 Charly Gaul
Charly Gaul Stefanie Förderreuther
Stefanie Förderreuther Walter Lehmacher3
Walter Lehmacher3 Thomas Weiser
Thomas Weiser- 1Headache Center Frankfurt, Frankfurt, Germany
- 2Department of Neurology, Ludwig Maximilian University, Munich, Germany
- 3Emeritus, Institute for Medical Statistics, Informatics and Epidemiology, University of Cologne, Cologne, Germany
- 4Medical Consumer Healthcare, Sanofi, Frankfurt, Germany
Introduction: Observational studies are valuable for investigating correlations between patient-reported treatment outcomes. In this study, we report a secondary analysis of a published pharmacy-based observational (patient-centered “real-world” outcomes) study on experiences reported by patients who treated their headache with an over-the-counter analgesic.
Methods: A pharmacy-based exploratory survey was conducted in German community pharmacies. Patients buying a fixed-dose analgesic combination product (400 mg ibuprofen + 100 mg caffeine; IbuCaff) to treat their headache were offered a questionnaire that contained—among others—questions about time to onset of pain relief (OPR), assessment of time to onset of pain relief (AOPR), assessment of efficacy and tolerability, and pain intensity 2 h after intake. A correlation analysis of the data was performed. Moreover, perceived treatment effects compared to other acute headache medications used in the past were collected.
Results: The correlation between OPR and AOPR was high (Spearman rank correlation r = 0.594, p < 0.0001). Headache patients assessed the onset of analgesic action within 15 min as “very fast” and within 30 min as “fast”. The other readouts were correlated as well [assessment of efficacy and % pain intensity difference (%PID) at 2 h: r = 0.487; OPR/AOPR and %PID at 2 h: r = 0.295/0.318; OPR/AOPR and assessment of tolerability: r = 0.206/0.397; OPR/AOPR and assessment of efficacy: r = 0.406/0.594; assessment of efficacy and assessment of tolerability: r = 0.608; p < 0.0001 for all correlations]. Compared to previous treatments, most patients (>89%) assessed the speed of analgesic action, efficacy, and tolerability of IbuCaff as equal to or better than for the previous treatment.
Discussion: Headache patients assessed the onset of analgesia within 15 min as “very fast” and within 30 min as “fast”. Efficacy assessments for acute headache medication appear to be highly correlated.
1. Introduction
Acute headache is often treated with over-the counter (OTC) analgesics available in community pharmacies (1). Observational studies, such as pharmacy-based patient surveys, are suited to gain information on patient-reported treatment outcomes and can complement randomized controlled clinical studies, and more adequate observational studies are needed to address aspects that clinical trials cannot explore (2). Such pharmacy-based surveys have been run for cough and cold treatments (3, 4), antispasmodics for gastrointestinal complaints (5, 6), or other acute pain medications (7–9), and their methodology is well established.
Evidence from multiple sources shows that patients expect that acute headache treatments relieve pain as fast and completely as possible. For instance, over 80% of migraine patients ranked complete pain relief and fast onset of action as the most important expectation from their acute pain medication (10). In a questionnaire on patient expectations from migraine treatment, fast pain relief was defined to be important (11). Others used the “willingness to pay” approach and found that patients were willing to pay more money for acute migraine treatment when it acted faster (12). However, the latter two studies did not investigate actual treatments. In contrast, the analysis of two controlled clinical trials investigating sumatriptan for treating acute migraine attacks found that early onset of pain relief correlated with the percentage of pain-free patients (13). How these parameters were correlated with patients' assessment of efficacy was not investigated. Thus, to date, the question of what exactly headache patients mean when they speak of “fast” or “very fast” onset of pain relief is still not clear. Therefore, we analyzed the data from a previously reported, observational, pharmacy-based patient survey (patient-centered “real world” outcomes study) that was run in German community pharmacies and investigated the effects of the fixed-dose combination 400 mg ibuprofen plus 100 mg caffeine (IbuCaff) (9). This product is available without a prescription in Germany and other European countries. The general aim of our analysis was to learn how different efficacy and tolerability readouts were correlated. One focus was how the onset of headache pain relief correlated with the qualitative assessment of speed of action.
2. Patients and methods
Details of the survey underlying the present analyses have been reported previously (9). Briefly, patients buying IbuCaff (Thomapyrin TENSION DUO ®) between February and June 2019 in German community pharmacies were offered participation in a survey. After giving consent, they were handed a questionnaire that was to be filled out by the patients after taking the product to treat an acute pain event. Questionnaires were sent anonymously in envelopes provided to the participants to the institute that collected the data and performed the primary analysis (Winicker Norimed GmbH, Nuremburg, Germany). The identification of participants was therefore not possible (i.e., full anonymity was provided). No incentive was given to participants. According to German laws and regulations, ethical committee participation was neither required nor recommended for this kind of investigation.
The inclusion criteria were the purchase and use of the respective product, willingness and ability to fill out the questionnaire, usage of the product according to the packaging label, and age of 18 years or older. There were no exclusion criteria. This analysis was restricted to data from patients who reported intake of the product to treat a headache episode. No diagnosis for headache etiology (e.g., tension-type headache or migraine) was performed. The following data on efficacy and tolerability parameters were analyzed: Perceived onset of pain relief (“how long did it take for your pain to start getting better?” OPR; categories: 0–5/6–15/16–30/31–45/46–60/>60 min), assessment of onset of pain relief (“how would you describe the onset of the effect of IbuCaff?”; AOPR; categories: very fast/fast/moderately fast/slow), and assessment of efficacy/tolerability (categories: very good/good/not so good/bad). Pain intensities at baseline and 2 h after intake of the medication (on a 0–10 numerical rating scale) were used to calculate the relative pain intensity difference (%PID). Moreover, participants were asked how they assessed onset of action, efficacy, and tolerability in comparison to the last analgesic product they had taken before to treat a similar pain episode (categories: worse/equal/better).
2.1. Data analysis
Data management and primary analysis were done by Winicker Norimed using SAS (version 9.2). Additional analyses were conducted by the authors using GraphPad Prism, version 9.3.1. Spearman's rank coefficients were calculated to assess correlations between OPR and AOPR, OPR and %PID, AOPR and %PID, efficacy ratings and %PID, OPR/AOPR and baseline pain intensity, as well as ratings of efficacy and tolerability. Relative and cumulative relative frequencies of OPR categories stratified by AOPR categories were calculated; rate ratios (relative rates) of these cumulated relative frequencies were used to assess which AOPR category steps discriminated between cumulative OPR rates. The relative rate (RR) cutoff for the discrimination between AOPR categories was set to a value of 2.
3. Results
In total, 1,124 participants provided analyzable questionnaires, 229 treated other pain than headache, and 895 of them reported the use of IbuCaff for treating a headache episode (9). The correlation between OPR and AOPR was high (Spearman r = 0.594; 95% CI: 0.5468 to 0.6373; p < 0.0001). Most of the participants experienced OPR as “very fast” (21.8%) or “fast” (58.8%), and only 17.5% and 1.9% assessed it as “moderately fast” or “slow,” respectively (Supplementary Table). Figure 1 gives a graphical representation of the OPR data stratified by the four AOPR categories. A total of 76% of patients reporting onset of pain relief within 15 min assessed this as “very fast,” and 87% of those reporting onset within 30 min assessed this as “fast”.
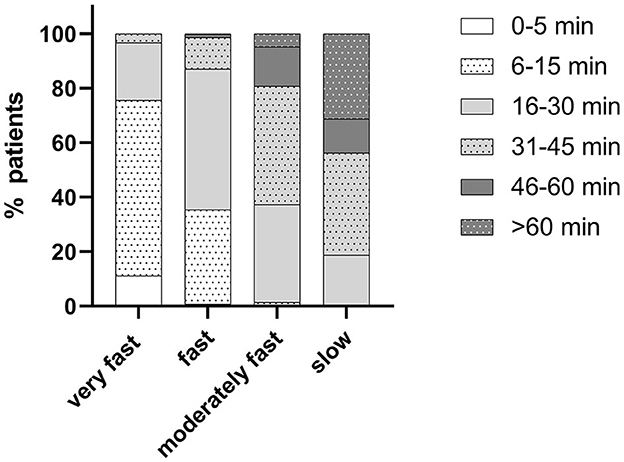
Figure 1. Onset of pain relief (OPR) data stratified by the assessment of onset of pain relief (AOPR) categories.
Next, we used the cumulated relative frequencies to assess which AOPR category steps discriminated between cumulative OPR rates. Comparison of RRs for the different OPR values for AOPR categories “very fast” vs. “fast” showed that these rates were relatively high for OPR ≤ 5 min, >2 for OPR ≤ 15 min, and then leveled around a value of 1. Thus, OPR later than 15 min made no difference for the two AOPR categories and, in consequence, suggests that this is the cutoff point for the distinction between AOPR of “very fast” vs. “fast”. For the AOPR category “fast” vs. “moderately fast,” this cutoff OPR was 30 min. The analysis of the AOPR category “moderately fast” vs. “slow” gave no interpretable results (Table 1).

Table 1. Ratios of cumulative relative frequencies of OPR categories (RR) with 95% confidence intervals (CI) and p-values for the comparisons of different assessments of onset of pain relief.
Figure 2 shows graphical representations of other correlations. A higher %PID at 2 h corresponded to higher percentages of patients with higher ranking efficacy (Figure 2A), earlier OPR (Figure 2B), and AOPR (Figure 2C). AOPR was also correlated with the assessment of tolerability (Figure 2D). Baseline pain intensity correlated only weakly with OPR but not AOPR. OPR and AOPR correlated with efficacy and tolerability outcomes, and perceived efficacy was correlated with tolerability as well. More detailed information on correlation analysis of the various parameters is given in Table 2.
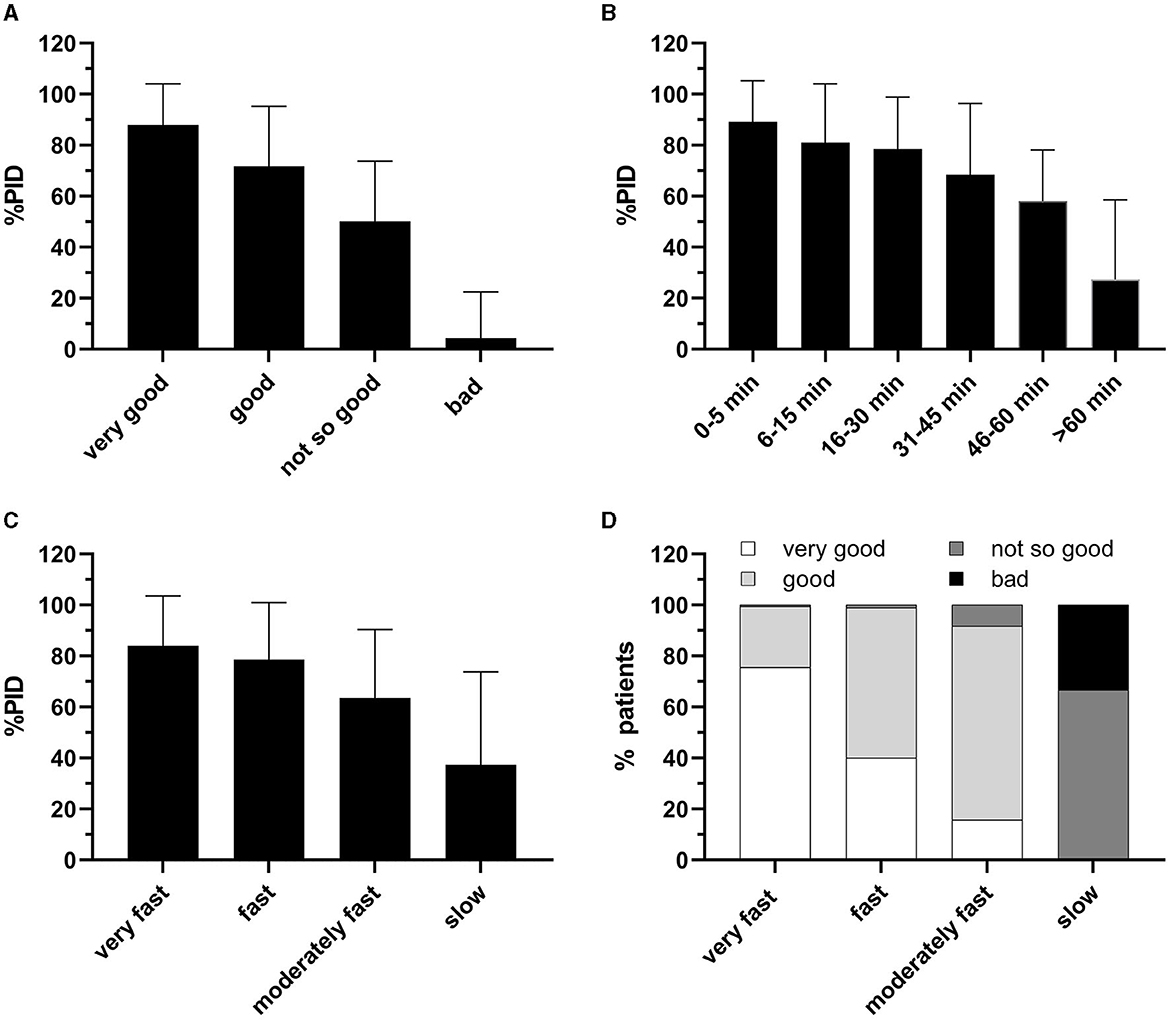
Figure 2. (A) %PID at 2 h by assessment of efficacy; (B) % PID at 2 h by onset of pain relief (OPR); (C) %PID at 2 h by assessment of time to onset of pain relief (AOPR). (D) Assessment of tolerability by AOPR. Data in (A–C) are shown as means with standard deviations.
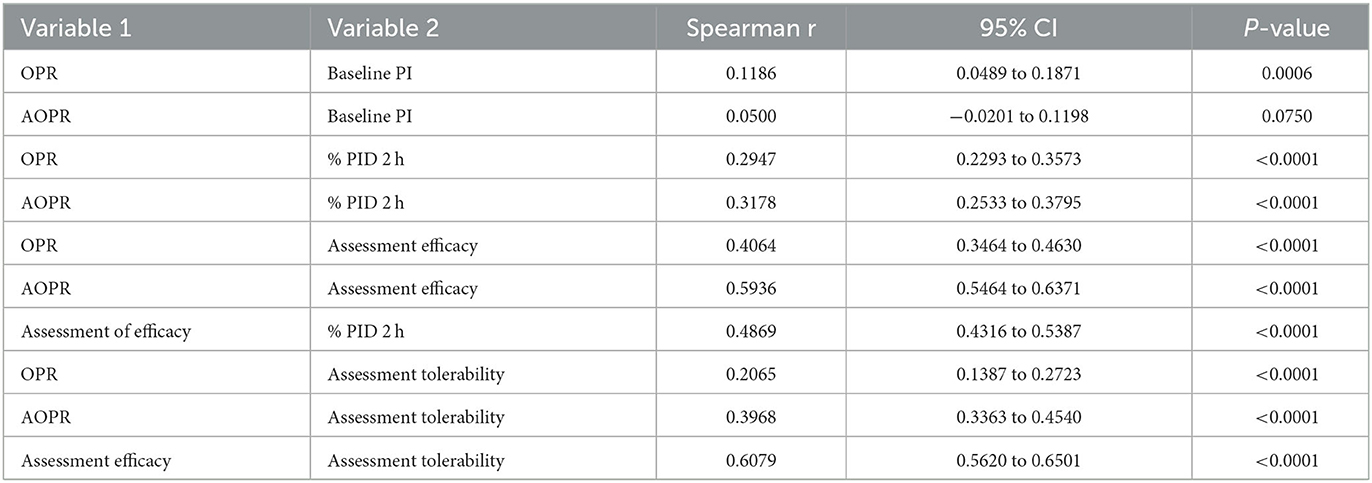
Table 2. Correlations of analyzed parameters.
Participants were asked which other acute treatment they had taken before IbuCaff for the last comparable pain episode, and how they assessed overall efficacy, how fast the analgesic acted, and overall tolerability in comparison to IbuCaff. Relative percentages of assessments are shown in Figure 3. Only low percentages of participants rated efficacy worse compared to the last individual treatment (between 0% and 8.1%; Figure 3A). The percentages of those who ranked IbuCaff efficacy better ranged from 35% (in comparison to ibuprofen lysinate) to 65.5% (in comparison to paracetamol). Between 1.0% (paracetamol) and 10.2% (naproxen) reported that IbuCaff acted not as fast as the previously taken analgesic, and between 37.5% (ibuprofen lysinate) and 66.1% (paracetamol) found IbuCaff to act faster (Figure 3B). The tolerability of IbuCaff was rated lower by between 1.0% (ibuprofen) and 4.1% (naproxen) and higher by 12.8% (ibuprofen lysinate) to 44.9% (naproxen; Figure 3C).
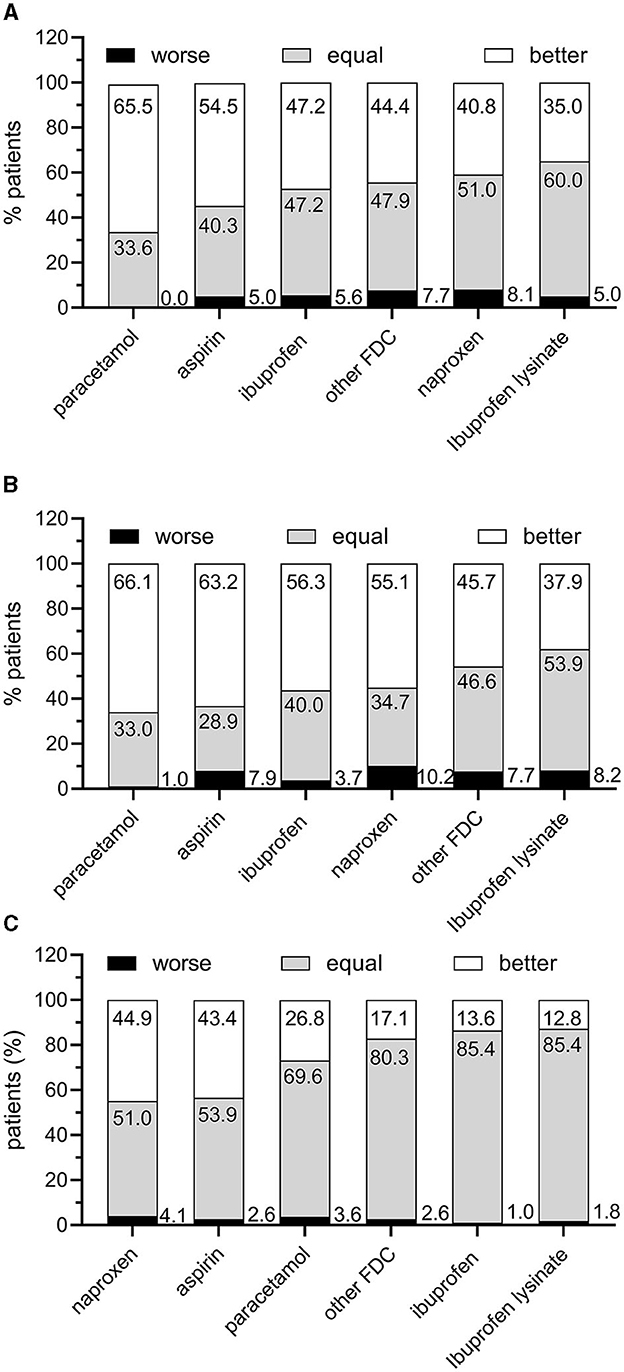
Figure 3. Patient perception of IbuCaff compared to the last acute medication taken to treat a similar pain episode. (A) Assessment of speed of analgesic action. (B) Assessment of efficacy. (C) Assessments of tolerability.
4. Discussion
Pharmacy-based patient surveys can gain information on how patient-reported readouts are correlated and complement data obtained from randomized controlled clinical trials (2). One limitation of studies with this design is that they do not allow for the comparison of an active treatment with a control (e.g., placebo) group and, therefore, cannot be used to show, e.g., efficacy in general. Since the combination of ibuprofen and caffeine (400/200 mg) has been shown to be superior compared to 400 mg ibuprofen in tension-type headache (14) and meta-analyses of controlled trials on ibuprofen for treating tension-type and migraine headaches and for the effects of caffeine as co-analgesic are available (15–17), it is beyond doubt that IbuCaff can reduce acute headache. Other limitations are that no headache diagnosis was performed and that for assessing historical treatment, data recall bias could not be excluded. One strength of this study design is the focus on the patient, and studies of this kind allow for characterizing patient demographics and behaviors, as well as perceived treatment effects in general practice (3–9). Another strength of this study is that it allows for more general conclusions of the kind “if a headache treatment has an effect X, how does this correlate with effect Y,” which can be assumed to be independent of the treatment per se and therefore should be transferrable to any abortive headache treatment.
Our study shows that the onset of headache pain relief earlier than 15 min after intake of IbuCaff was perceived as “very fast” by the patients and onset earlier than 30 min was perceived as “fast”. Altogether more than 80% of patients belonged to these two categories. The onset of pain relief within the first 5 min after intake was reported by 24 patients and most probably is due to placebo effects because even under best conditions (i.e., in the fasted state), only a small amount of ibuprofen and caffeine from IbuCaff can be expected to be absorbed that fast (18). A randomized controlled trial on dental extraction pain showed that IbuCaff was superior to 400 mg ibuprofen as early as 15 min after intake (19) and, therefore, the reported onset of pain relief in the category (“6–15 min” and later) can be assumed to reflect a pharmacological effect.
Interestingly, other patient-reported efficacy parameters were correlated with OPR and AOPR as well. The earlier the pain was relieved, the higher the %PID was compared to baseline at 2 h. This is not surprising if one assumes a steady increase in pain relief over the time up to 2 h after intake of an analgesic. In consequence, an early onset of pain relief was correlated with the overall impression of treatment efficacy. Correlations of baseline pain with OPR and AOPR were very weak to absent.
The strong correlation between the assessment of efficacy of an analgesic and %PID has been shown in a randomized controlled trial before (20).
Somewhat surprising was the correlation between AOPR and assessment of tolerability: Early pain relief and high tolerability went hand in hand. Controlled clinical trial occurrence of untoward effects was correlated with treatment efficacy/pain reduction [i.e., lower tolerability was correlated with higher efficacy; (21–23)]. One explanation might be that adverse events lead to unblinding in a controlled clinical trial (since patients experiencing adverse events will assume that they have received an active treatment), which cannot be the case in our study. Further studies will be needed to explain this finding.
One guideline-recommended endpoint for clinical trials investigating migraine headache is the analysis of treatment preference (in comparison to prior treatments) (24). Although in our study no formal diagnosis for the headache etiology was performed, it can be hypothesized that various migraine-trial relevant parameters can be transferred to acute headache in general.
In terms of perceived efficacy, onset of action, and tolerability, IbuCaff was rated worse than previous OTC treatments by only small percentages of patients (usually in the one-digit range). On the other hand, large percentages of patients rated IbuCaff better than the comparators. This is not surprising since caffeine-containing analgesics have been shown to be superior to those without caffeine (16). In comparison to other analgesics (including ibuprofen and ibuprofen lysinate), tolerability was generally rated at least as equal.
Comparisons with historical data bear the risk of bias (such as recall bias). If this was the case for our analysis, one should expect random distributions, which was obviously not the case. For the parameters such as “perceived efficacy” and “onset of effect,” the highest percentages reporting superiority were found for paracetamol [a relatively weak analgesic; (25)] and the lowest for ibuprofen lysinate. For “tolerability,” the highest superiority was reported compared to naproxen and lowest for ibuprofen lysinate. Thus, the assessments are not randomly distributed, which underpins their validity. Moreover, probably not all patients have found their optimal acute headache treatment yet, and a different analgesic might work better for them. In consequence, each patient should be encouraged to try various acute pain analgesics to find the one that works the best individually.
Taken together, this analysis shows that an abortive headache treatment relieving pain within 15 min after intake can be considered to act “very fast” from the patient's perspective and that within 30 min can be considered to act “fast”. The fast onset of analgesic effects was positively correlated with several other efficacy readouts, suggesting that an early onset of action is a key factor for successfully treating acute headache. This might be an interesting aspect of patient education: when pain relief starts early, chances are high for an overall successful headache treatment.
Data availability statement
Publicly available datasets were analyzed in this study. Qualified researchers may request access to data and related study documents including the study report, study protocol with any amendments, statistical analysis plan, and dataset specifications. Further details on Sanofi's data sharing criteria, eligible studies, and process for requesting access can be found at: https://www.vivli.org/.
Ethics statement
The manuscript represents a secondary analysis of a published study. Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author contributions
CG: Conceptualization, Investigation, Writing—review and editing. SF: Conceptualization, Investigation, Writing—review and editing. WL: Conceptualization, Investigation, Methodology, Writing—review and editing. TW: Conceptualization, Investigation, Methodology, Project administration, Writing—original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The underlying survey had been funded by Sanofi. Medical writing support was provided by Michel Pharma Solutions (Mainz, Germany) and funded by Sanofi.
Conflict of interest
CG has received honoraria for consulting and lectures within the past 3 years from Allergan, Eli Lilly, Grünenthal, Hormosan, Lundbeck Perfood, Novartis Pharma, Sanofi-Aventis, TEVA, and Weber and Weber and is honorary secretary of the German Migraine and Headache Society. SF received consultant, speaker, and/or advisory board member honoraria from Eli Lilly, Hormosan, Lundbeck, Novartis, Sanofi, Pharm Allergan, and Teva. WL received honoraria for statistical consulting and for membership in independent Data Monitoring and Safety Boards from Bayer, Bial, Biotronik, ClinCompetenceCologne, CRM Biometrics, Sanofi, Schwabe, and several universities. TW is an employee of Sanofi.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1273846/full#supplementary-material
References
1. Porst M, Wengler A, Leddin J, Neuhauser H, Katsarava S, Lippe E, et al. Migraine and tension-type headache in Germany. Pevalence and disease severity from the BURDEN 2020 Burden of Disease Study. J Health Monitor. (2020) 5:2–24. doi: 10.25646/6990.2
2. Caparrotta TM, Dear JW, Colhoun HM, Webb DJ. Pharmacoepidemiology: Using randomised control trials and observational studies in clinical decision-making. Br J Clin Pharmacol. (2019) 85:1907–24. doi: 10.1111/bcp.14024
3. Kardos P, Beeh K-M, Sent U, Mueck T, Gräter H, Michel MC. Characterization of differential patient profiles and therapeutic responses of pharmacy customers for four ambroxol formulations. BMC Pharmacol Toxicol. (2018) 19:40. doi: 10.1186/s40360-018-0229-y
4. Klimek L, Schumacher H, Schütt T, Gräter H, Mueck T, Michel MC. Factors associated with efficacy of an ibuprofen/pseudoephedrine combination drug in pharmacy customers with common cold symptoms. Int J Clin Pract. (2017) 71:e12907. doi: 10.1111/ijcp.12907
5. Müller-Lissner S, Schäfer E, Kondla A. Symptoms and their interpretation in patients self-treating abdominal cramping and pain with a spasmolytic (butylscoplolamine bromide) - a pharmacy-based survey. Pharmacol Pharmacy. (2011) 2:82–7. doi: 10.4236/pp.2011.22010
6. Storr M, Weigmann H, Landes S, Michel MC. Self-medication for the treatment of abdominal cramps and pain - a real-life comparison of three frequently used preparations. J Clin Med. (2022) 11:6361. doi: 10.3390/jcm11216361
7. Göbel H, Gessner U, Petersen-Braun M, Weingärtner U. Acetylsalicylic acid in self-medication of migraine. A pharmacy-based observational study. Schmerz. (2007) 21:49–54, 56. doi: 10.1007/s00482-006-0499-y
8. Gaul C, Gräter H, Weiser T. Results from a pharmacy-based patient survey on the use of a fixed combination analgesic containing acetylsalicylic acid, paracetamol and caffeine by self-diagnosing and self-treating patients. Springerplus. (2016) 5:721. doi: 10.1186/s40064-016-2369-0
9. Gaul C, Gräter H, Weiser T, Michel M, Lamperi A, Plomer M, et al. Impact of the neck and/or shoulder pain on self-reported headache treatment responses–results from a pharmacy-based patient survey. Front Neurol. (2022) 13:902020. doi: 10.3389/fneur.2022.902020
10. Lipton RB, Stewart WF. Acute migraine therapy: do doctors understand what patients with migraine want from therapy? Headache. (1999) 39:S20–6. doi: 10.1111/j.1526-4610.1999.00006.x
11. Smelt AFH, Louter MA, Kies DA, Blom JW, Terwindt GM, van der Heijden GJMG, et al. What do patients consider to be the most important outcomes for effectiveness studies on migraine treatment? Results of a Delphi study. PLoS ONE. (2014) 9:e98933. doi: 10.1371/journal.pone.0098933
12. Hamelsky SW, Lipton RB, Stewart WF. An assessment of the burden of migraine using the willingness to pay model. Cephalalgia. (2005) 25:87–100. doi: 10.1111/j.1468-2982.2005.00797.x
13. Sheftell FD, Dahlöf CGH, Brandes JL, Agosti R, Jones MW, Barrett PS. Two replicate randomized, double-blind, placebo-controlled trials of the time to onset of pain relief in the acute treatment of migraine with a fast-disintegrating/rapid-release formulation of sumatriptan tablets. Clin Ther. (2005) 27:407–17. doi: 10.1016/j.clinthera.2005.04.003
14. Diamond S, Balm TK, Freitag FG. Ibuprofen plus caffeine in the treatment of tension-type headache. Clin Pharmacol Ther. (2000) 68:312–9. doi: 10.1067/mcp.2000.109353
15. Rabbie R, Derry S, Moore RA. Ibuprofen with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Syst Rev. (2013) 2013:Cd008039. doi: 10.1002/14651858.CD008039.pub3
16. Derry CJ, Derry S, Moore RA. Caffeine as an analgesic adjuvant for acute pain in adults. Cochrane Database Syst Rev. (2014) 12:CD009281. doi: 10.1002/14651858.CD009281.pub3
17. Derry S, Wiffen PJ, Moore RA. Single dose oral ibuprofen plus caffeine for acute postoperative pain in adults. Cochrane Database Syst Rev. (2015) 2015:CD011509. doi: 10.1002/14651858.CD011509
18. Weiser T, Schepers C, Mück T, Lange R. Pharmacokinetic properties of ibuprofen (IBU) from the fixed-dose combination IBU/caffeine (400/100 mg; FDC) in comparison with 400 mg IBU as acid or lysinate under fasted and fed conditions—data from 2 single-center, single-dose, randomized crossover studies in healthy volunteers. Clini Pharmacol Drug Dev. (2019) 8:742–53. doi: 10.1002/cpdd.672
19. Weiser T, Richter E, Hegewisch A, Muse DD, Lange R. Efficacy and safety of a fixed-dose combination of ibuprofen and caffeine in the management of moderate to severe dental pain after third molar extraction. Eur J Pain. (2018) 22:28–38. doi: 10.1002/ejp.1068
20. Aicher B, Peil H, Peil B, Diener HC. Responsiveness of efficacy endpoints in clinical trials with over the counter analgesics for headache. Cephalalgia. (2012) 32:953–62. doi: 10.1177/0333102412452047
21. Max MB, Schafer SC, Culnane M, Dubner R, Gracely RH. Association of pain relief with drug side effects in postherpetic neuralgia: a single-dose study of clonidine, codeine, ibuprofen, and placebo. Clin Pharmacol Ther. (1988) 43:363–71. doi: 10.1038/clpt.1988.44
22. Berna C, Kirsch I, Zion SR, Lee YC, Jensen B, Sadler P, et al. Pain. (2017) 158:1014–20. doi: 10.1097/j.pain.0000000000000870
23. Fernandez A, Kirsch I, Noël L, Rodonti Y, Kaptech T, Suter M, et al. A test of positive suggestions about side effects as a way of enhancing the analgesic response to NSAIDs. PLoS ONE. (2019) 14:e0209851. doi: 10.1371/journal.pone.0209851
24. Diener H-C, Tassorelli C, Dodick DW, Silberstein SD, Lipton RB, Ashina M, et al. Guidelines of the International Headache Society for controlled trials of acute treatment of migraine attacks in adults: Fourth edition. Cephalalgia. (2019) 39:687–710. doi: 10.1177/0333102419828967
Keywords: ibuprofen, caffeine, headache, onset of analgesia, epidemiological study
Citation: Gaul C, Förderreuther S, Lehmacher W and Weiser T (2023) Correlation of effectiveness and tolerability assessments from a pharmacy-based observational study investigating the fixed-dose combination of 400 mg ibuprofen plus 100 mg caffeine for the treatment of acute headache. Front. Neurol. 14:1273846. doi: 10.3389/fneur.2023.1273846
Received: 07 August 2023; Accepted: 28 September 2023;
Published: 24 October 2023.
Edited by:
Parisa Gazerani, Oslo Metropolitan University, NorwayReviewed by:
Damiana Scuteri, University of Calabria, ItalyAmanda Tinsley, Georgetown University, United States
John Rothrock, Inova Health System, United States
Copyright © 2023 Gaul, Förderreuther, Lehmacher and Weiser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thomas Weiser, VGhvbWFzLndlaXNlckBzYW5vZmkuY29t