 Leonard E. G. Mboera1*
Leonard E. G. Mboera1* Calvin Sindato1,2
Calvin Sindato1,2 Irene R. Mremi1,3
Irene R. Mremi1,3 Susan F. Rumisha3,4
Susan F. Rumisha3,4 Janeth George1
Janeth George1 Renfrid Ngolongolo1
Renfrid Ngolongolo1 Gerald Misinzo1,5
Gerald Misinzo1,5 Esron D. Karimuribo1,6
Esron D. Karimuribo1,6 Mark M. Rweyemamu1
Mark M. Rweyemamu1 Najmul Haider7
Najmul Haider7 Muzamil Abdel Hamid8
Muzamil Abdel Hamid8 Richard Kock7
Richard Kock7- 1SACIDS Foundation for One Health, Sokoine University of Agriculture, Morogoro, Tanzania
- 2National Institute for Medical Research, Tabora, Tanzania
- 3National Institute for Medical Research, Dar es Salaam, Tanzania
- 4Malaria Atlas Project, Geospatial Health and Development, Telethon Kids Institute, West Perth, WA, Australia
- 5Department of Veterinary Microbiology, Parasitology and Biotechnology, Sokoine University of Agriculture, Morogoro, Tanzania
- 6Department of Veterinary Medicine and Public Health, Sokoine University of Agriculture, Morogoro, Tanzania
- 7The Royal Veterinary College, University of London, London, United Kingdom
- 8Institute of Endemic Diseases, Medical Campus, University of Khartoum, Khartoum, Sudan
Introduction: Since 2010, Tanzania has been experiencing frequent outbreaks of dengue. The objectives of this study were to carry out a socio-ecological systems (SES) analysis to identify risk factors and interventions and assess the readiness of the district in the prevention and control of dengue.
Methods: The study utilized a cross-sectional purposive selection of key stakeholders responsible for disease surveillance and response in human and animal sectors in Ilala and Kinondoni districts in Tanzania. A SES framework was used to identify drivers and construct perceived thematic causal explanations of the dengue outbreaks in the study districts. A mapping exercise was carried out to analyse the performance of the disease surveillance system at district and facility levels. A semi-structured questionnaire was used to assess the districts’ readiness in the response to dengue outbreak.
Results: The two districts were characterized by both urban and peri-urban ecosystems, with a mixture of planned and unplanned settlements which support breeding and proliferation of Aedes mosquitoes. The results indicate inadequate levels of readiness in the management and control of dengue outbreaks, in terms of clinical competence, diagnostic capacities, surveillance system and control/prevention measures. Mosquito breeding sites, especially discarded automobile tyres, were reported to be scattered in the districts. Constraining factors in implementing disease surveillance included both intrapersonal and interpersonal factors, lack of case management guidelines, difficult language used in standard case definitions, inadequate laboratory capacity, lack of appropriate rapid response teams, inadequate knowledge on outbreak investigation and inadequate capacities in data management.
Conclusion: The two districts had limited readiness in the management and control of dengue, in terms of clinical competence, diagnostic capacities, surveillance system and prevention and control measures. These challenges require the immediate attention by the authorities, as they compromise the effectiveness of the national strategy for community health support.
Introduction
Tanzania has experienced several outbreaks of mosquito-borne viral diseases (MBVDs) including dengue, chikungunya and Rift Valley fever over the last two decades (1–4). These diseases are ecologically sensitive, since environmental conditions, such as temperature and precipitation, affect both the infectious pathogens and the vectors that transmit them (5, 6). MBVDs have received little attention, most likely due to inadequate knowledge, awareness and inadequate diagnostic capacity. The ecology and transmission of MBVDs are closely related to environmental resource management, social and behavioural patterns (7). Thus, the mechanisms underlying MBVDs require exploring complex interactions within and among coupled natural and human systems, considering human and natural ecologies, and the multiple layers of interaction among them (8–10). Usually, MBVD risk increases as a result of the effect of heavy rainfall providing habitat suitability for mosquito breeding opportunities (5, 11). Furthermore, repeated drought conditions and inadequate/unreliable water supply encourage storage of water for human and livestock consumption, the practices which provide breeding sites for Aedes aegypti, the primary vector of dengue (12).
A better understanding of the relationship between development transitions and emerging and re-emerging infectious diseases is critical for improving capability to predict and respond to epidemics. The complex nature of emerging and re-emerging infectious diseases highlights the need for new approaches to understand the mechanisms and processes underlying pathogen emergence to improve disease prevention and control. Moreover, it is important to understand how transformations in socio-ecological systems caused by multifaceted interactions between anthropogenic environmental changes such as urbanization, livelihoods activities, and natural habitat alterations, produce feedbacks that affect natural communities and ultimately their pathogens, animal and human populations (13, 14). However, there are limited studies that have attempted to apply socio-ecological systems (SES) framework analysis on emerging and re-emerging infectious diseases in low-and middle-income countries (15).
The socio-ecological theory provides a framework for examining how individuals, their health, and surrounding physical and social environments interact at multiple levels of a health problem and their interdependency (5, 16). The levels are: (i) Intrapersonal factors such as individual attitudes, behaviours, knowledge, and skills; (ii) Interpersonal processes and community factors, such as social networks made of family, friends, or colleagues that provide support; (iii) Institutional factors such as formal or informal organizations that may have rules or expectations that impact health behaviours; and (iv) laws, policies or regulations that promote or inhibit certain health practices that impact disease management, control or prevention (17–20).
The development of a framework for analysing social-ecological models aims to understand how these systems function, and the processes through which they interact to influence disease outbreaks. To our knowledge, only a single study carried out in Tanzania has so far documented socio-ecological factors as regards to dengue epidemics (21). Moreover, the readiness of national and sub-national levels in dengue and other mosquito-borne viral disease mitigations has not been assessed in Tanzania. Identifying district level health determinant factors for dengue transmission will provide specific targets for public health interventions. With the decentralised health system management structure in Tanzania, most operational activities for disease surveillance are conducted at the district level. The objectives of this study were to (i) carry out a socio-ecological systems analysis on dengue to identify risk factors and interventions at the district level; and (ii) assess the readiness of the district in the prevention and control of dengue.
Methods
Study Area
This study was carried out during October 2019 and involved Ilala and Kinondoni districts of Dar es Salaam city in eastern Tanzania. It is the largest city in Tanzania with an area of 1,339km2, is made up of five administrative districts, namely Ilala, Kigamboni, Kinondoni, Temeke and Ubungo. The city human population is 4,364,541 (Ilala=1,220,611; Kinondoni= 1,775,049), with an annual growth rate of 5.6% (22). The climate of Dar es Salaam is generally hot and humid with small seasonal and daily variations in temperature. The mean daily temperature is 26°C, the mean seasonal range is 4°C, and the mean daily range is about 8°C. There are two rainy seasons, long (March-June) and short (October-December) with total annual rainfall averages 1,100mm. The relative humidity is generally high, reaching 100% almost every night throughout the year, but falling to 60% during the day (23, 24).
Dar es Salaam has been facing continued dengue outbreaks with increased frequency and occurrence during the past 10 years. The occurrence of dengue outbreaks was reported in 2010, 2012, 2013, 2014, 2018 and 2019 (2, 3, 25, 26). During the 2019 outbreak, about 6,917 cases including 13 deaths were reported between January and July 2019 in Tanzania (27). Two districts of Dar es Salaam, namely Kinondoni and Ilala were selected for this study because of their experience in dengue outbreaks since 2010 (2, 3). We hypothesized that following experience of several dengue outbreaks, the districts would have plans and built their capacities on outbreak preparedness and response.
Dar es Salaam is characterized by a high human population density, occupied by multiple activities and diverse socio-ecological systems ranging from informal housing, transport infrastructure, dump sites, agriculture, industrial commercial activities, fishing and sand mining. It is highly polluted by effluents from Msimbazi river tributaries originating from different sources, leakage of effluent from waste dumps, abattoirs and domestic wastewater. It remains unclear how these diverse socioecological features interact to influence vulnerability of the region to Dengue outbreaks. We focused on two districts in the region for an exploratory baseline data analysis to guide mitigations against the disease prevention and control and future studies.
Data Collection
Participants
The study utilized a cross-sectional purposive selection of key stakeholders responsible for disease surveillance and response in human and animal sectors. The participants were brought together to foster interdisciplinary collaboration and stimulate transdisciplinary approaches to improve prevention and control of MBVDs. They were from the departments responsible for human and animal health of the Dar es Salaam city council and Ilala and Kinondoni districts. Data collection process was implemented through a consultative workshop adapted as a participatory rapid appraisal method to explore practices related to prevention and control of dengue in the study districts. Based on the study objectives, the participants were considered through a purposefully selection process with a sample representing the key components of disease surveillance functions related to MBVDs.
District SES Framework Analysis
We applied SES framework (28–31) to identify drivers and construct perceived thematic causal explanations of the dengue outbreaks in the study districts. The SES approach allows the application of a variety of methodological process to study the field of interest (32). The major components of SES framework include social, economic, and political settings; resource systems; governance systems; resource units; actors; interactions; implementation outcomes; and related ecosystems (33). Application of this theory-based framework to understand the multifaceted and interactive effects of different actors and environmental factors on the outcome of interest, involves five nested, hierarchical levels of the socioecological model, which are individual, interpersonal, community, organizational, and policy/enabling environment (34). Building on a conceptual framework developed by ecologists to address natural resource management issues (28–31), we adapted the steps to the interface of human and natural systems to assess the capacity of the districts in addressing MBVDs. Participants worked in two groups, each for the respective district. Group works were followed by group presentations and discussions.
The themes in the SES framework analysis tool included, ecosystem descriptor (rural, urban, semi-urban; forest (tropical, savannah), human settlement type (population density; settlement in valley areas; planned/unplanned squatter), economic activities (subsistence agriculture; industry; mining extractive; business), agricultural production system (subsistence crop, type of crops; season of cropping), and housing structure (sand brick, mud brick, flooring mud; concrete, iron roofed, grass thatched roof). Others were infrastructure (transport system, water sources and waste disposal), actors influencing disease events (individuals, community), policies (education, nutrition, dengue prevention and control and treatment) and external shock to health system (climate variability/change and other related policies).
District Readiness to Epidemics
An interview guide with semi-structured questions was used to assess and document the districts’ clinical competence of healthcare providers, diagnostic capacity, and surveillance, prevention and control interventions. The themes included were clinical competence of healthcare providers (standard case definition, case management guidelines, availability of human resource), diagnostic capacity (availability of diagnostic test, consumables, guidelines, standard operating procedures and job aids), functionality of surveillance system (data quality (timeliness, completeness, consistency), data analytical capacity and data sharing policy and practices). Others were control interventions (availability of contingency plan, community involvement in surveillance activities, health education and promotion) and availability of partners in the surveillance, prevention and control of dengue in the respective districts.
The assessment of the surveillance system covered the following items: structures of the surveillance system, staff and resources, responsibility units and capacity to respond to infectious disease outbreaks. Disease surveillance, response and control programmes and networks were assessed to evaluate the capacity to detect, notify, assess and respond to known, new, and unknown infectious disease threats. The gaps were identified and solutions to enhance utilization of data for relevant sources for decision making process were proposed. Exploration was made to map how the districts were working and what actions would be needed to improve surveillance and response strategies in the districts.
Data Collection Approach
Five researchers facilitated a two-day consultative workshop and a chairperson moderated each session. The workshop comprised of series of presentations, group exercises and plenary sessions based on themes pre-defined in the data collection tools. Presentations included general overview of MBVDs in Tanzania, SES framework analysis and principles and functions of public and animal health surveillance systems.
The workshop participants were oriented to the objectives of the study and expected outcomes. They were taken through data collection tools for a common understanding of different fields related to disease surveillance functions. Participants were asked to complement the pre-defined themes in the respective data collection tools. This was followed by a questions and answers session before participants were organized into breakout groups of theme-based sessions involving three to five participants from each district in an interactive discussion for each of the questions in the data collection tools. The group working sessions focused on specific assignments on SES framework analysis on dengue. A mapping exercise was also carried out to analyse the performance of the disease surveillance system at district and facility levels.
The results (for each theme) from the group sessions were reported and discussed with the reconvened larger group during the plenary sessions. This pattern—the reiteration of the research theme by researchers, followed by small group discussion for a particular theme, convening of a larger group plenary discussion—were repeated until when participants had worked through all the themes presented in each of the analysis tool. The collected data were typed in the Microsoft word format and discussed with participants during the plenary session before they were regarded as final. While describing the specific theme in each of the data collection tool, participants were asked to qualify their responses to the possible extent. Depending on the nature of the questions, the expected responses were categorized into “poor or good”, “sufficient or insufficient”, “weak or strong”, “available or not available”, and “available and in use or available but not in use”. While describing a specific theme, where applicable, participants were asked to extend qualification of their responses beyond the priori-defined responses.
Data Management and Analysis
We used data from the in-depth interviews to assess levels, practices and factors influencing socio-ecological system, epidemic readiness, disease surveillance capacity, and dengue prevention and control. Content analysis technique was applied using manifest surface structure approach to group different expressions provided by participants into discrete categorical responses reflecting the specific themes defined by different variables in the SES framework analysis epidemic readiness, disease surveillance capacity, and dengue prevention and control tools used (34). Data was summarized using a narrative structure for SES and were interpreted based on existing related literature, theories and knowledge/experience of the researchers.
Ethical Considerations
This study received ethical approval by the Medical Research Coordinating Committee of the National Institute for Medical Research (Ref. NIMR/HQ/R.8c/Vol 1/1168).
Results
Socio-Ecological System Analysis
The workshop brought together 27 participants comprising of regional and district medical/health officers, regional and district health management information systems officers, district vector control officers, veterinary officers, information and communication technology specialists, surveillance officers and researchers. A number of observations and issues were raised as regards to the capacity of the country in addressing MBVDs. It was explained that until early 2000s, the Ministry of Health had a department responsible for the coordination of all issues pertaining to vector-borne diseases. However, the department does not exist anymore; and the activities related to vector-borne diseases were being implemented separately through vertical programmes. Such programmes focused on specific diseases such as malaria, lymphatic filariasis, trachoma and onchocerciasis.
The two districts were characterized by both urban and peri-urban ecosystems, with mostly medium to high density human populations. A mixture of planned and unplanned settlements was common in both districts. Backyard poultry, pig and dairy farming were common in Ilala, but limited in Kinondoni district. Housing was characterized by iron roofing, with some of the houses having roof rain gutters. The main economic activities in Kinondoni included small-scale industries, business and extractive quarrying mining activities. In Ilala they included medium to large-scale food and non-food industries, business, fishing activities, crop production and extractive quarrying of sand. Seasonal cropping of vegetables and pot flower gardening were common practices in the two districts (Figure 1). The sources of energy in both districts included electricity, charcoal, firewood, solar, gas and kerosene. Though solid waste management and disposal was centralized, improper household waste disposal was common in the two districts.
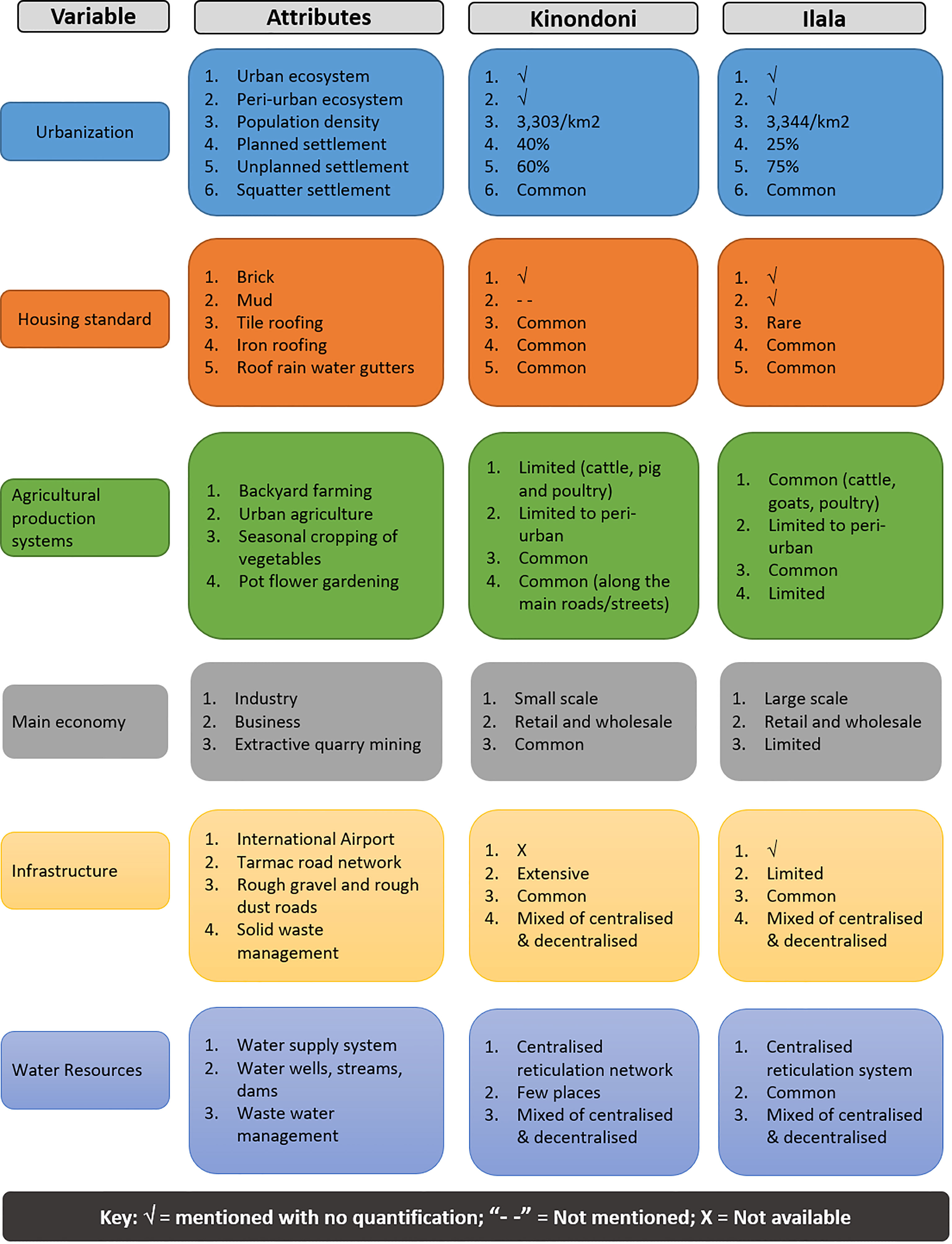
Figure 1 District profiles and socio-ecological factors.
Epidemic Readiness
Overall, none of the two districts reported adequate readiness in the management and control of dengue, both in terms of clinical competence, diagnostic capacities, surveillance and control/prevention measures. The challenges related to clinical competence included lack of standard case definition (SCD), standard operating procedures, inadequate rapid diagnostic tests, lack of case management guidelines, inadequate human resource and lack of job aids. The major challenges in surveillance were poor data quality (completeness and consistency), timeliness, inadequate data analysis capacity and unavailability of data sharing policy and practices. Community-based disease surveillance programme was not part of the surveillance system in the two districts. None of the districts had a contingency plan for dengue. Treatment guidelines for dengue were available, but not disseminated widely at all levels in the districts (Table 1).
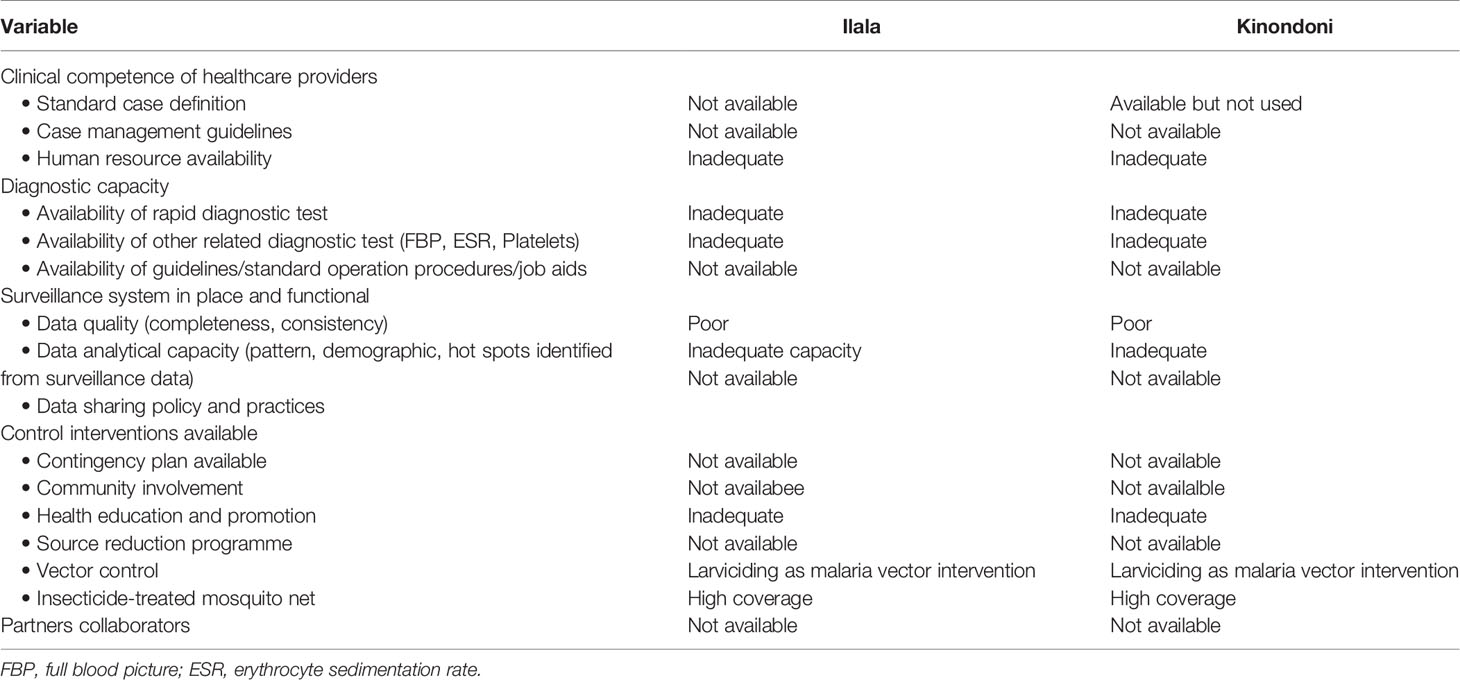
Table 1 District readiness in the management and control of dengue.
Disease Surveillance
Facility Level
At the facility level (which include district hospital, health centre and dispensary), participants from Kinondoni identified availability of forms for reporting and routine meetings with local authorities as the only facilitating factors in implementing surveillance programme. The constraining factors reported included lack of guidelines, dissemination and translation of SCDs (which were in English) and low diagnostic capacities for dengue. Lack of smooth communication network and appropriate rapid response team were reported. Low capacity on data management, including analysis, was reported to negatively affect the decision-making process at health facility level. Inadequate knowledge on outbreak investigation among health facility workers and shortage of sample collection equipment were identified as critical gaps. In Ilala, although the SCD were available, most of the clinicians reported to have not received orientation/training on their use. Data analysis and interpretation at health facility level was not been routinely done due to inadequate knowledge and skills. Like in Kinondoni, the participants reported that facility level health care workers were not part of the outbreak investigation team.
District Level
In Kinondoni the identified constraining factors were (i) lack of data collection tools, shortage of staff and insufficient laboratory reagents; (ii) external and internal transfer of trained staff; insufficient knowledge and unreliable internet connectivity; (iii) inadequate communication tools; (iv) delays in receiving reports from the lower levels (facilities or community); (vi) lack of periodic supportive supervision from higher levels; (vi) low capacity of the district outbreak response team; and (vii) inadequate budget for surveillance activities.
Participants from Ilala reported on lack of feedback on data analysis as the most critical challenge in the use of surveillance data. Moreover, they were not able to compare current and previous pattern (trends) of the disease due to poor quality data. Unavailability of sample collection tools and unclear responsibilities for health care workers were underscored as the key limiting factors in the outbreak investigation. It was pointed out that although the district team is sometimes involved in disease outbreak management, its staff lacked training and budget on emergency preparedness and responses. They also reported that an Epidemic Response Committee in the district was not functioning. Most of the guidelines were reported to be in English, voluminous and difficult to follow. It was proposed that the guidelines be translated into Kiswahili (the national language) and made available in simple user-friendly formats.
In the two districts, analysis tools for surveillance data were not in place. Moreover, it was reported that the surveillance officers were not skilled enough on data management especially, analysis and interpretation. There were a number of health information systems for district and facility to use, which included the Health Management Information System (HMIS), National System for Government Health Officials and Government of Tanzania Hospital Management Information System. All these were described to bring confusion to health workers. There was no information, knowledge, skills and experience sharing practices on data management between surveillance and HMIS officers at the district level.
Dengue Prevention and Control
During the discussion, an issue on unchecked mosquito breeding sites in Dar es Salaam city was raised and discussed. There was no functional entomology surveillance programme in the study districts. Participants were concerned with the lack of appropriate actions as regards to disposal of discarded automobile tyres and water-carrying containers. Mosquito breeding sites especially discarded automobile tyres were reported to be scattered and found in almost all areas of the city. The automobile tyres were described to contribute to over two-thirds of the breeding sites for Aedes mosquitoes. It was reported that in the old days, the destruction of used automobile tyres was done by burning. However, the programme failed, as it required burning chambers, which were not available. It was noted that although a malaria larviciding programme was been implemented in the city, it was ineffective against Aedes mosquitoes. Participants noted that the malaria mosquito larviciding project focused on large water bodies and left small water bodies and containers unchecked. Moreover, the programme was being implemented in only 60% of the wards in the city. The participants raised their concerns for the districts inadequate budget for outbreaks response. The low level of awareness on dengue and other mosquito-borne viral diseases was reported by participants from both districts (Figure 2).
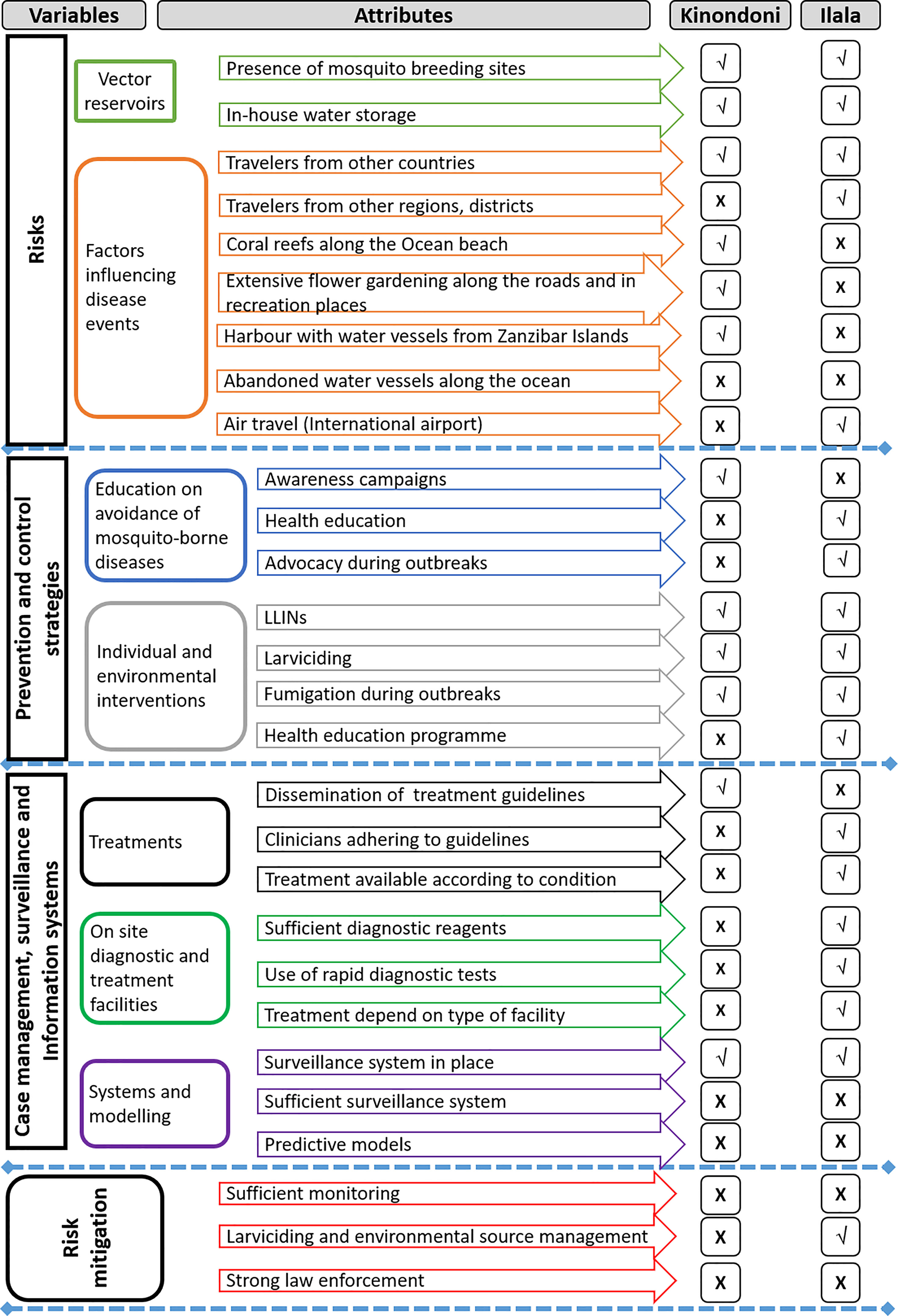
Figure 2 Presence (√) and absence (X) of risks, prevention and control activities for dengue in the study districts.
The following were proposed as the way forward in addressing the challenges in the control of dengue: (i) revising the larviciding programme to cover much larger areas of the city and target the priority mosquito-borne disease vectors; (ii) enhancing capacity in dengue diagnosis and case management; and (iii) developing a strategic plan to address advocacy to the regional and district government authorities as regards to the importance of outbreak preparedness.
Discussion
Dengue has become an increasingly important public health problem in the tropical world in terms of morbidity and mortality. With rapidly changing human population and activities, the ecology of both the pathogens and vectors, climate change coupled with weak health systems, dengue outbreaks are likely to become more frequent. In our approach, we addressed the reality that effective prevention and control of dengue cannot be achieved from narrow perspectives, but would largely benefit from a holistic approach that considers an improved understanding of SES and health system readiness. The basic idea of SES is to be explicit in system thinking and linking together the ‘human system’ and the ‘natural system’ in a two-way feedback relationship.
The interactions between humans, pathogens and environment, suggest that SES is crucial in disease occurrence and transmission dynamics. Moreover, the readiness of national and sub-national levels in dengue mitigations is central in the designing and planning of appropriate intervention measures. It is against this background that we conducted this analysis to identify socioecological factors and readiness of the districts in the control and prevention of dengue. In our data collection process, we adopted a consultative workshop method, which has been found to foster engagement through collaborative discussions and constructive feedback between participants from different the district and sectors on a particular topic (35, 36). The approach helped us to obtain information-rich data and persistent observation on dengue management and control in the study districts from purposively selected key stakeholders, which is similar to a consideration reported elsewhere (37).
In the SES framework analysis, we found that the ecological descriptors of Ilala and Kinondoni were characterised by both urban and peri-urban ecosystems with planned and unplanned settlements. Although in our study we did not establish the impact of urbanization on the occurrence of dengue, urban and peri-urban areas have been reported to be vulnerable to the disease, the outcome which is driven by rapid and uncontrolled urbanization that support Aedes mosquito productivity (2, 38, 39). The intrapersonal factors such as in-house water storage, improper household waste water disposal were common practices in the districts. The presence of potential mosquito breeding sites including discarded automobile car tyres, flower pots and water stagnation were reported to support habitat suitability for mosquito breeding and thereby increasing the risk of occurrence of dengue in the two districts (2, 21).
It was reported that to date, there have been no effective measures in the disposal of used automobile tyres. As a result, they were improperly discarded and continued to stockpile in the districts. This creates a great health risk as tyres provide permissive breeding grounds for mosquitoes (40). Used automobile tyres and domestic water storage containers have been reported as the most important larval habitats for Ae. aegypti in Dar es Salaam and Zanzibar (41, 42). These observations suggest that the solution to proper management of mosquito breeding sites does not fall clearly within the boundaries of a single discipline or sector but rather a multi-sectoral approach.
Vulnerability to dengue was considered disproportionately distributed within each of the study districts. This suggests that interventions to address them should be repackaged based on specific-area risk profiles. However, as we have highlighted on the inefficiency of surveillance systems based on district-level SES framework analysis, we cannot account explicitly on the representation of vulnerability of sub-district levels to dengue. SES framework analysis at the sub-district levels is likely to complement our understanding on the vulnerability profiles at different ecological levels.
One of the strategic mosquito prevention measures in the districts was larviciding. However, in the two districts, larviciding, which was introduced for malaria control (43), was implemented without consideration of the evidence to guide appropriate timing, areas and potential breeding sites of focus. We suggest that in order to effectively prevent dengue, it is important to implement integrated vector management measures. This should be implemented by targeting the most suitable mosquito habitats to suppress mosquito larval stages thereby reducing adult emergence. Although larviciding has been recommended as a complementary intervention to control malaria (44), we suggest to conduct monitoring and evaluation of such interventions against the Aedes mosquitoes.
It has been established that indices of mosquito and climate factors are the main determinants of dengue (45–47). Since microclimate dynamics is largely determined by human activities it is imperative to suggest that a key strategy to prevent and control dengue is to focus on addressing the anthropogenic factors. A number of ecological, biological and social factors are involved in mosquito breeding and pathogen transmission (48). A study in Sri Lanka revealed that dengue outbreaks were significantly associated with ecological, socio-economic and demographic factors; including the presence of built-up area, and areas with higher human population density (49). Existing evidence on the complexity of eco-bio-social contexts repeatedly argues that dengue control necessitates sound intersectoral approaches that combine environmental management practices with community mobilization (50–52). Probably intensification of public health education on proper management of water storage containers, discarded car tyres, periodic draining or removal of artificial containers could be the most effective strategy of reducing Aedes mosquito breeding habitats. Based on SES framework analysis results, we hypothesise that interventions on the management of potential mosquito breeding sites in domestic and peri-domestic environments and ecological health could generate data to guide sustainable community-based prevention strategies against dengue and other Aedes-borne viral diseases.
On assessing the capacity in responding to outbreaks, none of the two districts reported the readiness in the management of dengue outbreak. The availability of disease surveillance and management guidelines in English language was reported as a utilization impediment and participants proposed that they should be translated into Kiswahili (the national language). In our study, the guidelines were reported to be voluminous and not user-friendly. Since a number of guidelines continue to proliferate on the same or similar subjects, it is likely to be impractical for the practitioners to use them efficiently. The successful implementation of guidelines depends on many factors including participatory development, dissemination and implementation strategy as well as evaluation of their effectiveness (53). The presence of guidelines may not guarantee their implementation or utility, and some studies have reported failure of guidelines to influence the implementation of health programmes (54–56). The reasons that have been associated with failure of guidelines to achieve their objectives, include inadequate consultation, lack of consideration of technical capacity, attitude and behaviour of health professionals and lack of training on the use of the guidelines (57–59). Adoption of a web- or mobile-based electronic platform to enhance, on the one hand data collection especially at community level and on the other, prompt searching by topic of interest or based on prevailing needs is likely to be a breakthrough. We believe that with increasing occurrence of infectious disease epidemics the efficiency of disease surveillance, early detection and early warning will require use of such web or mobile technologies (60). This can be enhanced through application of machine learning data-mining integration with socio-ecological and geospatial analyses (61), specifically designed for low- and middle- income countries like Tanzania.
The capacities of the districts in dengue epidemic readiness was limited, and this calls for concerted efforts to improve resource availability, and capacity strengthening. Measuring readiness in epidemic preparedness and response is likely to present some challenges. This is because in this study epidemic preparedness focused mainly on human resource, infrastructure, and surveillance. The study did not document the relevant processes in epidemic preparedness or the activities executed during an epidemic response, including isolation and quarantine, public communication, and others (62).
Generally, the overall performance of the surveillance system in the two districts was not satisfactory in detecting and or monitoring trends of dengue. We recorded inadequate skills and capacity in outbreak investigation, insufficient laboratory supplies, poor surveillance data quality, inadequate skill on data analysis, interpretation and use, and poor information/data sharing practices between sectors. The surveillance systems were reported to be inefficient with inadequate involvement of community and therefore not tailored for early detection and response. Limited or no evidence of routine data analysis at sub-national levels due to lack of clear guidelines on how and when to analyse data has been reported in previous studies (63–66). It has been described that when the health facilities do not analyse and use the data, the utility of the surveillance system becomes minimal, which makes the system too weak to pick outbreaks early that could guide prompt response. The absence of data analysis, interpretation and utilization for local action seen in the present study is in line with findings of studies in Ethiopia, Nigeria and Tanzania (67–70). Skill gap in data management system, weak supervision and feedback system, low or no legal enforcement to the surveillance activities, lack of incentives, lack of continued capacity building training, and lack of sense of ownership have been reported as factors affecting analysis and use of surveillance data (67).
It is important to note that, this exploratory study utilized a cross-sectional purposive selection of key stakeholders responsible for disease surveillance and response in one region of the country that has repeatedly reported Dengue outbreaks. This means that it will be difficult to draw a generalizable inference over the entire country from these results. However, the findings could apply to areas with similar settings as the study areas and provide the baseline data for future socio-ecological studies. The quality and quantity of information reported by participants might have been affected by recall bias and/or preferences to report amongst them.
Conclusion
Using the SES framework analysis, through a consultative workshop data collection approach, we have managed to identify important features, the processes and assess the functioning of multifaceted and complex systems involved in management 0f dengue in the two districts of Tanzania. The findings illustrate that the districts have limited readiness in the management and control of dengue outbreaks. The surveillance system is faced by lack of or inappropriate format of guidelines, dissemination and translation for use of SCDs and inadequate laboratory capacity to confirm cases. Low capacity in data management, analysis and use was common in both districts. Inadequate knowledge on outbreak investigation among facility workers and shortage of sample collection and processing tools were identified as critical gaps. To strengthen epidemic preparedness at the district level, a well-functioning supervised surveillance system, with appropriate systems of analysis and feedback covering key indicator variables related to dengue outbreak, is essential.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
LM and CS contributed to the study design. IM, JG, and RN gathered the data. SR, CS, JG, and LM analysed the data. NH, MA, RK, MR, GM, and EK contributed to drafting of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study received financial support from the European and Developing Countries Clinical Trials Partnership (EDCTP2) Programme (Grant RIA2016E-1609) which is supported under Horizon 2020, the European Union’s Framework Programme for Research and Innovation.
Conflict of Interest
The authors declare that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the Dar es Salaam City Council, Ilala and Kinondoni Municipal Councils for their enthusiasm and support to the accomplishment of this study.
References
1. Sindato C, Karimuribo ED, Pfeiffer DU, Mboera LEG, Kivaria F, Dautu G, et al. Spatial and Temporal Pattern of Rift Valley Fever Outbreaks in Tanzania; 1930 to 2007. PloS One (2014) 9(2):e88897. doi: 10.1371/journal.pone.0088897
2. Mboera LEG, Mweya CN, Rumisha SF, Tungu PK, Stanley G, Makange MR, et al. The Risk of Dengue Virus Transmission in Dar Es Salaam, Tanzania During an Epidemic Period of 2014. PloS Negl Trop Dis (2016) 10(1):e004313. doi: 10.1371/journal.pntd.0004313
3. Vairo F, Mboera LEG, De Nardo P, Oriyo NM, Meschi S, Rumisha SF, et al. Clinical, Virologic, and Epidemiologic Characteristics of Dengue Outbreak, Dar Es Salaam, Tanzania, 2014. Emerg Infect Dis (2016) 22(5):895–9. doi: 10.3201/eid2205.151462
4. Kinimi E, Shayo M, Bisimwa P, Angwenyi S, Kasanga C, Weyer J, et al. Evidence of Chikungunya Virus Infection Among Febrile Patients Seeking Healthcare in Selected Districts of Tanzania. Infect Ecol Epidemiol (2018) 8:1553460. doi: 10.1080/20008686.2018.1553460
5. Cao Z, Liu T, Li X, Wang J, Lin H, Chen L, et al. Individual and Interactive Effects of Socio-Ecological Factors on Dengue Fever at Fine Spatial Scale: A Geographical Detector-Based Analysis. Int J Environ Res Public Health (2017) 14:795. doi: 10.3390/ijerph14070795
6. Thomson MC, Muñoz ÁG, Cousin R, Shumake-Guillemot J. Climate Drivers of Vector-Borne Diseases in Africa and Their Relevance to Control Programmes. Infect Dis Poverty (2018) 7:81. doi: 10.1186/s40249-018-0460-1
7. Parham PE, Waldock J, Christophides GK, Hemming D, Agusto F, Evans KJ, et al. Climate, Environmental and Socio-Economic Change: Weighing Up the Balance in Vector-Borne Disease Transmission. Philos Trans R Soc B (2015) 370(1665):20130551. doi: 10.1098/rstb.2013.0551
8. Berkes F, Colding J, Folke C. Navigating Social-Ecological Systems: Building Resilience for Complexity and Change. New York: Cambridge University Press (2003).
9. Walker B, Holling CS, Carpenter SR, Kinzig A. Resilience, Adaptability and Transformability in Social–Ecological Systems. Ecol Soc (2004) 9:5. doi: 10.5751/ES-00650-090205
10. Liu J, Dietz T, Carpenter SR, Alberti M, Folke C, Moran E, et al. Complexity of Coupled Human and Natural Systems. Science (2007) 317:1513–6. doi: 10.1126/science.1144004
12. Powell JR, Tabachnick WJ. History of Domestication and Spread of Aedes Aegypti - A Review. Mem (2013) 108:11–7. doi: 10.1590/0074-0276130395
13. Wilcox BA, Colwell RR. Emerging and Re-Emerging Infectious Diseases: Biocomplexity as an Interdisciplinary Paradigm. EcoHealth (2005) 2(4):244–57. doi: 10.1007/s10393-005-8961-3
14. Wilcox BA, Gubler DJ. Disease Ecology and the Global Emergence of Zoonotic Pathogens. Environ Health Prev Med (2005) 10(5):263–72. doi: 10.1007/bf02897701
15. Smith KR, Ezzati M. How Environmental Health Risks Change With Development: The Epidemiologic and Environmental Risk Transitions Revisited. Ann Rev Environ Res (2005) 30:291–333. doi: 10.1146/annurev.energy.30.050504.144424
16. McLaren L, Hawe P. Ecological Perspectives in Health Research. J Epidemiol Comm Health (2005) 59(1):6–14. doi: 10.1136/jech.2003.018044
17. McLeroy K, Bibeau D, Steckler A, Glanz K. An Ecological Perspective on Health Promotion Programs. Health Edu Behav (1988) 15(4):351–77. doi: 10.1177/109019818801500401
18. Gregson J, Foerster S, Orr R, Jones L, Benedict J, Clarke B, et al. System, Environmental, and Policy Changes: Using the Social-Ecological Model as a Framework for Evaluating Nutrition Education and Social Marketing Programs With Low-Income Audiences. J Nutr Educ Behav (2001) 33:4–15. doi: 10.1016/s1499-4046(06)60065-1
19. Robinson T. Applying the Socio-Ecological Model to Improving Fruit and Vegetable Intake Among Low-Income African Americans. J Comm Health (2008) 33:395–406. doi: 10.1007/s10900-008-9109-5
20. Aguirre AA, Basu N, Kahn LH, Morin XK, Echaubard P, Wilcox BA, et al. Transdisciplinary and Social-Ecological Health Frameworks—Novel Approaches to Emerging Parasitic and Vector-Borne Diseases. Parasite Epidemiol Control (2019) 4:e00084. doi: 10.1016/j.parepi.2019.e00084
21. Camara N, Ngasala B, Leyna G, Abade A, Rumisha SF, Oriyo NM, et al. Socio-Demographic Determinants of Dengue Infection During an Outbreak in Dar Es Salaam City, Tanzania. Tanzania J Health Res (2018) 20(2):21–5. doi: 10.4314/thrb.v20i2.3
22. Population and Housing Census 2012. National Bureau of Statistics, Ministry of Finance (Dar es Salaam), Office of Chief Government Statistician, President’s Office, Finance, Economy and Development Planning. United Republic of Tanzania. (2013).
23. Trpis M. Seasonal Changes in the Larval Populations of Aedes Aegypti in Two Biotypes in Dar Es Salaam, Tanzania. Bull World Health Org (1972) 47:245–55.
24. Trpis M. Dry Season Survival of Aedes Aegypti Eggs in Various Breeding Sites in the Dar Es Salaam Area, Tanzania. Bull World Health Org (1972) 47(3):433–7.
25. Vairo F, Nicastri E, Yussuf SM, Cannas A, Meschi S, Mahmoud MA, et al. IgG Against Dengue Virus in Healthy Blood Donors, Zanzibar, Tanzania. Emerg Infect Dis (2014) 20:465–8. doi: 10.3201/eid2003.130150
26. Okada K, Morita R, Egawa K, Hirai Y, Kaida A, Shirano M. Dengue Virus Type 1 Infection in Traveller Returning From Tanzania to Japan, 2019. Emerg Infect Dis (2019) 25(9):1782–4. doi: 10.3201/eid2509.190814
27. World Health Organization. Weekly Bulletin on Outbreaks and Other Emergencies. Geneva, Switzerland: World Health Organization. (2019). pp. 31–47.
28. Ostrom E. A Diagnostic Approach for Going Beyond Panaceas. Proc Natl Acad Sci USA (2007) 104(39):15181–7. doi: 10.1073/pnas.0702288104
29. Ostrom E. A General Framework for Analyzing Sustainability of Social-Ecological Systems. Science (2009) 325(5939):419–22. doi: 10.1126/science.1172133
30. Poteete A, Janssen MA, Ostrom E. Working Together: Collective Action, the Commons and Multiple Methods in Practice. Princeton, New Jersey, USA: Princeton University Press (2002). doi: 10.1515/9781400835157
31. McGinnis MD, Ostrom E. Social-Ecological System Framework: Initial Changes and Continuing Challenges. Ecol Soc (2014) 19(2):30. doi: 10.5751/ES-06387-190230
32. Partelow S. Key Steps for Operationalizing Social–Ecological System Framework Research in Small-Scale Fisheries: A Heuristic Conceptual Approach. Mar Policy (2015) 51(C):507–11. doi: 10.1016/j.marpol.2014.09.005
33. Hinkel J, Bots PWG, Schlüter M. Enhancing the Ostrom Social-Ecological System Framework Through Formalization. Ecol Soc (2014) 19(3):51. doi: 10.5751/ES-06475-190351
34. Bengtsson M. How to Plan and Perform a Qualitative Study Using Content Analysis. Nurs Open (2016) 8(2):8–14. doi: 10.1016/j.npls.2016.01.001
35. Sharma RC, Thakur A, Sharma M, Mishra S. Teachers’ Perception of Open Educational Resources: Data Collection Through Workshops (ROER4D). Paper Presented at the Open Education Global Conference 2015. Calgary, Ab. (2015).
37. Lain S. Show, Don’t Tell: Reading Workshop Fosters Engagement and Success. TJLE (2017) 5(2):160–7.
38. Knudsen AB, Slooff R. Vector-Borne Disease Problems in Rapid Urbanization: New Approaches to Vector Control. Bull World Health Organ (1992) 70:1–6.
39. Kendall C, Hudelson P, Leontsini E, Winch P, Lloyd L. Urbanization, Dengue, and the Health Transition: Anthropological Contributions to International Health. Med Anthropol Q (1993) 5:257–68. doi: 10.1525/maq.1991.5.3.02a00050
40. Rubio A, Cardo V, Vezzani D. Tire-Breeding Mosquitoes of Public Health Importance Along an Urbanisation Gradient in Buenos Aires, Argentina. Mem Inst Oswaldo Cruz (2011) 16(6):678–84. doi: 10.1590/s0074-02762011000600006
41. Philbert A, Ijumba JN. Preferred Breeding Habitats of Aedes Aegypti (Diptera- Culicidae) Mosquito and its Public Health Implications in Dar Es Salaam, Tanzania. J Environ Res Manage (2013) 4:344–51.
42. Mathias L, Baraka V, Philbert A, Innocent E, Francis F, Nkwengulila G, et al. Habitat Productivity and Pyrethroid Susceptibility Status of Aedes Aegypti Mosquitoes in Dar Es Salaam, Tanzania. . Infect Dis Poverty (2017) 6:1–10. doi: 10.1186/s40249-017-0316-0
43. Saleh F, Kitau J, Konradsen F, Alifrangis M, Lin C, Juma S, et al. Habitat Characteristics for Immature Stages of Aedes Aegypti in Zanzibar City, Tanzania. J Am Mosq Control Assoc (2018) 18(34):190–200. doi: 10.2987/17-6709.1
44. Maheu-Giroux M, Castro MC. Impact of Community-Based Larviciding on the Prevalence of Malaria Infection in Dar Es Salaam, Tanzania. PloS One (2013) 8(8):e71638. doi: 10.1371/journal.pone.0071638
45. World Health Organization. Larval Source Management: A Supplementary Measure for Malaria Vector Control. Geneva, Switzerland: World Health Organization. (2013).
46. Hales S, Weinstein P, Souares Y, Woodward A. El Nino and the Dynamics of Vector-Borne Disease Transmission. Environ Health Perspect (1999) 107(2):99–102. doi: 10.1289/ehp.9910799
47. Pham HV, Doan HTM, Phan TTT, Minh NNT. Ecological Factors Associated With Dengue Fever in a Central Highlands Province, Vietnam. BMC Infect Dis (2011) 11:172. doi: 10.1186/1471-2334-11-172
48. Arunachalam N, Tana S, Espino F, Kittayapong P, Abeyewickreme W, Wai KT, et al. Eco-Bio-Social Determinants of Dengue Vector Breeding: A Multicountry Study in Urban and Periurban Asia. Bull World Health Organ (2010) 88(3):173–84. doi: 10.2471/BLT.09.067892
49. Ault SK. Environmental Management: A Re-Emerging Vector Control Strategy. Am J Trop Med Hyg (1994) 50:35–49. doi: 10.4269/ajtmh.1994.50.35
50. Anno S, Imaoka K, Tadono T, Igarashi T, Sivaganesh S, Kannathasan S, et al. Space–time Clustering Characteristics of Dengue Based on Ecological, Socio-Economic, and Demographic Factors in Northern Sri Lanka. Geosp Health (2015) 10(376):215–22. doi: 10.4081/gh.2015.376
51. Gubler DJ, Clark GG. Community Involvement in the Control of. Aedes aegypti Acta Trop (1996) 61:169–79. doi: 10.1016/0001-706x(95)00103-1
52. Parks W, Lloyd L. Planning Social Mobilization and Communication for Dengue Fever Prevention and Control a Step-By-Step Guide. Geneva: World Health Organization (2004).
53. Grimshaw JM, Russell IT. Effect of Clinical Guidelines on Medical Practice: A Systematic Review of Rigorous Evaluations. Lancet (1993) 342:1317–22. doi: 10.1016/0140-6736(93)92244-n
54. Nathwani D, Rubinstein E, Barlow G, Davey P. Do Guidelines for Community-Acquired Pneumonia Improve the Cost-Effectiveness of Hospital Care? Clin Infect Dis (2001) 32(5):728–41. doi: 10.1086/319216
55. Grol R, Grimshaw J. From Best Evidence to Best Practice: Effective Implementation of Change in Patients’ Care. Lancet (2003) 362(9391):1225–30. doi: 10.1016/S0140-6736(03)14546-1
56. Gagliardi AR, Brouwers MC, Palda VA, Lemieux-Charles L, Grimshaw JM. How can We Improve Guideline Use? A Conceptual Framework of Implementability. Implement Sci (2011) 6:26. doi: 10.1186/1748-5908-6-2.6
57. Armstrong PW. Do Guidelines Influence Practice? Heart (2003) 89(3):349–52. doi: 10.1136/heart.89.3.349
58. Schunemann HJ, Fretheim A, Oxman AD. Improving the Use of Research Evidence in Guideline Development: 1. Guidelines for Guidelines. Health Res Policy Syst (2006) 4:13. doi: 10.1186/1478-4505-4-13
59. Stanback J, Griffey S, Lynam P, Ruto C, Cummings S. Improving Adherence to Family Planning Guidelines in Kenya: An Experiment. Int J Qual Health Care (2007) 19(2):68–73. doi: 10.1093/intqhc/mzl072
60. Francke AL, Smit MC, de Veer AJ, Mistiaen P. Factors Influencing the Implementation of Clinical Guidelines for Health Care Professionals: A Systematic Meta-Review. BMC Med Inform Dec (2008) 8:38. doi: 10.1186/1472-6947-8-38
61. Karimuribo ED, Mutagahywa E, Sindato C, Mboera L, Mwabukusi M, Kariuki Njenga M, et al. A Smartphone App (AfyaData) for Innovative One Health Disease Surveillance From Community to National Levels in Africa: Intervention in Disease Surveillance. JMIR Public Health Surv (2017) 3(4):e94. doi: 10.2196/publichealth.7373
62. Anno S, Hara T, Kai H, Chang Y, Lee M-A, Oyoshi K, et al. Deep Learning Applications for Predicting Dengue Fever Outbreak. J Environ Res (2018) 2:21.
63. Nelson C, Lurie N, Wasserman J. Assessing Public Health Emergency Preparedness: Concepts, Tools, and Challenges. Annu Rev Public Health (2008) 28:1–18. doi: 10.1146/annurev.publhealth.28.021406.144054
64. Mghamba JM, Mboera LEG, Krekamoo W, Senkoro KP, Rumisha SF, Shayo E, et al. Challenges of Implementing an Integrated Disease Surveillance and Response Strategy Using the Current Health Management Information System in Tanzania. Tanzania Health Res Bull (2004) 6:57–63. doi: 10.4314/thrb.v6i2.14243
65. Phalkey RK, Yamamoto S, Awate P, Marx M. Challenges With the Implementation of an Integrated Disease Surveillance and Response (IDSR) System: Systematic Review of the Lessons Learned. Health Policy Plann (2015) 30(1):131–43. doi: 10.1093/heapol/czt097
66. Rumisha SF, Mboera LE, Senkoro KP, Gueye D, Mmbuji PK. Monitoring and Evaluation of Integrated Disease Surveillance and Response in Selected Districts in Tanzania. Tanzania Health Res Bull (2007) 9:1–11. doi: 10.4314/thrb.v9i1.14285
67. Alemu T, Gutema H, Legesse S, Nigussie T, Yenew Y, Gahse K. Evaluation of Public Health Surveillance System Performance in Dangila District, Northwest Ethiopia: A Concurrent Embedded Mixed Quantitative/Qualitative Facility-Based Cross-Sectional Study. BMC Public Health (2019) 19:1343. doi: 10.1186/s12889-019-7724-y
68. Begashaw B, Tesfaye T. Assessment of Integrated Disease Surveillance and Response Implementation in Special Health Facilities of Dawuro Zone. J Anesthesiol (2016) 4(3):11–5. doi: 10.11648/j.ja.20160403.11
69. Motilewa O, Akwaowo CD, Ekanen AM. Assessment of Implementation of Integrated Disease Surveillance and Response in Akwaibom State, Nigeria. Ibom Med J (2015) 8(1):24–5.
Keywords: dengue, outbreak, readiness, surveillance, Tanzania, socio-ecological systems
Citation: Mboera LEG, Sindato C, Mremi IR, Rumisha SF, George J, Ngolongolo R, Misinzo G, Karimuribo ED, Rweyemamu MM, Haider N, Hamid MA and Kock R (2021) Socio-Ecological Systems Analysis and Health System Readiness in Responding to Dengue Epidemics in Ilala and Kinondoni Districts, Tanzania. Front. Trop. Dis 2:738758. doi: 10.3389/fitd.2021.738758
Received: 09 July 2021; Accepted: 26 August 2021;
Published: 10 September 2021.
Edited by:
Suraj Bhattarai, Global Institute for Interdisciplinary Studies (GIIS), NepalReviewed by:
Basu Dev Pandey, Nagasaki University, JapanJohnson Matowo, Kilimanjaro Christian Medical University College, Tanzania
Copyright © 2021 Mboera, Sindato, Mremi, Rumisha, George, Ngolongolo, Misinzo, Karimuribo, Rweyemamu, Haider, Hamid and Kock. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leonard E. G. Mboera, bG1ib2VyYUBnbWFpbC5jb20=