 Antonio Rivero-Juarez1*†
Antonio Rivero-Juarez1*† Mario Frias1†
Mario Frias1† Pedro Lopez-Lopez1
Pedro Lopez-Lopez1 Juan Berenguer2
Juan Berenguer2 Federico García3Juan Macias4Begoña Alcaraz5Angeles Castro-Iglesias6
Federico García3Juan Macias4Begoña Alcaraz5Angeles Castro-Iglesias6 Javier Caballero-Gomez1,7
Javier Caballero-Gomez1,7 Antonio Rivero1 on behalf of CoRIS Cohort‡
Antonio Rivero1 on behalf of CoRIS Cohort‡- 1Instituto Maimonides de Investigación Biomédica de Córdoba, Hospital Universitario Reina Sofía de Córdoba, Universidad de Córdoba, Córdoba, Spain
- 2Hospital General Universitario Gregorio Marañón, Instituto de Investigación Sanitaria Gregorio Marañón, Madrid, Spain
- 3Hospital Universitario San Cecilio, Instituto de Investigación Biosantaria Ibs, Granada, Spain
- 4Hospital Nuestra Señora de Valme, Seville, Spain
- 5Hospital General Universitario Santa Lucía, Cartagena, Spain
- 6Complejo Hospitalario Universitario a Coruña, A Coruña, Spain
- 7University of Córdoba - Agrifood Excellence International Campus, Córdoba, Spain
Background: The objective of our study was to assess the prevalence and incidence of HEV in people living with HIV (PLWH) in a Spanish national cohort.
Methods: Retrospective longitudinal study including PLWH recruited in the cohort of adult HIV-infected patients of the AIDS Research Network in follow-up at 28 Spanish hospitals with available serum samples in 2014 and 2015. All samples were tested for HEV IgG, IgM, and RNA. Samples with detectable HEV viral loads were genotyped. Prevalence and incidence of HEV infection were calculated.
Results: The study sample comprised 845 PLWH. At baseline, 101 patients were positive for HEV IgG antibodies (11.9%), none had HEV IgM antibodies, and 2 presented detectable HEV RNA (0.23%). Forty-two seroconverted for IgG, supposing a cumulative incidence of 5.7%. One subject was positive for IgM (0.13%), and 2 showed detectable HEV RNA (0.27%). One case was infected by the emergent HEV genotype 3ra.
Conclusion: Our study identifies one case of HEV 3ra genotype infection, the main host of which is rabbit, showing a potential zoonotic role of this emerging genotype in Spain.
Introduction
Hepatitis E virus (HEV) is an emerging infectious disease worldwide. In Europe, the majority of cases are related to local infections, represented by HEV genotype 3 (Aspinall et al., 2017). Although HEV infection by this autochthonous genotype usually presents as subclinical or self-limiting acute hepatitis, there are several related complications that substantially worsen the prognosis of the infection (Faber et al., 2018). HEV genotype 3 has tropism for the peripheral and central nervous system, producing neurological injury, including serious manifestations such as Guillen-Barré syndrome (Dalton et al., 2017). On the other hand, immunosuppressed patients infected by HEV genotype 3 could develop chronic infection (Kamar et al., 2008). Cases of chronic HEV infection have been described in transplant recipients, leukemia patients treated with rituximab, patients on therapy with anti-tumoral necrosis factor drugs, and subjects infected by HIV with a low CD4 + cell count (Rivero-Juárez et al., 2020). Finally, in the context of underlying liver disease, HEV infection can trigger liver failure and may require liver transplantation (Frias et al., 2018). Consequently, there are subsets of patients in whom HEV could have a serious outcome. Among the population in which HEV infections may have a worse prognosis, persons living with HIV (PLWH) represent a high-sensitivity population because of the high rate of advanced liver fibrosis due to common hepatotropic virus coinfection and the underlying immunosuppression (Rivero-Juarez et al., 2019).
In Europe, the main HEV genotype is 3 (Abravanel et al., 2017; Oeser et al., 2019; Suin et al., 2019). Nevertheless, in recent years, an important number of new viral strains have emerged that encompass a growing caseload in countries such as Switzerland, France, Belgium and Spain (Abravanel et al., 2017; Caballero-Gómez et al., 2019; Oeser et al., 2019; Suin et al., 2019). The emergence of these new strains has an important clinical implication because the introduction of new viral strains could have a negative impact in terms of an increased number of symptomatic and worst prognosis cases (Oeser et al., 2019). In addition, recently, there has been awareness about the zoonotic behavior of several HEV viral strains, the main host of which are lagomorphs and rodents (Abravanel et al., 2017; Sridhar et al., 2018; Suin et al., 2019). These strains have been described in a high proportion of patients with chronic hepatitis, suggesting that those patients with underlying immunosuppression could be more suitable for infection by these emerging viruses (Sridhar et al., 2018; Sahli et al., 2019).
For these reasons, our study assessed the prevalence and incidence of HEV, as well as the prevalence of chronic HEV infection, in a large national cohort of PLWH, describing the HEV viral strains.
Materials and Methods
Study Population
The cohort of adult HIV-infected patients of the AIDS Research Network (CoRIS) is an open, prospective, multicentre cohort of adult subjects with confirmed HIV infection who are naïve to antiretroviral therapy (ART) at cohort entry and who are recruited to HIV care units of the Spanish Public Health System (Caro-Murillo et al., 2007), which constitutes the standard place of treatment for the great majority of persons in Spain. CoRIS was launched in 2004. Each center recruits into the cohort all subjects seen for the first time at the center who meet the following criteria: confirmed HIV diagnosis, and naïve to ART. Written informed consent is obtained from all patients. Demographic, clinical, laboratory, microbiological and treatment information is recorded. The cohort is linked to a centralized BioBank, where patients’ blood samples are processed and cryopreserved immediately after reception and then stored (García-Merino et al., 2009). Participating centers are encouraged to obtain an initial blood sample at entry in the cohort, preferentially before starting ART, and follow-up samples preferentially annually, or at least biannually thereafter. The BioBank has obtained the UNE-EN-ISO 9001:2008 Systems of Quality Management Requirements. For the proposed study, we included patients recruited in the cohort at follow-up in 28 hospitals belonging to 15 Spanish provinces with available serum samples in the centralized BioBank in 2014 (baseline) and 2015.
HEV Serological and Molecular Determination
First, all patients were tested for HEV IgG and IgM antibodies. Serum samples were tested for anti-HEV IgG and IgM (Wantai HEV-IgM ELISA®; Beijing Wantai Biological Pharmacy Enterprise© LTD, Beijing, China). ELISA tests were carried out in duplicate in accordance with the instructions provided by the manufacturer, using the automated ELISA Triturus System (Grifols S. A, Barcelona, Spain). The cut-off value for positive samples was > 1.1, following the manufacturer’s instructions. Patients who were positive for HEV anti-IgG antibody at baseline (prevalence) were not evaluated for IgG antibodies in the follow-up (incidence).
Second, all patients were tested for HEV RNA using RT-qPCR. RNA was extracted from 400 μL of serum pools of 4 patients using the commercial QIAamp MinElute Virus Spin Kit (QIAgen. Hilden, Germany) and an automated procedure (QIAcube. QIAgen, Hilden, Germany). The purified RNA was eluted in a total elution volume of 30 μL. As a positive extraction control, 50 μL of the reconstituted WHO Standard HEV strain (supplied by the Paul-Ehrlich-Institute [code 6329/10]) was diluted in 350 μL of Ambion® DEPC-treated water (Thermo Fisher Scientifics. Waltham, MA, United States). RT-qPCR was performed on all pooled samples using the CFX Connect (Bio-Rad, Hercules, California), using primer and probe designed and validated by our group and described recently (Caballero-Gómez et al., 2020). These primers and probes were obtained by aligning all whole-genome sequences of the Orthohepeviridae A species available in GenBank. The procedure was validated using the WHO international reference panel for HEV RNA genotypes for nucleic acid amplification technique (ıNAT)ı-based assays (including genotypes 1a, 1e, 3b, 3c, 3e, 3f, 3ra, 4c, 4g, and 2a) supplied by the Paul-Ehrlich-Institut (code 8578/13). For the reaction, the QIAgen One-Step PCR Kit (QIAgen, Hilden, Germany) was used using 25 μL of RNA template. An external (in-run) standard curve (using 18 dilutions) was used to calculate the HEV viral load using the WHO Standard HEV strain (code 6329/10) with a unitage of 250,000 International Units/mL. Positive pools were individually evaluated by the same RT-qPCR procedure. The sensitivity of PCR in individual samples was 21 IU/mL, and in 4 samples-pools it was set at 350 IU/mL.
Samples with detectable HEV viral loads were genotyped according to the protocol described by HEVnet. For phylogenetic analysis, nested RT-PCR was performed, targeting the ORF2 region (structural proteins), using primers HEV_5920S (5′-CAAGGHTGGCGYTCKGTTGAGAC-3′) and HEV_6425A (5′-CAAGGHTGGCGYTCKGTTGAGAC-3′) in the first round and HEV_5930S (5′-GYTCKGTTGAGACCWCBGGBGT-3′) and HEV_6334A (5′-TTMACWGTRGCTCGCCATTGGC-3′) in the second round. The second amplification product of 467 bp was sequenced using the BigDye Terminator Cycle Sequencing Ready Reaction Kit on an ABI PRISM 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA, United States). SnapGene software (Version 3.1; GSL Bio-tech, snapgene.com) was used for sequence analysis. The consensus sequence was obtained using SeqMan Software SeqMan NGen® Version 12.0 (DNASTAR. Madison, WI). Subtype assignment and phylogenetic analyses were performed using the HEVnet genotyping tool1 (Mulder et al., 2019), and confirmed by BLAST. Sequence alignments were generated by the MAFFT online service: multiple sequence alignment, interactive sequence choice and visualization. Phylogenetic trees were constructed using the maximum likelihood method using the proposed HEV genotype/subtype standard reference (Smith et al., 2016). Reference sequences of genotype 4 were included as an outgroup to root the tree. The final tree was obtained with MEGA Software (Version 6) using the bootstrap method (bootstrapped with 1000 replicates).
Statistical Analysis
Three outcome variables were established: (i) positivity for IgG antibodies against HEV, (ii) positivity for IgM antibodies against HEV, and (iii) detection of HEV RNA. These variables were evaluated at baseline. The prevalence of IgG, IgM, and HEV RNA was calculated. For those patients who were negative for all outcome variables, three outcome variables were evaluated at the end of the follow-up: (i) seroconversion for IgG antibodies against HEV, (ii) seroconversion for IgM antibodies against HEV, and (iii) detection of HEV RNA. The incidence rate of HEV was calculated. The accumulated incidence was expressed as a percentage. Continuous variables were expressed as the median and quartiles (Q1–Q3). Student’s t-test, the Welch test or the Mann-Whitney U-test was used to compare two independent variables, and a Kruskal-Wallis test, one-way ANOVA or Welch test was used to compare more than two independent variables. The most appropriate test was chosen based on a normal distribution (using the Shapiro-Wilk test) or equality of variances (using the Levene test). Categorical variables were expressed as the number of cases (percentage) compared using the χ2-test or Fisher’s exact test. Significance was determined as a two-tailed p-value of less than 0.05. Bivariate analysis comparing the prevalence and incidence rate between groups was carried out to identify variables related to the different outcome variables. All analyses were carried out using the SPSS statistical software package version 18.0 (IBM Corporation, Somers, NY, United States), GraphPad Prism version 7 (Mac OS X version; GraphPad Software; San Diego, California, United States) and Winpepi software version 11.36 (Brixton Health).
Ethics
This study was designed and performed according to the Helsinki Declaration. The local and national Clinical Trial and Ethical Committee approved the study protocol.
Results
Study Population and Baseline Characteristics
A total of 845 individuals were included in the study. Seven hundred and fifty-one (88.9%) were male and had a median age of 36.9 years (30.7–45.2 years). Regarding HIV-related variables, 616 (72.9%) were men who had sex with men (MSM), and 80 (9.4%) had prior AIDS-defining conditions, with a median CD4 + cell count of 574 cells/mL (413–787 cells/mL), and 410 (48.5%) with detectable HIV viral load. Because patients are included in the cohort if they are naïve to antiretroviral therapy, the population presents a high proportion of patients with a detectable viral load.
Prevalence and Incidence of HEV Infection
One hundred and one patients showed positivity of IgG against HEV (11.9%; 95% CI: 9.9–14.3%). There were no variables associated with IgG positivity in the univariate and multivariate analyses (Table 1). Among the previously described risk factors for HEV in HIV-infected patients, neither men who had sex with men (MSM) nor CD4 + cell counts were associated with a higher rate of HEV seroprevalence. Any of the patients included in the study were positive for IgM anti-HEV. Two patients showed detectable HEV viral load (0.23%; 95% CI: 0.0–0.9%). Both patients were male and were negative for both IgG and IgM antibodies.
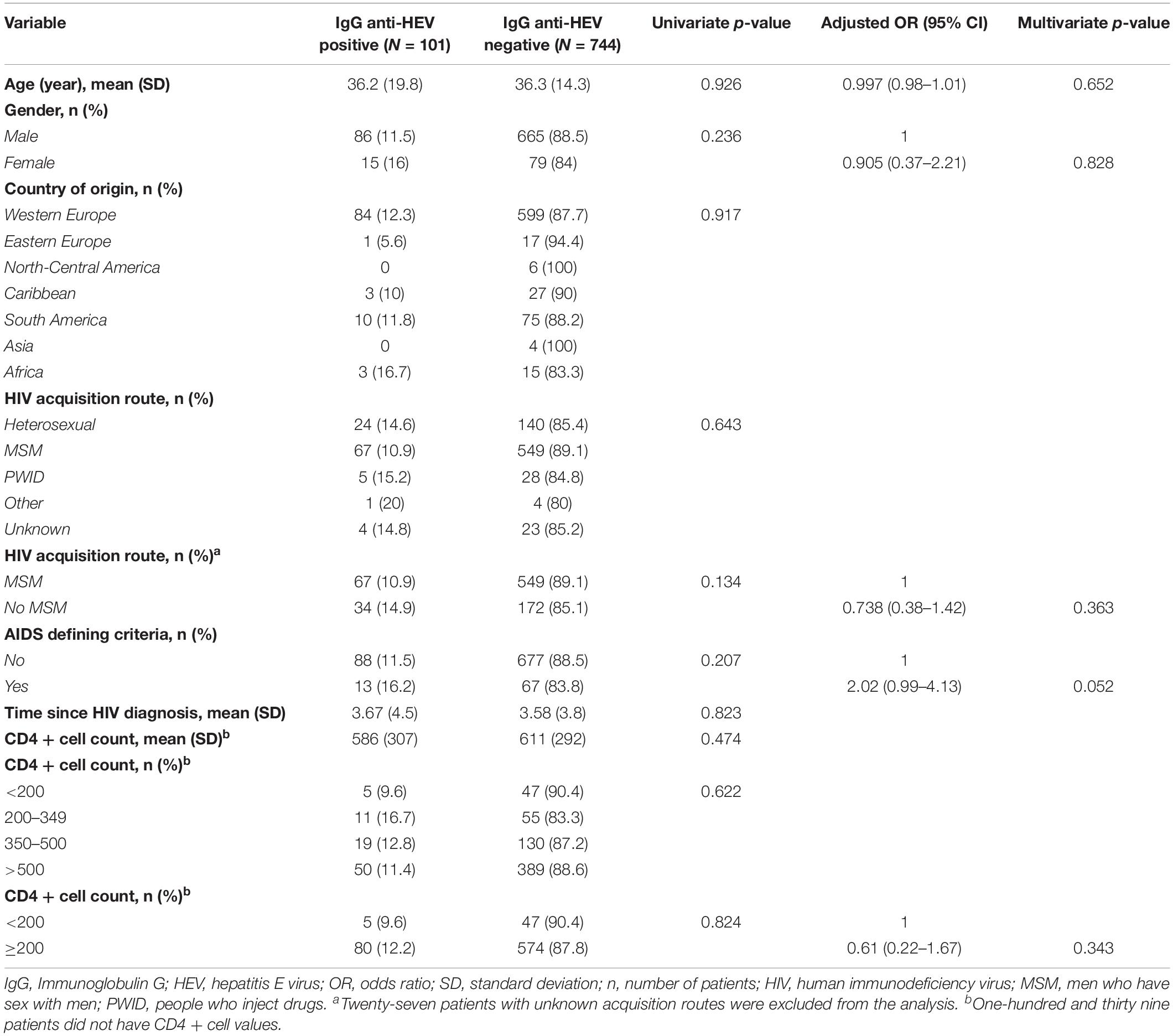
Table 1. Univariate and multivariate analysis for IgG anti-HEV at baseline.
Of the 744 patients negative for IgG antibodies at baseline, 733 (98.5%) had available serum samples in the follow-up. Forty-two patients showed seroconversion for IgG antibodies after 1 year of follow-up, supposing a cumulative incidence of 5.7% (95% CI: 4.3–7.7%). Similar to the prevalence analysis, by univariate and multivariate analysis, all factors were not associated with HEV seroconversion during the follow-up (Table 2). One patient showed both positive IgG and IgM antibodies but did not have detectable HEV RNA. HEV RNA was detected in two patients, but they were negative for IgG and IgM antibodies.
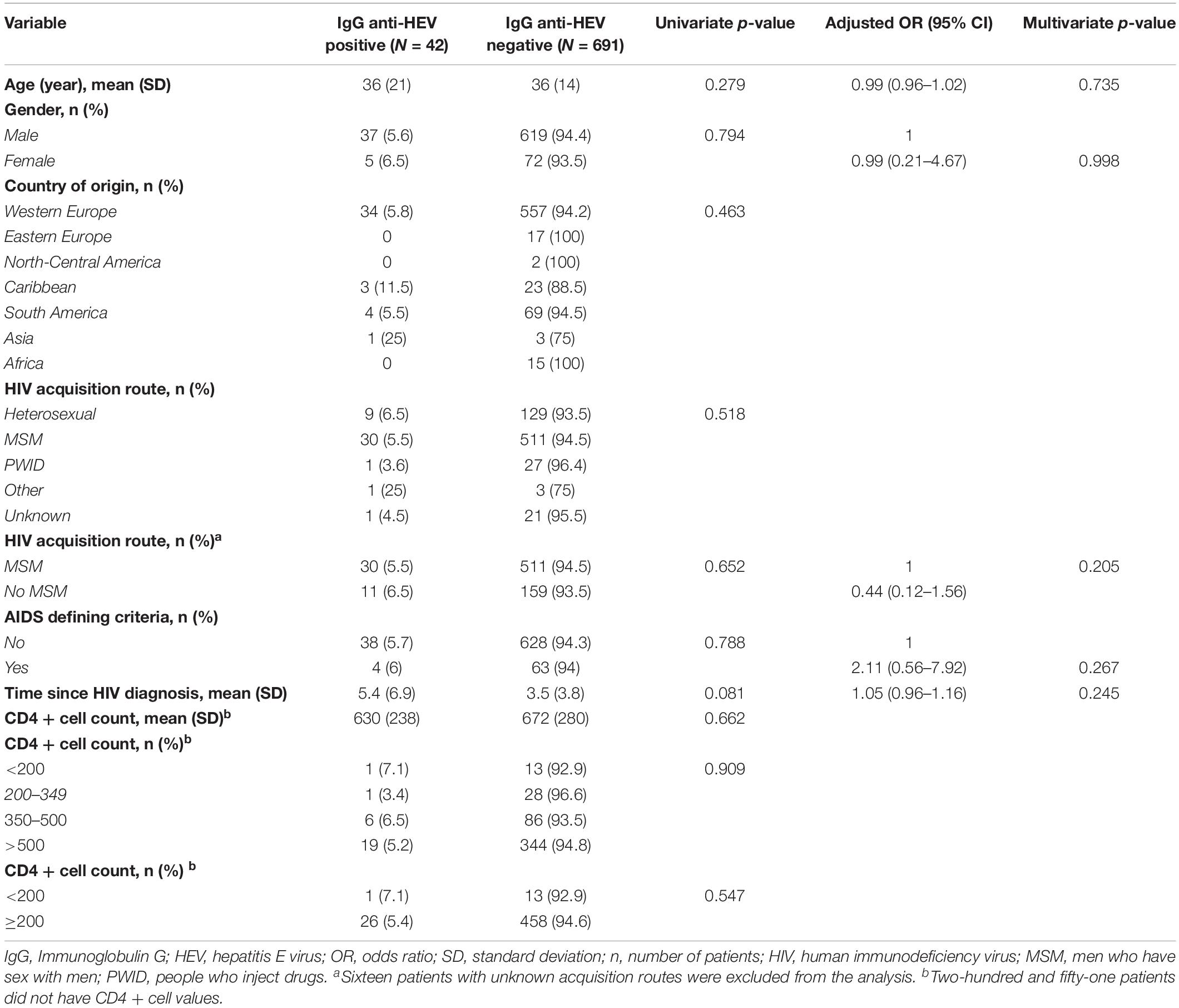
Table 2. Univariate and multivariate analysis for IgG anti-HEV seroconversion during follow-up.
Phylogenetic Analysis
Of the 4 patients with detectable viral load in the study, three were successfully genotyped. In two cases, viral strains were consistent with genotype 3f (Genbank accession numbers MN914126 and MN914127). Interestingly, in the other patient, the isolated viral strain was consistent with genotype 3ra (Genbank accession number MN537838) (Table 3). Phylogenetic analysis is shown in Figure 1. No patient had a detectable HEV viral load in the follow-up, indicating spontaneous viral clearance.

Table 3. Characteristics of patients with detectable HEV RNA.
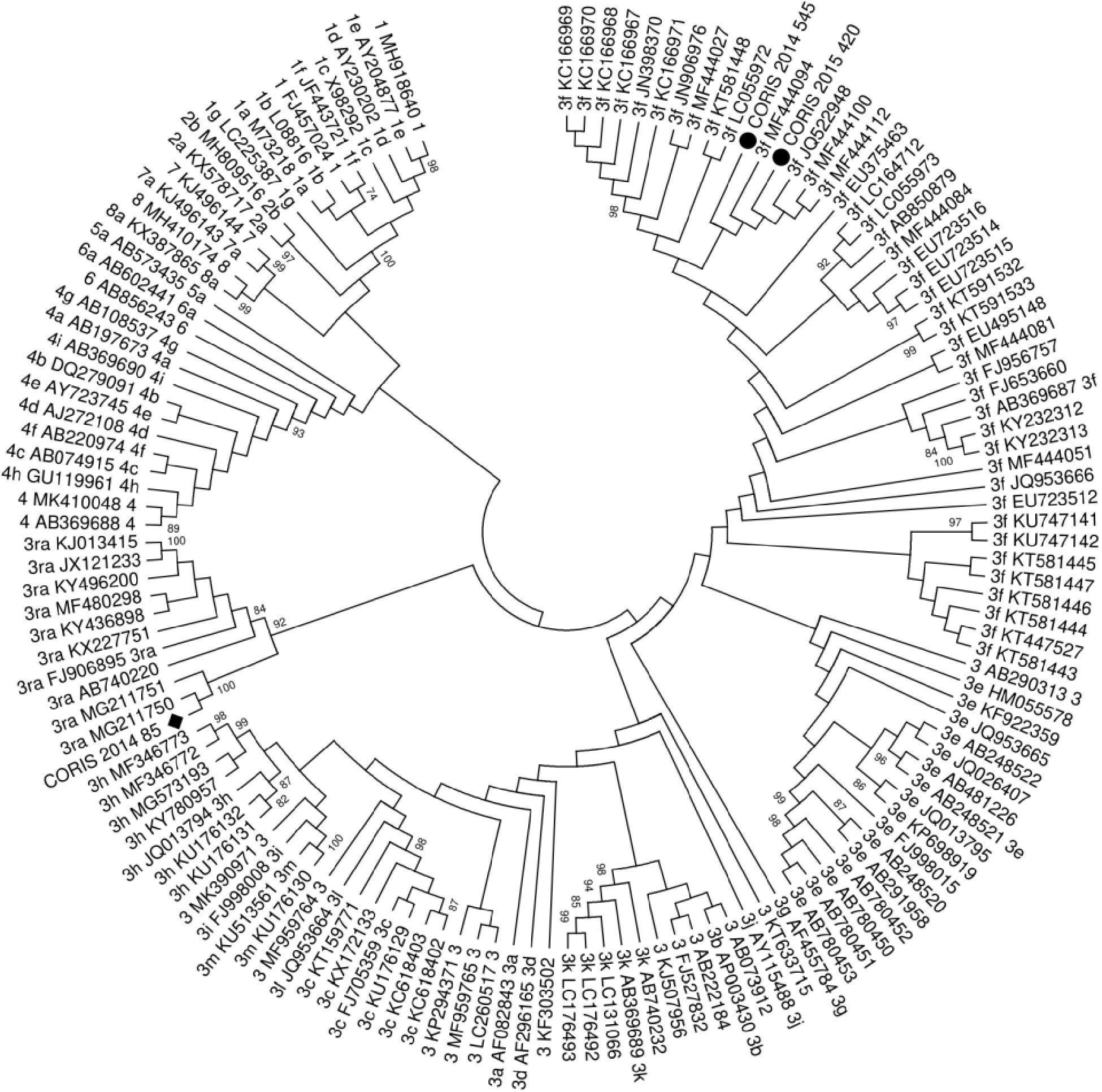
Figure 1. Molecular phylogenetic analysis by Maximum Likelihood method. The evolutionary history was inferred by using the Maximum likelihood method based on the Tamura-Nei model. The bootstrap consensus tree inferred from 1000 replicates is taken to represent the evolutionary history of the taxa analyzed. Branches corresponding to partitions reproduced in less than 50% bootstrap replicates are collapsed. Initial tree(s) for the heuristic search were obtained automatically by applying the Neighbor-Joining and BioNJ algorithms to a matrix of pairwise distances estimated using the Maximum Composite Likelihood (MCL) approach and then selecting the topology with superior log likelihood value. The analysis involved 120 nucleotide sequences. The codon positions included were 1st + 2nd + 3rd + Non-coding. All positions containing gaps and missing data were eliminated. Novel subtypes sequences proposed by HEVnet are referred in the tree as p.
Discussion
The prevalence of HEV among PLWH strongly depends on the country of origin and the immunoassays employed in the study. In this sense, in high endemic areas, such Africa or Asia, the reported seroprevalence is higher than 40%; in addition, in other regions, such as Europe, these data vary between 29 and 10% (World Health Organization [WHO], 2014). Our study found a Spanish seroprevalence of HEV infection of 11.9% and a cumulative incidence of 5.9% in 1 year. These results suggest widespread circulation of HEV among PLWH in Spain.
The main route of transmission of the HEV genotype 3 is the consumption of raw or undercooked meat, including game species and pork (Aspinall et al., 2017; Faber et al., 2018). In two large case series reported in France and Switzerland, the major subtype belonged to clade 3efg and the emerging subtype 3s, respectively (Abravanel et al., 2017; Sahli et al., 2019). In a large temporal series in Belgium, the majority of patients were infected by genotype 3f (Suin et al., 2019). Interestingly, these studies found several cases of HEV infection due to the viral genotype 3ra, whose main host are rabbits. Our study identified one case of HEV infection by genotype 3ra, confirming the zoonotic role of this genotype and the first description of a case of its type in Spain. It should be highlighted that the viral strain identified in our study shows a high similarity with two viral strains isolated in France (MG211750 and MG211751; Figure 1), suggesting the widespread of this strain in Europe. Remarkably, none of the cases found in France and Switzerland documented the consumption of rabbit meat or were in contact with them (Abravanel et al., 2017; Sahli et al., 2019). We cannot determine the source of infection because of the retrospective character of the analysis of the study. Further investigations are needed to evaluate other possible routes of infection of this genotype in addition to consumption or contact with rabbits. Remarkably, in these series, the rate of chronic infection among patients infected with genotype 3ra is higher than those observed in other subtypes. Presently, several cases of chronic HEV infection have been reported in PLWH (Rivero-Juarez et al., 2019). In our study, none of the patients with detectable HEV viral loads developed chronic infections, including those infected with emergence genotype 3ra. Therefore, chronic HEV infection seems to be a rare event in PLWH.
On the other hand, there are several variables related to HIV infection that could be associated with a higher risk for HEV infection in this population. In this sense, the association between the CD4 + cell count and the seroprevalence of HEV is controversial. There are studies that found no differences in the rate of HEV IgG antibodies and the CD4 + cell count (Pineda et al., 2014; Rivero-Juarez et al., 2015; Zeng et al., 2017). Other studies found that this variable could influence a higher or lower rate of infection (Kenfak-Foguena et al., 2011; Zhou et al., 2018). Our study did not find any association between the CD4 + cell count, using different cut-offs, and the presence of IgG antibody, either in the baseline or during the follow-up. In the same way, it is controversial whether MSM constituted a risk population for HEV infection. Studies conducted in Europe report a higher HEV seroprevalence in MSM than in non-MSM populations (Payne et al., 2013; Lanini et al., 2015). In our study, MSM showed a similar HEV seroprevalence and seroincidence to non-MSM. This finding is consistent with a recent study conducted in Asia, where MSM did not show a higher risk for HEV infection in comparison with non-MSMs (Lin et al., 2019), unlike other enteric viruses, such as hepatitis A.
Several limitations should be noted. First, despite the high number of hospitals involved in the present study, there is a lack of patients from different regions. Therefore, our study lacks the power to identify differences in prevalence between regions. Finally, due to the anonymous character of the samples, additional patient data (such epidemiological variables related to risk for HEV acquisition) cannot be evaluated.
Conclusion
In conclusion, our study found that HEV infection in PLWH from Spain is frequent, showing a relatively high annual incidence. Despite the number of acute infections identified in our study, none of the cases involved chronic infection. We identified one case of infection by the HEV genotype 3ra, the main host of which is the rabbit, confirming the zoonotic role of this emerging genotype.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation to, any qualified researcher.
Ethics Statement
The studies involving human participants were reviewed and approved by the Comité de Ética de la Investigación de Córdoba. Portal de Ética de la Investigación Biomédica de Andalucia. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AR-J and AR: concept and design. JB, FG, JM, BA, AC-I, and AR: collection of samples. MF, PL-L, and JC-G: EIA analysis. MF, PL-L, JC-G, and AR-J: RNA extraction and HEV-PCR. PL-L and AR-J: sequencing and phylogenetic analysis. AR-J, AR, and MF: draft the manuscript. All authors: critical revision of the manuscript. Funding: AR-J, AR, and MF.
Funding
The RIS cohort (CoRIS) was supported by the Instituto de Salud Carlos III through the Red Temática de Investigación Cooperativa en Sida (RD16/0025/0017; RD16/0025/0034; RD16/0025/0040) as part of the Plan Nacional I + D + i and cofinanced by ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER). This work was supported by the Ministerio de Sanidad (RD12/0017/0012) integrated in the Plan Nacional de I + D + I and cofinanced by the ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER), Fundación para la Investigación en Salud (FIS) del Instituto Carlos III (PI16/01297), and Fundación Progreso y Salud de la Junta de Andalucía (PIN-0477-2017). AR-J was awarded with the I Premio de Jóvenes Investigadores de GeSIDA, which benefits were used to fund the present work. AR-J was the recipient of a Miguel Servet Research Contract by the Ministerio de Ciencia, Promoción y Universidades of Spain (CP18/00111). MF is the recipient of a Sara Borrell contract by the Ministerio de Ciencia, Promoción y Universidades of Spain (CD18/00091). JC-G was supported by an FPU grant from the Spanish Ministry of Education, Culture and Sport (FPU17/01319). The funders did not play any role in the design, conclusions or interpretation of the study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to Ismael Zafra and Laura Ruiz for their technical support.
Funding: A Rivero-Juarez, A Rivero and Mario Frias.
Centers and investigators involved in CoRIS
Executive committee: Santiago Moreno, Inma Jarrín, David Dalmau, Maria Luisa Navarro, Maria Isabel González, Jose Luis Blanco, Federico Garcia, Rafael Rubio, Jose Antonio Iribarren, Félix Gutiérrez, Francesc Vidal, Juan Berenguer, Juan González.
Fieldwork, data management and analysis: Belén Alejos, Victoria Hernando, Cristina Moreno, Carlos Iniesta, Luis Miguel Garcia Sousa, Nieves Sanz Perez.
BioBanK HIV: Hospital General Universitario Gregorio Marañón: M Ángeles Muñoz-Fernández, Isabel María García-Merino, Irene Consuegra Fernández, Coral Gómez Rico, Jorge Gallego de la Fuente, Paula Palau Concejo.
Participating centres
Hospital General Universitario de Alicante (Alicante): Joaquín Portilla, Esperanza Merino, Sergio Reus, Vicente Boix, Livia Giner, Carmen Gadea, Irene Portilla, María Pampliega, Marcos Díez, Juan Carlos Rodríguez, José Sánchez-Payá.
Hospital Universitario de Canarias (San Cristobal de la Laguna): Juan Luis Gómez, Jehovana Hernández, María Remedios Alemán, María del Mar Alonso, María Inmaculada Hernández, Felicitas Díaz-Flores, Dácil García, Ricardo Pelazas., Ana López Lirola.
Hospital Universitario Central de Asturias (Oviedo): José Sanz Moreno, Alberto Arranz Caso, Cristina Hernández Gutiérrez, María Novella Mena.
Hospital Universitario 12 de Octubre (Madrid): Rafael Rubio, Federico Pulido, Otilia Bisbal, Asunción Hernando, Lourdes Domínguez, David Rial Crestelo, Laura Bermejo, Mireia Santacreu.
Hospital Universitario de Donostia (Donostia-San Sebastián): José Antonio Iribarren, Julio Arrizabalaga, María José Aramburu, Xabier Camino, Francisco Rodríguez-Arrondo, Miguel Ángel von Wichmann, Lidia Pascual Tomé, Miguel Ángel Goenaga, Ma Jesús Bustinduy, Harkaitz Azkune, Maialen Ibarguren, Aitziber Lizardi, Xabier Kortajarena.
Hospital General Universitario De Elche (Elche): Félix Gutiérrez, Mar Masiá, Sergio Padilla, Andrés Navarro, Fernando Montolio, Catalina Robledano, Joan Gregori Colomé, Araceli Adsuar, Rafael Pascual, Marta Fernández, Elena García., José Alberto García, Xavier Barber.
Hospital Universitari Germans Trias i Pujol (Can Ruti) (Badalona): Roberto Muga, Arantza Sanvisens, Daniel Fuster.
Hospital General Universitario Gregorio Marañón (Madrid): Juan Berenguer, Juan Carlos López Bernaldo de Quirós, Isabel Gutiérrez, Margarita Ramírez, Belén Padilla, Paloma Gijón, Teresa Aldamiz-Echevarría, Francisco Tejerina, Francisco José Parras, Pascual Balsalobre, Cristina Diez, Leire Pérez Latorre.
Hospital Universitari de Tarragona Joan XXIII (Tarragona): Francesc Vidal, Joaquín Peraire, Consuelo Viladés, Sergio Veloso, Montserrat Vargas, Miguel López-Dupla, Montserrat Olona, Anna Rull, Esther Rodríguez-Gallego, Verónica Alba.
Hospital Universitario y Politécnico de La Fe (Valencia): Marta Montero Alonso, José López Aldeguer, Marino Blanes Juliá, María Tasias Pitarch, Iván Castro Hernández, Eva Calabuig Muñoz, Sandra Cuéllar Tovar, Miguel Salavert Lletí, Juan Fernández Navarro.
Hospital Universitario La Paz/IdiPAZ: Juan González-garcia, Francisco Arnalich, José Ramón Arribas, Jose Ignacio Bernardino de la Serna, Juan Miguel Castro, Luis Escosa, Pedro Herranz, Victor Hontañón, Silvia García-Bujalance, Milagros García López-Hortelano, Alicia González-Baeza, Maria Luz Martín-Carbonero, Mario Mayoral, Maria Jose Mellado, Rafael Esteban Micán, Rocio Montejano, María Luisa Montes, Victoria Moreno, Ignacio Pérez-Valero, Berta Rodés, Talia Sainz, Elena Sendagorta, Natalia Stella Alcáriz, Eulalia Valencia.
Hospital San Pedro Centro de Investigación Biomédica de La Rioja (CIBIR) (Logroño): José Ramón Blanco, José Antonio Oteo, Valvanera Ibarra, Luis Metola, Mercedes Sanz, Laura Pérez-Martínez.
Hospital Universitario Miguel Servet (Zaragoza): Piedad Arazo, Gloria Sampériz.
Hospital Universitari MutuaTerrassa (Terrasa): David Dalmau, Angels Jaén, Montse Sanmartí, Mireia Cairó, Javier Martinez-Lacasa, Pablo Velli, Roser Font, Mariona Xercavins, Noemí Alonso.
Complejo Hospitalario de Navarra (Pamplona): María Rivero, Jesús Repáraz, María Gracia Ruiz de Alda, María Teresa de León Cano, Beatriz Pierola Ruiz de Galarreta.
Corporació Sanitària Parc Taulí (Sabadell): Ferrán Segura, María José Amengual, Gemma Navarro, Montserrat Sala, Manuel Cervantes, Valentín Pineda, Sonia Calzado, Marta Navarro.
Hospital Universitario de La Princesa (Madrid): Ignacio de los Santos, Jesús Sanz Sanz, Ana Salas Aparicio, Cristina Sarriá Cepeda, Lucio Garcia-Fraile Fraile, Enrique Martín Gayo.
Hospital Universitario Ramón y Cajal (Madrid): Santiago Moreno, José Luis Casado, Fernando Dronda, Ana Moreno, María Jesús Pérez Elías, Cristina Gómez Ayerbe, Carolina Gutiérrez, Nadia Madrid, Santos del Campo Terrón, Paloma Martí, Uxua Ansa, Sergio Serrano, María Jesús Vivancos.
Hospital General Universitario Reina Sofía (Murcia): Enrique Bernal, Alfredo Cano, Antonia Alcaraz García, Joaquín Bravo Urbieta, Ángeles Muñoz, Maria Jose Alcaraz, Maria del Carmen Villalba.
Hospital Nuevo San Cecilio (Granada): Federico García, José Hernández, Alejandro Peña, Leopoldo Muñoz, Paz Casas, Marta Alvarez, Natalia Chueca, David Vinuesa, Clara Martinez-Montes.
Centro Sanitario Sandoval (Madrid): Jorge Del Romero, Carmen Rodríguez, Teresa Puerta, Juan Carlos Carrió, Mar Vera, Juan Ballesteros, Oskar Ayerdi.
Hospital Clínico Universitario de Santiago (Santiago de Compostela): Antonio Antela, Elena Losada.
Hospital Universitario Son Espases (Palma de Mallorca): Melchor Riera, María Peñaranda, María Leyes, Ma Angels Ribas, Antoni A Campins, Carmen Vidal, Francisco Fanjul, Javier Murillas, Francisco Homar.
Hospital Universitario Virgen de la Victoria (Málaga): Jesús Santos, Crisitina Gómez Ayerbe, Isabel Viciana, Rosario Palacios, Carmen María González.
Hospital Universitario Virgen del Rocío (Sevilla): Pompeyo Viciana, Nuria Espinosa, Luis Fernando López-Cortés.
Hospital Universitario de Bellvitge (Hospitalet de Llobregat): Daniel Podzamczer, Elena Ferrer, Arkaitz Imaz, Juan Tiraboschi, Ana Silva, María Saumoy.
Hospital Universitario Valle de Hebrón (Barcelona): Esteban Ribera, Adrian Curran.
Hospital Costa del Sol (Marbella): Julián Olalla, Alfonso del Arco, Javier de la torre, José Luis Prada, José María García de Lomas Guerrero, Javier Pérez Stachowski.
Hospital General Universitario Santa Lucía (Cartagena): Onofre Juan Martínez, Francisco Jesús Vera, Lorena Martínez, Josefina García, Begoña Alcaraz, Amaya Jimeno.
Complejo Hospitalario Universitario a Coruña (Chuac) (A Coruña): Angeles Castro Iglesias, Berta Pernas Souto, Alvaro Mena de Cea.
Hospital Universitario Basurto (Bilbao): Josefa Muñoz, Miren Zuriñe Zubero, Josu Mirena Baraia-Etxaburu, Sofía Ibarra Ugarte, Oscar Luis Ferrero Beneitez, Josefina López de Munain, Ma Mar Cámara López, Mireia de la Peña, Miriam Lopez.
Hospital Universitario Virgen de la Arrixaca (El Palmar): Carlos Galera, Helena Albendin, Aurora Pérez, Asunción Iborra, Antonio Moreno, Maria Angustias Merlos, Asunción Vidal.
Hospital de la Marina Baixa (La Vila Joiosa): Concha Amador, Francisco Pasquau, Javier Ena, Concha Benito, Vicenta Fenoll., Concepcion Gil Anguita, Jose Tomas Algado Rabasa.
Hospital Universitario Infanta Sofia (San Sebastian de los Reyes): Inés Suárez-García, Eduardo Malmierca, Patricia González-Ruano, Dolores Martín Rodrigo, Ma Pilar Ruiz Seco.
Complejo Hospitalario de Jaén (Jaén): Mohamed Omar Mohamed-Balghata, María Amparo Gómez Vidal.
Hospital San Agustín (Avilés): Miguel Alberto de Zarraga.
Hospital Clínico San Carlos (Madrid): Vicente Estrada Pérez, Maria Jesus Téllez Molina, Jorge Vergas García, Juncal Pérez-Somarriba Moreno.
Hospital Universitario Fundación Jiménez Díaz (Madrid): Miguel Górgolas., Alfonso Cabello., Beatriz Álvarez., Laura Prieto.
Hospital Universitario Príncipe de Asturias (Alcalá de Henares): José Sanz Moreno, Alberto Arranz Caso, Cristina Hernández Gutiérrez, María Novella Mena.
Hospital Clínico Universitario de Valencia (València): María José Galindo Puerto, Ramón Fernando Vilalta, Ana Ferrer Ribera.
Hospital Reina Sofía (Córdoba): Antonio Rivero Román, Maria Teresa Brieva Herrero, Antonio Rivero Juárez, Pedro López López, Isabel Machuca Sánchez, Mario Frías Casas, José Peña Martínez.
Hospital Universitario Severo Ochoa (Leganés): Miguel Cervero Jiménez, Rafael Torres Perea, Juan José Jusdado Ruiz-Capillas.
Nuestra Señora de Valme: Juan A Pineda, Juan Macías Sánchez, Nicolás Merchante Gutiérrez, Pilar Rincón.
Footnotes
References
Abravanel, F., Lhomme, S., El Costa, H., Schvartz, B., Peron, J. M., Kamar, N., et al. (2017). Rabbit Hepatitis E virus infections in humans. Fran. Emerg. Infect. Dis 23, 1191–1193. doi: 10.3201/eid2307.170318
Aspinall, E. J., Couturier, E., Faber, M., Said, B., Ijaz, S., Tavoschi, L., et al. (2017). Hepatitis E virus infection in Europe: surveillance and descriptive epidemiology of confirmed cases, 2005 to 2015. Euro. Surveill. 22:30561.
Caballero-Gómez, J., García Bocanegra, I., Gómez-Guillamón, F., Camacho-Sillero, L., Zorrilla, I., Lopez-Lopez, P., et al. (2020). Absence of Hepatitis E virus circulation in wild rabbits (Oryctolagus cuniculus) and Iberian hares (Lepus granatensis) in Mediterranean ecosystems in Spain. Transbound. Emerg. Dis. 67, 1422–1427. doi: 10.1111/tbed.13478
Caballero-Gómez, J., Jiménez-Ruiz, S., Lopez-Lopez, P., Vicente, J., Risalde, M. A., Cano-Terriza, D., et al. (2019). Emergent subtype of hepatitis E virus genotype 3 in wild boar in Spain. Transbound. Emerg. Dis. 66, 1803–1808. doi: 10.1111/tbed.13251
Caro-Murillo, A. M., Castilla, J., Pérez-Hoyos, S., Miró, J. M., Podzamczer, D., Rubio, R., et al. (2007). Cohorte RIS de pacientes con infección por VIH sin tratamiento antirretroviral previo (CoRIS): metodología y primeros resultados [Spanish cohort of naïve HIV-infected patients (CoRIS): rationale, organization and initial results]. Enferm. Infecc. Microbiol. Clin. 25, 23–31. doi: 10.1157/13096749
Dalton, H. R., van Eijk, J., Cintas, P., Madden, R. G., Jones, C., Webb, G. W., et al. (2017). Hepatitis E virus infection and acute non-traumatic neurological injury: a prospective multicentre study. J. Hepatol. 67, 925–932. doi: 10.1016/j.jhep.2017.07.010
Faber, M., Askar, M., and Stark, K. (2018). Case-control study on risk factors for acute hepatitis E in Germany, 2012 to 2014. Euro. Surveill. 23:e100469.
Frias, M., López-López, P., Rivero, A., and Rivero-Juarez, A. (2018). Role of Hepatitis E Virus Infection in Acute-on-Chronic Liver Failure. Biomed. Res. Intern. 2018:9098535.
García-Merino, I., de Las Cuevas, N., Jiménez, J. L., Gallego, J., Gómez, C., Prieto, C., et al. (2009). The Spanish HIV BioBank: a model of cooperative HIV research. Retrovirology 6:27. doi: 10.1186/1742-4690-6-27
Kamar, N., Selves, J., Mansuy, J. M., Ouezzani, L., Péron, J. M., Guitard, J., et al. (2008). Hepatitis E virus and chronic hepatitis in organ-transplant recipients. N. Engl. J. Med. 358, 811–817.
Kenfak-Foguena, A., Schöni-Affolter, F., Bürgisser, P., Witteck, A., Darling, K. E., Kovari, H., et al. (2011). Hepatitis E Virus seroprevalence and chronic infections in patients with HIV, Switzerland. Emerg. Infect. Dis. 17, 1074–1078. doi: 10.3201/eid/1706.101067
Lanini, S., Garbuglia, A. R., Lapa, D., Puro, V., Navarra, A., Pergola, C., et al. (2015). Epidemiology of HEV in the Mediterranean basin: 10-year prevalence in Italy. BMJ Open 5:e007110. doi: 10.1136/bmjopen-2014-007110
Lin, K. Y., Lin, P. H., Sun, H. Y., Chen, Y. T., Su, L. H., Su, Y. C., et al. (2019). Hepatitis E virus infections among human immunodeficiency virus-positive individuals during an outbreak of acute hepatitis a in Taiwan. Hepatology 70, 1892–1902. doi: 10.1002/hep.30771
Mulder, A. C., Kroneman, A., Franz, E., Vennema, H., Tulen, A. D., Takkinen, J., et al. (2019). HEVnet: a One Health, collaborative, interdisciplinary network and sequence data repository for enhanced hepatitis E virus molecular typing, characterisation and epidemiological investigations. Euro. Surveill. 24:1800407.
Oeser, C., Vaughan, A., Said, B., Ijaz, S., Tedder, R., Haywood, B., et al. (2019). Epidemiology of Hepatitis E in England and Wales: a 10-Year retrospective surveillance study, 2008-2017. J. Infect. Dis. 220, 802–810. doi: 10.1093/infdis/jiz207
Payne, B. A., Medhi, M., Ijaz, S., Valappil, M., Savage, E. J., Gill, O. N., et al. (2013). Hepatitis E virus seroprevalence among men who have sex with men, United Kingdom. Emerg. Infect. Dis. 19, 333–335. doi: 10.3201/eid1902.121174
Pineda, J. A., Cifuentes, C., Parra, M., Merchante, N., Pérez-Navarro, E., Rivero-Juárez, A., et al. (2014). Incidence and natural history of hepatitis E virus coinfection among HIV-infected patients. AIDS 28, 1931–1937. doi: 10.1097/qad.0000000000000378
Rivero-Juárez, A., Aguilera, A., Avellón, A., García-Deltoro, M., García, F., Gortazar, C., et al. (2020). Executive summary: consensus document of the diagnosis, management and prevention of infection with the hepatitis E virus: study Group for Viral Hepatitis (GEHEP) of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC). Enferm. Infecc. Microbiol. Clin. 38, 28–32. doi: 10.1016/j.eimc.2018.06.014
Rivero-Juarez, A., Lopez-Lopez, P., Frias, M., and Rivero, A. (2019). Hepatitis E infection in HIV-infected patients. Front. Microbiol. 10:1425. doi: 10.3389/fmicb.2019.01425
Rivero-Juarez, A., Martinez-Dueñas, L., Martinez-Peinado, A., Camacho, A., Cifuentes, C., Gordon, A., et al. (2015). High hepatitis E virus seroprevalence with absence of chronic infection in HIV-infected patients. J. Infect. 70, 624–630. doi: 10.1016/j.jinf.2014.10.016
Sahli, R., Fraga, M., Semela, D., Moradpour, D., and Gouttenoire, J. (2019). Rabbit HEV in immunosuppressed patients with hepatitis E acquired in Switzerland. J. Hepatol. 70, 1023–1025. doi: 10.1016/j.jhep.2019.01.025
Smith, D. B., Simmonds, P., Izopet, J., Oliveira-Filho, E. F., Ulrich, R. G., Johne, R., et al. (2016). Proposed reference sequences for hepatitis E virus subtypes. J. Gen. Virol. 97, 537–542. doi: 10.1099/jgv.0.000393
Sridhar, S., Yip, C., Wu, S., Cai, J., Zhang, A. J., Leung, K. H., et al. (2018). Rat Hepatitis E Virus as cause of persistent hepatitis after liver transplant. Emerg. Infect. Dis. 24, 2241–2250. doi: 10.3201/eid2412.180937
Suin, V., Klamer, S. E., Hutse, V., Wautier, M., Jacques, M., Abady, M., et al. (2019). Epidemiology and genotype 3 subtype dynamics of hepatitis E virus in Belgium, 2010 to 2017. Eur. Commun. Dis. Bull. 24:1800141.
World Health Organization [WHO] (2014). The Global Prevalence of Hepatitis E Virus Infection and Susceptibility: A Systematic Review. Geneva: World Health Organization.
Zeng, H., Wang, L., Liu, P., Liao, L., Wang, L., and Shao, Y. (2017). Seroprevalence of hepatitis E virus in HIV-infected patients in China. AIDS 31, 2019–2021. doi: 10.1097/qad.0000000000001585
Keywords: hepatitis E, HIV, survey, genotype 3ra, seroprevalence
Citation: Rivero-Juarez A, Frias M, Lopez-Lopez P, Berenguer J, García F, Macias J, Alcaraz B, Castro-Iglesias A, Caballero-Gomez J and Rivero A (2020) Hepatitis E 3ra Genotype Infection in People Living With HIV in Spain. Front. Microbiol. 11:564486. doi: 10.3389/fmicb.2020.564486
Received: 21 May 2020; Accepted: 18 August 2020;
Published: 11 September 2020.
Edited by:
Anna Kramvis, University of the Witwatersrand, South AfricaReviewed by:
Maria Guadalupe Vizoso Pinto, Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET), ArgentinaAnna Rosa Garbuglia, Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani (IRCCS), Italy
Florence Abravanel, Centre Hospitalier Universitaire de Toulouse, France
Copyright © 2020 Rivero-Juarez, Frias, Lopez-Lopez, Berenguer, García, Macias, Alcaraz, Castro-Iglesias, Caballero-Gomez and Rivero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Rivero-Juarez, YXJqdmV0QGdtYWlsLmNvbQ==; cml2ZXJvQGltaWJpYy5vcmc=
†These authors have contributed equally to this work
‡The complete membership of the CoRIS cohort can be found in the Acknowledgments