 Angela Lumba-Brown
Angela Lumba-Brown Kian Niknam
Kian Niknam Jordan Cornwell
Jordan Cornwell Courtney Meyer
Courtney Meyer Jamshid Ghajar4
Jamshid Ghajar4- 1Department of Emergency Medicine, Stanford University, Palo Alto, CA, United States
- 2University of California, San Francisco Medical School, San Francisco, CA, United States
- 3Athletic Training, Department of Sports Medicine, Stanford University, Palo Alto, CA, United States
- 4Department of Neurosurgery, Brain Performance Center, Stanford University, Palo Alto, CA, United States
Background: There is heterogeneity in neurosensory alterations following mild traumatic brain injury. Commonly assessed neurosensory symptoms following head injury include symptom reports and measures of oculomotor impairment, auditory changes, and vestibular impairment.
Hypothesis/Purpose: Neurosensory alterations are prevalent acutely following mild traumatic brain injury secondary to blunt head trauma during collegiate varsity sports and may vary by sex and sport.
Study Design: Retrospective study of a large collegiate athletic database.
Methods: Analyses were performed using an established single University dataset of 177 male and female collegiate varsity athletes who were diagnosed with concussion/mild traumatic brain injury between September 2013 and October 2019. Descriptive and comparative analyses were performed on individual and grouped acute concussion assessments pertaining to neurosensory alterations obtained within 72 h of injury using components of the Sports Concussion Assessment Tool Version 5 and Vestibular/Ocular-Motor Screening.
Results: Females had significantly more abnormal smooth pursuit (p-value: 0.045), convergence (p-value: 0.031), and visual motion sensitivity tests results (p-value: 0.023) than males. There were no differences in neurosensory alterations when grouped by overall auditory, vestibular, or oculomotor impairments. The majority of sports-related concussions occurred during football (50, 28.25%), wrestling (21, 11.86%), water polo (15, 8.47%), and basketball (14, 7.91%). Abnormal vestibular assessments were high in these top four sports categories, but statistically significant differences in overall auditory, vestibular, or oculomotor impairments were not reached by individual sport. However, water polo players had higher abnormal individual assessments related to balance reports on the sideline (60.00%, p-value: 0.045) and in the clinic setting (57.14%, p-value: 0.038) as compared to all other sports.
Conclusion: While neurosensory alterations are prevalent in both male and female athletes acutely post-concussion, females have a higher incidence of abnormalities in smooth pursuit, convergence, and visual motion sensitivity and may benefit from early rehabilitation.
Introduction
Neurosensory alterations following blunt head trauma can be debilitating because sensory input informs how we interact with the world. Heterogeneity in neurosensory alterations following mild traumatic brain injury (TBI), including concussion, may be related to premorbid conditions, medications, injury-related factors, and other modifying factors such as co-existing injuries or intoxication (1, 2). Some neurosensory-related symptoms are assessed in common post-concussion symptom scales and measures of vestibulo-oculomotor impairment following mild TBI in children and adults (3–5).
Neurosensory alterations are examined to various degrees in a variety of concussion assessments employed acutely, throughout recovery, and in the long-term setting. For example, the assessment of symptom burden and symptom provocation following vestibulo-oculomotor assessment has been reported in pediatric athletes in the acute setting (5, 6). Visual processing impairments are identifiable in adults following childhood concussion, upon long-term assessment (7). Though outcomes of tests used for concussion assessment have been reported at varying time-points following injury, there is limited data reporting thematically-grouped neurosensory alterations using subjective and objective measures following acute blunt head injury resulting in sports-related concussion in men and women.
Understanding the comparative prevalence of neurosensory alterations in physically fit individuals in the acute setting is particularly important to inform the range of acute impairments that may be seen in soldiers injured in austere environments, where traditional concussion assessment may not be feasible. We hypothesized that neurosensory alterations are acutely prevalent in physically fit, varsity collegiate athletes following on-field, blunt head injury resulting in sports-related concussion and that these symptoms and impairments would be higher in sports with more frequent person-to-person blunt impacts such as football and wrestling. This study presents the immediate, on-scene reports of neurosensory symptoms in varsity collegiate athletes, as well as reports from the initial concussion clinic visit within 72-h of injury.
Methods
This study was a retrospective review of an existing sports concussion database of collegiate varsity athletes sustaining concussion at a single university. All athletes are evaluated by a concussion specialist (a neurosurgeon or sports-medicine physician) and diagnosed with concussion in accordance with the 5th Consensus Statement on Concussion in Sport recommendations upon their first clinic visit within 72-h of injury (8). Athletes completed post-concussion symptom assessments on the sideline, immediately following injury, as well as at the first concussion clinic visit. Clinic assessments included the complete Sports Concussion Assessment Tool Version 5 (SCAT5), Vestibular/Ocular-Motor Screening (VOMS), and eye-tracking utilizing virtual reality goggles. Athletes sustaining concussion from 2013 to 2019 were included in this analysis.
Measures
The SCAT5 is a concussion assessment tool that includes a post-concussive symptom evaluation, memory and cognitive screen, Glasgow Coma Scale score, and balance assessment (9). The symptom evaluation employs a rating scale of 22 symptoms with severity ratings from 0 (no symptom) to 6 (maximum symptom). Balance is assessed at the clinic visit using the Balance Error Scoring System (BESS) and on the sideline using the modified BESS.
The Vestibular Ocular Motor Screening (VOMS) measures symptom provocation while testing the ability of a patient to complete a set of balance, vision, and movement-integrated tasks (10). In our cohort, this assessment was completed by physical therapists in the initial concussion clinic visit. Patients were prompted to rate their symptom levels on a scale from 0 to 10 before testing began and following each task. The 4 patient-reported symptoms queried are “headache,” “dizziness,” “nausea,” and “fogginess.” Our cohort performed 7 tests related to the VOMS: smooth pursuit, horizontal and vertical saccades, convergence, horizontal and vertical VOR, and visual motion sensitivity.
Our institution's internal review board approved the population of this research database (IRB-47124) and de-identified data analysis was adjudicated as exempt.
Dichotomization and Statistical Analysis
Continuous scores from the SCAT5 and individual tests comprising the VOMS were dichotomized into two groups: normal and abnormal. Modified BESS and sideline symptoms were taken from the SCAT5, whereas clinic BESS, clinic symptoms, and VOMS were taken from the physical therapy screening performed within 72 h of injury at the initial concussion clinic visit with the diagnosing neurosurgeon or sports medicine physician. Sideline modified BESS and clinic BESS scores of ≥5 and ≥15, respectively, were designated as abnormal (11). The presence of a symptom, of any severity, at sideline or clinic was labeled as abnormal. For each VOMS assessment, any single symptom with a severity ≥2 or a near point convergence of ≥5 cm was marked as abnormal (10).
A novel categorization system was used to dichotomize the BESS, VOMS, and reported symptoms as normal or abnormal based on auditory, vestibular, or oculomotor impairments. Abnormal vestibular assessments included any abnormal scoring on components of the VOMS, BESS, or symptoms of “dizziness” and/or “balance problems.” Abnormal oculomotor assessments included abnormal scoring on components of the VOMS or symptoms including “vision changes,” “light sensitivity,” or “blurred vision.” Abnormal auditory reports were designated as the presence of “noise sensitivity” or “ringing in ears.”
Descriptive statistics were calculated for the subjects' demographics and scores on concussion assessments. Dichotomized variables were analyzed using chi squared or Fisher's exact test, as appropriate. Logistic regression was used to assess effect size, and Levene's test was used to asses equalities in variance between males and females with regards to outcomes. Analyses were run using Stata 14/SE for Windows (StataCorp, LP College Station, TX).
Results
We identified 177 varsity collegiate athletes diagnosed with sports-related concussion/mild TBI following blunt head injury from 2013 to 2019. Within this population, 103 (58.19%) were male, and 74 (41.81%) were female, as reported in Table 1. The subjects participated in a variety of sports, with the majority of sports-related concussion occurring from football (50, 28.25%), wrestling (21, 11.86%), water polo (15, 8.47%), and basketball (14, 7.91%).
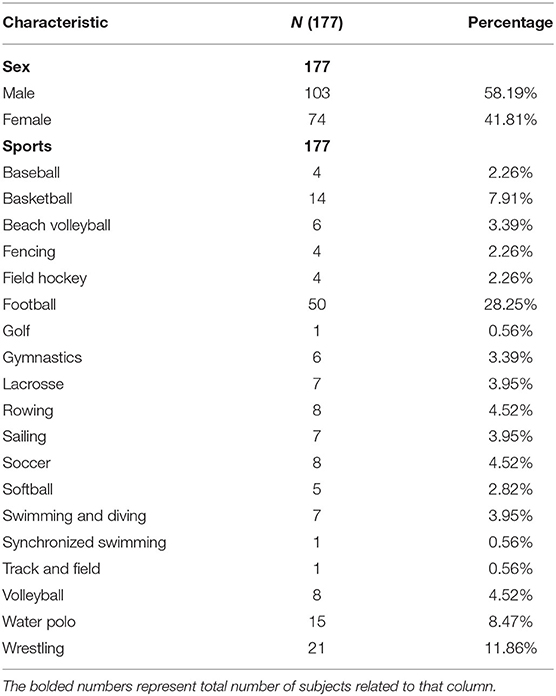
Table 1. Demographics and subject characteristics.
Sex-based differences in specific portions of the VOMS were identified. Females had consistently more abnormal VOMS measurements with statistical significance being reached for smooth pursuit (p-value: 0.045), convergence (p-value: 0.031), and visual motion sensitivity tests (p-value: 0.023), as depicted in Table 2. Though males consistently had higher rates of light sensitivity and females had higher rates of noise sensitivity, these differences were not statistically significant, as reported in Tables 2, 3. No significant differences were found in grouped vestibular, oculomotor, or auditory assessments between males and females, described in Table 4.
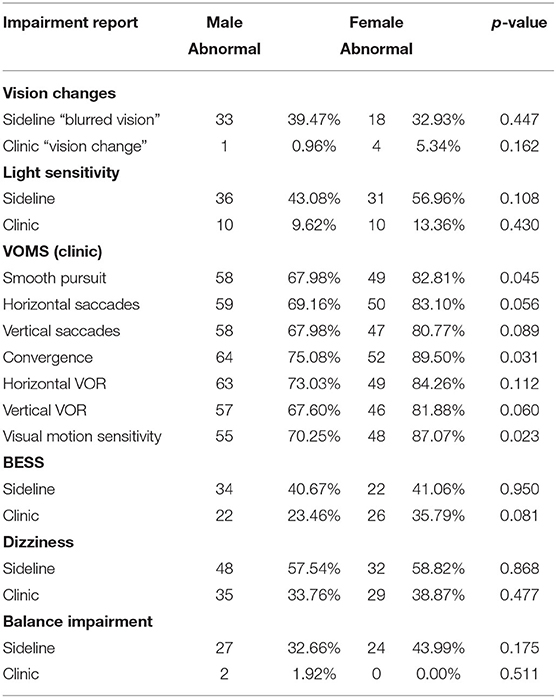
Table 2. Vestibular and oculomotor impairment report by sex.
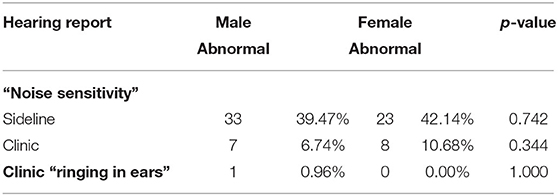
Table 3. Auditory impairment report by sex.
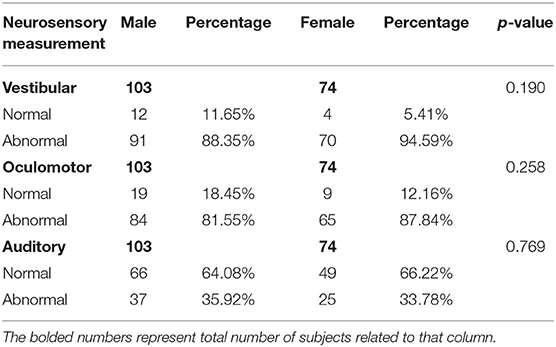
Table 4. Neurosensory reports by sex.
Logistic regression was used to assess neurosensory alteration differences by sex. Male athletes had 0.43 times the odds of vestibular impairment (95%CI: 0.13–1.40, p-value: 0.163) and 0.61 times the odds of oculomotor impairment (95%CI: 0.26–1.44, p-value: 0.261) relative to females. However, males had 1.10 times the odds of having hearing issues following a blunt head injury relative to females (95%CI: 0.59–2.06, p-value: 0.769).
Levene's test was used to assess for variance equality between groups and their outcomes. We found no significant differences in variances between sex and vestibular (p-value: 0.155), oculomotor (p-value: 0.261), and hearing (p-value: 0.770) impairments.
When comparing overall and grouped assessments of vestibular, oculomotor, or auditory impairments, football players had higher rates of abnormal assessments, however, statistical significance was not reached, as reported in Table 5. Among the sports with the highest internal concussion rates (football, wrestling, basketball, and water polo), water polo players had significantly higher rates of abnormal BESS assessments (57.14%, p-value: 0.038) and reports of balance problems (60.00%, p-value: 0.045), in the clinic and sideline settings, respectively, as reported in Table 6. Abnormal VOMS and other oculomotor assessments were common in the top four sports, but statistically significant differences were not reached. Overall, abnormal vestibular and oculomotor assessments were more common than reports of abnormal auditory symptoms.
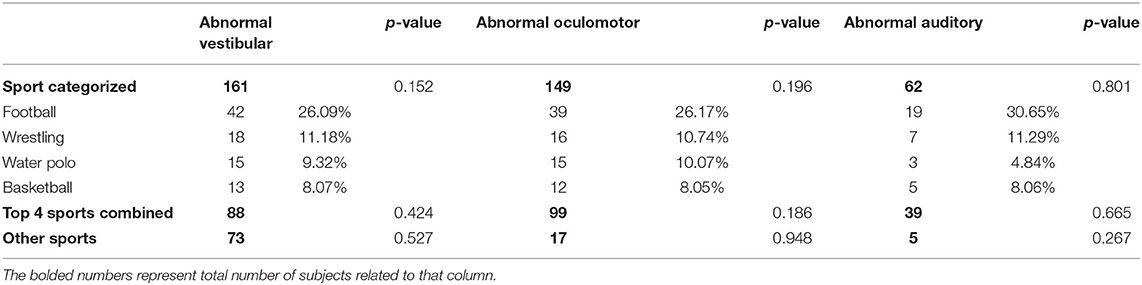
Table 5. Neurosensory alterations by sport.
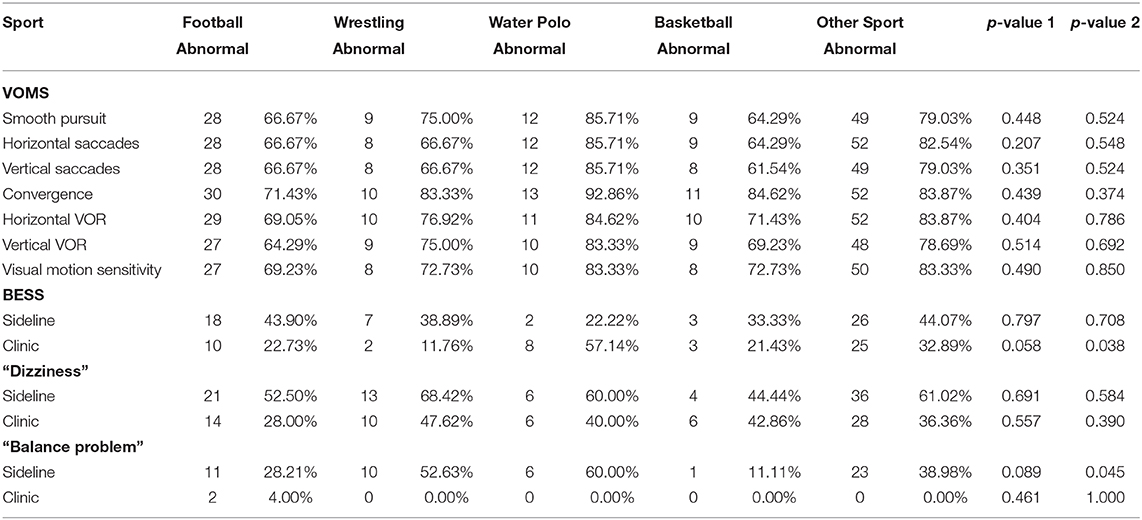
Table 6. Vestibular impairment reports by sport.
Discussion
This study demonstrated that females have higher rates of abnormal outcomes on specific measures of the VOMS (smooth pursuit, convergence, and visual motion sensitivity tests) as compared to males, which has been reported previously (12). The pathophysiology of this finding has yet to be determined. Females appear to be more susceptible to certain neurosensory alterations related to oculomotor control and motion perception, representing a potential injury vulnerability. Clinical assessment in the acute post-injury period is warranted to allow for the potential benefit of early rehabilitation. There is no difference in the grouped neurosensory alterations by sex, underscoring the importance of considering all outcomes derived from larger concussion assessment batteries.
The vast majority of concussions included in this dataset were sustained by subjects while playing football, wrestling, water polo, and basketball, which is consistent with previous reports of concussion incidence in sport. These sports also had the highest incidence of repeat concussions, though statistical significance when grouped by neurosensory alterations was not reached. This study reported greater neurosensory alterations in football, wrestling, water polo, and basketball compared to other sports present in our dataset including baseball, beach volleyball, fencing, field hockey, golf, gymnastics, lacrosse, sailing, softball, swimming and diving, synchronized swimming, track and field, rowing, soccer, and volleyball. Statistically significant differences in grouped auditory, vestibular, or oculomotor impairments were not reached by individual sport suggesting that mechanisms of injury in relation to a specific sport may not affect neurosensory alteration patterns. When examining individual outcomes by sport, water polo players had relatively more abnormal balance reports than other sports. Differences in balance assessments and training have been queried in previous literature, including comparing land to water-sports, but the significance is unclear (13, 14).
The strengths of this research are that 100% of subjects had complete reports of pre-defined neurosensory alterations pertaining to groupings of oculomotor, vestibular, and auditory symptoms and impairments at sideline and initial concussion clinic assessment. Much data has been reported on neurosensory alterations in sub-acute and chronic settings, especially pertaining to children (3–5, 7); however, this work represents the first study to report and compare grouped neurosensory outcomes in the immediate-acute time frame in highly physically fit collegiate athletes, by sex and sport. It also supports recent work identifying sex-based differences in vestibular-oculomotor assessments.
This study was limited by a small number of subjects populating individual “other sports” which included: baseball, beach volleyball, fencing, field hockey, golf, gymnastics, lacrosse, sailing, softball, swimming and diving, synchronized swimming, track and field, rowing, soccer, and volleyball. Identifying specific differences in neurosensory alterations in association with these sports requires a larger sample size pertaining to these sports. This study was also limited by the examination of inherently subjective and semi-objective measures, such as balance assessments and symptom scale reports, which may not sufficiently reflect the scope of symptomatology or impairment (14–16). Objective evaluation of neurosensory alterations, such as pin-prick testing, hearing examinations, and Snellen's chart for vision testing, were not obtained in this sample, limiting further interpretation of more objective impairments.
Concussion causes immediate neurosensory alterations, most commonly represented by vestibular and oculomotor symptoms and impairments, followed by auditory symptoms. While concussion recovery is traditionally defined by the resolution of post-concussive symptoms, bridging the gap between symptomatology and objective measures is critical to understanding the pathophysiology of injury and its recovery (16). Future research should aim to elucidate the pathophysiology of sex-based differences in order to address more personalized care including injury prevention strategies.
As our study demonstrated, important impairments may be determined from specific tests within larger, commonly used concussion assessments. In order to advance the field and allow for continued scientific hypotheses, the outcomes of specific tests within common concussion assessments should be analyzed for secondary outcomes, such as sex-based differences. Additionally, further research is needed to understand how targeted treatments may address these complaints early on, improving symptoms and quality of life in the acute setting, as well as shortening recovery trajectories in both females and males. Finally, research identifying neurosensory alterations contributing to common concussion subtypes, considering the presence or absence of cervical strain as an associated condition, will further inform overlap between physiologic systems and direct targeted treatments (1, 2).
Data Availability Statement
The data analyzed in this study was subject to the following licenses/restrictions: the dataset has not been approved by Stanford University for dissemination. Requests to access these datasets should be directed to ZmFsZW5lQHN0YW5mb3JkLmVkdQ==.
Ethics Statement
The studies involving human participants were reviewed and approved by Stanford University Internal Review Board. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
AL-B, JC, and JG designed and conducted the study. AL-B, CM, and KN authored the manuscript. All authors contributed to major edits and revisions, and agree to be accountable for the content of the work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Lumba-Brown A, Teramoto M, Bloom OJ, Brody D, Chesnutt J, Clugston JR, et al. Concussion guidelines step 2: evidence for subtype classification. Neurosurgery. (2019) 86:2–13. doi: 10.1093/neuros/nyz332
2. Maruta J, Lumba-Brown A, Ghajar J. Concussion subtype identification with the rivermead post-concussion symptoms questionnaire. Front Neurol. (2018) 9:1034. doi: 10.3389/fneur.2018.01034
3. Tommerdahl M, Dennis RG, Francisco EM, Holden JK, Nguyen R, Favorov OV. Neurosensory assessments of concussion. Mil Med. (2016) 181(Suppl. 5):45–50. doi: 10.7205/MILMED-D-15-00172
4. Hoffer ME. Mild traumatic brain injury: neurosensory effects. Curr Opin Neurol. (2015) 28:74–7. doi: 10.1097/WCO.0000000000000164
5. Mayer AR, Wertz CJ, Robertson-Benta CR, Reddy SP, Stephenson DD, Dodd AB, et al. Neurosensory screening and symptom provocation in pediatric mild traumatic brain injury. J Head Trauma Rehabilit. (2020) 35:270–8. doi: 10.1097/HTR.0000000000000560
6. Sherry NS, Fazio-Sumrok V, Sufrinko A, Collins MW, Kontos AP. Multimodal assessment of sport-related concussion. Clin J Sport Med. (2019). doi: 10.1097/JSM.0000000000000740. [Epub ahead of print].
7. Moore RD, Broglio SP, Hillman CH. Sport-related concussion and sensory function in young adults. J Athl Train. (2014) 49:36–41. doi: 10.4085/1062-6050-49.1.02
8. McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, et al. Consensus statement on concussion in sport—the 5 th International Conference on Concussion in Sport Held in Berlin, October 2016. Br J Sports Med. (2017) 51:838–47. doi: 10.1136/bjsports-2017-097699
9. Sport concussion assessment tool - 5th edition. Br J Sports Med. (2017) 51:851–8. doi: 10.1136/bjsports-2017-097506SCAT5
10. Mucha A, Collins MW, Elbin R, Furman JM, Troutman-Enseki C, DeWolf RM, et al. A brief vestibular/ocular motor screening (VOMS) assessment to evaluate concussions. Am J Sports Med. (2014) 42:2479–86. doi: 10.1177/0363546514543775
11. Iverson GL, Koehle MS. Normative data for the balance error scoring system in adults. Rehabilit. Res. Pract. (2013) 2013:846418. doi: 10.1155/2013/846418
12. Kontos AP, Sufrinko A, Elbin RJ, Puskar A, Collins MW. Reliability and associated risk factors for performance on the vestibular/ocular motor screening (VOMS) tool in healthy collegiate athletes. Am J Sports Med. (2016) 44:1400–6. doi: 10.1177/0363546516632754
13. Roth AE, Miller MG, Ricard M, Ritenour D, Chapman BL. Comparisons of static and dynamic balance following training in aquatic and land environments. J. Sport Rehabilit. (2006) 15:299–311. doi: 10.1123/jsr.15.4.299
14. Johnston W, Coughlan GF, Caulfield B. Challenging concussed athletes: the future of balance assessment in concussion. QJM Int J Med. (2017) 110:779–83. doi: 10.1093/qjmed/hcw228
15. Lumba-Brown A, Ghajar J, Cornwell J, Bloom OJ, Chesnutt J, Clugston JR, et al. Representation of concussion subtypes in common postconcussion symptom-rating scales. Concussion. (2019) 4:CNC65. doi: 10.2217/cnc-2019-0005
Keywords: concussion, mild traumatic brain injuries, vestibular, oculomotor, subtypes, neurosensory alterations, sports related concussion
Citation: Lumba-Brown A, Niknam K, Cornwell J, Meyer C and Ghajar J (2020) Sex-Related Differences in Neurosensory Alterations Following Blunt Head Injury. Front. Neurol. 11:1051. doi: 10.3389/fneur.2020.01051
Received: 21 April 2020; Accepted: 11 August 2020;
Published: 15 September 2020.
Edited by:
Catherine Tenn, Defence Research and Development Canada (DRDC), CanadaReviewed by:
Andres M. Rubiano, El Bosque University, ColombiaLauren E. Sergio, York University, Canada
Copyright © 2020 Lumba-Brown, Niknam, Cornwell, Meyer and Ghajar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Angela Lumba-Brown, YWx1bWJhQHN0YW5mb3JkLmVkdQ==