 Huiyuan Wang1,2
Huiyuan Wang1,2 Xinyi Chen
Xinyi Chen Yu Geng
Yu Geng- 1Department of Clinical Medicine, Bengbu Medical College, Bengbu, China
- 2Center for Rehabilitation Medicine, Department of Neurology, Zhejiang Provincial People's Hospital (Affiliated People's Hospital, Hangzhou Medical College), Hangzhou, China
Spiller syndrome is a rare subtype of medial medullary infarction (MMI). Herein, we report on a patient with progressing stroke who presented with the initial features of acute peripheral vestibulopathy and MMI (Spiller syndrome), as confirmed by magnetic resonance imaging (MRI). A 42-year-old man experienced acute persistent vertigo with nausea, vomiting, and severe gait instability for 6 h before presenting to the emergency department. He exhibited spontaneous right-beating horizontal-torsional nystagmus that intensified on rightward gaze. The patient fell to the left side during the Romberg test. Cranial computed tomography (CT) performed immediately upon admission did not provide evidence for ischemia or hemorrhage of the brainstem and cerebellum; however, the symptoms underwent exacerbation 4 h after admission, manifesting as left-sided limb weakness and dysarthria, without dysphagia. Furthermore, bedside examination revealed difficulty in extending the tongue to the right, positive left Babinski's sign, and abnormal vibration and position sense in the paralyzed limb. Head impulse test recording revealed a normal gain in the vestibulo-ocular reflex, and numerous consistent covert corrective saccades were captured upon turning the head to the left side. Cranial MRI depicted an acute infarct confined to the right side of the medial medulla, which met the diagnostic criteria for Spiller syndrome. Our study underscores the importance of considering the possibility of a nucleus prepositus hypoglossi lesion even if the signs and symptoms support the diagnosis of peripheral lesions in patients with acute vestibular syndrome exhibiting vascular risk factors.
1. Introduction
Spiller syndrome, a rare subtype of medial medullary infarction (MMI), is characterized by a triad of contralateral hemiparesis sparing the face, the contralateral loss of deep sensation, and ipsilateral hypoglossal paralysis (1, 2). Owing to the complexity and variability of the vascular supply to the medial medulla oblongata (3, 4), a typical triadic presentation of Spiller syndrome is uncommon (5–7).
Acute vestibular syndrome (AVS) manifests as recent-onset continuous vertigo, nausea, vomiting, motion intolerance, and gait instability lasting from days to weeks (8). Vestibular neuritis (9) is a common etiology of AVS. However, it also occurs in patients with stroke involving the cerebellum or brainstem, i.e., pseudo-vestibular neuritis (10, 11), which has rarely been reported in Spiller syndrome.
This case report describes a patient with progressing stroke who initially presented with the features of both acute peripheral vestibulopathy and MMI (Spiller syndrome), as confirmed by magnetic resonance imaging (MRI).
2. Case description
A 42-year-old man presented with acute persistent vertigo, concomitant with nausea, vomiting, and severe gait instability for 6 h prior to admission to the emergency department (ED). He denied experiencing headaches, neck pain, auditory symptoms, diplopia, dysphagia, dysarthria, and other focal neurological symptoms. He had a history of cerebral hemorrhage, hypertension for 7 years, and diabetes mellitus for 5 years. Physical examination revealed spontaneous right-beating horizontal-torsional nystagmus that became more prominent on rightward gaze (Supplementary Video 1). There were no corrective saccades on the bedside head impulse test (HIT), without head tilt or skew deviation (Supplementary Video 2). The patient fell to the left side during the Romberg test. The general physical and remaining neurological examinations yielded normal results. Cranial computed tomography (CT) performed immediately upon arrival to the ED did not provide any (imaging) evidence for ischemia or hemorrhage of the brainstem and cerebellum (Figure 1). However, CT revealed leftward conjugate ocular deviation upon closing the eyes (Figure 1B). Since the bedside HITs were normal, we considered this patient to have a “pseudo-vestibular neuritis” with central HINTS and administered pharmacotherapy for symptom relief.
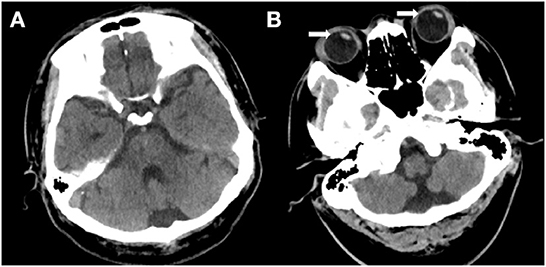
Figure 1. (A, B) Cranial computed tomography (CT) demonstrates no abnormality in the brain tissue. (B) A leftward conjugate ocular deviation is observed while the eyes are closed (white arrow).
Four hours following admission, the symptoms underwent exacerbation, manifesting as left-sided limb weakness and dysarthria, without dysphagia. A bedside examination revealed spontaneous right-beating nystagmus, difficulty in extending the tongue to the right, positive left Babinski's sign, and abnormal vibration and position sense in the paralyzed limb; nonetheless, the patient did not have pain and fever. Subsequently, he underwent cranial magnetic resonance imaging (MRI), which revealed an acute infarct confined to the right side of the medial medulla (Figures 2A–C). Cervical and cranial CT angiography revealed occlusion of the left vertebral artery at the V4 segment (Figure 2D). Furthermore, we recorded nystagmus using a video-oculography system (ICS Impulse, Otometrics, Denmark). The patient exhibited spontaneous right-beating nystagmus with a mean slow-phase velocity (SPV) of 7.7°/s, which decreased during visual fixation, with a mean SPV of 1.6°/s (Figure 3A). Nystagmus was identical to spontaneous nystagmus in all gaze directions but was more intense upon gazing to the right (Figure 3B). HIT recording using the ICS Impulse system revealed a normal gain in the vestibulo-ocular reflex (VOR) (0.99 for the right horizontal canal and 0.84 for the left horizontal canal; normal value >0.80), and numerous consistent covert corrective saccades were captured upon turning the head to the left side (Figure 3C). Echocardiography and electrocardiography did not provide any evidence for a cardiogenic etiology.
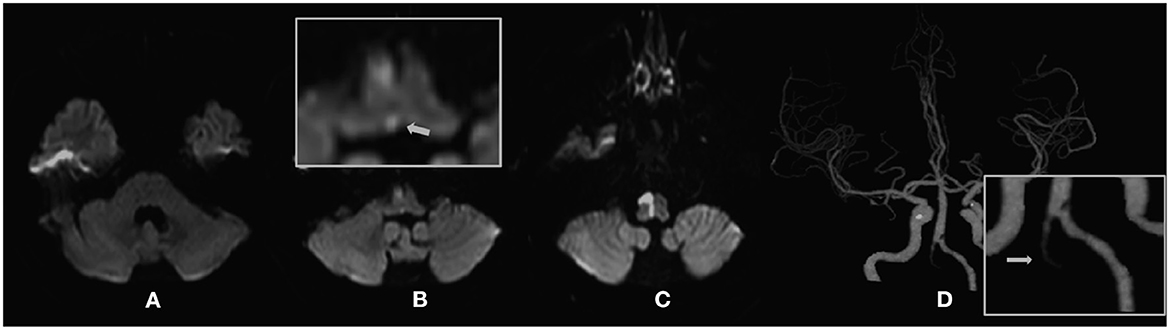
Figure 2. (A–C) Diffusion-weighted magnetic resonance imaging (DWI) of the patient. (A) No abnormal signal is observed in the vestibular nucleus of the pons. (B) Acute infarction in the medial medulla, which involves the nucleus prepositus hypoglossal (NPH) (white arrow). (D) Cranial computed tomography angiography (CTA) of the patient demonstrates total occlusion of the left intracranial vertebral artery (ICVA), which represents the offending vessel.

Figure 3. (A) Without visual fixation, the patient demonstrates spontaneous right-beating nystagmus with a linear nystagmus waveform and a mean slow-phase velocity (SPV) of 7.7°/s, which decreases during visual fixation, with a mean SPV of 1.6°/s. (B) Nystagmus in all gaze directions is similar with spontaneous nystagmus, and is more intense upon staring to the right. (C) Results of the video-oculography-based HIT (vHIT) (RHC, right horizontal semicircular canal; LHC, left horizontal semicircular canal). The vHIT results demonstrate numerous corrective saccades in the left horizontal semicircular canal, but the VOR gain is in the normal range, thereby suggesting damage in the central nervous system. vHIT examination of the bilateral anterior semicircular canal and posterior semicircular canal reveals no abnormality.
Following 1 week, the vestibular symptoms and nystagmus had largely disappeared, and the left limb weakness and deep sensory deficits had partially improved; however, he was still unable to walk independently.
3. Discussion
The patient presented with central unilateral paralysis of the hypoglossal nerve, contralateral limb hemiparesis, and deep sensory hemianopia; thus, the lesion was localized clinically to the sublingual nucleus, corticospinal tract, and medial tegmental tract. Moreover, cranial MRI revealed an acute cerebral infarct in the medial medulla, which met the diagnostic criteria for Spiller syndrome (1). The initial clinical symptoms and abnormal oculomotor signs presented a diagnostic challenge. This is because infarcts located at this anatomical site present only with symptoms of isolated acute vestibular damage commonly arising from the brainstem root entry zone, vestibular nucleus, or cerebellum (12), but not the medial medulla. Therefore, the functional and anatomical relationship between the signs and symptoms of vertigo and medullary infarction in this patient requires further explanation (12, 13).
Interestingly, HIT examinations of the patient demonstrated covert left corrective saccades at 4 days following onset. Furthermore, the gain in the VOR was still within the normal range at 4 days, which confirmed the presence of a clear central vestibular compensatory effect (13, 14), thus suggesting the symptoms of vertigo were closely related to the impairment of central vestibular function (11, 15–18). Fibers originating from the nucleus prepositus hypoglossi (NPH) near the dorsal midline of the medulla oblongata can affect contralateral vestibular function by inhibiting the pathway formed by the inferior olive–cerebellar lobule–vestibular nucleus on the contralateral side (12, 19, 20) (Figure 4). Therefore, damage to one side of the NPH leads to vestibular dysfunction on the side opposite to the lesion, vertigo symptoms resembling vestibular neuritis, spontaneous horizontal nystagmus, and vestibular ataxia (12, 20). Moreover, the fibers emanating from the NPH can affect the excitability of the contralateral paramedian pontine reticular formation (PPRF) by affecting the neural pathways between the ipsilateral cerebellar flocculus and fastigial nucleus. Damage to one side of the NPH leads to a decline in the inhibitory effect on the PPRF on the contralateral side, thus increasing excitability; furthermore, the patients may exhibit an ocular contrapulsion (Figure 1B) (21–23). Moreover, an NPH lesion reduces the inhibitory effect on the vestibular nucleus, thus contributing to the establishment of central compensatory function and shortening the duration of the vestibular symptoms.
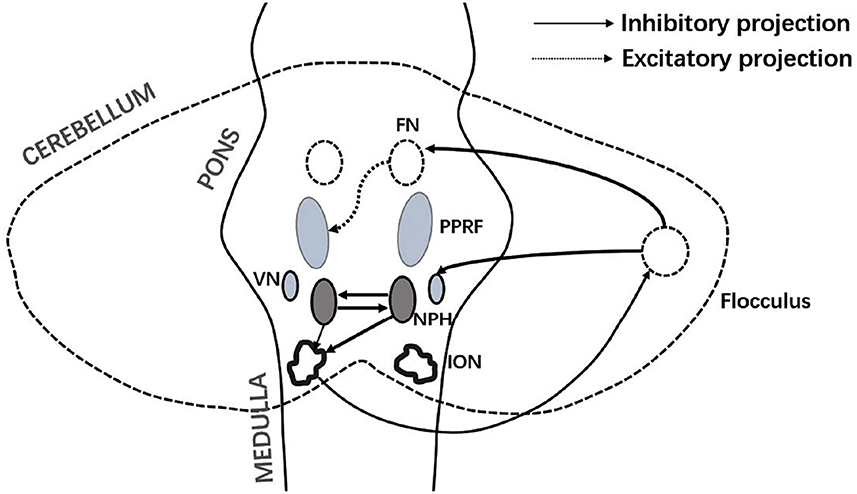
Figure 4. Connections between the NPH and vestibular-brainstem-cerebellar system. FN, fastigial nucleus; VN, vestibular nucleus; NPH, nucleus prepositus hypoglossal; PPRF, paramedian pontine reticular formation; and ION, inferior olivary nucleus. The ION principally accepts inhibitory fibers from the contralateral NPH. Damage to one side of the NPH excites the contralateral Purkinje fibers. The contralateral VN and cerebellar fastigial nucleus are suppressed, and the excitability of the contralateral PPRF increases.
4. Conclusion
This case report described a clinically rare case of progressive classic Spiller syndrome that initially mimicked vestibular neuritis. Clinicians unfamiliar with the NPH may require clarification about the correlation between the initial presentation of contralateral pseudovestibular neuritis to the lesion of this progressive stroke. This case report explains the anatomical site of the NPH and its pathophysiological mechanism in the vestibular-ocular movement pathway such that non-nerve-otology professionals can understand the pathogenesis and clinical manifestations of NPH-mediated “pseudovestibular neuritis.”
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
HW and YG mainly wrote this article. TS participated in the revision and provided valuable medical records and professional advice. All authors helped organize the case data and provided valuable advice. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.1072220/full#supplementary-material
References
1. Pergami P, Poloni TE, Imbesi F, Ceroni M, Simonetti F. Dejerine's syndrome or Spiller's syndrome? Neurol Sci. (2001) 22:333–6. doi: 10.1007/s10072-001-8178-3
2. Fukuoka T, Takeda H, Dembo T, Nagoya H, Kato Y, Deguchi I, et al. Clinical review of 37 patients with medullary infarction. J Stroke Cerebrovasc Dis. (2012) 21:594–9. doi: 10.1016/j.jstrokecerebrovasdis.2011.01.008
3. Tatu L, Moulin T, Bogousslavsky J, Duvernoy H. Arterial territories of human brain: brainstem and cerebellum. Neurology. (1996) 47:1125–35. doi: 10.1212/wnl.47.5.1125
4. Bassetti C, Bogousslavsky J, Mattle H, Bernasconi A. Medial medullary stroke: report of seven patients and review of the literature. Neurology. (1997) 48:882–90. doi: 10.1212/wnl.48.4.882
5. Pongmoragot J, Parthasarathy S, Selchen D, Saposnik G. Bilateral medial medullary infarction: a systematic review. J Stroke Cerebrovasc Dis. (2013) 22:775–80. doi: 10.1016/j.jstrokecerebrovasdis.2012.03.010
6. Kim JS, Han YS. Medial medullary infarction: clinical, imaging, and outcome study in 86 consecutive patients. Stroke. (2009) 40:3221–5. doi: 10.1161/STROKEAHA.109.559864
7. Akimoto T, Ogawa K, Morita A, Suzuki Y, Kamei S. Clinical study of 27 patients with medial medullary infarction. J Stroke Cerebrovasc Dis. (2017) 26:2223–31. doi: 10.1016/j.jstrokecerebrovasdis.2017.05.004
9. Jeong SH, Kim HJ, Kim JS. Vestibular neuritis. Semin Neurol. (2013) 33:185–94. doi: 10.1055/s-0033-1354598
10. Thömke F, Hopf HC. Pontine lesions mimicking acute peripheral vestibulopathy. J Neurol Neurosurg Psychiatry. (1999) 66:340–9. doi: 10.1136/jnnp.66.3.340
11. Tarnutzer AA, Berkowitz AL, Robinson KA, Hsieh YH, Newman-Toker DE. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ. (2011) 183:E571–92. doi: 10.1503/cmaj.100174
12. Seo SW, Shin HY, Kim SH, Han SW, Lee KY, Kim SM, et al. Vestibular imbalance associated with a lesion in the nucleus prepositus hypoglossi area. Arch Neurol. (2004) 61:1440–3. doi: 10.1001/archneur.61.9.1440
13. Tighilet B, Bordiga P, Cassel R, Chabbert C. Peripheral vestibular plasticity Vs Central compensation: evidence and questions. J Neurol. (2019) 266:27–32. doi: 10.1007/s00415-019-09388-9
14. Swamy Suman N, Kumar Rajasekaran A, Yuvaraj P, Pruthi N, Thennarasu K. Measure of central vestibular compensation: a review. J Int Adv Otol. (2022) 18:441–6. doi: 10.5152/iao.2022.21207
15. Strupp M, Bisdorff A, Furman J, Hornibrook J, Jahn K, Maire R, et al. Acute unilateral vestibulopathy/vestibular neuritis: diagnostic criteria. J Vestib Res. (2022) 32:389–406. doi: 10.3233/VES-220201
16. Newman-Toker DE, Kattah JC, Alvernia JE, Wang DZ. Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology. (2008) 70:2378–85. doi: 10.1212/01.wnl.0000314685.01433.0d
17. Mantokoudis G, Tehrani AS, Wozniak A, Eibenberger K, Kattah JC, Guede CI, et al. Vor gain by head impulse video-oculography differentiates acute vestibular neuritis from stroke. Otol Neurotol. (2015) 36:457–65. doi: 10.1097/mao.0000000000000638
18. Machner B, Erber K, Choi JH, Sprenger A, Helmchen C, Trillenberg P, et al. Simple gain-based evaluation of the video head impulse test reliably detects normal Vestibulo-Ocular Reflex indicative of stroke in patients with acute vestibular syndrome. Front Neurol. (2021) 12:741859. doi: 10.3389/fneur.2021.741859
19. Kim JS, Choi KD, Oh SY, Park SH, Han MK, Yoon BW, et al. Medial medullary infarction: abnormal ocular motor findings. Neurology. (2005) 65:1294–8. doi: 10.1212/01.wnl.0000180627.80595.10
20. Cho HJ, Choi HY, Kim YD, Seo SW, Heo JH. The clinical syndrome and etiological mechanism of infarction involving the nucleus prepositus hypoglossi. Cerebrovasc Dis. (2008) 26:178–83. doi: 10.1159/000145325
21. Kim SH, Zee DS, du Lac S, Kim HJ, Kim JS. Nucleus Prepositus Hypoglossi lesions produce a unique ocular motor syndrome. Neurology. (2016) 87:2026–33. doi: 10.1212/wnl.0000000000003316
22. Choi WY, Gold DR. Ocular motor and vestibular disorders in brainstem disease. J Clin Neurophysiol. (2019) 36:396–404. doi: 10.1097/WNP.0000000000000593
Keywords: Spiller syndrome, vestibular neuritis (VN), nucleus prepositus hypoglossal, ischemic stroke (IS), vertigo, nystagmus
Citation: Wang H, Shi T, Shang Y, Chen X, Xu J and Geng Y (2023) Case report: Spiller syndrome initially mimicking vestibular neuritis. Front. Neurol. 13:1072220. doi: 10.3389/fneur.2022.1072220
Received: 17 October 2022; Accepted: 14 December 2022;
Published: 09 January 2023.
Edited by:
Michael Strupp, Ludwig Maximilian University of Munich, GermanyReviewed by:
Jorge Kattah, University of Illinois at Chicago, United StatesSun-Uk Lee, Korea University Medical Center, Republic of Korea
Copyright © 2023 Wang, Shi, Shang, Chen, Xu and Geng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Geng,  Z2VuZ3l1QGhtYy5lZHUuY24=
Z2VuZ3l1QGhtYy5lZHUuY24=