 Limei Shi†
Limei Shi† Bin Wang
Bin Wang KaiYu Zhang
KaiYu Zhang Yang Wang
Yang Wang- Center of Infectious Disease and Pathogen Biology, Department of Infectious Diseases, The First Hospital of Jilin University, Changchun, China
Brucellosis is a highly contagious zoonotic disease characterized by a non-specific clinical presentation and complex disease progression and outcome. Hemophagocytic lymphohistiocytosis (HLH) is an abnormal immune response syndrome marked by potentially fatal cytokine storms. Brucella-associated HLH is exceedingly rare and associated with a high mortality rate. We report a case involving a 23-year-old male residing in a brucellosis-endemic region, with a documented history of exposure to cattle and sheep. He was admitted to the hospital presenting with fever and arthralgia. Laboratory tests indicated splenomegaly, pancytopenia, elevated serum aminotransferases and ferritin levels, as well as decreased fibrinogen levels. Blood and bone marrow cultures yielded negative results. The Brucella serum agglutination test returned a positive result (titer, 1:200). Bone marrow aspirate results revealed an increased number of hemophagocytes, and PET-CT scans demonstrated splenomegaly, suggesting hemophagocytic changes. Following a comprehensive exclusion of hematological malignancies and neoplastic diseases, the patient was diagnosed with probable Brucella infection complicated by secondary HLH. Standard anti-brucellosis therapy was initiated immediately upon hospital admission. Remarkably, significant clinical improvement was observed within 7 days of targeted antibiotic treatment, without the need for corticosteroid therapy. This case, when analyzed alongside a systematic review of 12 published HLH cases associated with brucellosis, underscores the importance of maintaining a heightened clinical suspicion for this life-threatening complication in endemic regions, which may facilitate earlier diagnosis and optimized antimicrobial management strategies.
Introduction
Brucella spp. are facultative intracellular gram-negative pathogens responsible for brucellosis, a globally prevalent zoonotic disease transmitted through direct exposure to infected livestock or the consumption of unpasteurized dairy products. This disease imposes a substantial economic burden and presents ongoing public health challenges. While classical manifestations include undulant fever, sweats, and migratory polyarthralgia, severe complications may arise, such as hematological emergencies, including secondary HLH. HLH is a life-threatening hyperinflammatory syndrome characterized by dysregulated cytotoxic T-cell (CTL) and natural killer (NK) cell activity, as well as macrophage activation, rather than being a distinct disease entity (1, 2). Pathophysiologically, HLH manifests as a cytokine storm, which can culminate in multiorgan failure. Its clinical management remains challenging due to overlapping features with septicemia (3). Here, we present a diagnostically challenging case involving a 23-year-old male patient who exhibited fever, arthralgia, splenomegaly, and pancytopenia. The patient showed improvement following anti-brucellosis treatment, with no corticosteroid therapy administered. He was diagnosed with probable Brucella infection complicated by secondary HLH. The cases of Brucella infection complicated by HLH are exceedingly rare. This case underscores the importance of obtaining a comprehensive epidemiological history and conducting serological testing for brucellosis during the diagnostic process. It also highlights the necessity of initiating empirical anti-brucellosis therapy in patients with rapid disease progression when clinical suspicion is high. For brucellosis-associated HLH, bone marrow biopsy and PET-CT imaging are effective tools that expedite diagnostic evaluation and help differentiate it from other underlying conditions.
Case report
Clinical manifestation
A 23-year-old male from Inner Mongolia, China, presented to our hospital with persistent joint pain lasting one year and an acute onset of fever accompanied by a cough over the past three days. The patient initially developed migratory polyarthralgia affecting large joints (knees and ankles) for one year prior to admission, which had not been medically evaluated. Three days before admission, he experienced a sudden onset of fever (peak temperature of 38.8°C) accompanied by chills and a paroxysmal non-productive cough. Initial treatment at a local clinic included intravenous cephalosporin therapy (2.0 g, QD, i.v.). Within a few hours of the initial treatment, he developed facial edema, conjunctival hemorrhage, and epigastric pain. Despite continued treatment with cephalosporin, his symptoms did not improve, prompting his referral to our institution. During the outpatient visit to our hospital, the patient’s laboratory tests indicated pancytopenia, increased levels of aminotransferases, elevated ultrasensitive C-reactive protein, and decreased fibrinogen. Upon admission, the physical examination revealed facial edema, bilateral conjunctival congestion, enlarged cervical lymph nodes, abdominal tenderness without rebound pain, and muscle tension. The patient resided in Inner Mongolia and kept cows and sheep at home, with a history of feeding them. Notably, there was an incident of abortion in the cows and sheep one month prior to admission. The patient did not wear gloves while handling the fetus. There was no history of tuberculosis, recent travel, blood transfusions, alcohol consumption, smoking, or other relevant factors. Additionally, there was no family history of similar conditions.
Diagnostics and examinations
The patient was admitted to the hospital with a fever of unknown origin. Major laboratory tests conducted post-admission revealed pancytopenia, elevated aminotransferases, elevated C-reactive protein (CRP), and decreased fibrinogen (Table 1). To determine the cause of the fever, we performed a series of etiological tests, including procalcitonin, antibodies against the epidemic hemorrhagic fever virus, cytomegalovirus nucleic acid quantification and antibodies, Epstein-Barr virus (EBV) nucleic acid quantification and antibodies, as well as a tuberculosis interferon-gamma release assay and a tuberculin skin test, all of which yielded negative results. We also tested for rheumatic immunology markers, including rheumatological factor, anti-cyclic citrullinated peptide antibodies, and antinuclear antibodies, all of which were negative. Blood cultures also returned negative. Given the patient’s epidemiological history and clinical manifestations, including fever, arthralgia, splenomegaly, and lymphadenopathy, there was a strong suspicion of Brucella infection. Further testing using the Brucella serum agglutination test (SAT) confirmed this suspicion, yielding a positive result at a titer of 1:200. Due to the patient’s severe condition, characterized by pancytopenia and elevated ferritin levels upon admission, we conducted bone marrow aspiration, tumor marker testing, and PET-CT to rule out other hematological or neoplastic diseases. Simultaneously, a bone marrow culture was performed. The bone marrow smear exhibited myeloproliferative activity, with histiocytes and phagocytes clearly visible; histiocytes accounted for 2.5%, and phagocytes also accounted for 2.5% (Figure 1). The bone marrow biopsy revealed markedly active myeloproliferative activity with an elevated red lineage ratio, and megakaryocytes were readily observed (Figure 2). However, the bone marrow culture returned negative results. Additionally, the PET-CT scan indicated splenomegaly, characterized by hypermetabolic nodules, and did not exclude hemophagocytic changes (Figure 3). Furthermore, abdominal CT demonstrated splenomegaly, edema of the gallbladder wall, and ascites. Lung CT revealed bronchitis in the right middle lobe, inflammation in the left lingula lobe, scattered inflammation in both lower lobes, and bilateral pleural effusion. Abdominal ultrasound confirmed splenomegaly and identified an intrasplenic, flaky, hypoechoic lesion. Cardiac ultrasound indicated a small pericardial effusion. Following the hematologist’s advice, we monitored for HLH. Soluble CD25 was 20984 pg/ml (normal range: <6,400), and NK cell activity was recorded at 18.57% (normal range: 47.6%-76.8%). Consequently, a probable Brucella infection with secondary HLH was suspected.
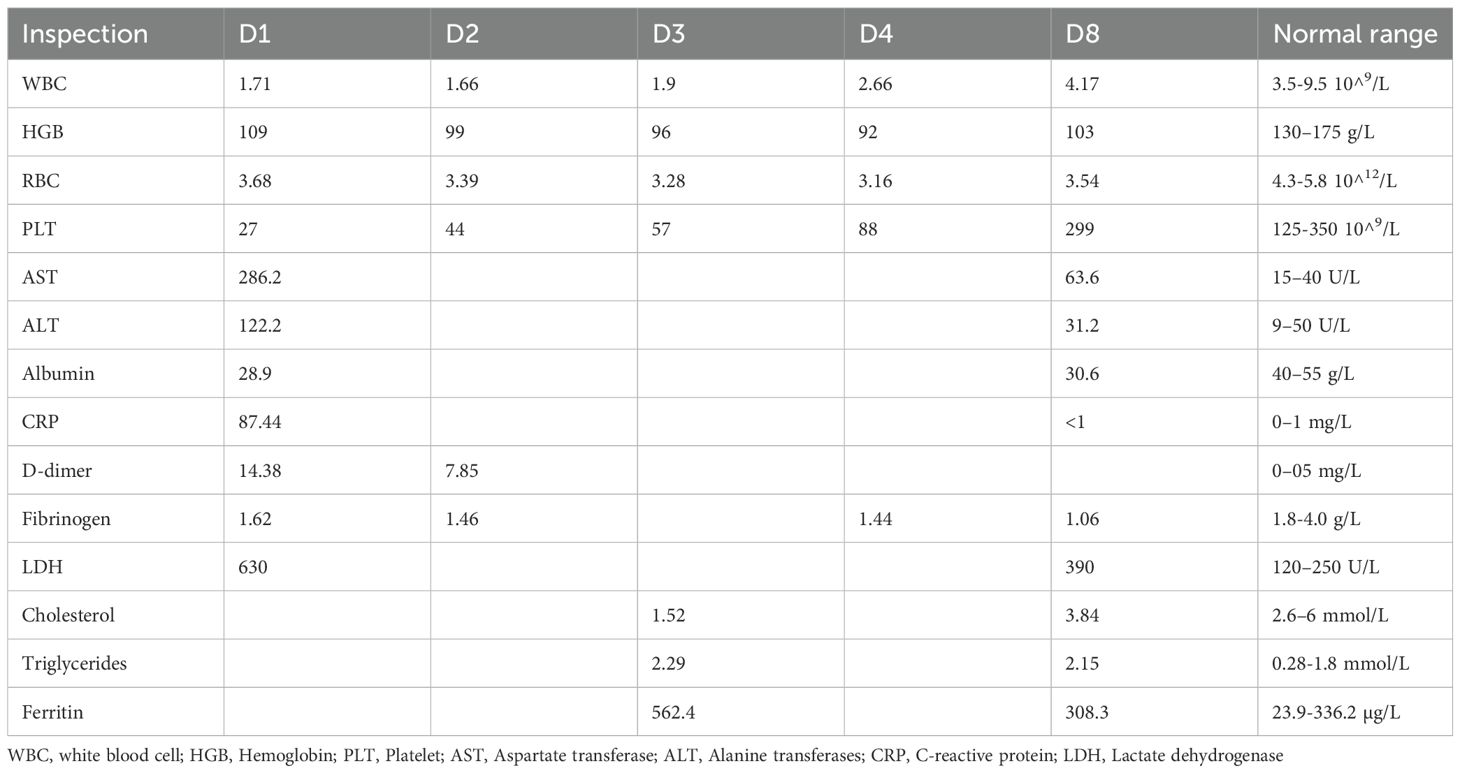
Table 1. Summary of the laboratory tests in the patient.
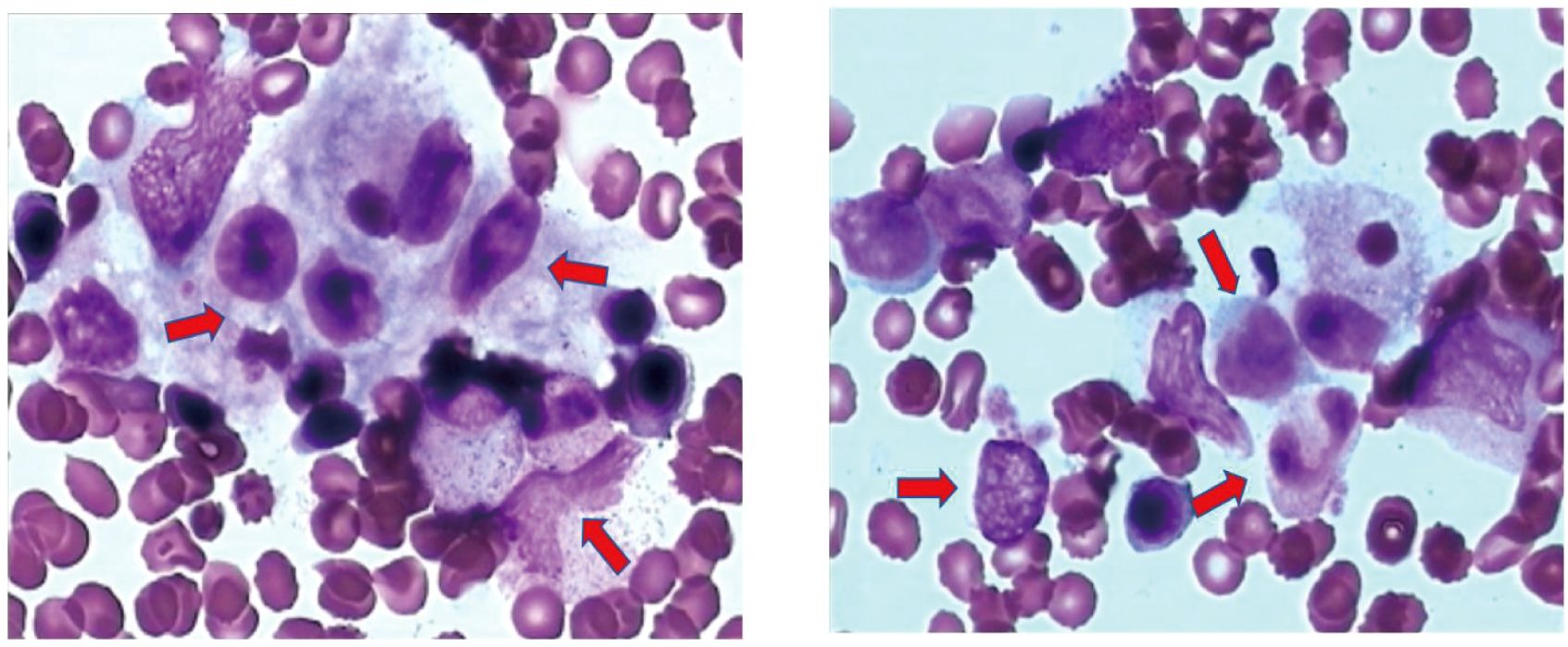
Figure 1. Bone marrow smear. Histiocytes and phagocytes are easily visible. Histiocytes accounted for 2.5% and phagocytic cells accounted for 2.5%, and phagocytic erythrocytes were visible. Arrows indicate hemophagocytes. Hemophagocytosis refers to the pathological process where macrophages (a type of immune cell) engulf and destroy other blood cells, such as red blood cells, white blood cells, or platelets.
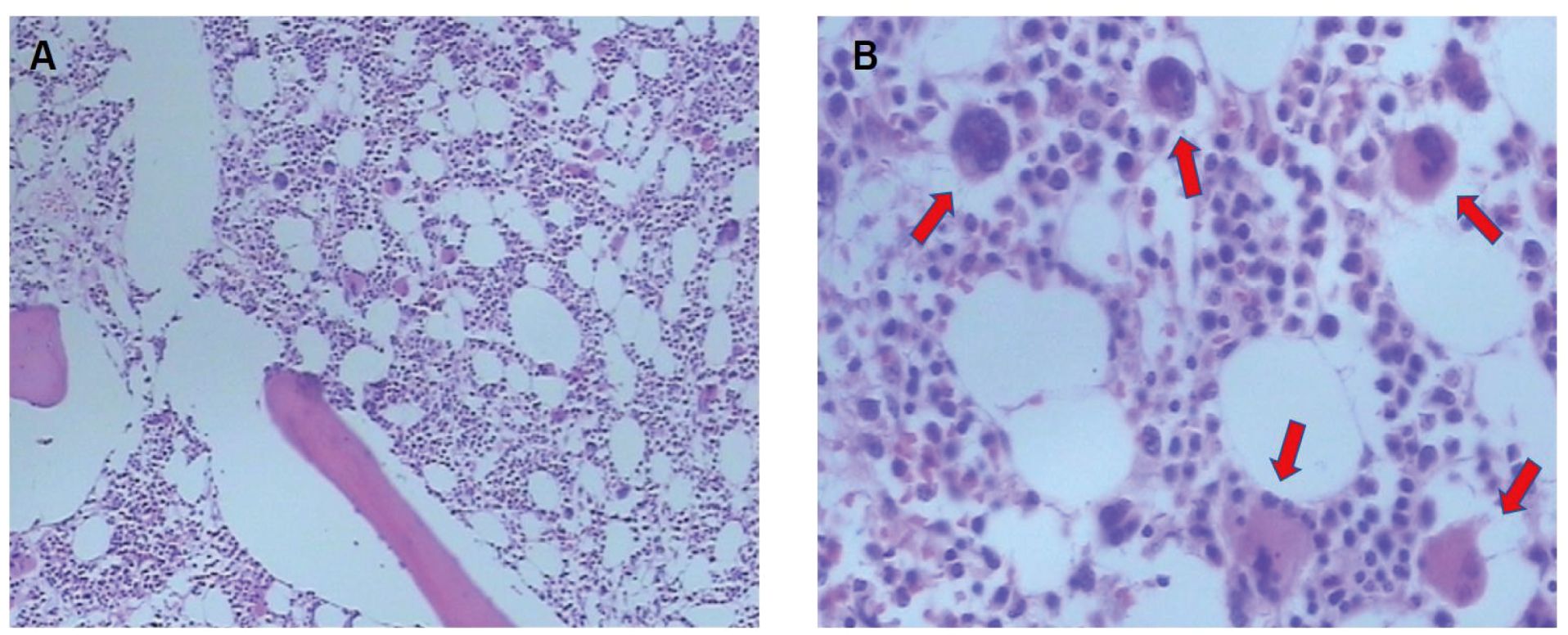
Figure 2. Bone marrow aspiration biopsy. (A) Bone marrow proliferation is markedly active, with an increased percentage of red lineage. (B) The arrows point to the easily visible megakaryocytes.
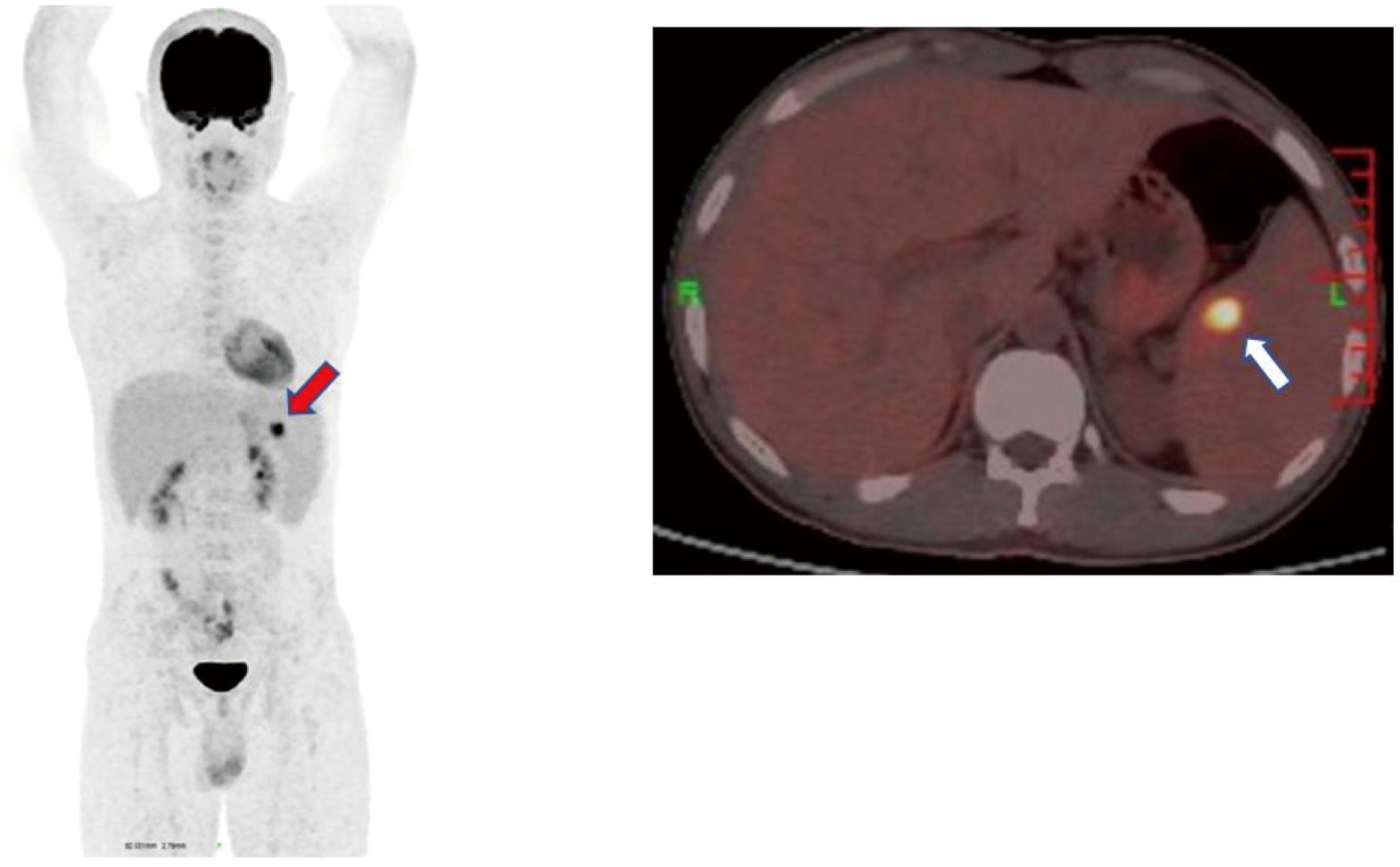
Figure 3. PET-CT whole-body imaging splenomegaly. There are focal hypermetabolic nodules inside, which cannot be ruled out as hemophagocytic changes. Both red and white arrows indicate spleens with hypermetabolic nodules. .
Treatment and regression
Initially, an anti-brucellosis treatment regimen consisting of doxycycline combined with amikacin was administered. However, due to elevated transaminase levels, rifampicin was temporarily withheld, and hepatoprotective therapy was initiated. On the fourth day of anti-brucellosis treatment, the patient’s fever showed improvement. By the eighth day, the patient was afebrile, blood counts had improved, aminotransferase levels had decreased, ferritin levels returned to normal, and triglyceride levels had diminished (Table 1). Rifampicin was subsequently added to the treatment plan. The patient was discharged on the ninth day of treatment. Following discharge, the patient continued an oral regimen of doxycycline (0.1 g, BID, p.o.) combined with rifampicin (0.6 g, QD, p.o.) for six weeks, along with intravenous amikacin (0.6 g, QD, i.v.) for two weeks. After six weeks of consistent treatment, the patient was followed up in the outpatient clinic and achieved complete recovery.
Discussion
In this case, the patient was admitted to the hospital with a persistent fever and migratory polyarthralgia as the initial symptoms. The patient exhibited typical epidemiological characteristics of Brucella infection, including: long-term residence in Inner Mongolia, a brucellosis-endemic region, and a clear history of occupational exposure to cattle and sheep. Therefore, brucellosis was prioritized as the initial differential diagnosis. However, the patient also presented with pancytopenia and elevated inflammatory markers, necessitating prompt intervention to prevent clinical deterioration. We identified the following potential conditions in the early stages: (1) hematologic malignancies, such as acute leukemia or myelodysplastic syndrome; (2) lymphoproliferative disorders, such as lymphoma-related HLH; and (3) autoimmune diseases, such as systemic lupus erythematosus. Following the WHO guidelines for the management of brucellosis, we initiated empiric dual antimicrobial therapy immediately upon hospitalization, alongside confirmatory tests, including serum tube agglutination tests and blood cultures. In this high-risk epidemiological context, this aggressive treatment approach effectively balances diagnostic investigations with timely antimicrobial intervention.
Brucellosis is a prevalent and often overlooked zoonotic disease. In recent years, it has reemerged in various regions of China, particularly in Inner Mongolia, where animal husbandry is the predominant industry (4). The disease can affect individuals of any age group. Recently, the clinical symptoms have become increasingly atypical, with some patients lacking a clear epidemiological history or presenting with negative blood cultures. Consequently, diagnosis has become progressively challenging (5). Brucellosis can lead to a range of complications. When the hematologic system is involved, it may present with various manifestations, including anemia, leukopenia, thrombocytopenia, and pancytopenia. Our patient exhibited pancytopenia upon admission. This condition may be associated with factors such as infection, hypersplenism, and bone marrow suppression. In rare cases, severe pancytopenia can be attributed to diffuse intravascular coagulation, increased hemophagocytes, or immune-mediated cell destruction (6, 7). The association between brucellosis and pancytopenia may be attributed to HLH. HLH consists of both primary and secondary components. Primary HLH (pHLH) is a hereditary condition that is more commonly observed in children, whereas secondary HLH (sHLH) predominantly affects adults. sHLH is characterized by immune overactivation and dysregulation triggered by various factors, including infections, tumors, and autoimmune diseases. The Epstein-Barr virus is the most frequently identified pathogen associated with infections, while Brucella is relatively rare (8). An innate immune response triggered by toll-like receptors (TLRs) in response to an infectious agent is one of the mechanisms leading to HLH. Brucella infection led to a significant change in the composition of peripheral immune cells, and inflammation was a key feature of brucellosis. The highest inflammatory state can be observed in acute patients. Excessive production of cytokines, such as interleukin-6 (IL-6), IL-1β, and IFN-γ, can lead to life-threatening complications (9, 10). Additionally, some patients may possess a genetic variant that hinders the resolution of the immune response, leading to excessive inflammation (11). There is a notable overlap of symptoms between brucellosis and sHLH, including persistent fever, hepatosplenomegaly, and pancytopenia. These symptoms are also prevalent in other infectious diseases, hematological disorders, and tumors, which can complicate the diagnostic process and increase the risk of misdiagnosis (12).
In the process of diagnosing brucellosis, our patient presents a clear epidemiological history, with clinical manifestations consistent with those of brucellosis, thereby raising a strong suspicion of Brucella infection. Additionally, SAT titers showed a notable increase following admission, reaching 1:200. Titers of 1:100 or higher, with at least 50% agglutination, were classified as positive. SAT titers of 1:160 or more, when aligned with the clinical symptoms, are considered diagnostic. While SAT tests are conducted as a standalone assessment, they are frequently utilized as the main diagnostic standard in clinical settings when paired with exposure history and symptoms. Nevertheless, using several serological tests can enhance the accuracy of the diagnosis (13–15). To enhance the specificity of the SAT, a cutoff of 1:320 has been recommended for the serodiagnosis of brucellosis in endemic regions. However, raising the threshold may reduce sensitivity and compromise the accuracy of the diagnosis. Simultaneously, both blood and bone marrow cultures returned negative results. The reasons for these negative results may include a short incubation period for Brucella, the presence of a chronic infection, or prior antibiotic use. This suggests a high likelihood of brucellosis (16, 17) (18, 19). While positive blood cultures remain the gold standard for confirming brucellosis, their sensitivity ranges from 50% to 90%, depending on the disease stage, Brucella species, and technical factors (13, 20). Bone marrow cultures demonstrate a marginally higher but still suboptimal yield, and their sensitivity remains a subject of debate. Eduardo Gotuzzo et al. found that among 50 patients diagnosed with Brucella infection through culture testing, 46 patients (92%) had positive bone marrow cultures, while 35 patients (70%) had positive blood cultures (21). Mantur et al. reported that Brucella was isolated from bone marrow cultures in 85 (82.5%) of 103 patients, whereas blood cultures detected it in only 47 (45.6%) (22). However, Asem Shehabi et al. found that blood culture (44.4%) was more sensitive than bone marrow culture (27.7%) (23). Following the HLH-2004 diagnostic criteria: (1) fever; (2) splenomegaly; (3) cytopenias; (4) hypertriglyceridemia and/or hypofibrinogenemia; (5) hemophagocytosis in bone marrow or spleen or lymph nodes, no evidence of malignancy; (6) low or no NK cell activity; (7) ferritin ≥500 μg/L; (8) sCD25 (ie, soluble IL-2 receptor) ≥2400 U/ml. Our patients fulfilled all 8 criteria. Thus, the diagnosis of HLH can be definitively made. The comprehensive exclusion of alternative etiologies, including viral, autoimmune, hematologic, and neoplastic disorders, further strengthens the diagnostic validity (11).
A systematic literature review identified 12 previously reported cases of brucellosis complicated by secondary HLH (Table 2). The cohort consisted of 12 patients aged 25 to 75 years, with a balanced male-to-female ratio of 1:1. Epidemiological exposure was documented in 11/12 cases, including occupational or direct animal contact (6 cases: livestock farming or sheepherding), dietary exposure (2 cases: consumption of unpasteurized dairy), and recent travel to brucellosis-endemic regions (1 case). All these patients were admitted to the hospital with a fever of unknown origin, similar to our patient. Blood cultures were performed in all 12 cases of brucellosis, and three of these patients underwent additional bone marrow cultures. Brucella species were isolated in 9 blood cultures. Among the 3 patients with negative blood cultures, bone marrow culture was performed in one case, which also showed negative results, but the Brucella serology was positive. All 12 cases met the HLH-2004 diagnostic criteria. Each patient presented with fever, pancytopenia, and hyperferritinemia. Bone marrow aspiration was conducted in all patients. However, only three patients were tested for NK cell activity and soluble CD25 (sCD25). Notably, one case showed no evidence of hemophagocytosis on the bone marrow smear and lacked both NK cell activity and sCD25 testing. Given that fever and splenomegaly are common manifestations of brucellosis and also key diagnostic criteria for HLH, a comprehensive diagnostic evaluation is strongly recommended for patients with brucellosis complicated by HLH. In the cases reported here, the diagnostic tests for HLH included assessment of NK cell activity, sCD25 levels, and even PET-CT imaging, providing robust justification for the diagnosis.
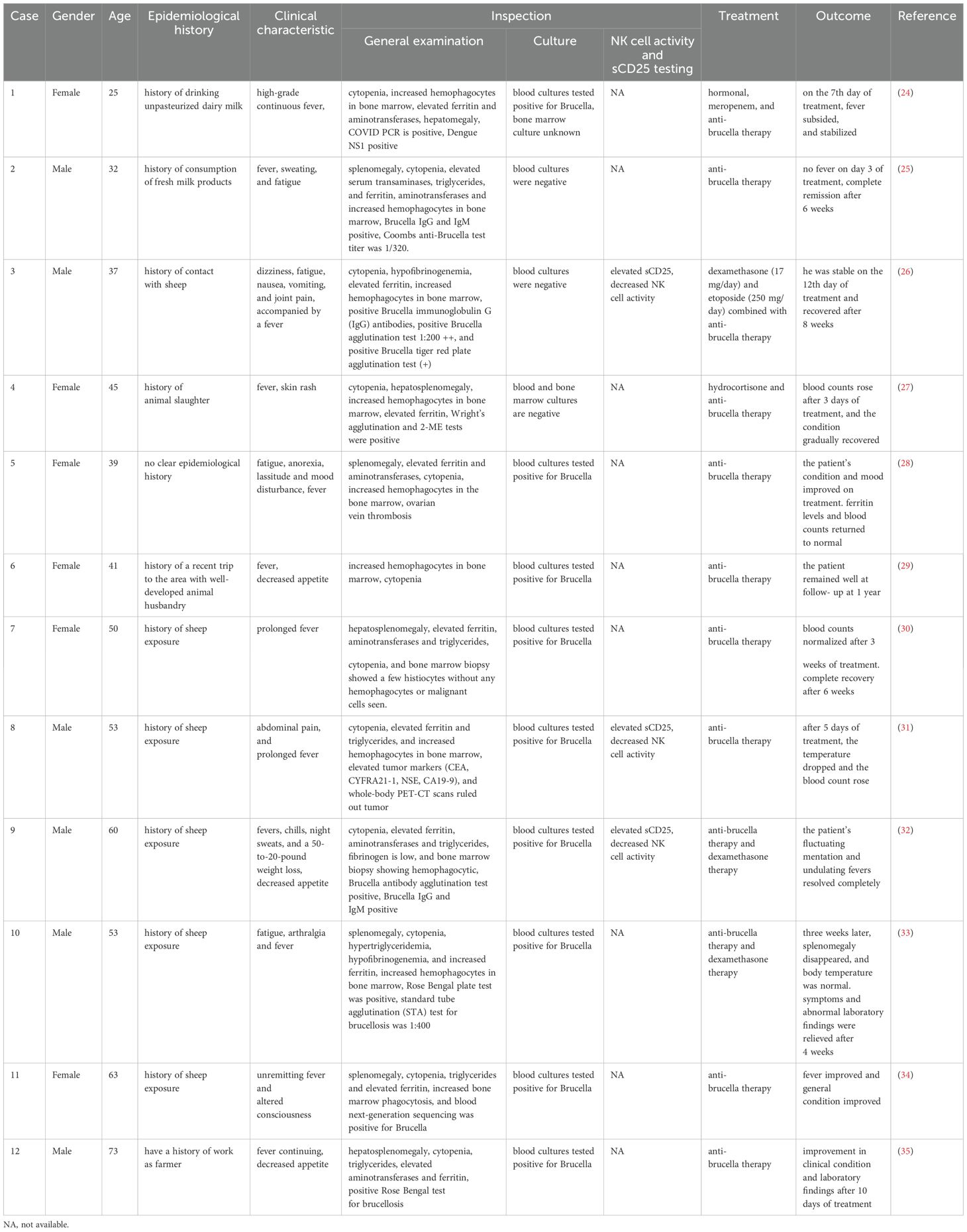
Table 2. Case report and summary of brucellosis complicated with hemophagocytic syndrome.
Brucella-associated HLH progresses rapidly and has a high mortality rate. The prognosis for patients varies based on the severity of the underlying disease and the symptoms presented. Previous studies have indicated that HLH induced by intracellular infections typically does not necessitate HLH-94 therapy and is more effectively treated with specific antimicrobial therapy (36, 37). Among the 12 cases reviewed, 5 patients received a combination of corticosteroids and anti-brucellosis therapy, one patient underwent a regimen of corticosteroids, chemotherapy, and anti-brucellosis treatment, while six patients were managed exclusively with anti-brucellosis therapies (Table 2). Corticosteroids may be avoided in patients who respond quickly to antibiotic therapy and exhibit mild clinical manifestations of HLH. However, in severe cases, especially those complicated by other infections or organ failure. A short course of corticosteroids and/or intravenous immunoglobulin therapy should be considered to manage HLH. Although clear diagnostic criteria for brucellosis combined with HLH are lacking, patients exhibiting clinical features of Brucella-associated HLH require immediate empirical anti-brucellosis therapy. These findings suggest that controlling the primary infection may directly interrupt the pathological process of HLH. Timely intervention significantly reduces the risk of mortality, as delayed treatment can exacerbate organ damage mediated by inflammation storms.
Limitations
As the main type of participants included were case reports, the quality of the studies was not high. This significantly reduces the robustness of the synthesis. Due to the limited data in this review, further similar cases are needed to elucidate this disease.
Summary
Brucella infections cannot be overlooked. HLH associated with brucellosis typically affects children but is increasingly being diagnosed in adults. Brucellosis should be suspected in patients presenting with a fever of unknown origin and pancytopenia, regardless of their epidemiological history. Furthermore, HLH should be included in the differential diagnosis of severe complications arising from brucellosis. To ensure that patients receive effective treatment, clinicians urgently need to establish a clear definition of Brucella-associated HLH for accurate diagnosis. A prospective multicenter cohort study can be conducted to determine the incidence, risk factors, and early prediction models of Brucella-related HLH. Multi-omics analysis can reveal the key immune pathways involved in Brucella-induced HLH, and further investigation to inform targeted therapies.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
LS: Writing – original draft, Validation. BW: Visualization, Writing – original draft. DP: Visualization, Writing – original draft. KZ: Project administration, Supervision, Writing – review & editing, Conceptualization. YW: Conceptualization, Project administration, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Natural Science Foundation of China (No. 81801972 to YW), Science and Technology Research Project of Jilin Provincial Department of Education (JKH20211179KJ to YW), and the Jilin Provincial Natural Science Foundation of Jilin Provincial Department of Science and Technology (20210101341JC to YW).
Acknowledgments
The authors are grateful for the helpful discussions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Griffin G, Shenoi S, and Hughes GC. Hemophagocytic lymphohistiocytosis: An update on pathogenesis, diagnosis, and therapy. Best Pract Res Clin Rheumatol. (2020) 34:101515. doi: 10.1016/j.berh.2020.101515
2. Qureshi KA, Parvez A, Fahmy NA, Abdel Hady BH, Kumar S, Ganguly A, et al. Brucellosis: epidemiology, pathogenesis, diagnosis and treatment–a comprehensive review. Ann Med. (2024) 55:2295398. doi: 10.1080/07853890.2023.2295398
3. Hutchinson M, Tattersall RS, and Manson JJ. Haemophagocytic lymphohisticytosis—an underrecognized hyperinflammatory syndrome. Rheumatology. (2019) 58:vi23–30. doi: 10.1093/rheumatology/kez379
4. Liu Z-g, Wang M, Ta N, Fang MG, Mi JC, Yu RP, et al. Seroprevalence of human brucellosis and molecular characteristics of Brucella strains in Inner Mongolia Autonomous region of China, from 2012 to 2016. Emerging Microbes Infections. (2020) 9:263–74. doi: 10.1080/22221751.2020.1720528
5. Jin M, Fan Z, Gao R, Li X, Gao Z, and Wang Z. Research progress on complications of Brucellosis. Front Cell Infection Microbiol. (2023) 13:1136674. doi: 10.3389/fcimb.2023.1136674
6. Demir C, Karahocagil MK, Esen R, Atmaca M, Gönüllü H, and Akdeniz H. Bone marrow biopsy findings in brucellosis patients with hematologic abnormalities. Chin Med J (Engl). (2012) 125:1871–6.
7. Kaya S, Elaldi N, Deveci O, Eskazan AE, Bekcibasi M, and Hosoglu S. Cytopenia in adult brucellosis patients. Indian J Med Res. (2018) 147:73–80. doi: 10.4103/ijmr.IJMR_542_15
8. Canna SW and Marsh RA. Pediatric hemophagocytic lymphohistiocytosis. Blood. (2020) 135:1332–43. doi: 10.1182/blood.2019000936
9. Mitroulis I, Chrysanthopoulou A, Divolis G, Ioannidis C, Ntinopoulou M, Tasis A, et al. A gene expression map of host immune response in human brucellosis. Front Immunol. (2022) 13:951232. doi: 10.3389/fimmu.2022.951232
10. Wang Y, Yang S, Han B, Du X, Sun H, Du Y, et al. Single-cell landscape revealed immune characteristics associated with disease phases in brucellosis patients. iMeta. (2024) 3:e226. doi: 10.1002/imt2.226
11. Al-Samkari H and Berliner N. Hemophagocytic lymphohistiocytosis. Annu Rev Pathology: Mech Dis. (2018) 13:27–49. doi: 10.1146/annurev-pathol-020117-043625
12. La Rosée P, Horne A, Hines M, von Bahr Greenwood T, Machowicz R, Berliner N, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. (2019) 133:2465–77. doi: 10.1182/blood.2018894618
13. Yagupsky P, Morata P, and Colmenero JD. Laboratory diagnosis of human brucellosis. Clin Microbiol Rev. (2019) 33:e00073-19. doi: 10.1128/cmr.00073-19
14. O’Callaghan D, Xu N, Qu C, Sai L, Wen S, Yang L, et al. Evaluating the efficacy of serological testing of clinical specimens collected from patients with suspected brucellosis. PloS Negl Trop Dis. (2023) 17:e0011131. doi: 10.1371/journal.pntd.0011131
15. Vinetz JM, Loubet P, Magnan C, Salipante F, Pastre T, Keriel A, et al. Diagnosis of brucellosis: Combining tests to improve performance. PloS Negl Trop Dis. (2024) 18:e0012442. doi: 10.1371/journal.pntd.0012442
16. Orduña A, Almaraz A, Prado A, Gutierrez MP, Garcia-Pascual A, Dueñas A, et al. Evaluation of an immunocapture-agglutination test (Brucellacapt) for serodiagnosis of human brucellosis. J Clin Microbiol. (2000) 38:4000–5. doi: 10.1128/jcm.38.11.4000-4005.2000
17. Araj GF. Update on laboratory diagnosis of human brucellosis. Int J Antimicrobial Agents. (2010) 36:S12–7. doi: 10.1016/j.ijantimicag.2010.06.014
18. Jiang H, Feng L, and Lu J. Updated guidelines for the diagnosis of human brucellosis - Chin. China CDC Wkly. (2020) 2:487–9. doi: 10.46234/ccdcw2020.129
19. Elbehiry A, Aldubaib M, Marzouk E, Abalkhail A, Almuzaini AM, Rawway M, et al. The development of diagnostic and vaccine strategies for early detection and control of human brucellosis, particularly in endemic areas. Vaccines. (2023) 11:654. doi: 10.3390/vaccines11030654
20. Pappas G, Akritidis N, Bosilkovski M, and Tsianos E. Brucellosis. N Engl J Med. (2005) 352:2325–36. doi: 10.1056/NEJMra050570
21. Gotuzzo E, Carrillo C, Guerra J, and Llosa L. An evaluation of diagnostic methods for brucellosis–the value of bone marrow culture. J Infect Dis. (1986) 153:122–5. doi: 10.1093/infdis/153.1.122
22. Mantur BG, Mulimani MS, Bidari LH, Akki AS, and Tikare NV. Bacteremia is as unpredictab le as clinical manifestations in human brucellosis. Int J Infect Dis. (2008) 12:303–7. doi: 10.1016/j.ijid.2007.09.004
23. Shehabi A, Shakir K, el-Khateeb M, Qubain H, Fararjeh N, and Shamat AR. Diagnosis and treatment of 106 cases of human brucellosis. J Infect. (1990) 20:5–10. doi: 10.1016/s0163-4453(90)92214-6
24. Kazi AN, Ahmed M, Wasim MA, Abbasi LI, Herekar FF, and Patel MJ. A vector borne, airborne and food borne infection with secondary hemophagocytic lymphohistocytosis: Case of triple infections in an immuno-competent patient. Indian J Med Microbiol. (2024) 52:100752. doi: 10.1016/j.ijmmb.2024.100752
25. El Euch M, Kaabar MY, Bouaziz R, Mahfoudhi M, Jaziri F, Kefi A, et al. Successful resolution of Hemophagocytic lymphohistiocytosis associated to brucellosis in the adult. Tunis Med. (2018) 96:458–61.
26. Xu M, Mo S, and Fu X. Brucella infection-induced hemophagocytic syndrome with subsequent development of the probable vanishing bile duct syndrome: A case report and literature review. SAGE Open Med Case Rep. (2023) 11:2050313X231207562. doi: 10.1177/2050313x231207562
27. Heydari AA, Ahmadi F, Sarvghad MR, Safari H, Bajouri A, and Saeidpour M. Hemophagocytosis and pulmonary involvement in brucellosis. Int J Infect Dis. (2007) 11:89–90. doi: 10.1016/j.ijid.2006.01.003
28. Elzein FE, Al Sherbini N, Alotaibi MM, and Al-Hassan WM. Brucellosis accompanied by haemophagocytic lymphohistiocytosis and multiple splenic abscesses in a patient with depression. BMJ Case Rep. (2018) 1:224018. doi: 10.1136/bcr-2017-224018
29. Zhang Y, Li K, Yang L, and Li T. Bone marrow histiocytic hyperplasia and hemophagocytosis revealing brucellosis. Int J Lab Hematol. (2021) 44:49–50. doi: 10.1111/ijlh.13589
30. Al Noumani J, Al Busaidi I, and Al Hajri M. Brucellosis-induced hemophagocytic lymphohistiocytosis. Cureus. (2021) 13:e15677. doi: 10.7759/cureus.15677
31. Yin X, Li Y, Zeng L, Yu N, Song S, Zhang W, et al. Acute brucellosis with typical hemophagocytic lymphohistiocytosis accompanying elevated tumor markers. Arch Iran Med. (2014) 17:722–3.
32. Park D, Yoon K, Lo A, and Bolos D. Hemophagocytic lymphohistiocytosis induced by brucellosis: A case report. Cureus. (2024) 7:e64287. doi: 10.7759/cureus.64287
33. Jin JG. Fludarabine is effective in treating refractory hemophagocytic lymphohistiocytosis with brucellosis. Int J Rheum Dis. (2017) 20:2256–7. doi: 10.1111/1756-185x.12995
34. Guo M, Zhang L, Chen K, Huang D, Feng C, Liu H, et al. Hemophagocytic lymphohistiocytosis associated with brucellosis. Diagn Microbiol Infect Dis. (2024) 109:116289. doi: 10.1016/j.diagmicrobio.2024.116289
35. Aydın S, Günal Ö, Taşkın MH, Atilla A, and Kılıç SS. Brucellosis as a cause of hemophagocytic syndrome. Mikrobiyol Bul. (2015) 49:292–4. doi: 10.5578/mb.9332
36. Schram AM and Berliner N. How I treat hemophagocytic lymphohistiocytosis in the adult patient. Blood. (2015) 125:2908–14. doi: 10.1182/blood-2015-01-551622
Keywords: brucellosis, hemophagocytic syndrome, pancytopenia, diagnosis, anti-brucellosis therapy
Citation: Shi L, Wang B, Peng D, Zhang K and Wang Y (2025) Brucella-associated hemophagocytic syndrome: case report of a potentially life-threatening condition and literature review. Front. Immunol. 16:1592089. doi: 10.3389/fimmu.2025.1592089
Received: 12 March 2025; Accepted: 07 July 2025;
Published: 25 July 2025.
Edited by:
Changyong Cheng, Zhejiang A & F University, ChinaReviewed by:
M. Victoria Delpino, CONICET Instituto de Investigaciones Biomédicas en Retrovirus y SIDA (INBIRS), ArgentinaLauren Wood Stranahan, Texas A and M University, United States
Nazan Tuna, Namik Kemal University, Türkiye
Copyright © 2025 Shi, Wang, Peng, Zhang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: KaiYu Zhang, a2FpeXVAamx1LmVkdS5jbg==; Yang Wang, d3lhbmdAamx1LmVkdS5jbg==
†These authors have contributed equally to this work