 Nathália Villa dos Santos1,2*
Nathália Villa dos Santos1,2* Victor Yuji Yariwake1
Victor Yuji Yariwake1 Karina do Valle Marques3
Karina do Valle Marques3 Mariana Matera Veras1
Mariana Matera Veras1 Laís Fajersztajn1
Laís Fajersztajn1- 1Laboratório de Poluição Ambiental, Departamento de Patologia, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
- 2Departamento de Saude Ambiental, Faculdade de Saude Publica, Universidade de São Paulo, São Paulo, Brazil
- 3Departamento de Cirurgia, Universidade Federal de Uberlandia, Uberlândia, Brazil
The risk of dementia and Alzheimer's disease in Latin America and the Caribbean (LAC) rises with increasing age and polluted air. Currently, at least 172 million people breathe unhealthy levels of air pollution in LAC countries. Several cohort studies have indicated that air pollution increases the risk of developing dementia and neurodegenerative diseases, but the mechanisms underlying the association are still not clear. Air pollution causes and aggravates five established risk factors for dementia (obesity, hypertension, stroke, diabetes mellitus, and heart diseases) and is linked to three other risk factors (physical inactivity, cognitive inactivity, and depression). Some of these risk factors could be mediating the association between air pollution and dementia. Reducing the risks for dementia is crucial and urgently needed in LAC countries. There is room for improving air quality in many urban areas in the LAC region and other low- and middle-income countries (LMICs), a routealready explored by many urban areas in developing regions. Moreover, reducing air pollution has proved to improve health outcomes before. In this article, we propose that despite the ongoing and valid scientific discussion, if air pollution can or cannot directly affect the brain and cause or aggravate dementia, we are ready to consider air pollution as a potentially modifiable risk factor for dementia in LAC and possibly in other LMICs. We suggest that controlling and reducing current air pollution levels in LAC and other LMIC regions now could strongly contribute.
Introduction
Despite the ongoing and valid scientific discussion about whether air pollution can or cannot directly affect the brain, and cause or aggravate dementia, in this article, we propose that we are ready to consider air pollution as a modifiable risk factor for dementia in Latin America and the Caribbean (LAC), and in other low- and middle-income countries (LMICs). We argue that controlling and lowering current air pollution levels in these regions could strongly contribute to reducing the high burden of dementia cases that has been projected for these countries. We base our argument on the following findings: 1) air pollution causes and/or aggravates at least five of the established risk factors for dementia (i.e., obesity, hypertension, stroke, diabetes mellitus, and heart diseases), 2) reducing air pollution has been proven to lower some of these risks, and 3) there is room for improving air quality in many urban LAC areas and other LMICs, a path already explored in many urban developing regions. First, we will introduce the topic and our hypothesis. In the following subsections, we will discuss how air pollution causes obesity, hypertension, stroke, diabetes mellitus, and heart diseases, and how these conditions can lead to dementia. We will also discuss the potential relations between air pollution and three other risk factors for dementia, for which evidence is less robust (physical inactivity, cognitive inactivity, and depression). Finally, we will discuss the evidence supporting the idea that air pollution can directly cause dementia. In the discussion, we will address why controlling air pollution should be used as a risk reduction strategy to tackle the burden of dementia in the LAC region and LMICs.
Air Pollution as a Modifiable Risk Factor for Dementia in Latin America and the Caribbean
Dementia
Dementia is an expensive disease with no cure to date, and its estimated global cost has already exceeded 1 trillion dollars. This is an extraordinarily high number for LMICs, a region that will concentrate 68% of the dementia cases by 2050 (1).
The burden of dementia in LAC countries is high and will continue to rise. By 2050, the region will have more than 17 million dementia cases, a 4-fold increase in 35 years (1). The average world increase for the same period will be three times lower (1). Other reports have described how rapid demographic changes, a higher prevalence of risk factors for dementia in the population, and other specific issues have made dementia prominent in the LAC region (2–4). Risk reduction is a crucial public health response to dementia (5), one that is urgently needed in the LAC countries. Our message is that air pollution could figure among the risk reduction strategies in LAC.
Air Pollution
Air pollution is a complex mixture of particles and gases in the air. Its composition varies depending on the emission source and prevailing weather conditions (6). Fine particulate matter [PM with an aerodynamic diameter of ≤ 2.5 μm (PM2.5)] is frequently presented as an indicator of exposure to air pollution in health studies (7, 8), including studies on the effects of air pollution on dementia (9–14). Rather than a single pollutant, PM2.5 reflects different sources of air pollution in the atmosphere. Because of the tiny particle size, PM2.5 can penetrate the lung barrier and enter the blood system. No matter its composition, PM is considered carcinogenic (15). The most frequent gas used to indicate exposure to air pollution in studies investigating the effects of air pollution on dementia is nitrogen dioxide (NO2), a marker of vehicle exhaust (11–14, 16). Some specific heavy metals, such as lead and cadmium, can trigger neurodegenerative processes and dementia (17). Widely used in industrial and agricultural activities, heavy metals are present in the soil and water and can affect the air, too. Once in the air, they become a major occupational health concern and a threat to the surrounding population. It is crucial to identify the sources of heavy metal air pollution and prevent hazard exposures.
Air pollution is ubiquitous and unevenly distributed (18–20), but it can be reduced. From a global perspective, pollution levels are higher in LMICs (20), the ones that will concentrate approximately 80% of dementia cases in the coming years (1). This makes tackling air pollution a relevant strategy to promote equity in brain health. The unequal distribution of air pollution is also true at smaller scales. Within the same city, those living closer to high traffic roads breathe worse air quality than those living further away. The same goes for those of lower socioeconomic status (21–23).
In 2015, air pollution caused 7.6% of the total global deaths and 4.2% of the total global disability-adjusted life-years (DALYs), a measure of loss in quality of life (7). This estimation was based on the risk for selective cardiovascular (CVD) and respiratory diseases, with no cognitive impairment burden included. It is reasonable to assume that a great part of this burden could be reduced just by lowering levels of air pollution. Indeed, some studies have used natural experiments to show that not only does bad air quality impair health, but also good air quality improves it (24–27). In other words, reducing air pollution can reduce global premature mortality and enhance the quality of life.
Air Pollution in Latin America and the Caribbean
Air pollution in LAC countries does not receive much attention on the global stage (19, 20). This is probably because, when compared with Africa, Asia, and the Middle East, air pollution in this region is not very high (18). However, between 1990 and 2013, particulate pollution increased in parts of the LAC territory (18). If one considers the current knowledge on pollution control and the performance of high-income countries, the decreases in the air pollution levels in LAC countries have been modest. From a public health perspective, the slight reduction in pollution in some regions of LAC has been offset by population growth (7). Although levels of fine particulate matter were decreasing since 2010 in some of the larger LAC cities, such as São Paulo and Bogotá, the current trends point towards an increase (28). At least 172 million people breathe unhealthy levels of air pollution in the LAC region, according to a recent estimation including 100,000 urban residents (29). The total number of LAC residents breathing bad air is higher if we include the rural residents, and remember that the LAC population is nearly 65 times larger than the population used in this estimate. Some rural LAC areas are highly polluted (18) because of wildfires (intentional or not) (30, 31), preharvest sugar cane burning (32, 33), and the more frequent use of wood for cooking and heating (34). At least 172 million LAC residents could reduce their risk for several diseases if air quality improved.
Hypothesis
Reducing the risk of dementia in LAC countries is urgent. The World Health Organization (WHO) strongly recommends that countries take national actions to lower well-established risk factors for dementia at the individual and population levels (5). These risk factors include obesity, hypertension, stroke, diabetes mellitus, heart disease, physical inactivity, poor diet, alcohol abuse, tobacco use, cognitive inactivity, depression, and isolation (5, 35–37). At least five of these risks can be caused or aggravated by breathing bad air quality. This means that controlling air pollution through policies and regulations could help reduce the burden of dementia. This is particularly relevant in LAC countries, where cases will increase, and pollution control is not typically stringent. Large urban areas of the most populated LAC territories, such as São Paulo and Mexico City, present poor air quality far above the health safety levels recommended by the WHO. Both these metropolitan regions rank among the global cities with the highest traffic intensity indexes. Reducing traffic intensity is an example of a pollution control policy that has already been successfully adopted in other large urban areas in Europe, for example.
Recently, mechanistic studies have suggested that air pollution particles can cross the olfactory barrier and reach directly the brain (38). Once in the brain, these particles could trigger neuroinflammation (39, 40) and exaggerated protein misfolding, leading to dementia (9, 40–42). This evidence is still in its early stages and is not yet robust. However, a growing number of epidemiological studies in Europe (11, 13, 16, 43), North America (9, 12, 14, 44–46), and Asia (10) are showing that living in highly polluted areas increases the risk of dementia. Some studies suggest that the link is driven by cardiovascular alterations caused by air pollution (13, 14), but the direct effect pathway was not ruled out. The hypothesis that the association between air pollution and dementia is mediated by cardiovascular disease and metabolic syndrome is reasonable since air pollution is known to cause and aggravate cardiovascular conditions. Nevertheless, the scientific community does not seem to be ready to affirm that air pollution affects the brain and causes dementia (47). Studies in the field are susceptible to a wide range of biases, from the selection of dementia cases to the characterization of long-term exposure to air pollution for each participant. This might explain why air pollution has not yet been included in the list of established and potentially modifiable risk factors for dementia (35–37). We suggest that it is important to change this perspective and consider air pollution a risk factor for dementia, to reduce the burden of the disease in LAC countries. Furthermore, this should be done posthaste. We are not alone. In August 2020, for the first time, a report on dementia prevention listed air pollution as a modifiable risk for the condition (48).
Indirect Associations: Chronic Diseases Linked to Dementia and Air Pollution
Air pollution causes and/or aggravates obesity, hypertension, stroke, diabetes mellitus, and heart diseases. These are all established risk factors for dementia (35–37). Air pollution has also been linked to three other established risk factors for dementia (i.e., physical inactivity, cognitive inactivity, and depression), but the evidence is weaker. In this section, we will discuss these links.
Obesity, Diabetes Mellitus, and Physical Inactivity
Approximately 302 million adults living in the LAC region are overweight, and more than 100 million are obese (49). By the year 2030, overweight and obesity are expected to affect 50% of men and 60% of women in Latin America (50). The countries with the highest prevalence of obesity are El Salvador and Paraguay for females, and Uruguay and Chile for males (51).
Overweight and obesity can be reversed and prevented. Air pollution is linked to metabolic disorders (52). For this reason, safe air quality is among the actions that may reduce the burden of overweight and obesity, alongside healthy diets and physical exercise. Various mechanisms underlie the link between air pollution and increased body weight. Air pollution can cause metabolic dysfunction by increasing oxidative stress in adipose tissue (53) and inflammation. Besides this, liver cells can accumulate more lipids, and skeletal muscles may use less glucose. Obesity is a significant health challenge, as it substantially increases the risk for diseases, such as type 2 diabetes mellitus, fatty liver disease, stroke, and dementia (54). More recently, obesity has been identified as a risk factor for Alzheimer's disease due to hyperglycemia (55). Air pollution can indirectly affect body weight, thus, increasing the risk of other chronic diseases.
Air pollution also prevents people from engaging in regular physical activity, resulting in sedentary behavior (56, 57). Significant levels of air pollution have been negatively associated with physical activity due to decreased lung function, high blood pressure, and other cardiovascular and respiratory symptoms that impair exercise capacity and performance (56, 57).
Cardiovascular and Cerebrovascular Diseases
Epidemiological and observational studies have deepened the knowledge we have about air pollution and its effects on human health (58). Cardiovascular diseases and high blood pressure have been associated with short and long term exposure to air pollution, generated by inflammation, oxidative stress, and arterial remodeling (58, 59).
There are two main types of exposure to air pollution. The first is acute exposure, defined as short-term exposure or a slow but brief increase in pollutant concentrations that may vary in a single day or over several days. Chronic or long-term exposure is exposure to air pollutants over several months or years. Acute exposure to air pollution can result in a similar acute event, such as a thrombosis-induced stroke (60), a rapid rise in blood pressure, or cardiac arrhythmia. Chronic exposure to air pollution can have a direct effect on the brain, triggering and/or furthering neurodegeneration (61) or silent ischemic injuries (62).
Short-term exposure to air pollution can induce vasoconstriction, rupture of atheromatous plaques through inflammatory processes, and cause oxidative stress and thrombin activation. Regarding PM2.5 concentrations, these may cause reduced blood flow in the brain, and ozone can induce cardioembolic strokes, affect heart rate variability, and stimulate atrial fibrillation. On the other hand, chronic exposure can manifest clinically as recurrent strokes provoked by the genesis and progression of atheromas and myocardial infarction (63).
Exposure to air pollution can trigger changes in the cardiovascular system, and these effects can develop acutely, with increased atherosclerosis accelerating the response to chronic disease. Air pollution has also been related to lowering the density of high-density lipoproteins (HDL) due to oxidative stress and inflammation. These processes can cause changes in the structure and function of HDL, resulting in pro-atherogenic or dysfunctional HDL (64). Furthermore, air pollution has been correlated with an increased risk for ventricular arrhythmias and increased ventricular electrical instability, highlighting the potential link between air pollution and sudden cardiac deaths (65).
High concentrations of air pollutants may be correlated with the risk for angina and acute myocardial infarction. Short-term exposure to PM2.5 at levels of 10 mg/m3 or higher contributes to acute coronary syndromes, especially in patients with preexisting heart disease. The effects are more severe after long-term exposure to traffic (66, 67). Recent studies have suggested that even modest increases in airborne pollutants can trigger an increase in blood pressure in a few hours (68) and affect heart rate variability, vascular tone, and blood coagulation, as well as promote atherosclerosis (69). Even short-term exposure to air pollution has been associated with increased cardiovascular issues and deaths from myocardial ischemia, arrhythmia, and heart failure (59, 70, 71).
Hypertension and heart disease are the main diseases that affect the population worldwide (72). Several studies have indicated that air pollution is a risk factor for hypertension, heart disease (73, 74), and stroke (72, 73).
Research has produced some evidence regarding the association between hypertension, changes in blood pressure, and exposure to PM2.5 and PM10 (particles with an aerodynamic diameter of_or greater than 10 μm). Results indicated that long-term exposure to a 10-μg/m3 increase in PM10 and PM2.5 is significantly associated with higher systolic and diastolic blood pressure, in addition to a greater risk of hypertension (74). The hypertensive effects of air pollution were more pronounced among men, smokers, drinkers, individuals with a high-fat diet, and those with a high level of physical activity (75).
Elderly patients demonstrate a more apparent association between high blood pressure and cognitive decline when the former condition first arises in middle age. Hypertension can promote changes in the structure and function of the brain through remodeling cerebral vessels. This can lead to disruptions in cerebral self-regulation, reductions in cerebral perfusion, and limitations in the brain's ability to clear potentially harmful proteins, such as β-amyloid (76). Moreover, hypertension disrupts the structure and function of brain blood vessels and can lead to ischemic damage in the white matter that is critical for cognitive function, thus, favoring the development of neurodegenerative diseases (77).
In the case of cerebrovascular diseases, exposure to air pollution particles has also been associated with neuroinflammation (78). The first evidence of neuroinflammation caused by the inhalation of pollution was published in a study involving dogs that had been exposed to significant concentrations of ozone, PM, and other pollutants. Researchers detected inflammation in the brain of the animals with endothelial damage (79). Other in vivo studies have shown that PM can stimulate inflammatory and oxidative responses in the CNS (80, 81). Mice exposed to diesel inhalation showed acceleration in the development of Alzheimer's disease characteristics (82), and activated microglial and inflammatory responses. These animal studies demonstrated signs of cellular damage associated with air pollution (83, 84).
Air Pollution, Depression, and Cognitive Inactivity
Studies have shown that exposure to air pollution may be associated with more frequent incidence of depression, anxiety, and cognitive inactivity, especially in people who suffer from concomitant chronic diseases (85). Another study has shown that increases in air pollution may lead to the onset of depressive symptoms among the elderly (41). The pathogenesis may involve oxidative stress and generalized inflammation induced by PM. The pathomechanisms have been linked to vascular lesions and neurodegenerative disorders (86). As a result, these processes may cause or exacerbate the symptoms of depression (87).
Toxicity Mechanisms of Air Pollution
Exposure to contaminated external air is considered an environmental risk factor that promotes brain aging; in contrast, the effects of air pollution on the central nervous system (CNS) are not broadly recognized. Air pollution can cause various neurological disorders as a result of nervous system inflammation and oxidative stress. Damage to neuronal cells caused by fine dust, especially in fetuses and infants, can cause permanent brain damage or lead to neurological disease in adulthood. Epidemiological studies have reported that the risk of developing dementia and Alzheimer's disease is increased by exposure to fine particulates (60).
The role of air pollution in causing metabolic dysfunction is already known (53). The mechanisms by which air pollutants affect the body systems are intimately related to the type and size of inhaled pollutants. The size, load, chemical composition, and propensity to form aggregates determine a pollutant's ability to cross the lung and the blood barrier. The large-diameter PM (PM10) cannot be transported directly into the blood circulation and require neural or proinflammatory responses to mediate extrapulmonary actions, whereas the ultrafine or soluble PM that constitutes smaller particles can enter the bloodstream directly.
In Figure 1, we show the plausible mechanisms of how air pollution affects the human health leading to neurologic impairments highlighting the increased oxidative stress and the pronounced inflammatory responses associated with cardiovascular diseases and metabolic syndromes.
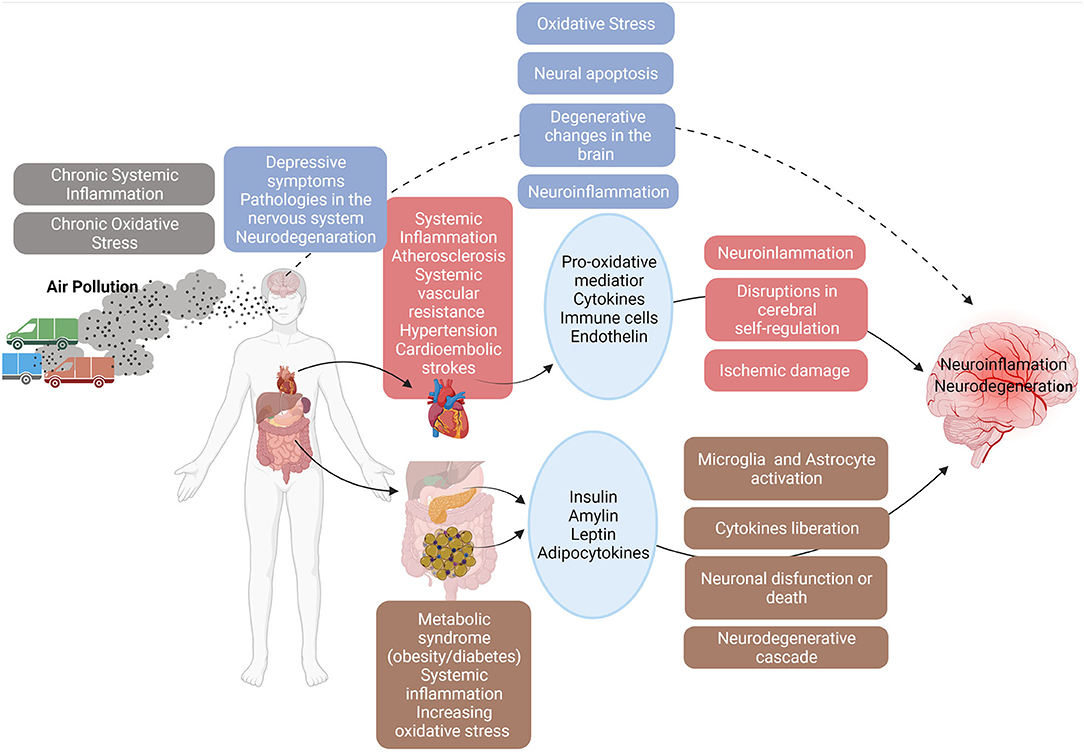
Figure 1. The toxicity mechanisms: air pollution acts directly in brain and indirectly in cardiovascular diseases and metabolic syndromes causing neuroinflammation and neurodegeneration. Created with BioRender.com.
The toxic effects of pollution on cardiovascular diseases are also known (58, 59). The first response caused by inhalation of air pollutants is characterized by the release of pro-oxidative/inflammatory mediators (cytokines, activated immune cells, or platelets) and/or vasoactive mediators (endothelin) in the systemic circulation. Particle inhalation can trigger systemic inflammation, atherosclerosis, and endothelial dysfunction, resulting in increased systemic vascular resistance and hypertension. It is worth noting that the duration of exposure, the levels of co-pollutants, and patient sensitivity are factors that determine subsequent responses (70, 71).
In the second path of action, air pollutants accumulate in the respiratory tree. This can directly stimulate the lung's nervous reflexes, leading to an autonomic imbalance that subsequently favors vasoconstriction (70, 71). In the third pathway, metallic particles and ultrafine PM are inhaled. These can pass through the alveolar and capillary membrane, reach the circulatory system, and cause damage to vasomotor regulation (58, 70, 71, 88).
The direct or indirect effects of air pollution can be associated with stroke and dementia risks. Direct damage can be caused by neuroinflammation and neurodegeneration leading to neurodegenerative diseases (38). Magnetite findings in the magnetic resonance images of human brains exposed to air pollution explain the direct relationship between PM air pollution and AD (89). The indirect mechanism of air pollution in the cerebrovascular system causes stroke, vascular dementia, or other types of dementia. This may be mediated by certain effects on the cardio-neuro-vascular system, such as atherosclerosis, plaque formation and rupture, endothelial dysfunction, cardiac arrhythmia, hypertension, and activated thrombin (90, 91).
By itself, the obesity–diabetes–dementia connection occurs through inflammation and oxidative stress in the brain, caused by systemic inflammation. It is characterized by increased levels of systemic inflammatory mediators (cytokines) that cross the blood–brain barrier (BBB) and metabolic mediators released by adipose tissue and the pancreas (leptin, insulin, and amylin) that play additional important roles in mediating central nervous system inflammation and neuronal regulation (92), and leading to activation of microglia and astrocytes, inducing the release of cytokines and oxidants. This inflammatory microenvironment causes neuronal dysfunction or death and creates a neurodegenerative cascade.
In obesity and diabetes, there is evidence that exposure to PM 2.5 alters endothelial function, increasing serum levels of tumor necrosis factor alpha (TNF-a), as well as higher levels of interleukin-6 (IL-6), resistin, and leptin (93). Furthermore, Gasparotto et al. (94) investigated oxidative damage and inflammation in different brain regions of obese rats exposed to coal ash, and the results showed that obese rats that inhaled coal ash were more affected by oxidative damage with subsequent inflammation in the hippocampus. This type of damage can lead to chronic neurodegeneration (94).
There are many mechanisms through which air pollutants may cause pathologies in the nervous system, such as nervous system inflammation, oxidative stress, microglial cell activation, protein condensation, and cerebral vascular barrier disorders, but how these mechanisms occur is still unclear (60). The main components of air pollution, PM2.5, as well as the compounds absorbed on their surfaces arrest cell cycles and cause neural apoptosis. These effects, together with the oxidative stress and gene expression alteration induced by these particles, may lead to degenerative changes in the brain (95). Substances found in smog may also cause systemic inflammation with an increased number of active immune cells producing proinflammatory cytokines that pass through the BBB via active transport. As a result, the migration of monocytes to the central nervous system is intensified, aggravating the neuroinflammation process (96).
Direct Association: Air Pollution and Dementia
Higher prevalence of neurodegenerative diseases will certainly come along with population aging. Taking dementia as a reference, the higher increase will occur in LMICs (97).
Air pollution represents an important source of premature mortality and morbidity globally (98) but unevenly distributed across the Globe, since household and outdoor air pollution concentrations are higher in developing countries (20). Adverse effects of air pollution on human health have been mostly attributed to cardiorespiratory events. However, recent studies provide evidence that other health conditions may be influenced by exposures to airborne contaminants, including central neurodegenerative diseases such as Alzheimer's disease, Parkinson's disease, and mood disorders (99–101).
A series of studies conducted in Mexico demonstrated the usefulness of autopsies in exploring the links between air pollution and cerebral damage (38, 81, 87–89, 102). Thus, a study combining precise measures of exposure, collected cerebral tissues, and autopsy materials could provide important information about the role of air pollution in the development of neurodegenerative diseases.
Other researchers investigated the distribution of the alpha-emitting radon progeny 210-Polonium (210Po) in the olfactory epithelium, olfactory bulb, frontal lobe, and lung tissues of cadavers in São Paulo, Brazil (103). The findings showed that the olfactory bulbs presented higher concentrations of 210Po in comparison with other tissues. The higher concentrations of 210Po in olfactory bulbs suggest that this is a major path entryway for transporting radon progeny from nasal tissues to the central nervous system.
In children, respiratory inflammation is recurrent, especially in the nasal epithelium (99). This leads to changes in the nasal mucous membranes, causing the breakdown of the nasal epithelial barrier and facilitates the passage of xenobiotics into the systemic circulation and the brain. Such damage causes neuroinflammation and the breakdown of the BBB and can affect the olfactory bulb, prefrontal cortex, and brain stem. In patients with apolipoprotein E4, it can significantly accelerate olfactory decline, attention, and short-term memory contributing to neurodegeneration and the progress of Alzheimer's disease (80, 104, 105).
Discussion
The burden of dementia in LAC is high and will increase (1). Reducing dementia risks is crucial and urgently needed in this region. Reducing the levels of air pollution has been shown to improve health outcomes (24–26, 106). Several parts of the LAC region experience bad air quality, and some areas will see an increasing trend in air pollution levels in the coming years (18, 28). At least 172 million LAC inhabitants breathe unhealthy levels of air pollution (29), but there is room to improve their air quality. A better air quality in the region could reduce their risk of developing dementia.
Air pollution control and regulations in LAC countries are not robust (107) and could be improved. Official ground-level information on pollutants is rare (107), and only eight countries have set National Air Quality Standards for fine particulates (108), all above the level recommended by the World Health Organization (109). Three countries in the LAC region were studied in a systematic review on interventions to improve air quality (106), but the reported policies have had little to no success in improving pollution levels. In Ecuador, government action during highly polluted periods effectively reduced the levels of particulate pollution by 20% (110). Although this is a positive policy that will prevent peaks in air pollution, it provides little to no aid in managing the hazards of long-term exposure to polluted air. In Chile, reducing the number of buses alone was not effective in reducing pollution (111). The reported reforms in the public transportation systems in Mexico City and Santiago resulted in a large number of cars and higher levels of pollution (112). Despite the scarcity of documented reports in the literature, the region has had successful experiences controlling air pollution. A proof is the reduction in fine particulate pollution after 2010 in São Paulo and Bogotá (18). At least in São Paulo, the better air quality is mostly attributed to a national pollution control program in Brazil that set progressively more stringent standards to reduce vehicular emission of new models and the large scale of ethanol and biodiesel enforced by law (113). The targets and deadlines of the Brazilian pollution control program were postponed in different occasions along the years. It is important to notice that the improvement in air quality was achieved for some, but not all, pollutants in the air. The control of secondary pollutants (pollutants formed in the atmosphere, not directly emitted from a source, such as fine particulates) remain a challenge, and despite the improvement in air quality, pollution levels in São Paulo do not yet conform to the WHO's safety recommendations (113). Pollution control and management in São Paulo and in LAC need to be more aggressive to achieve the air pollution safety levels recommended by the WHO. A discussion on possible interventions to improve air quality and health outcomes can be found elsewhere (106).
As explained in detail in previous sections of this manuscript, air pollution causes and aggravates five established risk factors for dementia (obesity, hypertension, stroke, diabetes mellitus, and heart diseases) and has been linked to three others physical inactivity, cognitive inactivity, and depression (35–37). CVD and diabetes mellitus (DM) are the leading causes of mortality and morbidity in the LAC region, resulting in almost 1 million deaths. In 2016, 18.4 million DALYs were lost to cardiovascular disease (114, 115). For diabetics, there were 195,000 deaths, and 8.5 million DALYs were lost in 2016 (114–117). In 2019, these numbers improved by 1% for both diseases (114). The prevalence of these risk factors is higher in LAC countries when compared with the world and other LMICs. The population attributable fractions (PAF) for hypertension is 9% in the LAC region vs. 2% around the world, 6% in China, and 4% in India. The obesity numbers show a similar situation: 8% in the LAC territory vs. 1% around the world, 6% in China, and 3% in India. For diabetes, the LAC PAF is 3% vs. 1% around the world, and 2% in China and India (118). Fifty-six percent of the dementia cases in LAC countries could be avoided if individual risk factors were eliminated. That proportion is higher than in China (49%) and India (41%) (118).
Reducing air pollution could attenuate the prevalence of these established risk factors in the population and, therefore, lower the high burden of dementia in the region. Indeed, two recent cohort studies in Europe (13) and North America (14) have suggested that cardiovascular diseases mediate the association between air pollution and dementia. No similar studies regarding LAC countries were found. However, there is no reason to speculate that cardiovascular disease triggered by air pollution would not culminate in dementia in the LAC population.
As we mentioned in the Introduction section, it is plausible to think that air pollution may directly cause dementia. The body of evidence on air pollution and dementia is growing rapidly, with many relevant studies published recently (13–16). Further studies will collaborate to elucidate if air pollution can enter the brain and cause dementia. Nevertheless, whether the agency is direct or indirect, it is clear that air pollution has been associated with dementia, and it is reasonable to expect that reductions in air pollution would help decrease the burden of this disorder.
Given the urgent need to lower the burden of dementia in LAC countries, we recommend implementing strategies to reduce air pollution levels and related risks. We base our argument on the findings that (1) air pollution causes and/or aggravates at least five of the established risk factors of dementia (obesity, hypertension, stroke, diabetes mellitus, and heart diseases), (2) reducing air pollution has been shown to reduce some of these risks, and (3) there is room for improving the air quality in many urban LAC areas and other LMICs. These improvements are already being explored by several urban centers in developing regions with proven health benefits for their population. Although we will just be possible to estimate the real impact of reducing the levels of air pollution in LAC in the burden of dementia in the future, there is no reported side effect for breathing better air quality.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
LF designed the study, reviewed the literature, and wrote the manuscript. NVS and MMV reviewed he literature and wrote the manuscript. VYY interpreted and synthetize the data and revised the manuscript. KVM updated the literature review and revised the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding
This research was funded by the São Paulo Research Foundation (FAPESP), grant #16/22793-0.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. International A-AsD. World Alzheimer Report 2015. The Global Impact of Dementia: an Analysis of Prevalence, Incidence. Costs and Trends. London: Alzheimer's Disease International (ADI). (2015).
2. Custodio N, Wheelock A, Thumala D, Slachevsky A. Dementia in Latin America: epidemiological evidence and implications for public policy. Front Aging Neurosci. (2017) 9:221. doi: 10.3389/fnagi.2017.00221
3. Ibanez A, Parra MA, Butlerfor C, Latin A, the Caribbean Consortium on D. The latin america and the caribbean consortium on dementia (LAC-CD): from networking to research to implementation science. J Alzheimers Dis. (2021) 82:S379–S394. doi: 10.3233/JAD-201384
4. Parra MA, Baez S, Allegri R, Nitrini R, Lopera F, Slachevsky A, et al. Dementia in latin America: assessing the present and envisioning the future. Neurology. (2018) 90:222–31. doi: 10.1212/WNL.0000000000004897
5. Organization WH. Global Action Plan on the Public Health Response to Dementia 2017–2025. Geneva: World Health Organization. (2017).
6. Adams DR, Ajmani GS, Pun VC, Wroblewski KE, Kern DW, Schumm LP, et al. Nitrogen dioxide pollution exposure is associated with olfactory dysfunction in older U.S. adults. Int Forum Allergy Rhinol. (2016) 6:1245–52. doi: 10.1002/alr.21829
7. Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study (2015). Lancet. (2017) 389:1907–18. doi: 10.1016/S0140-6736(17)30505-6
8. Forouzanfar MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1659–724. doi: 10.1016/S0140-6736(16)31679-8
9. Cacciottolo M, Wang X, Driscoll I, Woodward N, Saffari A, Reyes J, et al. Particulate air pollutants, APOE alleles and their contributions to cognitive impairment in older women and to amyloidogenesis in experimental models. Transl Psychiatry. (2017) 7:e1022. doi: 10.1038/tp.2016.280
10. Jung CR, Lin YT, Hwang BF. Ozone, particulate matter, and newly diagnosed Alzheimer's disease: a population-based cohort study in Taiwan. J Alzheimers Dis. (2015) 44:573–84. doi: 10.3233/JAD-140855
11. Carey IM, Anderson HR, Atkinson RW, Beevers SD, Cook DG, Strachan DP, et al. Are noise and air pollution related to the incidence of dementia? A cohort study in London England. BMJ Open. (2018) 8:e022404. doi: 10.1136/bmjopen-2018-022404
12. Chen H, Kwong JC, Copes R, Hystad P, van Donkelaar A, Tu K, et al. Exposure to ambient air pollution and the incidence of dementia: a population-based cohort study. Environ Int. (2017) 108:271–7. doi: 10.1016/j.envint.2017.08.020
13. Grande G, Ljungman PLS, Eneroth K, Bellander T, Rizzuto D. Association between cardiovascular disease and long-term exposure to air pollution with the risk of dementia. JAMA Neurol. (2020) 77:801–9. doi: 10.1001/jamaneurol.2019.4914
14. Ilango SD, Chen H, Hystad P, van Donkelaar A, Kwong JC, Tu K, et al. The role of cardiovascular disease in the relationship between air pollution and incident dementia: a population-based cohort study. Int J Epidemiol. (2020) 49:36–44. doi: 10.1093/ije/dyz154
15. Cancer IAfRo. Air Pollution and Cancer France. World Health Organization. (2013). Report No.: 978-92-832-2166-1.
16. Oudin A, Forsberg B, Adolfsson AN, Lind N, Modig L, Nordin M, et al. traffic-related air pollution and dementia incidence in northern sweden: a longitudinal study. Environ Health Perspect. (2016) 124:306–12. doi: 10.1289/ehp.1408322
17. Huat TJ, Camats-Perna J, Newcombe EA, Valmas N, Kitazawa M, Medeiros R. Metal toxicity links to alzheimer's disease and neuroinflammation. J Mol Biol. (2019) 431:1843–68. doi: 10.1016/j.jmb.2019.01.018
18. Brauer M, Freedman G, Frostad J, van Donkelaar A, Martin RV, Dentener F, et al. Ambient air pollution exposure estimation for the global burden of disease 2013. Environ Sci Technol. (2016) 50:79–88. doi: 10.1021/acs.est.5b03709
19. Fajersztajn L, Saldiva P, Pereira LAA, Leite VF, Buehler AM. Short-term effects of fine particulate matter pollution on daily health events in Latin America: a systematic review and meta-analysis. Int J Public Health. (2017) 62:729–38. doi: 10.1007/s00038-017-0960-y
20. Fajersztajn L, Veras M, Barrozo LV, Saldiva P. Air pollution: a potentially modifiable risk factor for lung cancer. Nat Rev Cancer. (2013) 13:674–8. doi: 10.1038/nrc3572
21. Martins MCH, Fatigati FL, Ve'spoli TC, Martins LC, Pereira LAA, Martins MA, et al. Influence of socioeconomic conditions on air pollution adverse health effects in elderly people: an analysis of six regions in Sa~o Paulo, Brazil. J Epidemiol Community Health. (2004) 58:41–6. doi: 10.1136/jech.58.1.41
22. Hajat A, Diez-Roux AV, Adar SD, Auchincloss AH, Lovasi GS, O'Neill MS, et al. Air pollution and individual and neighborhood socioeconomic status: evidence from the Multi-Ethnic Study of Atherosclerosis (MESA). Environ Health Perspect. (2013) 121:1325–33. doi: 10.1289/ehp.1206337
23. Hajat A, Hsia C, O'Neill MS. Socioeconomic disparities and air pollution exposure: a global review. Curr Environ Health Rep. (2015) 2:440–50. doi: 10.1007/s40572-015-0069-5
24. Laden F, Schwartz J, Speizer FE, Dockery DW. Reduction in fine particulate air pollution and mortality: extended follow-up of the harvard six cities study. Am J Respir Crit Care Med. (2006) 173:667–72. doi: 10.1164/rccm.200503-443OC
25. Clancy L, Goodman P, Sinclair H, Dockery DW. Effect of air-pollution control on death rates in Dublin, Ireland: an intervention study. Lancet. (2002) 360:1210–4. doi: 10.1016/S0140-6736(02)11281-5
26. Rich DQ, Kipen HM, Huang W, Wang G, Wang Y, Zhu P, et al. Association between changes in air pollution levels during the Beijing Olympics and biomarkers of inflammation and thrombosis in healthy young adults. JAMA. (2012) 307:2068–78. doi: 10.1001/jama.2012.3488
27. Yinon L, Thurston G. An evaluation of the health benefits achieved at the time of an air quality intervention in three Israeli cities. Environ Int. (2017) 102:66–73. doi: 10.1016/j.envint.2016.12.025
28. Gómez Peláez LM, Santos JM, de Almeida Albuquerque TT, Reis NC, Andreão WL, de Fátima Andrade M. Air quality status and trends over large cities in South America. Environ Sci. Policy. (2020) 114:422–35. doi: 10.1016/j.envsci.2020.09.009
29. Gouveia N, Kephart JL, Dronova I, McClure L, Granados JT, Betancourt RM, et al. Ambient fine particulate matter in Latin American cities: levels, population exposure, and associated urban factors. Sci Total Environ. (2021) 772:145035. doi: 10.1016/j.scitotenv.2021.145035
30. Jacobson Lda S, Hacon Sde S, de Castro HA, Ignotti E, Artaxo P, Saldiva PH, et al. Acute effects of particulate matter and black carbon from seasonal fires on peak expiratory flow of schoolchildren in the Brazilian Amazon. PLoS ONE. (2014) 9:e104177. doi: 10.1371/journal.pone.0104177
31. Marlier ME, Bonilla EX, Mickley LJ. How do Brazilian fires affect air pollution and public health? Geohealth. (2020) 4:e2020GH000331. doi: 10.1029/2020GH000331
32. Matsuda M, Braga ALF, Marquezini MV, Monteiro MLR, Saldiva PHN, de Santos U. Occupational effect of sugarcane biomass burning on the conjunctival mucin profile of harvest workers and residents of an adjacent town-A Brazilian panel study. Exp Eye Res. (2020) 190:107889. doi: 10.1016/j.exer.2019.107889
33. Cancado JE, Saldiva PH, Pereira LA, Lara LB, Artaxo P, Martinelli LA, et al. The impact of sugar cane-burning emissions on the respiratory system of children and the elderly. Environ Health Perspect. (2006) 114:725–9. doi: 10.1289/ehp.8485
34. Maas A, Kothe H, Centeno IP, Leiva MJG, Dalhoff1 K. Prevalence of chronic bronchitis and respiratory health profile of a population exposed to wood smoke in Nicaragua. J Health Pollut. (2020) 10:1–9. doi: 10.5696/2156-9614-10.26.200607
35. Livingston G, Sommerlad A, Orgeta V, Costafreda SG, Huntley J, Ames D, et al. Dementia prevention, intervention, and care. Lancet. (2017) 390:2673–734. doi: 10.1016/S0140-6736(17)31363-6
36. Barnes DE, Yaffe K. The projected effect of risk factor reduction on Alzheimer's disease prevalence. Lancet Neurol. (2011) 10:819–28. doi: 10.1016/S1474-4422(11)70072-2
37. International AsD. From plan to impact Progress towards targets of the Global action plan on dementia (2018). London: Alzheimer's Disease International (ADI) (2018).
38. Maher BA, Ahmed IA, Karloukovski V, MacLaren DA, Foulds PG, Allsop D, et al. Magnetite pollution nanoparticles in the human brain. Proc Natl Acad Sci USA. (2016) 113:10797–801. doi: 10.1073/pnas.1605941113
39. Block ML, Elder A, Auten RL, Bilbo SD, Chen H, Chen JC, et al. The outdoor air pollution and brain health workshop. Neurotoxicology. (2012) 33:972–84. doi: 10.1016/j.neuro.2012.08.014
40. Cacciottolo M, Morgan TE, Saffari AA, Shirmohammadi F, Forman HJ, Sioutas C, et al. Traffic-related air pollutants (TRAP-PM) promote neuronal amyloidogenesis through oxidative damage to lipid rafts. Free Radic Biol Med. (2020) 147:242–51. doi: 10.1016/j.freeradbiomed.2019.12.023
41. Calderon-Garciduenas L, Kavanaugh M, Block M, D'Angiulli A, Delgado-Chavez R, Torres-Jardon R, et al. Neuroinflammation, hyperphosphorylated tau, diffuse amyloid plaques, and down-regulation of the cellular prion protein in air pollution exposed children and young adults. J Alzheimers Dis. (2012) 28:93–107. doi: 10.3233/JAD-2011-110722
42. Calderon-Garciduenas L, Reynoso-Robles R, Perez-Guille B, Mukherjee PS, Gonzalez-Maciel A. Combustion-derived nanoparticles, the neuroenteric system, cervical vagus, hyperphosphorylated alpha synuclein and tau in young Mexico City residents. Environ Res. (2017) 159:186–201. doi: 10.1016/j.envres.2017.08.008
43. Oudin A, Segersson D, Adolfsson R, Forsberg B. Association between air pollution from residential wood burning and dementia incidence in a longitudinal study in Northern Sweden. PLoS ONE. (2018) 13:e0198283. doi: 10.1371/journal.pone.0198283
44. Chen H, Kwong JC, Copes R, Tu K, Villeneuve PJ, van Donkelaar A, et al. Living near major roads and the incidence of dementia. Parkinson's disease, and multiple sclerosis: a population-based cohort study. Lancet. (2017) 389:718–26. doi: 10.1016/S0140-6736(16)32399-6
45. Kulick ER, Elkind MSV, Boehme AK, Joyce NR, Schupf N, Kaufman JD, et al. Long-term exposure to ambient air pollution, APOE-epsilon4 status, and cognitive decline in a cohort of older adults in northern Manhattan. Environ Int. (2020) 136:105440. doi: 10.1016/j.envint.2019.105440
46. Kulick ER, Wellenius GA, Boehme AK, Joyce NR, Schupf N, Kaufman JD, et al. Long-term exposure to air pollution and trajectories of cognitive decline among older adults. Neurology. (2020) 94:e1782–e92. doi: 10.1212/WNL.0000000000009314
47. Weuve J. Are we ready to call exposure to air pollution a risk factor for dementia? Neurology. (2020) 94:727–8. doi: 10.1212/WNL.0000000000009318
48. Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
49. FAO OPS WFP y UNICEF. Panorama de la seguridad alimentaria y nutrición en América Latina y el Caribe 2019. Santiago. 136 (2019). Licencia: CC BY-NC-SA 3.0 IGO.
50. Aschner P. Obesity in Latin America BT-Metabolic Syndrome: A Comprehensive Textbook. Ahima RS, editor. Cham: Springer International Publishing. (2014) p. 1–8.
51. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2014) 384:766–81. doi: 10.1016/S0140-6736(14)60460-8
52. Rao X, Patel P, Puett R, Rajagopalan S. Air pollution as a risk factor for type 2 diabetes. Toxicol Sci. (2015) 143:231–41. doi: 10.1093/toxsci/kfu250
53. Mullins J, Bharadwaj P. Effects of Short-Term Measures to Curb Air Pollution: Evidence from Santiago, Chile. Am J Agric Econ. (2014) 97:1107–34.
54. Blüher M. Obesity. global epidemiology and pathogenesis. Nat Rev Endocrinol. (2019) 15:288–98. doi: 10.1038/s41574-019-0176-8
55. Xue J, Ideraabdullah FY. An assessment of molecular pathways of obesity susceptible to nutrient, toxicant and genetically induced epigenetic perturbation. J Nutr Biochem. (2016) 30:1–13. doi: 10.1016/j.jnutbio.2015.09.002
56. An R, Ji M, Yan H, Guan C. Impact of ambient air pollution on obesity: A systematic review. Int J Obes. (2018) 42:1112–26. doi: 10.1038/s41366-018-0089-y
57. Croft DP, Zhang W, Lin S, Thurston SW, Hopke PK, Masiol M, et al. The association between respiratory infection and air pollution in the setting of air quality policy and economic change. (2019). Ann Am Thorac Soc. 16:321–30. doi: 10.1513/AnnalsATS.201810-691OC
58. Sanidas E, Papadopoulos DP, Grassos H, Velliou M, Tsioufis K, Barbetseas J, et al. Air pollution and arterial hypertension. A new risk factor is in the air. J Am Soc Hypertens. (2017) 11:709–15. doi: 10.1016/j.jash.2017.09.008
59. Jalaludin B, Cowie C. Particulate air pollution and cardiovascular disease - It is time to take it seriously. Rev Environ Health. (2014) 29:129–32. doi: 10.1515/reveh-2014-0031
60. Kim H, Kim WH, Kim YY, Park HY. Air Pollution and Central Nervous System Disease: A Review of the Impact of Fine Particulate Matter on Neurological Disorders. Front Public Health. (2020) 8:575330. doi: 10.3389/fpubh.2020.575330
61. Béjot Y, Reis J, Giroud M, Feigin V. A review of epidemiological research on stroke and dementia and exposure to air pollution. Int J Stroke. (2018) 13:687–95. doi: 10.1177/1747493018772800
62. Calderon-Garciduenas L, Mora-Tiscareno A, Ontiveros E, Gomez-Garza G, Barragan-Mejia G, Broadway J, et al. Air pollution, cognitive deficits and brain abnormalities: a pilot study with children and dogs. Brain Cogn. (2008) 68:117–27. doi: 10.1016/j.bandc.2008.04.008
63. Kim Y, Myung W, Won H-H, Shim S, Jeon HJ, Choi J, et al. Association between air pollution and suicide in South Korea: a nationwide study. PLoS ONE. (2015) 18 10:e0117929. doi: 10.1371/journal.pone.0117929
64. Jianping L, Changping Z, Hongbing XD, BR, Shengcong L, Tieci Y, et al. Ambient air pollution is associated with HDL (high-density lipoprotein) dysfunction in healthy adults. Arterioscler Thromb Vasc Biol. (2019) 39:513–22. doi: 10.1161/ATVBAHA.118.311749
65. Folino F, Buja G, Zanotto G, Marras E, Allocca G, Vaccari D, et al. Association between air pollution and ventricular arrhythmias in high-risk patients (ARIA study): a multicentre longitudinal study. Lancet Planet Heal. (2017) 1:e58–64. doi: 10.1016/S2542-5196(17)30020-7
66. Mishra S. Is smog innocuous? Air pollution and cardiovascular disease. Indian Heart J. (2017) 69:425–9. doi: 10.1016/j.ihj.2017.07.016
67. Tonne C, Melly S, Mittleman M, Coull B, Goldberg R, Schwartz J. A case-control analysis of exposure to traffic and acute myocardial infarction. Environ Health Perspect. (2007) 115:53–7. doi: 10.1289/ehp.9587
68. Cai Y, Zhang B, Ke W, Feng B, Lin H, Xiao J, et al. Associations of short-term and long-term exposure to ambient air pollutants with hypertension: a systematic review and meta-analysis. Hypertension. (2016) 68:62–70. doi: 10.1161/HYPERTENSIONAHA.116.07218
69. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. (2012) 380:2224–60. doi: 10.1016/S0140-6736(12)61766-8
70. Brook RD. Cardiovascular effects of air pollution. Clin Sci (Lond). (2008) 115:175–87. doi: 10.1042/CS20070444
71. Mills NL, Donaldson K, Hadoke PW, Boon NA, MacNee W, Cassee FR, et al. Adverse cardiovascular effects of air pollution. Nat Clin Pract Cardiovasc Med. (2009) 6:36–44. doi: 10.1038/ncpcardio1399
72. Wellenius GA, Schwartz J, Mittleman MA. Air pollution and hospital admissions for ischemic and hemorrhagic stroke among medicare beneficiaries. STROKE. (2005) 36:2549–53. doi: 10.1161/01.STR.0000189687.78760.47
73. Yang BY, Guo Y, Bloom MS, Xiao X, Qian Z (Min), Liu E, et al. Ambient PM1 air pollution, blood pressure, and hypertension: Insights from the 33 Communities Chinese Health Study. Environ Res. (2019) 170:252–9. Available from:. doi: 10.1016/j.envres.2018.12.047
74. Li N, Chen G, Liu F, Mao S, Liu Y, Liu S, et al. Associations between long-term exposure to air pollution and blood pressure and effect modifications by behavioral factors. Environ Res. (2020) 182:1–8. doi: 10.1016/j.envres.2019.109109
75. Sun Q, Hong X, Wold LE. Cardiovascular effects of ambient particulate air pollution exposure. Circulation. (2010) 121:2755–65. doi: 10.1161/CIRCULATIONAHA.109.893461
76. Iadecola C, Yaffe K, Biller J, Bratzke LC, Faraci FM, Gorelick PB, et al. Impact of hypertension on cognitive function: a scientific statement from the American heart association. Hypertension. (2016) 68: e67–e94. doi: 10.1161/HYP.0000000000000053
77. Calderón-Garcidueñas L, Reed W, Maronpot RR, Henríquez-Roldán C, Delgado-Chavez R, Calderón-Garcidueñas A, et al. Brain inflammation and Alzheimer's-like pathology in individuals exposed to severe air pollution. Toxicol Pathol. (2004) 32:650–8. doi: 10.1080/01926230490520232
78. Calderón-Garcidueñas L, Leray E, Heydarpour P, Torres-Jardón R, Reis J. Air pollution, a rising environmental risk factor for cognition, neuroinflammation and neurodegeneration: The clinical impact on children and beyond. Rev Neurol. (2016) 172:69–80. doi: 10.1016/j.neurol.2015.10.008
79. Calderón-Garcidueñas L, Torres-Jardón R, Kulesza RJ, Park S-B, D'Angiulli A. Air pollution and detrimental effects on children's brain. The need for a multidisciplinary approach to the issue complexity and challenges. Front Hum Neurosci. (2014) 8:613. doi: 10.3389/fnhum.2014.00613
80. Calderon-Garciduenas L, Reynoso-Robles R, Vargas-Martinez J, Gomez-Maqueo-Chew A, Perez-Guille B, Mukherjee PS, et al. Prefrontal white matter pathology in air pollution exposed Mexico City young urbanites and their potential impact on neurovascular unit dysfunction and the development of Alzheimer's disease. Environ Res. (2016) 146:404–17. doi: 10.1016/j.envres.2015.12.031
81. Hullmann M, Albrecht C, van Berlo D, Gerlofs-Nijland ME, Wahle T, Boots AW, et al. Diesel engine exhaust accelerates plaque formation in a mouse model of Alzheimer's disease. Part Fibre Toxicol. (2017) 14:35. doi: 10.1186/s12989-017-0213-5
82. Morgan TE, Davis DA, Iwata N, Tanner JA, Snyder D, Ning Z, et al. Glutamatergic neurons in rodent models respond to nanoscale particulate urban air pollutants in vivo and in vitro. Environ Health Perspect. (2011) 119:1003–9. doi: 10.1289/ehp.1002973
83. Dimakakou E, Johnston HJ, Streftaris G, Cherrie JW. Exposure to environmental and occupational particulate air pollution as a potential contributor to neurodegeneration and diabetes: a systematic review of epidemiological research. Int J Environ Res Public Health. (2018) 15:1704. doi: 10.3390/ijerph15081704
84. Ravi M, Paul E. Stroke mortality associated with living near main roads in england and wales. Stroke. (2003) 34:2776–80. doi: 10.1161/01.STR.0000101750.77547.11
85. Lim Y-H, Kim H, Kim JH, Bae S, Park HY, Hong Y-C. Air pollution and symptoms of depression in elderly adults. Environ Health Perspect. (2012) 120:1023–8. doi: 10.1289/ehp.1104100
86. Anisman H, Hayley S. Inflammatory factors contribute to depression and its comorbid conditions. Sci Signal. (2012) 5:pe45. doi: 10.1126/scisignal.2003579
87. Wei H, Feng Y, Liang F, Cheng W, Wu X, Zhou R, et al. Role of oxidative stress and DNA hydroxymethylation in the neurotoxicity of fine particulate matter. Toxicology. (2017) 380:94–103. doi: 10.1016/j.tox.2017.01.017
88. Dockery DW, Pope CA. Acute respiratory effects of particulate air pollution. Annu Rev Public Health. (1994) 15:107–32. doi: 10.1146/annurev.pu.15.050194.000543
89. Juha P, Annette P, Gerard H, Pekka T, Bert B, Jeroen de H, et al. Particulate air pollution and risk of ST-segment depression during repeated submaximal exercise tests among subjects with coronary heart disease. Circulation. (2002) 106:933–8. doi: 10.1161/01.CIR.0000027561.41736.3C
90. Graber M, Mohr S, Baptiste L, Duloquin G, Blanc-Labarre C, Mariet AS, et al. Air pollution and stroke. A new modifiable risk factor is in the air. Rev Neurol. (2019) 175:619–24. doi: 10.1016/j.neurol.2019.03.003
91. Sahathevan R, Brodtmann A, Donnan GA. Dementia, stroke, and vascular risk factors a review. Int J Stroke. (2012) 7:61–73. doi: 10.1111/j.1747-4949.2011.00731.x
92. Shalev D, Arbuckle MR. Metabolism and memory: obesity, diabetes, and dementia. Biol Psychiatry. (2017) 82:e81–3. doi: 10.1016/j.biopsych.2017.09.025
93. Baron AD, Steinberg HO, Chaker H, Leaming R, Johnson A, Brechtel G. Insulin-mediated skeletal muscle vasodilation contributes to both insulin sensitivity and responsiveness in lean humans. J Clin Invest. (1995) 96:786–92. doi: 10.1172/JCI118124
94. Gasparotto J, Chaves PR, da Boit Martinello K, Silva Oliveira LF, Gelain DP, Fonseca Moreira JC. Obesity associated with coal ash inhalation triggers systemic inflammation and oxidative damage in the hippocampus of rats. Food Chem Toxicol. (2019) 133:110766. doi: 10.1016/j.fct.2019.110766
95. D'Mello C, Le T, Swain MG. Cerebral microglia recruit monocytes into the brain in response to tumor necrosis factoralpha signaling during peripheral organ inflammation. J Neurosci. (2009) 18 29:2089–102. doi: 10.1523/JNEUROSCI.3567-08.2009
96. Calderon-Garcidueñas L, Osorno-Velazquez A, Bravo-Alvarez H, Delgado-Chavez R, Barrios-Marquez R. Histopathologic changes of the nasal mucosa in southwest Metropolitan Mexico City inhabitants. Am J Pathol. (1992) 140:225–32.
97. Sleeman KE, de Brito M, Etkind S, Nkhoma K, Guo P, Higginson IJ, et al. The escalating global burden of serious health-related suffering: projections to 2060 by world regions. age groups, and health conditions. Lancet GlobHealth. (2019) 7: e883–92. doi: 10.1016/S2214-109X(19)30172-X
98. Richard B, Chen H, Szyszkowicz M, Fann N, Hubbell B, Pope CA, Apte JS, et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc Natl Acad Sci USA. (2018) 115:9592–97. doi: 10.1073/pnas.1803222115
99. Gładka A, Rymaszewska J, Zatoński T. Impact of air pollution on depression and suicide. Int J Occup Med Environ Health. (2018) 31:711–721. doi: 10.13075/ijomeh.1896.01277
100. Kilian J, Kitazawa M. The emerging risk of exposure to air pollution on cognitive decline and Alzheimer's disease - Evidence from epidemiological and animal studies. Biomed J. (2018) 41:141–62. doi: 10.1016/j.bj.2018.06.001
101. Shou Y, Huang Y, Zhu X, Liu C, Hu Y, Wang H. A review of the possible associations between ambient PM2.5 exposures and the development of Alzheimer's disease. Ecotoxicol Environ Saf. (2019) 174:344–52. doi: 10.1016/j.ecoenv.2019.02.086
102. Calderon-Garciduenas L, Gonzalez-Maciel A, Reynoso-Robles R, Kulesza RJ, Mukherjee PS, Torres-Jardon R, et al. Alzheimer's disease and alpha-synuclein pathology in the olfactory bulbs of infants, children, teens and adults < /=40 years in Metropolitan Mexico City. APOE4 carriers at higher risk of suicide accelerate their olfactory bulb pathology. Environ Res. (2018) 166:348–62. doi: 10.1016/j.envres.2018.06.027
103. Villa N, Leticia C, Zilli V. Levels of Polonium-210 in brain and pulmonary tissues : Preliminary study in autopsies conducted in the city of Saõ Paulo, Brazil. Sci. Rep. (2020). 10:180. doi: 10.1289/isee.2020.virtual.P-0612
104. Calderón-Garcidueñas L, Mora-Tiscareño A, Franco-Lira M, Zhu H, Lu Z, Solorio E, et al. Decreases in short term memory, IQ, and altered brain metabolic ratios in urban Apolipoprotein ε4 children exposed to air pollution. J Alzheimers Dis. (2015) 45:757–70. doi: 10.3233/JAD-142685
105. Calderon-Garciduenas L, Serrano-Sierra A, Torres-Jardon R, Zhu H, Yuan Y, Smith D, et al. The impact of environmental metals in young urbanites' brains. Exp Toxicol Pathol. (2013) 65:503–11. doi: 10.1016/j.etp.2012.02.006
106. Burns J, Boogaard H, Polus S, Pfadenhauer LM, Rohwer AC, van Erp AM, et al. Interventions to reduce ambient air pollution and their effects on health: An abridged Cochrane systematic review. Environ Int. (2020) 135:105400. doi: 10.1016/j.envint.2019.105400
107. Riojas-Rodríguez H SdSA, Texcalac-Sangrador JL, Moreno-Banda GL. Air pollution management and control in Latin America and the Caribbean: implications for climate change. Rev Panam Salud Publica. (2016) 40:150–9. doi: 10.1289/isee.2016.4675
109. World Health Organization. Regional Office for Europe. (2006). Air quality guidelines: global update 2005: particulate matter, ozone, nitrogen dioxide and sulfur dioxide. World Health Organization. Regional Office for Europe. Available online at: https://apps.who.int/iris/handle/10665/107823
110. Mullins J, Bharadwaj P. Effects of Short-Term Measures to Curb Air Pollution: Evidence from Santiago, Chile. Am J Agric Econ. (2014) 97:1107–34. doi: 10.1093/ajae/aau081
111. Gramsch E, Le Nir G, Araya M, Rubio MA, Moreno F, Oyola P. Influence of large changes in public transportation (Transantiago) on the black carbon pollution near streets. Atmos Environ. (2013) 65:153–63. doi: 10.1016/j.atmosenv.2012.10.006
112. Gallego F, Montero J-P, Salas C. The effect of transport policies on car use: evidence from Latin American cities. J Public Econ. (2013) 107:47–62. doi: 10.1016/j.jpubeco.2013.08.007
113. Andrade MdF, Kumar P, de Freitas ED, Ynoue RY, Martins J, Martins LD, et al. Air quality in the megacity of São Paulo: evolution over the last 30 years and future perspectives. Atmos Environ. (2017) 159:66–82. doi: 10.1016/j.atmosenv.2017.03.051
114. Sisa I, Abeyá-Gilardon E, Fisberg RM, Jackson MD, Mangialavori GL, Sichieri R, et al. Impact of diet on CVD and diabetes mortality in Latin America and the Caribbean: a comparative risk assessment analysis. Public Health Nutr. (2020) 2016:2577–91. doi: 10.1017/S1368980020000646
115. GDB Results Tool 2021. University of Washington Institute of Health Metrics and Evaluation. (2021).
116. Barceló A, Aedo C, Rajpathak S, Robles S. The cost of diabetes in Latin America and the Caribbean. Bull World Health Organ. (2003) 81:19–27.
117. Diabetes TL. Obesity prevention in Latin America: Now is the time. Lancet Diabetes Endocrinol. (2014) 2:263. doi: 10.1016/S2213-8587(14)70079-8
Keywords: air pollution, particulate matter, dementia, Alzheimer, Latin America, low-and-middle income countries, developing countries
Citation: Santos NVd, Yariwake VY, Marques KdV, Veras MM and Fajersztajn L (2021) Air Pollution: A Neglected Risk Factor for Dementia in Latin America and the Caribbean. Front. Neurol. 12:684524. doi: 10.3389/fneur.2021.684524
Received: 23 March 2021; Accepted: 21 June 2021;
Published: 22 July 2021.
Edited by:
Agustin Ibanez, Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET), ArgentinaReviewed by:
Ju Yeon Kim, Soongsil University, South KoreaAhmed M. Sarki, Aga Khan University, Uganda
Octavio Jiménez-Garza, University of Guanajuato, Mexico
Copyright © 2021 Santos, Yariwake, Marques, Veras and Fajersztajn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nathália Villa dos Santos, bmF0aGF2aWxsaWFAZ21haWwuY29t