous study analyzing different genetic data to find predictors of response to fingolimod (20), but none analyzing HLA apart from one searching for HLA alleles that differentially regulate John Cunningham (JC) virus antibody serostatus in MS patients treated with fingolimod (34). The term DR4 refers to the HLA-DRB1*04, that is associated with an increased risk of developing MS, mainly in some Mediterranean populations (35). Regarding MS, HLA-DRB1*04 alleles have been associated with primary progressive MS (PP-MS) (36); however, other studies could only either suggest a non-significant trend to a positive association of HLA-DRB1*04 alleles with PP-MS (37), or no effect at all (38). The possible association of HLA-DRB1*04 with PP-MS and the results of our study showing absence of progression in DR4 carriers treated with fingolimod, suggest further studies to solve this intriguing association.
Finally, we described an interesting association between EBNA-1 IgG titers and the progression of the disease. The 73.3% of RAW patients experienced a decrease of those antiviral titers between baseline visit and six-month visit after two years of fingolimod treatment vs. only 20.0% of PIRA patients. EBV is currently considered one of the main risk factors in MS (39). A recent study showed that an immune response against EBV could turn against the host, triggering disease progression (40). Different studies have supported the role of EBV in the progression of the disease in the last years (41). Here we first describe a different behavior of EBV depending on the different progression of the disease. We could speculate that EBV would be associated to those mechanisms involved in the progression of the disease that are independent of relapse activity, also referred to as smoldering MS (42), rather than in the relapse-associated worsening. The re-analysis of previous clinical trials or observational studies from the perspective here described of a different behavior of EBV in PIRA and RAW patients could be very valuable.
However, one limitation of the study could be its retrospective design. Thus, we should be aware about possible selection bias of the patients recruited for the study, and therefore, the level of evidence could be inferior compared with prospective studies. Other limitation of the study, related to one of the significant results obtained, could be the small size of the cohorts resulting from dividing those MS patients who progressed after two years of fingolimod treatment, between PIRA and RAW. It would also have been desirable to have a measurement of the EBV antibody titers in serum samples collected at 24 months to confirm the titer variations obtained at the 6 month visit.
In conclusion, here we describe four early predictors that could help to identify optimal responders to fingolimod treatment. Thus, according to the current study, MS patients that are male, older, and with a low clinical and radiological activity at fingolimod initiation have a greater probability to reach NEDA-3 condition after two years with this therapy. An intriguing association of EBV with the progression of the disease has also been described, but it should be further study in a larger cohort to confirm these results.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Comité Ético de Investigación Clínica del Hospital Clínico San Carlos. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MD-M: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing, Validation. VG: Writing – review & editing, Resources. LR-T: Resources, Writing – review & editing. AQ: Resources, Writing – review & editing. EQ: Resources, Writing – review & editing. LV: Resources, Writing – review & editing. LC-F: Resources, Writing – review & editing. JF: Resources, Writing – review & editing. NV: Resources, Writing – review & editing. AM: Investigation, Methodology, Writing – review & editing. RA: Resources, Writing – review & editing. RA-L: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. AM has a technician contract from “REI: Red de Enfermedades Inflamatorias” (RD21/0002/0038). This work was financially supported by Ministerio de Ciencia e Innovación (Proyectos de generación de conocimiento)-Fondo Europeo de Desarrollo Regional (Feder) (PID2021-126041OB-I00) and “Fundación LAIR”.
Conflict of interest
VG has received support for attending meetings and speaking honoraria from Merck, Biogen, Novartis and Sanofi-Genzyme. LR-T has received compensation for consulting services and speaking honoraria from Biogen, Novartis, Bayer, Merck, Sanofi, Genzyme, Janssen, Horizon, Teva Pharmaceutical Industries Ltd, Almirall. AQ has received travel support from Merck and Novartis for conference attendance. LV has served at scientific advisory boards, participated in meetings sponsored by, received speaking honoraria or travel funding or research grants from Roche, Sanofi, Merck, Biogen, Bristol Myers, and Novartis. LC-F reports compensation for consulting services and speaker honoraria from Biogen, Bristol Myers Squibb, Janssen, Merck-Serono, Novartis, Sanofi, Roche, and Teva. RA has been a speaker or has participated in the advisory board of Novartis, Teva, Roche, Bristol, Janssen, Biogen, Merck and Sanofi-Genzyme. RA-L has received support for attending meetings from Biogen, Merck, Novartis and Sanofi-Genzyme.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1384411/full#supplementary-material
References
1. Kappos L, Radue E-W, O'Connor P, Polman C, Hohlfeld R, Calabresi P, et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med. (2010) 362:387–401. doi: 10.1056/NEJMoa0909494
2. Cyster JG. Chemokines, sphingosine-1-phosphate, and cell migration in secondary lymphoid organs. Annu Rev Immunol. (2005) 23:127–59. doi: 10.1146/annurev.immunol.23.021704.115628
3. European Medicines Agency: Gilenya (fingolimod) product information EMEA/H/C/002202 -II-26G. Available online at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002202/human_med_001433.jsp&mid=WC0b01ac058001d125 (Accessed June 21, 2017).
4. Calabresi PA, Radue EW, Goodin D, Jeffery D, Rammohan KW, Reder AT, et al. Safety and efficacy of fingolimod in patients with relapsing-remitting multiple sclerosis (FREEDOMS II): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. (2014) 13:545–56. doi: 10.1016/S1474-4422(14)70049-3
5. Uzunköprü C, Beckmann Y, Türe S. Long-term effectiveness of fingolimod for multiple sclerosis in a real-world clinical setting. Eur Neurol. (2021) 84:200–5. doi: 10.1159/000514828
6. Lanzillo R, Carotenuto A, Moccia M, Saccà F, Russo CV, Massarelli M, et al. A longitudinal real-life comparison study of natalizumab and fingolimod. Acta Neurol Scand. (2017) 136:217–22. doi: 10.1111/ane.2017.136.issue-3
7. Galán Sánchez-Seco V, Casanova-Peño I, Álvarez-Lafuente R, Sánchez-Jiménez M, García-Martínez A, Domínguez-Mozo MI, et al. Fingolimod use for the treatment of multiple sclerosis in a clinical practice setting in madrid. Clin Neuropharmacol. (2017) 40:29–33. doi: 10.1097/WNF.0000000000000196
8. Ferrè L, Clarelli F, Pignolet B, Mascia E, Frasca M, Santoro S, et al. Combining clinical and genetic data to predict response to fingolimod treatment in relapsing remitting multiple sclerosis patients: A precision medicine approach. J Pers Med. (2023) 13:122. doi: 10.3390/jpm13010122
9. Lattanzi S, Rocchi C, Danni M, Taffi R, Cerqua R, Carletti S, et al. Long-term outcome in multiple sclerosis patients treated with fingolimod. Mult Scler Relat Disord. (2020) 45:102416. doi: 10.1016/j.msard.2020.102416
10. Mazdeh M, Taheri M, Sayad A, Bahram S, Omrani MD, Movafagh A, et al. HLA genes as modifiers of response to IFN-β-1a therapy in relapsing-remitting multiple sclerosis. Pharmacogenomics. (2016) 17:489–98. doi: 10.2217/pgs.16.2
11. Ross CJ, Towfic F, Shankar J, Laifenfeld D, Thoma M, Davis M, et al. A pharmacogenetic signature of high response to Copaxone in late-phase clinical-trial cohorts of multiple sclerosis. Genome Med. (2017) 9:50. doi: 10.1186/s13073-017-0436-y
12. Comabella M, Fernández-Arquero M, Río J, Guinea A, Fernández M, Cenit MC, et al. HLA class I and II alleles and response to treatment with interferon-beta in relapsing-remitting multiple sclerosis. J Neuroimmunol. (2009) 210:116–9. doi: 10.1016/j.jneuroim.2009.01.012
13. Gomez-Gaitan EA, Garcia-Ortega YE, Saldaña-Cruz AM, Contreras-Haro B, Gamez-Nava JI, Pérez-Guerrero EE, et al. Genetic variant HLA-DRB1*0403 and therapeutic response to disease-modifying therapies in multiple sclerosis: A case-control study. Int J Mol Sci. (2023) 24:14594. doi: 10.3390/ijms241914594
14. Gontika M, Skarlis C, Markoglou N, Evangelopoulos ME, Velonakis G, Chrousos GP, et al. Fingolimod as a first- or second-line treatment in a mini-series of young Hellenic patients with adolescent-onset multiple sclerosis: focus on immunological data. Neurol Sci. (2022) 43:2641–9. doi: 10.1007/s10072-021-05623-2
15. Dominguez-Mozo MI, Perez-Perez S, Villar LM, Oliver-Martos B, Villarrubia N, Matesanz F, et al. Predictive factors and early biomarkers of response in multiple sclerosis patients treated with natalizumab. Sci Rep. (2020) 10:14244. doi: 10.1038/s41598-020-71283-5
16. Domínguez-Mozo MI, González-Suárez I, Villar LM, Costa-Frossard L, Villarrubia N, Aladro Y, et al. Teriflunomide and Epstein-Barr virus in a Spanish multiple sclerosis cohort: in vivo antiviral activity and clinical response. Front Immunol. (2023) 14:1248182. doi: 10.3389/fimmu.2023.1248182
17. Ortega-Madueño I, Garcia-Montojo M, Dominguez-Mozo MI, García-Martínez A, Arias-Leal AM, Casanova I, et al. Anti-human herpesvirus 6A/B IgG correlates with relapses and progression in multiple sclerosis. PLoS One. (2014) 9:e104836. doi: 10.1371/journal.pone.0104836
18. Pender MP, Csurhes PA, Smith C, Douglas NL, Neller MA, Matthews KK, et al. Epstein-Barr virus-specific T cell therapy for progressive multiple sclerosis. JCI Insight. (2018) 3:e124714. doi: 10.1172/jci.insight.124714
19. Houen G, Trier NH, Frederiksen JL. Epstein-barr virus and multiple sclerosis. Front Immunol. (2020) 11:587078. doi: 10.3389/fimmu.2020.587078
20. Kappos L, Bar-Or A, Cree BAC, Fox RJ, Giovannoni G, Gold R, et al. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet. (2018) 391:1263–73. doi: 10.1016/S0140-6736(18)30475-6
21. Kappos L, Fox RJ, Burcklen M, Freedman MS, Havrdová EK, Hennessy B, et al. Ponesimod compared with teriflunomide in patients with relapsing multiple sclerosis in the active-comparator phase 3 OPTIMUM study: A randomized clinical trial. JAMA Neurol. (2021) 78:558–67. doi: 10.1001/jamaneurol.2021.0405
22. Comi G, Kappos L, Selmaj KW, Bar-Or A, Arnold DL, Steinman L, et al. Safety and efficacy of ozanimod versus interferon beta-1a in relapsing multiple sclerosis (SUNBEAM): a multicentre, randomised, minimum 12-month, phase 3 trial. Lancet Neurol. (2019) 180:1009–20. doi: 10.1016/S1474-4422(19)30239-X
23. Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, Ebers GC, et al. New diagnostic criteria for multiple sclerosis: Guidelines for research protocols. Ann Neurol. (1983) 13:227–31. doi: 10.1002/ana.410130302
24. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. (2011) 69:292–302. doi: 10.1002/ana.22366
25. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
26. Prosperini L, Ruggieri S, Haggiag S, Tortorella C, Pozzilli C, Gasperini C. Prognostic accuracy of NEDA-3 in long-term outcomes of multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. (2021) 8:e1059. doi: 10.1212/NXI.0000000000001059
27. Medina S, Villarrubia N, Sainz de la Maza S, Lifante J, Costa-Frossard L, Roldán E, et al. Optimal response to dimethyl fumarato associates in MS with a shift from an inflammatory to a tolerogenic blood cell profile. Mult Scler J. (2018) 24:1317–27. doi: 10.1177/1352458517717088
28. Comi G, Pozzilli C, Morra VB, Bertolotto A, Sangalli F, Prosperini L, et al. Effectiveness of fingolimod in real-world relapsing-remitting multiple sclerosis Italian patients: the GENIUS study. Neurol Sci. (2020) 41:2843–51. doi: 10.1007/s10072-020-04380-y
29. Guerra T, Caputo F, Orlando B, Paolicelli D, Trojano M, Iaffaldano P. Long-term comparative analysis of no evidence of disease activity (NEDA-3) status between multiple sclerosis patients treated with natalizumab and fingolimod for up to 4 years. Neurol Sci. (2021) 42:4647–55. doi: 10.1007/s10072-021-05127-z
30. Baroncini D, Ghezzi A, Annovazzi PO, Colombo B, Martinelli V, Minonzio G, et al. Natalizumab versus fingolimod in patients with relapsing-remitting multiple sclerosis non-responding to first-line injectable therapies. Mult Scler. (2016) 22:1315–26. doi: 10.1177/1352458516650736
31. Curti E, Tsantes E, Baldi E, Caniatti LM, Ferraro D, Sola P, et al. The real-world effectiveness of natalizumab and fingolimod in relapsing-remitting multiple sclerosis. An Italian multicentre study. Mult Scler Relat Disord. (2019) 33:146–52. doi: 10.1016/j.msard.2019.05.026
32. Havrdova E, Galetta S, Hutchinson M, Stefoski D, Bates D, Polman CH, et al. Effect of natalizumab on clinical and radiological disease activity in multiple sclerosis: a retrospective analysis of the Natalizumab Safety and Efficacy in Relapsing-Remitting Multiple Sclerosis (AFFIRM) study. Lancet Neurol. (2009) 8:254–60. doi: 10.1016/S1474-4422(09)70021-3
33. Kappos L, De Stefano N, Freedman MS, Cree BA, Radue EW, Sprenger T, et al. Inclusion of brain volume loss in a revised measure of 'no evidence of disease activity' (NEDA-4) in relapsing-remitting multiple sclerosis. Mult Scler. (2016) 22:1297–305. doi: 10.1177/1352458515616701
34. Watanabe M, Nakamura Y, Isobe N, Tanaka M, Sakoda A, Hayashi F, et al. Two susceptible HLA-DRB1 alleles for multiple sclerosis differentially regulate anti-JC virus antibody serostatus along with fingolimod. J Neuroinflamm. (2020) 17:206. doi: 10.1186/s12974-020-01865-7
35. Compston A. The genetic epidemiology of multiple sclerosis. Philos Trans R Soc Lond B Biol Sci. (1999) 354:1623–34. doi: 10.1098/rstb.1999.0507
36. Weinshenker BG, Santrach P, Bissonet AS, McDonnell SK, Schaid D, Moore SB, et al. Major histocompatibility complex class II alleles and the course and outcome of MS: a population-based study. Neurology. (1998) 51:742–7. doi: 10.1212/WNL.51.3.742
37. Smestad C, Brynedal B, Jonasdottir G, Lorentzen AR, Masterman T, Akesson E, et al. The impact of HLA-A and –DRB1 on age at onset, disease course and severity in Scandinavian multiple sclerosis patients. Eur J Neurol. (2007) 14:835–40. doi: 10.1111/j.1468-1331.2007.01825.x
38. Greer JM, Pender MP. The presence of glutamic acid at positions 71 or 74 in pocket 4 of the HLA-DRbeta1 chain is associated with the clinical course of multiple sclerosis. Psychiatry. (2005) 76:656–62. doi: 10.1136/jnnp.2004.042168
39. Bjornevik K, Cortese M, Healy BC, Kuhle J, Mina MJ, Leng Y, et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. (2022) 375:296–301. doi: 10.1126/science.abj8222
40. Lanz TV, Brewer RC, Ho PP, Moon JS, Jude KM, Fernández D, et al. Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Nature. (2022) 603:321–7. doi: 10.1038/s41586-022-04432-7
41. Lünemann JD, Tintoré M, Messmer B, Strowig T, Rovira A, Perkal H, et al. Elevated Epstein–Barr virus-encoded nuclear antigen-1 immune responses predict conversion to multiple sclerosis. Ann Neurol. (2010) 67:159–69. doi: 10.1002/ana.21886
Keywords: multiple sclerosis, fingolimod, Epstein-Barr virus, human herpesvirus 6, human leukocyte antigen
Citation: Dominguez-Mozo MI, Galán V, Ramió-Torrentà L, Quiroga A, Quintana E, Villar LM, Costa-Frossard L, Fernández-Velasco JI, Villarrubia N, Garcia-Martinez MA, Arroyo R and Alvarez-Lafuente R (2024) A two-years real-word study with fingolimod: early predictors of efficacy and an association between EBNA-1 IgG titers and multiple sclerosis progression. Front. Immunol. 15:1384411. doi: 10.3389/fimmu.2024.1384411
Received: 09 February 2024; Accepted: 23 May 2024;
Published: 07 June 2024.
Edited by:
Gunnar Houen, University of Copenhagen, DenmarkReviewed by:
Peter A. Maple, Nottingham University Hospitals NHS Trust, United KingdomNicole Trier, Rigshospitalet Glostrup, Denmark
Copyright © 2024 Dominguez-Mozo, Galán, Ramió-Torrentà, Quiroga, Quintana, Villar, Costa-Frossard, Fernández-Velasco, Villarrubia, Garcia-Martinez, Arroyo and Alvarez-Lafuente. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberto Alvarez-Lafuente, cmFsdmFyZXpsYWZ1ZW50ZUB5YWhvby5lcw==