 Philipp Balcerak
Philipp Balcerak Sydney Corbiere1
Sydney Corbiere1 Georg Kägi
Georg Kägi- 1Department of Neurology and Stroke Center, Cantonal Hospital St. Gallen, St. Gallen, Switzerland
- 2Department of Neurology, Inselspital, Bern University Hospital, and University of Bern, Bern, Switzerland
Purpose: Post-stroke dysphagia is an underdiagnosed but relevant complication, associated with worse outcome, dependency and quality of life of stroke survivors. Detailed mechanisms of post-stroke dysphagia are not very well understood, but established therapeutic concepts are needed. Different interventional studies have been published dealing with post-stroke dysphagia. This systematic review wants to collect and give an overview over the published evidence.
Methods: PubMed, Embase, Cochrane, CINAHL were searched for relevant interventional studies on post-stroke dysphagia in the (sub-)acute setting (within 3 months of stroke onset). The search has been filtered for randomized trials with an inactive control and the relevant data extracted.
Results: After initially finding 2,863 trials, finally 41 trials have been included. Seven different therapeutic concepts have been evaluated (Acupuncture, behavioral/physical therapy, drug therapy, neuromuscular electrical stimulation, pharyngeal electrical stimulation, transcranial direct current stimulation and repetitive transcranial magnetic stimulation). Studies of all modalities have shown some effect on post-stroke dysphagia with several studies raising concerns about the potential bias.
Conclusion: The amount and quality of studies are not enough to suggest certain therapies. Some therapeutical concepts (intensive physical therapy, transcranial magnetic stimulation, drug therapy) seem to be good potential therapeutic options, but further research is needed.
Introduction
The prevalence of dysphagia in stroke patients differs with the diagnostic method in the acute phase: 51–55% with clinical testing and 64–78% with instrumental examinations (1, 2). Impairment of swallowing still persists in up to 50% of the cases in the following course (1) and complications frequently arise. In about 40% of stroke survivors dysphagia is persistent. Patients with dysphagia have an increased risk for pneumonia which is probably linked with the severity of dysphagia since the risk is even much greater in patients with aspiration (2) and even more in patients with silent aspiration (3). Other common complications include malnutrition and dehydration, especially in the long-term (4). Malnourished and/or dehydrated stroke patients have a relevant risk of further complications and an elevated rate of mortality and dependency (5, 6). The detailed mechanisms of post-stroke dysphagia are not well understood.
Neuroanatomically different localisations of brain lesions, infra- and supratentorial, can cause dysphagia. As to frequency, brain stem lesions more often cause dysphagia compared to hemispheric strokes. Combined lesions have the highest risk for developing oropharyngeal dysphagia (7). Infratentorial lesions usually cause dysphagia through motor deficits whereas in supratentorial stroke dysphagia is usually caused by sensory-afferent deficits (8). Sensory deficits are more pronounced in dysphagic patients with aspiration.
Early recognition of the problem is linked with a better outcome. The Predictive Swallowing Score (PRESS) (9) has been developed to identify patients who are at risk for persistent dysphagia, so that treatment and potentially the placement of a percutanous enteral tube can be initiated at an early stage. Although clinical screening of dysphagia after stroke has been established routinely in several countries, instrumental screening is restricted in most. The latter has a higher diagnostic accuracy and allows a more detailed evaluation of the swallowing function, so that the problem and potentially the treatment can be adapted more specifically. FEES (10) (Flexible endoscopic evaluation of swallowing) and VFS (11) (Videofluoroscopy) are different in the procedure and in the results they provide, but allow an elaborated view of the deglutition function.
Therapeutic options comprise dietary and nutritional interventions, behavioral treatments, oral care, pharmacological- and neuro-stimulation.
Treatment guidelines contain different physical therapies and preventive measures to avoid dysphagia-associated complications, but lack medical or electrophysiological interventions to enhance dysphagia recovery after stroke in the acute or subacute setting.
The aim of this systematic review is to search the literature for published data on interventions for post-stroke dysphagia in the acute and subacute setting and to identify potential interventions and targets for further scientific research.
Methods
The PRISMA statement (12) (Preferred Reporting Items in Systematic reviews and Meta-Analyses) has been followed throughout the process.
Search Strategy and Selection Criteria
A systematic review of the literature was conducted to indentify all randomized cotrolled trials which assess the effect of therapeutic interventions of post-stroke dysphagia in the acute and subacute setting. The following databases were searched: Pubmed/MEDLINE, Embase, CENTRAL/Cochrane Library and The Cumulative Index to Nursing and Allied Health Literature (CINAHL). Search dates in all database were during August 2021 and consisted of the following searched terms: (*stroke* OR cerebrovascular* OR “brain ischemia”) AND (dysphagia* OR “deglutition disorder” OR “impaired swallowing” OR “swallowing disorder” OR “swallowing impairment”) AND (RCT OR placebo OR “randomized controlled trial” OR double-bIind OR placebo OR “controlled clinical trial”). If possible in the database, the search was filtered using “human” and “English language”.
The reference lists of the screened articles were searched for articles which have not been included in the original search.
Inclusions and Exclusions
All studies were included who were interventional trials about post-stroke dysphagia with a randomized controlled design. After the above-mentioned literature search duplicates were removed and titles and abstracts screened for the eligibility criteria. Here, the PICO concept has been followed. The control arm had to be an inactive comparator with all possible interventions (medication, electrical stimulation, physical therapy, etc.) included, while usual care or standard therapy were counted as eligible for this review. Dysphagia had to be assessed clinically or instrumentally prior to the start of treatment.
The treatment had to be started within 3 months after ischemic stroke. Inclusion was restricted to studies examining interventions aiming to improve mechanisms of the impaired swallowing function are examined, so that trials assessing preventive measures i.e., prophylactic antibiotic treatment or measures trying to prevent dysphagia associated complications were not included here.
Only original data/publications have been included. Comments, case series, reviews etc. were excluded, latest at full-text-screening. Literature dealing with dysphagia due to other cause than stroke or healthy individuals and their swallowing function were not included. Full-text articles in English had to be available to be included in this review.
If treatment was started after 3 months after stroke or this relevant information is missing in the data, the publication was not included. Outcome or safety outcome parameters were not part of the inclusion criteria, although publications were excluded if they did not provide dysphagia- or swallowing-specific outcomes, whereas the methodology of obtaining those (clinical, instrumental/paraclinical) was not of interest at that stage of the process. A scaling of the global swallowing function had to be provided as any outcome parameter, where all scores (already established or explained in the publication) were accepted. Studies dealing only with parts of the swallowing act i.e., only the oral transit time, were not included.
Data Extraction
One reviewer (PB) performed the database search while two reviewers (PB, RZ) performed the screening. After removal of duplications, a title and abstract assessment was performed in a first step which was followed by a full-text screening. In case of divergent assessments, a consensus was found.
Data of the included papers were extracted into a pre-formed electronic sheet and then the trials were assessed by two reviewers (PB, SC). The data extraction followed the PICO approach: (1) Participants–stroke patients with dysphagia, (2) Interventions–any active intervention/therapy with or without the combination of conventional routine therapy, (3) Comparison–any inactive control/placebo, (4) Outcome–swallowing functions, measured instrumentally and clinically, and complications (if available). The risk of bias of every trial included was assessed according the Cochrane's Handbook with the RoB-2-tool (13). The tool was used according to the guidelines. Risk grades were high risk (+), low risk (-) and unclear risk or some concern were put together (o). The overall assessment was performed according to RoB-2-algorithm.
In case of conflicting results, a consensus was found.
Results
Literature Retrieved
The search strategy was applied and resulted in 1,367 hits with 479 duplicates, leaving 888 citations. After screening the title and abstracts 169 publications seemed eligible. After exclusion of 30 papers, which were not available in English and full-text screening for the above-mentioned eligibility criteria 41 trials were included in the review. The reasons for exclusion are mentioned after grouping in Figure 1.
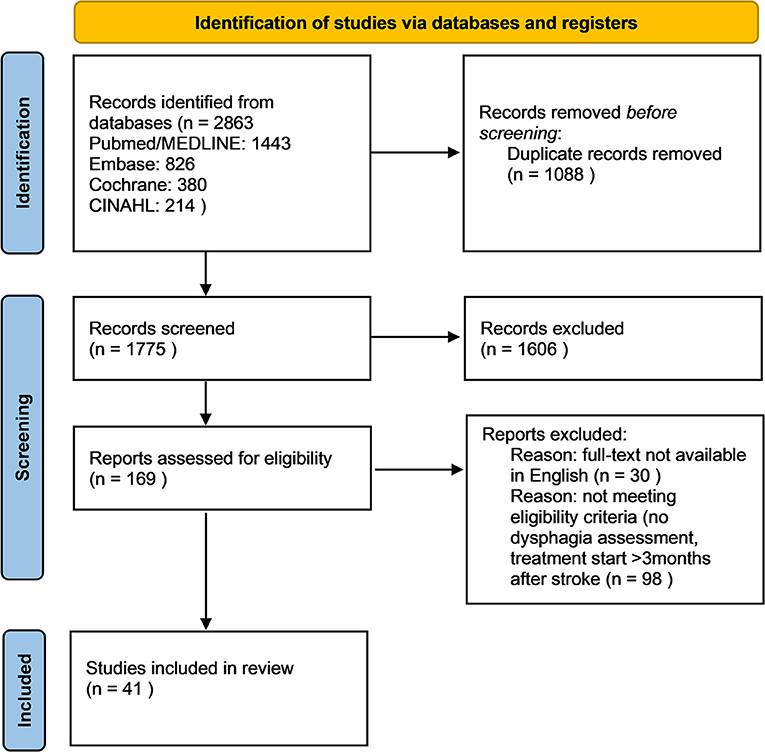
Figure 1. Flow diagram on literature retrieval.
Interventions
Seven different interventional modalities have been evaluated in the trials: acupuncture in two trials, behavioral/physical therapy in 13, drug therapy in five, neuromuscular electrical stimulation (NMES) in nine, pharyngeal electrical stimulation (PES) in four, transcranial direct current stimulation (tDCS) in four and six studies assessed repetitive transcranial magnetic stimulation (two studies assessed two modalities in a three-arm design).
The start of the interventions complied with our eligibility criteria and was started within 3 months after stroke onset.
Outcome Measures
All of the included trials had a swallowing assessment as an outcome parameter, as mentioned in the eligibility criteria. Thirty-three trials used instrumental evaluations of dysphagia as outcome assessments. For the instrumental assessments, the flexible endoscopic evaluation of swallowing (FEES) was performed in three trials, whereas videofluoroscopy (VFS) was used in 30. During both procedures different scores and scales were obtained to assess the swallowing function. Twenty-three of the included studies had clinical examinations as outcome assessments of dysphagia with different scores and scales used for the evaluation.
Summary of Results
Forty-one trials dealing with seven different therapeutic concepts were included in this review and provided results on their effect on dysphagia recovery after stroke with a total of 2,166 participants included in these studies. Table 1 shows the study characteristics from extracted data and its findings of the single studies (Further information can be found in the Supplementary Material).
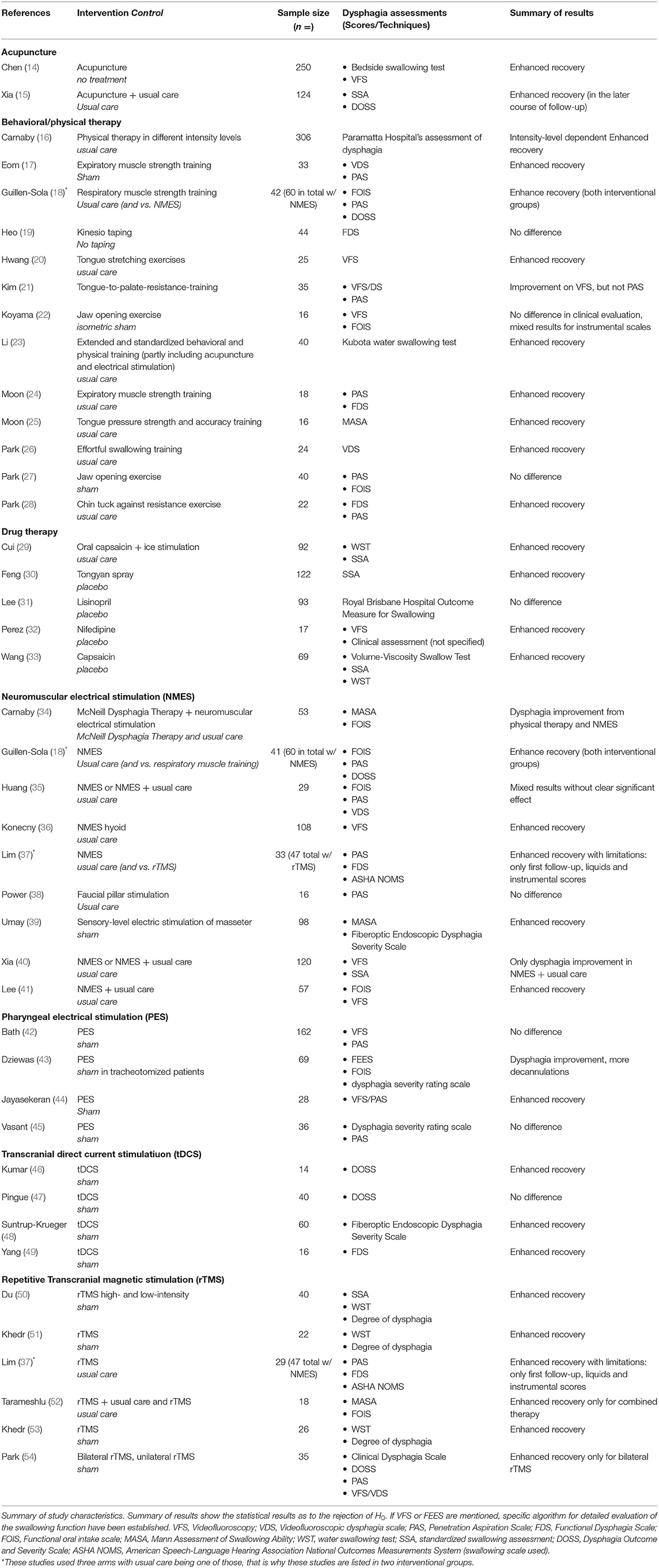
Table 1. Summary of results.
Acupuncture
Two studies (14, 15) were included which compared Acupuncture vs. no specific therapy or standard care. In one study (14), patients with hemiplegic stroke were included with swallowing outcome on instrumental testing (videofluoroscopy) as a secondary endpoint, so that only a subgroup of the initial sample size was included. Acupuncture showed some effect on post stroke dysphagia within the first 7 weeks after stroke onset. In the other trial (15), the intervention showed some effect, but only in the later course of the trial, which lasted only 4 weeks.
Behavioral/Physical Therapies
Thirteen trials (16–28) have been included which assess the impact physical training and/or the intensity (15, 19) of physical therapy on dysphagia recovery. Three studies (17, 18, 24) evaluated forced respiratory muscle training against resistance and its effect on post-stroke dysphagia, where all could show enhanced dysphagia recovery. Among the other trials, two of them assess jaw opening exercises (22, 27), while the other concepts had similar aspects, but different maneuvers used in their studies (for details see Table 1, or Supplementary Material). The assessments differed within the studies, so that three trials (16, 23, 25) only used clinical measurements for dysphagia evaluation. In total, nine trials showed positive impact of the therapies on dysphagia recovery, whereas two (19, 27) did not show any difference and two other (21, 22) showed mixed results in different dysphagia assessments. Out of the nine studies showing positive impact, two (20, 26) only had impact on the oral phase of the swallowing act.
Drug Therapy
Four different medication classes have been assessed as to their effect on dysphagia rehabilitation. Caspaicin was used in two trials (29, 33), nifedipine (32), lisinopril (31) and tongyan spray (30) in one each. All studies except lisinopril showed significant differences as to recovery of the swallowing function.
Neuromuscular Electrical Stimulation
In the big majority of included trials (18, 34–41), a therapeutical effect on post-stroke dysphagia could have been shown, with one (35) having mixed results and one (38) showing no difference, though. Five of the studies (18, 34, 35, 40, 41) assessed the addition of NMES to standard or physical therapy. The combination of NMES and standard therapy has been shown to be more effective than NMES alone in the comparative studies. Whereas, most studies used stimulation of hyoid muscles, two (38, 39) used different stimulation locations. The stimulation of faucial pillars (38) failed to show a significant improvement over standard therapy. The sensory-level stimulation of the masseter muscle (39) seems to have a bigger benefit over standard care on dysphagia recovery.
Pharyngeal Electrical Stimulation
Of the four studies (42–45) in this review, two (43, 44) reached the study goal and showed a positive effect on post-stroke dysphagia. One study (43) included was in a further specified study population with stroke survivors needing tracheotomy.
Transcranial Direct Current Stimulation
In this modality group, all trials (46–49) used instrumental dysphagia assessments, but not structured clinical scales. All of them used sham procedures as control groups, but had different concepts of stimulation. Two studies (46, 48) implemented anodal tDCS over the unaffected hemisphere, one study (49) used anodal tDCS over the affected motor cortex and all achieved to show a positive effect. The other trial (47) had a dual concept with anodal stimulation over the lesioned and cathodal over the contralesional side. This failed to show an enhanced dysphagia rehabilitation.
Repetitive Transcranial Magnetic Stimulation
All of the six included trials (37, 50–54) showed at least some therapeutic effect of rTMS on post-stroke dysphagia. The concept of applying the stimulation over the affected motor cortex using the hotspotting technique was similar in the included trials. The frequency varied between 1 Hz up to 10 Hz. Tarameshlu (52) used three groups with one rTMS alone, rTMS and standard therapy combined and standard therapy only as the control, where only the combined therapy showed a significant effect. Park (54) compared bi- and unilateral TMS to a sham procedure where only the bilateral stimulation showed a significant effect.
Risk of Bias
Every trial was evaluated for risk of bias applying the RoB-2-tool. The results can be found in Table 2 grouped by interventions performed in the trials. Since mentioned in the inclusion criteria, all studies were randomized and were compared to an inactive control group.
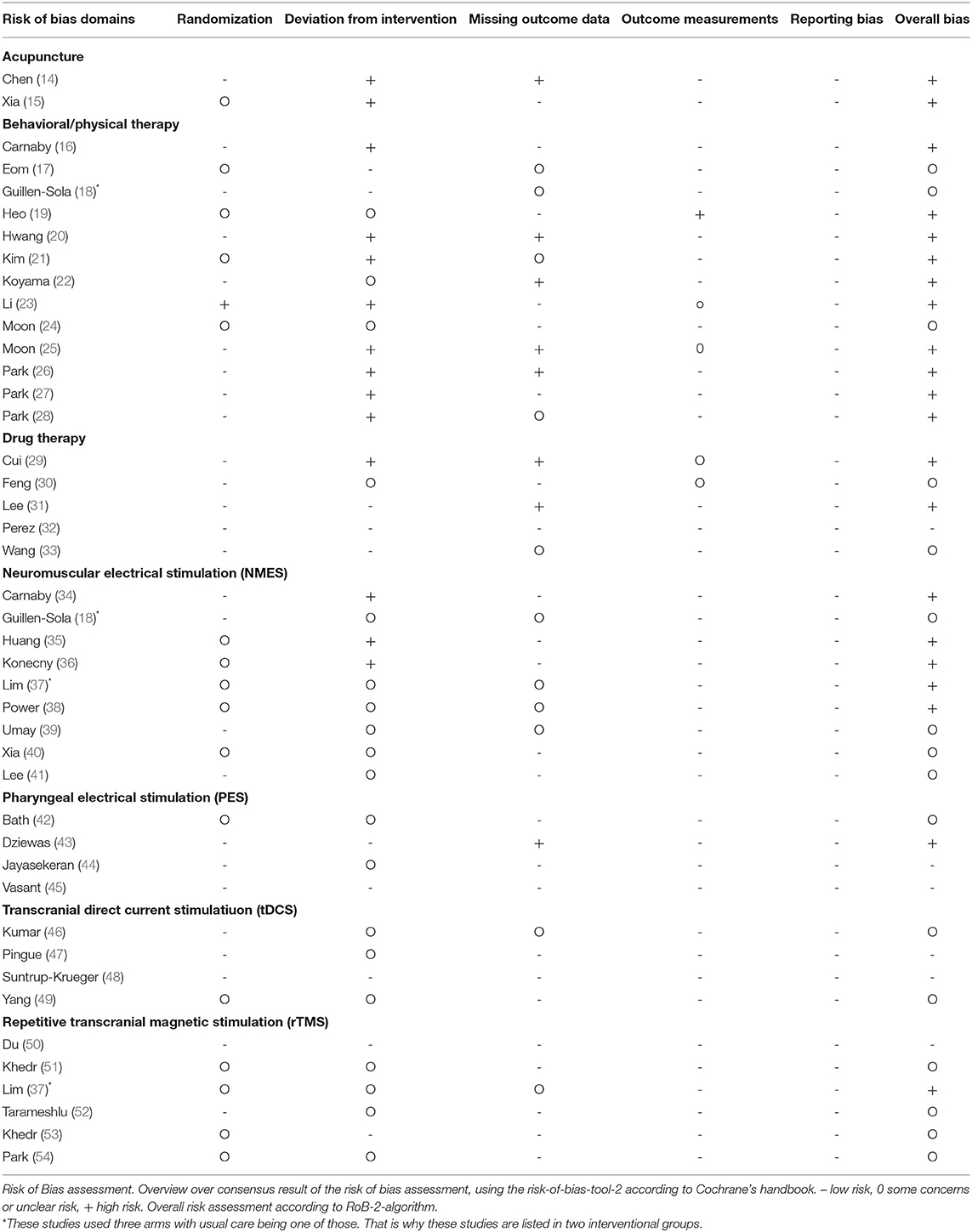
Table 2. Summary of risk of bias assessment.
Overall, in several studies data for the assessment of bias was missing, so that the risk of bias could not be assessed properly (graded as 0 = some concerns / unclear bias). Other studies were evaluated as high risk (+) of bias which was majorly in the blinding (of the therapy and the outcome assessments) as well as the allocation or randomization process. Some studies were missing relevant outcome data. No relevant concerns were raised as to the reporting bias. Overall bias was performed according to the RoB-2-algorithms with an overall high risk with one domain being at high risk and low risk with all domains being at low risk. Results in between were evaluated according to the assessors' judgement.
All of the studies assessing behavioral or physical therapy and NMES were assessed overall as at least “some concerns”, with a vast majority due to concerns as to the deviation from intervention, to a major part because of blinding issues. The PES and tDCS group of trials were the only ones with the a relevant part of studies being assessed as low-risk (Detailed results in Table 2).
Discussion
This systematic review gives an overview over the RCTs in the field of therapeutic interventions for post-stroke dysphagia. In this review, especially the (sub-)acute phase was of interest, so that only trials assessing therapeutic modalities, which have started within 3 months after stroke were included.
In total, 41 RCTs were included with seven different therapeutic concepts.
As to acupuncture, two studies were included, which showed an effect on post-stroke dysphagia. It has to be mentioned, though, that in one study (14), only a subgroup of these 250 participants received distinct dysphagia assessments and were therefore included in the statistical analyses. Together with the high risk of bias for both acupuncture studies, results of the study have to be interpreted cautiously. Having this in mind the European guidelines (55) give a weak recommendation that acupuncture may be used in the rehabilitation of swallowing function.
Most studies assess behavioral and physical options, but are at high risk of bias, so that conclusions cannot be made based on these results definitively. Additionally, most studies examine similar, but different kind of therapeutic maneuvers. It seems that the intensity of swallowing therapy has a positive effect on dysphagia recovery and should be a safe procedure. As to the specification of therapy, this review cannot give a clear answer. Respiratory muscle strength training seems to give a positive effect on post-stroke dysphagia based on the three studies (17, 18, 24) in this review. Otherwise, different kind of tongue strengthening interventions were observed with mixed result as to oropharyngeal dysphagia, since some showed only effect on the oral phase (without effect on the pharyngeal phase). Some studies only used clinical scores which are known to be less sensitive than instrumental ones. Jaw opening exercises failed to show an effect (for details see Table 1 or Supplementary Material). If any, respiratory muscle strength training seem to be safe and potentially beneficial choice, but due to the high risk of bias the evidence has to be improved in this area. Nevertheless, a patient tailored behavioral therapy can be recommended.
As yet, no concept of drug therapy has been established, so that four different drug classes have been used. The mechanisms and concepts of drug therapy in the context of post stroke dysphagia mainly goes into the direction of increasing pharyngeal levels of substance P. This can be achieved by stimulating TRPV1 and TRPM8 (56, 57) agonists. Even ACE inhibitors are also believed to increase substance P (58). All drugs except Lisinopril have shown promising results with most of them leading to concerns about the risk of bias. Due to the lack of large clinical trials and systematic instrumental dysphagia assessments, Nifedipine and Capsaicin (TRPV1 agonist) are substances of interest but can't be recommended for clinical routine so far. Nevertheless, further studies with these substances to evaluate their clinical impact on clinical outcome measures in stroke patients are needed and should be performed.
The majority of studies about neurostimulation techniques in dysphagia are superficial stimulation (NMES), tDCS, rTMS and PES. The latter three endeavor to change neuroplasticity of specific brain areas. In theory, this can include facilitation of a lesioned brain region or facilitation of healthy brain areas. In case of post stroke dysphagia, the interventions have the goal to facilitate brain regions involved in swallowing through increasing synaptic efficiency and cortical reorganization. Functional imaging studies (59, 60) succeeded to show that the primary motor cortex seems to play a major role in the act of volitional swallowing and can be associated with post-stroke dysphagia (61).
The studies about tDCS in the rehabilitation of post stroke dysphagia can't be specified further as to the localization and mode of stimulation. Two out of the four studies used the anodal stimulation over the unaffected hemisphere and did show some effect. Another one stimulated the affected side and showed improved swallowing rehabilitation, too. The other study used a dual stimulation concept without the proof of benefit. These concepts have to be confirmed in further studies given the very low number of RCTs included in this review.
Studies investigating rTMS in the rehabilitation of post stroke dysphagia show also a fair methodological quality leading to some concerns of bias. All show some effect on post-stroke dysphagia. It does not come as a surprise that the trials with combined rTMS and standard therapy have better effects, neither that bilateral stimulation seems to have a more pronounced therapeutical impact. Different aspects of the swallowing function seem to be represented in different hemispheres and different parts of those (62). Furthermore, studies with instrumental and clinical testing of dysphagia assessment are broadly lacking because most of those included in this review have used either clinical or instrumental dysphagia assessments only.
The studies assessing PES are of comparably low risk of bias, but only two did show some effect on post-stroke dysphagia. This effect was only seen in one study in a subgroup of tracheotomized stroke survivors, which seemed to profit from the stimulation therapy.
The trials on neurostimulation all show some methodological weaknesses, leading to concerns about the risk of bias. Some effect, especially in combination with standard therapy or additional physical therapy has been shown and is promising. Nevertheless, this has to be proven in further high-quality research with clinical endpoints. The ESO guidelines (55) give a weak recommendation on the adjunct use of neurostimulation in post stroke dysphagia.
This review covers most of the relevant databases. The search strategy is quite selective due to restricting to RCT with inactive controls, allowing only interventions targeting the swallowing function and therefore leaving out preventive, dietary or nutritional measures. The selected start of the intervention within 3 months of stroke focused on the acute/subacute phase. Therefore, there could be a lack of some therapeutic concepts for post-stroke dysphagia, but we believe that it gives a comprehensive overview over the existing publications of RCT in order to help to enhance further scientific research and develop therapies.
It becomes clear, that the field of dysphagia needs more research to establish therapeutic guidelines. According to the findings above it seems safe and reasonable to say that an intensive swallowing or respiratory muscle strength therapy should be applied with rTMS and some drug candidates as potential future options for additional therapeutical concepts. It has to be stated that main outcome measurements for primary endpoints should be instrumental in addition to clinical ones, whenever feasible.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This work was supported from internal resources of the Department of Neurology and Stroke Center, Cantonal Hospital St. Gallen, St. Gallen, Switzerland.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.823189/full#supplementary-material
References
1. Mann G, Hankey GJ, Cameron D. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. (1999) 30:744–8. doi: 10.1161/01.STR.30.4.744
2. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke. (2005) 36:2756–63. doi: 10.1161/01.STR.0000190056.76543.eb
3. Nakajoh K, Nakagawa T, Sekizawa K, Matsui T, Arai H, Sasaki H. Relation between incidence of pneumonia and protective reflexes in post-stroke patients with oral or tube feeding. J Intern Med. (2000) 247:39–42. doi: 10.1046/j.1365-2796.2000.00565.x
4. Foley NC, Martin RE, Salter KL, Teasell RW. A review of the relationship between dysphagia and malnutrition following stroke. J Rehabil Med. (2009) 41:707–13. doi: 10.2340/16501977-0415
5. Dávalos A, Ricart W, Gonzalez-Huix F, Soler S, Marrugat J, Molins A, et al. Effect of malnutrition after acute stroke on clinical outcome. Stroke. (1996) 27:1028–32. doi: 10.1161/01.STR.27.6.1028
6. FOOD Trial Collaboration. Poor nutritional status on admission predicts poor outcomes after stroke: observational data from the FOOD trial. Stroke. (2003) 34:1450–6. doi: 10.1161/01.STR.0000074037.49197.8C
7. Horner J, Buoyer FG, Alberts MJ, Helms MJ. Dysphagia following brain-stem stroke. Clinical correlates and outcome. Arch Neurol. (1991) 48:1170–3. doi: 10.1001/archneur.1991.00530230078026
8. González-Fernández M, Ottenstein L, Atanelov L, Christian AB. Dysphagia after stroke: an overview. Curr Phys Med Rehabil Rep. (2013) 1:187–96. doi: 10.1007/s40141-013-0017-y
9. Galovic M, Stauber AJ, Leisi N, Krammer W, Brugger F, Vehoff J, et al. Development and Validation of a prognostic model of swallowing recovery and enteral tube feeding after ischemic stroke. JAMA Neurol. (2019) 76:561–70. doi: 10.1001/jamaneurol.2018.4858
10. Langmore SE, Schatz K, Olsen N. Fiberoptic endoscopic examination of swallowing safety: a new procedure. Dysphagia. (1988) 2:216–9. doi: 10.1007/BF02414429
11. Logemann JA. Manual for the Videofluoroscopic Study of Swallowing. 2nd Edition Austin, Texas: PRO-ED (1993).
12. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
13. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
14. Chen L, Fang J, Ma R, Gu X, Chen L, Li J, et al. Additional effects of acupuncture on early comprehensive rehabilitation in patients with mild to moderate acute ischemic stroke: a multicenter randomized controlled trial. BMC Complement Altern Med. (2016) 16:226. doi: 10.1186/s12906-016-1193-y
15. Xia W, Zheng C, Zhu S, Tang Z. Does the addition of specific acupuncture to standard swallowing training improve outcomes in patients with dysphagia after stroke? A randomized controlled trial. Clin Rehabil. (2016) 30:237–46. doi: 10.1177/0269215515578698
16. Carnaby G, Hankey GJ, Pizzi J. Behavioural intervention for dysphagia in acute stroke: a randomised controlled trial. Lancet Neurol Januar. (2006) 5:31–7. doi: 10.1016/S1474-4422(05)70252-0
17. Eom MJ, Chang MY, Oh DH, Kim HD, Han NM, Park JS. Effects of resistance expiratory muscle strength training in elderly patients with dysphagic. stroke. (2017) 41:747–52. doi: 10.3233/NRE-172192
18. Guillén-Solà A, Messagi Sartor M, Bofill Soler N, Duarte E, Barrera MC, Marco E. Respiratory muscle strength training and neuromuscular electrical stimulation in subacute dysphagic stroke patients: a randomized controlled trial. Clin Rehabil. (2017) 31:761–71. doi: 10.1177/0269215516652446
19. Heo SY, Kim KM. Immediate effects of kinesio taping on the movement of the hyoid bone and epiglottis during swallowing by stroke patients with dysphagia. J Phys Ther Sci. (2015) 27:3355–7. doi: 10.1589/jpts.27.3355
20. Hwang N-K, Kim H-H, Shim J-M, Park J-S. Tongue stretching exercises improve tongue motility and oromotor function in patients with dysphagia after stroke: a preliminary randomized controlled trial. Arch Oral Biol. (2019) 108:104521. doi: 10.1016/j.archoralbio.2019.104521
21. Kim HD, Choi JB, Yoo SJ, Chang MY, Lee SW, Park JS. Tongue-to-palate resistance training improves tongue strength and oropharyngeal swallowing function in subacute stroke survivors with dysphagia. J Oral Rehabil Januar. (2017) 44:59–64. doi: 10.1111/joor.12461
22. Koyama Y, Sugimoto A, Hamano T, Kasahara T, Toyokura M, Masakado Y. Proposal for a modified jaw opening exercise for dysphagia: a randomized, controlled trial. Tokai J Exp Clin Med. (2017) 42:71–8.
23. Li W, Kang X, Ren J-L, Lai X-Z, Tai L-W. Effects of extended in-patient treatment training on outcome of post-stroke dysphagia. Eur Rev Med Pharmacol Sci. (2017) 21:5711–6. doi: 10.26355/eurrev_201712_14017
24. Moon JH, Jung JH, Won YS, Cho HY, Cho K. Effects of expiratory muscle strength training on swallowing function in acute stroke patients with dysphagia. J Phys Ther Sci. (2017) 29:609–12. doi: 10.1589/jpts.29.609
25. Moon J-H, Hahm S-C, Won YS, Cho H-Y. The effects of tongue pressure strength and accuracy training on tongue pressure strength, swallowing function, and quality of life in subacute stroke patients with dysphagia: a preliminary randomized clinical trial. Int J Rehabil Res. 41:204–10. doi: 10.1097/MRR.0000000000000282
26. Park H-S, Oh D-H, Yoon T, Park J-S. Effect of effortful swallowing training on tongue strength and oropharyngeal swallowing function in stroke patients with dysphagia: a double-blind, randomized controlled trial. Int J Lang Commun Disord. (2019) 54:479–84. doi: 10.1111/1460-6984.12453
27. Park J-S, An D-H, Kam K-Y, Yoon T, Kim T, Chang M-Y. Effects of resistive jaw opening exercise in stroke patients with dysphagia: a double- blind, randomized controlled study. J Back Musculoskelet Rehabil. (2020) 33:507–13. doi: 10.3233/BMR-181477
28. Park J-S, An D-H, Oh D-H, Chang M-Y. Effect of chin tuck against resistance exercise on patients with dysphagia following stroke: a randomized pilot study. Neuro Rehabilitation. (2018) 42:191–7. doi: 10.3233/NRE-172250
29. Cui F, Yin Q, Wu C, Shen M, Zhang Y, Ma C, et al. Capsaicin combined with ice stimulation improves swallowing function in patients with dysphagia after stroke: a randomised controlled trial. J Oral Rehabil. (2020) 47:1297–303. doi: 10.1111/joor.13068
30. Feng X, Hao W, Ding Z, Sui Q, Guo H, Fu J. Clinical study on tongyan spray for post-stroke dysphagia patients: a randomized controlled trial. Chin J Integr Med. (2012) 18:345–9. doi: 10.1007/s11655-012-1140-9
31. Lee JS, Chui PY, Ma HM, Auyeung TW, Kng C, Law T, et al. Does low dose angiotensin converting enzyme inhibitor prevent pneumonia in older people with neurologic dysphagia–a randomized placebo-controlled trial. J Am Med Dir Assoc. 16:702–7. doi: 10.1016/j.jamda.2015.05.009
32. Perez I, Smithard DG, Davies H, Kalra L. Pharmacological treatment of dysphagia in stroke. Dysphagia. (1998) 13:12–6. doi: 10.1007/PL00009543
33. Wang Z, Wu L, Fang Q, Shen M, Zhang L, Liu X. Effects of capsaicin on swallowing function in stroke patients with dysphagia: a randomized controlled trial. J Stroke Cerebrovasc Dis. (2019) 28:1744–51. doi: 10.1016/j.jstrokecerebrovasdis.2019.02.008
34. Carnaby GD, LaGorio L, Silliman S, Crary M. Exercise-based swallowing intervention (McNeill Dysphagia Therapy) with adjunctive NMES to treat dysphagia post-stroke: A double-blind placebo-controlled trial. J Oral Rehabil. 47:501–10. doi: 10.1111/joor.12928
35. Huang K-L, Liu T-Y, Huang Y-C, Leong C-P, Lin W-C, Pong Y-P. Functional outcome in acute stroke patients with oropharyngeal Dysphagia after swallowing therapy. J Stroke Cerebrovasc Dis. (2014) 23:2547–53. doi: 10.1016/j.jstrokecerebrovasdis.2014.05.031
36. Konecny P, Elfmark M. Electrical stimulation of hyoid muscles in post-stroke dysphagia. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2018) 162:40–2. doi: 10.5507/bp.2017.043
37. Lim KB, Lee HJ, Yoo J, Kwon YG. Effect of low-frequency rTMS and NMES on subacute unilateral hemispheric stroke with dysphagia. Ann Rehabil Med. (2014) 38:592–602. doi: 10.5535/arm.2014.38.5.592
38. Power ML, Fraser CH, Hobson A, Singh S, Tyrrell P, Nicholson DA, et al. Evaluating oral stimulation as a treatment for dysphagia after stroke. Dysphagia. (2006) 21:49–55. doi: 10.1007/s00455-005-9009-0
39. Umay EK, Yaylaci A, Saylam G, Gundogdu I, Gurcay E, Akcapinar D, et al. The effect of sensory level electrical stimulation of the masseter muscle in early stroke patients with dysphagia: a randomized controlled study. Neurol India. (2017) 65:734–42. doi: 10.4103/neuroindia.NI_377_16
40. Xia W, Zheng C, Lei Q, Tang Z, Hua Q, Zhang Y, et al. Treatment of post-stroke dysphagia by vitalstim therapy coupled with conventional swallowing training. J Huazhong Univ Sci Technolog Med Sci. (2011) 31:73–6. doi: 10.1007/s11596-011-0153-5
41. Lee KW, Kim SB, Lee JH, Lee SJ, Ri JW, Park JG. The effect of early neuromuscular electrical stimulation therapy in acute/subacute ischemic stroke patients with Dysphagia. Ann Rehabil Med. (2014) 38:153–9. doi: 10.5535/arm.2014.38.2.153
42. Bath PM, Scutt P, Love J, Clavé P, Cohen D, Dziewas R, et al. Pharyngeal electrical stimulation for treatment of dysphagia in subacute stroke: a randomized controlled trial. Stroke. (2016) 47:1562–70. doi: 10.1161/STROKEAHA.115.012455
43. Dziewas R, Stellato R, van der Tweel I, Walther E, Werner CJ, Braun T, et al. Pharyngeal electrical stimulation for early decannulation in tracheotomised patients with neurogenic dysphagia after stroke (PHAST-TRAC): a prospective, single-blinded, randomised trial. Lancet Neurol. (2018) 17:849–59. doi: 10.1016/S1474-4422(18)30255-2
44. Jayasekeran V, Singh S, Tyrrell P, Michou E, Jefferson S, Mistry S, et al. Adjunctive functional pharyngeal electrical stimulation reverses swallowing disability after brain lesions. Gastroenterology. (2010) 138:1737–46. doi: 10.1053/j.gastro.2010.01.052
45. Vasant DH, Michou E, O'Leary N, Vail A, Mistry S, Hamdy S. Greater Manchester Stroke Research Network. Pharyngeal electrical stimulation in dysphagia poststroke: a prospective, randomized single-blinded interventional study. Neurorehabil Neural Repair. (2016) 30:866–75. doi: 10.1177/1545968316639129
46. Kumar S, Wagner CW, Frayne C, Zhu L, Selim M, Feng W, et al. Noninvasive brain stimulation may improve stroke-related dysphagia: a pilot study. Stroke. 42:1035–40. doi: 10.1161/STROKEAHA.110.602128
47. Pingue V, Priori A, Malovini A, Pistarini C. Dual transcranial direct current stimulation for poststroke dysphagia: a randomized controlled trial. Neurorehabil Neural Repair. (2018) 32:635–44. doi: 10.1177/1545968318782743
48. Suntrup-Krueger S, Ringmaier C, Muhle P, Wollbrink A, Kemmling A, Hanning U, et al. Randomized trial of transcranial direct current stimulation for poststroke dysphagia. Ann Neurol. (2018) 83:328–40. doi: 10.1002/ana.25151
49. Yang EJ, Baek SR, Shin J, Lim JY, Jang HJ, Kim YK, et al. Effects of transcranial direct current stimulation (TDCS) on post-stroke dysphagia. Restorative Neurol Neurosci. (2012) 30:303–11. doi: 10.3233/RNN-2012-110213
50. Du J, Yang F, Liu L, Hu J, Cai B, Liu W, et al. Repetitive transcranial magnetic stimulation for rehabilitation of poststroke dysphagia: a randomized, double-blind clinical trial. Clin Neurophysiol März. (2016) 127:1907–13. doi: 10.1016/j.clinph.2015.11.045
51. Khedr EM, Abo-Elfetoh N. Therapeutic role of rTMS on recovery of dysphagia in patients with lateral medullary syndrome and brainstem infarction. J Neurol Neurosurg Psychiatry Mai. (2010) 81:495–9. doi: 10.1136/jnnp.2009.188482
52. Tarameshlu M, Ansari NN, Ghelichi L, Jalaei S. The effect of repetitive transcranial magnetic stimulation combined with traditional dysphagia therapy on poststroke dysphagia: a pilot double-blinded randomized-controlled trial. Int J Rehabil Res. (2019) 42:133–8. doi: 10.1097/MRR.0000000000000336
53. Khedr EM, Abo-Elfetoh N, Rothwell JC. Treatment of post-stroke dysphagia with repetitive transcranial magnetic stimulation. Acta Neurol Scand. (2009) 119:155–61. doi: 10.1111/j.1600-0404.2008.01093.x
54. Park E, Kim MS, Chang WH, Oh SM, Kim YK, Lee A, et al. Effects of bilateral repetitive transcranial magnetic stimulation on post-stroke dysphagia. Brain Stimul. (2017) 10:75–82. doi: 10.1016/j.brs.2016.08.005
55. Dziewas R, Michou E, Trapl-Grundschober M, Lal A, Arsava EM, Bath PM, et al. European Stroke Organisation and European Society for Swallowing Disorders guideline for the diagnosis and treatment of post-stroke dysphagia. Eur Stroke J. (2021) 6:LXXXIX–CXV. doi: 10.1177/23969873211039721
56. Nakato R, Manabe N, Shimizu S, Hanayama K, Shiotani A, Hata J, et al. Effects of capsaicin on older patients with oropharyngeal dysphagia: a double-blind, placebo-controlled, crossover study. Digestion. (2017) 95:210–20. Erratum in: Digestion. (2017) 96:184. doi: 10.1159/000463382
57. Rofes L, Arreola V, Martin A, Clavé P. Effect of oral piperine on the swallow response of patients with oropharyngeal dysphagia. J Gastroenterol. (2014) 49:1517–23. doi: 10.1007/s00535-013-0920-0
58. Arai T, Yoshimi N, Fujiwara H, Sekizawa K. Serum substance p concentrations and silent aspiration in elderly patients with stroke. Neurolo. (2003) 61:1625–6. doi: 10.1212/01.WNL.0000096395.80826.23
59. Martin RE, MacIntosh BJ, Smith RC, Barr AM, Stevens TK, Gati JS, et al. Cerebral areas processing swallowing and tongue movement are overlapping but distinct: a functional magnetic resonance imaging study. J Neurophysiol. (2004) 92:2428–43. doi: 10.1152/jn.01144.2003
60. Hamdy S, Mikulis DJ, Crawley A, Xue S, Lau H, Henry S, et al. Cortical activation during human volitional swallowing: an event-related fMRI study. Am J Physiol. (1999) 277:G219–25. doi: 10.1152/ajpgi.1999.277.1.G219
61. Dehaghani SE, Yadegari F, Asgari A, Chitsaz A, Karami M. Brain regions involved in swallowing: evidence from stroke patients in a cross-sectional study. J Res Med Sci. (2016) 21:45. doi: 10.4103/1735-1995.183997
Keywords: swallowing, cerebrovascular, nutrition, therapy, ischemia, deglutition
Citation: Balcerak P, Corbiere S, Zubal R and Kägi G (2022) Post-stroke Dysphagia: Prognosis and Treatment–A Systematic Review of RCT on Interventional Treatments for Dysphagia Following Subacute Stroke. Front. Neurol. 13:823189. doi: 10.3389/fneur.2022.823189
Received: 26 November 2021; Accepted: 29 March 2022;
Published: 25 April 2022.
Edited by:
Sook-Lei Liew, University of Southern California, United StatesReviewed by:
Domenico Antonio Restivo, Garibaldi Hospital, ItalyHaewon Byeon, Inje University, South Korea
Copyright © 2022 Balcerak, Corbiere, Zubal and Kägi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philipp Balcerak, cGhpbGlwcC5iYWxjZXJha0Brc3NnLmNo