 Hala Al-Obaidi1†Zainab Khidhair2†
Hala Al-Obaidi1†Zainab Khidhair2† Feras Jirjees3
Feras Jirjees3 Muna Barakat4,5
Muna Barakat4,5 Husam AlSalamat6,7
Husam AlSalamat6,7 Zelal Kharaba8,9Yassen Alfoteih10
Zelal Kharaba8,9Yassen Alfoteih10 Chadia Haddad11,12Sara Mansour13
Chadia Haddad11,12Sara Mansour13 Souheil Hallit12,14§
Souheil Hallit12,14§ Diana Malaeb13,15*‡Hassan Hosseini16,17‡
Diana Malaeb13,15*‡Hassan Hosseini16,17‡- 1Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates
- 2Department of Biology, College of Science, University of Baghdad, Baghdad, Iraq
- 3Department of Pharmacy Practice and Pharmacotherapeutics, College of Pharmacy, University of Sharjah, Sharjah, United Arab Emirates
- 4Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan
- 5MEU Research Unit, Middle East University, Amman, Jordan
- 6Department of Basic Medical Sciences, Faculty of Medicine, Al-Balqa Applied University, Al-Salt, Jordan
- 7Department of Biopharmaceutics and Clinical Pharmacy, School of Pharmacy, University of Jordan, Amman, Jordan
- 8Department of Clinical Pharmacy, College of Pharmacy, Al-Ain University, Abu Dhabi, United Arab Emirates
- 9Honorary Associate Lecturer, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, United Kingdom
- 10Department of Dental Surgery, City University College of Ajman, Ajman, United Arab Emirates
- 11INSPECT-LB (Institut National de Santé Publique, d'Épidémiologie Clinique et de Toxicologie-Liban), Beirut, Lebanon
- 12Research Department, Psychiatric Hospital of the Cross, Jal Ed Dib, Lebanon
- 13School of Pharmacy, Lebanese International University, Beirut, Lebanon
- 14School of Medicine and Medical Sciences, Holy Spirit University of Kaslik, Jounieh, Lebanon
- 15College of Pharmacy, Gulf Medical University, Ajman, United Arab Emirates
- 16Neurology Department, Henri Mondor Hospital, AP-HP, Créteil, France
- 17INSERM U955-E01, IMRB, UPEC-Universite Paris-Est, Créteil, France
Introduction: Stroke is a highly prevalent condition with high rates of death and disability in Iraq and around the world. Knowledge of stroke and its associated risk factors is essential for disease prevention and rapid response when confronted with a stroke patient.
Purpose: The purpose of this study is to assess stroke knowledge and identify factors associated with awareness among the Iraqi public.
Material and methods: A questionnaire-based, cross-sectional survey was conducted on the Iraqi population. The self-administered online questionnaire contained three sections. The study got ethical approval from the Research Ethics Committee at the University of Baghdad.
Results: The results showed that 26.8% of the participants reported knowledge regarding identifying all risk factors. In addition, 18.4% and 34.8% of the participants recognized all symptoms and mentioned all possible consequences of stroke, respectively. Previous medical history with chronic diseases had essential relationships with the response when faced with a person having an acute stroke. In addition, there was a significant relationship between gender, smoking history, and identification of early stroke symptoms.
Conclusion: There was a lack of knowledge about risk factors for stroke among the participants. There is a need for an awareness program among the Iraqi people to raise their understanding of stroke that can reduce stroke mortality and morbidity.
1. Introduction
Globally, more than 12 million people suffer a stroke yearly, with an annual mortality rate above 5.5 million in the last two decades (1, 2). According to statistics, stroke is the second greatest cause of mortality and causes lasting disability in almost 5 million people (1, 3). As a result, it significantly increases the financial and social load on families and societies (2). Risk factors that affect stroke onset and progression include hypertension, diabetes mellitus, smoking, obesity, psychological factors, physical activity, and food. Approximately 80% of stroke cases can be halted if necessary precautions and appropriate measures are taken (2). Stroke risk is dramatically increasing more in emerging nations than in industrialized ones (2, 4, 5). In wealthy nations during the past four decades, stroke incidence has decreased by 42%, in contrast to developing (low- to middle-income) nations, where stroke rates have soared by 100%. (1). This change in stroke rates from industrialized to developing nations results from new risk factors, such as an unhealthy lifestyle, unbalanced diets, socioeconomic inequality, and a lack of access to the necessary treatment for individuals (1, 4).
Mortality from non-communicable diseases, including strokes, accounts for 55% of all deaths (6). In the context of Iraq, a country in the Middle East, coronary heart diseases and stroke are predominant diseases encountered in clinical practice. Incidence rates of stroke in Iraq ranged from 196.2 to 218.3 per 100,000 people in 2019, according to Global Burden of Disease 2019 Stroke Collaborators (2). Furthermore, 35.8% of Iraqis are estimated to suffer from hypertension, 14% from diabetes mellitus, 38% are smokers, and more than 30% are obese (6). Moreover, many Iraqi people have reported an unhealthy lifestyle, including a lack of physical activity and poor nutrition with high-calorie foods (7, 8). Therefore, several risk factors, including the high incidence of chronic diseases as well as the adoption of an unhealthy lifestyle, have been associated with the prevalence of stroke among the Iraqi population (9, 10). It is well-documented in the literature that the incidence of stroke can be prevented and reduced by knowing the risk factors that cause the disease, such as high blood pressure, smoking, and an unhealthy lifestyle (11–13). By identifying these factors, the initiation of preventive measures and raising awareness among the population can be achieved. In addition, complications from an acute stroke can be minimized by knowing what action is required for people who witness someone having a stroke (13, 14). Therefore, a careful assessment of the overall knowledge of stroke and its associated aggravating factors in the population is needed to assess the best preventive measure and implement community-oriented educational programs. Therefore, it is vital to explore features such as lifestyle, behavior, academic level, history of smoking, and socioeconomic status to understand the disparities in stroke knowledge between different sociodemographic groups.
Iraq's latest national epidemiological research on stroke is insufficient to determine the level of public knowledge. In order to reduce the burden of stroke, it is imperative to implement preventative measures, assess public knowledge and awareness of stroke and its risk factors, and improve patient knowledge and awareness through educational programs. Thus, this study aimed to evaluate stroke knowledge and determine the factors associated with stroke awareness among the Iraqi population.
2. Materials and methods
2.1. Study design
A cross-sectional observational study was conducted in Iraq between April and May 2021 from the general population using an anonymous survey. A Google forms-based electronic survey was produced and disseminated through social media platforms (i.e., WhatsApp and Facebook). Participants in this study had to be older than 18 to be eligible, and those with a stroke history were excluded. Participation was voluntary.
2.2. Minimal sample size
The target sample size was determined to be approximately 385 individuals based on another study's findings that approximately 71.8% of the participants were able to name at least three out of the five stroke risk factors (15) and because there were no comparable studies conducted in Iraq. Based on a confidence interval of 95%, a standard deviation of 0.5, and a margin of error of 5%, the Raosoft software sample size calculator calculated this amount as the minimum sample size required for an unlimited population size.
2.3. Questionnaire
The questionnaire was self-administered and required approximately 10 min to complete. The questionnaire was in Arabic, the native language of Iraqi people. The authors and five academic members reviewed the questionnaire, which then underwent a pilot test with five Iraqis in order to ensure the clarity of the questions. Next, the questions were modified based on their feedback.
The survey has been developed using the general principles of good survey design (16). Participants filled it out without the help of the researchers to avoid any potential influence when answering the questions. The current questionnaire, methods, and tools used in this study were mainly adapted from a study conducted in Jordan in which the general knowledge about stroke was assessed (17). The questionnaire was structured similarly to the one in Jordan in all the aspects that covered stroke knowledge except for the sociodemographic factors (i.e., economic status and residence area) because of the discrepancy between the two countries. However, differences were only in the sociodemographic characteristics due to the slight variation between the two countries. The questionnaire was structured to collect information about stroke in terms of symptoms, risk factors, early warning signs, and complications. Participants completed it without the assistance of investigators to avoid any potential influence when responding to questions. The opening section of the questionnaire covered the sociodemographic characteristics, including age, marital status, smoking status (positive when participant smoked for at least a year), employment status (employed vs. unemployed), monthly income, residence (urban vs. rural), educational level, and past medical history determined by self-report such as ever being diagnosed with a medical condition by a healthcare professional (e.g., hypertension, diabetes mellitus, dyslipidemia). Age was classified into four categories (18–29, 30–49, and above 50 years), while family income was divided into three categories: low (<400 K), intermediate (400–1,000 K), and high (>1,000 K) (18).
The second section evaluated the general knowledge related to stroke. Participants responded to whether the stroke is a disease that: (1) affects the brain, (2) is an old person's disease, (3) is contagious, (4) is hereditary, and (5) and can be prevented. Furthermore, this section assessed awareness of the risk factors of stroke, including old age, hypertension, diabetes mellitus, heart disease, high cholesterol, smoking, alcohol consumption, physical inactivity, obesity, and stress. This section also focused on participants' knowledge of early stroke warning signs, including (1) sudden numbness or weakness of the face, arms, or legs, (2) sudden difficulty speaking or understanding speech, (3) sudden blurry vision or visual impairment in one or both eyes, (4) sudden dizziness or loss of balance or coordination, and (5) sudden severe headache (18). In addition, participants reported potential consequences of stroke: (1) movement and functional problems (i.e., one-sided paralysis, loss of ability to walk, tiredness, fatigue), (2) cognitive and memory problems (i.e., loss of ability to speak, write, read, remember or understand), (3) visual problems (i.e., loss of sight or blurred vision), (4) emotional and personality changes (i.e., depression, anger, mood changes), and (5) long-term disabilities. Three questions assessed people's attitudes and reactions toward a patient experiencing stroke (e.g., willingness to take a patient to hospital care); two others were on curiosity and self-assessment, while the last one was to determine the sources of information of knowledge about stroke. Participants were given one point for each correct response to the earlier statements (19, 20). Missing answers were not counted. Sometimes, multiple answers were allowed, so the total score was higher than the total number of questions. The third section identified sources of information related to stroke among the participants.
2.4. Ethical approval
The study got ethical approval from the Research Ethics Committee at the University of Baghdad [SA 3/6502]. The study followed the Declaration of Helsinki's ethical standards and its later amendments or comparable ethical standards. All participants gave written informed consent to participate in the study.
2.5. Statistical analysis
Data collected were analyzed using the Statistical Package for Social Sciences (SPSS) version 25.0. Continuous variables were presented as mean ± standard deviation and 95% confidence interval. Categorical and ordinal variables were shown as frequencies (n) and percentages (%). Correlations between risk factors, early symptoms, and consequences of stroke with the socio-demographics and past medical history were determined by the Pearson chi-square or Fisher's exact test if the cell count was less than five. Logistic regression identified stroke risk factors, early symptoms, consequences, and response if faced with stroke as dependent variables and sociodemographic characteristics (gender, residence area, educational level, employment status, and smoking history) and health status as independent variables. Variables with a p-value of <0.2 in the bivariate analysis were included in the regression analysis (21). Potential confounders were eliminated if the p-value was >0.2 to protect against residual confounding. The results were presented as odds ratios (ORs) and 95% confidence interval. Statistical tests were two-tailed and indicated statistical significance at a p-value of < 0.05.
3. Results
3.1. Sociodemographic characteristics
A total of 609 participants completed the questionnaire. The majority of the participants lived in urban areas (93.6%), were female (78.3%), single (75.4%), and had a college degree (69.6%). The sociodemographic variables and health status of the participants are presented in Table 1. The most common comorbidities were heart disease (25.1%), followed by depression (22.6%) and obesity (16.1%). A family history of stroke was reported in 35.3% of the participants.

Table 1. Sociodemographic characteristics of the participants (N = 609).
3.2. Stroke knowledge
Familiarity with stroke was so high that 604 participants (99.2%) knew about it. In addition, most participants (76.2%) knew at least one person, a relative or friend, who had a stroke.
The level of knowledge about stroke is presented in Figure 1 and Table 2. Most of the sample were aware that stroke is a brain disease and can be prevented (92.8% and 85.6%, respectively) (Figure 1A). Furthermore, 91.1% believed that hypertension was the most common risk factor for stroke, followed by psychosocial stress (87.2%) and high cholesterol level (82.3%) (Figure 1B). The majority of participants stated that stroke could affect movement and functional problems (92.5%), lead to long-term disabilities (86.2%), and affect cognitive and memory problems (81.0%) (Figure 1C). The most common warning signs identified were “sudden difficulty in speaking or understanding speech” and “sudden weakness/numbness/tingling,” with 88.0% and 86.9%, respectively (Figure 1D).
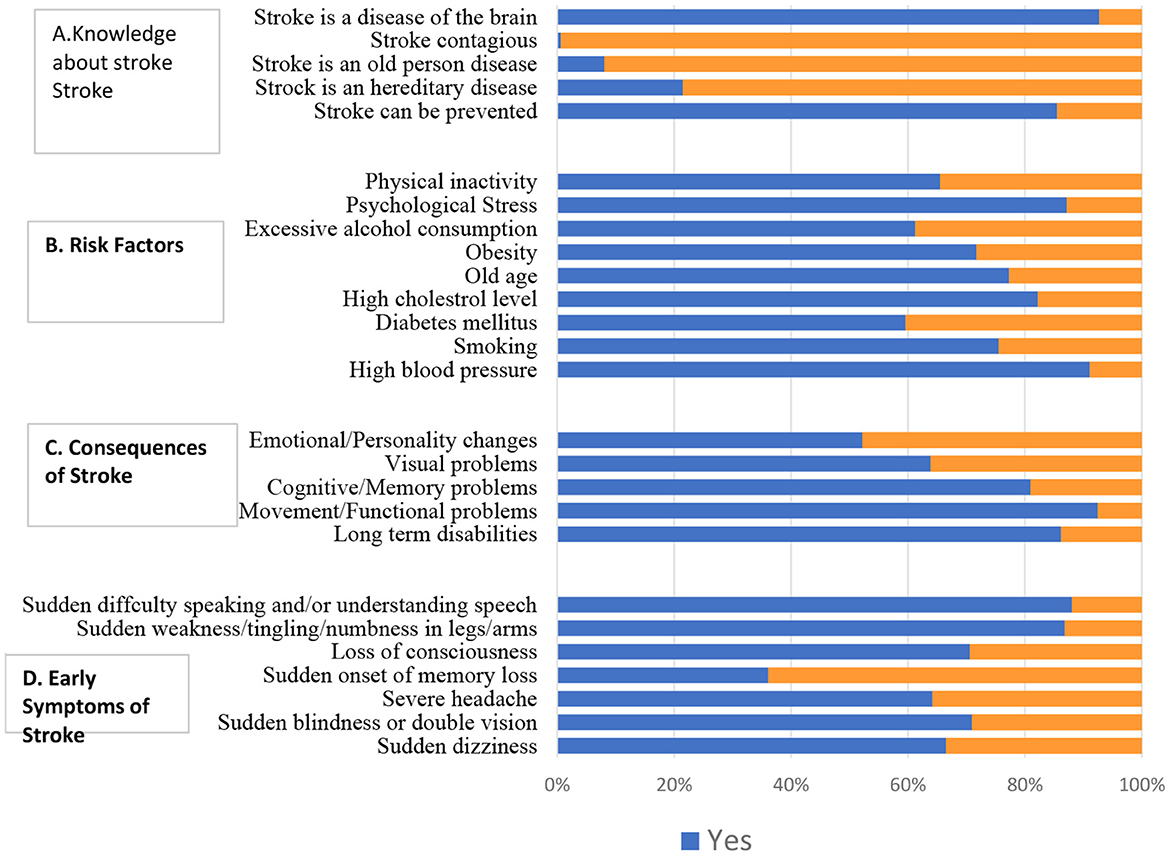
Figure 1. Knowledge among the participants (n = 609).
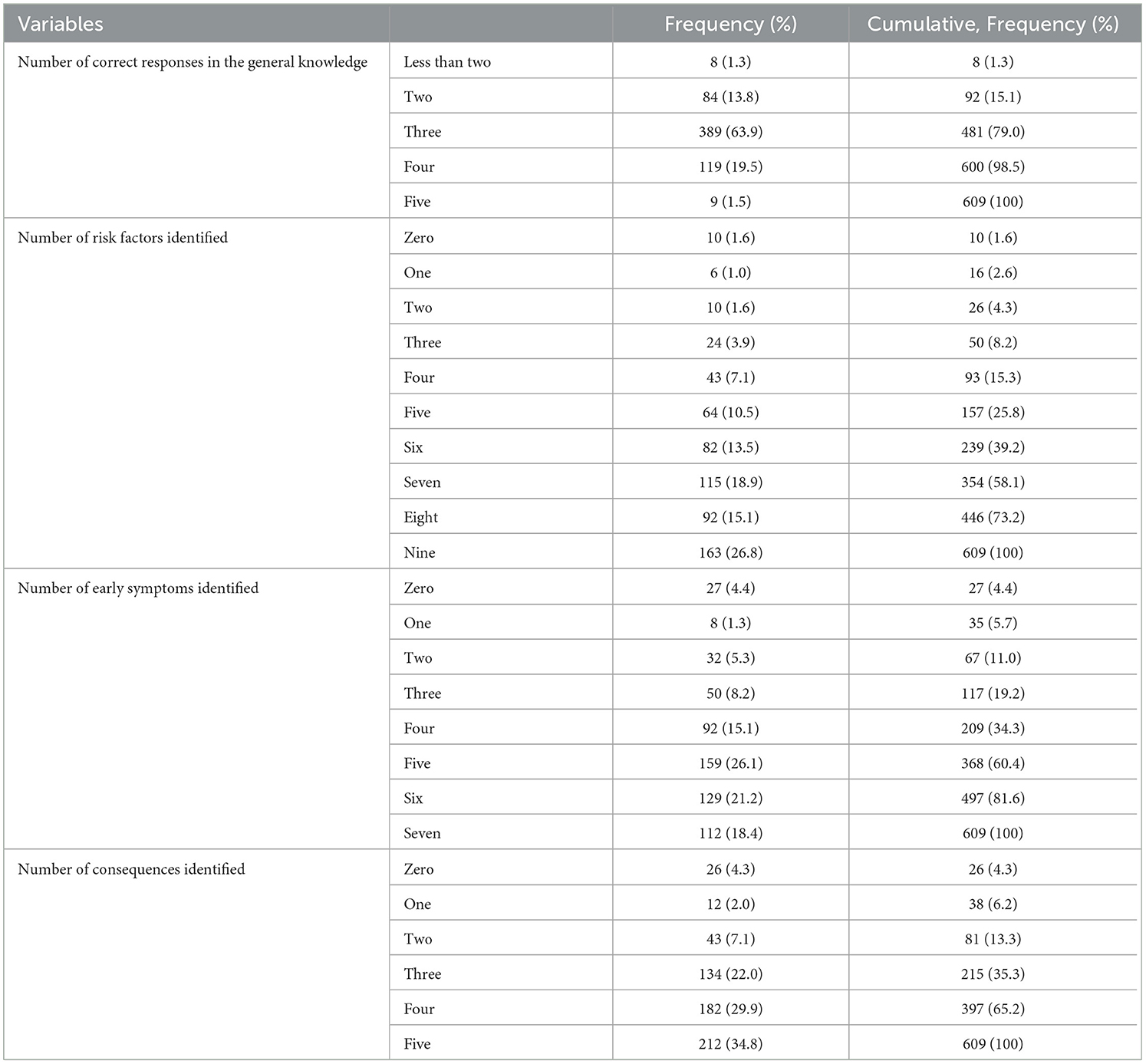
Table 2. Number of risk factors, early symptoms, and consequences identified by the participants (n = 609).
Regarding identifying stroke risk factors, only 26.8% identified all risk factors, 18.4% of the participants identified all symptoms, and 34.8% reported all possible consequences of stroke. The primary sources of information were the Internet/social media (35.0%), healthcare professionals (25.6%), and family/relatives (25.1%) (Figure 2).
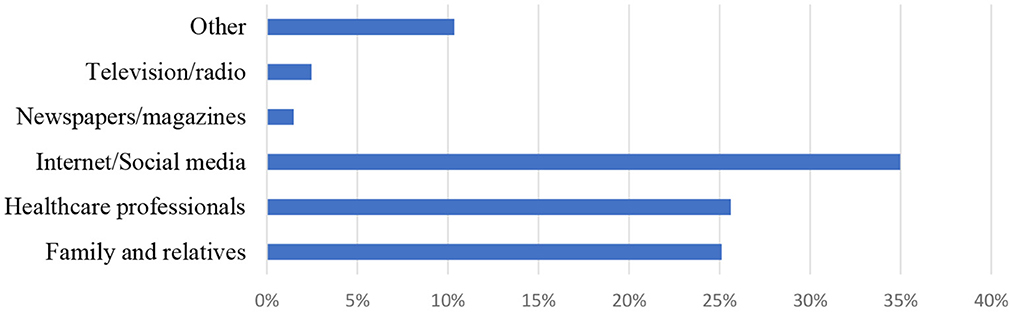
Figure 2. Sources of information (%) related to stroke among the participants (n = 609).
About a quarter of participants (26.6%) believed that they did not know stroke's effects well. However, the majority of the participants (91.1%) were curious to have more information related to stroke, including symptoms, emergency signs, and response when facing someone with a stroke attack and the consequences of the stroke. In addition, most participants (97.2%) believed that the role of the family is essential in providing care to a patient with a stroke at an early stage. In addition, more than three-quarters of participants (77.8%) believed that stroke disease could make patients' lives unhappy.
3.3. Bivariate analysis
In the bivariate analysis, a significantly higher proportion of female participants than male participants (97.1% vs. 90.1%) recognized at least one warning symptom of stroke. Furthermore, the participants without a history of smoking vs. a positive history of smoking (96.7% vs. 88.4%) recognized at least one warning symptom of stroke. A significantly higher proportion of participants without a history of diabetes mellitus compared to patients diagnosed with diabetes (96.4% vs. 87.5%) correctly identified the consequences emerging from stroke (Table 3).
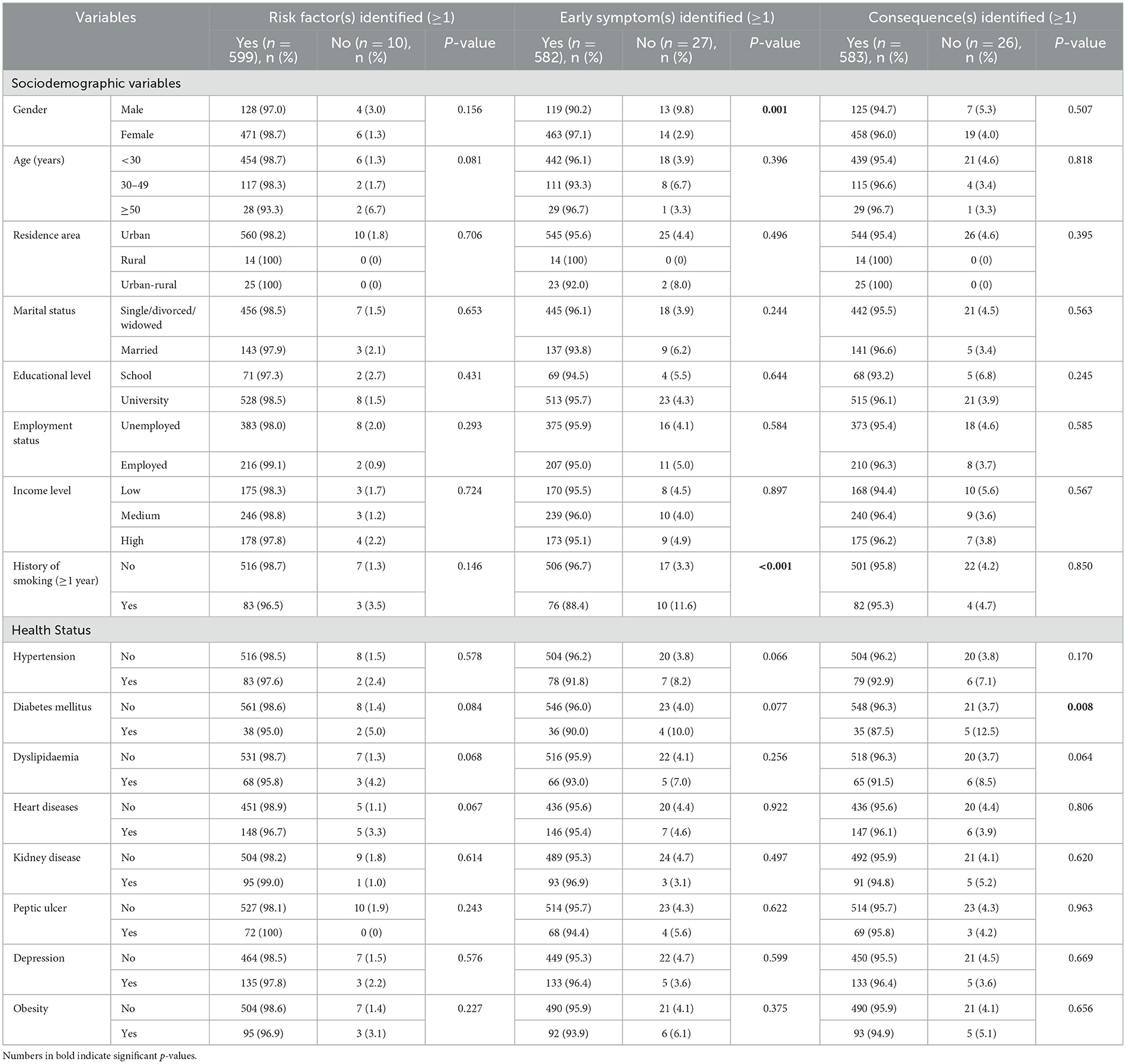
Table 3. Association of risk factors, early symptoms, and consequences of stroke with the sociodemographic variables and health status (n = 609).
3.4. Response to somebody with symptoms of stroke
The majority of participants (88.7%) reported that their first action in response to witnessing a patient with stroke symptoms was to take the patient directly to a hospital; the reset was either calling the doctor (5.42%) or not knowing what to do 5.91%. Regarding the response in case of facing somebody with acute stroke symptoms by taking them to the hospital, a significantly higher proportion of single participants compared to married responded by taking the patient to the hospital (90.3% vs. 83.6%, p = 0.026). Furthermore, the number of correct answers was associated with people with no history of hypertension compared to those having hypertension (90.3% vs. 78.8%, p = 0.002), people with no history of diabetes compared to those having diabetes (90.0% vs. 70.0%, p < 0.001), and people with no history of dyslipidemia compared to having dyslipidemia (89.6% vs. 81.7%, p = 0.048) (Table 4).
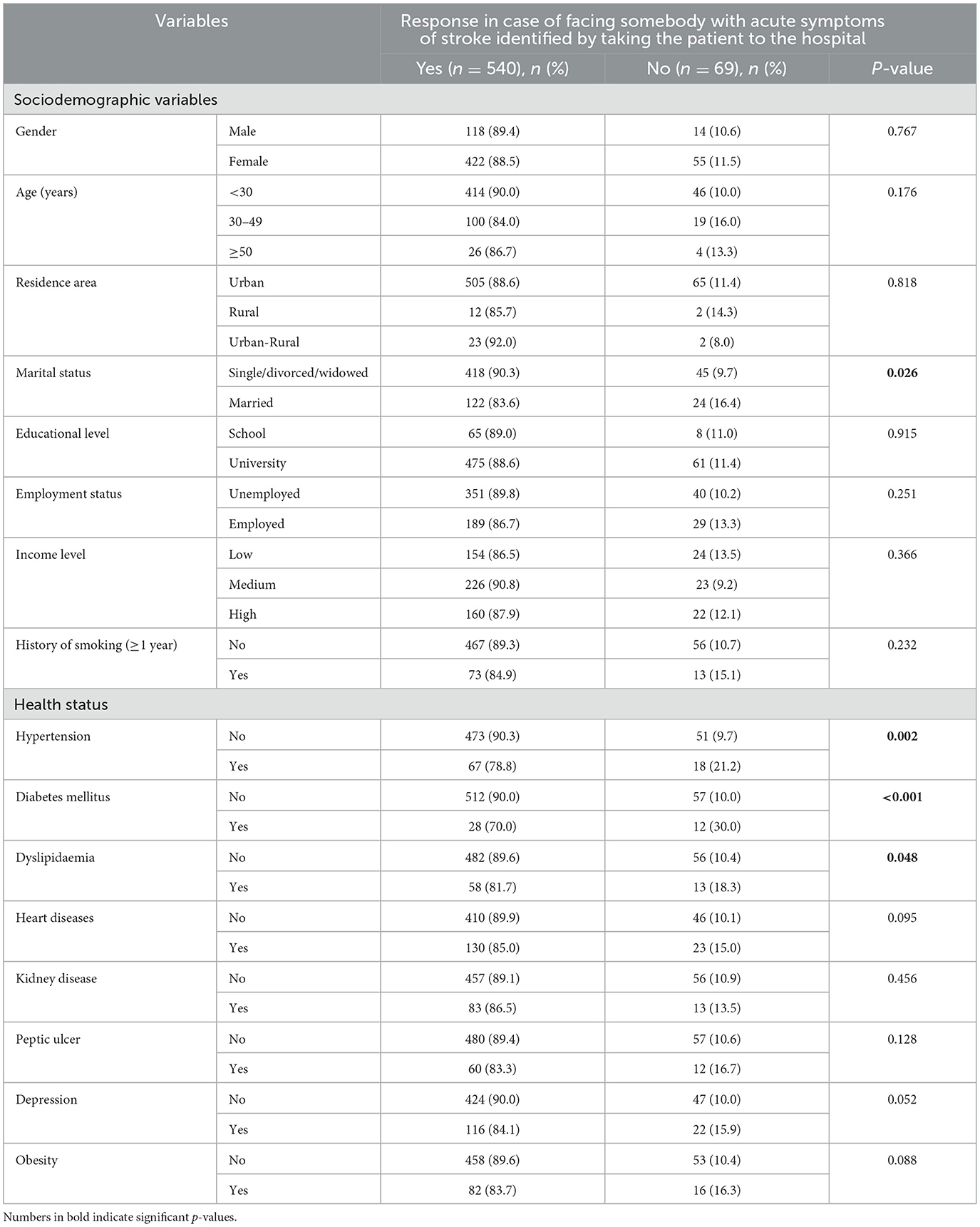
Table 4. Association of response in case of facing somebody with acute symptoms of a stroke (identified by taking the patient to the hospital) and with sociodemographic variables and health status of the participants (n = 609).
3.5. Multivariable analysis
The multivariable analysis demonstrated that female participants were more likely than male participants to identify a risk factor when recognizing at least one risk factor as the dependent variable (OR = 2.5, p-value of 0.047). Moreover, smokers were less likely to name a risk factor than non-smokers (OR = 0.38, p-value of 0.044). Diabetic patients exhibited significantly lower odds of recognizing stroke symptoms than non-diabetic patients (OR = 0.35), with a p-value of 0.024 when the response to stroke symptoms discovered through bringing the patient to the hospital was the dependent variable (Table 5).

Table 5. Multivariate analysis of associations between sociodemographic data of the participants (n = 609) and identification of risk factors, early symptoms, consequences of stroke, and taking a patient to a hospital.
4. Discussion
The study evaluated knowledge of stroke among a sample of the general Iraqi community. Nearly every participant had heard about stroke. Nonetheless, the findings revealed that 21.0% of participants had 75% of the right answers concerning stroke, 60.8% had identified risk factors, 39.6% had identified early symptoms, and 64.5% had recognized the effects of the disease. The percentages of correct responses, however, are higher than those seen in numerous other studies conducted internationally among the general population (22–27), indicating that more than half of the sample may be able to identify at least one stroke risk factor. The high awareness toward stroke and its associated elements in our study may be explained by the fact that the majority of the study participants are young and have high level of education.
The results revealed that hypertension and psychological stress were the most well-known risk factors for stroke in nearly 90% of the participants. This is higher than results reported in other studies on the general population conducted in several countries (25, 28, 29). However, similarities were found in other studies conducted in Jordan and Lebanon (17, 19). Although diabetes is the most well-known risk factor for stroke, it was the lowest reported among the study participants (<60%). Similarly, another study found that approximately three-quarters of the sample did not identify diabetes as a risk factor for stroke (25). In the current study, the majority of participants (88.9%) understood the significance of getting to the hospital as soon as possible after a stroke was identified, which is consistent with other published findings demonstrating that a high percentage of participants understood the need for immediate medical care (2–4, 27). A key tactic in reducing mortality, enhancing prognosis, and limiting long-term sequelae is raising general public knowledge of the significance of early hospital presentation.
The results showed that female participants had better knowledge about the early symptom(s) identified (≥1) than male participants. However, several studies did not detect gender differences in the early symptom(s) identified (5, 27). Women tend to be more knowledgeable and might have a greater interest in health topics than men and take more time to seek information (6). Moreover, non-smokers outperformed smokers in terms of their understanding of early-detected symptoms (1). Yet, among study participants, there was no correlation with any other kind of knowledge. Diabetes patients showed higher awareness of the known effects of stroke and improved responsiveness when a stroke victim displayed symptoms by bringing the patient to the hospital. Furthermore, married participants and individuals with hypertension or dyslipidemia reported knowing this last statement better. There may be a strong indicator that individuals with chronic illnesses are more knowledgeable about strokes. However, the percentage of knowledgeable subjects was low because of other important factors, such as failure to recognize stroke warning symptoms, which sometimes induced hospital presentation delays and worsened stroke effects (6).
In light of these findings, awareness programs are required for the general Iraqi population, targeting people at particular risk of stroke. These programs should include educating people regarding the focus on the association of symptoms of stroke, the potential severity of the disease, and how avoiding delays in visiting the hospital correlates with a more favorable prognosis.
4.1. Clinical implications
The study added interesting data about stroke disease awareness to the literature, highlighting the lack of knowledge regarding stroke and related issues among the Iraqi population. Several factors influenced knowledge about stroke among Iraqi participants, such as previous medical history with chronic diseases, marital status, gender, and history of smoking.
4.2. Limitations
This study has several limitations. The results could not be representative of the entire Iraqi population as the majority of participants were well-educated with computer literacy and internet access; thus, less-educated people and those who did not have access to the internet were not assessed. Thus, selection bias plays a role in our study because the study targeted educated urban people and involved snowball sampling. Additionally, its cross-sectional design cannot infer causality. Information bias could also exist as the study questionnaire was online and answers were self-reported. The answers to stroke awareness might be overestimated because the questionnaire used consisted of multiple-choice questions with limited options available; thus, the participants could have guessed the answers.
5. Conclusion
There was a lack of knowledge of the risk factors for stroke among the Iraqi participants. Health status with chronic disease, female gender, married status, and smoking history was associated with good knowledge to identify some stroke-related issues. Knowledge and awareness among the Iraqi people regarding stroke risk factors, symptoms, complications, and actions to treat stroke patients should be addressed as an essential effect of reducing stroke mortality and morbidity.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Research Ethics Committee at the University of Baghdad [SA 3/6502]. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HA-O, FJ, DM, and SH: conceptualization. HA-O and ZaK: project administration. SH and CH: formal analysis. DM: investigation. HA-O, FJ, DM, and HH: methodology. HA-O, ZaK, FJ, MB, HA, ZeK, YA, CH, and SM: writing the original draft. DM, SH, and HH: reviewing and editing. All authors read and approved the final manuscript.
Acknowledgments
The authors would like to thank the participants who joined this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liu D, Ahmet A, Ward L, Krishnamoorthy P, Mandelcorn ED, Leigh R, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy, asthma, and clinical immunology. J Can Soc Allergy Clin Immunol. (2013) 9:30. doi: 10.1186/1710-1492-9-30
2. National Institutes of Health (NIH). COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. (2022). Available online at: https://www.covid19treatmentguidelines.nih.gov/ (accessed March 6, 2023).
3. Buchman AL, Side. effects of corticosteroid therapy. J Clin Gastroenterol. (2001) 33:289–94. doi: 10.1097/00004836-200110000-00006
4. Li AW, Yin ES, Antaya RJ. Topical corticosteroid phobia in atopic dermatitis: a systematic review. JAMA Dermatol. (2017) 153:1036–42. doi: 10.1001/jamadermatol.2017.2437
5. Saqib A, Atif M, Ikram R, Riaz F, Abubakar M, Scahill S. Factors affecting patients' knowledge about dispensed medicines: a Qualitative study of healthcare professionals and patients in Pakistan. PLoS ONE. (2018) 13:e0197482. doi: 10.1371/journal.pone.0197482
6. Mueller SM, Itin P, Vogt DR, Walter M, Lang U, Griffin LL, et al. Assessment of “corticophobia” as an indicator of non-adherence to topical corticosteroids: a pilot study. J Dermatolog Treat. (2017) 28:104–11. doi: 10.1080/09546634.2016.1201189
7. Alsukait SF, Alshamlan NM, Alhalees ZZ, Alsuwaidan SN, Alajlan AM. Topical corticosteroids knowledge, attitudes, and practices of primary care physicians. Saudi Med J. (2017) 38:662–5. doi: 10.15537/smj.2017.6.17586
8. Sekler O, Segev-Becker A, Interator H, Brener A, Schachter-Davidov A, Elkon-Tamir E, et al. Paediatricians' practices and knowledge of corticosteroids: a national survey. Acta Paediatrica. (2021) 110:711–7. doi: 10.1111/apa.15481
9. El Hachem M, Gesualdo F, Ricci G, Diociaiuti A, Giraldi L, Ametrano O, et al. Topical corticosteroid phobia in parents of pediatric patients with atopic dermatitis: a multicentre survey. Ital J Pediatr. (2017) 43:22. doi: 10.1186/s13052-017-0330-7
10. Moawad S, Mahé E, Aubert-Wastiaux H, Phan A, Maruani A, Chiaverini C, et al. Topical corticosteroid concerns among parents of children with psoriasis versus atopic dermatitis: a French multicenter cross-sectional study. Am J Clin Dermatol. (2018) 19:261–5. doi: 10.1007/s40257-017-0318-5
11. Özçeker D, Uçkun U, Islamova D, Tamay Z, Güler N. Corticosteroid phobia among parents of asthmatic children. Turk J Pediatr. (2018) 60:142–6. doi: 10.24953/turkjped.2018.02.004
12. Yakar HI, Kanbay A. Evaluation of corticophobia in asthmatic patients. Niger J Clin Pract. (2020) 23:1033–8. doi: 10.4103/njcp.njcp_341_19
13. Ashique KT, Kaliyadan F, Mohan S, Vijayan S, Chandrasekhar D. Knowledge, attitudes and behavior regarding topical corticosteroids in a sample of pharmacy students: a cross sectional survey. Indian Dermatol Online J. (2018) 9:432–4. doi: 10.4103/idoj.IDOJ_143_18
14. Aubert-Wastiaux H, Moret L, Le Rhun A, Fontenoy AM, Nguyen JM, Leux C, et al. Topical corticosteroid phobia in atopic dermatitis: a study of its nature, origins and frequency. Br J Dermatol. (2011) 165:808–14. doi: 10.1111/j.1365-2133.2011.10449.x
15. van Paassen J, Vos JS, Hoekstra EM, Neumann KMI, Boot PC, Arbous SM. Corticosteroid use in COVID-19 patients: a systematic review and meta-analysis on clinical outcomes. Critical Care. (2020) 24:696. doi: 10.1186/s13054-020-03400-9
16. Chatterjee K, Wu C-P, Bhardwaj A, Siuba M. Steroids in COVID-19: an overview. Cleve Clin J Med. (2020) 8:1–4. doi: 10.3949/ccjm.87a.ccc059
17. Barakat M, AlSalamat HA, Jirjees F, Al-Obaidi H, El Hadidi S, Mansour S, et al. Factors associated with knowledge and awareness of stroke among the jordanian population: a cross-sectional study. F1000 Res. (2021) 10:492. doi: 10.12688/f1000research.74492.1
18. Ahmed AAA, Al-Shami AM, Jamshed S, Fata Nahas AR. Development of questionnaire on awareness and action towards symptoms and risk factors of heart attack and stroke among a Malaysian population. BMC Public Health. (2019) 19:1–10. doi: 10.1186/s12889-019-7596-1
19. Malaeb D, Dia N, Haddad C, Hallit S, Sacre H, Barakat M, et al. Factors associated with knowledge and awareness of stroke among the Lebanese population: a cross-sectional study. F1000 Res. (2022) 11:2. doi: 10.12688/f1000research.108734.2
20. Han CH, Kim H, Lee S, Chung JH. Knowledge and poor understanding factors of stroke and heart attack symptoms. Int J Environ Res Public Health. (2019) 16:3665. doi: 10.3390/ijerph16193665
21. Mickey RM, Greenland S. The impact of confounder selection criteria on effect estimation. Am J Epidemiol. (1989) 129:125–37. doi: 10.1093/oxfordjournals.aje.a115101
22. Shetty YC, Vinchurkar P, More S, Siddiqui A, Tilak S, Ginodia S, et al. Knowledge and awareness regarding corticosteroids and effectiveness of a novel steroid educational module among people visiting general OPD of a tertiary care hospital. Indian J Pharm Pract. (2022) 15:8. doi: 10.5530/ijopp.15.1.8
23. Sheth NK, Nair PA. Topical steroids: awareness and misuse among patients, pharmacists and general medical practitioner. Indian J Dermatol Venereol Leprol. (2021) 87:54–9. doi: 10.4103/ijdvl.IJDVL_84_18
24. Seo H, Song SY, Kim D, Park JH, Shin Y, Lee KH, et al. General public knowledge regarding topical corticosteroids: a nationwide survey in South Korea. Korean J Clin Pharm. (2022) 32:84–92. doi: 10.24304/kjcp.2022.32.2.84
25. Lau WM, Donyai P. Knowledge, attitude and advice-giving behaviour of community pharmacists regarding topical corticosteroids. Pharmacy. (2017) 5:41. doi: 10.3390/pharmacy5030041
26. Robert S. Community-level socioeconomic status effects on adult health. J Health Soc Behav. (1998) 3:18–37. doi: 10.2307/2676387
27. Case A, Lubotsky D, Paxson C. Economic status and health in childhood: the origins of the gradient. Am Econ Rev. (2002) 92:1308–34. doi: 10.1257/000282802762024520
28. Yuan F, Qian D, Huang C, Tian M, Xiang Y, He Z, et al. Analysis of awareness of health knowledge among rural residents in Western China. BMC Public Health. (2015) 15:55. doi: 10.1186/s12889-015-1393-2
Keywords: stroke, knowledge of stroke, awareness of stroke, symptoms of stroke, Iraq stroke, Iraq, factors associated
Citation: Al-Obaidi H, Khidhair Z, Jirjees F, Barakat M, AlSalamat H, Kharaba Z, Alfoteih Y, Haddad C, Mansour S, Hallit S, Malaeb D and Hosseini H (2023) Factors associated with knowledge and awareness of stroke in the Iraqi population: a cross-sectional study. Front. Neurol. 14:1144481. doi: 10.3389/fneur.2023.1144481
Received: 14 January 2023; Accepted: 20 March 2023;
Published: 18 April 2023.
Edited by:
Patricia Martínez Sánchez, Torrecárdenas University Hospital, SpainReviewed by:
Sachin Sureshbabu, Meitra Hospital, IndiaAswi Aswi, State University of Makassar, Indonesia
Copyright © 2023 Al-Obaidi, Khidhair, Jirjees, Barakat, AlSalamat, Kharaba, Alfoteih, Haddad, Mansour, Hallit, Malaeb and Hosseini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diana Malaeb, ZHIuZGlhbmFAZ211LmFjLmFl
†These authors have contributed equally to this work and share first authorship
‡These authors share last authorship
§ORCID: Souheil Hallit orcid.org/0000-0001-6918-5689