 Jeffrey Cummings1*
Jeffrey Cummings1* Julie Hviid Hahn-Pedersen2
Julie Hviid Hahn-Pedersen2 Christian Stefan Eichinger3
Christian Stefan Eichinger3 Caroline Freeman3
Caroline Freeman3 Alice Clark2
Alice Clark2 Luis Rafael Solís Tarazona2
Luis Rafael Solís Tarazona2 Krista Lanctôt4,5
Krista Lanctôt4,5- 1Chambers-Grundy Center for Transformative Neuroscience, Department of Brain Health, School of Integrated Health Sciences, University of Nevada, Las Vegas, NV, United States
- 2Novo Nordisk A/S, Søborg, Denmark
- 3Oxford PharmaGenesis, Oxford, United Kingdom
- 4Hurvitz Brain Sciences Program, Sunnybrook Research Institute, Toronto, ON, Canada
- 5Department of Psychiatry, University of Toronto, Toronto, ON, Canada
Background: People with Alzheimer’s disease (AD) have difficulties in performing activities of daily living (ADLs) as the disease progresses, commonly experience neuropsychiatric symptoms (NPS), and often have comorbidities such as cardiovascular disease. These factors all contribute to a requirement for care and considerable healthcare costs in AD. The Clinical Dementia Rating (CDR) scale is a widely used measure of dementia staging, but the correlations between scores on this scale and patient-/care partner-relevant outcomes have not been characterized fully. We conducted a systematic literature review to address this evidence gap.
Methods: Embase, MEDLINE, and the Cochrane Library were searched September 13, 2022, to identify published studies (no restriction by date or country) in populations with mild cognitive impairment due to AD or AD dementia. Studies of interest reported data on the relationships between CDR Global or CDR–Sum of Boxes (CDR-SB) scores and outcomes including NPS, comorbidities, ADLs, nursing home placement, healthcare costs, and resource use.
Results: Overall, 58 studies met the inclusion criteria (42 focusing on comorbidities, 14 on ADLs or dependence, five on nursing home placement, and six on economic outcomes). CDR/CDR-SB scores were correlated with the frequency of multiple NPS and with total scores on the Neuropsychiatric Inventory. For cardiovascular comorbidities, no single risk factor was consistently linked to AD progression. Increasing CDR/CDR-SB scores were correlated with decline in multiple different measures of ADLs and were also associated with nursing home placement and increasing costs of care.
Conclusion: NPS, ADLs, and costs of care are clearly linked to AD progression, as measured using CDR Global or CDR-SB scores, from the earliest stages of disease. This indicates that scores derived from the CDR are a meaningful way to describe the severity and burden of AD for patients and care partners across disease stages.
1. Introduction
In Alzheimer’s disease (AD), ongoing cognitive decline leads to difficulties in performing instrumental activities of daily living (IADLs), such as meal preparation, shopping, and household tasks, and ultimately to inability to perform basic activities of daily living (ADLs) such as dressing, bathing, and eating (1). AD is also associated with neuropsychiatric symptoms (NPS), which may manifest at early stages of the disease. Symptoms such as depression and apathy can herald the onset of the disease, with other NPS such as delusions and hallucinations typically appearing at advanced stages (2).
With increasing impairment in ADLs and mounting behavioral changes, people with AD require more care as the disease progresses. In many cases, a family member or spouse acts as a care partner for the individual affected by AD, but there may be a requirement for formal care, particularly in later disease stages (3). When care requirements cannot be met in the home, or when care partners are no longer able to act as the sole provider of care, individuals with AD may require admission to an assisted living residence, a nursing home, or other care facility (4).
AD is associated with considerable healthcare costs (5). The formal costs of AD are attributable in large part to the cost of nursing home placement; informal costs include care contributions made by care partners and employment opportunity losses (6, 7). AD is more prevalent with advancing age (8), and many patients have comorbidities, which require the use of additional healthcare resources (9, 10). Comorbidities have been implicated in the development and progression of AD, although the causality of these relationships remain to be fully elucidated (11).
The Clinical Dementia Rating (CDR) scale is commonly used to define AD stages and disease progression in research settings and clinical trials, but it is infrequently used in clinical practice. CDR Global and CDR-Sum of Boxes (CDR-SB) scores are derived from severity scores in six domains (see Measurement scales in the Materials and methods section), with higher scores indicating more severe AD (12). The specific impacts of AD can be quantified using various patient-, physician-, or care partner-reported outcome measures, including ADL and IADL questionnaires, and the Neuropsychiatric Inventory (NPI), which is used to assess the type, severity, and number of NPS (13). The relationships between these measures and the CDR scale, and their impact on costs as patients progress through AD stages, are incompletely characterized. A deeper understanding of these associations is vital to understand how CDR-SB and CDR Global scores relate to outcomes in clinical practice and costs of care, and the extrapolation of clinical trial data. Quantifying the impacts of reaching a particular AD stage may help to identify the potential benefits of interventions that slow progression and allow assessment of the economic impact of treatment-related changes.
We conducted a systematic literature review (SLR) to assess how comorbidities, NPS, ADL declines, nursing home placement, and economic costs are linked to AD severity and progression, as measured by CDR Global or CDR-SB scores.
2. Materials and methods
2.1. Systematic literature review
The SLR was designed to identify relevant evidence in populations with AD (both mild cognitive impairment [MCI] due to AD and AD dementia), on the relationship between CDR-SB or CDR Global scores and outcomes. All study types, including randomized controlled trials (RCTs), observational studies, and case studies and reports, were considered relevant. Following consultation with a panel of clinical experts, outcomes of specific interest were NPS, cardiovascular disease (CVD), epilepsy, bedsores, infections, incontinence, obstructive sleep apnea, falls, ADLs, dependence, nursing home placement, economic consequences, and healthcare resource use.
Both journal and congress publications were considered relevant. Primary publications and SLRs or meta-analyses were included, but narrative reviews were not. Only English language publications were included, but there was no restriction by date or geography.
The study protocol was designed and conducted in line with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (14), and registered with PROSPERO (registration number: CRD42023392801). Searches of Embase, MEDLINE, and the Cochrane Library were conducted on September 13, 2022. Titles and abstracts were screened by one reviewer to determine whether they met the eligibility criteria (Table 1). All publications meeting the criteria were obtained as full articles and reassessed against the eligibility criteria.
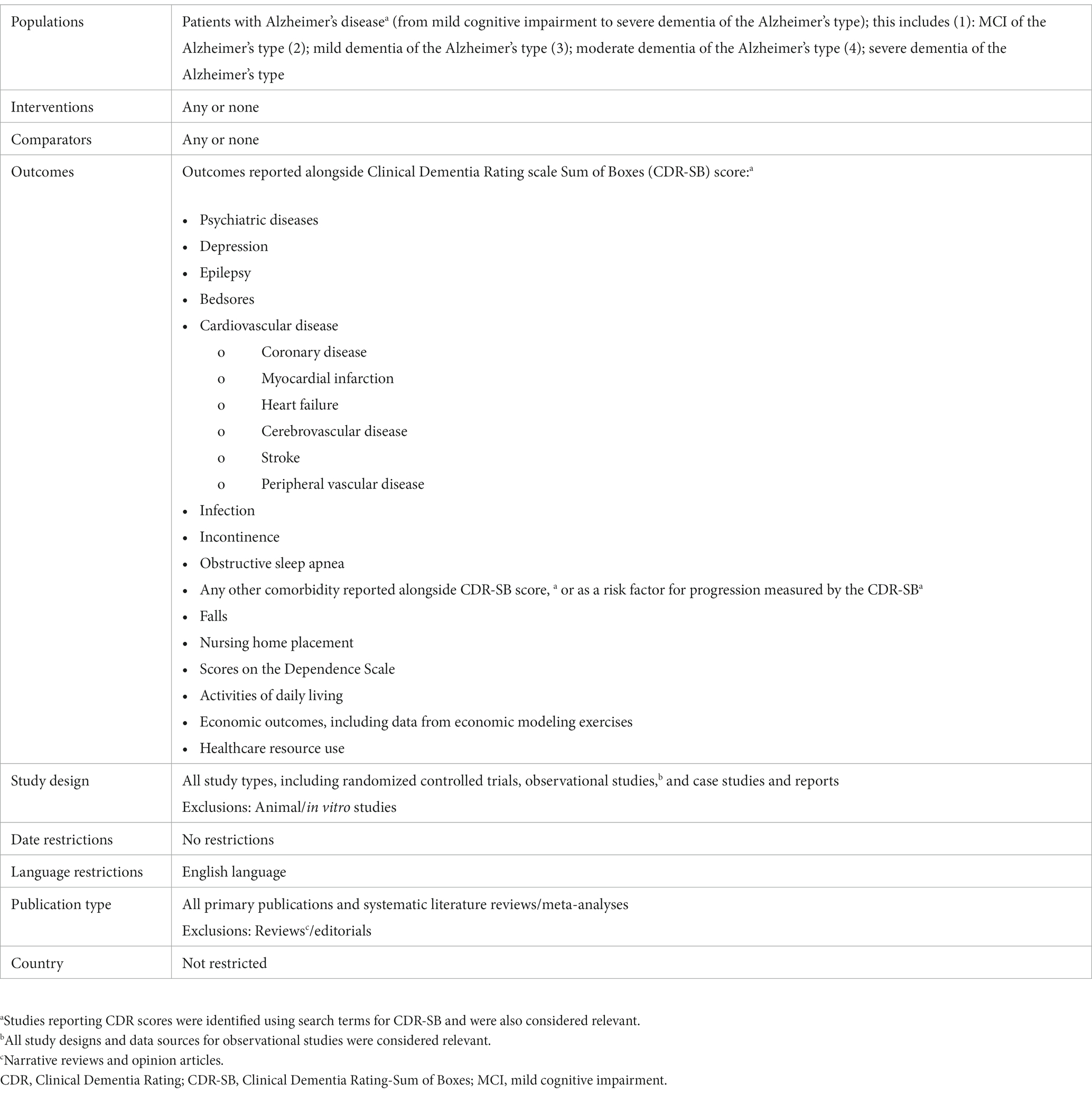
Table 1. Eligibility criteria for the systematic literature review.
2.2. Data extraction
Detailed data, including study setting, methods, patient characteristics, and study results, were entered into a data extraction table, and quality checked by an independent reviewer.
Some studies reported longitudinal relationships between CDR-SB/CDR score progression and the progression of outcomes, whereas others reported cross-sectional data examining outcomes in different stages of AD severity. A third type of study reported how disease severity at baseline affected subsequent progression or how baseline characteristics affected AD progression.
2.3. Measurement scales
The CDR scale comprises six domains: memory, orientation, judgement and problem solving, community affairs, home and hobbies, and personal care (12), each of which is assigned a score of 0, 0.5, 1.0, 2.0, or 3.0.
CDR Global scores (referred to hereafter throughout this review as CDR scores for brevity) reflecting dementia severity, are calculated from the domain scores using an algorithm, which generates the following categories of severity:
• CDR 0 – no dementia
• CDR 0.5 – questionable dementia (can also be classified as MCI)
• CDR 1.0 – mild dementia
• CDR 2.0 – moderate dementia
• CDR 3.0 – severe dementia.
The CDR-SB score is derived by adding the scores of the six domains; the total score ranges between 0 and 18 (12).
The original 10-item version of the NPI (15) includes delusions, hallucinations, agitation/aggression, depression, anxiety, euphoria, apathy, disinhibition, irritability, and motor disturbances (13); night-time behavior disturbances, and appetite and eating abnormalities were later added (16). Each of the 12 items is scored on scales for frequency (1–4), severity (0–3), and distress (0–5). Individual scores for each domain are calculated as frequency × severity, and the total NPI score is the sum of the domain scores (13).
Various measures to assess ADLs and IADLs are used in AD research and clinical practice. Table 2 summarizes the scales included in this manuscript.
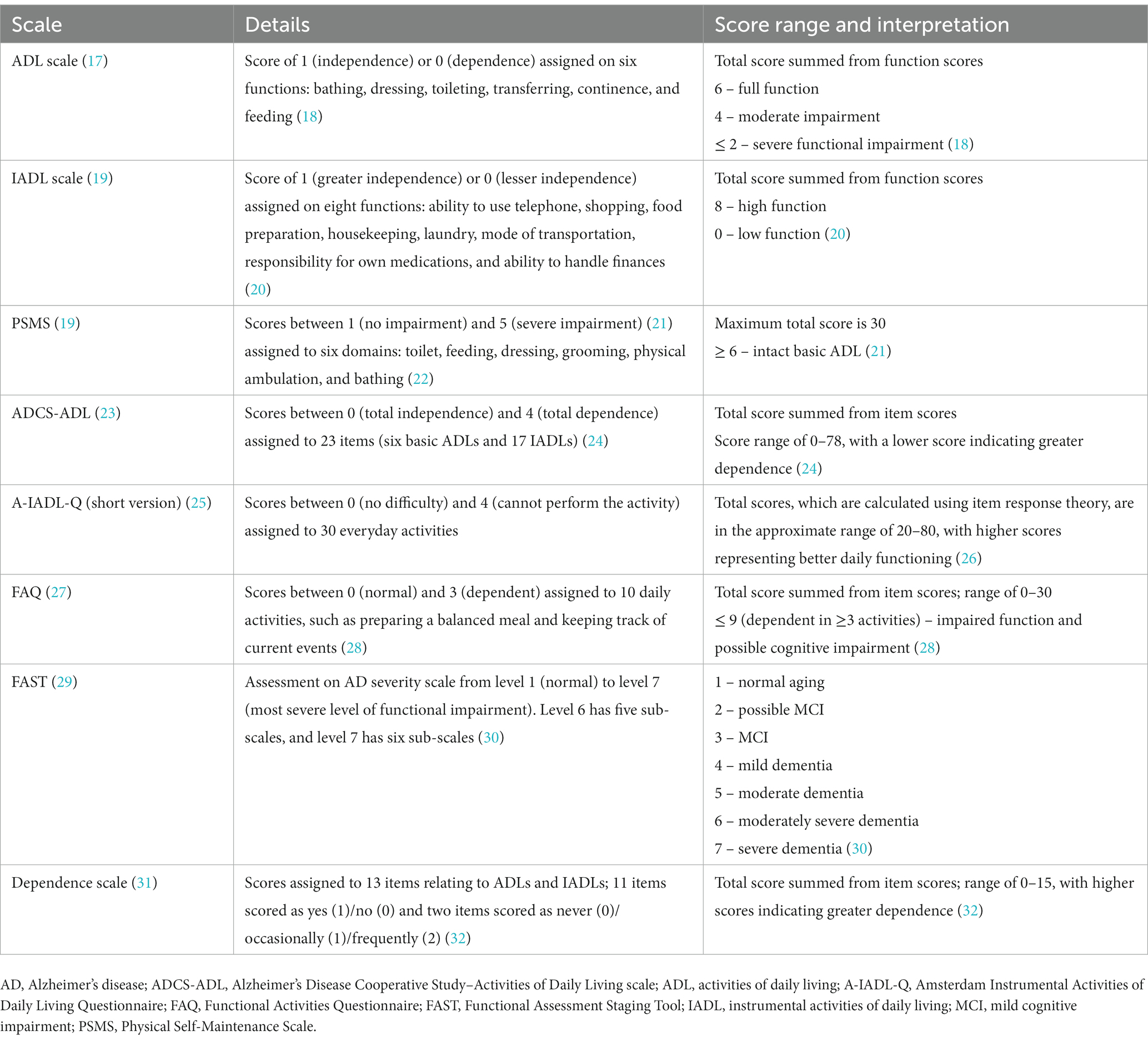
Table 2. Summary of relevant ADL measurement scales.
3. Results
3.1. Search results
In total, 925 references were included for screening by abstract and title, resulting in 125 references included for full paper review (see Figure 1 for PRISMA flow diagram). In total, 57 references met the inclusion criteria at full paper review and were included for data extraction, along with one additional relevant reference that was identified in supplementary searches, resulting in 58 studies in total. Overall, 42 studies reported data on comorbidities (33–74), Twelve studies reported data on ADLs (21, 38, 49, 53, 62, 65, 67, 68, 75–78), two reported data on dependence (79, 80), five reported data on nursing home placement (68, 81–84), and six reported data on economic outcomes or resource use (68, 85–89). No studies reported data on bedsores, infections, obstructive sleep apnea, or falls.
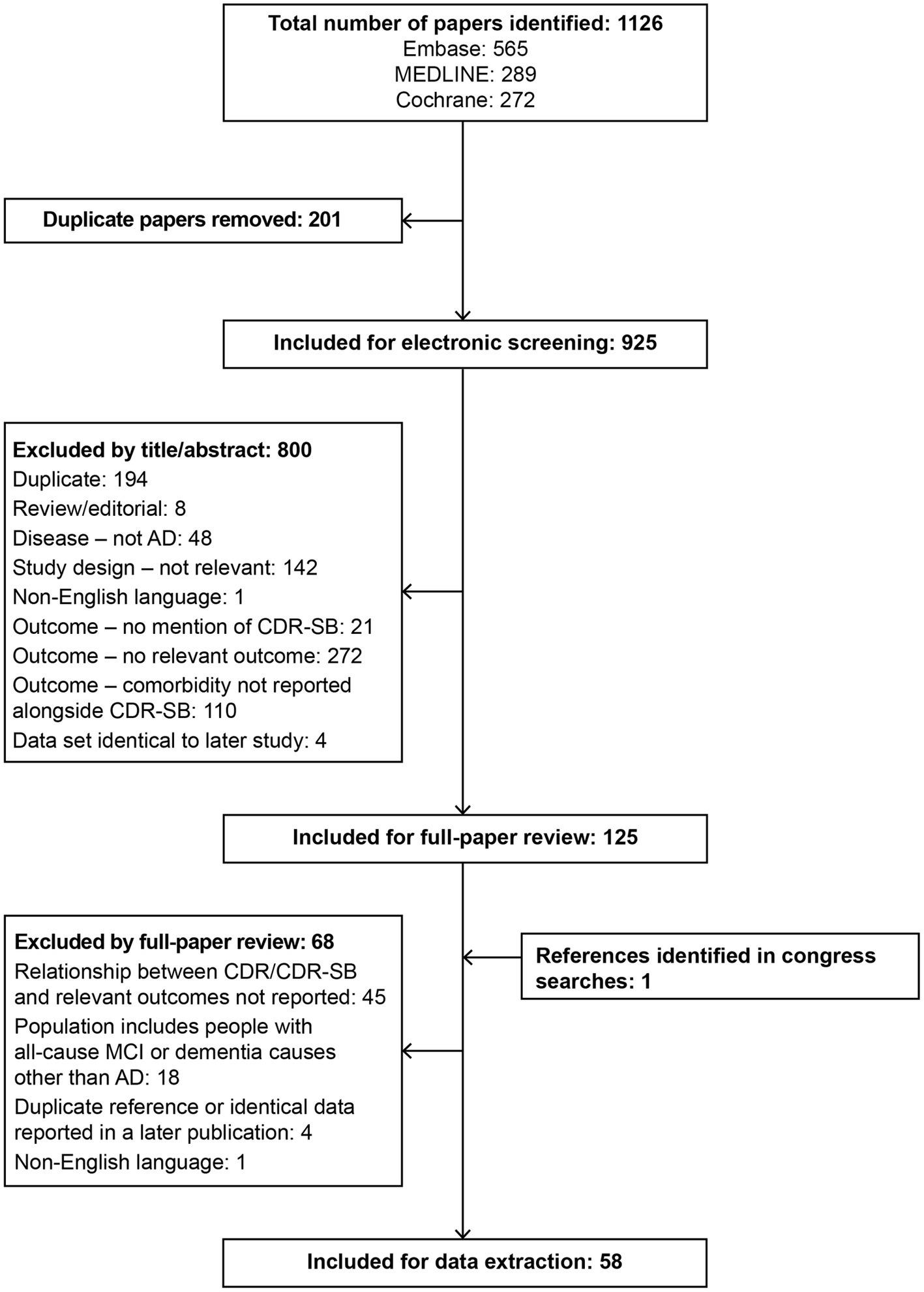
Figure 1. PRISMA diagram for the SLR. AD, Alzheimer’s disease; CDR, Clinical Dementia Rating; CDR-SB, Clinical Dementia Rating–Sum of Boxes; MCI, mild cognitive impairment; SLR, systematic literature review.
3.2. Data sources and study characteristics
Nineteen studies reported data from Asia (China, India, Japan, Singapore, South Korea, Taiwan, and Thailand) (33, 38, 40–43, 57, 58, 60, 61, 63, 67, 73, 74, 76, 78, 82, 83, 87), 17 reported data from Europe (Finland, France, Germany, Italy, Norway, Spain, Turkey, and the UK) (34–37, 39, 44, 48–50, 53, 54, 56, 62, 80, 85, 88, 89), and 12 reported data from North America, all of which were from the USA (21, 51, 52, 55, 59, 64, 65, 68–72). Five studies reported data from multiple countries (75, 77, 79, 81, 86), three reported data from South America (Brazil) (45–47), and two publications did not report the country (66, 84). More than two-thirds of the studies used primary data (39 studies); the remainder were conducted using secondary data, with the exception of one study with an unclear design (80). Individuals with AD were typically recruited from memory clinics, neurology departments, or hospitals, or as part of cohort studies of ageing, dementia, or AD. A small number of studies analyzed data collected in RCTs.
3.3. AD diagnosis and staging
Most studies diagnosed AD according to standard clinical criteria, typically the National Institute of Neurological and Communicative Disorders and Stroke−Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria (90). However, only five studies (34, 49, 72, 75, 77) confirmed the diagnosis of AD using biomarkers. Four studies measured β-amyloid and/or tau in cerebrospinal fluid (34, 49, 75, 77), one of which detected amyloid deposits via positron emission tomography scans as an alternative method (75). The fifth study detected amyloid deposits using immunohistochemistry post mortem (72).
3.4. Comorbidities
3.4.1. Neuropsychiatric symptoms
Increasing AD severity, as measured using CDR or CDR-SB scores, was predictably linked to greater occurrence of NPS, but there was variation in which NPS were most closely associated with progression to more advanced stages of AD. Differences may be attributable in part to sample sizes, residential setting, comorbidities and concomitant medications, and data collection strategies.
Overall 22 studies reported data on NPS (33, 34, 36–39, 41, 42, 44, 53, 54, 56, 57, 62, 65–67, 69, 71–74), of which the majority used the NPI.
Figure 2 shows data from the studies that reported the prevalence of specific NPS by AD stage (37, 44, 57, 62, 74). The frequency of these symptoms and their link to disease severity differed across studies. For delusions, hallucinations, agitation/aggression, apathy, disinhibition, aberrant motor behavior, night-time behavior disturbances, and appetite and eating abnormalities, there was a stepwise relationship between prevalence and AD severity in most studies. For depression, anxiety, euphoria, and irritability, there were smaller differences in prevalence across AD stages.
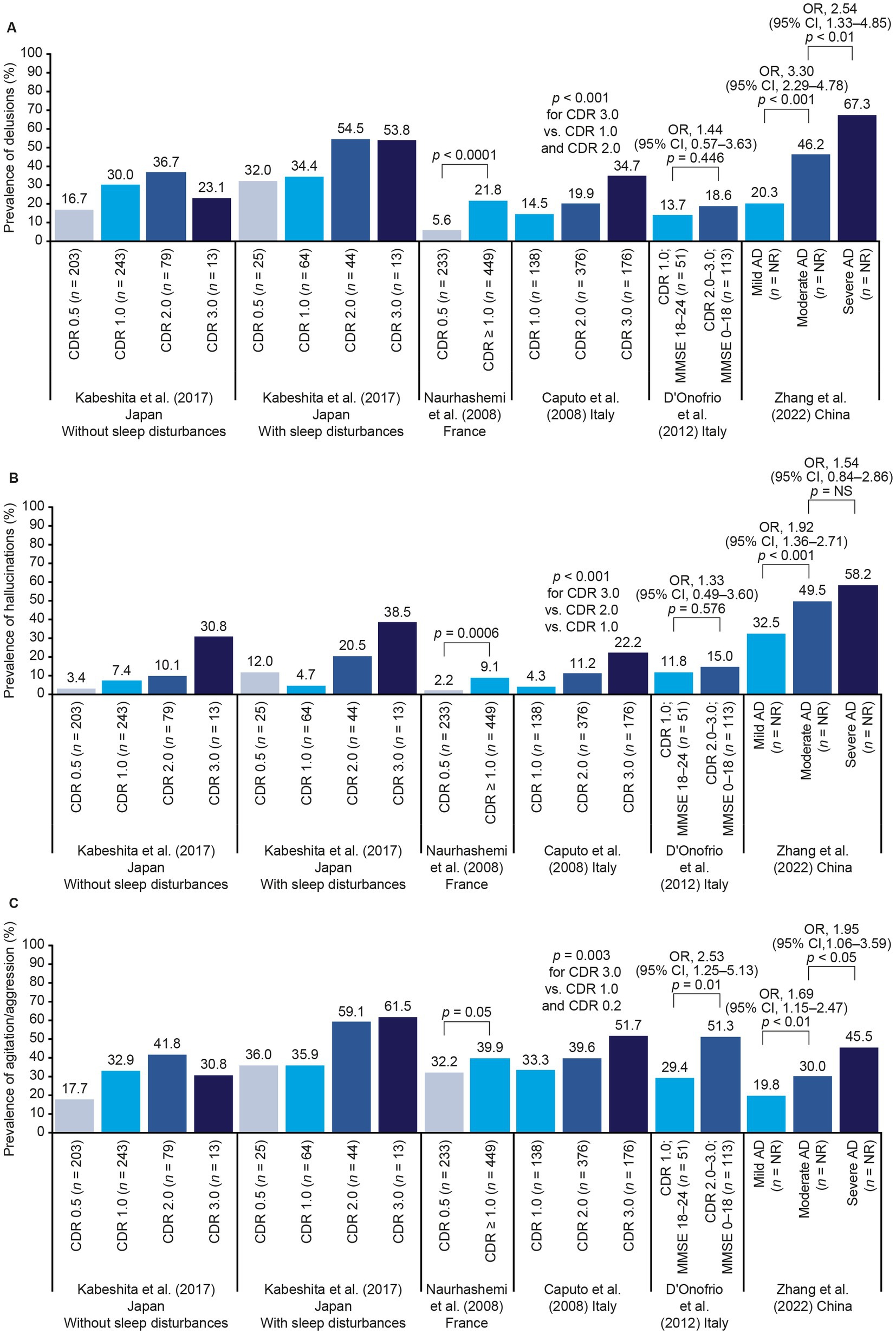
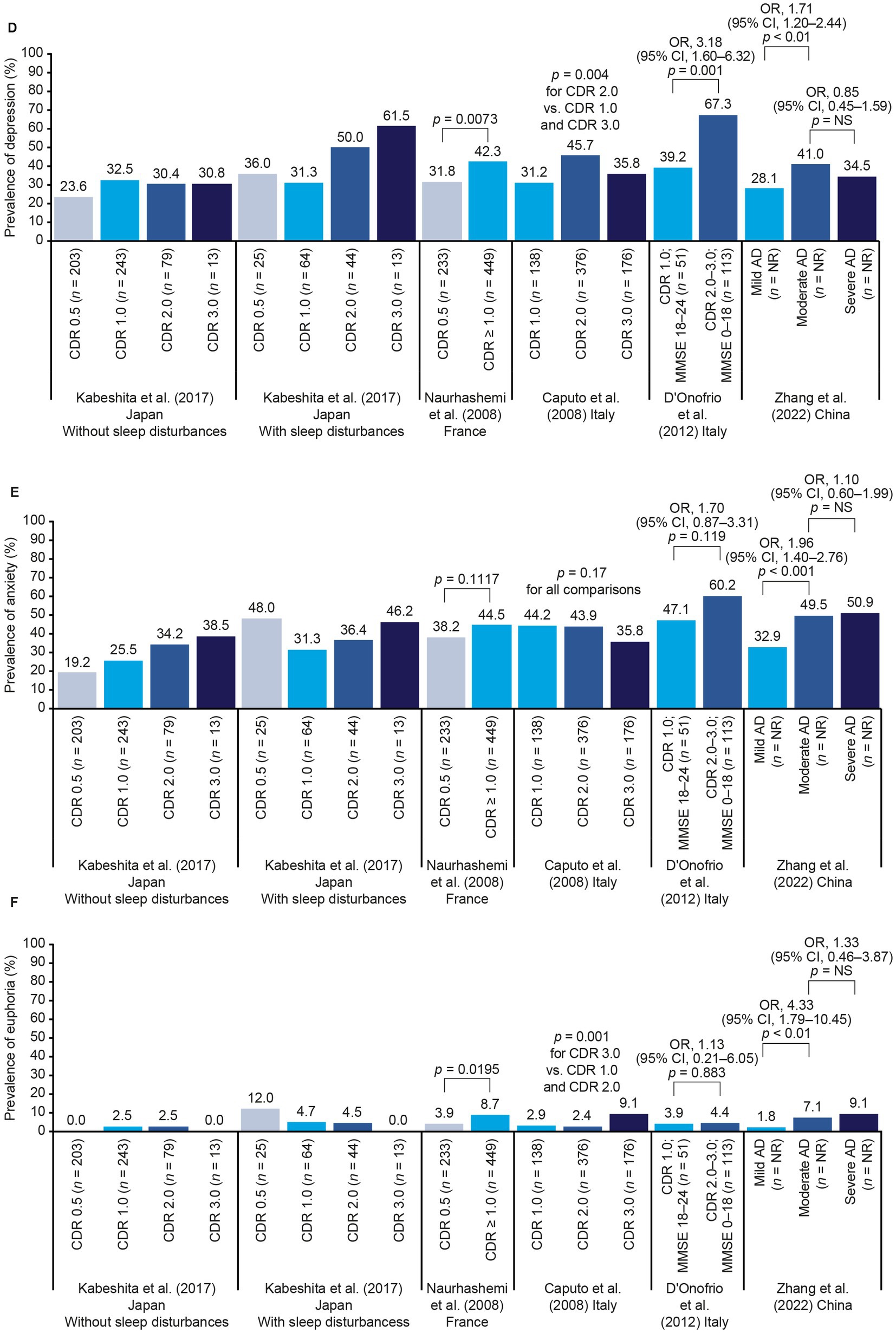
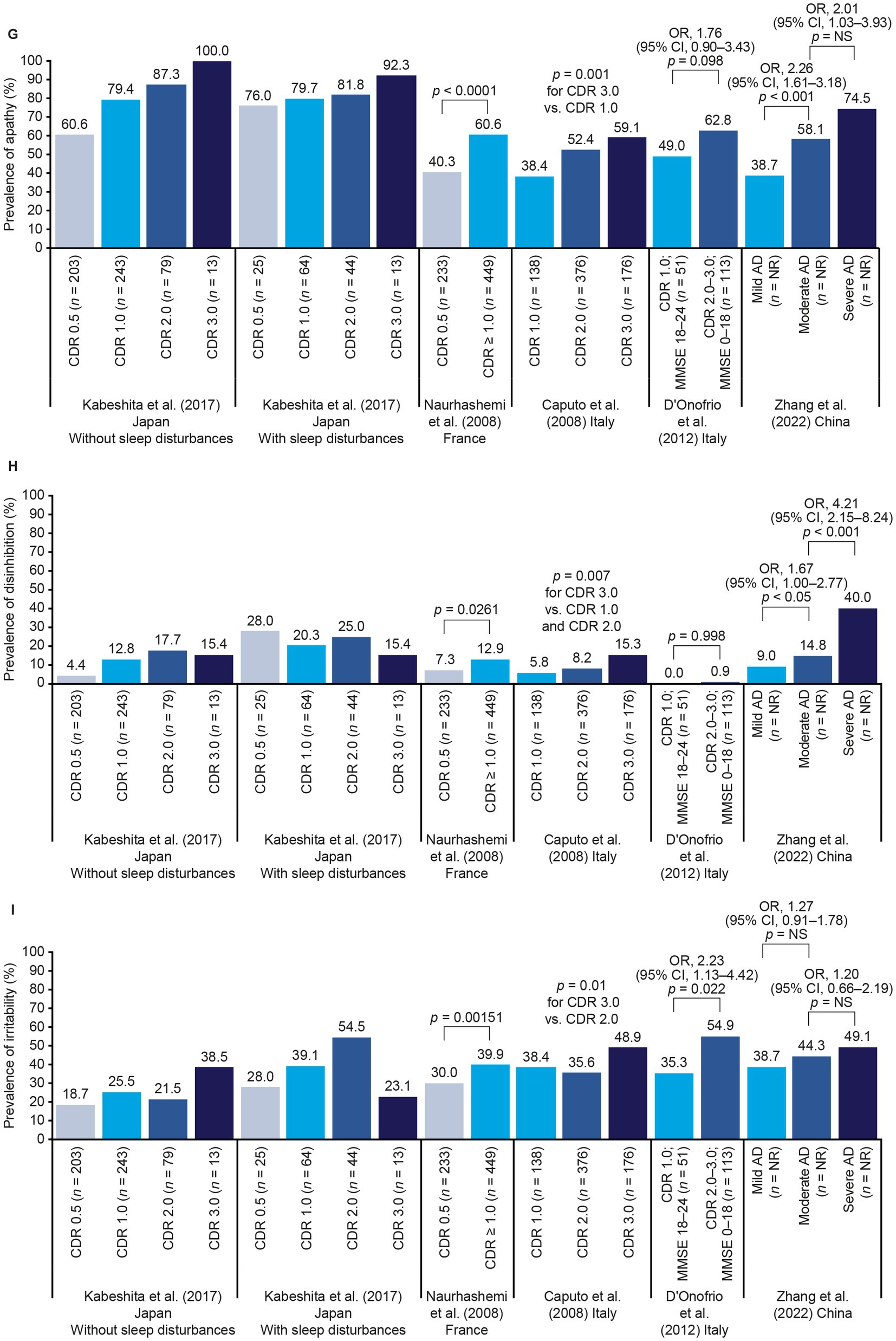
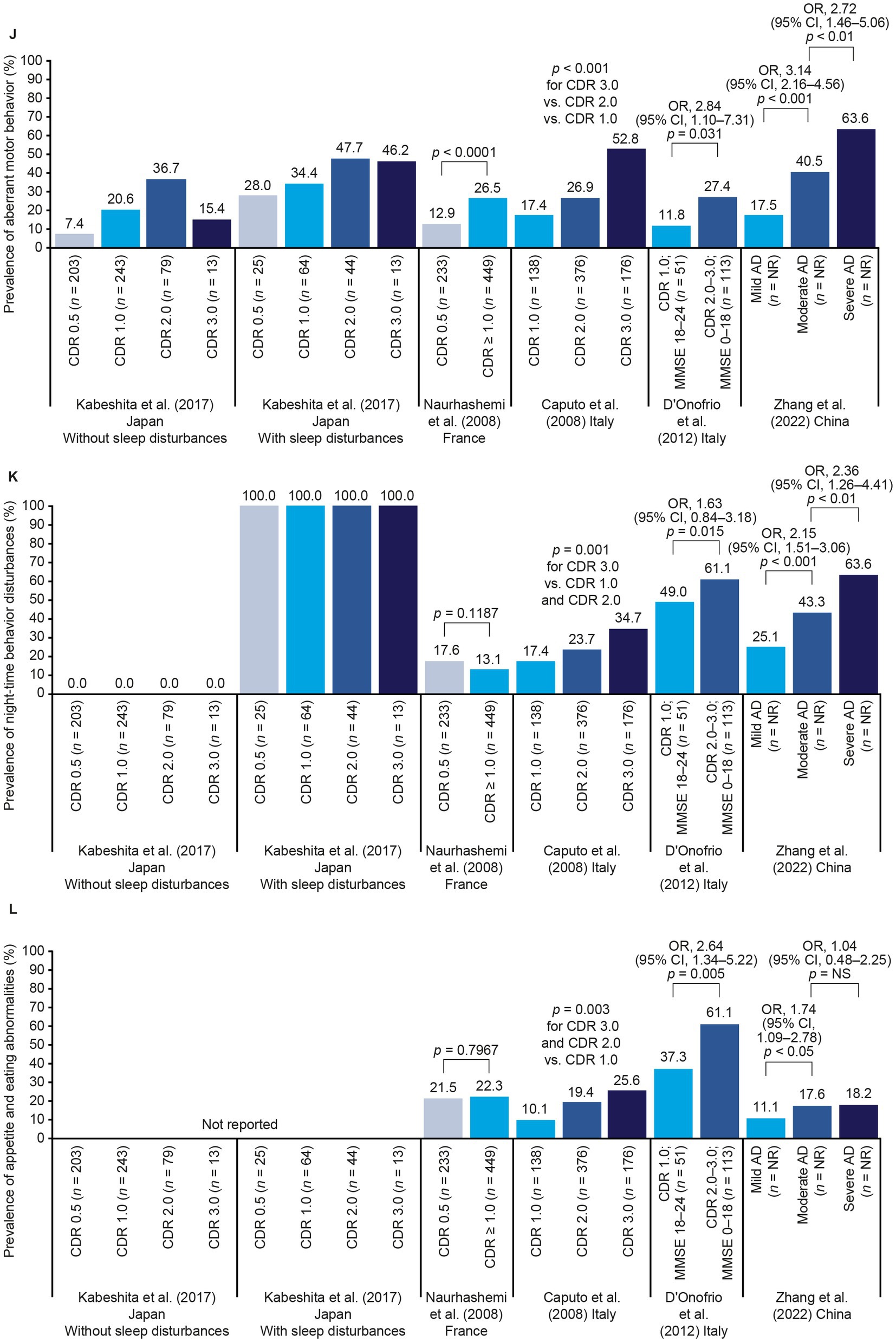
Figure 2. NPS frequency by AD stage. Panels (A–L) show data for each individual NPS (see labels on y-axes). Where p values are not shown, statistical tests were not conducted. p values across multiple categories represent tests of linear trends. Zhang et al. (74) used the CDR to determine disease severity, but did not specify exactly how each AD stage was defined (74). AD, Alzheimer’s disease; CDR, Clinical Dementia Rating; CI, confidence interval; MMSE, Mini Mental State Examination; NPS, neuropsychiatric symptom(s); NR, not reported; OR, odds ratio.
Another subset of studies reported links between NPS and disease progression (Supplementary Table 2). Barca et al. found that CDR-SB score and trajectories of depressive symptoms were correlated over time (34). Caroline et al. found that individuals with mild-to-moderate AD dementia who experienced fast CDR-SB score progression had a higher prevalence of delusions, depression, anxiety, apathy, and aberrant motor behavior at baseline than those with slow progression (38). Hallikainen et al. found that delusions and euphoria predicted AD progression, as measured using CDR-SB scores, in multivariate analyses, and AD severity during follow-up was associated with the longitudinal occurrence of hallucinations, delusions, agitation, apathy, aberrant motor behavior, and sleep and appetite disturbances (54). Some inconsistencies were noted among the studies identified. Wadsworth et al. found that CDR-SB scores were associated only with apathy at baseline and were not associated with any NPS over follow-up (71), and Breitve et al. found no link between CDR or CDR-SB scores and patient-or care partner-reported anxiety (36).
Charernboon et al. found that people with higher CDR scores tended to have significantly more NPS than those with lower scores (41), and Bandyopadhyay et al. found a weak positive correlation between CDR score and number of NPS (Supplementary Table 2) (33).
Both Hallikainen et al. (53) and Naurhashemi et al. (62) found that people with higher CDR scores tended to have higher NPI scores, but Jenner et al. (56) found no correlation between CDR scores and NPI severity scores. Tschanz et al. reported only a weak correlation between CDR-SB and NPI scores over a mean of 3.8 years’ follow-up (69), Caroline et al. found that baseline NPI score was a significant predictor of fast CDR-SB score progression over 1 year (38). In contrast, Tay et al. found no significant differences in baseline NPI score between people who did and did not progress in terms of CDR-SB score over 1 year; those who progressed experienced significantly greater changes in their NPI score over this time (67).
The CDR/CDR-SB assesses cognition and function but does not include any measures or questions regarding behavior. Collecting behavioral and NPS data with alternative tools such as the NPI assists in a more robust characterization of the patient’s clinical status.
3.4.2. CVD
In total, 17 studies reported data on CVD or cardiovascular risk factors (35, 42, 43, 45–47, 49, 50, 55, 58–60, 64, 67, 68, 72, 73) (Supplementary Table 3). These studies present some evidence that the presence of cardiovascular risk factors can influence AD progression, but there was little concordance across studies in terms of which particular risk factors are associated with more severe AD stages or with faster disease progression.
Figure 3 shows data from studies that reported the prevalence of various comorbidities by AD stage, as denoted by categories of CDR or CDR-SB scores (50, 68, 72). The only clear difference between stages was in the study conducted by Ton et al. in which people with more severe AD dementia were relatively more likely to have experienced stroke; other conditions did not appear to be linked to AD stage (68). Of the other studies that reported data on multiple comorbidities, Lee et al. found no link between individual vascular risk factors and CDR-SB progression, but found that having three or more vascular risk factors (coronary heart disease, cardiac arrhythmia, cerebrovascular accident, hypertension, diabetes mellitus, obesity, smoking, or physical inactivity) was linked to progression (58). Mielke et al. found that baseline atrial fibrillation, high systolic blood pressure (as a categorical variable), angina, coronary artery bypass graft, diabetes, or receipt of antihypertensive medication, but not myocardial infarction or stroke, were linked to CDR-SB score progression (59).
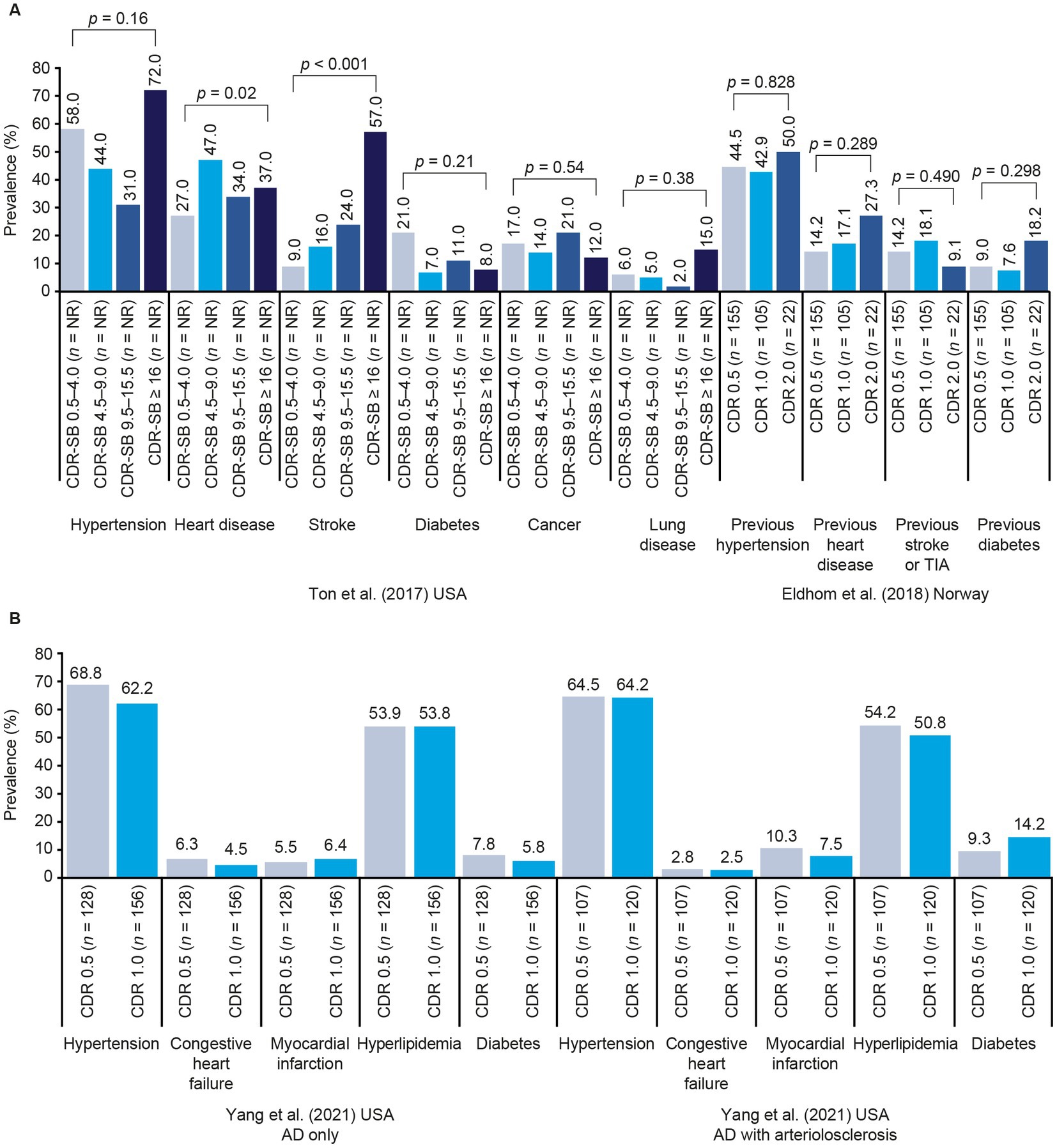
Figure 3. Prevalence of comorbidities by AD stage in Ton et al. (68) and Eldholm et al. (50) (A) and Yang et al. (72) (B). p values across multiple categories represent tests of linear trends. Tests of statistical significance in Ton et al. (68) also include a group with normal cognition (data not shown). AD, Alzheimer’s disease; CDR, Clinical Dementia Rating; CDR-SB, Clinical Dementia Rating–Sum of Boxes; TIA, transient ischemic attack.
3.4.3. Other comorbidities of interest
Three publications reported cross-sectional data on AD severity and urinary incontinence. Na et al. conducted analyses adjusted for age and various AD severity and symptom scores, and found that urinary incontinence was significantly associated with CDR-SB score (odds ratio [OR], 1.56; 95% CI, 1.21–2.01; p < 0.05) among 464 people with AD dementia in South Korea (61); similar results were reported in a previous abstract by the same authors (63). Chang et al. found that scores on the Overactive Bladder Symptom Score questionnaire were not significantly associated with CDR or CDR-SB score in 43 people from Taiwan with AD dementia, but the individual symptom score of urge incontinence was highly correlated with CDR-SB score (r = 0.314; p < 0.05) (40).
Only one study that assessed epilepsy was identified; Voglein et al. assessed US National Alzheimer’s Coordinating Center data from 20,745 individuals, and found that those who experienced seizures had a higher mean CDR-SB score than those who did not (9.3 vs. 6.8; p < 0.0001) in a model adjusted for age and disease duration (70).
3.5. ADLs and dependence
Twelve studies assessed ADLs (Table 3), and these data demonstrated, not surprisingly, that CDR and CDR-SB scores were reliably correlated with decline in ADLs and IADLs, irrespective of the ADL measurement instrument used in the study.
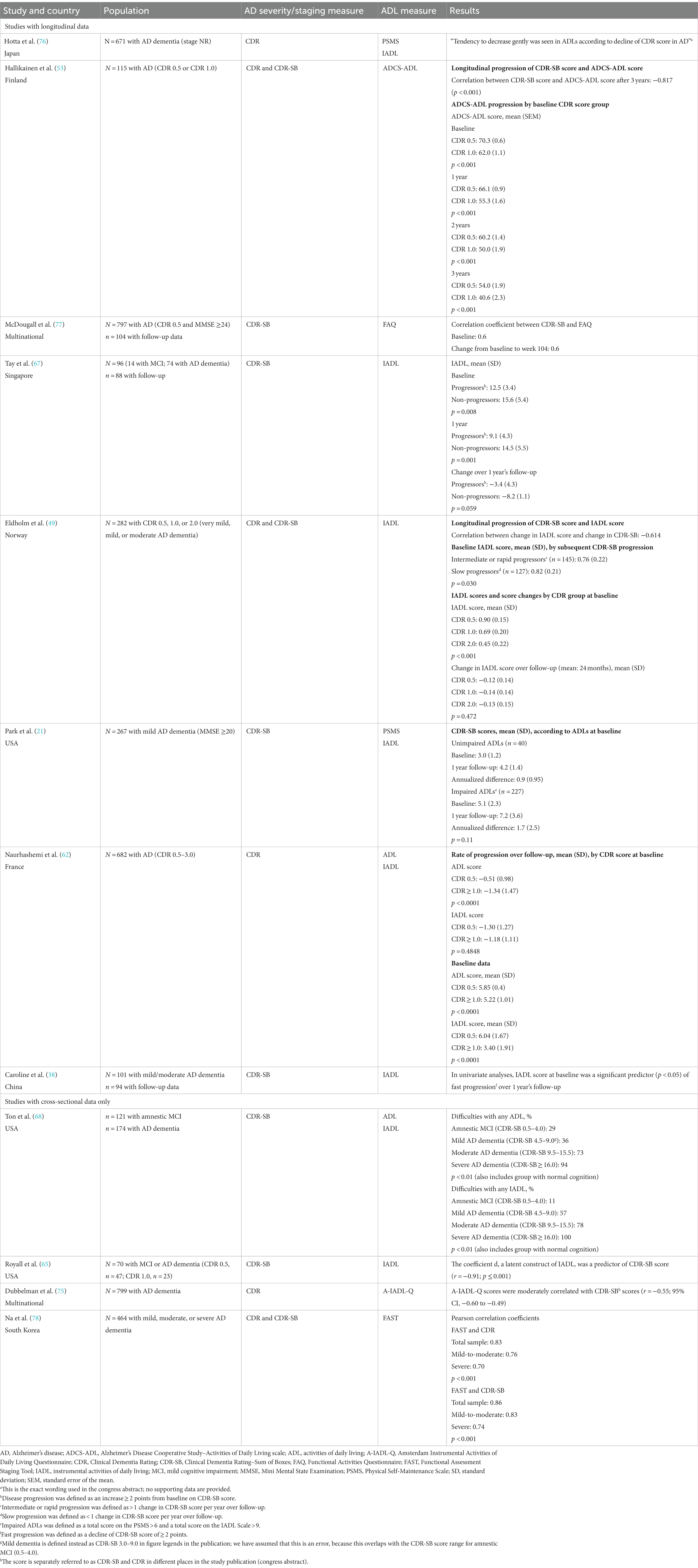
Table 3. Studies reporting ADL data.
Five studies assessed AD progression and ADLs longitudinally. Hotta et al. found that the ability to perform ADLs, assessed using the Physical Self-Maintenance Scale (PSMS) and the IADL Scale, decreased with increasing CDR score over time (76). Eldholm et al. (49), Hallikainen et al. (53), and McDougall et al. (77) found correlations between changes in CDR-SB scores and decline in ADLs as measured using the IADL Scale, the Alzheimer’s Disease Cooperative Study (ADCS)-ADL scale, and the Functional Activities Questionnaire (FAQ), respectively. Tay et al. found that IADL scores were significantly worse at both baseline and follow-up for people who progressed by 2 CDR-SB points or more from baseline over 1 year than for those who did not progress, although no significant differences were detected in terms of the extent of IADL score change (67).
Four studies used cross-sectional data. Royall et al. (65), Dubbelman et al. (75), and Ton et al. (68) found that IADL scores were correlated with CDR or CDR-SB scores; the latter study also found that ADL scores were correlated with CDR-SB scores. Na et al. found that both CDR and CDR-SB scores were correlated with Functional Assessment Staging Tool (FAST) stage (78).
Five studies assessed correlations at baseline and subsequent progression. Hallikainen et al. found that patients with a CDR score of 0.5 at baseline maintained better ADCS-ADL scores each year over 3 years of follow-up than those with a baseline CDR score of 1.0 (53). Naurhashemi et al. found that individuals with AD who had a CDR score of 1.0 or greater at baseline experienced significantly greater ADL decrements over the following 2 years than those with a baseline score of CDR 0.5; however, there was no significant difference between the groups in terms of changes in the ability to perform IADLs (62). Similarly, Eldholm et al. found no significant differences between annual IADL score changes in patients with baseline CDR scores of 0.5, 1.0, or 2.0, which correspond to MCI due to AD, mild AD dementia, and moderate AD dementia, respectively (49). Caroline et al. found that baseline IADLs were a predictor of fast CDR-SB score progression (38), but Park et al. classified patients as having impaired or unimpaired ADLs at baseline using the PSMS and IADL Scale, and found no difference between groups in terms of CDR-SB score decline over the following year (21).
Two studies reported a correlation between scores on the Dependence Scale and CDR-SB scores, using cross-sectional data. Cohen et al. found that a 1-point change in CDR-SB score corresponded to a change of 0.68 points on the Dependence Scale in a multinational cohort with MCI or mild-to-moderate AD dementia (79), whereas Jones et al. found a Dependence Scale score increase of 0.47 for a 1-point increase in CDR-SB score in a UK population with AD dementia (80). For context, total score ranges are broadly similar for the CDR-SB and the Dependence Scale (0–18 and 0–15, respectively; Table 2).
3.6. Nursing home placement
Five studies examined associations between the risk of nursing home placement and CDR-SB or CDR scores (68, 81–84). AD severity, denoted using CDR or CDR-SB scores, was linked to nursing home placement in studies reporting cross-sectional and short-term longitudinal data.
Park et al. assessed the risk of nursing home placement over approximately 3 years’ follow-up in people recently diagnosed with AD in South Korea (n = 2,470 with baseline data; n = 816 with follow-up data) (83). According to the results of Cox proportional hazards models to identify predictors of nursing home placement, baseline CDR-SB score was not a significant predictor (hazard ratio [HR], 1.04; 95% CI, 0.99–1.09; p = 0.05), but annual CDR-SB score change was a predictor (HR, 1.15; 95% CI, 1.06–1.23; p < 0.01) (21). Knopman et al. analyzed data from the multinational ADCS trial of tocopherol and selegiline, comparing people with AD dementia who moved to a nursing home (n = 114) with those who did not (n = 227) (81). While baseline CDR-SB scores were not linked to nursing home placement, there was a significant link between reaching CDR 3.0 over 2 years’ follow-up, versus not reaching CDR 3.0, and nursing home placement (OR adjusted for baseline Mini Mental State Examination [MMSE] and total Behavior Rating Scale for Dementia scores, 7.0; 95% CI, 3.99–12.37; HR adjusted for baseline MMSE, 4.8; p < 0.001) (81). Ota et al. analyzed data from 633 people with MCI (etiology not specified) or AD dementia in Japan (82). Baseline CDR score was linked to the risk of nursing home placement during follow-up, although the duration of follow-up was not stated. Relative to a CDR score of 0.5, HRs were 1.40 (95% CI, 0.78–2.53; p = 0.269) for CDR 1.0, 2.82 (1.52–5.22; p = 0.001) for CDR 2.0, and 6.13 (2.47–15.24; p < 0.000) for CDR 3.0 (82). However, Rountree et al. followed 500 people with AD dementia (country not reported) for 20 years, and found that change in CDR-SB score was not related to the time to nursing home placement (84).
One study included only cross-sectional data. Ton et al. analyzed secondary data from 121 people with amnestic MCI and 174 with mild, moderate, or severe AD in the US Ageing, Demographics and Memory Study (ADAMS), with normal cognition as the reference group. Higher baseline disease severity, as determined via CDR-SB score category, was associated with use of nursing homes during the preceding 2 years (OR from linear trend tests across all five cognitive states, 2.28; 95% CI, 1.64–3.17; p < 0.001) (68).
3.7. Costs and healthcare resource use
Six studies reported data on costs and/or healthcare resource use (68, 85–89) (Supplementary Table 4). These data clearly demonstrated a strong relationship between the increasing requirement for formal and informal care with AD progression as assessed by CDR/CDR-SB scores. Direct medical costs also increased in the later stages of AD and were linked to the cost of residential care.
Two analyses used data from the Alzheimer’s disease Follow-Up Study (ALSOVA) study in Finland. Ruokostenpohja et al. assessed the likelihood of receiving the Finnish care partner’ allowance (89), which is a fee paid to family care partners providing care at home to a person with reduced functional capacity, illness, or disability. The allowance is not an automatic entitlement, and the value varies according to region (91). CDR-SB score was significantly associated with the likelihood of receiving the care partners’ allowance (89). Declining ADCS-ADL score was also a significant predictor of receiving the care partners’ allowance, but increasing NPI score was not a predictor (89). Jetsonen et al. found that people in higher baseline CDR-SB score categories incurred significantly higher annual costs for both formal and informal care during 5 years’ of follow-up, relative to those with lower CDR-SB scores (88).
In the analysis of data from the US ADAMS study reported by Ton et al. individuals in higher CDR-SB score categories had a relatively higher chance of using home care, as well as higher direct medical costs and lower household income (68). In an analysis of baseline multinational RCT data by Gustavsson et al., CDR-SB score was correlated with the following cost categories: total informal care (value of lost productivity for care partners younger than 65 years, and value of lost leisure time for those 65 years or older, not including time spent on supervision), patient accommodation, and community services (86). In this study, declining ADCS-ADL score was also correlated with these cost categories, and increasing total NPI score was correlated with use of informal care and community services. ADLs were identified as the largest cost driver in the analyses, with a 1-point decrease in ADCS-ADL score translating into a 3.6% increase in total costs of care (86).
Two studies reported cross-sectional data by CDR score. Darba et al. found that direct medical care costs increased with CDR score in a Spanish population, particularly at CDR 3.0. There were also notable increases in informal care costs (contributed by time spent on ADLs, IADLs and supervision) at CDR 2.0 and 3.0, compared with earlier stages. Social care costs and indirect costs arising from lost productivity of the care partner were highest at CDR 0.5, and lowest at CDR 1.0 (Figures 4A,B) (85). Ikeda et al. conducted a targeted literature review in Japan, finding that higher public long-term care costs and total medical costs (excluding AD medications) were linked to higher CDR scores (Figure 4C) (87).
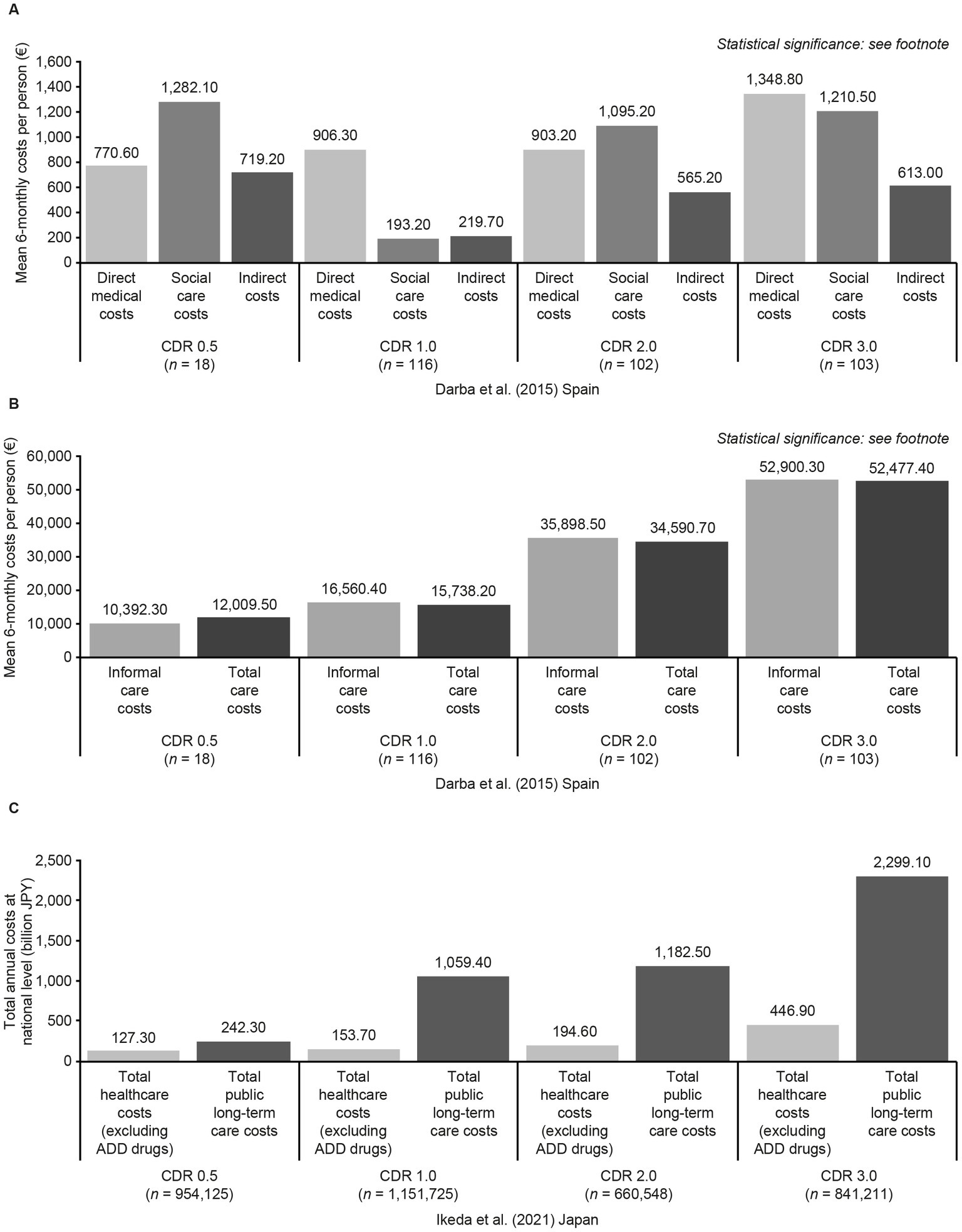
Figure 4. Economic costs associated with CDR score categories in Darba et al. (85) (A,B) and Ikeda et al. (87) (C). Statistical significance in Darba et al. (85). Direct medical costs: p = 0.02 (CDR 1.0 and CDR 3.0). Social care costs p < 0.001 (CDR 1.0 and CDR 2.0; CDR 1.0 and CDR 3.0). Indirect costs: p = 0.9. Informal care costs and total care costs: p < 0.001 (CDR 0.5 and CDR 2.0, CDR 0.5 and CDR 3.0, CDR 1.0 and CDR 2.0, CDR 1.0 and CDR 3.0, and CDR 2.0 and CDR 3.0). Sample sizes in Ikeda et al. (87) refer to estimated patient numbers for the whole of Japan. Statistical significance was not tested. Estimated per-person costs are also included in the study publication but are not presented here because an estimate for total per-person healthcare costs for CDR 0.5 was not available. ADD, Alzheimer’s disease dementia; CDR, Clinical Dementia Rating; JPY, Japanese Yen.
Data on resource use were mixed. Gustavsson et al. found no significant association between CDR-SB score and hospitalization (86); however Ton et al. reported that increasing CDR-SB score was associated with a higher likelihood of hospitalization but a decreasing chance of outpatient visits (68). There was a linear but less pronounced relationship between increasing CDR-SB score and visits to a doctor and the same was true of drug utilization (68).
3.8. Summary of outcomes by CDR score
Figures 2–4 and Table 4 summarize the 12 studies that reported outcomes by CDR score category (37, 41, 49, 53, 54, 57, 62, 65, 72, 82, 85, 87). These studies suggest that NPI score increases with progression from MCI due to AD to mild AD dementia (CDR 0.5 to CDR 1.0) (53, 54). Both the number of NPS and the frequency of specific NPS increased across CDR score categories (37, 41, 57, 62, 65, 72). Caputo et al. found that hallucinations, and apathy were significantly more common at CDR 2.0 and CDR 3.0 than at CDR 1.0, and disinhibition and aberrant motor behavior were significantly more common at CDR 3.0 than at CDR 1.0 (37). Most CVD comorbidities had no clear relationship with CDR score, but people with a score of CDR 2.0 were slightly more likely to have experienced previous hypertension or heart disease than those at CDR 0.5 or CDR 1.0 (50). A steady decline in ADL scores was observed across CDR score categories, including between CDR 0.5 and CDR 1.0 (49, 53, 62). The likelihood of nursing home placement increased across CDR score categories (82). Accordingly, both Darba et al. (85) and Ikeda et al. (87) found that care costs increased with CDR score, with the largest increases being seen at CDR 3.0. However, there was no clear linear relationship between CDR score and healthcare costs in these studies. Darba et al. found that direct medical costs were higher at CDR 0.5 than at CDR 1.0, and increased again at CDR 2.0 and CDR 3.0, and in Ikeda et al. total healthcare costs did not increase notably until CDR 3.0.
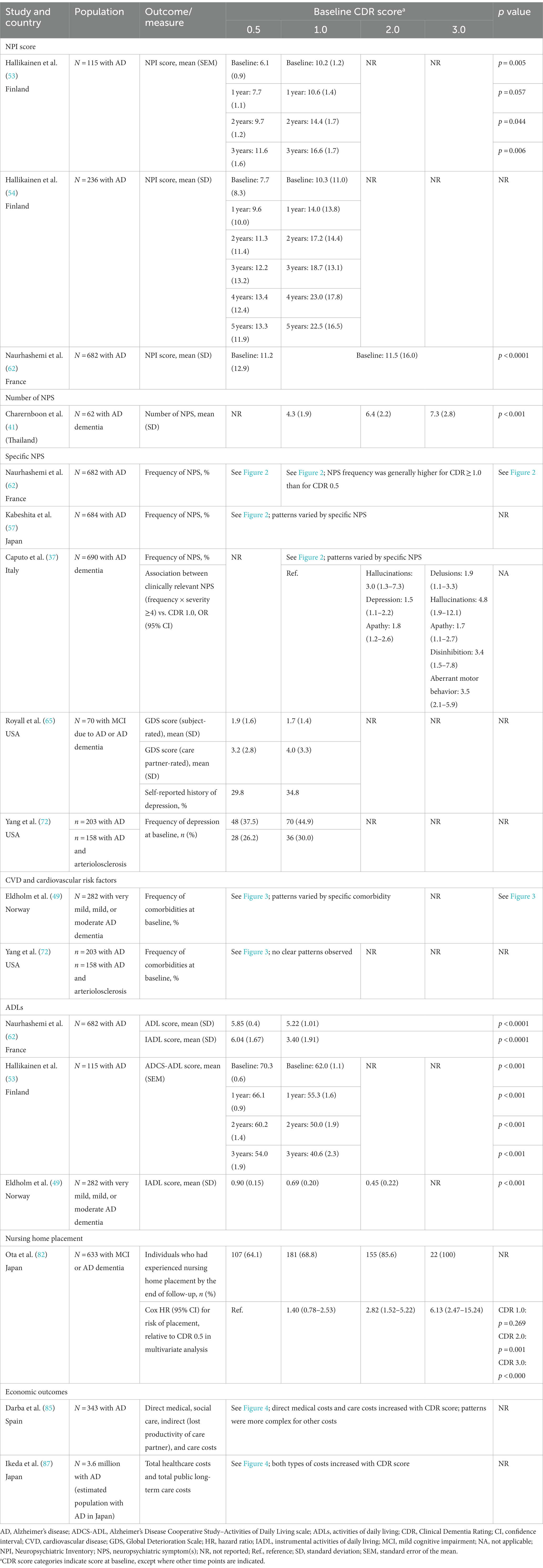
Table 4. Outcomes by CDR score.
4. Discussion
In this comprehensive SLR, we included a broad range of outcomes. We found strong evidence for a link between CDR or CDR-SB scores and NPS, although there was variation across the studies in terms of the specific symptoms linked to AD severity or progression. The relationships between AD progression and CVD were highly inconsistent across studies: although there was some evidence for an association between individual cardiovascular conditions, such as stroke, or risk factors such as diabetes, and CDR or CDR-SB scores, other studies found no such links. There were strong correlations between CDR-SB or CDR scores and a wide range of different ADL measures, indicating that the functional measures included in the CDR scale align closely with ability to perform ADLs. This may also be explained by close overlap between the categories included in the CDR scale and the functional categories in many ADL scales. Multiple studies found that both NPS and ADLs worsen even in the early stages of AD, with decline apparent from CDR 0.5 (MCI due to AD) and CDR 1.0 (mild AD dementia).
Nursing home placement was linked to AD severity and progression, although not all studies found significant correlations, and the study with the longest time horizon found no association between CDR-SB score change and time to placement (84). The use of nursing homes is likely to be particularly dependent on multiple factors that differ across studies and may be difficult to control for, such as the involvement of care partners (92), cultural, ethnic or socioeconomic disparities (93, 94), and the nature and extent of formal care available (95). Therefore, likelihood and timing of placement may differ between countries and geographical regions. However, economic data from Europe, Asia, and the USA indicated that higher CDR-SB or CDR scores are linked to increased requirements for both formal and informal care in all regions, with a stepwise progression of costs across AD stages and a large increase observed at CDR 3.0. Increasing AD severity was also linked to reductions in household income in one study (68), highlighting the broader impact of AD on affected individuals and their care partners. Declining ability to perform ADLs was identified as a driver of care requirements in two studies (86, 89). The first of these two studies found that increasing NPI scores can drive care costs, although less so than declining ADCS-ADL scores (86), but the second study found that NPI score did not predict receipt of a care partners’ allowance (89). A relationship between NPI score and the requirement for care is well recognized, and higher NPI scores have been linked to increases in unpaid care, long-term care, prescription medication use, and physician visits (96). However, the impacts of specific NPS on care requirements and costs differ: an analysis using data from the Cache County Dementia Progression Study found that aggression, psychotic symptoms (delusions and hallucinations), and affective symptoms (depression, anxiety, and irritability) had greater impacts on informal care costs than apathy, sleep disturbances, or appetite disturbances (97).
Direct medical costs typically increased with increasing CDR-SB or CDR score in the studies identified in this SLR, but this was most apparent at later stages of AD dementia. This can be contrasted with the results of a recent analysis of US data, in which the costs of unpaid care increased steadily with AD stage, but direct medical costs, which were assumed to be identical for people receiving care at home and those receiving care in an institution, were similar for all stages of AD (98).
With the exception of some comorbidities, the SLR identified a number of relevant studies for each outcome of interest. There was also good geographical coverage and representation of Asia, Europe, and North America in the studies identified, although other regions, notably South America, Africa, and the Middle East, were not well represented in the data. Some countries were over-represented within particular regions, such as wealthier Asian countries (South Korea and Japan), and Nordic countries with ongoing cohort studies that have generated multiple publications, such as ALSOVA in Finland and the Progression of AD and Resource use (PADR) study in Norway. Disparities among study populations and designs, particularly in terms of demographic factors, AD dementia stage and/or adjustment for these factors, mean that the collation of data should be carried out with caution. For example, studies focused only on patients with a care partner will not be representative of patients with AD living in different circumstances, and the subsets of studies in this SLR that included only patients with MCI due to AD or mild AD dementia may not detect associations between CDR-SB/CDR progression and outcomes that occur predominantly at more severe stages, such as nursing home placement. Economic and healthcare resource utilization data should be interpreted in the context of the healthcare system in each relevant country. As the majority of studies did not confirm AD diagnosis via the assessment of biomarkers, it is highly likely that some patients did not have AD, which may have introduced bias into the findings.
The design of the SLR required that there must be an indication in the title or abstract that relevant outcomes are reported alongside CDR-SB or CDR score. Therefore, it is likely that some excluded publications reported relevant data as baseline characteristics, which were not identified. Comorbidity search terms in the SLR were not exhaustive, and there are additional outcomes that may be relevant to AD, such as cancer, weight loss, and use of antidementia or psychotropic medications, that were not included as search terms. Our searches primarily identified studies that used formal NPS and ADL scales, and more qualitative assessments of factors that are important to patients and care partners, such as the US What Matters Most survey, which highlighted memory and communication problems as key issues (99), were not included in the review.
In conclusion, NPS, ADLs, and costs of care are clearly linked to AD severity and progression, as measured using CDR or CDR-SB scores, beginning at the earliest stages of AD. Although data are available on the links between cardiovascular comorbidities and AD progression, the results of published studies are not consistent, and further investigation is warranted. Future studies on nursing home placement, healthcare costs and resource use, and the relationships between these outcomes, ADLs and NPI, ideally using biomarkers to confirm AD diagnosis, would be highly valuable to indicate how the effects of AD on patients, care partners, and healthcare systems might be mitigated. Further assessments of correlations between rating scales commonly used in AD and dementia should be conducted, to determine what degree of change is clinically meaningful in different populations. Our findings indicate that CDR and CDR-SB scores correlate with multiple patient-and care partner-relevant measures and are a reliable proxy measure for the burden of AD.
Author contributions
All authors contributed to design of the systematic literature review and data interpretation. CF conducted the systematic literature review. All authors contributed to review and revision of the manuscript, and approved it for publication.
Funding
This systematic literature review was funded by Novo Nordisk A/S. Medical writing support was provided by Oxford PharmaGenesis, Oxford, UK with funding from Novo Nordisk A/S.
Conflict of interest
KL has acted as an advisor/consultant for BioXcel Therapeutics, Bright Minds Biosciences, Cerevel Therapeutics, Eisai, GW Pharmaceuticals, IGCPharma, Kondor Pharma, Lundbeck, Merck, Novo Nordisk A/S, Praxis Precision Medicines, and Sumitomo Pharma. JH-P, AC, and LT are employed by Novo Nordisk A/S, which funded the systematic literature review. They contributed to design of the systematic literature review, data interpretation, review and revision of the manuscript, and approval for publication. CE and CF are employed by Oxford PharmaGenesis, which received funding for conducting the systematic literature review. JC has provided consultation to Acadia, Alkahest, AlphaCognition, AriBio, Biogen, Cassava, Cortexyme, Diadem, EIP Pharma, Eisai, GemVax, Genentech, Green Valley, Grifols, Janssen, Karuna, Lilly, LSP, Merck, NervGen, Novo Nordisk A/S, Oligomerix, Ono, Otsuka, PRODEO, Prothena, ReMYND, Resverlogix, Roche, Signant Health, Suven, and United Neuroscience pharmaceutical, assessment, and investment companies. He is supported by US National Institute of General Medical Sciences (NIGMS) grant P20GM109025; National Institute of Neurological Disorders and Stroke (NINDS) grant U01NS093334; National Institute on Aging (NIA) grants R01AG053798, P20AG068053, P30AG072959, and R35AG71476; the Alzheimer’s Disease Drug Discovery Foundation (ADDF); the Ted and Maria Quirk Endowment; and the Joy Chambers-Grundy Endowment.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1208802/full#supplementary-material
References
1. Marshall, GA, Amariglio, RE, Sperling, RA, and Rentz, DM. Activities of daily living: where do they fit in the diagnosis of Alzheimer’s disease? Neurodegener Dis Manag. (2012) 2:483–91. doi: 10.2217/nmt.12.55
2. Lyketsos, CG, Carrillo, MC, Ryan, JM, Khachaturian, AS, Trzepacz, P, Amatniek, J, et al. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement. (2011) 7:532–9. doi: 10.1016/j.jalz.2011.05.2410
3. Alzheimer’s Disease International. Global estimates of informal care. (2018). Available at: www.alzint.org/u/global-estimates-of-informal-care.pdf [Accessed December 23, 2022].
4. Toot, S, Swinson, T, Devine, M, Challis, D, and Orrell, M. Causes of nursing home placement for older people with dementia: a systematic review and meta-analysis. Int Psychogeriatr. (2017) 29:195–208. doi: 10.1017/S1041610216001654
5. Kosaner Kliess, M, Martins, R, and Connolly, MP. Major cost drivers in assessing the economic burden of Alzheimer’s disease: a structured, rapid review. J Prev Alzheimers Dis. (2021) 8:362–70. doi: 10.14283/jpad.2021.17
6. Deb, A, Thornton, JD, Sambamoorthi, U, and Innes, K. Direct and indirect cost of managing alzheimer’s disease and related dementias in the United States. Expert Rev Pharmacoecon Outcomes Res. (2017) 17:189–202. doi: 10.1080/14737167.2017.1313118
7. Wong, W. Economic burden of Alzheimer disease and managed care considerations. Am J Manag Care. (2020) 26:S177–83. doi: 10.37765/ajmc.2020.88482
8. Alzheimer’s Association. 2022 Alzheimer’s Disease Facts and Figures. (2023). Available at: https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf [Accessed February 24, 2023].
9. Kuo, TC, Zhao, Y, Weir, S, Kramer, MS, and Ash, AS. Implications of comorbidity on costs for patients with Alzheimer disease. Med Care. (2008) 46:839–46. doi: 10.1097/MLR.0b013e318178940b
10. Liu, YS, Barner, JC, Rascati, KL, and Bhattacharjee, S. Economic burden of chronic comorbidities among community-dwelling older adults with dementia: a propensity score matched National-Level Study. Alzheimer Dis Assoc Disord. (2022) 36:244–52. doi: 10.1097/WAD.0000000000000504
11. Santiago, JA, and Potashkin, JA. The impact of disease comorbidities in Alzheimer’s disease. Front Aging Neurosci. (2021) 13:631770. doi: 10.3389/fnagi.2021.631770
12. Knight, ADRC. CDR® dementia staging instrument. (2015). Available at: https://knightadrc.wustl.edu/professionals-clinicians/cdr-dementia-staging-instrument/ [Accessed December 23, 2022].
13. Cummings, J. The neuropsychiatric inventory: development and applications. J Geriatr Psychiatry Neurol. (2020) 33:73–84. doi: 10.1177/0891988719882102
14. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
15. Cummings, JL, Mega, M, Gray, K, Rosenberg-Thompson, S, Carusi, DA, and Gornbein, J. The neuropsychiatric inventory: comprehensive assessment of psychopathology in dementia. Neurology. (1994) 44:2308–14. doi: 10.1212/WNL.44.12.2308
16. Cummings, JL. The neuropsychiatric inventory: assessing psychopathology in dementia patients. Neurology. (1997) 48:S10–6. doi: 10.1212/wnl.48.5_suppl_6.10s
17. Katz, S. Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc. (1983) 31:721–7. doi: 10.1111/j.1532-5415.1983.tb03391.x
18. Wallace, M. Katz index of independence in Activities of Daily Living (ADL). (2007). Available at: https://www.alz.org/careplanning/downloads/katz-adl.pdf [Accessed March 10, 2023].
19. Lawton, MP, and Brody, EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86. doi: 10.1093/geront/9.3_Part_1.179
20. Graf, C. The Lawton Instrumental Activities of Daily Living (IADL) scale. (2008). Available at: https://www.alz.org/careplanning/downloads/lawton-iadl.pdf [Accessed March 10, 2023].
21. Park, KW, Pavlik, VN, Rountree, SD, Darby, EJ, and Doody, RS. Is functional decline necessary for a diagnosis of Alzheimer’s disease? Dement Geriatr Cogn Disord. (2007) 24:375–9. doi: 10.1159/000109268
22. Physical Self-Maintenance Scale (n.d.). Physical Self-Maintenance Scale (Activities of Daily Living, or ADLs). Available at: https://www.psychdb.com/_media/teaching/psms.pdf [Accessed March 10, 2023].
23. Galasko, D, Bennett, D, Sano, M, Ernesto, C, Thomas, R, Grundman, M, et al. An inventory to assess activities of daily living for clinical trials in Alzheimer’s disease. The Alzheimer’s disease cooperative study. Alzheimer Dis Assoc Disord. (1997) 2:S33–9. doi: 10.1097/00002093-199700112-00005
24. Kahle-Wrobleski, K, Coley, N, Lepage, B, Cantet, C, Vellas, B, Andrieu, S, et al. Understanding the complexities of functional ability in Alzheimer’s disease: more than just basic and instrumental factors. Curr Alzheimer Res. (2014) 11:357–66. doi: 10.2174/1567205011666140317101419
25. Jutten, RJ, Peeters, CFW, Leijdesdorff, SMJ, Visser, PJ, Maier, AB, Terwee, CB, et al. Detecting functional decline from normal aging to dementia: development and validation of a short version of the Amsterdam IADL questionnaire. Alzheimers Dement (Amst). (2017) 8:26–35. doi: 10.1016/j.dadm.2017.03.002
26. Dubbelman, MA, Terwee, CB, Verrijp, M, Visser, LNC, Scheltens, P, and Sikkes, SAM. Giving meaning to the scores of the Amsterdam instrumental activities of daily living questionnaire: a qualitative study. Health Qual Life Outcomes. (2022) 20:47. doi: 10.1186/s12955-022-01958-2
27. Pfeffer, RI, Kurosaki, TT, Harrah, CH Jr, Chance, JM, and Filos, S. Measurement of functional activities in older adults in the community. J Gerontol. (1982) 37:323–9. doi: 10.1093/geronj/37.3.323
28. Mayo, AM. Use of the Functional Activities Questionnaire in older adults with dementia. (2016). Available at: https://www.alz.org/careplanning/downloads/functional-activities-questionnaire.pdf [Accessed March 10, 2023].
30. Medical Care Corporation (n.d.). Functional Assessment Staging Test. Available at: https://www.mccare.com/pdf/fast.pdf [Accessed March 10, 2023].
31. Stern, Y, Albert, SM, Sano, M, Richards, M, Miller, L, Folstein, M, et al. Assessing patient dependence in Alzheimer’s disease. J Gerontol. (1994) 49:M216–22. doi: 10.1093/geronj/49.5.M216
32. Zhu, CW, Bruinsma, BG, and Stern, Y. Utility of the dependence scale in dementia: validity, meaningfulness, and health economic considerations. Alzheimers Res Ther. (2018) 10:78. doi: 10.1186/s13195-018-0414-7
33. Bandyopadhyay, TK, Biswas, A, Roy, A, Guin, DS, Gangopadhyay, G, Sarkhel, S, et al. Neuropsychiatric profiles in patients with Alzheimer’s disease and vascular dementia. Ann Indian Acad Neurol. (2014) 17:325–30. doi: 10.4103/0972-2327.138520
34. Barca, ML, Persson, K, Eldholm, R, Benth, JS, Kersten, H, Knapskog, AB, et al. Trajectories of depressive symptoms and their relationship to the progression of dementia. J Affect Disord. (2017) 222:146–52. doi: 10.1016/j.jad.2017.07.008
35. Bleckwenn, M, Kleineidam, L, Wagner, M, Jessen, F, Weyerer, S, Werle, J, et al. Impact of coronary heart disease on cognitive decline in Alzheimer’s disease: a prospective longitudinal cohort study in primary care. Br J Gen Pract. (2017) 67:e111–7. doi: 10.3399/bjgp16X688813
36. Breitve, MH, Hynninen, MJ, Bronnick, K, Chwiszczuk, LJ, Auestad, BH, Aarsland, D, et al. A longitudinal study of anxiety and cognitive decline in dementia with Lewy bodies and Alzheimer’s disease. Alzheimers Res Ther. (2016) 8:3. doi: 10.1186/s13195-016-0171-4
37. Caputo, M, Monastero, R, Mariani, E, Santucci, A, Mangialasche, F, Camarda, R, et al. Neuropsychiatric symptoms in 921 elderly subjects with dementia: a comparison between vascular and neurodegenerative types. Acta Psychiatr Scand. (2008) 117:455–64. doi: 10.1111/j.1600-0447.2008.01175.x
38. Caroline, C, and Chan, PC. Baseline behavioural symptoms impact on clinical disease progression in Alzheimer’s dementia. Ann Acad Med Singap. (2015) 44:S340.
39. Castrillo Sanz, A, Andres Calvo, M, Repiso Gento, I, Izquierdo Delgado, E, Gutierrez Rios, R, Rodriguez Herrero, R, et al. Anosognosia in Alzheimer disease: prevalence, associated factors, and influence on disease progression. Neurologia. (2016) 31:296–304. doi: 10.1016/j.nrl.2015.03.006
40. Chang, CW, Juan, YS, Yang, YH, and Lee, HY. The relationship between lower urinary tract symptoms and severity of Alzheimer’s disease. Am J Alzheimers Dis Other Dement. (2021) 36:1533317521992657. doi: 10.1177/1533317521992657
41. Charernboon, T, and Phanasathit, M. Prevalence of neuropsychiatric symptoms in Alzheimer’s disease: a cross-sectional descriptive study in Thailand. J Med Assoc Thail. (2014) 97:560–5.
42. Chew, J, Abengana, J, Ali, N, Chan, M, Tay, L, and Lim, WS. Self-reported sleep duration as a predictor of cognitive decline in mild cognitive impairment (MCI) and mild Alzheimer’s dementia (AD). Alzheimers Dement. (2019) 15:P1185. doi: 10.1016/j.jalz.2019.06.3589
43. Chou, PS, Kao, YH, Wu, MN, Chou, MC, Chen, CH, Lin, RT, et al. Effect of the interaction between hypertension and cerebral white matter changes on the progression of Alzheimer disease. Curr Alzheimer Res. (2018) 15:1354–60. doi: 10.2174/1567205015666181002141013
44. D’Onofrio, G, Sancarlo, D, Panza, F, Copetti, M, Cascavilla, L, Paris, F, et al. Neuropsychiatric symptoms and functional status in Alzheimer’s disease and vascular dementia patients. Curr Alzheimer Res. (2012) 9:759–71. doi: 10.2174/156720512801322582
45. de Oliveira, FF, Chen, ES, Smith, MC, and Bertolucci, PH. Associations of blood pressure with functional and cognitive changes in patients with Alzheimer’s disease. Dement Geriatr Cogn Disord. (2016) 41:314–23. doi: 10.1159/000447585
46. de Oliveira, FF, Chen, ES, Smith, MC, and Bertolucci, PHF. Longitudinal lipid profile variations and clinical change in Alzheimer’s disease dementia. Neurosci Lett. (2017) 646:36–42. doi: 10.1016/j.neulet.2017.03.003
47. de Oliveira, FF, Pereira, FV, Pivi, GAK, Smith, MC, and Bertolucci, PHF. Effects of APOE haplotypes and measures of cardiovascular risk over gender-dependent cognitive and functional changes in one year in Alzheimer’s disease. Int J Neurosci. (2018) 128:472–6. doi: 10.1080/00207454.2017.1396986
48. Dost, FS, Erken, N, Ontan, MS, Ates Bulut, E, Kaya, D, Kocyigit, SE, et al. Muscle strength seems to be related to the functional status and severity of dementia in older adults with Alzheimer’s disease. Curr Aging Sci. (2022) 16:75–83. doi: 10.2174/1573411018666220616114641
49. Eldholm, RS, Barca, ML, Persson, K, Knapskog, AB, Kersten, H, Engedal, K, et al. Progression of Alzheimer’s disease: a longitudinal study in Norwegian memory clinics. J Alzheimers Dis. (2018) 61:1221–32. doi: 10.3233/JAD-170436
50. Eldholm, RS, Persson, K, Barca, ML, Knapskog, AB, Cavallin, L, Engedal, K, et al. Association between vascular comorbidity and progression of Alzheimer’s disease: a two-year observational study in Norwegian memory clinics. BMC Geriatr. (2018) 18:120. doi: 10.1186/s12877-018-0813-4
51. Gilbert, M, Hess, K, Corcoran, C, Snyder, C, Norton, M, Rao, V, et al. Does the length of time between traumatic brain injury and the onset of Alzheimer’s disease affect the rate of cognitive and functional progression?: the Cache County dementia progression study. Alzheimers Dement. (2012) 8:P500–1. doi: 10.1016/j.jalz.2012.05.1357
52. Gilbert, M, Snyder, C, Corcoran, C, Norton, MC, Lyketsos, CG, and Tschanz, JT. The association of traumatic brain injury with rate of progression of cognitive and functional impairment in a population-based cohort of Alzheimer’s disease: the Cache County dementia progression study. Int Psychogeriatr. (2014) 26:1593–601. doi: 10.1017/S1041610214000842
53. Hallikainen, I, Hanninen, T, Fraunberg, M, Hongisto, K, Valimaki, T, Hiltunen, A, et al. Progression of Alzheimer’s disease during a three-year follow-up using the CERAD-NB total score: Kuopio ALSOVA study. Int Psychogeriatr. (2013) 25:1335–44. doi: 10.1017/S1041610213000653
54. Hallikainen, I, Hongisto, K, Valimaki, T, Hanninen, T, Martikainen, J, and Koivisto, AM. The progression of neuropsychiatric symptoms in Alzheimer’s disease during a five-year follow-up: Kuopio ALSOVA study. J Alzheimers Dis. (2018) 61:1367–76. doi: 10.3233/JAD-170697
55. Irimata, KE, Dugger, BN, and Wilson, JR. Impact of the presence of select cardiovascular risk factors on cognitive changes among dementia subtypes. Curr Alzheimer Res. (2018) 15:1032–44. doi: 10.2174/1567205015666180702105119
56. Jenner, C, Reali, G, Puopolo, M, and Silveri, MC. Can cognitive and behavioural disorders differentiate frontal variant-frontotemporal dementia from Alzheimer’s disease at early stages? Behav Neurol. (2006) 17:89–95. doi: 10.1155/2006/812760
57. Kabeshita, Y, Adachi, H, Matsushita, M, Kanemoto, H, Sato, S, Suzuki, Y, et al. Sleep disturbances are key symptoms of very early stage Alzheimer disease with behavioral and psychological symptoms: a Japan multi-center cross-sectional study (J-BIRD). Int J Geriatr Psychiatry. (2017) 32:222–30. doi: 10.1002/gps.4470
58. Lee, WJ, Liao, YC, Wang, YF, Lin, YS, Wang, SJ, and Fuh, JL. Summative effects of vascular risk factors on the progression of Alzheimer disease. J Am Geriatr Soc. (2020) 68:129–36. doi: 10.1111/jgs.16181
59. Mielke, MM, Rosenberg, PB, Tschanz, J, Cook, L, Corcoran, C, Hayden, KM, et al. Vascular factors predict rate of progression in Alzheimer disease. Neurology. (2007) 69:1850–8. doi: 10.1212/01.wnl.0000279520.59792.fe
60. Moon, Y, Moon, WJ, Kim, JO, Kwon, KJ, Joung, J, and Han, SH. Predictors of poor clinical outcome and role of muscle profile in Alzheimer’s disease: a 3-year longitudinal study. Alzheimers Dement. (2019) 15:P700–1. doi: 10.1016/j.jalz.2019.06.2705
61. Na, HR, Park, MH, Cho, ST, Lee, BC, Park, S, Kim, KH, et al. Urinary incontinence in Alzheimer’s disease is associated with clinical dementia rating-sum of boxes and Barthel activities of daily living. Asia Pac Psychiatry. (2015) 7:113–20. doi: 10.1111/appy.12007
62. Naurhashemi, F, Ousset, PJ, Gillette-Guyonnet, S, Cantent, C, Andrieu, S, and Vellas, B. A 2-year follow-up of 233 very mild (CDR 0.5) Alzheimer’s disease patients (REAL.FR cohort). Int J Geriatr Psychiatry. (2008) 23:460–5. doi: 10.1002/gps.1904
63. Park, MH, and Na, H. Urinary incontinence in Alzheimer’s disease is associated with clinical dementia rating: sum of boxes and Barthel’s activities of daily living. Alzheimers Dement. (2012) 8:P128. doi: 10.1016/j.jalz.2012.05.339
64. Pavlik, VN, Chan, W, and Darby, E. Cohort effects in progression rate on cognitive and functional measures in an Alzheimer’s disease clinical cohort. J Alzheimers Dis. (2019) 71:659–69. doi: 10.3233/JAD-190661
65. Royall, DR, Palmer, RF, Vidoni, ED, and Honea, RA. The default mode network may be the key substrate of depressive symptom-related cognitive changes. Adv Alzheimer’s Dis. (2015) 4:247–61. doi: 10.3233/978-1-61499-542-5-247
66. Shim, YS, Choi, SH, and Park, KW. Response to medical treatment is affected by which neuropsychiatric symptoms patients with Alzheimer’s disease have. Alzheimers Dement. (2015) 11:P671. doi: 10.1016/j.jalz.2015.06.997
67. Tay, L, Leung, B, Yeo, A, Chan, M, and Lim, WS. Elevations in serum Dickkopf-1 and disease progression in community-dwelling older adults with mild cognitive impairment and mild-to-moderate Alzheimer’s disease. Front Aging Neurosci. (2019) 11:278. doi: 10.3389/fnagi.2019.00278
68. Ton, TGN, DeLeire, T, May, SG, Hou, N, Tebeka, MG, Chen, E, et al. The financial burden and health care utilization patterns associated with amnestic mild cognitive impairment. Alzheimers Dement. (2017) 13:217–24. doi: 10.1016/j.jalz.2016.08.009
69. Tschanz, JT, Corcoran, CD, Schwartz, S, Treiber, K, Green, RC, Norton, MC, et al. Progression of cognitive, functional, and neuropsychiatric symptom domains in a population cohort with Alzheimer dementia: the Cache County dementia progression study. Am J Geriatr Psychiatry. (2011) 19:532–42. doi: 10.1097/JGP.0b013e3181faec23
70. Voglein, J, Ricard, I, Noachtar, S, Kukull, WA, Dieterich, M, Levin, J, et al. Epilepsy in Alzheimer disease is frequent and characterized by high recurrence. Alzheimers Dement. (2019) 15:P700. doi: 10.1016/j.jalz.2019.06.2704
71. Wadsworth, LP, Rentz, D, Lorius, N, Johnson, K, Sperling, R, Locascio, J, et al. Neuropsychiatric symptoms are associated with current and future global functional impairment in mild cognitive impairment. Alzheimers Dement. (2011) 7:S168–9. doi: 10.1016/j.jalz.2011.05.456
72. Yang, D, and Masurkar, AV. Clinical profiles of arteriolosclerosis and Alzheimer disease at mild cognitive impairment and mild dementia in a national neuropathology cohort. Alzheimer Dis Assoc Disord. (2021) 35:14–22. doi: 10.1097/WAD.0000000000000411
73. Yeo, A, Chong, MS, Tay, L, Yap, J, and Chan, M. Assessing clinical progression in Alzheimer’s disease (AD) subjects: an alternative pre-progression rate in a Singapore memory clinic population. Ann Acad Med Singap. (2013) 42:S268.
74. Zhang, W, Lü, Y, and Yu, W. (2022). Neuropsychiatric symptoms in mild cognitive impairment and Alzheimer’s Disease: relation with disease stage, sex, and daily function impairment. Presented at the Alzheimer’s Association International Conference, July 31 to August 4, San Diego, CA, USA.
75. Dubbelman, M, Postema, M, Scheltens, P, Van Der Flier, W, and Sikkes, S. The Amsterdam instrumental activities of daily living questionnaire: validation of a clinically meaningful outcome measure in asymptomatic and early symptomatic Alzheimer’s disease. J Prev Alzheimers Dis. (2021) 8:S134–5. doi: 10.14283/jpad.2021.58
76. Hotta, M, Hashimoto, M, Fukuhara, R, Koyama, A, Murata, M, Yoshiura, K, et al. Relationship between cognitive declines and independency in the activities of daily living in patients with frontotemporal dementia. J Neurochem. (2016) 138:296. doi: 10.1111/jnc.13692
77. McDougall, F, Edgar, C, Mertes, M, Delmar, P, Fontoura, P, Abi-Saab, D, et al. Psychometric properties of the clinical dementia rating - sum of boxes and other cognitive and functional outcomes in a prodromal Alzheimer’s disease population. J Prev Alzheimers Dis. (2021) 8:151–60. doi: 10.14283/jpad.2020.73
78. Na, HR, Kim, SY, Chang, YH, Park, MH, Cho, ST, Han, IW, et al. Functional assessment staging (FAST) in Korean patients with Alzheimer’s disease. J Alzheimers Dis. (2010) 22:151–8. doi: 10.3233/JAD-2010-100072
79. Cohen, JT, McLaughlin, TP, Neumann, P, Mucha, L, Liu, E, Grundman, M, et al. P1‐212: estimating dependence scale scores based on clinical dementia rating ‐ sum of boxes scores in patients with mild cognitive impairment or mild to moderate Alzheimer’s disease. Alzheimers Dement. (2009) 5:238–9. doi: 10.1016/j.jalz.2009.04.219
80. Jones, RW, Lacey, L, Knapp, M, Romeo, R, Sato, A, Niecko, T, et al. Poster session 1, Sunday 9 September. Eur J Neurol. (2012) 19:90–457. doi: 10.1111/j.1468-1331.2012.03888.x
81. Knopman, DS, Berg, JD, Thomas, R, Grundman, M, Thal, LJ, and Sano, M. Nursing home placement is related to dementia progression: experience from a clinical trial. Neurology. (1999) 52:714–8. doi: 10.1212/WNL.52.4.714
82. Ota, K, Arikawa, M, Ohashi, S, Azekawa, T, and Matsumoto, T. Factors influencing nursing home placement of patients with dementia: a retrospective, single-Centre study in Japan. Psychogeriatrics. (2019) 19:111–6. doi: 10.1111/psyg.12373
83. Park, DG, Lee, S, Moon, YM, Na, DL, Jeong, JH, Park, KW, et al. Predictors of institutionalization in patients with Alzheimer’s disease in South Korea. J Clin Neurol. (2018) 14:191–9. doi: 10.3988/jcn.2018.14.2.191
84. Rountree, S, Chan, W, Pavlik, V, and Doody, R. Factors that influence nursing home placement in an Alzheimer’s disease cohort. Alzheimers Dement. (2012) 8:P375. doi: 10.1016/j.jalz.2012.05.1030
85. Darba, J, Kaskens, L, and Lacey, L. Relationship between global severity of patients with Alzheimer’s disease and costs of care in Spain; results from the co-dependence study in Spain. Eur J Health Econ. (2015) 16:895–905. doi: 10.1007/s10198-014-0642-0
86. Gustavsson, A, Cattelin, F, and Jonsson, L. Costs of care in a mild-to-moderate Alzheimer clinical trial sample: key resources and their determinants. Alzheimers Dement. (2011) 7:466–73. doi: 10.1016/j.jalz.2010.06.002
87. Ikeda, S, Mimura, M, Ikeda, M, Wada-Isoe, K, Azuma, M, Inoue, S, et al. Economic burden of Alzheimer’s disease dementia in Japan. J Alzheimers Dis. (2021) 81:309–19. doi: 10.3233/JAD-210075
88. Jetsonen, V, Kuvaja-Kollner, V, Valimaki, T, Selander, T, Martikainen, J, and Koivisto, AM. Total cost of care increases significantly from early to mild Alzheimer’s disease: 5-year ALSOVA follow-up. Age Ageing. (2021) 50:2116–22. doi: 10.1093/ageing/afab144
89. Ruokostenpohja, N, Valimaki, T, Martikainen, J, Hallikainen, M, Vehvilainen-Julkunen, K, and Koivisto, A. Entitlement of carer’s allowance to support home care of persons with Alzheimer’s disease: evaluation of current decision criteria. Eur Geriatr Med. (2018) 9:477–83. doi: 10.1007/s41999-018-0060-4
90. McKhann, G, Drachman, D, Folstein, M, Katzman, R, Price, D, and Stadlan, EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology. (1984) 34:939–44. doi: 10.1212/WNL.34.7.939
91. Linnosmaa, I, Jokinen, S, Vilkko, A, Noro, A, and Siljander, E. (2014). Report on the fees and services of informal care support in municipalities in 2012. National Institute for Health and Welfare (THL). Helsinki.
92. Friedman, SM, Steinwachs, DM, Temkin-Greener, H, and Mukamel, DB. Informal caregivers and the risk of nursing home admission among individuals enrolled in the program of all-inclusive care for the elderly. Gerontologist. (2006) 46:456–63. doi: 10.1093/geront/46.4.456
93. Estrada, LV, Agarwal, M, and Stone, PW. Racial/ethnic disparities in nursing home end-of-life care: a systematic review. J Am Med Dir Assoc. (2021) 22:e1. doi: 10.1016/j.jamda.2020.12.005
94. Fitzgerald, MH, Mullavey-O’Byrne, C, and Clemson, L. Families and nursing home placements: a cross-cultural study. J Cross Cult Gerontol. (2001) 16:333–51. doi: 10.1023/A:1014505219291
95. Coe, NB, Konetzka, RT, Berkowitz, M, Blecker, E, and Van Houtven, CH. The effects of home care provider mix on the care recipient: an international, systematic review of articles from 2000 to 2020. Annu Rev Public Health. (2021) 42:483–503. doi: 10.1146/annurev-publhealth-090419-102354
96. Murman, DL, and Colenda, CC. The economic impact of neuropsychiatric symptoms in Alzheimer’s disease: can drugs ease the burden? PharmacoEconomics. (2005) 23:227–42. doi: 10.2165/00019053-200523030-00004
97. Rattinger, GB, Sanders, CL, Vernon, E, Schwartz, S, Behrens, S, Lyketsos, CG, et al. Neuropsychiatric symptoms in patients with dementia and the longitudinal costs of informal care in the Cache County population. Alzheimers Dement (N Y). (2019) 5:81–8. doi: 10.1016/j.trci.2019.01.002
98. Razavi, M, Herring, WL, Gillis, C, Maserejian, N, Pemberton-Ross, P, and Nejati, M. (2022). Economic burden of daily transitions to later stages of AD dementia in the US. Poster LP95. Presented at the 15th Clinical Trials on Alzheimer’s Disease (CTAD) Conference, November 29 to December 2, San Francisco, CA, USA.
99. DiBenedetti, DB, Slota, C, Wronski, SL, Vradenburg, G, Comer, M, Callahan, LF, et al. Assessing what matters most to patients with or at risk for Alzheimer’s and care partners: a qualitative study evaluating symptoms, impacts, and outcomes. Alzheimers Res Ther. (2020) 12:90. doi: 10.1186/s13195-020-00659-6
Keywords: activities of daily living, Alzheimer’s disease, clinical dementia rating (CDR), comorbidity, healthcare costs, healthcare resource use, neuropsychiatric inventory (NPI), nursing home placement
Citation: Cummings J, Hahn-Pedersen JH, Eichinger CS, Freeman C, Clark A, Tarazona LRS and Lanctôt K (2023) Exploring the relationship between patient-relevant outcomes and Alzheimer’s disease progression assessed using the clinical dementia rating scale: a systematic literature review. Front. Neurol. 14:1208802. doi: 10.3389/fneur.2023.1208802
Edited by:
Maria Isabel Behrens, University of Chile, ChileReviewed by:
John Morris, Washington University in St. Louis, United StatesDorothee Oberdhan, Otsuka Pharmaceutical Development & Commercialization, Inc., United States
Copyright © 2023 Cummings, Hahn-Pedersen, Eichinger, Freeman, Clark, Tarazona and Lanctôt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jeffrey Cummings, amN1bW1pbmdzQGNuc2lubm92YXRpb25zLmNvbQ==