 Rolf Weimer1*
Rolf Weimer1* Hristos Karakizlis1
Hristos Karakizlis1 Fabrice Renner1
Fabrice Renner1 Hartmut Dietrich1
Hartmut Dietrich1 Volker Daniel2
Volker Daniel2 Caner Süsal2,3Christian Schüttler4Daniel Kämper1
Caner Süsal2,3Christian Schüttler4Daniel Kämper1 Dominik Leicht1Michael Wörlen1Katrin Milchsack1Lene Renner1Maximilian Stich1Hermann-Josef Gröne5,6
Dominik Leicht1Michael Wörlen1Katrin Milchsack1Lene Renner1Maximilian Stich1Hermann-Josef Gröne5,6 Andreas Hecker7Rüdiger Hörbelt7Winfried Padberg7Gerhard Opelz2
Andreas Hecker7Rüdiger Hörbelt7Winfried Padberg7Gerhard Opelz2- 1Department of Internal Medicine, University of Giessen, Giessen, Germany
- 2Institute of Immunology, University of Heidelberg, Heidelberg, Germany
- 3Transplant Immunology Research Center of Excellence TIREX, Koç University School of Medicine, Istanbul, Türkiye
- 4Institute of Medical Virology, University of Giessen, Giessen, Germany
- 5Medical Faculty, University of Heidelberg, Heidelberg, Germany
- 6Institute of Pharmacology, University of Marburg, Marburg, Germany
- 7Department of Surgery, University of Giessen, Giessen, Germany
Background: An increased risk of severe infectious disease and acute antibody-mediated rejection (AMR) has been described after ABOi renal transplantation. We performed a prospective renal transplant study up to 5 years posttransplant to detect long-term immunological effects of rituximab administration.
Methods: Mononuclear cell subsets in peripheral blood, regional lymph nodes and protocol biopsies, in-vitro T and B cell responses, serum sCD30 and neopterin were assessed in 85 renal transplant recipients (living donation: n=25 ABOi, n=30 ABO compatible (ABOc); deceased donation (DD): n=30, all ABO compatible), and IgG anti-HLA antibodies by single antigen assay in ABOc and ABOi patients.
Results: An increased frequency of severe infectious diseases in ABOi recipients (doubled versus ABOc within 2 years, P = 0.042) coincided with profoundly downregulated peripheral blood B cell subsets for at least 2 years, impaired in-vitro B cell responses (T-dependent: 2 years, versus ABOc: P = 0.004) and significantly lower CD4+ and CD8+ T cell counts (versus ABOc; 6 months, P = 0.046 and 3 months, P = 0.011, respectively). In regional lymph nodes, we found a significant downregulation of naive B cells (P = 0.031) and short lived plasma cells (P<0.0005) at the time of transplantation. In protocol graft biopsies, rituximab induced B cell depletion at 3 months (P<0.001), but counter-regulatory enhanced counts of T cells (P = 0.041), macrophages (P = 0.021) and plasma cells (P = 0.033) at 1 year. This immune activation was associated with a temporary rise in neopterin levels (P ≤ 0.024 versus ABOc, day 14 until 1 year), CD4 helper activity (P = 0.019 versus ABOc at 2 years) and NK cell counts (P = 0.034 versus ABOc, 4 years; P ≤ 0.040 versus DD, 3–5 years), a missing impact of rituximab on sCD30 levels and HLA antibody formation, and an increased frequency of biopsy-proven acute rejection (3–12 months, P = 0.003) and AMR (P = 0.008 within 5 years).
Conclusions: An increased frequency of severe infectious diseases in ABOi renal transplant recipients may be explained by rituximab-induced long-term immunological effects on CD4+ and CD8+ T cell counts and the prolonged depletion of B cell subsets together with compromised B cell responses. In protocol graft biopsies, rituximab induced early B cell depletion but counter-regulatory proinflammatory effects coinciding with an increased acute rejection frequency.
Registration Details: ClinicalTrials.gov, identifier NCT01136395; EudraCT, identifier No.: 2009-012198-36.
1 Introduction
Rituximab has been proven to suppress anti-ABO titer rebound in ABOi renal transplantation. However, an increased risk of severe infectious disease (1–3) and AMR (2, 3) has been described after ABOi compared to ABOc renal transplantation in two meta-analyses (2, 3) and by CTS registry data (1), respectively. In both meta-analyses, AMR was more frequent in ABOi renal transplantation, whereas overall biopsy-proven acute rejection was found to be more frequent only by de Weerd and Betjes (2). CTS data showed a significantly but only slightly decreased ABOi patient survival in the first posttransplant year only, which was caused by early severe infectious complications (1). In the meta-analysis of de Weerd and Betjes (2), usually rituximab was used as induction in ABOi patients. Studies using splenectomy – known for increased rates of severe infectious complications - were excluded. They also found a small 1% decline of 1-year patient survival and a significantly increased rate of severe nonviral infections, slightly increased CMV viremia and conflicting results regarding BK viremia. Scurt et al. (3) found an increased mortality in ABOi patients up to 5 years posttransplant compared to ABOc patients, and in the rituximab treated subgroup of ABOi patients up to 3 years. Sepsis was more frequent in ABOi patients, whereas the rituximab treated ABOi subgroup did not show an increased risk of infectious complications, and only a trend for a higher risk of BK-virus associated nephropathy. A more recent meta-analysis (4) found rather high rates of infectious complications in 5 of the 15 extracted studies, but detailed data are lacking and rejection data are not provided.
Aim of this prospective pilot study is to assess short- and long-term effects of rituximab induction in ABOi renal transplant recipients and of living compared to deceased donation on immunological parameters of graft outcome and on viral replication. The focus of the current presentation is to detect short-term and especially long-term immunological effects of rituximab induction on graft outcome in ABOi renal transplantation. For this purpose, we analyzed clinically relevant immune parameters such as CD4 helper activity, in-vitro B cell responses, serum sCD30 and neopterin levels, HLA antibody formation and protocol biopsies in a prospective renal transplant study up to 5 years posttransplant.
2 Materials and methods
2.1 Patient groups
In this non-randomized, prospective, open pilot study (phase 2 study; off-label use of rituximab) 30 consecutive deceased brain-death donor (DD) renal transplant recipients (ABO blood group compatible (ABOc); allocation by Eurotransplant), 30 consecutive ABOc and 25 consecutive ABO incompatible (ABOi; with rituximab induction) living donor renal transplant recipients of the Giessen transplant center were included in the study between January 2010 and May 2014; follow-up was 5 years. Inclusion criteria were adult renal transplant recipients, first or retransplants, and informed study consent. Exclusion criteria were combined transplants of more than one organ and contraindications against study drugs. Primary endpoints were immune parameters relevant for transplant outcome (CD4 helper activity, in-vitro B cell responses, serum sCD30 and neopterin levels), HLA antibody formation and counts and distribution of immune cells in protocol biopsies. Secondary endpoints were patient and graft survival, graft function and proteinuria, incidence of acute rejections and of severe infectious diseases. Maintenance immunosuppressive (intention-to-treat) treatment consisted of tacrolimus (Tacr; Prograf®) with early switch to Tacr-MR (modified release; Advagraf®), enteric-coated mycophenolate sodium (Myfortic®) and prednisolone according to the Giessen protocol. In ABOi patients, maintenance immunosuppression was started one day before the first immunoadsorption (IA; blood group specific IA, in case of donor-specific HLA antibodies (DSA) blood group unspecific IA). IA was performed pretransplant usually every other day to reach a target anti-ABO titer of 1:8, and posttransplant only if anti-ABO titers exceeded 1:8 in the first and 1:16 in the second week posttransplant. Induction therapy consisted of rituximab (Mabthera®; 375mg/m2) in ABOi patients (2–4 weeks before transplantation according to the baseline anti-ABO titer; a second or third administration of the standard dosage was allowed if no complete B cell depletion (<8 B cells/µl of peripheral blood) was achieved or the target anti-ABO titer could otherwise not be reached) and generally of basiliximab (Simulect®). Instead of basiliximab, prophylactic rabbit ATG (rATG; Fresenius, Oberursel, Germany; 9mg/kg preoperatively, 3mg/kg days 1–3 according to CD3 counts) was given in patients with maximum panel reactive antibodies (PRA) ≥20% or retransplantation. 10g IVIG was given in DD and ABOc patients pretransplant and on days 1,2 and 4 posttransplant. In ABOi patients, 0.5g/kg IVIG was given 4 days pretransplant, after testing of anti-ABO titers in 3 different IVIG preparations.
The patient groups were comparable with respect to most of the clinical features and transplant data including donor and recipient age, immunization events, induction therapy (with the exception of rituximab administration; Table 1), maintenance immunosuppression (Table 1), renal diseases (P = 0.143; data not shown; low incidence of diabetic nephropathy (n=7/85 (8%))), and pretransplant cytomegalovirus (CMV) serostatus of donors and recipients (P = 0.107; data not shown). As expected, preemptive transplants were more frequent and waiting times were shorter in living versus DD renal transplant recipients (with differences between ABOi and ABOc patients not reaching statistical significance; Table 1), as were shorter cold ischemia times and the worse HLA matching compared to DD patients.

Table 1. Clinical features and transplant data of patients who received a renal graft from a living donor (ABOc, blood group compatible; ABOi, blood group incompatible) and from a deceased donor (DD; blood group compatible), respectively.
All patients at high CMV risk (CMV-IgG positive donor and negative recipient; rATG treatment) received valganciclovir prophylaxis for 6 months. Oral cotrimoxazole and pentamidine inhalation, respectively, was used in all patients for pneumocystis jiroveci prophylaxis (9 months). Rituximab treated patients received fluconazole prophylaxis (14 days posttransplant) in addition, and an antiviral prophylaxis with valaciclovir (3 months) and valganciclovir in high CMV risk patients (6 months), respectively. Immunological tests were performed pretransplant (in ABOi recipients also before rituximab administration), 14 days, 3 and 6 months and 1, 2, 3, 4 and 5 years posttransplant.
2.2 Flow cytometric analysis of peripheral blood mononuclear cells
PBMC subsets and their expression of costimulatory ligands were determined by double- and triple-fluorescence (triple fluorescence for the indicated B cell subsets) and laser flow-cytometry as described previously (5, 6). The following monoclonal antibodies (MoAb) were used: anti-CD4-FITC, anti-CD4-PE, anti-CD4-PE-Cy7, anti-CD8-FITC, anti-CD14-FITC, anti-CD19-FITC, anti-CD20-FITC, anti-CD25-PE, anti-CD28-PE and anti-CD40-PE (Becton Dickinson (BD), Heidelberg, Germany). Mouse IgG1-PE (BD) was used as isotype control. For detection of B cell subsets, anti-CD19-FITC/anti-CD27-PE/anti-CD20-PE-Cy7, anti-CD19-FITC/anti-CD22-PE/anti-CD20-PE-Cy7 and anti-CD19-FITC/anti-CD138-PE/anti-CD38-PE-Cy7 were used together with anti-CD19-FITC/mouse IgG1-PE/mouse IgG1-PE-Cy7 as isotype controls (all antibodies from BD).
Simultest IMK-Lymphocyte (BD) reagents and software were used to detect granulocytes, PBMC, monocytes (CD14+), lymphocytes, NK cells (CD3-CD16+ and/or CD56+), CD3+ T cells, CD4+ T cells, CD8+ T cells and CD19+ B cells in peripheral blood. Absolute cell counts were assessed using BD Trucount tubes (BD) according to the manufacturer´s protocol.
FoxP3+ Tregs (FoxP3+ CD25+ CD4 cells) in peripheral blood were determined essentially according to the manufacturer´s protocol (lysed whole blood cells were used instead of isolated PBMC) using the following MoAbs: anti-human FoxP3-PE (clone 259D/C7; BD), anti-human CD25-PE-Cy7 (clone M-A251, BD) and anti-human CD4-FITC (clone RPA-T4; BD). Mouse IgG1-PE and mouse IgG1-PE-Cy7 (BD) were used as isotype controls, and anti-CD4-FITC, anti-CD4-PE and anti-CD4-PE-Cy7 (BD) for compensation of the flow cytometer. The Human FoxP3 Buffer Set (BD) was applied to fixation and permeabilization of lysed whole blood cells, staining of the given cell surface markers and intracellular staining of Human FoxP3. BD CellWash (BD) with 2% fetal calf serum was used as a modified staining buffer. Tregs (CD25high CD127low CD4 cells) in peripheral blood were determined using the following MoAbs: anti-CD4-FITC (BD)/anti-CD25-PE (BD)/anti-CD127-PE-Cy7 (eBioscience, Thermo Fisher Scientific GmBH, Munich, Germany) and anti-CD4-FITC/mouse IgG1-PE/mouse IgG1-PE-Cy7 (BD) as isotype controls.
Measurements were performed using a FACSCalibur flow cytometer (BD). Exclusion of dead cells was done by forward and side-scatter gating. 100,000 mononuclear cells were typically acquired for analysis. Results are given in % of gated cells and molecules of equivalent phycoerythrin (MEPE) for indicated parameters (those showing better discrimination from isotype controls by MEPE), respectively. MEPE describes the molecule density per cell and was calculated by comparing staining of samples with a standard curve. Individual standard curves were established for each assessment by analysis of a mixture of 8 calibrated bead populations containing 8 different MEPE levels per bead (Sphero Rainbow Calibration Particles, 8 peaks, 3.0-3.4 µm; BD). The results were calculated by subtracting the respective isotype controls results.
2.3 Serum sCD30 and neopterin
Sera were thawed and tested by ELISA for sCD30 (Bender MedSystems, Vienna, Austria) and neopterin (Brahms, Berlin, Germany). Neopterin values were corrected for graft function by dividing values by the serum creatinine (Neopterin/S-Cr, given in nmol/g S-Cr (5)).
2.4 Flow cytometric analysis of iliac lymph nodes
One regional (iliac) lymph node - removed during transplant surgery - was dissected with scissors and scalpel, rinsed with staining buffer (BD CellWash (BD) with 2% fetal calf serum (BD)) and passed through a 40µm sieve. After washing, the resulting cell suspension (107/ml) was stained as described above for PBMC (Simultest IMK-Lymphocyte kit (BD); staining of B cell subsets and Tregs (CD25high CD127low CD4 cells)).
2.5 PWM-stimulated allogeneic cocultures and SAC I-stimulated B cell cultures
T-cell dependent B cell responses of PWM-stimulated allogeneic cocultures of patient B and control T cells, T-independent B cell responses of SAC I-stimulated B cell cultures and helper and suppressor activity of whole T cells and CD4+ T cells, respectively, were determined as described previously (5–7).
2.6 IgG anti-HLA antibodies
IgG anti-HLA antibodies were assessed on a Luminex basis in ABOc and ABOi recipients pretransplant and 3 and 6 months, and 1, 2, 3, 4 and 5 years posttransplant. LABScreen™ Mixed Class I & II (One Lambda, West Hills, CA, US) was used for screening, and single antigen assays were used in case of positive screening results (LABScreen™ Single Antigen Class I, LABScreen™ Single Antigen Class II; One Lambda). This analysis was not done in DD recipients, as the full HLA donor typing (9 loci) was not available.
2.7 Immunohistochemistry of protocol biopsies
Protocol biopsies were generally recommended 3 and 12 months posttransplant and were performed at 3 months in 58 of 83 patients with functioning grafts (70%; 22/30 (73%), ABOc; 15/23 (65%), ABOi; 21/30 (70%), DD) and at 12 months in 34 of 82 (41%; 14/30 (47%), ABOc; 9/22 (41%), ABOi; 11/30 (37%), DD) patients. Immunohistochemistry was performed as described previously (8). For immunostaining, we used primary antibodies against CD3 (monoclonal rabbit anti-CD3, ab135372, clone SP162, 1:200; Abcam, Cambridge, UK), CD19 (monoclonal rabbit anti-CD19, ab134114, clone EPR5906, 1:250; Abcam), CD20 (monoclonal mouse anti-CD20cy, M0755, clone L26, 1:200; Dako/Agilent), CD38 (monoclonal rabbit anti-CD38, ab183326, clone SP149, 1:100; Abcam), CD68 (monoclonal mouse anti-CD68, MO876, clone PG-M1, 1:100; Dako/Agilent), CD138 (monoclonal mouse anti-CD138, ab128936, clone EPR 6454, 1:700; Abcam), FoxP3 (monoclonal mouse anti-FoxP3, ab20034, clone 236A/E7, 1:50; Abcam) and SV40 T-antigen (monoclonal mouse anti-SV40T, clone PAb416, 1:200 Millipore/Merck, Darmstadt, Germany), respectively. Visualization was performed using the Dako REAL Detection System (alkaline phosphatase/red for rabbit and mouse antibodies; K5005; Dako/Agilent).
Biopsy samples were scanned using a Hamamatsu Scanner (Nanozoomer 2.0 RS, Hamamatsu Photonics, Japan). Manual evaluation of the data files was performed using the NDP.view 2.7.39 software (free edition). For quantitative analysis, results were given in cells per mm2 of biopsy area. Semiquantitative estimation of distribution patterns was analyzed for CD3+ T cells, FoxP3+ Treg, CD19+ B cells and CD20+ B cells (given in % of biopsies with missing or very rare occurrence versus diffuse infiltration versus focal infiltration versus nodular infiltration) and for plasma cells (% of biopsies with missing versus scattered occurrence versus focal infiltration).
2.8 Virological screening
BK and JC virus screening was performed by an in-house real time PCR (9) with hybridization probes in serum and urine specimens pretransplant (serum testing only), 3 and 6 months, and 1,2,3,4 and 5 years posttransplant. JC viremia was not detected. CMV PCR (Artus CMV LC PCR Kit, No. 4503065, Qiagen, Hilden, Germany) screening was performed in serum at the same time points.
2.9 Statistics
Data are presented as means and SEM. Wilcoxon signed-rank test, Mann-Whitney U test, Kruskall-Wallis H test and Chi-square or Fisher`s exact test were used for statistical analysis. A 0.05 significance level was defined for univariate testing.
3 Results
3.1 Patient and graft outcome
We found no significant differences in patient and graft survival between the three patient groups, although no patient death occurred in ABOc patients in contrast to 3 deaths in ABOi and also in DD patients during the 5-year posttransplant follow-up (details given in Table 2). 5-year death-censored graft survival, graft function and proteinuria were also comparable between the patient groups (Table 2), whereas 1-year graft function (but not proteinuria, P = 0.370) was significantly different (ClCr: 74 ± 4 ml/min, ABOc; 62 ± 5 ml/min, ABOi; 56 ± 5 ml/min, DD; P = 0.031; ABOc versus DD, P = 0.011; other comparisons between two patient groups: not significant). We found no significant differences between the measured creatinine clearance values (mean of two calculations) of ABOc and ABOi living kidney donors (116 ± 2 ml/min, ABOc versus 117 ± 4 ml/min, ABOi; P = 0.660).

Table 2. Five year outcome in the ABOc and ABOi living-donor and the deceased donor (DD) patient groups.
These data imply a surprisingly good outcome in the DD patient group, which, perhaps importantly, showed comparable recipient and donor age and also immunization events, but better HLA compatibility compared to ABOc and ABOi patients (Table 1). Only one DD patient was transplanted via the Eurotransplant senior program.
Clinical outcome data regarding acute rejection and infectious complications are remarkable despite the relatively low patient numbers in each of the patient groups. Although usually acute rejections occur more frequently in the first three months posttransplant, we found a significantly increased frequency of acute rejections between 3 and 12 months posttransplant in ABOi compared to ABOc and DD patients (6/23 (26%), ABOi; 1/30 (3%), ABOc; 0/30 (0%), DD; P = 0.002; ABOi versus ABOc, P = 0.034; ABOi versus DD, P = 0.004), but no differences in other posttransplant periods (Table 2). Overall, the 1-year acute rejection incidence was increased in ABOi versus ABOc patients (8/24 (33%) versus 3/30 (10%), P = 0.046), whereas statistical comparison of all three patient groups did not reach significance (P = 0.067, Table 2). When rituximab treated ABOc and DD patients were excluded (n=4 (2 pretransplant administrations), ABOc; n=3 (1 pretransplant), DD; details see Table 2), 5-year acute AMR but not AIR incidence was significantly increased in ABOi patients (P = 0.008; Table 2). It has to be considered, however, that pretransplant rituximab was given in 3 non-ABOi patients because of an increased rejection risk due to donor-specific HLA antibodies.
3.1.1 Infectious complications
Noteworthy, severe infectious diseases occurred twice often in ABOi compared to ABOc patients in the first two years posttransplant but not beyond (P=0.042; Table 2). Urinary tract infection (especially urosepsis) was the most frequent severe infectious disease. Types of severe infections did not differ significantly between the groups (Table 2) and also not between overall rituximab treated versus non-treated patients (data given for urosepsis in Table 2). CMV disease was numerically less frequent in ABOi compared to ABOc and DD patients (Table 2), possibly due to antiviral prophylaxis performed in all ABOi patients. BK viremia was somewhat more frequent in ABOi compared to ABOc and DD patients, but differences did not reach statistical significance (Table 2). The incidence of BK-virus associated nephropathy was less than 10% in all patient groups.
3.2 PBMC subsets, costimulatory ligand expression and Tregs
The increased risk of severe infectious complications within the first 2 years posttransplant coincided with lower peripheral blood T cell counts in ABOi versus ABOc recipients up to 6 months (CD4+ T cells: 3 months, P = 0.025; 6 months, P = 0.046; CD8+ T cells: 3 months, P = 0.011; 6 months, not significant P = 0.095; Table 3), whereas no significant differences were found between ABOi and DD patients. CD25 (IL-2R alpha) and CD28 costimulatory ligand expression on T cells was comparable between ABOi and ABOc patients but significantly different compared with DD patients (lower CD25 expression on CD4+ T cells (P = 0.013, 3 months); increased CD28 expression on CD4+ T cells (P = 0.001, 1 year; P = 0.018, 2 years; P = 0.032, 5 years) and CD8+ T cells (P = 0.006, 1 year; P = 0.056, 2 years; P = 0.013, 5 years); Table 3). FoxP3+ Treg counts were slightly, but significantly lower in DD patients at 1 and 2 years posttransplant (1 year, P = 0.028 versus ABOc; 2 years, P = 0.043 versus ABOi; Table 3) without significant differences between ABOc and ABOi patients. However, CD25high CD127 low Treg showed no significant differences between the 3 patient groups (Table 3). Pretransplant rituximab induction showed no impact on Tregs, as shown by comparison of Treg levels in ABOi patients before ritxumab induction with pretransplant levels (21 ± 2 days after administration; before start of other immunosuppressive drugs). Interestingly, NK cell counts were significantly increased in ABOi versus ABOc recipients at 4 years (P = 0.034) and versus DD patients 3–5 years posttransplant (P = 0.017, 3 years; P = 0.024, 4 years; P = 0.040, 5 years), whereas NK cell counts of ABOc and DD patients were comparable (Table 3).
3.3 B cell repopulation after rituximab administration
After rituximab induction in ABOi recipients, all of the presented B cell subsets in peripheral blood declined significantly before start of any other immunosuppressive treatment. B cells were virtually absent up to 1 year posttransplant and the profound downregulation of the B cell subsets lasted at least 2–3 years, most pronounced with regard to memory B cells (for 4 years; Figure 1). At 2 years posttransplant, most of the B cell subsets in ABOi patients reached about 50% of the counts in ABOc or DD patients (Figure 1), whereas memory B cells were scarcely found (19 ± 4/µl, ABOc; 2 ± 0/µl, ABOi; 15 ± 3/µl, DD; P<0.0005). At 3 years posttransplant, ABOi patients still showed reduced counts of naive B cells (P = 0.025 versus ABOc), mature B cells (P = 0.028 versus ABOc, P = 0.023 versus DD) and short lived plasma cells (P = 0.023 versus ABOc, P = 0.053 versus DD). Interestingly, B cell CD40 costimulatory ligand expression in ABOi patients was significantly downregulated 1 year and 2 years posttransplant (no analysis performed earlier due to low B cell counts) compared to DD patients (P = 0.003, 1 year; P = 0.024, 2 years; Table 3) without significant differences between ABOc and ABOi patients. ABOc patients also showed reduced B cell CD40 expression compared to DD patients 1 to 5 years posttransplant (3 months, P = 0.454; 1 year, P = 0.020; 2 years, P = 0.004; 5 years, P = 0.041) thereby excluding an impact of rituximab on the downregulated CD40 expression. In ABOi patients, B cell CD25 expression was slightly reduced only at 1 year posttransplant (P = 0.036 versus ABOc; Table 3).

Figure 1. Peripheral blood B cell subsets (CD19+ B cells, CD20+ B cells, memory B cells (CD27+ CD19+ cells), naive B cells (CD27- CD19+ cells), mature B cells (CD22+ CD19+ cells) and short lived plasma cells (CD19+ CD38+ CD138- cells)) in ABO incompatible (ABOi; red line) and ABO compatible (ABOc; blue line) living donor renal transplant recipients, and in DD renal transplant recipients (DD; green line) before rituximab administration (pre Rtx; in ABOi patients), pretransplant (pretpl; before start of any other immunosuppressive treatment), 3 und 6 months, and 1,2,3,4 and 5 years postttransplant. Long lived plasma cells (CD19- CD38+ CD138+ cells) were only occasionally found (mean frequencies of 1±0 up to 2±1 cells/μl) in all patient groups and were therefore not included in the diagram. Mean and SEM are indicated. P values are given for statistically significant differences between the patient groups (Kruskall-Wallis H test). After rituximab induction in ABOi recipients, all of the presented pretransplant B cell subset counts (obtained before start of any other immunosuppressive treatment) showed a significant decline compared to the counts before rituximab administration (P<0.0005). This resulted in profoundly downregulated peripheral blood B cell subset counts in ABOi recipients compared to ABOc and DD patients for at least 2-3 years, most pronounced with regard to memory B cells (even 4 years).
3.4 CD4 helper activity, in-vitro B cell responses
The prolonged downregulation of B cell subsets after rituximab induction in ABOi recipients coincided with impaired in-vitro B cell responses up to 2 years posttransplant (T-dependent: 3 months, P = 0.041 vs. ABOc, P = 0.021 vs. DD; 1 year, not significant (P = 0.111 vs. ABOc, P = 0.075 vs. DD); 2 years, P = 0.004 vs. ABOc, P = 0.012 vs. DD; T-independent: 3 months and 1 year, not significant; 2 years, P = 0.053 vs. ABOc, P = 0.657 vs. DD; Table 3). CD4 helper and suppressor activity was comparable between the patient groups with the exception of the 2 year posttransplant time point (lower CD4 helper function in ABOc vs. ABOi (P = 0.019) and DD patients (P = 0.007); lower CD4 suppressor function in DD vs. ABOi (P = 0.034) and ABOc patients (P = 0.007; Table 3 and Figure 2).

Table 3. Peripheral blood granulocytes and mononuclear cell subsets (PBMC), expression of costimulatory ligands, helper and suppressor activity of whole T cells and CD4+ T cells, in-vitro T cell-independent and T cell-dependent B cell responses (immunoglobulin-secreting cell (ISC) formation) and serum sCD30 and neopterin levels in living-donor ABO-compatible (ABOc), ABO-incompatible (ABOi) and deceased-donor ABO-compatible (DD) renal transplant recipients before rituximab administration (in ABOi patients), pretransplant and at different time points up to 5 years posttransplant.
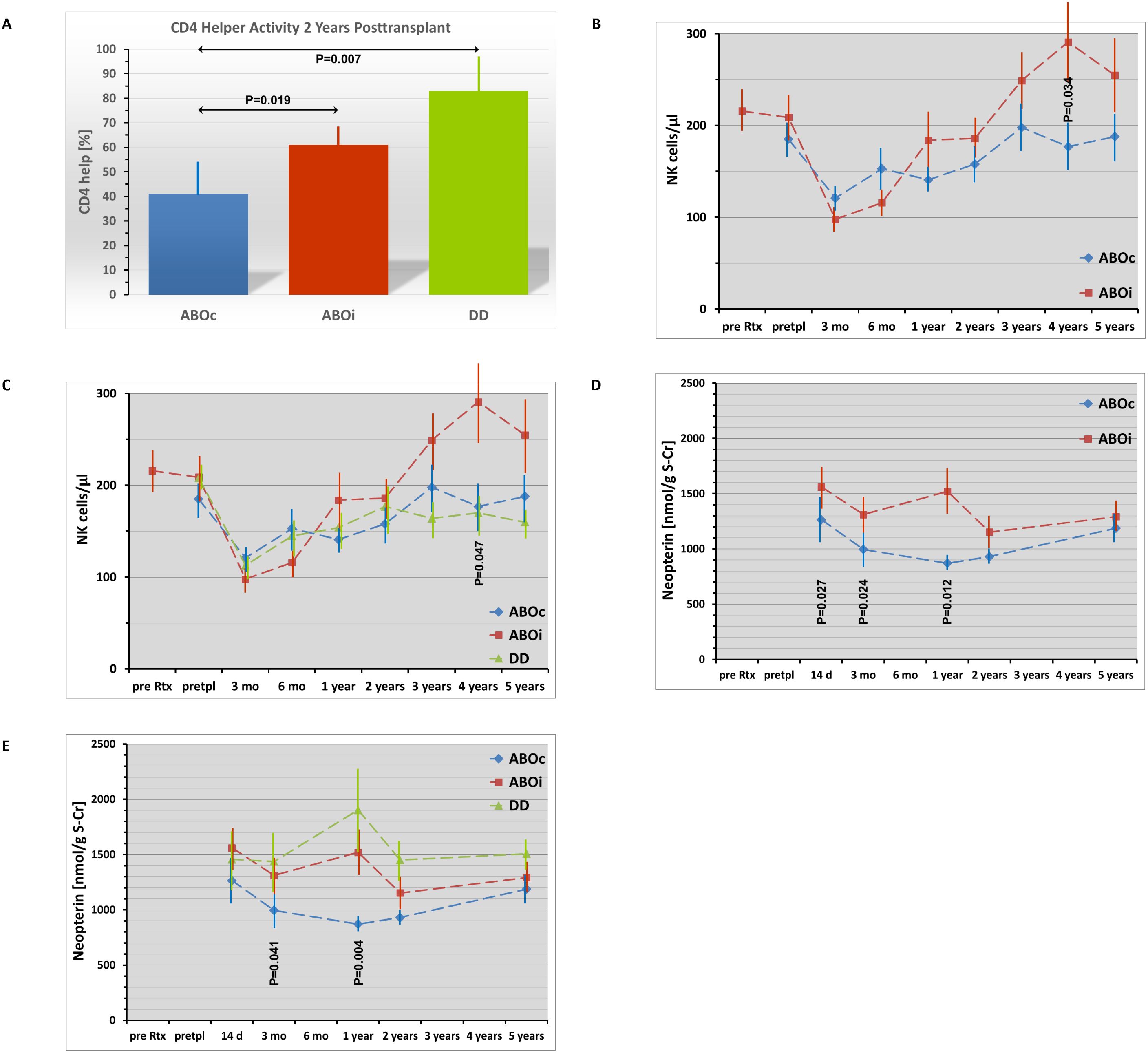
Figure 2. Temporary immune activation in ABO incompatible (ABOi; marked in red) compared to ABO compatible (ABOc; marked in blue) living donor renal transplant recipients shown for CD4 helper activity at 2 years posttransplant (A) and for peripheral blood NK cell counts (B, C) and serum neopterin (D, E) during the 5-year posttransplant follow-up (pre Rtx: before rituximab administration in ABOi patients; pretpl: pretransplant, before start of any other immunosuppressive treatment). Mean and SEM are indicated. P values are given for statistically significant differences between the patient groups. Kruskall-Wallis H Test was used for statistical comparison of the three patient groups, Mann-Whitney U Test (Wilcoxon rank-sum test) for statistical comparison between 2 of the 3 patient groups. The numerically increased CD4 helper activity in ABOi versus ABOc patients did not reach statistical significance at 1 year (P=0.077) but did at 2 years (P=0.019; Figure 2A) followed by comparable helper activity at 5 years (P=0.228; see table 3). Peripheral blood NK cell counts significantly increased at 4 years in ABOi compared to ABOc patients (Figure 2B) and were elevated compared to DD patients at 3 (P=0.017), 4 (P=0.024) and 5 years (P=0.040; overall significant differences between the 3 patient groups only at 4 years, see Figure 2C). Serum neopterin levels showed a temporary increase in ABOi compared to ABOc patients at 14 days up to 1 year posttransplant (Figure 2D) indicating an increased activation of the T cell / monocyte system in this period, whereas DD patients demonstrated significantly elevated serum neopterin levels compared to ABOc recipients 3 months up to 5 years posttransplant (P=0.042, 3 months; P=0.002, 1 year; P=0.038, 2 years; P=0.035, 5 years; Figure 2E) without significant differences between DD and ABOi patients during the complete 5-year follow-up.
3.5 Serum sCD30 and neopterin
In ABOi patients, comparison of serum sCD30 levels before rituximab administration with pretransplant levels (21 ± 2 days later; before start of other immunosuppressive drugs) showed no effect of rituximab an sCD30 levels (P = 0.254; Table 3). Differences of sCD30 levels between the patient groups were found only 1 year (increased levels in DD versus ABOc patients, P = 0.016; Table 3) and 2 years posttransplant (increased levels in DD vs. ABOc and ABOi patients; P = 0.010 and P<0.001, respectively; Table 3). Serum neopterin (corrected for graft function) was increased in ABOi versus ABOc patients 14 days posttransplant (P = 0.027; Figure 2 and Table 3) and in both ABOi and DD patient groups compared to ABOc recipients 3 months (P = 0.024 and P = 0.042, respectively) and 1 year posttransplant (P = 0.012 and P = 0.002, respectively; Table 3). At 2 and 5 years, levels of ABOi and ABOc patients were comparable, whereas DD patients showed elevated levels compared to ABOc patients (P = 0.038 and P = 0.035, respectively; Table 3).
3.6 Flow cytometric analysis of regional lymph nodes
At the time of transplantation, we found a significant rituximab-induced downregulation of CD20+ but not CD19+ B cells (P<0.0005), of naive B cells (P = 0.031) and short lived plasma cells (P<0.0005; Table 4). Thus, the overall rate of B cells appeared not to be reduced after rituximab induction. The low percentage of CD20+ but not of CD19+ B cells may be explained by prevention of CD20 MoAb binding by rituximab coverage of the B cells.

Table 4. Flow cytometric analysis of regional lymph nodes at the time of transplantation in living-donor ABO-compatible (ABOc), ABO-incompatible (ABOi) and deceased-donor ABO-compatible (DD) renal transplant recipients.
3.7 Protocol biopsies
Protocol biopsies were performed in 70% and 41% of patients with functioning grafts at the 3 and 12 month posttransplant time point, respectively (see methods section). Cell subset analysis in these biopsies showed rituximab-induced B cell depletion in ABOi patients at 3 months (P<0.001 vs. ABOc and DD), but comparable B cell counts and even enhanced counts of CD3+ T cells (P = 0.041; ABOi vs. ABOc, P = 0.030; ABOi vs. DD, P = 0.050), CD68+ macrophages (P = 0.021; ABOi vs. ABOc, P = 0.008; ABOi vs. DD, P = 0.051; without a difference in the rate of macrophage infiltrated glomeruli) and CD138+ plasma cells (P = 0.033; ABOi vs. ABOc, P = 0.164 (not significant); ABOi vs. DD, P = 0.043) at 1 year (Table 5). Interestingly, in 2 of 14 (14%) ABOi patients diffuse or focal B cell infiltration was found at 3 months despite rituximab induction, and even nodular infiltration with CD19+ B cells in 3 of 8 (38%) ABOi patients at 1 year together with diffuse or focal plasma cell infiltration in 5 of 7 (71%) patients (Table 5). Treg counts and their pattern of distribution were not significantly different between the patient groups.

Table 5. CD3+ T cells, FoxP3+ regulatory cells, CD68+ macrophages, CD19+ B cells, CD20+ B cells and CD138+ plasma cells in 3 month and 1 year protocol biopsies of living-donor ABO-compatible (ABOc), ABO-incompatible (ABOi) and deceased-donor ABO-compatible (DD) renal transplant recipients.
Remarkably, the percentage of interstitial fibrosis/tubular atrophy (IF/TA, given in % of the renal cortex) was significantly increased in the 1-year protocol biopsies of ABOi recipients (26 ± 6% vs. 8 ± 3% in ABOc and 22 ± 4% in DD patients, P = 0.009), and the frequency of nephrosclerosis was also increased in ABOi patients (6/9 (67%) ABOi vs. 2/14 (14%) ABOc and 4/11 (36%) DD patients, P = 0.038).
3.8 IgG anti-HLA antibodies
IgG anti-HLA antibody formation against class I and II antigens was not significantly different between ABOi and ABOc patients up to 5 years posttransplant (Figure 3). Also no significant differences in HLA antibody formation were found in peripheral blood when patients with early rituximab treatment (all ABOi patients and 3 ABOc patients with treatment pretransplant or up to 4 months posttransplant) were compared with ABOc recipients without early rituximab administration (data not given). One further ABOc patient received posttransplant rituximab from month 43 on because of PTLD and was therefore not included in the early rituximab group. De novo formation of donor-specific HLA antibodies (DSA) occurred in only 1/30 (3%) ABOc and 2/23 (9%) ABOi patients (P = 0.573), whereas pretransplant detectable DSAs (in 6/30 (20%) ABOc vs. 8/25 (32%) ABOi patients; P = 0.363) were lost in 4 of the 6 (67%) ABOc and 7 of the 8 (88%) ABOi patients (P = 0.538), respectively, usually within 6 months posttransplant. Thus, no significant impact of rituximab induction on IgG anti-HLA antibody formation was found, also no impact on de-novo HLA antibody formation nor on disappearance of pretransplant HLA antibodies. However, due to the low numbers of de-novo DSA formation and pretransplant DSA disappearance, these data do not prove the absence of a relationship.
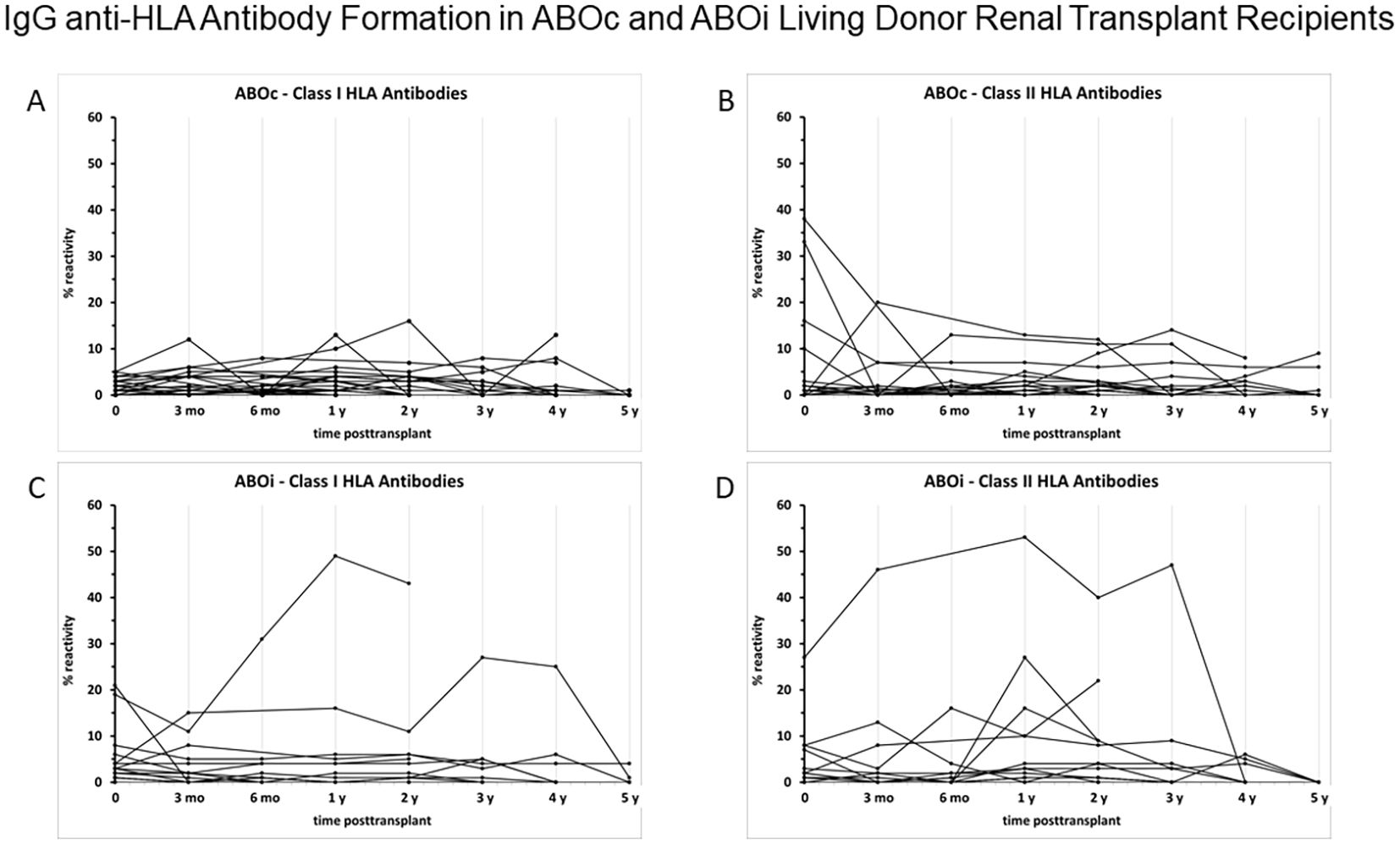
Figure 3. IgG anti-HLA antibody formation in ABOc (A: class I; B: class II) and ABOi living donor renal transplant recipients (C: class I; D: class II) pretransplant, 3 and 6 months, and 1,2,3,4 and 5 years posttransplant. IgG anti-HLA antibodies were assessed by single antigen assay on a Luminex basis in ABOi patients (all with rituximab administration pretransplant) and ABOc patients. Three of the ABOc patients received rituximab in the first 4 months postttransplant (protocol violation), two because of donor-specific HLA antibodies (IgG and IgM antibodies, respectively) already pretransplant and one patient because of an acute antibody-mediated rejection 4 months posttransplant. Another ABOc patient received rituximab 6 times because of PTLD starting 43 months posttransplant. Statistical analysis (Mann-Whitney U test) showed no significant differences in HLA antibody formation between ABOc and ABOi recipients with the exception of a clinically not meaningful difference of HLA antibody formation against MHC II antigens 5 years posttransplant (1.0±0.5 %, ABOc versus 0.0±0.0 %, ABOi; P=0.048). No significant differences in HLA antibody formation were found, when patients with early rituximab treatment (all ABOi patients and 3 ABOc patients with treatment pretransplant or up to 4 months posttransplant) were compared with living donor renal transplant recipients without rituximab administration (data not shown).
4 Discussion
Newer protocols in blood group incompatible (ABOi) renal transplantation usually use rituximab instead of the previously performed splenectomy pretreatment to suppress anti-ABO titer rebound and anti-ABO associated AMR after ABOi transplantation (10, 11). Rituximab administration was found to improve patient and graft survival compared to pretransplant splenectomy (3, 12). Rituximab has been shown to suppress anti-ABO titer rebound in ABOi renal transplantation. This is also true for suppression of pretransplant anti-ABO titer rebound in so-called high responders, who comprise 10-20% of our patients and do not reach the target anti-ABO titer enabling successful ABOi renal transplantation. We could show that repeated pretransplant rituximab infusions may enable successful ABOi living-donor renal transplantation even in these high responders, without increasing the risk of BK viremia (13). However, an increased risk of severe infectious disease (1–3) and of AMR (2, 3) has been observed after ABOi compared to ABOc renal transplantation. The CTS data (1) described a significantly but only slightly decreased ABOi patient survival in the first posttransplant year only, caused by early severe infectious complications. However, rituximab pretreatment showed no impact on patient survival and also not on death-censored graft survival up to 3 years posttransplant compared to no rituximab treatment. In our current prospective pilot study we confirmed an increased incidence of severe infectious complications, however, only within 2 years posttransplant and not beyond. The incidence of BK viremia in ABOi patients was not significantly elevated, adding to conflicting results in meta-analyses (2, 3). The increased risk of severe infectious complications within 2 years posttransplant in ABOi recipients may be explained by the observed long-term immunological effects after rituximab induction. These comprise downregulated CD4+ and CD8+ T cell counts up to 6 and 3 months, respectively, the profoundly delayed B cell repopulation, most pronounced with regard to memory B cells, and compromised B cell responses found up to 2 years posttransplant. Rituximab-induced B cell elimination together with the observed impaired B cell function may also affect antigen presentation and thereby decrease T-cell activation and infection control. Decreased T cell and CD4+ T cell counts together with impaired CMV-specific T-cell immunity up to 90 days posttransplant has previously been described by Schachtner et al. (14). Thus, antiviral and antifungal prophylaxis is strongly recommended after rituximab induction in ABOi recipients. Pretransplant IVIG is also administered in our center according to the Stockholm and Freiburg ABOi protocols (15, 16). The recommendation of antiviral and antifungal prophylaxis is underlined by data of the Toulouse center (17) showing an increased rate of fungal infections in 77 renal transplant recipients who received rituximab without fungal prophylaxis compared to non-rituximab treated controls. The Hannover transplant center reported an increased incidence of viral infections among 21 consecutive ABOi compared to 47 ABOc renal allograft recipients. ABOi and ABOc patients received CMV prophylaxis in the high risk donor CMV-IgG positive/recipient CMV-IgG negative setting, but no general antiviral prophylaxis with aciclovir or valaciclovir, respectively, or pretransplant IVIG (18).
Meta-analyses of de Weerd and Betjes (2) and Scurt et al. (3) show an increased incidence of AMR in ABOi compared to ABOc patients. Whereas splenectomy patients were involved in the meta-analysis of Scurt et al. (3), de Weerd and Betjes (2) excluded older studies using splenectomy and thus predominantly analyzed rituximab treated ABOi recipients. In contrast to Scurt et al. (3), they also found an increased rate of overall acute rejections in ABOi versus ABOc recipients. Interestingly, in our prospective pilot study with a focus on long-term immunological effects after rituximab induction, we found a low, but significantly increased frequency of AMR in the 5-year follow-up of ABOi versus ABOc and DD recipients, and an increased frequency of overall acute rejections only between 3 and 12 months posttransplant. The lower incidence of acute rejections in the first 3 months posttransplant coincided with the rituximab-induced graft protective effects in regional lymph nodes (decline in naive B cell and short lived plasma cell frequencies) at the time of transplantation and the depletion of B cells in the graft at 3 months posttransplant, whereas evidence of counterregulatory immune activation in 1-year graft biopsies (increase in B cell counts reaching comparable counts with ABOc and DD patients, even enhanced counts of CD3+ T cells, CD68+ macrophages and CD138+ plasma cells) may explain the increased risk of acute rejection between 3 and 12 months posttransplant. The increased AMR frequency in ABOi patients - despite long-term profoundly delayed B cell repopulation together with compromised B cell responses after rituximab induction - may be explained by the missing impact of rituximab on IgG anti-HLA antibody formation, the described immune activation in the graft at 1 year, the increased CD4 helper activity compared to ABOc patients at 2 years when B cell counts were rising, and an increase in NK cell counts 3–5 years posttransplant. Rituximab showed no effect on Tregs in peripheral blood and protocol graft biopsies.
Serum sCD30 and neopterin levels serve as markers of graft outcome. CD30 is an important costimulatory molecule in the regulation of the Th1/Th2 balance and serum sCD30 levels are elevated in diseases with a predominant Th2-type immune response (19). Süsal et al. (20, 21) found that high pretransplant sCD30 levels were associated with impaired kidney graft survival. We showed previously that 1-year serum levels of sCD30 and the T cell/monocyte activation marker neopterin predict graft deterioration by chronic allograft dysfunction (22). In our current study, sCD30 levels in ABOi patients were not significantly elevated compared to ABOc patients, whereas DD patients showed significantly elevated sCD30 levels at 1 year compared to ABOc patients and at 2 years compared to both ABOc and ABOi patients, thereby predicting a worse graft outcome in DD but not in ABOi recipients. Serum neopterin levels were elevated in ABOi compared to ABOc patients at 14 days till 1 year posttransplant, whereas levels in DD versus ABOc patients remained elevated from 3 months to 5 years. These data indicate an increased activation of the T cell/monocyte system up to 1 year posttransplant in ABOi compared to ABOc patients, corresponding to the increased macrophage and T cell infiltration in the 1-year protocol biopsies of ABOi recipients. Overall, evidence of a temporary immune activation in ABOi recipients coincided with an increased AMR incidence and increased interstitial fibrosis/tubular atrophy (IF/TA) in the 1-year protocol biopsies, possibly also a result of the increased acute rejection rate in ABOi patients between 3 and 12 months. It has to be considered, however, that the 1-year protocol biopsy data are less conclusive, as only 41% of the patients were biopsied at 1 year in contrast to 70% at 3 months.
As rituximab induction in ABOi recipients exerts long-term immunosuppressive effects associated with an increased rate of severe infectious complications, but also counterregulatory immune activation and an increased risk of AMR, rituximab-free induction may be an option. Chow et al. (23) used standard immunosuppression without splenectomy or rituximab in 54 unsensitized ABOi recipients and demonstrated a low incidence of 8% (2/25) AMR in 1-year graft biopsies, excellent patient and graft survival and low rates of IF/TA progression. Although these data from Melbourne, Australia, favor a rituximab-free immunosuppression at least in unsensitized ABOi recipients, there is a risk of posttransplant AMR without rituximab induction. Bliesel et al. (24) reported 66 consecutive ABOi transplants in Sidney, Australia, without rituximab induction and found a profoundly increased 39% risk of acute rejection within 3 months with anti-ABO titer rebound in 20%, AMR in 17% of patients, 6 refractory AMR cases requiring splenectomy and 2 early graft losses due to suspected AMR. The historical rituximab-treated ABOi patient group showed only a 6% acute rejection rate and no anti-ABO titer rebound or AMR. In our own series of rituximab-free ABOi living-donor renal transplantation (2016–2024) performed only in patients with baseline anti-ABOi titers of ≤1:16, we experienced an anti-ABO titer rebound with suspected AMR in 1/10 patients which could be completely reversed by 2 rituximab administrations and immunoadsorption (data not published).
The question arises whether the increased risk of severe infectious diseases in rituximab induced ABOi recipients might be avoided by a lower rituximab dosage without increasing the risk of posttransplant anti-ABO titer rebound and AMR. This appears feasible. Lee J et al. (25) found that ABOi recipients induced with a reduced rituximab dosage (200mg absolute dosage) compared with a standard dosage (375mg/m2) showed reduced frequencies of severe infectious complications but no significant differences in acute rejection frequencies, patient and graft survival. Moreover, in a report of Masutani et al. (26), 3- and 12-month graft pathology including microvascular inflammation and IF/TA were comparable in a cohort of 101 ABOi recipients after desensitization with low-dose rituximab (200mg) versus 226 ABOc recipients without rituximab. In a review of 21 trials including 1193 ABOi recipients after induction with different dosages of rituximab, Lee HR et al. (27) confirmed the previously mentioned data that low-dose rituximab induction (200mg) lowers the risk of infectious complications without impairing graft outcome. In contrast to our data of a missing effect of rituximab on HLA antibody production, Tomita et al. (28) described a reduced de-novo anti-HLA DSA production and reduced acute rejection frequency within 5 years in a propensity score analysis of 318 non-sensitized ABOc living kidney transplants with or without a low-dose rituximab induction (100mg). It has to be discussed, however, whether low-dose rituximab induction is also sufficient in patients with high anti-ABO titers (not analyzed in the review (27)) or even in so-called high responders. Potential differences in long-term immunological effects of low-dose compared to standard-dose rituximab would be of interest.
Our study has limitations. This is a single-center study with a relatively small sample size which compromises the statistical power of the clinical transplant data. However, due to the focus on rituximab-induced long-term immunological effects and the elaborate immunological testing, the analysis of a larger number of patients was not feasible in our center. It is of advantage that all patients were treated with the same maintenance immunosuppression and all ABOi patients received the same desensitization protocol. As there was protocol violation in 4 ABOc and 3 DD patients who received rituximab treatment (pretransplant: ABOc, n=2; DD, n=1), we extended the statistical analysis and evaluated also overall rituximab treated patients and non-treated ABOc and DD patients, respectively. As protocol biopsies were performed in 70% and 41% of patients with functioning grafts at 3 and 12 months, respectively, the 12 month data are less conclusive. Data of de-novo HLA antibody formation are not conclusive because of low numbers.
5 Conclusions
Our data show that rituximab induction in ABOi recipients is associated with long-term potentially graft protective effects (partial depletion of naive B cells and short lived plasma cells in regional lymph nodes at the time of transplantation, complete B cell depletion in 3-month protocol biopsies, decline of CD4+ and CD8+ T cells and long-term comprised B cell repopulation in peripheral blood, compromised B cell responses) but also a missing impact on HLA antibody formation and even counterregulatory immune activation (recovered B cell counts and even enhanced T cell, macrophage and plasma cell counts in 1-year protocol biopsies, as well as a temporary rise of neopterin, CD4 helper activity and NK cell counts in peripheral blood), going along with an increased risk of acute rejection and especially AMR. Moreover, the long-term immunosuppressive effects of rituximab induction are associated with an increased risk of severe infectious complications. Thus, rituximab induction exerts harmful effects in ABOi patients although it appears to be useful in high-responder patients to enable ABOi transplantation and to suppress posttransplant anti-ABO titer rebound and the associated early AMR. As rituximab-free induction in ABOi recipients appears to carry a risk of anti-ABO titer rebound and AMR, a low dose rituximab induction regimen may provide an option to suppress anti-ABOi titer rebound without an increased risk of infectious complications.
Data availability statement
The datasets presented in this article are not readily available because there is no patient consent for unrestricted transfer of data. Requests to access the datasets should be directed to Prof. Dr. R. Weimer, cm9sZi53ZWltZXJAaW5uZXJlLm1lZC51bmktZ2llc3Nlbi5kZQ==.
Ethics statement
The studies involving humans were approved by the Ethical Board of the Justus-Liebig University of Giessen, Germany; Medizinisches Lehrzentrum 3. OG, Klinikstraße 29, 35392 Giessen, Germany. The studies were conducted in accordance with the German legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. HK: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. FR: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. HD: Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. VD: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. CSü: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. CSc: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. DK: Data curation, Investigation, Writing – original draft, Writing – review & editing. DL: Data curation, Investigation, Writing – original draft, Writing – review & editing. MW: Data curation, Investigation, Writing – original draft, Writing – review & editing. KM: Data curation, Investigation, Writing – original draft, Writing – review & editing. LR: Data curation, Investigation, Writing – original draft, Writing – review & editing. MS: Data curation, Investigation, Writing – original draft, Writing – review & editing. H-JG: Data curation, Investigation, Supervision, Writing – original draft, Writing – review & editing. AH: Investigation, Writing – original draft, Writing – review & editing. RH: Investigation, Writing – original draft, Writing – review & editing. WP: Investigation, Writing – original draft, Writing – review & editing. GO: Conceptualization, Formal analysis, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The author(s) declare that this study received funding from Astellas and Novartis Pharma. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The excellent technical assistance of Marita Heilke and Birgit Jennert is gratefully acknowledged. We thank Dr. Rolf-Hasso Bödeker (Institute of Medical Informatics, University of Giessen) for help with statistics. Rituximab was used off-label.
Conflict of interest
RW received a research grant for this study from Astellas and Novartis Pharma; Alexion Pharma: sponsoring of continuous medical education CME; Astellas Pharma: receipt of grants, research support, CME sponsoring; Biotest AG: CME sponsoring; Chiesi GmbH: CME sponsoring; MSD Sharp & Dohme GmbH: CME sponsoring; Neovii Biotech: reimbursement of congress expenses, CME sponsoring; Novartis Pharma: receipt of grants, research support, CME sponsoring. CSü and the TIREX center are supported by the European Union´s Horizon 2020 Research and Innovation Programme (grant 952512).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors (CSü, AH) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Glossary
ABOc: ABO blood group compatible
ABOi: ABO blood group incompatible
AIR: acute interstitial rejection
AMR: antibody-mediated rejection
AR: acute rejection
ARF: acute renal failure
ATG: antithymocyte globulin
BKV: BK virus
ClCr: creatinine clearance
CME: continuous medical education
DD: deceased donors
DSA: donor-specific HLA antibodies
HD: hemodialysis
IA: immunoadsorption
IF/TA: interstitial fibrosis/tubulus atrophy
ISC: immunoglobulin-secreting cell
IVIG: intravenous immunoglobulins
LPS: lipopolysaccharide
MEPE: molecules of equivalent phycoerythrin
MHC: major histocompatibility complex
MPGN: membranoproliferative glomerulonephritis
PBMC: peripheral blood mononuclear cells
PD: peritoneal dialysis
PMA: phorbol-12-myristate-13-acetate
PR: preemptive transplantation
PRA max: maximum panel reactive antibodies
PRA rec: recent panel reactive antibodies
PTLD: posttransplant lymphoproliferative disease
RRT: renal replacement therapy
sCD30: soluble CD30
S-Cr: serum creatinine
SEM: standard error of the mean
Tacr: tacrolimus
Tacr-MR: tacrolimus modified-release
References
1. Opelz G, Morath C, Süsal C, Tran TH, Zeier M, and Döhler B. Three-year outcomes following 1,420 ABO-incompatible living-donor kidney transplants performed after ABO antibody reduction: results from 101 centers. Transplantation. (2015) 99:400–4. doi: 10.1097/TP.0000000000000312
2. de Weerd AE and Betjes MGH. ABO-incompatible kidney transplant outcomes. A meta-analysis. Clin J Am Soc Nephrol. (2018) 13:1234–43. doi: 10.2215/CJN.00540118
3. Scurt FG, Ewert L, Mertens PR, Haller H, Schmidt BMW, and Chatzikyrkou C. Clinical outcomes after ABO-incompatible renal transplantation: a systematic review and meta-analysis. Lancet. (2019) 393:2059–72. doi: 10.1016/S0140-6736(18)32091-9
4. Xu P, Zhao N, and Wang J. Success rate and safety of living donor kidney transplantation in ABO blood group incompatible relatives: A systematic review and meta-analysis. Transplant Immunol. (2023) 81:1–9. doi: 10.1016/j.trim.2023.101921
5. Weimer R, Deisz S, Dietrich H, Renner F, Bödeker RH, Daniel V, et al. Impact of maintenance immunosuppressive regimens – balance between graft protective suppression of immune functions and a near physiological immune response. Transplant Int. (2011) 24:596–609. doi: 10.1111/j.1432-2277.2011.01241.x
6. Weimer R, Ettrich M, Renner F, Dietrich H, Süsal C, Deisz S, et al. ATG induction in renal transplant recipients: Long-term hazard of severe infection is associated with long-term functional T cell impairment but not the ATG-induced CD4 cell decline. Hum Immunol. (2014) 75:561–9. doi: 10.1016/j.humimm.2014.02.015
7. Weimer R, Melk A, Daniel V, Friemann S, Padberg W, and Opelz G. Switch from cyclosporine A to tacrolimus in renal transplant recipients: impact on Th1, Th2, and monokine responses. Hum Immunol. (2000) 61:884–97. doi: 10.1016/s0198-8859(00)00152-x
8. Zhou L, Pereiro MT, Li Y, Derigs M, Kuenne C, Hielscher T, et al. Glucocorticoids induce a maladaptive epithelial stress response to aggravate acute kidney injury. Sci Transl Med. (2024) 16:eadk5005. doi: 10.1126/scitranslmed.adk5005
9. Peters LK. Reactivation kinetics of human polyomaviruses in renal transplant recipients and quantification by differential real-time PCR. Doctoral thesis. University of Giessen, Germany. doi: 10.22029/jlupub-13427
10. Takahashi K, Saito K, Takahara S, Okuyama A, Tanabe K, Toma H, et al. Japanese ABO-incompatible kidney transplantation committee. Am J Transplant. (2004) 4:1089–96. doi: 10.1111/j.1600-6143.2004.00464.x
11. Zschiedrich S, Kramer-Zucker A, Jänigen B, Seidl M, Emmerich F, Pisarski P, et al. An update on ABO-incompatible kidney transplantation. Transplant Int. (2015) 28:387–97. doi: 10.1111/tri.12485
12. Lo P, Sharma A, Craig JC, Wyburn K, Lim W, Chapman JR, et al. Preconditioning therapy in ABO-incompatible living kidney transplantation: a systematic review and meta-Analysis. Transplantation. (2016) 100:933–42. doi: 10.1097/TP.0000000000000933
13. Weimer R, Rainer L, Feustel A, Wienzek-Lischka S, Schüttler C, Dietrich H, et al. Drop-outs in ABO-incompatible (ABOi) living-donor renal transplantation may be prevented – a single center experience. In: Abstracts of the 22nd Annual Meeting of the German Transplantation Society; 2013 Oct 24-26; Frankfurt/Main, Germany. Transplant Int. (2013) 26:8. doi: 10.1111/tri.12180
14. Schachtner T, Stein M, and Reinke P. ABO desensitization affects cellular immunity and infection control after renal transplantation. Transpl Int. (2015) 28:1179–94. doi: 10.1111/tri.12616
15. Tydén G, Kumlien G, and Fehrman I. Successful ABO-incompatible kidney transplantations without splenectomy using antigen-specific immunoadsorption and rituximab. Transplantation. (2003) 76:730–1. doi: 10.1097/01.TP.0000078622.43689.D4
16. Donauer J, Wilpert J, Geyer M, Schwertfeger E, Kirste G, Drognitz O, et al. ABO-incompatible kidney transplantation using antigen-specific immunoadsorption and rituximab: a single center experience. Xenotransplantation. (2006) 13:108–10. doi: 10.1111/j.1399-3089.2006.00293.x
17. Kamar N, Milioto O, Puissant-Lubrano B, Esposito L, Pierre MC, Mohamed AO, et al. Incidence and predictive factors for infectious disease after rituximab therapy in kidney-transplant patients. Am J Transplant. (2010) 10:89–98. doi: 10.1111/j.1600-6143.2009.02785.x
18. Habicht A, Bröker V, Blume C, Lorenzen J, Schiffer M, Richter N, et al. Increase of infectious complications in ABO-incompatible kidney transplant recipients - a single centre experience. Nephrol Dial Transplant. (2011) 26:4124–31. doi: 10.1093/ndt/gfr215
19. Pellegrini P, Berghella AM, Contasta I, and Adorno D. CD30 antigen: Not a physiological marker of TH2 cells but an important costimulator molecule in the regulation of the balance between TH1/TH2 response. Transpl Immunol. (2003) 12:49–61. doi: 10.1016/S0966-3274(03)00014-5
20. Süsal C, Pelzl S, Döhler B, and Opelz G. Identification of highly responsive kidney transplant recipients using pretransplant soluble CD30. J Am Soc Nephrol. (2002) 13:1650–6. doi: 10.1097/01.asn.0000014256.75920.5b
21. Süsal C, Pelzl S, and Opelz G. Strong HLA matching effect in nonsensitized kidney recipients with high pretransplant soluble CD30. Transplantation. (2003) 76:1231–2. doi: 10.1097/01.TP.0000085286.93715.E0
22. Weimer R, Süsal C, Yildiz S, Staak A, Pelzl S, Renner F, et al. Post-transplant sCD30 and neopterin as predictors of chronic allograft nephropathy: impact of different immunosuppressive regimens. Am J Transplant. (2006) 6:1865–74. doi: 10.1111/j.1600-6143.2006.01407.x
23. Chow KV, Flint SM, Shen A, Landgren A, Finlay M, Murugasu A, et al. Histological and extended clinical outcomes after ABO-incompatible renal transplantation without splenectomy or rituximab. Transplantation. (2017) 101:1433–40. doi: 10.1097/TP.0000000000001415
24. Bleasel JM, Wan SS, Chadban SJ, Ying T, Gracey DM, Aouad LJ, et al. ABO incompatible kidney transplantation without B-cell depletion is associated with increased early acute rejection: a single-center Australian experience. Transpl Int. (2023) 36:11567. doi: 10.3389/ti.2023.11567
25. Lee J, Lee JG, Kim S, Song SH, Kim BS, Kim HO, et al. The effect of rituximab dose on infectious complications in ABO-incompatible kidney transplantation. Nephrol Dial Transplant. (2016) 31:1013–21. doi: 10.1093/ndt/gfw017
26. Masutani K, Tsuchimoto A, Kurihara K, Okabe Y, Kitada H, Okumi M, et al. Histological analysis in ABO-compatible and ABO-incompatible kidney transplantation by performance of 3- and 12-month protocol biopsies. Transplantation. (2017) 101:1416–22. doi: 10.1097/TP.0000000000001324
27. Lee HR, Kim K, Lee SW, Song JH, Lee JH, and Hwang SD. Effect of rituximab dose on induction therapy in ABO-incompatible living kidney transplantation: A network meta-analysis. Med (Baltimore). (2021) 100:e24853. doi: 10.1097/MD.0000000000024853
Keywords: kidney transplantation, ABO incompatible, rituximab, B cell repopulation, protocol biopsies, acute rejection, severe infectious disease, HLA antibodies
Citation: Weimer R, Karakizlis H, Renner F, Dietrich H, Daniel V, Süsal C, Schüttler C, Kämper D, Leicht D, Wörlen M, Milchsack K, Renner L, Stich M, Gröne H-J, Hecker A, Hörbelt R, Padberg W and Opelz G (2025) Long-term compromised immune regulation after rituximab induction in blood group incompatible (ABOi) living-donor renal transplantation – 5 year results of a prospective pilot study. Front. Immunol. 16:1706158. doi: 10.3389/fimmu.2025.1706158
Received: 15 September 2025; Accepted: 07 November 2025; Revised: 19 October 2025;
Published: 12 December 2025.
Edited by:
Antonij Slavcev, Institute for Clinical and Experimental Medicine (IKEM), CzechiaReviewed by:
Ilias Doxiadis, University Hospital Leipzig, GermanyNaohiro Aida, Fujita Health University, Japan
Copyright © 2025 Weimer, Karakizlis, Renner, Dietrich, Daniel, Süsal, Schüttler, Kämper, Leicht, Wörlen, Milchsack, Renner, Stich, Gröne, Hecker, Hörbelt, Padberg and Opelz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rolf Weimer, cm9sZi53ZWltZXJAaW5uZXJlLm1lZC51bmktZ2llc3Nlbi5kZQ==