 Harsh Desai1†
Harsh Desai1† Mohammed Maan Al-Salihi2†
Mohammed Maan Al-Salihi2† Rami Z. Morsi1†
Rami Z. Morsi1† Omar R. Vayani3Sachin A. Kothari1Sonam Thind1Julián Carrión-Penagos1Archit Baskaran1Ammar Tarabichi4Veronica A. Bonderski5James E. Siegler1Mary Hahn6Elisheva R. Coleman1James R. Brorson1Scott J. Mendelson1
Omar R. Vayani3Sachin A. Kothari1Sonam Thind1Julián Carrión-Penagos1Archit Baskaran1Ammar Tarabichi4Veronica A. Bonderski5James E. Siegler1Mary Hahn6Elisheva R. Coleman1James R. Brorson1Scott J. Mendelson1 Ali Mansour1
Ali Mansour1 Guilherme Dabus7Michael Hurley8Shyam Prabhakaran1
Guilherme Dabus7Michael Hurley8Shyam Prabhakaran1 Italo Linfante7Tareq Kass-Hout1*
Italo Linfante7Tareq Kass-Hout1*- 1Department of Neurology, University of Chicago, Chicago, IL, United States
- 2Department of Neurological Surgery, School of Medicine and Public Health, University of Wisconsin, Madison, WI, United States
- 3Pritzker School of Medicine, University of Chicago, Chicago, IL, United States
- 4Department of Neurology, DENT Neurologic Institute, Amherst, NY, United States
- 5Department of Pharmacy, University of Chicago, Chicago, IL, United States
- 6Department of Neurology, Stony Brook University Hospital, Stony Brook, NY, United States
- 7Department of Neurology, Baptist Cardiac and Vascular Institute, Miami, FL, United States
- 8Department of Radiology, University of Chicago, Chicago, IL, United States
Background: The optimal antiplatelet therapy regimen for certain neuroendovascular procedures remains unclear. This study investigates the safety and feasibility of intravenous dose-adjusted cangrelor in patients undergoing acute neuroendovascular interventions.
Methods: We conducted a retrospective chart review of all consecutive patients on intravenous cangrelor for neuroendovascular procedures between September 1, 2020, and March 13, 2022. We also conducted an updated systematic review and meta-analysis using PubMed, Scopus, Web of Science, Embase and the Cochrane Library up to February 22, 2023.
Results: In our cohort, a total of 76 patients were included [mean age (years): 57.2 ± 18.2, males: 39 (51.3), Black: 49 (64.5)]. Cangrelor was most used for embolization and intracranial stent placement (n = 24, 32%). Approximately 44% of our patients had a favorable outcome with a modified Rankin Scale (mRS) score of 0 to 2 at 90 days (n = 25/57); within 1 year, 8% of patients had recurrent or new strokes (n = 5/59), 6% had symptomatic intracranial hemorrhage [sICH] (4/64), 3% had major extracranial bleeding events (2/64), and 3% had a gastrointestinal bleed (2/64). In our meta-analysis, 11 studies with 298 patients were included. The pooled proportion of sICH and intraprocedural thromboembolic complication events were 0.07 [95% CI 0.04 to 1.13] and 0.08 [95% CI 0.05 to 0.15], respectively.
Conclusion: Our study found that intravenous cangrelor appears to be safe and effective in neuroendovascular procedures, with low rates of bleeding and ischemic events. However, further research is needed to compare different dosing and titration protocols of cangrelor and other intravenous agents.
1 Introduction
The benefits of endovascular intervention for neurologic disease must be weighed against the risks, namely that of peri-procedural hemorrhage and cerebral infarction (1). Optimizing antithrombotic regimens during neuroendovascular procedures has become essential, particularly as new antiplatelet and anticoagulant agents are introduced to the market (2). Antiplatelet agents remain crucial during neuroendovascular interventions because the introduction of devices, such as stents, flow diverters, and embolization coils, promotes the adherence of fibrinogen and other plasma proteins to these foreign bodies, leading to thrombosis and obstruction (3). Commonly used antiplatelet agents include cyclo-oxygenase (COX)-1 inhibitors (e.g., aspirin), dipyridamole, glycoprotein IIb/IIIa inhibitors (e.g., tirofiban, eptifibatide), P2Y12 adenosine diphosphate (ADP) inhibitors (e.g., clopidogrel, prasugrel, ticagrelor), and phosphodiesterase (PDE) inhibitors (e.g., cilostazol) (2, 4, 5). However, these drugs come with the challenge of achieving a balance between thrombosis prevention and bleeding promotion (6).
Cangrelor is a newer generation P2Y12 ADP inhibitor that has demonstrated promise in achieving this balance. This drug has ideal pharmacokinetic properties, with rapid onset and short duration, allowing for more finer control of platelet inhibition (7). Cardiology trials have demonstrated that the drug effectively prevents periprocedural thrombotic events without significant increase in severe bleeding as well as a reduction in myocardial infarction and in-stent thrombosis (8, 9). Multiple case series and retrospective reviews have since demonstrated the therapeutic efficacy and safety of cangrelor in acute neuroendovascular interventions (10–16). Despite this, the evidence related to the safety and efficacy of intravenous cangrelor use for acute neuroendovascular interventions remains in question without any existing standardization in its utilization across institutions (17).
In this two-center study, we aimed to investigate the safety and feasibility of intravenous cangrelor in patients undergoing acute neurovascular interventions, such as acute stenting or embolization, and compare two different dosing titration regimens. We also aimed to conduct an updated systematic review and meta-analysis to assess the available literature about intravenous cangrelor in patients undergoing neuroendovascular procedures and pool the relevant data regarding cangrelor efficacy and safety.
2 Materials and methods
2.1 Retrospective study
2.1.1 Patient population
This is a two center retrospective study of all consecutive patients who underwent neuroendovascular procedures and were placed on intravenous cangrelor between September 1, 2020, and March 13, 2022. The Institutional Review Board at the University of Chicago approved the study protocol, and the need for informed consent was waived.
We included patients in this study if they met the following inclusion criteria: (1) age ≥ 18 years; patients underwent neuroendovascular procedures, such as endovascular thrombectomy (EVT), intracranial or carotid stenting, or aneurysm embolization using various techniques (e.g., stent-assisted coiling, flow diverter placement, etc.); and use of intravenous cangrelor regardless of duration.
2.1.2 Cangrelor protocol
Immediately after each neuroendovascular procedure, an intravenous (IV) bolus of 15 to 30 mcg/kg cangrelor was administered, followed by a starting maintenance infusion of 2 to 4 mcg/kg/min, depending on each institutional protocol (see Table 1). Due to the retrospective nature of the study the two protocols were only utilized at the respective centers where they were created. The cangrelor infusion was then titrated to goal P2Y12 reaction unit (PRU) level of 50 to 150 and maintained until bridging to oral antiplatelets was done. We used the VerifyNow P2Y12 (Accumetrics, San Diego, CA) to quantify the PRU level (18). P2Y12 reaction unit assays are typically done daily. Bridging to oral antiplatelet therapy is considered when PRU goal has been met, but can be provider-dependent, especially if there are other planned procedures (e.g., gastrostomy tube insertions, etc.). Titration to oral antiplatelet therapy (e.g., clopidogrel or ticagrelor) occurred before or immediately post-cangrelor infusion discontinuation, and patients were subsequently discharged on dual antiplatelet therapy (e.g., aspirin and clopidogrel, aspirin and ticagrelor). For example, patients were given a ticagrelor loading dose 2 h prior to cangrelor infusion cessation versus stopping the infusion and immediately giving a clopidogrel load. Table 1 further summarizes the two cangrelor infusion protocols and the timing of bridging with cangrelor infusion.
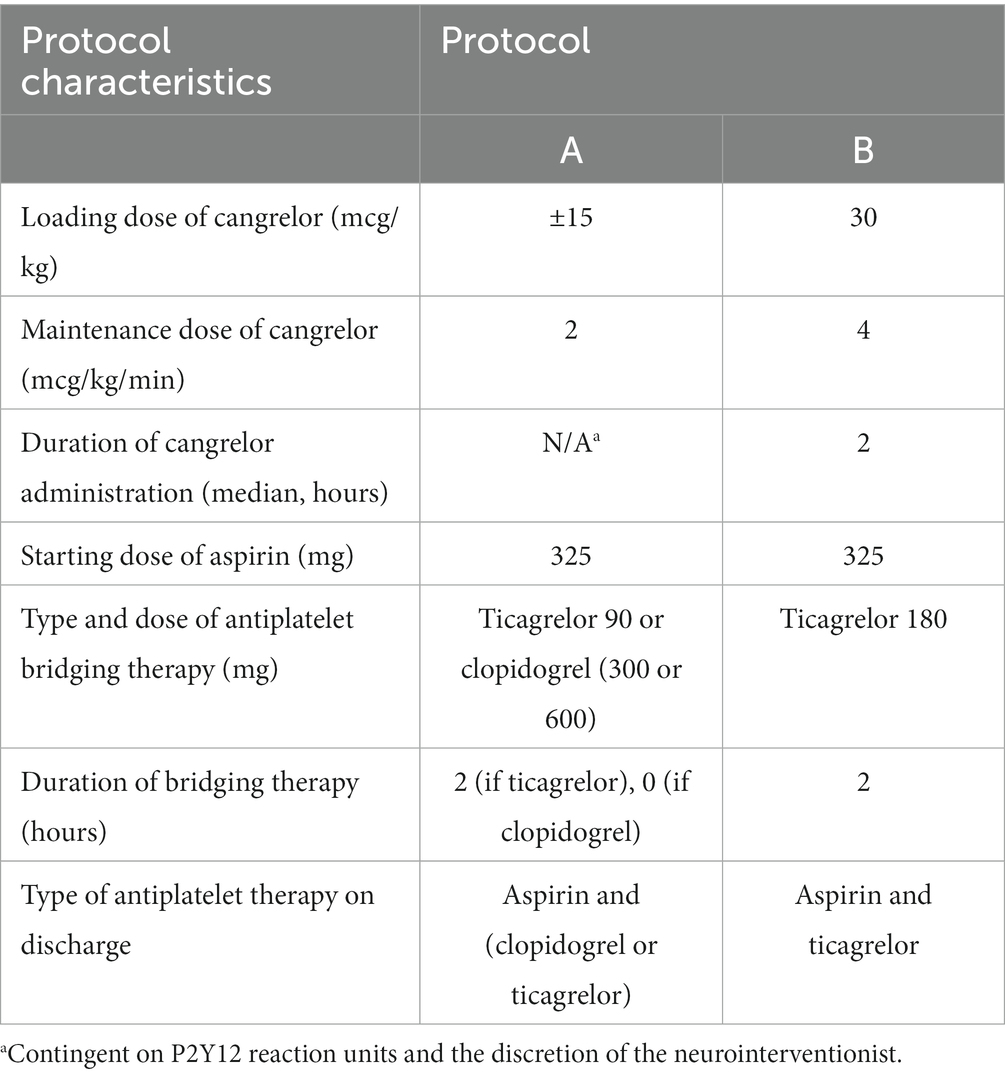
Table 1. Detailed outline of different cangrelor infusion protocols.
2.1.3 Patient outcomes
For patients with acute internal carotid artery (ICA) or another intracranial vessel occlusion, we defined favorable functional outcome as a modified Rankin Scale (mRS) score of 0 to 2 at 90 days. We also assessed for the following outcomes at 6 months to 1 year: recurrent or new strokes; symptomatic intracranial hemorrhage (sICH), defined as any intracranial hemorrhage associated with worsening neurologic exam, clinical deterioration or death, adapted from the Heidelberg Bleeding Classification (19); asymptomatic intracranial hemorrhage (aICH), defined as any intracranial hemorrhage without worsening neurologic exam, clinical deterioration or death; in-stent thrombosis; gastrointestinal bleeding events; or retroperitoneal hematoma.
2.2 Statistical analysis
Baseline characteristics are summarized using median and interquartile range (IQR) or mean and standard deviation for continuous variables. Frequency distribution was used for categorical variables, such as NIHSS and mRS scores. Dichotomous outcome measures, such as mortality at discharge and at 90 days, favorable functional outcomes at discharge and at 90 days, sICH, aICH, major extracranial and gastrointestinal bleeding events, new or recurrent and disposition between the two protocol groups were analyzed using chi-squared or Fisher’s exact test when appropriate. All statistical analysis of the cohort study was completed using SPSS V28.0.1.1.
2.3 Systematic review
2.3.1 Standardized reporting and registration
We designed our systematic review and meta-analysis according to the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (20, 21). We registered our systematic review protocol on PROSPERO (CRD42023403598).
2.3.2 Data sources and searches
With the help of an information specialist, we searched the following databases from inception to February 22, 2023: PubMed, Scopus, Web of Science, Embase and the Cochrane Library. We did not use any language restrictions. We used the following keywords: cangrelor, AR-C69931MX, Kengreal®, Canreal, stroke, strokes, CVA, brain vascular accident, apoplexy, cerebrovascular, and neuroendovascular. We also hand-searched the grey literature and reference lists of included studies to decrease the risk of publication bias.
2.3.3 Study selection and data extraction
We included studies assessing the safety and efficacy of intravenous cangrelor in the setting of acute neuroendovascular procedures, such as with stroke or aneurysm treatment. Editorials, commentaries, literature and systematic reviews, and case reports were excluded from the systematic review. In vitro, animal and cadaveric studies were also excluded. Otherwise, we did not place any restrictions on the study design due to the limited availability of data.
Teams of two reviewers participated in calibration exercises before the screening phase and subsequently screened each citation independently, then cross-verified each reference. Following the title and abstract screening portion, reviewers retrieved the full texts of eligible citations, screened each full text independently, and then cross-verified its eligibility. An additional reviewer resolved any disagreements using a modified Delphi consensus, when applicable. Reviewers then extracted data from each study independently and cross-verified the extracted data in duplicate using previously developed standardized extraction forms. Reviewers extracted the following data: study characteristics (e.g., country of origin, study design, sample size), intervention details (e.g., bolus, drip rate, aspirin dose, neuro-endovascular procedure), and treatment outcomes, including hemorrhagic and other procedural complications.
2.3.4 Risk of bias assessment
Teams of two reviewers independently assessed the quality of included studies using the Newcastle Ottawa scale (NOS) and the National Institutes of Health (NIH) Quality Assessment Tool for non-randomized studies (22, 23). We used the NIH tool for case series assessment, and NOS for cohort studies. We resolved any discrepancies via consensus.
2.3.5 Data synthesis and analysis
For our meta-analysis, all our assessed outcomes were categorical, which we analyzed as event rates with 95% CIs. The fixed effect model was first applied if the effect estimate was pooled from homogeneous studies; otherwise, the random effect model was used. Also, we investigated the statistical heterogeneity among studies using the I2 statistics chi-squared test, with p > 0.1 considered heterogeneous and I2 ≥ 50% suggestive of high heterogeneity. As our included studies for each assessed outcome were less than 10, the publication bias assessment by funnel plot and Egger’s test were not applicable (24). We conducted our meta-analysis using Comprehensive Meta-Analysis (CMA) software V3.
2.3.6 Certainty of evidence assessment
We used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) to assess the strength and degree of evidence for recommendations. The certainty level in the scale consisted of four categories: high quality, which implies that additional research is not required and the confidence in the estimated effects is unlikely to change; moderate quality, which implies that further studies may impact the confidence in the estimated effects; low quality, which implies that additional research is likely to significantly impact the confidence in the estimated effects and potentially alter the estimation; and very low quality, which indicates uncertainty in the estimation.
3 Results
3.1 Retrospective study
3.1.1 Baseline demographic and clinical characteristics
Seventy-six patients were included in our study. Sixty-six patients were administered protocol A, and 10 were administered protocol B cangrelor infusions. The average age was 57.2 ± 18.2 years, and 51% were males. Most were African American (65%). One quarter of our patients were active smokers (25%), and 46% had a history of hypertension.
Most of our patients underwent a neuroendovascular procedure for stroke or symptomatic carotid disease (44/76, 58%), followed by both ruptured or unruptured aneurysms (19/76, 25%). Other cases included carotid-cavernous fistulas, traumatic vessel injury or carotid blowout syndromes and idiopathic intracranial hypertension. Additional clinical and procedural characteristics are outlined in Table 2.
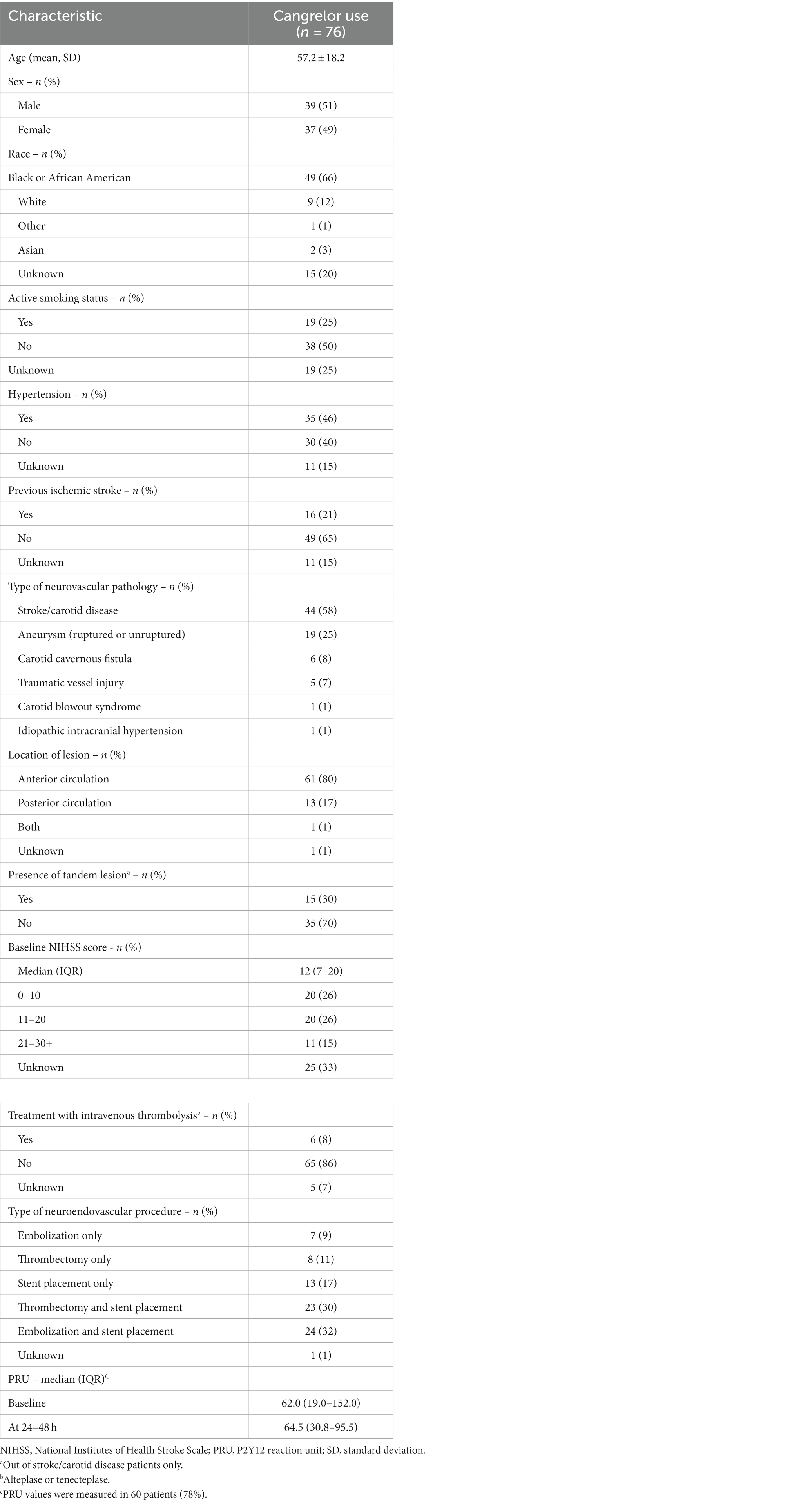
Table 2. Baseline demographic and clinical characteristics.
3.1.2 Outcomes
In our cohort, we assessed for the following patient-important outcomes: mortality at 90 days, favorable functional outcome, defined by an mRS score of 0 to 2 at 90 days, and sICH. In our stroke and carotid disease group, mortality and favorable functional outcomes at 90 days were seen in 9 (21%) and 8 (24%) patients, respectively. Symptomatic intracranial hemorrhage was seen in 2 patients (7%). Two patients had major extracranial bleeding events (7%), including gastrointestinal bleeding (1/44, 3%). Most ischemic patients were discharged to an acute rehabilitation facility (18/44, 41%). In our aneurysm cohort, mortality and favorable functional outcomes at 90 days were seen in 4 (21%) and 6 (40%) patients, respectively. Among the aneurysm group, symptomatic intracranial hemorrhage was seen in 1 patient (6%), and no other bleeding events were seen. Outcomes for stroke and aneurysm groups are detailed in Table 3, and outcomes for ischemic - stroke, symptomatic carotid disease - and non-ischemic patients - aneurysms, carotid-cavernous fistulas, traumatic vessel injury, and other pathologies - are highlighted in Supplementary Table S1. Additional outcomes relating to ruptured versus unruptured aneurysms can be found in Supplementary Table S2.
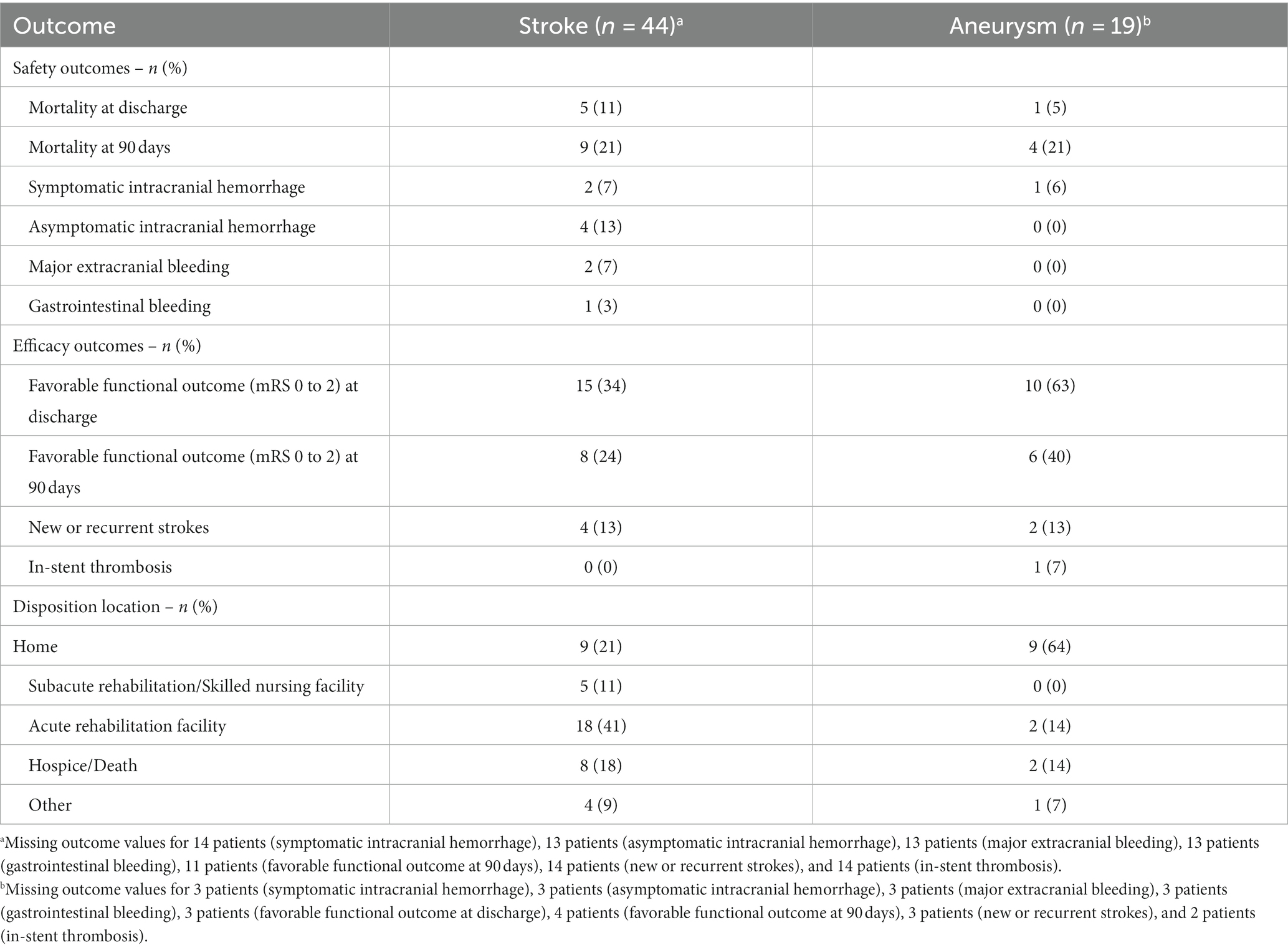
Table 3. Clinical outcomes by pathology – stroke versus aneurysm.
When we compared outcomes between patients placed on different cangrelor infusion protocols, we found that mortality at 90 days occurred in 26% of patients who received Protocol A compared to 20% of patients who received Protocol B, but this difference was not significant (p = 0.24). Similarly, the proportion of patients with favorable functional outcomes at 90 days was also lower in the Protocol A group compared to that seen in the Protocol B group, but this difference was also not significant (40% vs. 60%, p = 0.31). Symptomatic intracranial hemorrhage was higher in the Protocol A group, and none was seen in the Protocol B group, but this difference was insignificant (7% vs. 0%, p = 0.38). Other bleeding events, such as major extracranial and gastrointestinal bleeding, were seen less in Protocol A than in Protocol B, but this difference did not meet significance (2% vs. 10%, p = 0.29). In-stent thrombosis occurred in 1 patient under the Protocol A group, which was attributed to nonadherence to oral antiplatelet therapy after cangrelor termination. Outcomes by cangrelor infusion protocol can be seen in Table 4.
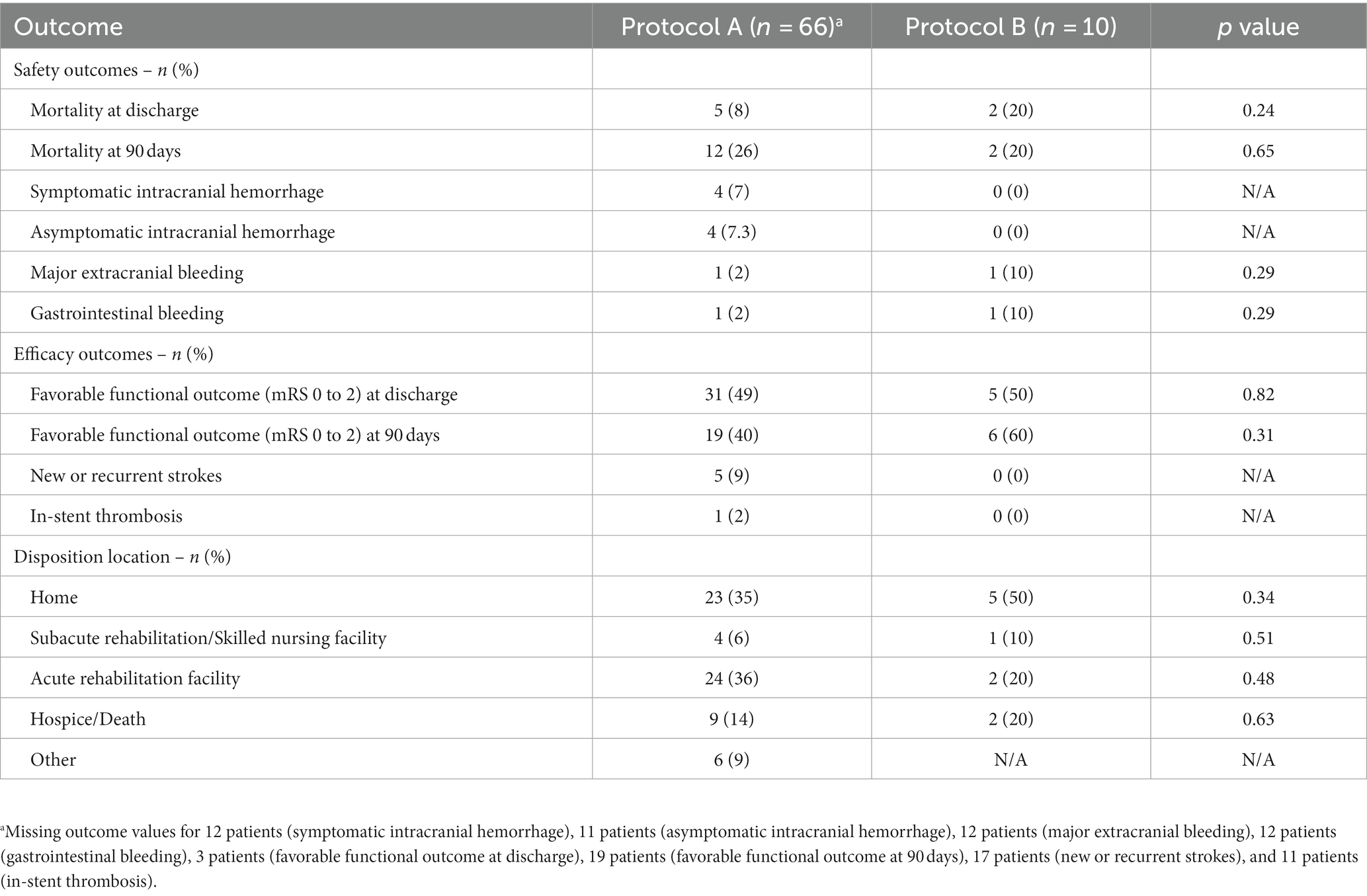
Table 4. Clinical outcomes by cangrelor infusion protocol.
3.2 Systematic review
3.2.1 Results of the literature search
Our search method using five databases resulted in 988 studies. After duplicate elimination, 506 studies were eligible for screening. Following title and abstract screening, 25 articles were found eligible for full-text screening. Of these, 14 were excluded, leaving 11 articles that met our inclusion criteria for our systematic review (10–15, 25–29), including nine studies eligible for meta-analysis (10–12, 14, 15, 25–27, 29). Figure 1 shows the PRISMA flow diagram for the study selection.
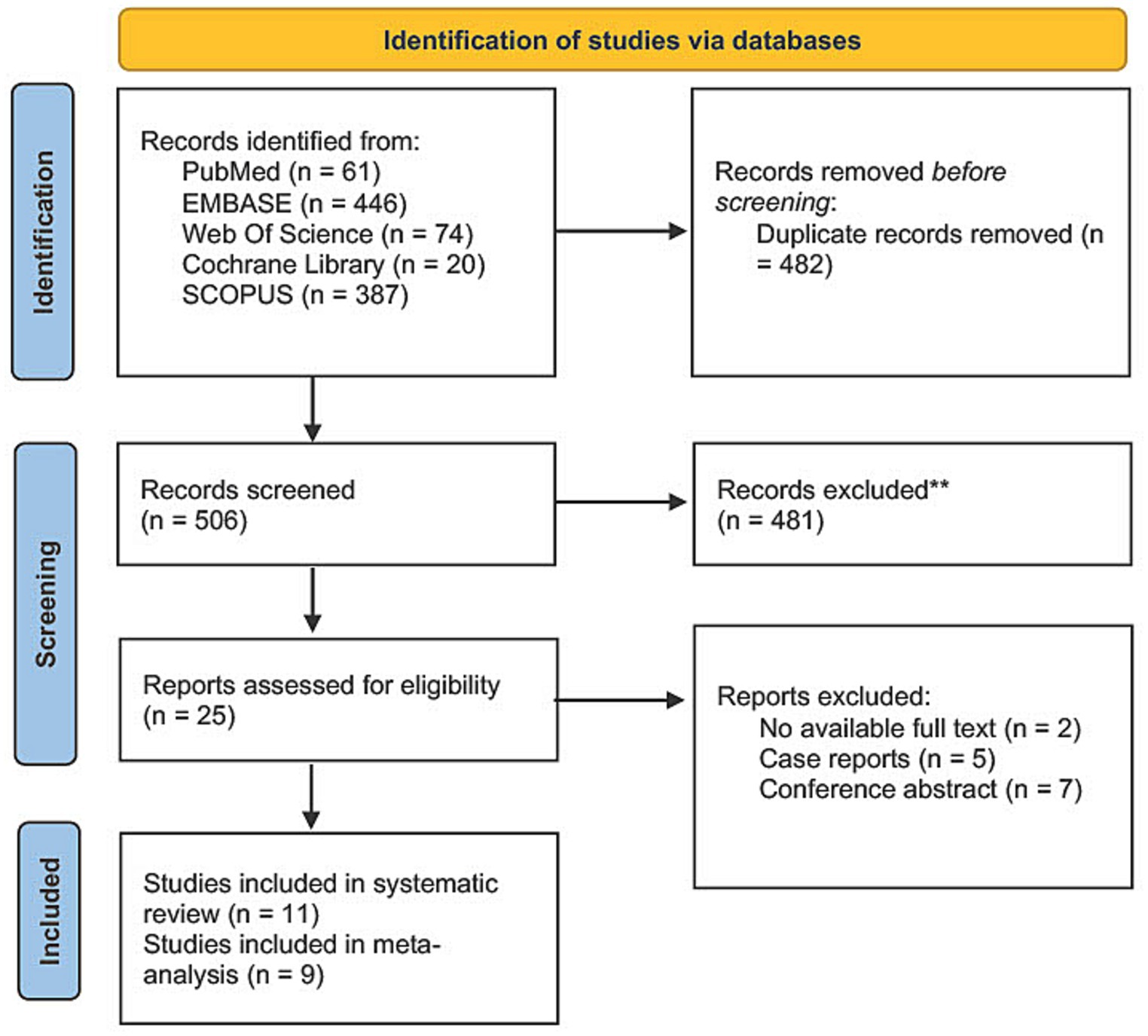
Figure 1. PRISMA flow diagram.
3.2.2 Characteristics of included studies
Our review included 11 studies with 298 patients, most of which were conducted in the USA. Ten studies were case series, while one study was a retrospective cohort. Five studies reported cangrelor use with stent-assisted coiling or flow-diverter stents (13–15, 25, 27), three reported using cangrelor with stent-retriever and/or aspiration (10, 12, 26), two reported using cangrelor with acute stenting (11, 29) and one reported using it with stenting or bridging (28). The bolus cangrelor regimen in included studies ranged from 5 to 40 μg/kg, while the infusion rate ranged from 0.75 to 4 μg/kg/min. In seven studies, aspirin was used as an adjuvant antiplatelet therapy with doses ranging from 75 to 500 mg daily. Supplementary Table S3 summarizes the characteristics of our included studies.
3.2.3 Risk of bias assessment
Ten of our studies were assessed by the NIH tool for case series, and one study was assessed using the NOS scale for cohort studies. Nine studies showed overall good quality assessment, while two studies were of fair quality. The fair quality of the latter two studies was attributed to the inadequate description of the studied population, intervention, and statistical method used. Supplementary Tables S4 and S5 summarize the authors’ judgments using the NIH tool and NOS for each parameter.
3.2.4 Outcomes
3.2.4.1 Symptomatic intracranial hemorrhage
Symptomatic intracranial hemorrhage with cangrelor use was assessed in nine studies and reported in 10 patients (7, 95% confidence interval [CI] 4.3 to 12.7). (10–12, 14, 15, 25–27, 29) The pooled studies were homogeneous, with I2 and p values were 0% and 0.90, respectively. The forest plot for sICH is shown in Figure 2.
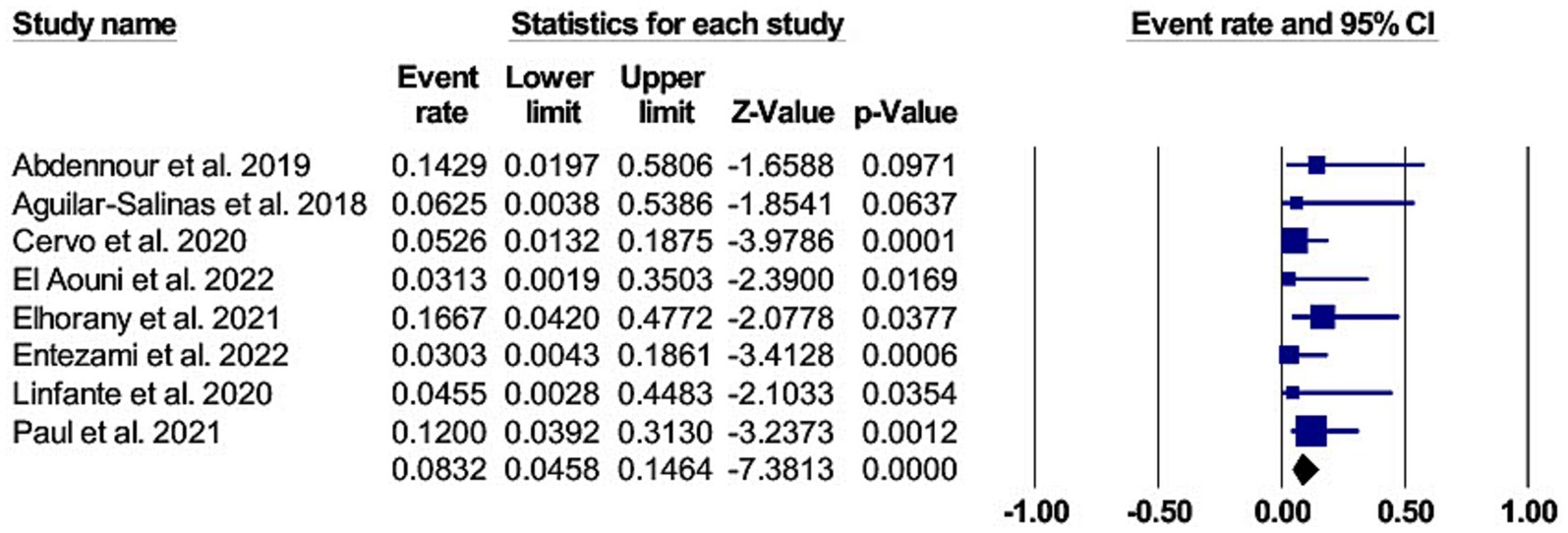
Figure 2. A forest plot of the asymptomatic intracranial hemorrhage.
3.2.4.2 Asymptomatic intracranial hemorrhage
Eight studies reported the occurrence of aICH in 13 patients with cangrelor use (8, 95% CI 4.6 to 14.6) (11, 12, 14, 15, 25–27, 29). The studies were homogenous, with I2 and p-values of 0% and 0.77, respectively. The forest plot for aICH is shown in Figure 3.
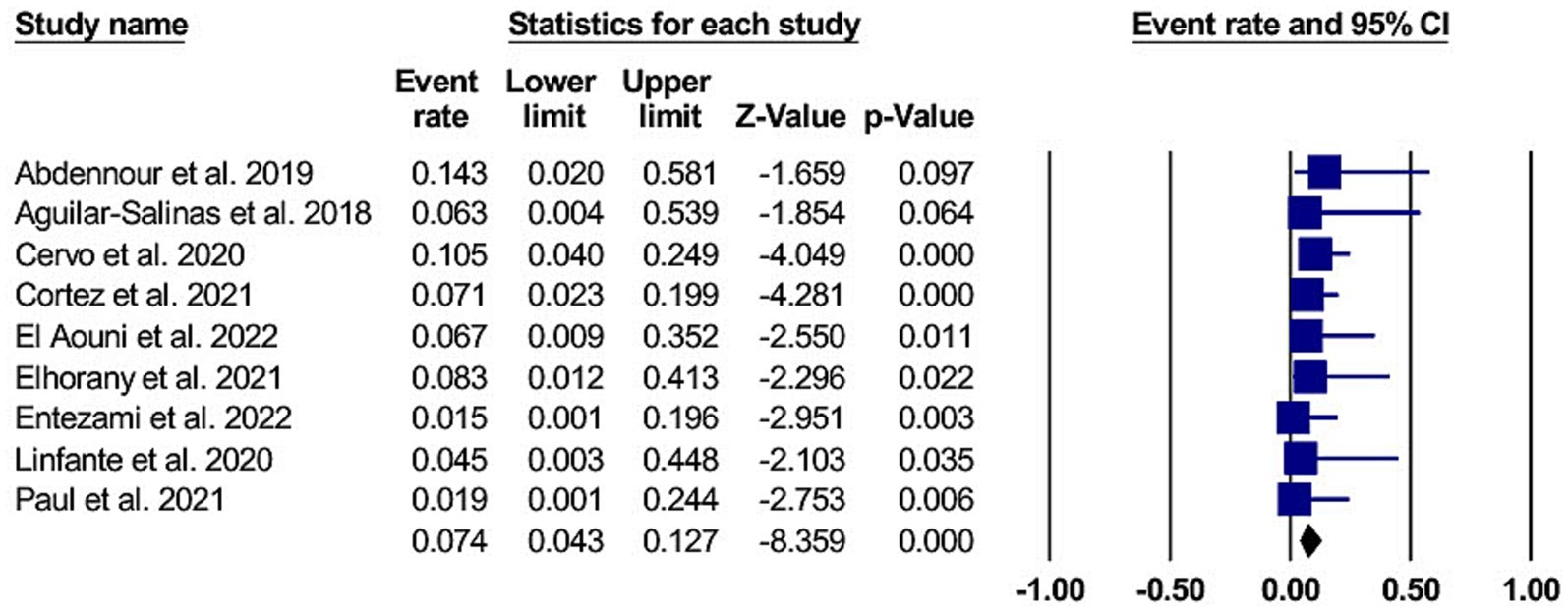
Figure 3. A forest plot of the symptomatic intracranial hemorrhage.
3.2.4.3 Retroperitoneal hematoma
The use of cangrelor and retroperitoneal hematoma occurrence was reported in nine studies involving two patients (3, 95% CI 1.5 to 7.7). (10–12, 14, 15, 25–27, 29) The pooled studies were homogenous, with I2 and p-values of 0% and 0.97, respectively. The forest plot for retroperitoneal hematoma is shown in Figure 4.
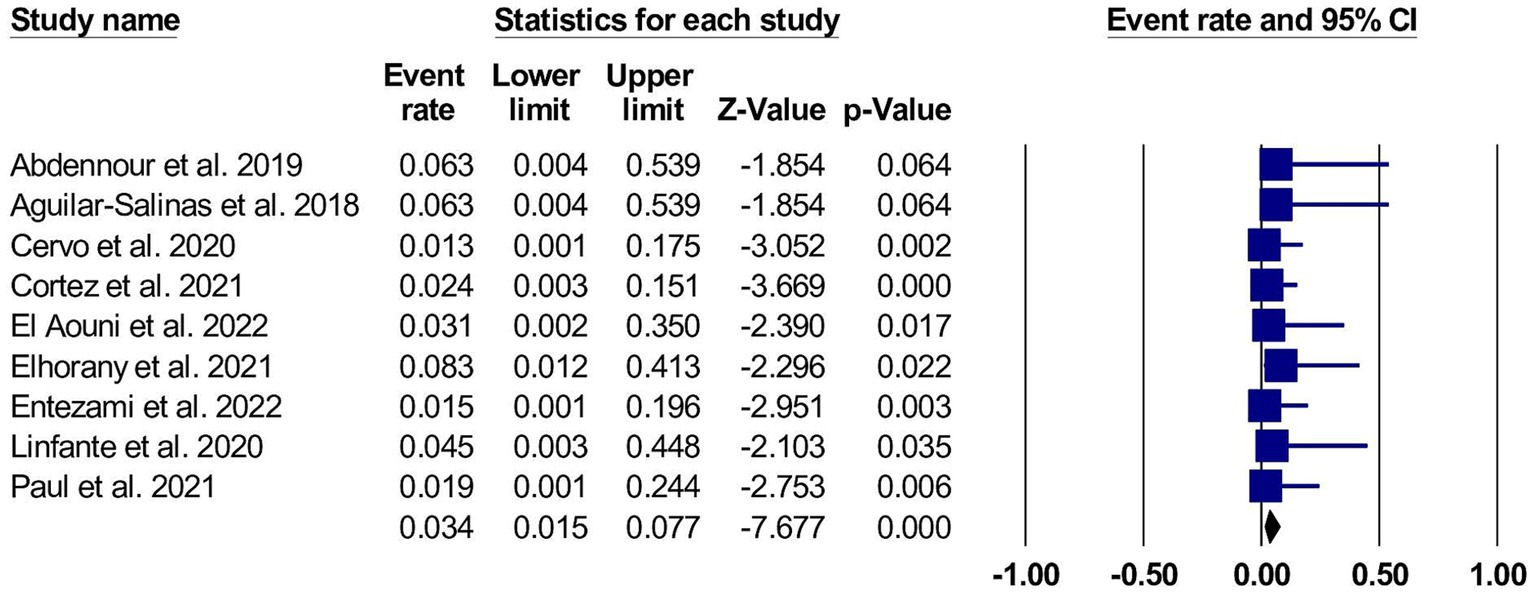
Figure 4. A forest plot of the retroperitoneal hematoma.
3.2.4.4 Intraprocedural thromboembolic complication
Nine studies reported the occurrence of this event when cangrelor was used for neuroendovascular procedures in two patients (3, 95% CI 1.2 to 6.8). (10–12, 14, 15, 25–27, 29) The studies were homogeneous, with I2 and p-values of 0% and 0.99, respectively. The forest plot for the intraprocedural thromboembolic complication is shown in Figure 5.
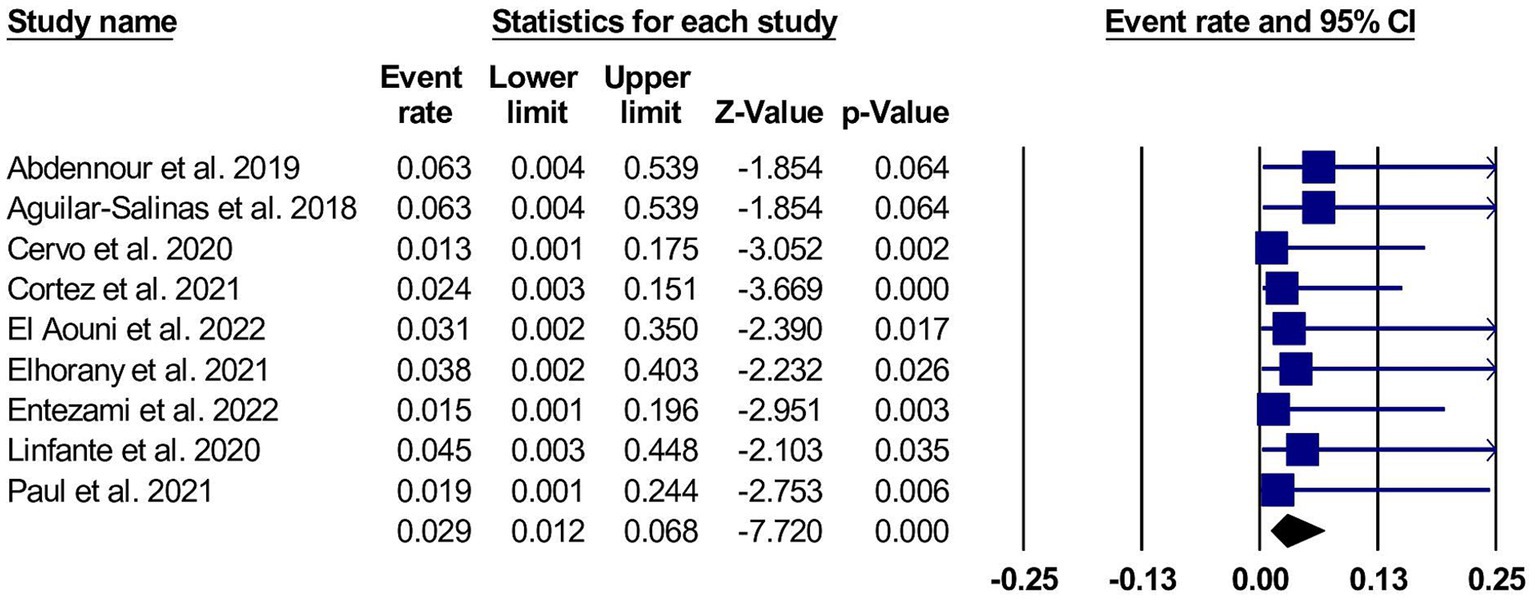
Figure 5. A forest plot of the intraprocedural thromboembolic complication.
3.2.5 GRADE assessment
The certainty of evidence assessed in our systematic review is detailed in Supplementary Table S6. According to GRADE, all our outcomes were at a very low level of certainty, and the causes of their downgrading were: small sample size in each assessed outcome, the evidence pooled from observational studies attributed it to publication bias.
4 Discussion
This study is one of the first few studies to demonstrate the safety and efficacy of intravenous dose-adjusted cangrelor for acute neuroendovascular procedures and to directly compare outcomes between two different cangrelor infusion protocols in this population. Our study also uses the largest cohort of patients on dose-adjusted cangrelor from a two center, adding to the growing body of evidence that cangrelor infusion protocols require adjustment when applied to neurovascular pathologies, such as strokes and aneurysms.
Our retrospective study found that 34% of our stroke patients had a favorable functional outcome upon discharge. Among our stroke and ICA occlusion cohort, the sICH rate was 7%, with one gastrointestinal bleeding event and one femoral artery puncture with bleeding complication. When we stratified the sICH rate by cangrelor infusion protocol, we found that the sICH rate was comparable among those who received a 30 mcg/kg bolus followed by a 4 mcg/kg/min dose to those who received a 15 mcg/kg bolus followed by 2 mcg/kg/min maintenance with dose adjusted to PRU levels. Additionally, the favorable outcomes in the lower bolus group were similar to that of the higher bolus group. It is difficult to interpret these findings given the small sample size for both groups. Our updated meta-analysis demonstrates that the sICH rate with periprocedural cangrelor in a largely ischemic stroke population is approximately 7%, which is similar to results from previous meta-analyses where pooled sICH rates ranged from 6 to 9% (29, 30). On the other hand, two previous meta-analyses evaluating the use of tirofiban in stroke reported the sICH rate ranged from 7 to 9% (31, 32), and one matched cohort study of patients undergoing thrombectomy with eptifibatide reported an sICH rate of 6% (33). In a cohort study including 15 stroke patients who underwent neuroendovascular procedures and were administered abciximab, an irreversible glycoprotein IIb/IIIa inhibitor, sICH was found in 20% of patients (34). Considering these findings, cangrelor may be a reasonable alternative option. The safety of intravenous cangrelor may be attributed, in part, to its short half-life of 2 to 5 min and the restoration of platelet activity within 30 to 60 min from the time of discontinuation (35). These properties make cangrelor suitable for neuroendovascular treatment, but the dosing protocols remain under scrutiny and real-time PRU testing is not widely available. Additionally, when comparing cangrelor to other P2Y12 receptor inhibitors, it had several advantages that could be attributed to its nonthienopyridine structure. For example, cangrelor is a reversible P2Y12 receptor inhibitor and is not dependent on hepatic metabolism for activation, unlike thienopyridines such as clopidogrel and prasugrel (36–39). Moreover, cangrelor can rapidly and effectively prevent platelet aggregation, and it acts more quickly and for a shorter duration than clopidogrel (40, 41). These properties mentioned above could make it a more attractive option when emergent platelet inhibition is needed and the risk of hemorrhage is substantial.
Among our 19 aneurysm patients who underwent neuroendovascular treatment, the sICH rate was 6%. When we stratified the sICH rate according to the cangrelor infusion protocol, we found that the cardiac dosing protocol for cangrelor (Protocol B) was associated with a similar sICH rate compared to the lower aforementioned dose. In comparison to a study comparing two different dosing protocols for tirofiban, tirofiban was correlated with an increased intracranial hemorrhage rate ranging from 4 to 6% in patients with intracranial aneurysms who underwent stent-assisted coil embolization and correlated with an increased thromboembolic complication rate of 6% (42, 43). Additionally, in our meta-analysis, the thromboembolic complication was 3%, which is lower than the previously mentioned literature.
In our cohort of aneurysm patients, only one in-stent thrombosis occurred, and this was unrelated to cangrelor infusion and more related to nonadherence to oral antiplatelet therapy after discharge. A pooled analysis by Entezami and colleagues also demonstrated only one case of in-stent thrombosis in a ruptured aneurysm case due to a subtherapeutic PRU (27), which is consistent with our findings.
While our study is the first to summarize outcomes in a single cohort of patients who underwent acute neuroendovascular procedures stratified by different cangrelor infusion protocols, other studies achieved similar findings indirectly only by pooling data (27, 29). Additionally, our systematic review is the first to use the GRADE criteria to declare the certainty of our evidence. However, our study was not free of limitations. One drawback of the retrospective portion of the study was the large variation in types of procedures that were completed. Due to this it can lead to complications unique to each individual pathology, which may affect the outcomes that were observed. Additionally, the patient population is heavily skewed to one race due to the geographic location of the treating institutions. The main drawback of our meta-analysis was the study design of our included studies which were all observational studies limiting its generalizability. The small sample size of our included studies also makes the evidence imprecise and prone to type II error (false negative results). Also, because the studies were observational by design, they may contribute to publication bias even if we cannot assess this due to the small number of pooled studies per outcome (less than 10) (44, 45). For the causes mentioned above, the overall certainty of evidence for all the outcomes was very low. Therefore, larger studies using standardized treatment protocols are called upon to validate these findings.
In conclusion, our two-center study and updated meta-analysis demonstrate intravenous cangrelor’s potential safety and efficacy, highlighted by the relatively low bleeding event rates and ischemic events. Our study also calls attention to the need for higher-quality studies comparing different dosing and titration protocols of cangrelor as well as different intravenous agents in the setting of neuroendovascular procedures.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The University of Chicago Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because of the retrospective nature of the study that did not require any direct patient contact.
Author contributions
HD: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft. MA-S: Conceptualization, Data curation, Formal analysis, Writing – original draft. RM: Conceptualization, Data curation, Writing – original draft. OV: Data curation, Writing – review & editing. SK: Data curation, Writing – review & editing. ST: Data curation, Writing – review & editing. JC-P: Data curation, Writing – review & editing. AB: Data curation, Writing – review & editing. AT: Data curation, Writing – review & editing. VB: Writing – review & editing. JS: Writing – review & editing. MaH: Writing – review & editing. EC: Writing – review & editing. JB: Writing – review & editing. SM: Writing – review & editing. AM: Writing – review & editing. GD: Data curation, Writing – review & editing. MiH: Writing – review & editing. SP: Writing – review & editing. IL: Data curation, Writing – review & editing. TK-H: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1304599/full#supplementary-material
References
1. Jumaa, MA, Salahuddin, H, and Burgess, R. The future of endovascular therapy. Neurology. (2021) 97:S185–93. doi: 10.1212/WNL.0000000000012807
2. Fiorella, D, Thiabolt, L, Albuquerque, FC, Deshmukh, VR, McDougall, CG, and Rasmussen, PA. Antiplatelet therapy in neuroendovascular therapeutics. Neurosurg Clin N Am. (2005) 16:517–40, vi. doi: 10.1016/j.nec.2005.03.003
3. Baier, RE, and Dutton, RC. Initial events in interactions of blood with a foreign surface. J Biomed Mater Res. (1969) 3:191–206. doi: 10.1002/jbm.820030115
4. Kamarova, M, Baig, S, Patel, H, Monks, K, Wasay, M, Ali, A, et al. Antiplatelet use in ischemic stroke. Ann Pharmacother. (2022) 56:1159–73. doi: 10.1177/10600280211073009
5. Powers, WJ, Rabinstein, AA, Ackerson, T, Adeoye, OM, Bambakidis, NC, Becker, K, et al. Guidelines for the early Management of Patients with Acute Ischemic Stroke: 2019 update to the 2018 guidelines for the early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211
6. Nishi, H, Nakahara, I, Matsumoto, S, Hashimoto, T, Ohta, T, Sadamasa, N, et al. Platelet reactivity and hemorrhage risk in neurointerventional procedures under dual antiplatelet therapy. J Neurointerv Surg. (2016) 8:949–53. doi: 10.1136/neurintsurg-2015-011844
7. Qamar, A, and Bhatt, DL. Current status of data on cangrelor. Pharmacol Ther. (2016) 159:102–9. doi: 10.1016/j.pharmthera.2016.01.004
8. Angiolillo, DJ, Bhatt, DL, Steg, PG, Stone, GW, White, HD, Gibson, CM, et al. Impact of cangrelor overdosing on bleeding complications in patients undergoing percutaneous coronary intervention: insights from the CHAMPION trials. J Thromb Thrombolysis. (2015) 40:317–22. doi: 10.1007/s11239-015-1233-3
9. de Luca, L, Steg, PG, Bhatt, DL, Capodanno, D, and Angiolillo, DJ. Cangrelor: clinical data, contemporary use, and future perspectives. J Am Heart Assoc. (2021) 10:e022125. doi: 10.1161/JAHA.121.022125
10. Cortez, GM, Monteiro, A, Sourour, N, Clarençon, F, Elhorany, M, Grigoryan, M, et al. The use of cangrelor in neurovascular interventions: a multicenter experience. Neuroradiology. (2021) 63:925–34. doi: 10.1007/s00234-020-02599-2
11. Aguilar-Salinas, P, Agnoletto, GJ, Brasiliense, LBC, Santos, R, Granja, MF, Gonsales, D, et al. Safety and efficacy of cangrelor in acute stenting for the treatment of cerebrovascular pathology: preliminary experience in a single-center pilot study. J Neurointerv Surg. (2019) 11:347–51. doi: 10.1136/neurintsurg-2018-014396
12. Cervo, A, Ferrari, F, Barchetti, G, Quilici, L, Piano, M, Boccardi, E, et al. Use of Cangrelor in cervical and intracranial stenting for the treatment of acute ischemic stroke: a "real life" single-Center experience. AJNR Am J Neuroradiol. (2020) 41:2094–9. doi: 10.3174/ajnr.A6785
13. Entezami, P, Holden, DN, Boulos, AS, Paul, AR, Field, NC, Nourollahzadeh, E, et al. Cangrelor dose titration using platelet function testing during cerebrovascular stent placement. Interv Neuroradiol. (2021) 27:88–98. doi: 10.1177/1591019920936923
14. Cheddad el Aouni, M, Magro, E, Abdelrady, M, Nonent, M, Gentric, JC, and Ognard, J. Safety and efficacy of Cangrelor among three antiplatelet regimens during stent-assisted endovascular treatment of Unruptured intracranial aneurysm: a single-Center retrospective study. Front Neurol. (2022) 13:727026. doi: 10.3389/fneur.2022.727026
15. Linfante, I, Ravipati, K, Starosciak, AK, Reyes, D, and Dabus, G. Intravenous cangrelor and oral ticagrelor as an alternative to clopidogrel in acute intervention. J Neurointerv Surg. (2021) 13:30–2. doi: 10.1136/neurintsurg-2020-015841
16. Barra, ME, Berger, K, Tesoro, EP, and Brophy, GM. Periprocedural Neuroendovascular antiplatelet strategies for thrombosis prevention in Clopidogrel-Hyporesponsive patients. Pharmacotherapy. (2019) 39:317–34. doi: 10.1002/phar.2228
17. Faught, RW, Satti, SR, Hurst, RW, Pukenas, BA, and Smith, MJ. Heterogeneous practice patterns regarding antiplatelet medications for neuroendovascular stenting in the USA: a multicenter survey. J Neurointerv Surg. (2014) 6:774–9. doi: 10.1136/neurintsurg-2013-010954
18. Malinin, A, Pokov, A, Spergling, M, Defranco, A, Schwartz, K, Schwartz, D, et al. Monitoring platelet inhibition after clopidogrel with the VerifyNow-P2Y12(R) rapid analyzer: the VERIfy thrombosis risk ASsessment (VERITAS) study. Thromb Res. (2007) 119:277–84. doi: 10.1016/j.thromres.2006.01.019
19. von Kummer, R, Broderick, JP, Campbell, BCV, Demchuk, A, Goyal, M, Hill, MD, et al. The Heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. (2015) 46:2981–6. doi: 10.1161/STROKEAHA.115.010049
20. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. (2021) 134:178–89. doi: 10.1016/j.jclinepi.2021.03.001
21. Higgins, JPT, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, et al. (editors) Cochrane handbook for systematic reviews of interventions version 6.4. Cochrane. (2023). Available at: https://www.training.cochrane.org/handbook.
22. Wells, GA, Shea, B, O’Connell, D, Peterson, J, Welch, V, Losos, M, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Oxford: (2000). Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
23. Institution, N.H. (n.d). Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
24. Terrin, N, Schmid, CH, Lau, J, and Olkin, I. Adjusting for publication bias in the presence of heterogeneity. Stat Med. (2003) 22:2113–26. doi: 10.1002/sim.1461
25. Abdennour, L, Sourour, N, Drir, M, Premat, K, Shotar, E, Taylor, G, et al. Preliminary experience with Cangrelor for endovascular treatment of challenging intracranial aneurysms. Clin Neuroradiol. (2020) 30:453–61. doi: 10.1007/s00062-019-00811-2
26. Elhorany, M, Lenck, S, Degos, V, Sourour, NA, Frasca Polara, G, Shotar, E, et al. Cangrelor and stenting in acute ischemic stroke: monocentric case series. Clin Neuroradiol. (2021) 31:439–48. doi: 10.1007/s00062-020-00907-0
27. Entezami, P, Dalfino, JC, Boulos, AS, Yamamoto, J, Holden, DN, Field, NC, et al. Use of intravenous cangrelor in the treatment of ruptured and unruptured cerebral aneurysms: an updated single-center analysis and pooled analysis of current studies. J Neurointerv Surg. (2022) 15:669–73. doi: 10.1136/neurintsurg-2022-018986
28. Holden, DN, Entezami, P, Bush, MC, Field, NC, Paul, AR, Boulos, AS, et al. Characterization of antiplatelet response to low-dose cangrelor utilizing platelet function testing in neuroendovascular patients. Pharmacotherapy. (2021) 41:811–9. doi: 10.1002/phar.2619
29. Paul, AR, Entezami, P, Holden, D, Field, N, Dalfino, J, and Boulos, A. Use of intravenous cangrelor and stenting in acute ischemic stroke interventions: a new single center analysis and pooled-analysis of current studies. Interv Neuroradiol. (2021) 27:837–42. doi: 10.1177/15910199211014417
30. Marnat, G, Finistis, S, Delvoye, F, Sibon, I, Desilles, JP, Mazighi, M, et al. Safety and efficacy of Cangrelor in acute stroke treated with mechanical Thrombectomy: endovascular treatment of ischemic stroke registry and meta-analysis. AJNR Am J Neuroradiol. (2022) 43:410–5. doi: 10.3174/ajnr.A7430
31. Gong, J, Shang, J, Yu, H, Wan, Q, Su, D, Sun, Z, et al. Tirofiban for acute ischemic stroke: systematic review and meta-analysis. Eur J Clin Pharmacol. (2020) 76:475–81. doi: 10.1007/s00228-019-02817-8
32. Tang, L, Tang, X, and Yang, Q. The application of Tirofiban in the endovascular treatment of acute ischemic stroke: a meta-analysis. Cerebrovasc Dis. (2021) 50:121–31. doi: 10.1159/000512601
33. Rana, A, Yu, S, Reid-Herrera, S, Kamen, S, Hunter, K, Shaikh, H, et al. Eptifibatide use in ischemic stroke patients undergoing endovascular thrombectomy: a matched cohort analysis. Front Neurol. (2022) 13:939215. doi: 10.3389/fneur.2022.939215
34. Walsh, RD, Barrett, KM, Aguilar, MI, Lanzino, G, Hanel, RA, Miller, DA, et al. Intracranial hemorrhage following neuroendovascular procedures with abciximab is associated with high mortality: a multicenter series. Neurocrit Care. (2011) 15:85–95. doi: 10.1007/s12028-010-9338-1
35. Akers, WS, Oh, JJ, Oestreich, JH, Ferraris, S, Wethington, M, and Steinhubl, SR. Pharmacokinetics and pharmacodynamics of a bolus and infusion of cangrelor: a direct, parenteral P2Y12 receptor antagonist. J Clin Pharmacol. (2010) 50:27–35. doi: 10.1177/0091270009344986
36. Bhatt, DL, Stone, GW, Mahaffey, KW, Gibson, CM, Steg, PG, Hamm, CW, et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events. New England J Med. (2013) 368:1303–13. doi: 10.1056/NEJMoa1300815
37. Franchi, F, Rollini, F, Muniz-Lozano, A, Rae Cho, J, and Angiolillo, DJ. Cangrelor: a review on pharmacology and clinical trial development. Expert Review of Cardiovascular Therapy. (2013) 11:1279–91. doi: 10.1586/14779072.2013.837701
38. Oestreich, JH, and Dobesh, PP. Cangrelor for treatment during percutaneous coronary intervention. Future Cardiol. (2014) 10:201–13. doi: 10.2217/fca.13.108
39. Wallentin, L. P2Y12 inhibitors: differences in properties and mechanisms of action and potential consequences for clinical use. European heart J. (2009) 30:1964–77. doi: 10.1093/eurheartj/ehp296
40. Lhermusier, T, Baker, NC, and Waksman, R. Overview of the 2014 food and drug administration cardiovascular and renal drugs advisory committee meeting regarding cangrelor. Am J Cardiol. (2015) 115:1154–61. doi: 10.1016/j.amjcard.2015.01.551
41. Tang, Y, Zhang, YC, Chen, Y, and Xiang, Y. Efficacy and safety of cangrelor for patients with coronary artery disease: a meta-analysis of four randomized trials. Intern J Clinical and Experimental Med. (2015) 8:800.
42. Chalouhi, N, Jabbour, P, Kung, D, and Hasan, D. Safety and efficacy of tirofiban in stent-assisted coil embolization of intracranial aneurysms. Neurosurgery. (2012) 71:710–4. doi: 10.1227/NEU.0b013e31826213f9
43. Yan, Y, He, X, Fang, Y, Xu, Y, Hong, B, Liu, J, et al. The safety and efficacy of low-dosage tirofiban for stent-assisted coiling of ruptured intracranial aneurysms. Neurosurg Rev. (2021) 44:2211–8. doi: 10.1007/s10143-020-01398-w
44. Egger, M, Davey Smith, G, Schneider, M, and Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34.
Keywords: cangrelor, anti-platelet therapy, endovascular, systematic review, stroke
Citation: Desai H, Al-Salihi MM, Morsi RZ, Vayani OR, Kothari SA, Thind S, Carrión-Penagos J, Baskaran A, Tarabichi A, Bonderski VA, Siegler JE, Hahn M, Coleman ER, Brorson JR, Mendelson SJ, Mansour A, Dabus G, Hurley M, Prabhakaran S, Linfante I and Kass-Hout T (2023) Intravenous cangrelor use for neuroendovascular procedures: a two-center experience and updated systematic review. Front. Neurol. 14:1304599. doi: 10.3389/fneur.2023.1304599
Edited by:
Slaven Pikija, University Hospital Salzburg, AustriaReviewed by:
Ahmed Mohamed Elhfnawy, University Medical Center Giessen, GermanyAlexander Sirakov, University Hospital St. Ivan Rilski, Bulgaria
Copyright © 2023 Desai, Al-Salihi, Morsi, Vayani, Kothari, Thind, Carrión-Penagos, Baskaran, Tarabichi, Bonderski, Siegler, Hahn, Coleman, Brorson, Mendelson, Mansour, Dabus, Hurley, Prabhakaran, Linfante and Kass-Hout. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tareq Kass-Hout, dGthc3Nob3V0QGJzZC51Y2hpY2Fnby5lZHU=
†These authors have contributed equally to this work