 Ramón Iglesias-Rey1,2*
Ramón Iglesias-Rey1,2* Antía Custodia2,3Maria Luz Alonso-Alonso1,2Iria López-Dequidt4
Antía Custodia2,3Maria Luz Alonso-Alonso1,2Iria López-Dequidt4 Manuel Rodríguez-Yáñez4
Manuel Rodríguez-Yáñez4 José M. Pumar1,5
José M. Pumar1,5 José Castillo1,2
José Castillo1,2 Tomás Sobrino2,3
Tomás Sobrino2,3 Francisco Campos2Andres da Silva-Candal2,6*
Francisco Campos2Andres da Silva-Candal2,6* Pablo Hervella1,2*
Pablo Hervella1,2*- 1Neuroimaging and Biotechnology Laboratory, Health Research Institute of Santiago de Compostela, Santiago de Compostela, Spain
- 2Clinical Neurosciences Research Laboratories, Health Research Institute of Santiago de Compostela, Santiago de Compostela, Spain
- 3NeuroAging Group, Health Research Institute of Santiago de Compostela (IDIS), Santiago de Compostela, Spain
- 4Stroke Unit, Department of Neurology, Hospital Clínico Universitario, Santiago de Compostela, Santiago de Compostela, Spain
- 5Department of Neuroradiology, Hospital Clínico Universitario de Santiago de Compostela, Universidade de Santiago de Compostela, Santiago de Compostela, Spain
- 6Neurovascular Diseases Laboratory, Neurology Service, University Hospital Complex of A Coruña, Biomedical Research Institute, A Coruña, Spain
Objective: This study aimed to explore the association between smoking habit and the serum levels of soluble tumor necrosis factor-like weak inducer of apoptosis (sTWEAK), in relation with the functional outcome of patients with acute ischemic stroke undergoing reperfusion treatment.
Methods: Observational and retrospective study of a series of patients with acute ischemic stroke subjected to reperfusion treatments. Clinical, analytical, and neuroimaging parameters were analyzed. The main endpoint was the functional outcome at 3 months, measured by the modified Ranking Scale (mRS). Logistic regression models were used to analyze the association between smoking and sTWEAK levels with functional outcome and leukoaraiosis.
Results: The results showed that smoking habit was associated with a good functional outcome at 3 months in patients with stroke (OR: 3.52; 95% CI: 1.03–11.9; p = 0.044). However, this independent association was lost after adjusting by sTWEAK levels (OR 1.73; 95% CI: 0.86–13.28; p = 0.116). sTWEAK levels were significantly lower in smoker patients [4015.5 (973.66–7921.83) pg/ml vs. 5,628 (2,848–10,202) pg/ml, p < 0.0001], while sTWEAK levels were significantly higher in patients with poor functional outcomes at 3 months [10,284 (7,388–13.247) pg/ml vs. 3,405 (2,329–6,629) pg/ml, p < 0.0001].
Conclusion: The decrease in sTWEAK levels was associated with a good functional outcome in smoker patients with stroke undergoing reperfusion therapy.
Introduction
Recent clinical studies in cerebrovascular diseases have shown unexpected associations of stroke progression with demographic and clinical data suggesting a better outcome for men (1), obese people (2, 3), and smokers (4) among patients with stroke. Moreover, these associations are even more pronounced in patients undergoing reperfusion treatments (5–7), although those studies are inconclusive and should be questioned.
The controversial beneficial effect of the smoking habit in patients with stroke has been associated with a lower number of complications and good functional outcome (4, 5, 8–10) and could be partially explained by the well-known increased fibrinolytic activity (11) in smoker patients, although there are other disagreeing studies on these associations (12, 13). Therefore, the actual mechanisms behind the positive neurovascular effect of tobacco remain unclear. Several possible mechanisms have been postulated, such as the tobacco effect over the blood-brain barrier (BBB), angiogenesis and increased capillary density, stimulation of growth factors, oxidative stress, or increased metabolic activity (14, 15), but all these hypotheses still need to be confirmed.
In this study, we hypothesize that smoking habit could enhance the thrombolytic activity partially through the activation of the tumor necrosis factor-like weak inducer of apoptosis-fibroblast growth factor-inducible molecule 14 (TWEAK-Fn14) pathway. This hypothesis is based on common neuroinflammatory mechanisms shared by the soluble TWEAK (sTWEAK) and tobacco, as well as on the similar action over the BBB integrity (16). Moreover, sTWEAK and tobacco share a possible common participation in phenomena associated with ischemic preconditioning and on the activation of the NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) (14, 15, 17–19).
Based on the paradoxical effect of tobacco over ischemic stroke, the objectives of our study were as follows: 1) to determine the influence of smoking habit on the outcome in a series of patients with acute ischemic stroke undergoing reperfusion treatments; 2) to study the possible association between tobacco consumption and sTWEAK levels measured at the time of admission of patients with acute ischemic stroke undergoing reperfusion treatment.
Methods
Ethics Approval
This study was carried out in accordance with the Declaration of Helsinki of the World Medical Association (2008) and was approved by the Clinical Research Ethics Committee of Galicia (registration codes 2019/616 and 2016/399). Informed consent was obtained from patients or their relatives at the time of inclusion in the registry, authorizing the anonymous use of data for further studies.
Study Design and Protocols
This is an observational and retrospective study of a series of patients with acute ischemic stroke included consecutively and prospectively in a data bank (BICHUS). The following inclusion criteria were previously defined as follows: 1) authorization for the anonymous use of patient data for research; 2) no history of previous ischemic or hemorrhagic stroke; 3) an MRI or CT study at admission and between the 4th day and the 7th day; 4) patients undergoing some kind of reperfusion treatment; 5) known time of the onset of stroke, with a latency time between the onset and administration of the reperfusion procedure in less than 6 h; 6) face-to-face or telephone monitoring at 3 months ± 15 days; and 7) blood sample stored in the biobank. Only 27 patients who died within the first 24 h were excluded.
All patients with smoking habits, at least during the last year, were considered smokers regardless of their intensity. On the other hand, patients who have never smoked or patients who were abstinent at least during the last year were identified as non-smokers. The stroke was classified according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) criteria (20). The intensity of the neurological deficit was determined by the National Institute of Health Stroke Scale (NIHSS) upon admission in the stroke unit and every 6 h during their stay in the unit. We consider early neurological deterioration with an increase of ≥ 4 points in the NIHSS in the first 48 h. The functional deficit was assessed by the modified Ranking Scale (mRS) at 3 months ± 15 days (face-to-face in 80.8% of the sample). Functional impairment at 3 months was categorized as a good outcome if the mRS ≤ 2 and a poor outcome if the mRS > 2. Both scales were evaluated by internationally certified neurologists. All patients were admitted to the stroke unit and were treated with the protocol of the Spanish Neurological Society, by neurologists trained in cerebrovascular diseases. The recanalization was assessed by the neurological improvement, determined by a decrease of eight points in the NIHSS in the first 24 h.
Analytical Variables
Blood samples were obtained from all patients at admission and collected in test tubes and centrifuged at 3,000 g for 15 min, and serum was immediately frozen and stored at −80°C. Serum concentrations of sTWEAK were determined in samples obtained at admission, before the administration of the reperfusion treatment. Serum levels of sTWEAK were measured using commercial ELISA kits (Elabsciences) following the manufacturer's instructions. The intra- and inter-assay variation coefficients were 5.1 and 5.2%, respectively. All determinations were performed in a laboratory blinded to clinical data. Other laboratory tests were conducted by the Laboratory of the University Clinical Hospital of Santiago de Compostela and were performed on fresh blood samples at the time of diagnosis or shortly after.
Neuroimaging Studies
The identification of the symptomatic hemorrhagic transformation (European Cooperative Acute Stroke Study (ECASS) criteria) (21) was performed at the time of recording the neurological worsening and, in any case, in a second CT performed between the 4th day and the 7th day. The volume of the lesion was determined in the CT performed between the 4th day and the 7th day. The volumes were determined using the ABC/2 method until 2016 and later through the automated planimetric method. The images of leukoaraiosis were stratified according to the Fazekas scale (22) and were identified in the neuroimaging performed at admission. All the neuroimaging studies were supervised by the same neuroradiologist.
Statistical Method
The number of patients was calculated in the base of sTWEAK determinations to achieve a power of 80% to detect differences in the contrast of the hypothesis null H0 (the difference in means is equal to the limit of superiority, by means of a unilateral t-student test of superiority for two independent samples). Taking into account that the level of significance is 5% and assuming that the upper limit is 20,000 pg/ml, the average of sTWEAK in the group of the good outcome is 2,035.5 pg/ml and of the poor outcome is 4,150 pg/ml. The standard deviation (SD) of both groups is ~500 pg/ml. It will be necessary to include at least 168 individuals with a poor outcome and 392 with a good outcome. In addition, 10 more cases should be included for each adjustment covariate in the multivariate analysis (3–4 of a poor outcome and 6–7 of a good outcome, depending on the proportion justified). Assuming the need to adjust the model for 220 covariables, at least 248 cases with a poor outcome and 497 with a good outcome are needed. The calculation has been made with Ene software version 3.0. For this analysis, we consecutively selected all the patients who met all of the inclusion criteria from December 2018 backward.
For statistical analysis, a descriptive analysis was primarily performed. Categorical variables were described with frequency and percentage and the continuous ones with mean and SD or median and interquartile range, depending on their adjustment to a normal distribution (which was determined with the Kolmogorov-Smirnov test with the Lilliefors correction). Then, the statistical inference was carried out with the chi-square test, Student's t-student, or the Mann-Whitney test according to the nature of the contrast variable and its adjustment to normality. Finally, multivariate logistic regression was proposed to be adjusted by the significant variables found in the previous analysis. ORs and their 95% CIs were calculated. All these analyses were performed with IBM SPSS 20 (IBM, Armonk, NY, USA). P < 0.05 were considered significant.
Data Availability
All data are available within the text of the manuscript. Further anonymized data could be made available to qualified investigators upon reasonable request.
Results
We included 875 patients in our study (45.9% women, mean age 72.0 ± 12.5 years), among which 197 patients (22.5%) were identified as smokers (34.0% women). All patients were cigarette smokers, except for 17 patients (11 cigar and 6 pipe smokers). The average time between the onset of symptoms and the administration of reperfusion treatment was 161.8 ± 61.2 min (95% CI: 30–352 min). Regarding the reperfusion treatment, 710 patients received systemic thrombolysis (tPA), 87 had thrombectomy, and 78 had intravenous or intraarterial thrombolysis followed by thrombectomy. According to the TOAST classification, 206 patients had an atherothrombotic infarction, 381 had cardioembolic, 11 had lacunar, and 277 had undetermined origin (among which 143 patients were identified as such due to the coexistence of two causes and 134 patients without a known cause).
Influence of Smoking Habit on the Functional Outcome
Good functional outcome, defined as a mRS ≤ 2 at 3 months, was observed in 79.7% of the smoker patients, as opposed to in 66.2% of non-smokers patients (p < 0.0001); we observed a higher percentage of smoker patients at all mRS ≤ 2 points at 3 months (Figure 1); while non-smoker patients showed higher percentages at mRS > 2. The bivariate analysis for functional outcome at 3 months (Supplementary Table S1) confirmed that the good outcome group included 25.9% of smoker patients, while only 14.9% of smoker patients were observed in the group with poor outcomes (p < 0.0001).
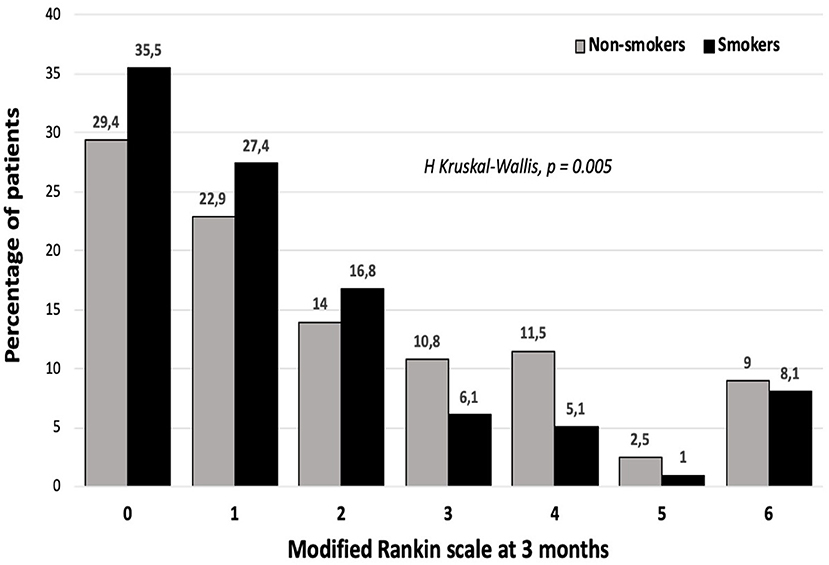
Figure 1. The Ranking scale distribution among smoker and non-smoker patients.
In a non-adjusted logistic regression model using the good functional outcome as the dependent variable, we observed an association between smoking habit and good functional outcome at 3 months with an OR of 1.725 (95% CI: 1.175–2.53; p = 0.005). This association was maintained after adjusting by the clinical and analytical variables that showed differences between patients with good and poor prognosis (summarized in Supplementary Table S1): age, sex, latency time, temperature at admission, NIHSS at admission, lesion volume in DWI, leukoaraiosis, hemorrhagic transformation and recanalization method (OR: 3.38; 95% CI: 1.004–11.42; p = 0.049). However, this association was lost after adjusting by sTWEAK levels (OR 3.07; 95% CI: 0.86–13.28; p = 0.085), while sTWEAK levels showed an inverse association with good outcomes in the abovementioned model (sTWEAK per 100 pg/ml: OR 0.87; 95% CI: 0.8–0.95; p < 0.0001).
Mechanisms Associated With Chronic Smoking Habit
The analysis of the clinical and analytical variables of patients classified as smokers and non-smokers is shown in Table 1. The average age was 6 years lower in smokers while the percentage of women was lower in smoker patients. The percentages of patients with hypertensive, diabetic, and atrial fibrillation were lower in the smoker group. Regarding the analytical variables, the fibrinogen levels in smoker patients were lower than that in the non-smoker group, although rest of the inflammation markers (leukocytes and C-reactive protein) were similar. The NIHSS at admission was similar in the two groups; however, effective reperfusion was more frequent in smoker patients.

Table 1. Clinical variables, biochemical parameters, and neuroimaging values of patients classified according to their smoking habit.
In the adjusted logistic regression model (Supplementary Table S2), smoking habit was independently associated with age (OR 0.97; 95% CI:0.96–0.99; p < 0.0001), alcohol consumption (OR 3.27; 95% CI: 2.03–5.27, p < 0.0001), and fibrinogen levels (OR 0.99; 95% CI: 0.99–0.99; p = 0.009).
Serum concentrations of sTWEAK were determined in samples obtained at admission before the administration of the reperfusion treatment. sTWEAK levels were significantly lower in smoker patients [4,015 (974–7,922) pg/ml vs. 5,629 (2,848–10,202) pg/ml, p < 0.0001] (Figure 2) and were significantly higher in patients with poor outcome at 3 months, compared with patients with good outcomes [10,284 (7,388–13,247) pg/ml vs. 3,405 (2,329–6,629) pg/ml, p < 0.0001] (Figure 3). Basal sTWEAK levels were independently associated with smoking habit (OR 0.9: 95% CI: 0.86–0.94; p < 0.0001) (Table 2).
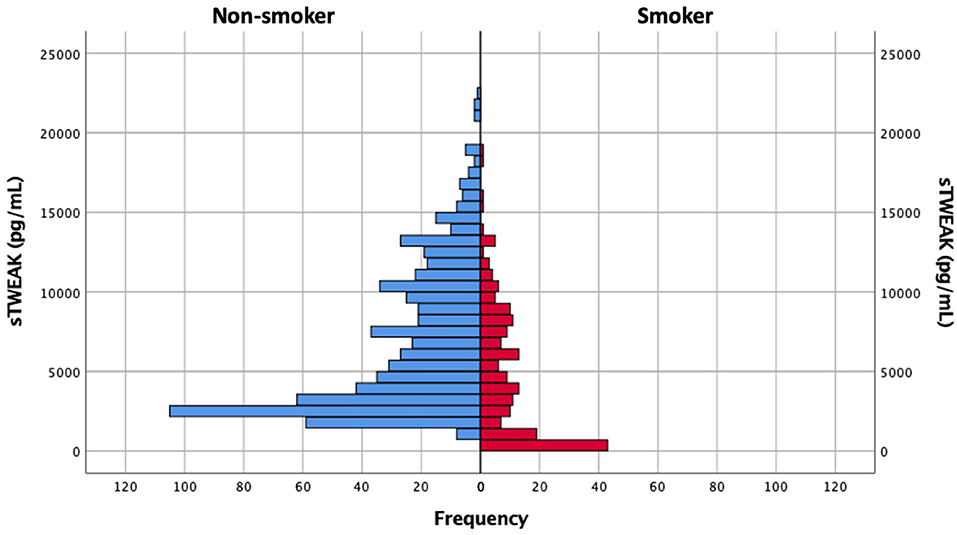
Figure 2. Distribution of soluble tumor necrosis factor-like weak inducer of apoptosis (sTWEAK) values in non-smoker and smoker patient populations.
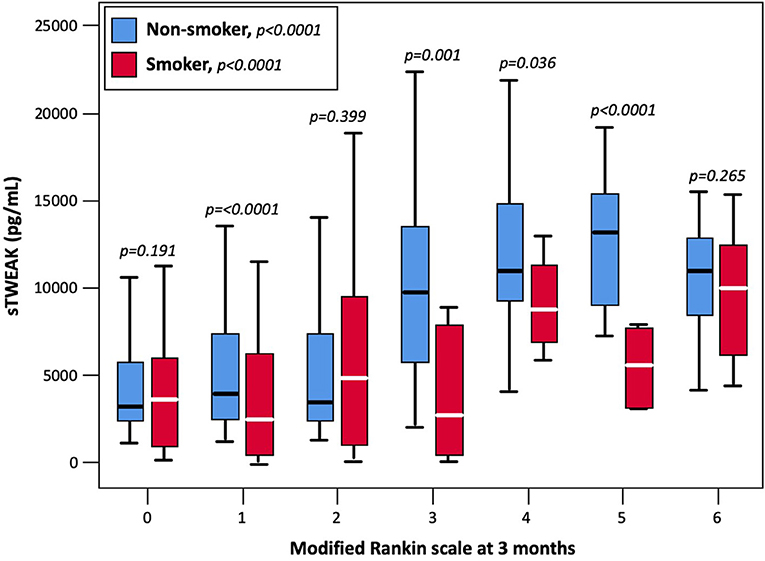
Figure 3. Basal sTWEAK concentrations at different points of the modified Rankin scale at 3 months in smoker and non-smokers patients.
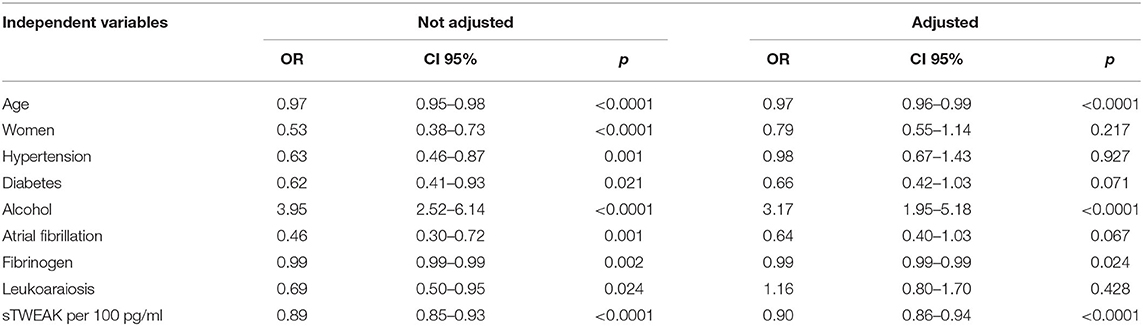
Table 2. Logistic regression models for factors associated with smoking habit.
Values in Non-smoker and Smoker Patient Populations
Smoker patients showed less early neurological deterioration (5.6 vs. 11.6%, p < 0.0001) and a higher percentage of early neurological improvement (66 vs. 47.9%, p < 0.0001) compared with non-smoking patients. The same relationship was observed for sTWEAK levels that were lower in smoker patients with early neurological improvement [4,234 (2,498–7,785) pg/ml vs. 6,571 (2,923–10,630) pg/ml, p < 0.0001] and higher in smokers who presented early neurological deterioration [10,125 (6,435–13,409) pg/ml vs. 4,704 (2,588–8,935) pg/ml, p < 0.0001]. The differences observed in sTWEAK levels between smokers and non-smoker patients were especially more pronounced among patients showing early neurological deterioration (Figure 4).
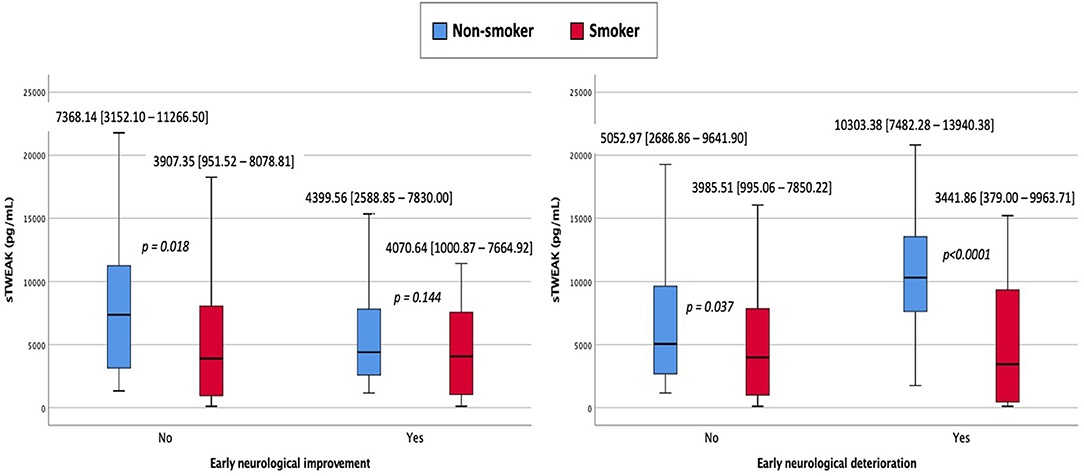
Figure 4. sTWEAK concentrations in smoker and non-smoker patients who presented early neurological improvement and early neurological deterioration.
Discussion
Nowadays, active and passive smoking are associated with the most prevalent causes of mortality and morbidity (23–25). Therefore, smoking suppression and hypertension control are undoubtedly two important objectives that should lead the actions to control preventable deaths (26). Among vascular diseases, the relationship between tobacco and coronary heart disease is well known (27), although its actual mechanism is still unclear (28), and the association of tobacco with stroke is still controversial (27, 29).
In our series of patients with stroke undergoing reperfusion treatment, the association between smoking and good outcome was confirmed. Recent studies suggest the influence of age over the association between stroke and smoke (30, 31). However, we observed in our series an independent association between smoking and good outcomes after adjusting by age.
The influence of tobacco on the fibrinolytic plasma activity remains inconclusive. Some studies showed that nicotine levels are associated with plasminogen activator inhibition (32), while others demonstrated that tobacco increases the fibrinolytic activity (11). In our sample, the clinical response to reperfusion was higher in smoker patients, and we did not observe an increase in the frequency or intensity of hemorrhagic transformations in smoker patients. These discrepancies have been explained by the increased tendency of thrombogenic strokes in smoker patients rather than strokes caused by the rupture of atheromatous plaques with the subsequent formation of platelet-rich clots (4). In this sense, our smoker patients were less cardioembolic and also presented fewer risk factors for atheromatosis and had a greater (non-significant) proportion of stroke of undetermined origin. Another controversial aspect is the association of tobacco with the inflammatory response. The abovementioned hypothesis of tobacco being less associated with the rupture of atheroma plaques (4) is in disagreement with the possibility of a high inflammatory response (33). Our patients had lower concentrations of fibrinogen and C-reactive protein and was also associated with a lower degree of leukoaraiosis (neuroimage associated with inflammatory response) (34, 35).
Most studies analyzing the molecular mechanisms associated with smoking were focused on its effect on the respiratory and cardiovascular systems (14), while the effect of tobacco on the cerebral parenchyma and microcirculation is less known. Some studies have identified effects due to nicotine (36, 37), oxidative stress linked to tobacco (36, 38), and alterations associated with other products derived from tobacco (39). Nicotine exposure could affect the integrity of the blood–brain barrier by causing a decrease in the expression of endothelial tight junction proteins and an increased permeability and edema associated with leukoaraiosis and small vessel disease (40). On the other hand, it was reported that nicotine decreases the activity of Na+/K+/Cl2− cotransporters through cell membranes (41) and increases the density through a stimulus of angiogenesis (42) and the expression of vascular growth factors (43).
Given the variety of compounds found in tobacco smoke, it is difficult to reach definitive conclusions justifying the smoker's paradox. One of the hypotheses is the ischemic preconditioning, caused by the chronic development of vasoconstriction of small cerebral vessels (4). In in vitro models, it was observed that tobacco smoke could actually increase cell death in a culture of cardiomyocytes; however, this effect was lower in cell cultures previously conditioned by oxygen and glucose deprivation (15). Overexpression of p53 is another route leading to cell death (44), which is partially inhibited by exposure to tobacco extracts in hypoxic conditions (15). These studies suggest that tobacco causes cell death in situations of normoxia, but in hypoxic conditions, there is a notable decrease in cell death, a situation that could explain the smoker's paradox.
The benefits of tobacco found in the thrombolysis efficiency are not translatable to clinical practice and under no circumstances should change the current guides regarding the prohibition of tobacco. As an alternative, some studies have focused on the molecular mechanisms behind the benefits of tobacco in acute cerebral ischemia. In this sense, we have evaluated the role of sTWEAK in several mechanisms associated with ischemic brain damage (45). sTWEAK is a part of the TNF superfamily that binds to Fn14 and is expressed in the very early stages of cerebral ischemia, which may explain its association with the early neurological improvement or deterioration. TWEAK-Fn14 induces a neuroinflammatory response, a secretion of proinflammatory cytokines and metalloproteases, and a disruption of the blood-brain barrier (18). Recently, TWEAK-Fn14 signaling has been shown to contribute to the protective effect associated with ischemic preconditioning (18). All these mechanisms are involved in cerebrovascular effects associated with tobacco. Based on these pieces of evidence, we analyzed the sTWEAK levels in patients with reperfused cerebral infarction, since this is a subgroup of patients where the smoker's paradox is clearer. Our results confirmed that the sTWEAK levels were lower in smokers. Similarly, the association between tobacco and good outcome disappeared after introducing the sTWEAK values into the model, which statistically implies an association between tobacco and sTWEAK. Therefore, sTWEAK could be a mechanism associated with the smoker's paradox, although it would need a deeper mechanistic study to confirm this association.
The weaknesses of our work are obvious since it is a retrospective study that does not explore any mechanistic aspect. Experimental studies are necessary to confirm our conclusions. Another weakness is the analysis of the sTWEAK instead of the TWEAK-Fn14 association.
In conclusion, sTWEAK was associated with a good functional outcome in smoker patients with stroke undergoing reperfusion therapy.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by Clinical Research Ethics Committee of Galicia (registration codes 2019/616 and 2016/399). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
RI-R, JC, and PH: design and conceptualized the study, analyzed the data, and wrote the manuscript. IL-D, MR-Y, JP, AC, MA-A, AS-C, TS, and FC: major role in the acquisition of data and critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was partially supported by grants from the Spanish Ministry of Science and Innovation (SAF2017-84267-R; PDC2021-121455-100), the Xunta de Galicia (Axencia Galega de Innovación-GAIN; Consellería de Cultura, Educación e Universidade: IN607A2018/3), the Instituto de Salud Carlos III (ISCIII) (PI17/00540; PI17/01103; PI20/01014; PI21/01256; AC21_2/00014; RETICS-INVICTUS PLUS - RD16/0019/0001; RICORS ICTUS - RD21/0006/0003), co funded by European Union, FEDER program. Furthermore, TS (CPII17/00027) and FC (CPII19/00020) are recipients of research contracts from the Miguel Servet Program of Instituto de Salud Carlos III. AS-C (CD20/00054) recipient of Sara Borrell grant funded by Instituto de Salud Carlos III and co-funded by European Union. The sponsors did not participate in the study design, collection, analysis, or interpretation of the data, in writing the report, or in the decision to submit the paper for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.841484/full#supplementary-material
References
1. Falsetti L, Viticchi G, Buratti L, Balucani C, Marra AM, Silvestrini M. From head to toe: sex and gender differences in the treatment of ischemic cerebral disease. Pharmacol Res. (2017) 121:240–50. doi: 10.1016/j.phrs.2017.05.006
2. Oesch L, Tatlisumak T, Arnold M, Sarikaya H. Obesity paradox in stroke - Myth or reality? a systematic review. PLoS ONE. (2017) 12:e0171334. doi: 10.1371/journal.pone.0171334
3. Rodriguez-Castro E, Rodriguez-Yanez M, Arias-Rivas S, Santamaria-Cadavid M, Lopez-Dequidt I, Hervella P, et al. Obesity paradox in ischemic stroke: clinical and molecular insights. Transl Stroke Res. (2019) 10:639–49. doi: 10.1007/s12975-019-00695-x
4. Ali SF, Smith EE, Bhatt DL, Fonarow GC, Schwamm LH. Paradoxical association of smoking with in-hospital mortality among patients admitted with acute ischemic stroke. J Am Heart Assoc. (2013) 2:e000171. doi: 10.1161/JAHA.113.000171
5. Ovbiagele B, Saver JL. The smoking-thrombolysis paradox and acute ischemic stroke. Neurology. (2005) 65:293–5. doi: 10.1212/01.WNL.0000168163.72351.f3
6. Reeves MJ, Wilkins T, Lisabeth LD, Schwamm LH. Thrombolysis treatment for acute stroke: issues of efficacy and utilization in women. Womens Health. (2011) 7:383–90. doi: 10.2217/WHE.11.31
7. Sarikaya H, Elmas F, Arnold M, Georgiadis D, Baumgartner RW. Impact of obesity on stroke outcome after intravenous thrombolysis. Stroke. (2011) 42:2330–2. doi: 10.1161/STROKEAHA.110.599613
8. Hussein HM, Niemann N, Parker ED, Qureshi AI. Searching for the smoker's paradox in acute stroke patients treated with intravenous thrombolysis. Nicotine Tob Res. (2017) 19:871–6. doi: 10.1093/ntr/ntx020
9. Kufner A, Nolte CH, Galinovic I, Brunecker P, Kufner GM, Endres M, et al. Smoking-thrombolysis paradox: recanalization and reperfusion rates after intravenous tissue plasminogen activator in smokers with ischemic stroke. Stroke. (2013) 44:407–13. doi: 10.1161/STROKEAHA.112.662148
10. Wahlgren N, Ahmed N, Eriksson N, Aichner F, Bluhmki E, Dávalos A, et al. Multivariable analysis of outcome predictors and adjustment of main outcome results to baseline data profile in randomized controlled trials: Safe Implementation of Thrombolysis in Stroke-MOnitoring STudy (SITS-MOST). Stroke. (2008) 39:3316–22. doi: 10.1161/STROKEAHA.107.510768
11. Janzon L, Nilsson IM. Smoking and fibrinolysis. Circulation. (1975) 51:1120–3. doi: 10.1161/01.CIR.51.6.1120
12. Schlemm L, Kufner A, Boutitie F, Nave AH, Gerloff C, Thomalla G, et al. Current smoking does not modify the treatment effect of intravenous thrombolysis in acute ischemic stroke patients-A Post-hoc analysis of the WAKE-UP trial. Front Neurol. (2019) 10:1239. doi: 10.3389/fneur.2019.01239
13. Zhang P, Guo ZN, Sun X, Zhao Y, Yang Y. Meta-analysis of the smoker's paradox in acute ischemic stroke patients receiving intravenous thrombolysis or endovascular treatment. Nicotine Tob Res. (2019) 21:1181–8. doi: 10.1093/ntr/ntz094
14. Naik P, Cucullo L. Pathobiology of tobacco smoking and neurovascular disorders: untied strings and alternative products. Fluids Barriers CNS. (2015) 12:25. doi: 10.1186/s12987-015-0022-x
15. Wittmann F, Türkcan A, Baranyi U, Eichmair E, Laufer G, Bernhard D, et al. To be or not to be: the “Smoker's Paradox”-an in-vitro study. Cell Physiol Biochem. (2018) 48:1638–51. doi: 10.1159/000492285
16. Pimentel E, Sivalingam K, Doke M, Samikkannu T. Effects of drugs of abuse on the blood-brain barrier: a brief overview. Front Neurosci. (2020) 14:513. doi: 10.3389/fnins.2020.00513
17. Blanco-Colio LM. TWEAK/Fn14 axis: a promising target for the treatment of cardiovascular diseases. Front Immunol. (2014) 5:3. doi: 10.3389/fimmu.2014.00003
18. Boulamery A, Desplat-Jégo S. Regulation of neuroinflammation: what role for the tumor necrosis factor-like weak inducer of apoptosis/Fn14 pathway? Front Immunol. (2017) 8:1534. doi: 10.3389/fimmu.2017.01534
19. Winkles JA. The TWEAK-Fn14 cytokine-receptor axis: discovery, biology and therapeutic targeting. Nature reviews Drug discovery. (2008) 7:411–25. doi: 10.1038/nrd2488
20. Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke. definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment. Stroke. (1993) 24:35–41. doi: 10.1161/01.STR.24.1.35
21. Berger C, Fiorelli M, Steiner T, Schäbitz WR, Bozzao L, Bluhmki E, et al. Hemorrhagic transformation of ischemic brain tissue: asymptomatic or symptomatic? Stroke. (2001) 32:1330–5. doi: 10.1161/01.STR.32.6.1330
22. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging. AJR Am J Roentgenol. (1987) 149:351–6. doi: 10.2214/ajr.149.2.351
23. Banks E, Joshy G, Korda RJ, Stavreski B, Soga K, Egger S, et al. Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study. BMC Med. (2019) 17:128. doi: 10.1186/s12916-019-1351-4
24. Lee PN, Forey BA, Thornton AJ, Coombs KJ. The relationship of cigarette smoking in Japan to lung cancer, COPD, ischemic heart disease and stroke: a systematic review. F1000Res. (2018) 7:204. doi: 10.12688/f1000research.14002.1
25. Pan B, Jin X, Jun L, Qiu S, Zheng Q, Pan M. The relationship between smoking and stroke: a meta-analysis. Medicine. (2019) 98:e14872. doi: 10.1097/MD.0000000000014872
26. Zhong XL, Dong Y, Xu W, Sun L, Wang HF Li HQ, et al. Blood pressure lowering and stroke prevention: a systematic review and network meta-analysis protocol. Ann Transl Med. (2019) 7:489. doi: 10.21037/atm.2019.08.99
27. Suzuki S, Otsuka T, Sagara K, Semba H, Kano H, Matsuno S, et al. Effects of smoking on ischemic stroke, intracranial hemorrhage, and coronary artery events in japanese patients with non-valvular atrial fibrillation. Int Heart J. (2017) 58:506–15. doi: 10.1536/ihj.16-228
28. Stallones RA. The association between tobacco smoking and coronary heart disease. Int J Epidemiol. (2015) 44:735–43. doi: 10.1093/ije/dyv124
29. Tonnesen P, Marott JL, Nordestgaard B, Bojesen SE, Lange P. Secular trends in smoking in relation to prevalent and incident smoking-related disease: a prospective population-based study. Tob Induc Dis. (2019) 17:72. doi: 10.18332/tid/112459
30. Wang H-K, Huang C-Y, Sun Y-T, Li J-Y, Chen C-H, Sun Y, et al. Smoking paradox in stroke survivors? Stroke. (2020) 51:1248–56. doi: 10.1161/STROKEAHA.119.027012
31. Havenon AHd, Mistry E, Yaghi S, Khatri P, Prabhakaran S. The smokers paradox after acute ischemic stroke, is it real or a cloud of smoke? Stroke. (2020) 51(Suppl_1):AWMP58. doi: 10.1161/str.51.suppl_1.WMP58
32. Zidovetzki R, Chen P, Fisher M, Hofman FM, Faraci FM. Nicotine increases plasminogen activator inhibitor-1 production by human brain endothelial cells via protein kinase C-associated pathway. Stroke. (1999) 30:651–5. doi: 10.1161/01.STR.30.3.651
33. Purcell IF, Newall N, Farrer M. Lower cardiac mortality in smokers following thrombolysis for acute myocardial infarction may be related to more effective fibrinolysis. QJM. (1999) 92:327–33. doi: 10.1093/qjmed/92.6.327
34. Fu Y, Yan Y. Emerging role of immunity in cerebral small vessel disease. Front Immunol. (2018) 9:67. doi: 10.3389/fimmu.2018.00067
35. Hase Y, Horsburgh K, Ihara M, Kalaria RN. White matter degeneration in vascular and other ageing-related dementias. J Neurochem. (2018) 144:617–33. doi: 10.1111/jnc.14271
36. Munakata S, Ishimori K, Kitamura N, Ishikawa S, Takanami Y, Ito S. Oxidative stress responses in human bronchial epithelial cells exposed to cigarette smoke and vapor from tobacco- and nicotine-containing products. Regul Toxicol Pharmacol. (2018) 99:122–8. doi: 10.1016/j.yrtph.2018.09.009
37. Niemann B, Rohrbach S, Miller MR, Newby DE, Fuster V, Kovacic JC. Oxidative stress and cardiovascular risk: obesity, diabetes, smoking, and pollution: part 3 of a 3-part series. J Am Coll Cardiol. (2017) 70:230–51. doi: 10.1016/j.jacc.2017.05.043
38. Carnevale R, Sciarretta S, Violi F, Nocella C, Loffredo L, Perri L, et al. Acute impact of tobacco vs electronic cigarette smoking on oxidative stress and vascular function. Chest. (2016) 150:606–12. doi: 10.1016/j.chest.2016.04.012
39. Tega Y, Yamazaki Y, Akanuma SI, Kubo Y, Hosoya KI. Impact of nicotine transport across the blood-brain barrier: carrier-mediated transport of nicotine and interaction with central nervous system drugs. Biol Pharm Bull. (2018) 41:1330–6. doi: 10.1248/bpb.b18-00134
40. Hossain M, Sathe T, Fazio V, Mazzone P, Weksler B, Janigro D, et al. Tobacco smoke: a critical etiological factor for vascular impairment at the blood-brain barrier. Brain Res. (2009) 1287:192–205. doi: 10.1016/j.brainres.2009.06.033
41. Paulson JR, Roder KE, McAfee G, Allen DD, Van der Schyf CJ, Abbruscato TJ. Tobacco smoke chemicals attenuate brain-to-blood potassium transport mediated by the Na,K,2Cl-cotransporter during hypoxia-reoxygenation. J Pharmacol Exp Ther. (2006) 316:248–54. doi: 10.1124/jpet.105.090738
42. Lee J, Cooke JP. Nicotine and pathological angiogenesis. Life Sci. (2012) 91:1058–64. doi: 10.1016/j.lfs.2012.06.032
43. Ebrahimpour A, Shrestha S, Bonnen MD, Eissa NT, Raghu G, Ghebre YT. Nicotine modulates growth factors and MicroRNA to promote inflammatory and fibrotic processes. J Pharmacol Exp Ther. (2019) 368:169–78. doi: 10.1124/jpet.118.252650
44. Gomez-Sanchez JC, Delgado-Esteban M, Rodriguez-Hernandez I, Sobrino T, Perez de la Ossa N, Reverte S, et al. The human Tp53 Arg72Pro polymorphism explains different functional prognosis in stroke. J Exp Med. (2011) 208:429–37. doi: 10.1084/jem.20101523
Keywords: stroke, reperfusion, leukoaraiosis, sTWEAK, endothelial dysfunction
Citation: Iglesias-Rey R, Custodia A, Alonso-Alonso ML, López-Dequidt I, Rodríguez-Yáñez M, Pumar JM, Castillo J, Sobrino T, Campos F, Silva-Candal Ad and Hervella P (2022) The Smoking Paradox in Stroke Patients Under Reperfusion Treatment Is Associated With Endothelial Dysfunction. Front. Neurol. 13:841484. doi: 10.3389/fneur.2022.841484
Received: 22 December 2021; Accepted: 22 February 2022;
Published: 24 March 2022.
Edited by:
Jean-Claude Baron, University of Cambridge, United KingdomReviewed by:
Marialuisa Zedde, IRCCS Local Health Authority of Reggio Emilia, ItalyBum Joon Kim, University of Ulsan, South Korea
Copyright © 2022 Iglesias-Rey, Custodia, Alonso-Alonso, López-Dequidt, Rodríguez-Yáñez, Pumar, Castillo, Sobrino, Campos, Silva-Candal and Hervella. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Hervella, cGFibG8uaGVydmVsbGEubG9yZW56b0BzZXJnYXMuZXM=; Andres da Silva-Candal, YW5kcmVzLmFsZXhhbmRlci5kYS5zaWx2YS5jYW5kYWxAc2VyZ2FzLmVz; Ramón Iglesias-Rey, cmFtb24uaWdsZXNpYXMucmV5QHNlcmdhcy5lcw==