 Larissa C. Rocha1Magda O. S. Carvalho2,3,4Valma M. L. Nascimento1Milena S. dos Santos5Tânia F. Barros3Elisângela V. Adorno3Joice N. Reis3Caroline C. da Guarda2Rayra P. Santiago2
Larissa C. Rocha1Magda O. S. Carvalho2,3,4Valma M. L. Nascimento1Milena S. dos Santos5Tânia F. Barros3Elisângela V. Adorno3Joice N. Reis3Caroline C. da Guarda2Rayra P. Santiago2 Marilda de Souza Gonçalves2,3*
Marilda de Souza Gonçalves2,3*- 1Fundação de Hematologia e Hemoterapia da Bahia, Bahia, Brazil
- 2Centro de Pesquisa Gonçalo Moniz-Fiocruz, Bahia, Brazil
- 3Faculdade de Farmácia, Universidade Federal da Bahia, Bahia, Brazil
- 4Hospital Universitário Professor Edgard Santos - Universidade Federal da Bahia (HUPES-UFBA), Bahia, Brazil
- 5Instituto Multidisciplinar em Saúde, Universidade Federal da Bahia, Bahia, Brazil
We investigated the nasopharynx and oropharynx microbiota in sickle cell disease (SCD) to identify the microorganisms, antibiotic sensitivity, prevalent serotypes, and association of with laboratorial markers. Oropharynx/nasopharynx secretions were investigated in 143 SCD children aging 6 months to 17 years. Pathogens were isolated using standard procedures, and laboratorial markers were performed by automated methods. Staphylococcus aureus (S. aureus) was isolated from nasopharynx and oropharynx of 64 and of 17 SCD children respectively. Streptococcus pneumoniae (S. pneumoniae) was isolated from the nasopharynx and oropharynx of eight SCD patients. Serotypes of S. pneumoniae were 19F, 23F, and 14. All isolates were susceptible to penicillin, and patients whose nasopharynx and oropharynx were colonized by S. pneumoniae had high concentrations of aspartate transaminase, alanine transaminase, and ferritin. S. pneumoniae isolated were not penicillin-resistant serotypes suggesting that the use of penicillin for prophylaxis and/or treatment of infections is safe. Our finding of colonization and laboratory evaluation in SCD patients suggests that microorganisms are involved in the modulation of chronic inflammatory. The association of colonized microorganisms and laboratorial markers suggest a new approach to these patients follow-up, and additional studies of microorganism colonization and their association with SCD patients' clinical outcome will improve control and prevention strategies.
Introduction
Infections are the major cause of death in children with sickle cell anemia (SCA) (Williams et al., 2009). Likewise, bacterial infection is the primary cause of death during childhood; infants and children younger than 3 years of age are at risk of mortality and morbidity from sepsis (Iughetti et al., 2016). Streptococcus pneumoniae (S. pneumoniae) is a genetically variable organism that colonizes the human upper respiratory mucosa coexisting with the normal microbiota and establishing a state of asymptomatic colonization (Cardozo et al., 2006; Mitchell and Mitchell, 2014). S. pneumoniae is an epidemiologically important pathogen with a worldwide distribution that causes invasive (i.e., pneumonia, bacteraemia, meningitis, sepsis, and arthritis) and non-invasive diseases (i.e., sinusitis, otitis media, conjunctivitis, bronchitis, and pneumonia) (Bogaert et al., 2004b; World Health Organization, 2007; Liñares et al., 2010). Staphylococcus aureus (S. aureus) infections have recently increased and represent a public health problem in the United States of America (USA) (Bogaert et al., 2004b; Fridkin et al., 2005; Kuehnert et al., 2006). S. aureus causes pneumonia, sepsis and osteo-articular, skin, and soft tissue infections (Gonzalez et al., 2005; Moran et al., 2005; Kuehnert et al., 2006). The growing number of community-acquired infections caused by methicillin-resistant S. aureus in children and healthy adults is a major problem (Fridkin et al., 2005; Gonzalez et al., 2005; Kuehnert et al., 2006), particularly in countries such as Brazil, where nasal carriage prevalence (48%) (Braga et al., 2014) is higher than those described in other countries of Latin America (Gardella et al., 2011).
Pneumococcal conjugate vaccine has minimal impact on overall carriage rate due to non-vaccine serotypes replacement, but could influence others bacterial species in the nasopharynx (Shak et al., 2013). It has been described after immunization by the 7-valent pneumococcal vaccine an inverse relationship between nasopharyngeal carriage of vaccine type S. pneumoniae and S. aureus, as well as an increase of infections, especially acute otitis media (Ferreira et al., 2001; Bogaert et al., 2004a; Moran et al., 2005; Kuehnert et al., 2006). Thus, the colonization of the upper respiratory tract may be an important factor in the occurrence of local or systemic disease among SCD patients.
Studies assessing the prevalence of pneumococcal nasopharyngeal colonization demonstrate that the presence of these bacteria may be influenced by several factors, such as age, genetic background, geographic area, and environmental conditions (Ferreira et al., 2001; Bogaert et al., 2004b). Fonseca et al. (2005) evaluated 98 children with SCD in the Brazilian state of Sao Paulo and found that the nasopharynx was colonized by pneumococcus in 13.3% of children. In the USA, the rate of nasopharyngeal colonization in SCD patients ranges from 5 to 17% (Anglin et al., 1984; Steele et al., 1996). Previous studies have described the exposure of these bacteria to penicillin and the selection of antibiotic resistant strains (Denno et al., 2002). However, previous studies assessing penicillin resistance in children with SCD who regularly use penicillin have reported controversial results. Norris et al. (1996) found that 33% of pneumococcus was penicillin-resistant and that 36% of these strains exhibited high resistance. However, Fonseca et al. (2005) found no strains that exhibited high resistance to penicillin. The aims of the present study were to evaluate the nasopharynx/oropharynx colonization in Brazilian children with SCD, identify the penicillin sensitivity profile among S. pneumoniae-colonized patients; describe the most prevalent serotypes causing invasive diseases. Furthermore, we described the association of microorganisms' colonization with biochemical laboratorial markers.
Materials and Methods
This study was conducted with 143 SCD patients, aged from 6 months to 17 years, who were prospectively selected from the outpatients at the pediatric hematology department of the Fundação de Hematologia e Hemoterapia do Estado da Bahia (HEMOBA), which is a reference center for clinical assistance, from March to December 2010. All the involved patients were from Bahia, a state on Northeast Brazil and the majority of patients lived in Salvador (state capital) or metropolitan area. All SCD patients were in a steady state, which was characterized by the absence of acute clinical events, infections or inflammatory episodes, and did not undergo any blood transfusion procedures prior to sampling.
Nasopharyngeal and oropharyngeal swabs samples were collected by a researcher on the day of the interview. Additional, clinical and epidemiological information were collected using questionnaires after interviews with the parents; this information was supplemented with information contained in the medical records, such as age, gender, race, SCD genotype (i.e., HbSS and HbSC), prophylaxis, vaccination with the pneumococcal 7-valent and 23-valent vaccines, and laboratory data (i.e., blood cell count, evidence of haemolysis, and evaluation of inflammation).
Nasopharyngeal material was collected during the patients' routine clinic visits using sterile swabs, which were introduced carefully into the right and left nostrils to a depth equal to two-thirds of the distance between the nose and ear lobe (Norris et al., 1996). After the nasopharynx material was collected, another swab was used to collect oropharynx material. Each swab was subsequently immersed in media for bacterial transport and was sent (at room temperature) to the bacteriology laboratory of the Faculdade de Farmácia at the Universidade Federal da Bahia within 1–2 h of collection.
Collected material was inoculated onto blood agar plates containing 5% sheep blood and was incubated at 36 ± 1°C with a 5–10% CO2 atmosphere. The presence of a gray-green zone around the colonies (i.e., alpha-haemolysis) was presumptive of S. pneumoniae. Confirmation was obtained using the rapid agglutination test with latex particles and by evaluating the inhibitory zone around Optochin differentiation disks; when necessary, the bile solubility test was also performed. Other bacteria were identified using the Gram method to analyse colony characteristics, such as size, color, shape, growth on selective media, and subsequent analysis of biochemical and metabolic activities.
Evaluation of susceptibility to penicillin was performed using the disk diffusion method with oxacillin (1 μg) according to Clinical and Laboratory Standards Institute guidelines (Clinical Laboratory Standards Institute (CLSI), 2012). When the inhibitory zone was >20 mm, the microorganism sample was considered penicillin-susceptible, and when the inhibitory zone was <19 mm, the microorganism was considered penicillin-resistant. The minimum inhibitory concentration (MIC) for penicillin was determined using the E-test in all pneumococcal strains resistant to oxacillin (i.e., halo <19 mm). The MIC for penicillin was interpreted as susceptible when the obtained value was <0.06 mg/mL; intermediate when the obtained value was 0.1–1 mg/mL; and resistant when the obtained value was > 2.0 μg/mL (Liñares et al., 2010). Bacterial resistance was also determined for erythromycin, trimethoprim-sulfamethoxazole, clindamycin, and cefotaxime. Serotyping of the isolated pneumococcal strains was performed using the Quellung Neufeld reaction with antisera produced at the Statem Serum Institute in Copenhagen, Denmark.
Chemical and immunological markers were evaluated by immunochemistry and with the A25 Immunoassay system (Biosystems SA, Costa Brava, Barcelona, Spain), the Access® 2 Immunoassay system X2 (Beckman Coulter, Inc., Fullerton, CA, USA) and the Immage® 800 system (Beckman Coulter, Fullerton, CA, USA). Haematological parameters were quantified using an electronic cell counter (Coulter Corporation, FL, USA), and hemoglobin (Hb) patterns were investigated using high performance liquid chromatography (HPLC) (Bio-Rad Variant-I; Bio-Rad, Hercules, CA, USA).
Statistical Analysis
The distribution of quantitative variables was evaluated using the Kolmogorov-Smirnov test. The Mann-Whitney test and the unpaired Student's t-test were used to estimate differences in hematological and chemical markers among steady-state SCD children with and without nasopharynx/oropharynx colonization. Differences were considered significant when the p-values were <0.05. The statistical analyses were performed using EPI info 6.04 (Centers for Disease Control & Prevention (CDC), Atlanta, GA, United States) and Graphpad Prism Software 5.01 (San Diego, CA).
Multivariate analyses were performed to estimate the likelihood of having pneumonia and infection as outcome (dependent variable) and a possible interaction with oropharynx colonization, neutrophils count, leukocytes count, platelets count, hemoglobin profile, reticulocytes count, and nasopharynx colonization as independent variables, adjusted for sex and age.
Ethics Statement
All children's guardians agreed to participate in the study after reading the terms of informed consent and signing the consent form. After that, the material was collected. The human subject research board of the Centro de Pesquisas Gonçalo Moniz- Fundação Oswaldo Cruz- Bahia (CPqGM-FIOCRUZ-BA) approved the study (CAAE 0031.0.225.000-06). The study was performed after obtaining written consent and followed the Brazilian standards for the development of research on humans. This work was conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983.
Results
A total of 143 SCD patients were investigated; 44/143 (30.8%) had SC disease (i.e., HbSC), and 99/143 (69.2%) had sickle cell anemia (SCA). The distribution according to sex was 66/143 (46.1%) female patients and 77/143 (53.9%) male patients. The average age of the SCD patients was 9.25 ± a standard deviation (SD) of 4.06 years. Also, 41/143 (28.6%) patients were less than or equal to 5 years old, and 102/143 (71.4%) patients were over 5 years old. Clinical manifestations of SCD patients are presented on Table 1.
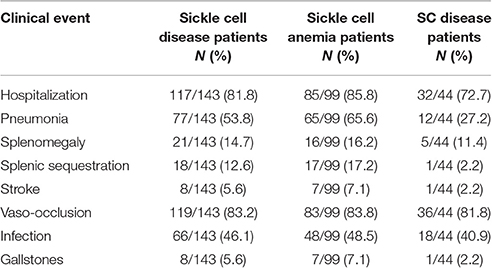
Table 1. Clinical manifestations of SCD patients.
We identified that 85.3% (122/143) of the patients received the pneumococcal 7-valent conjugate vaccine, through the public health Brazilian system. Approximately 14% (14.7%) (21/143) were not vaccinated or received at least one of the three commonly available doses.
Haematological and chemical markers were evaluated in the SCD patients (Table 2). The oropharynx/nasopharynx culture procedure enabled the collection of various microorganisms with an emphasis on S. aureus and S. pneumoniae. Pneumococcus was isolated from the nasopharynx/oropharynx in 16 of 143 children representing a colonization rate of 11.2%. One child with pneumococcal colonization was colonized by two different serogroups (Table 3).
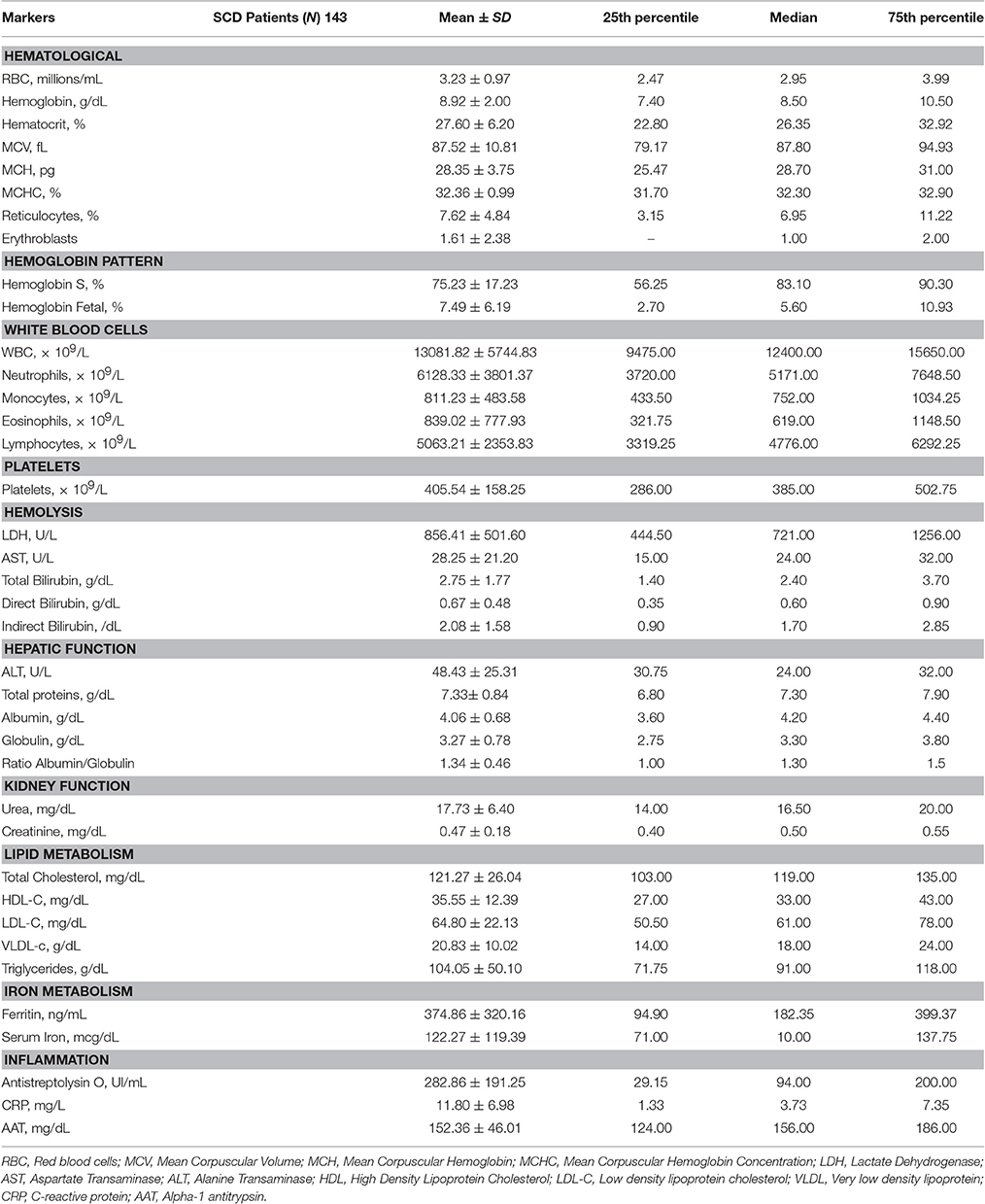
Table 2. Distribution of variables associated with lipid, renal, and hepatic metabolism; haemolysis; and inflammation in patients with sickle cell disease (SCD).
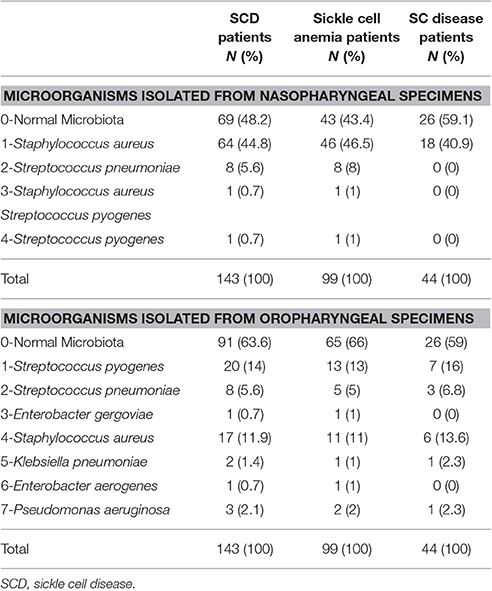
Table 3. Profile of the microorganisms identified in the analysis of specimens isolated from the nasopharynx and oropharynx of patients with sickle cell disease (SCD).
All children under 6 years of age used prophylactic penicillin and received pneumococcal vaccines according to the expected age. None of the pneumococcal isolates exhibited resistance to penicillin. Serotypes and their antibiotic susceptibility are shown in Table 4.
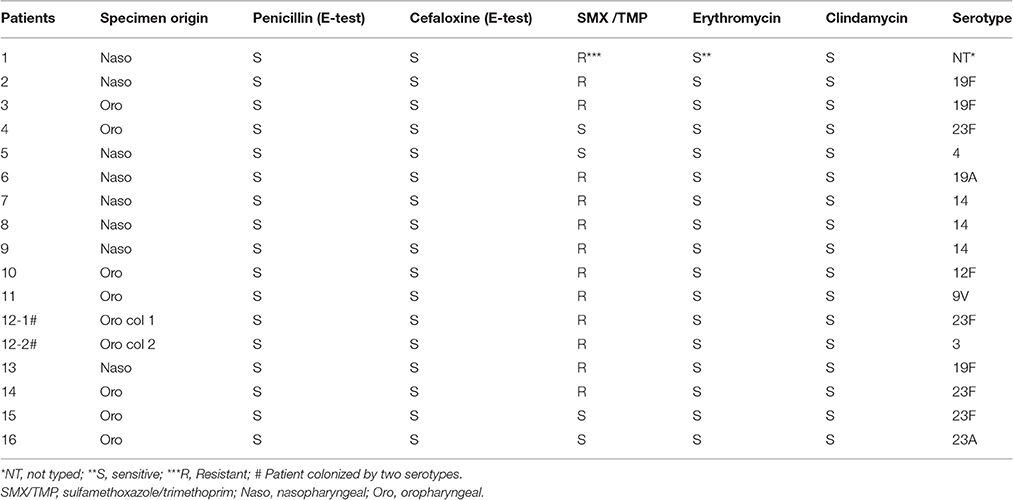
Table 4. Antibiogram and serotype profiles of Streptococcus pneumonia isolated from nasopharyngeal (Naso) and oropharyngeal (Oro) specimens from patients with sickle cell disease.
An analysis of the association of hematological and chemical markers with nasopharynx and oropharynx colonization revealed a significant association between ferritin (ng/mL) and oropharyngeal colonization by S. aureus and S. pneumoniae with a mean and SD of 245.1 ± 240.8 for subjects colonized by normal microbiota (91/143); 627.6 ± 624.4 for individuals colonized by S. pneumoniae (8/143); and 460.6 ± 148.8 for individuals colonized by S. aureus (17/143) (p = 0.0016). The analysis also revealed significant differences in ferritin between individuals colonized by normal microbiota and individuals colonized by S. aureus (p = 0.0144) and between individuals colonized by normal microbiota and individuals colonized by S. pneumoniae (p < 0.0001) (Figure 1).
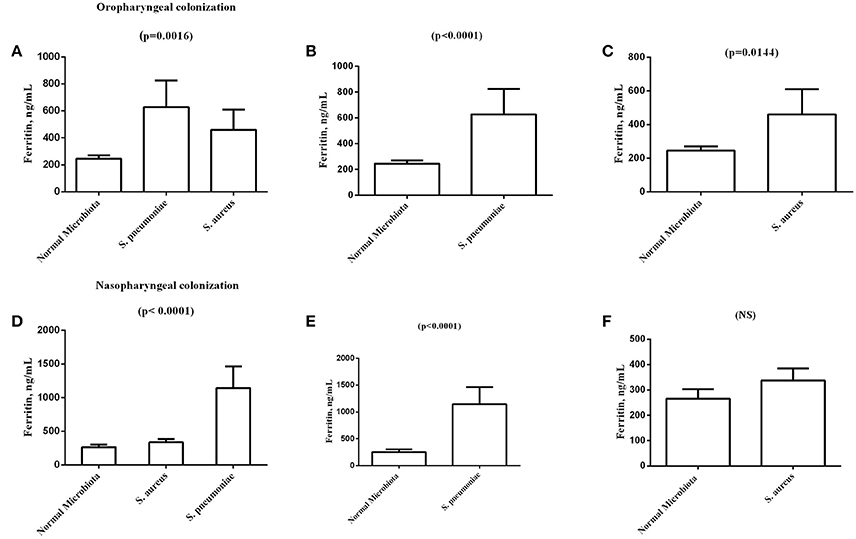
Figure 1. Graphical representation of the analysis of sickle cell anemia patients' oropharyngeal and nasopharyngeal colonization by normal microbiota, Staphylococcus aureus, and Streptococcus pneumoniae and by its association with ferritin values (ng /mL). (A) Comparison of ferritin levels among normal Microbiota, S. pneumonia, and S. aureus in oropharyngeal colonization. (B) Comparison of ferritin levels between normal Microbiota and S. pneumoniae in oropharyngeal colonization. (C) Comparison of ferritin levels between normal Microbiota and S. aureus oropharyngeal colonization. (D) Comparison of ferritin levels among normal Microbiota, S. pneumonia, and S. aureus in nasopharyngeal colonization. (E) Comparison of ferritin levels between normal Microbiota and S. pneumoniae in nasopharyngeal colonization. (F) Comparison of ferritin levels between Normal Microbiota and S. aureus nasopharyngeal colonization. S. aureus, Staphylococcus aureus; S. pneumonia, Streptococcus pneumoniae; NS, Not significant.
A statistical analysis of the association between biochemical markers and the presence of nasopharyngeal colonization by S. aureus and S. pneumoniae revealed significant differences in ferritin with a mean and standard deviation of 324.0 ± 46.06 for subjects who were colonized by normal microbiota (69/143), 383.1 ± 336.8 for individuals colonized by S. aureus (64/143), and 1144 ± 641.8 for individuals colonized by S. pneumoniae (8/143) (p < 0.0001). The analysis also revealed significant differences when comparing ferritin values in individuals colonized by normal microbiota and individuals colonized by S. pneumoniae (p < 0.0001) (Figure 1).
Statistical analysis of alanine transaminase (ALT)-values (U/L) revealed significant differences with a mean and standard deviation of 48.42 ± 22.19 for subjects colonized by normal microbiota (69/143); 48.38 ± 28.55 for individuals colonized by S. aureus (64/143); and 85.50 ± 29.22 for individuals colonized by S. pneumoniae (8/143) (p = 0.02). The analysis also revealed significant differences when comparing ALT-values in individuals colonized by normal microbiota and individuals colonized by S. pneumoniae (p = 0.002) (Figure 2).
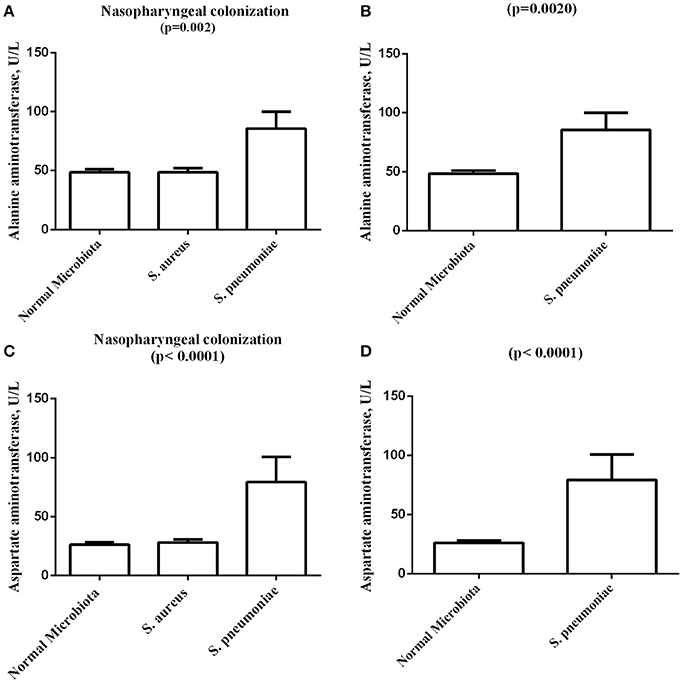
Figure 2. Graphical representation of the analysis of sickle cell anemia patients nasopharyngeal colonization by normal microbiota, Staphylococcus aureus, and Streptococcus pneumoniae and its association with biochemical variables. (A) Comparison of alanine aminotransferase levels among normal Microbiota, S. aureus, and S. pneumoniae nasopharyngeal colonization. (B) Comparison of alanine aminotransferase levels between normal Microbiota and S. pneumoniae nasopharyngeal colonization. (C) Comparison of aspartate aminotransferase levels among normal Microbiota, S. aureus, and S. pneumoniae nasopharyngeal colonization. (D) Comparison of aspartate aminotransferase levels between normal Microbiota and S. pneumoniae nasopharyngeal colonization. S. aureus, Staphylococcus aureus; S. pneumonia, Streptococcus pneumoniae.
Statistical analysis of aspartate transaminase (AST) values (U/L) revealed significant differences with a mean and standard deviation of 26.21 ± 16.76 for subjects colonized by normal microbiota (693/143); 28.02 ± 21.87 for individuals colonized by S. aureus (64/141); and 79.25 ± 43.15 for individuals colonized by S. pneumoniae (8/143) (p < 0.0001). The analysis also revealed significant differences when comparing AST values in individuals colonized by normal microbiota and individuals colonized by S. pneumoniae (p < 0.0001) (Figure 2).
The multivariate analysis adjusted for age and sex found that infection was independently associated to oropharynx colonization (P = 0.003; OR = 4.9; 95% IC 1.7–14.0) and leukocyte count (P = 0.0046; OR = 8.8; 95% IC 1.9–39.9) (Table 5), and that pneumonia was independently associated to hemoglobin profile (P = 0.006; OR = 4.3; 95% IC 1.5–12.5) (Table 6).
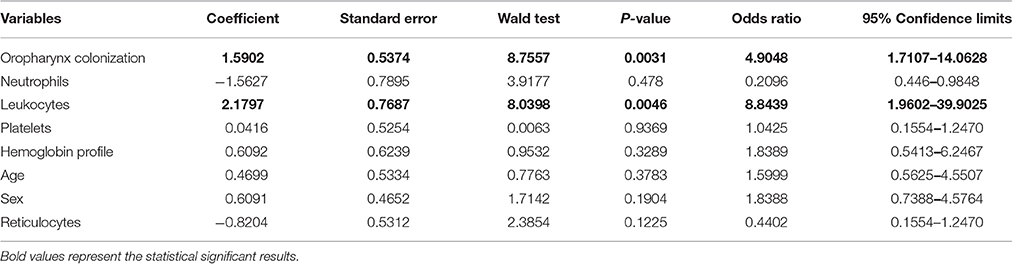
Table 5. Multivariate analyses models in sickle cell disease patients with infection as the dependent variable.
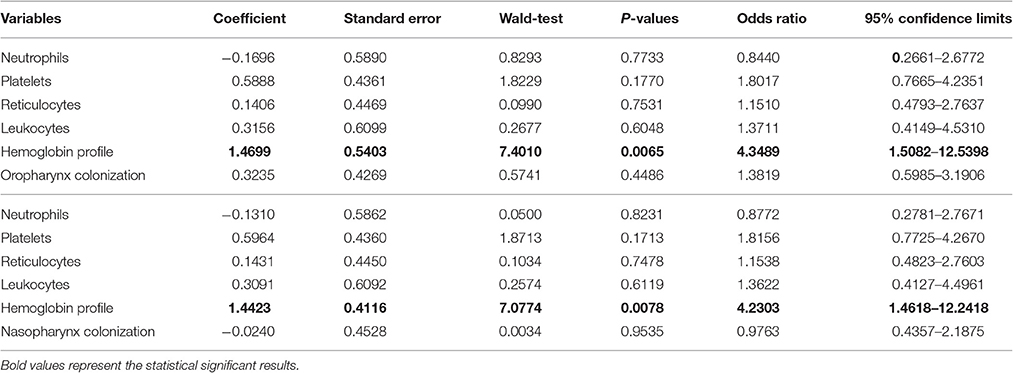
Table 6. Multivariate analyses models in sickle cell disease patients with pneumonia as the dependent variable.
Discussion
The SCD has a high prevalence worldwide with clinical variability and a variety of factors modulating the disease phenotype; these factors make understanding patient characteristics fundamental to improving patient care and to modifying the natural history of the disease (Quinn et al., 2004; Williams et al., 2009).
Infections caused by S. pneumoniae are a major cause of morbidity and mortality in children worldwide, particularly in children under 5 years old, and are frequent in individuals with chronic cardiopulmonary diseases and in elderly and immunocompromised individuals (Hausdorff et al., 2000). Similarly, the incidence of S. aureus infections are increasing and are now considered a public health problem in the United States of America (Denno et al., 2002; Bogaert et al., 2004b; Cardozo et al., 2006). Although an early onset of prophylaxis with Penicillin and a proper treatment of the infections have increased the overall survival in childhood (Iughetti et al., 2016). Given the high susceptibility to pneumococcal infection, children with SCD are routinely immunized with pneumococcal vaccines and administered prophylactic antibiotics alongside (Mitchell and Mitchell, 2014).
In the current study, we observed nasopharyngeal/oropharynx colonization by S. pneumoniae in 11.2% of SCD patients and by S. aureus in 56.7% of SCD patients. Steele et al. (1996) observed nasopharyngeal colonization by S. pneumonia in 33% of children with SCD who were under two years of age; in 10% of children 2–5 years of age; and in 6% of children 5 years of age. These results were similar to those described by Norris et al. (1996). Fonseca et al. (2005) reported a prevalence of 13.3% for nasopharyngeal colonization by S. pneumoniae among Brazilian children with SCD in São Paulo. We emphasize that none of the studies cited above included a description of colonization by other pathogens.
Results obtained in this study allow us to hypothesize that a reduction in nasopharyngeal colonization most likely occurs secondarily to proper use of pneumococcal vaccines suggesting the likely effectiveness of vaccination coverage for serotypes that cause invasive disease. In addition, the S. aureus colonization results suggest a possible role of nasopharyngeal colonization by this microorganism in SCD in the children investigated in this study. A similar role has been was suggested by Lee et al. (2009) who studied the epidemiology of and risk factors for colonization with S. aureus in children in Massachusetts (USA) and concluded that colonization by methicillin-resistant S. aureus remained stable among children from 2003 to 2004 and from 2006 to 2007 despite the widespread use of the pneumococcal conjugate vaccine. Nasal colonization varied with age and was inversely proportional to the recent use of antibiotics.
The profile of pneumococcal strain sensitivity described in the present study revealed no increase in resistance to penicillin compared to data obtained in previous studies in Brazil that included invasive and colonizing strains (Baynes et al., 1986; Moran et al., 2005; Marchese et al., 2011). However, the pneumococcal penicillin sensitivity results presented in this study corroborate those reported by Fonseca et al. (2005) who analyzed 98 Brazilian children from São Paulo and suggested that penicillin remains safe for both prophylaxis and treatment in children with SCD. The authors reported high pneumococcal resistance to clotrimoxazol (sulfamethoxazole/trimethoprim (SMX/TRP) combination) that was 64%. These results suggest that this antibiotic should be used with caution for the treatment of S. pneumoniae infections in patients similar to those included in this study.
Most of the identified strains of S. pneumoniae were from serotypes that cause invasive diseases in Brazil (Berezin et al., 2002; Mantese et al., 2003). In the present study, we observed the presence of serotypes that dominate in reports of infections in children worldwide (i.e., 6, 14, 19, 23) (Sniadack et al., 1995) with the exception that we did not identify serotype 6. Marchese et al. (2011) evaluated blood cultures from children up to 5 years of age in Italy who were hospitalized for community-acquired pneumonia and identified serotypes 19A and 14 more frequently than other serotypes corroborating the results reported in the present study. Brandileone et al. (1998) reported that infections caused by serotypes 1 and 5 are common in our country; however, in the present study, these serotypes were not isolated corroborating the results reported by Fonseca et al. (2005) and comments made by Berezin et al. (2002) who considered these serotypes significant in the context of nasopharyngeal colonization.
Chemical and hematological measurements are important for monitoring the clinical course of disease in patients with SCD. Children with HbSS exhibited significant differences in almost all analyses when compared to the HbSC group corroborating the results presented by Seixas et al. (2010) who studied children with SCD from the same population. These results also confirm existing data in the literature related to the clinical severity of HbSS compared to other types of SCD (Steinberg and Rodgers, 2001).
Among the biochemical markers analyzed in this study, those associated with inflammation, haemolysis, infection, and oxidative stress were highlighted with an emphasis on patients who exhibited serum ferritin concentrations above the mean values established for the group (≥320.16). Because this protein increases during inflammatory and infectious processes, an accumulation of iron may occur in these patients (Rogers, 1996). SCD is characterized by a proinflammatory state with the presence of abnormal endothelial activation (Belcher et al., 2014). At baseline, ferritin is an important protein for maintaining iron stores in the body. However, during the inflammatory processes, ferritin is regulated by hepcidin and interleukin-6 (IL-6) levels. Other proinflammatory cytokines, such as IL-1β and tumor necrosis factor alpha (TNF-α), also indirectly induce the synthesis of ferritin because they increase the incorporation of iron by hepatocytes (Baynes et al., 1986; Jurado, 1997). The association of a chronic inflammatory state with the observation of increased ferritin values in SCD patients colonized by microorganisms can serve as a marker of clinical severity.
It is known that encapsulated bacteria, in particular S. pneumoniae, have a polysaccharide capsule that impedes binding of complement or prevents complement assembled on the cell wall from interacting with macrophage receptors (Bohnsack and Brown, 1986). On the other hand, macrophages engulfing the abnormally sickle shaped cells may become “blocked,” impairing their phagocytosis of other particles, which may contribute to the infection prolongation (Booth et al., 2010). McCavit et al. (2011) described seven invasive pneumococcal diseases due to non-vaccinal serotypes on SCD patients after the pneumococcal 7-valent conjugate vaccine. These facts allow us to suggest that both inflammation and colonization processes are responsible for the abnormal ferritin levels found in our patients.
The results presented in this study demonstrate that patients whose nasopharynx is colonized by S. pneumoniae exhibit high levels of AST, ALT, and ferritin. These associations demonstrate that routine biochemical evaluations and assessments of nasopharynx colonization may be important when monitoring the clinical course of SCD patients. The significant differences observed in this study suggest that the colonization by microorganisms is involved in the modulation of inflammatory events in these patients; the presence of pathogens may increase reactive oxidative species maintaining the inflammatory state and increasing disease severity. Unfortunately, we did not compare our findings with previous reports because no similar data were available in the literature.
Studies of the colonization of the nasopharynx and oropharynx by microorganisms in children with SCD can provide important information for public health programs, avoiding severe infections. However, the finding of altered levels of molecules associated with hemolysis and inflammation among SCD individuals with nasopharynx and oropharynx colonization emphasizes the need to elucidate the mechanisms that may determine the development of an invasive infection disease, since the influence of colonization on therapeutic and vaccine effectiveness are poorly understood. Moreover, it is important to clarify the mechanisms by which the biomarkers involved are associated with the presence of these microorganisms and inflammatory processes among SCD patients. This type of information would improve our understanding of these processes and the clinical prognosis in these patients.
Author Contributions
LR and MdSG conceived the study; LR, MC, VN, MSdS, TB, EA, JR, and MdSG designed the study protocols; LR, MC, VN, and MdSG performed the clinical assessments; LR, MC, VN, MSdS, TB, EA, JR, and MdSG performed data analysis and interpreted the data; LR, CD, RS, and MdSG drafted the manuscript; LR, MC, TB, EA, JP, CD, RS, and MdSG critically revised the manuscript for intellectual content. All authors read and approved the final manuscript. MdSG is the guarantor of the paper.
Funding
This work and was supported by grants from the Brazilian National Council of Research (CNPq) (311888/2013-5) (MdSG); the Foundation Research and Extension of Bahia (FAPESB) (3626/2013, 1431040053063, and 9073/2007) (MdSG); and PPSUS/FAPESB (020/2013 EFP-00007295), (MdSG); the Instituto Nacional de Ciência e Tecnologia do Sangue (CNPq) (Coordinated by S.T.O.S.), and MCD/CNPq/MS-SCTIE-DECIT (409800/2006-6), (MdSG). Sponsors of this study are public or nonprofit organizations that support science in general. They had no role in gathering analyzing, or interpreting the data.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the nurses and all of the health professionals who assisted all patients, and provided technical support for this study, and all sickle cell disease patients included in this study and their families.
References
Anglin, D. L., Siegel, J. D., Pacini, D. L., Smith, S. J., Adams, G., and Buchanan, G. R. (1984). Effect of penicillin prophylaxis on nasopharyngeal colonization with Streptococcus pneumoniae in children with sickle cell anemia. J. Pediatr. 104, 18–22. doi: 10.1016/S0022-3476(84)80582-X
Baynes, R., Bezwoda, W., Bothwell, T., Khan, Q., and Mansoor, N. (1986). The nonimmune inflammatory response: serial changes in plasma iron, ironbinding capacity, lactoferrin, ferritin and C-reactive protein. Scand. J. Clin. Lab. Invest. 46, 695–704. doi: 10.3109/00365518609083733
Belcher, J. D., Chen, C., Nguyen, J., Milbauer, L., Abdulla, F., Alayash, A. I, et al. (2014). Heme triggers TLR4 signaling leading to endothelial cell activation and vaso-occlusion in murine sickle cell disease. Blood 123, 377–390. doi: 10.1182/blood-2013-04-495887
Berezin, E. N., Falleiros-Carvalho, L. H., Lopes, C. R., Sanajotta, A. T., Brandileone, M. C., Menegatti, S., et al. (2002). Pneumococcal meningitis in children: clinical findings, most frequent serotypes and outcome. J. Pediatr. 78, 19–23. doi: 10.2223/JPED.660
Bogaert, D., Hermans, P. W., Adrian, P. V., Rümke, H. C., and de Groot, R. (2004a). Pneumococcal vaccines: an update on current strategies. Vaccine 22, 2209–2220. doi: 10.1016/j.vaccine.2003.11.038
Bogaert, D., van Belkum, A., Sluijter, M., Luijendijk, A., de Groot, R., Rümke, H. C., et al. (2004b). Colonisation by Streptococcus pneumoniae and Staphylococcus aureus in healthy children. Lancet 363, 1871–1872. doi: 10.1016/S0140-6736(04)16357-5
Bohnsack, J. F., and Brown, E. J. (1986). The role of the spleen in resistance to infection. Annu. Rev. Med. 37, 49–59. doi: 10.1146/annurev.me.37.020186.000405
Booth, C., Inusa, B., and Obaro, S. K. (2010). Infection in sickle cell disease: a review. Int. J. Infect. Dis. 14, e2–e12. doi: 10.1016/j.ijid.2009.03.010
Braga, E. D., Aguiar-Alves, F., de Freitas Mde, F., de e Silva, M. O., Correa, T. V., Snyder, R. E., et al. (2014). High prevalence of Staphylococcus aureus and methicillin-resistant S. aureus colonization among healthy children attending public day care centers in informal settlements in a large urban center in Brazil. BMC Infect. Dis. 14:538. doi: 10.1186/1471-2334-14-538
Brandileone, M. C., Di Fabio, J. L., Vieira, V. S., Zanella, R. C., Casagrande, S. T., Pignatari, A. C., et al. (1998). Geographic distribution of penicillin resistance of Streptococcus pneumoniae in Brazil: genetic relatedness. Microb. Drug Resist. 4, 209–217. doi: 10.1089/mdr.1998.4.209
Cardozo, D. M., Nascimento-Carvalho, C. M., Souza, F. R., and Silva, N. M. (2006). Nasopharyngeal colonization and penicillin resistance among pneumococcal strains:a worldwide 2004 update. Braz. J. Infect. Dis. 10, 293–303. doi: 10.1590/S1413-86702006000400015
Clinical Laboratory Standards Institute (CLSI) (2012). Performance Standards for Antimicrobial Susceptibility Testing. Twenty-second Informational Supplement. CLSI document M100-S22. Wayne, PA: NCCLS.
Denno, D. M., Frimpong, E., Gregory, M., and Steele, R. W. (2002). Nasopharyngeal carriage and susceptibility patterns of Streptococcus pneumoniae in Kumasi, Ghana. West Afr. J. Med. 21, 233–236. doi: 10.4314/wajm.v21i3.28038
Ferreira, L. L., Carvalho, E. S., Berezin, E. N., and Brandileone, M. C. (2001). Nasopharyngeal colonization and antimicrobial resistance of Streptococcus pneumoniae isolated in children with acute rinofaringitis. J. Pediatr. 77, 227–234. doi: 10.1590/S0021-75572001000300014
Fonseca, P. B., Braga, J. A., Machado, A. M., Brandileone, M. C., and Farhat, C. K. (2005). Nasopharyngeal colonization by Streptococcus pneumoniae in children with sickle cell disease receiving prophylactic penicillin. J. Pediatr. 81, 149–154. doi: 10.2223/JPED.1321
Fridkin, S. K., Hageman, J. C., Morrison, M., Sanza, L. T., Como-Sabetti, K., Jernigan, J. A., et al. (2005). Methicillin-resistant Staphylococcus aureus disease in three communities. N. Engl. J. Med. 352, 1436–1444. doi: 10.1056/NEJMoa043252
Gardella, N., Murzicato, S., Di Gregorio, S., Cuirolo, A., Desse, J., Crudo, F., et al. (2011). Prevalence and characterization of methicillin-resistant Staphylococcus aureus among healthy children in a city of Argentina. Infect. Genet. Evol. 11, 1066–1071. doi: 10.1016/j.meegid.2011.03.019
Gonzalez, B. E., Hulten, K. G., Dishop, M. K., Lamberth, L. B., Hammerman, W. A., Mason, E. O. Jr., et al. (2005). Pulmonary manifestations in children with invasive community-acquired Staphylococcus aureus infection. Clin. Infect. Dis. 41, 583–590. doi: 10.1086/432475
Hausdorff, W. P., Bryant, J., Paradiso, P. R., and Siber, G. R. (2000). Which pneumococcal serougroups cause the most invasive disease: implications for conjugate vaccine formulation and use, part, I. Clin. Infect. Dis. 30, 100–121. doi: 10.1086/313608
Iughetti, L., Bigi, E., and Venturelli, D. (2016). Novel insights in the management of sickle cell disease in childhood. World J. Clin. Pediatr. 5, 25–34. doi: 10.5409/wjcp.v5.i1.25
Jurado, R. L. (1997). Iron, infections, and anemia of inflammation. Clin. Infect. Dis. 25, 888–895. doi: 10.1086/515549
Kuehnert, M. J., Kruszon-Moran, D., Hill, H. A., McQuillan, G., McAllister, S. K., Fosheim, G., et al. (2006). Prevalence of Staphylococcus aureus nasal colonization in the United States, 2001–2002. J. Infect. Dis. 93, 172–179. doi: 10.1086/499632
Lee, G. M., Huang, S. S., Rifas-Shiman, S. L., Hinrichsen, V. L., Pelton, S. I., Kleinman, K., et al. (2009). Epidemiology and risk factors for Staphylococcus aureus colonization in children in the post-PCV7 era. BMC Infect. Dis. 9:110. doi: 10.1186/1471-2334-9-110
Liñares, J., Ardanuy, C., Pallares, R., and Fenoll, A. (2010). Changes in antimicrobial resistance, serotypes and genotypes in Streptococcus pneumoniae over a 30-year period. Clin. Microbiol. Infect. 16, 402–410. doi: 10.1111/j.1469-0691.2010.03182.x
Mantese, O. C., Paula, A., Moraes, A. B., Moreira, T. A., Guerra, M. L., and Brandileone, M. C. (2003). Prevalence of serotypes and antimicrobial resistance of invasive strains of Streptococcus pneumoniae. J. Pediatr. 79, 537–542. doi: 10.2223/JPED.1115
Marchese, A., Esposito, S., Coppo, E., Rossi, G. A., Tozzi, A., Romano, M., et al. (2011). Detection of Streptococcus pneumoniae and identification of pneumococcal serotypes by real-time polymerase chain reaction using blood samples from Italian children ≤ 5 years of age with community-acquired pneumonia. Microb. Drug Resist. 17, 419–424. doi: 10.1089/mdr.2011.0031
McCavit, T. L., Quinn, C. T., Techasaensiri, C., and Rogers, Z. R. (2011). Increase in invasive Streptococcus pneumoniae infections in children with sickle cell disease since pneumococcal conjugate vaccine licensure. J. Pediatr. 158, 505–507. doi: 10.1016/j.jpeds.2010.11.025
Mitchell, T. J., and Mitchell, A. M. (2014). Pneumococcus adapts to the sickle cell host. Cell Host Microbe 15, 521–523. doi: 10.1016/j.chom.2014.04.013
Moran, G. J., Amii, R. N., Abrahamian, F. M., and Talan, D. A. (2005). Methicillin-resistant Staphylococcus aureus in community-acquired skin infections. Emerging Infect. Dis. 11, 928–930. doi: 10.3201/eid1106.040641
Norris, C. F., Mahannah, S. R., Smith-Whitley, K., Ohene-Frempong, K., and McGowan, K. L. (1996). Pneumococcal colonization in children with sickle cell disease. J. Pediatr. 129, 821–827. doi: 10.1016/S0022-3476(96)70025-2
Quinn, C. T., Rogers, Z. R., and Buchanan, G. R. (2004). Survival of children with sickle cell disease. Blood 103, 4023–4037. doi: 10.1182/blood-2003-11-3758
Rogers, J. T. (1996). Ferritin translation by interleukin-1and interleukin-6: the role of sequences upstream of the start codons of the heavy and light subunit genes. Blood 87, 2525–2537.
Seixas, M. O., Rocha, L. C., Carvalho, M. B., Menezes, J. F., Lyra, I. M., Nascimento, V. M., et al. (2010). Levels of high-density lipoprotein cholesterol (HDL-C) among children with steady-state sickle cell disease. Lipids Health Dis. 9:91. doi: 10.1186/1476-511X-9-91
Shak, J. R., Vidal, J. E., and Klugman, K. P. (2013). Influence of bacterial interactions on pneumococcal colonization of the nasopharynx. Trends Microbiol. 21, 129–135. doi: 10.1016/j.tim.2012.11.005
Sniadack, D. H., Schwartz, B., Lipman, H., Bogaerts, J., Butler, J. C., Dagan, R., et al. (1995). Potential interventions for the prevention of childhood pneumonia: geographic and temporal differences in serotype and serogroup distribution of sterile site pneumococcal isolates from children: implications for vaccine strategies. Pediatr. Infect. Dis. J. 14, 503–510. doi: 10.1097/00006454-199506000-00007
Steele, R. W., Warrier, R., Unkel, P. J., Foch, B. J., Howes, R. F., Shah, S., et al. (1996). Colonization with antibiotic-resistant Streptococcus pneumoniae in children with sickle cell disease. J. Pediatr. 128, 531–535. doi: 10.1016/S0022-3476(96)70365-7
Steinberg, M. H., and Rodgers, G. P. (2001). Pathophysiology of sickle cell disease: role of cellular and genetic modifiers. Semin. Hematol. 38, 299–306. doi: 10.1016/S0037-1963(01)90023-X
Williams, T. N., Uyoga, S., Macharia, A., Ndila, C., McAuley, C. F., Opi, D. H., et al. (2009). Bacteraemia in Keyan children with sickle-cell anaemia: a retrospective cohort and case-control study. Lancet 374, 1364–1370. doi: 10.1016/S0140-6736(09)61374-X
World Health Organization (2007). Pneumococcal conjugate vaccine for childhood immunization - WHO position paper. Wkly. Epidemiol. Rec. 82, 93–104. Available online at: http://www.who.int/wer/en/; http://www.who.int/wer/2007/wer8212.pdf
Keywords: nasopharyngeal, oropharyngeal, serotype, Staphylococcus aureus, Streptococcus pneumoniae
Citation: Rocha LC, Carvalho MOS, Nascimento VML, dos Santos MS, Barros TF, Adorno EV, Reis JN, da Guarda CC, Santiago RP and Gonçalves MdS (2017) Nasopharyngeal and Oropharyngeal Colonization by Staphylococcus aureus and Streptococcus pneumoniae and Prognostic Markers in Children with Sickle Cell Disease from the Northeast of Brazil. Front. Microbiol. 8:217. doi: 10.3389/fmicb.2017.00217
Received: 16 May 2016; Accepted: 31 January 2017;
Published: 15 February 2017.
Edited by:
Leonard Peruski, US Centers for Disease Control and Prevention, USAReviewed by:
Marquita Vernescia Gittens-St.Hilaire, University of the West Indies, BarbadosAvi Peretz, Poria Medical Center, Israel
Copyright © 2017 Rocha, Carvalho, Nascimento, dos Santos, Barros, Adorno, Reis, da Guarda, Santiago and Gonçalves. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marilda de Souza Gonçalves, bWFyaUBiYWhpYS5maW9jcnV6LmJy