 Guilherme Diogo Silva1*
Guilherme Diogo Silva1* João Paulo Mota Telles1
João Paulo Mota Telles1 Carolina de Medeiros Rimkus2
Carolina de Medeiros Rimkus2 Germana Titoneli Vieira2Emily Figueiredo Vieira Neves Yuki3
Germana Titoneli Vieira2Emily Figueiredo Vieira Neves Yuki3 Raymundo Soares de Azevedo4Gisela Tinone1Leandro Tavares Lucato2Rosa Maria Pereira3†Adriana Bastos Conforto5
Raymundo Soares de Azevedo4Gisela Tinone1Leandro Tavares Lucato2Rosa Maria Pereira3†Adriana Bastos Conforto5- 1Department of Neurology, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
- 2Department of Radiology, Instituto de Radiologia, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
- 3Department of Rheumatology, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
- 4Department of Pathology, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
- 5Laboratory of Medical Investigation (LIM) 44, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
Introduction: Cerebral small vessel disease (CSVD) is a research priority to reduce the burden of stroke and dementia. The total cerebral small vessel disease (tSVD) score provides a global view of CSVD burden combining lacunes of presumed vascular origin, cerebral microbleeds, enlarged perivascular spaces, and white matter hyperintensities of presumed vascular origin. While its use in research is expanding, a systematic review of the tSVD score’s reliability and validity had not yet been undertaken. We reviewed the inter-rater and intra-rater reliability for the tSVD score and its features. We also examined the associations between the tSVD score and age, hypertension, stroke and cognitive impairment.
Methods: We performed a systematic review of studies on Pubmed/MEDLINE, Embase, and Scopus databases from inception until June 21st, 2024. We included manuscripts that reported at least one of the following metrics for the tSVD or for its components: inter-rater reliability, intra-rater reliability, or associations with age, hypertension, stroke, and/or cognitive impairment. We provided summary Cohen’s kappa coefficients for inter and intra-rater reliability for each feature of the tSVD score. Subgroup analysis and meta-regression models were used to evaluate the impact of raters, MRI fields, age, and median tSVD score values in inter-rater reliability. We summarized studies reporting associations between the tSVD score, stroke and cognitive impairment.
Results: The summary Cohen’s kappa values for inter-rater reliability ranged from 0.79 to 0.82 for each CSVD feature (13 studies, 8,177 participants). We found a high heterogeneity between studies (I2 = 94%), which may be explained by differences in rater, age, and median tSVD score. The summary Cohen’s kappa values for intra-rater reliability ranged from 0.78 to 0.84 (four studies, 250 cases were randomized from 3,654 participants). Heterogeneity was low. Seven studies (6,022 participants) reported associations between tSVD scores and either age or hypertension. Fifteen studies (6,941 participants) reported associations between tSVD scores and either stroke or cognitive impairment.
Conclusion: The intra-rater reliability, inter-rater reliability, and construct validity of each feature of the tSVD support the use of this scale in CSVD research. However, inter-rater reliability might be influenced by rater characteristics, the median tSVD score, and participant age.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42022372599.
Introduction
Cerebral small vessel disease (CSVD), an intrinsic disorder of small perforating arterioles, causes one-fifth of ischemic strokes and contributes to 45% of dementia cases (1). The significant individual, social and economic burden of these conditions makes CSVD a research priority (2).
Classical measurements of CSVD rely on visual scales for white matter hyperintensities on neuroimaging (WMH) (3). However, CSVD affects both white and gray matter, with heterogenous ischemic and hemorrhagic brain damage (1). The Standards for Reporting Vascular Changes on Neuroimaging 2 (STRIVE-2) published in 2023 reinforced the need for summary measures of distinct CSVD features (4).
The total cerebral small vessel disease score (tSVD score) provides a comprehensive view of CSVD (5). Raters evaluate brain magnetic resonance images (T1, T2, FLAIR, diffusion-weighted and iron-susceptibility imaging) and score 0 to 4 in an ordinal visual scale based on the presence of lacunes of presumed vascular origin (LAC), enlarged perivascular spaces (EPVS), cerebral microbleeds (CMB) and WMH of presumed vascular origin (Figure 1).
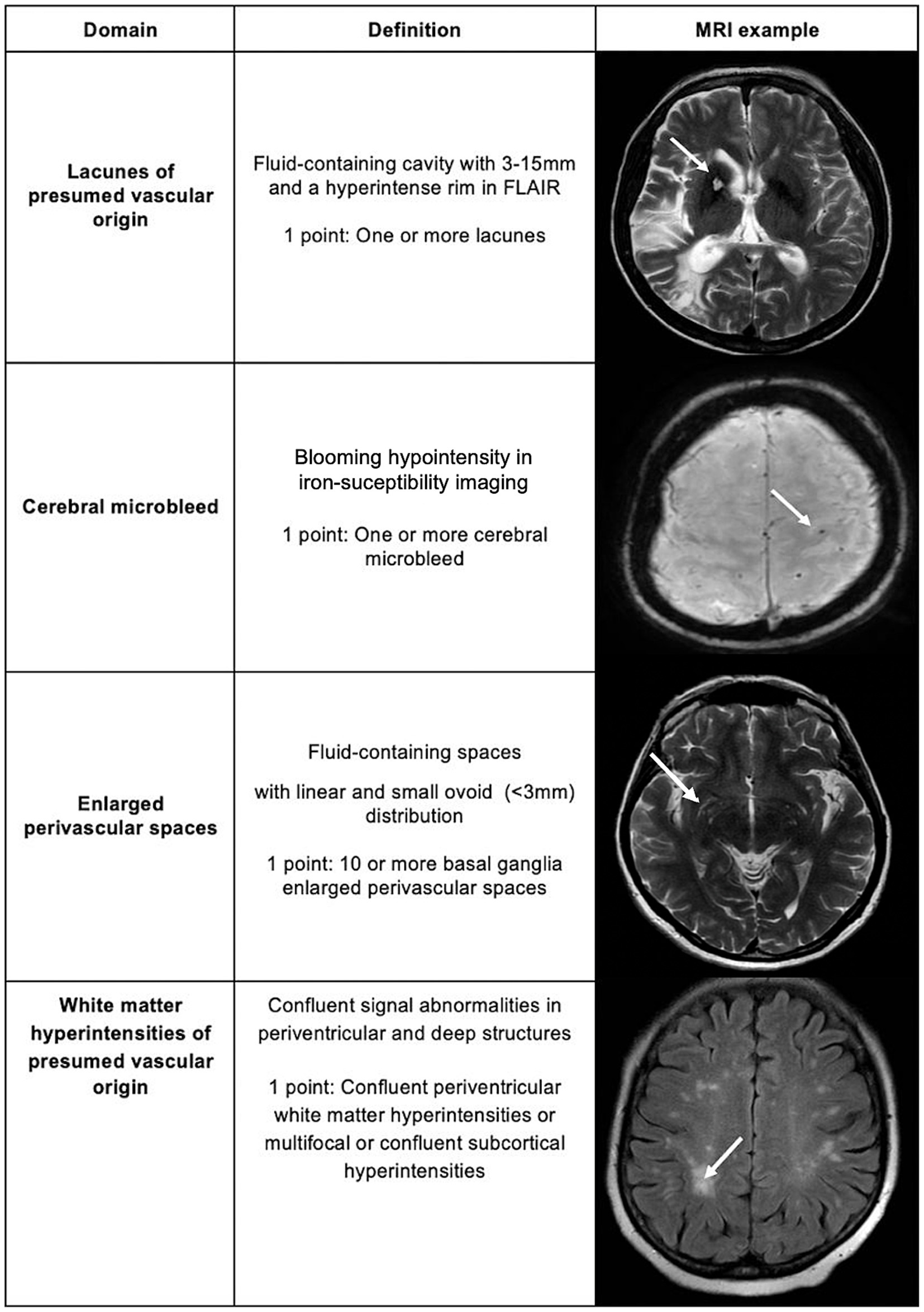
Figure 1. Total cerebral small vessel disease score.
Despite its growing use in research, significant knowledge gaps remain regarding the tSVD score as a whole, as well as the performance of its individual features. First, no systematic review has yet evaluated its reliability and validity, a recommended step to ensure scientific rigor. Second, limited data exist on how the reliability of the tSVD score and its features may vary across different populations and among raters assessing SVD. Finally, further studies are needed to explore the clinical utility of the tSVD score and its features in predicting recurrent strokes across various stroke etiologies and its potential to predict dementia in diverse populations.
We conducted a systematic review to address the following research questions: Among adults with cerebral small vessel disease (Population), what is the reliability and validity (Outcomes) of the tSVD score and each of its features (Investigation), as assessed in observational studies (Study Design)? What factors influence the reliability of the tSVD score? What gaps exist in the current research on the reliability and validity of the tSVD score?
Materials and methods
Data sources
We performed a systematic review and meta-analysis compliant with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (6). The study has been registered with the Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42022372599. The search strategy was “Total Cerebral Small Vessel Disease Score” OR “Total Small Vessel Disease Score” OR “tSVD score” OR “Total CSVD Score” in PubMed/MEDLINE, Embase and Scopus databases. Our final search was conducted on June 21, 2024, without any restrictions on publication year or language at this stage.
Study selection
Included manuscripts reported at least one of following characteristics of the tSVD score or any of its features: inter-rater reliability, intra-rater reliability, or associations with age, hypertension, stroke or cognitive impairment. We excluded papers without accessible full text and non-English language manuscripts. We also excluded studies that used modified versions of the tSVD score in which any features were added or removed.
Outcomes
Reliability, the agreement of two or more observations of the same entity (7), was evaluated by inter-rater and intra-rater agreement. Inter-rater agreement concerning the tSVD score or any of its features was measured by the comparison of scores from the same images by two independent raters. Intra-rater agreement was quantified on a single researcher’s repeat assessment of a sample of randomly selected brain scans. The effect sizes for the inter- and intra-rater reliability were measured with the Cohen’s kappa coefficient.
Validity was defined as the extent to which the results represent what they are supposed to measure (8). Validity of the tSVD score can be demonstrated by conceptual or operational strategies. It is reasonable to assume the tSVD score is valid based on a conceptual approach, given its features were derived from an expert consensus for reporting neuroimaging of CSVD (STRIVE) (1, 4). We used an operational strategy to assess construct validity, a review of the association between the tSVD score and age, hypertension, stroke and cognitive impairment. Both first-ever and recurrent strokes were considered, regardless of their causative classification. Cognitive impairment was included based on either a reported diagnosis of cognitive impairment or lower scores on screening tools such as the Montreal Cognitive Assessment (MOCA) scale. The effect size for the association between tSVD score, stroke and cognitive impairment was considered if the relative risk was higher than 2 or lower than 0.5 (9).
Two researchers independently reviewed titles and abstracts for eligibility using the Rayyan web-tool (10). In case of disagreement, consensus on which articles to screen full text was reached by discussion. Next, two researchers independently screened full-text articles for inclusion and, again, conflict was solved by consensus.
Data analysis
Two reviewers independently extracted author, date and country of publication, age, sex, risk factors, complications, rater (neuroradiologist, radiologist, neurologist, neurosurgeon, other), inter-rater, and intra-rater agreement. Extracted data were compared, with any discrepancies being resolved through discussion.
We assessed the risk of bias with the Quality Appraisal Tool for Studies of Diagnostic Reliability (QAREL) (7). Two authors independently applied the tool to each study included for assessment of inter-rater and intra-rater reliability. A low risk of bias was considered if: (1) the samples included patients with CSVD; (2) the raters were neurologists, neuroradiologists, neurosurgeons, or radiologists; (3) the raters were blinded to the findings of other raters and to clinical information; (4) the raters assessed the same neuroimaging study; and (5) the tSVD score was applied according to the original description for each feature and summary score.
Continuous variables were summarized as median and interquartile ranges, whereas qualitative variables were described in percentages and total counts. When only a range of inter or intra-rater agreement was reported, instead of a point value, we included the mean value for statistical analysis. Cohen’s kappa coefficients between 0.61 and 0.80 were considered to indicate substantial reliability, while those between 0.81 and 1.00 were considered almost perfect (11). The standard error of the kappa statistics was calculated using a nomogram and sample size (12). We provided a table with a pooled estimate of the Cohen’s kappa coefficient for each feature of the tSVD score using a random effects model meta-analysis in R Studio 2022.07.2 with package meta.
The presence and extent of statistical heterogeneity in the pooled estimate of the Cohen’s kappa coefficient was calculated using I2. Subgroup analysis was performed to investigate the role of the type of rater (neuroradiologist versus other raters) and MRI field strength (3 Tesla versus 1.5 Tesla) as a potential source of heterogeneity. We conducted a meta-regression analysis to assess median age, sex (percentage of males), and the median tSVD score as potential contributors to heterogeneity.
We assessed the presence of publication bias using a funnel plot for intra-rater and inter-rater reliability. A sensitivity analysis was performed excluding the studies responsible for funnel plot asymmetry.
The certainty in the body of evidence for intra-rater and inter-rater reliabilities of tSVD score was assessed by the Grading of Recommendations, Assessment, Development, and Evaluations approach (9) (Summary of Findings table). Large observational studies were initially regarded as high-quality evidence for reliability studies. The quality of evidence was downgraded in the presence of: (1) risk of bias, measured by the QAREL risk of bias tool (7); (2) indirectness, considered if studies were conducted only in a particular setting (e.g., only primary care); (3) imprecision, defined by wide confidence intervals; (4) inconsistency, evaluated by high unexplained heterogeneity (I2 > 50%); and (5) publication bias, based on funnel plot analysis.
Results
Figure 2 represents the flow diagram according to the PRISMA 2020 guidelines (6). We included 33 studies with 17,340 participants.
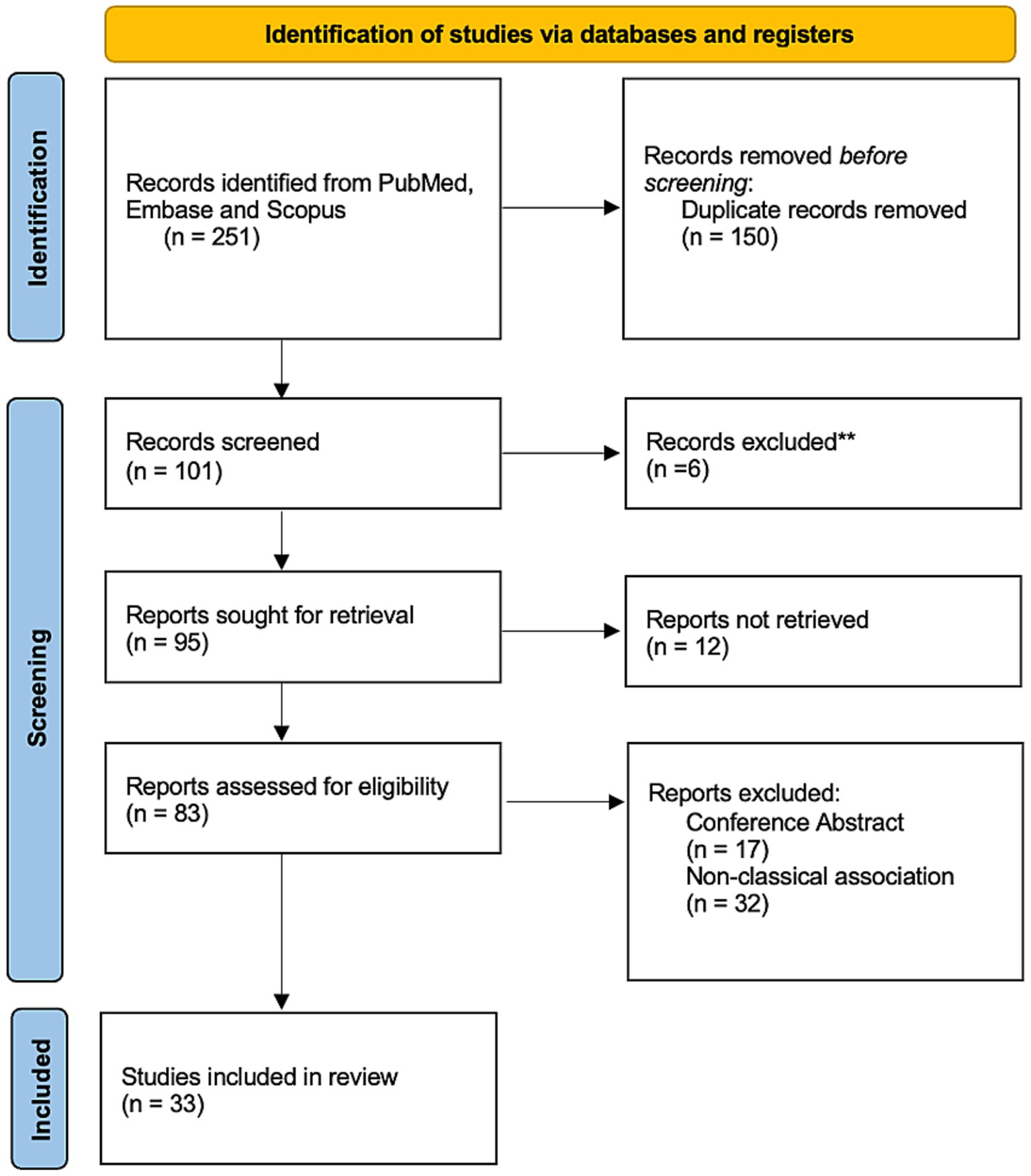
Figure 2. Flow diagram.
Inter-rater reliability
Inter-rater agreement was evaluated in 13 studies for a total of 8,177 participants (Supplementary Table S1) (13–25). All studies had low risk of bias based on the QAREL tool. Inter-rater reliability was reported for individual SVD markers but not for the total tSVD score across all studies. Pooled point estimates of Cohen’s kappa for LAC, WMH, EPVS, and CMB were classified as substantial or almost perfect (Figure 3). The most common cause of CSVD was sporadic CSVD in all included studies.
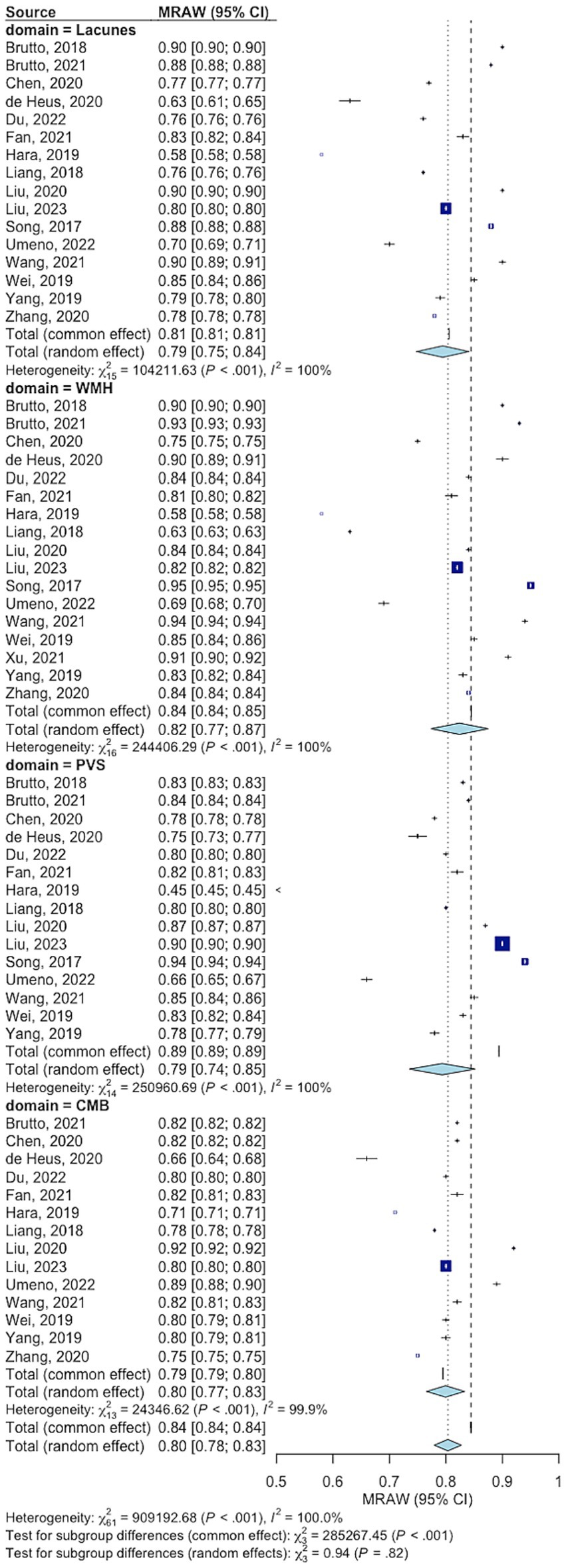
Figure 3. Summary Cohen’s kappa for inter-rater reliability of the total cerebral small vessel disease score by feature. WMH: White matter hyperintensity. CMB: Cortical microbleeds. EPVS, Enlarged perivascular spaces.
We found evidence of high heterogeneity between studies of inter-rater agreement, for each tSVD feature. We downgraded the quality of evidence based on inconsistency. A subgroup analysis of studies reporting the assessment of tSVD by neuroradiologists had a significantly lower heterogeneity (Supplementary Figure S1). The heterogeneity was high and comparable between studies using 1.5 and 3 Tesla MRI (Supplementary Figure S2). The meta-regression showed that older age and higher median tSVD score were linked to higher inter-rater agreement for cerebral microbleeds but did not affect agreements for the other features (Supplementary Table S2). Funnel plot showed a significant asymmetry (Supplementary Figure S3), a concern for publication bias. However, the Cohen’s kappa values for inter-rater agreement continued to be substantial or almost perfect after excluding studies responsible for funnel plot asymmetry in the sensitivity analysis (Supplementary Figure S4).
Intra-rater reliability
Intra-rater agreement was assessed in four studies using 250 random cases for test and re-test methodology for a total of 3,654 participants (Supplementary Table S3) (17, 23, 26, 27). The risk of bias for intra-rater reliability studies was low. Intra-rater reliability was reported for individual SVD markers but not for the total tSVD score across all studies. The Cohen’s kappa coefficient indicated substantial reliability for WMH (0.78, 95% CI 0.70; 0.86), and almost perfect reliabilities for the other features (Figure 4).
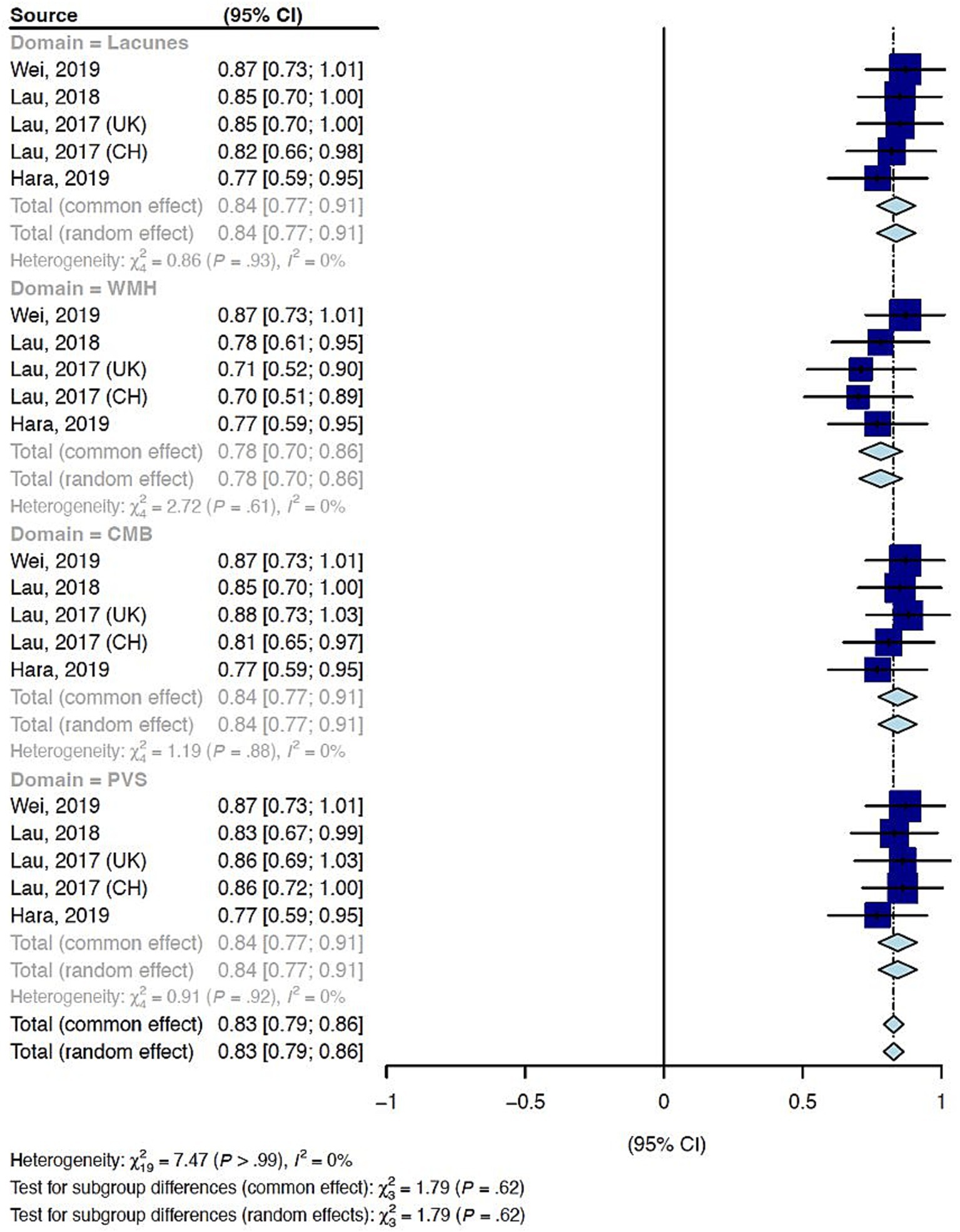
Figure 4. Summary Cohen’s kappa for intra-rater reliability of the total cerebral small vessel disease score by feature. WMH: White matter hyperintensity. CMB: Cortical microbleeds. EPVS, perivascular spaces.
Statistical heterogeneity measured by I2 was zero and funnel plots were symmetrical for all features of the tSVD score (Supplementary Figure S5). The most common cause of CSVD was sporadic CSVD in all included studies. Table 1 summarizes the summary measures and the certainty of evidence for inter-rater and intra-rater reliability of the tSVD score.
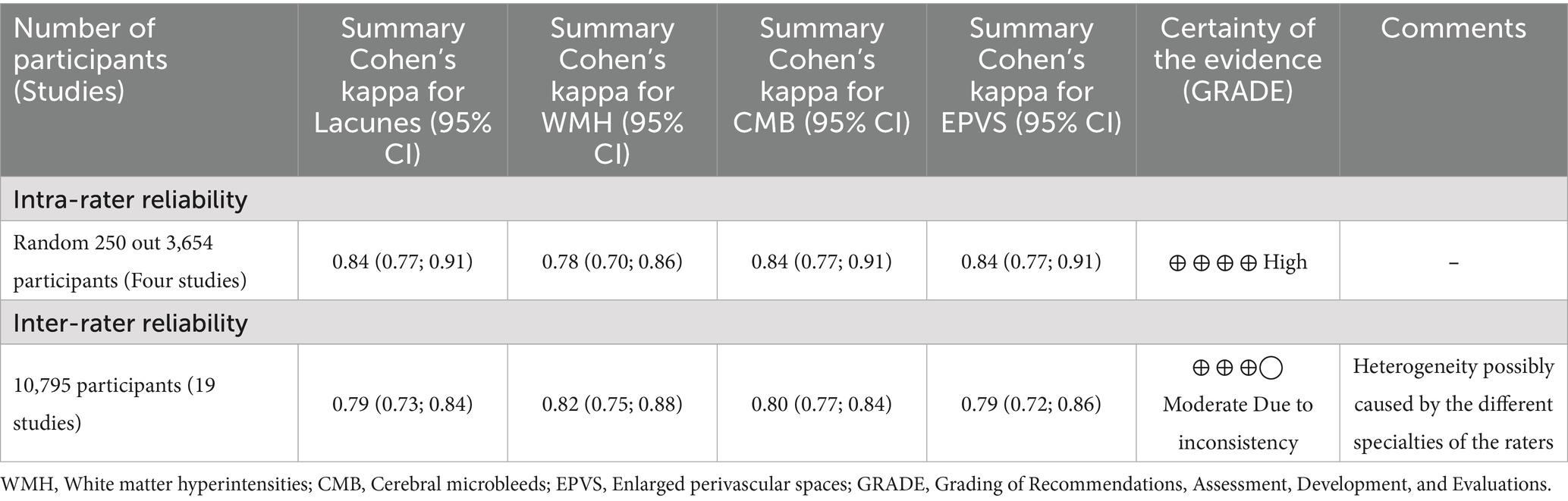
Table 1. Summary of reliability findings for each feature of the total cerebral small vessel disease score.
Construct validity
The evaluation of the association between the tSVD score with age and hypertension was performed in seven studies involving a total of 6,022 participants (Supplementary Table S4) (14, 17, 19, 28–32). The associations between the tSVD score with stroke or cognitive impairment were reported in 15 studies involving a total of 7,996 participants (Supplementary Table S5) (15, 21, 22, 27, 29, 30, 33–42). A large effect size was observed in the association of tSVD score and hypertension, cardio-cerebrovascular events, and lacunar stroke (Supplementary Tables S4, S5).
Discussion
The features of the tSVD score are reliable tool in the CSVD assessment. Cohen’s kappa’s values for inter and intra-rater agreements were substantial or almost perfect for WMH, LAC, CMB, and EPVS. The type of rater, age, and median score moderated the inter-rater reliability of the tSVD score. Age, hypertension, stroke, and cognitive impairment were linked to higher tSVD scores.
The use of highly reliable scores decreases the risk of type 2 errors (43). We classified the estimate Cohen’s kappa values as substantial or almost perfect for all of the features of the tSVD score. However, the reliability of a score depends on its raters. Notably, the raters in the studies reviewed were trained neuroradiologists, neurologists, neurosurgeons or radiologists. The statistical heterogeneity was lower in studies where tSVD scores were assessed exclusively by neuroradiologists. This finding highlights the influence of raters on tSVD reproducibility and underscores the potential need for standardized training on its application. All tSVD features were highly reliable, but the absence of studies reporting the intra- and inter-rater reliability of the total SVD score and the lack of individual-patient data limited the calculation of a summary reliability measure for the total SVD score. Future studies assessing the reliability of the tSVD score should report not only the reliability of each individual features but also the reliability of the overall tSVD score.
Our review primarily included studies from Asia, the United States, and Europe, with only a few from Latin America and none from Africa. It is crucial to validate the tSVD score across diverse populations, as ethnic differences in CSVD burden have been observed. Compared to Caucasians, Asians may have a higher prevalence of WMH (44), while MRIs from African American and Latin American subjects (45, 46) show a greater burden of CMB. Older age was associated with higher inter-rater reliability of the CMB in this study, but not the inter-rater reliability of other features of the tSVD score. Future research should further investigate how demographic characteristics influence the reliability of the tSVD score.
Non-arteriolosclerosis causes of CSVD are under-represented in the field, limiting the generalizability of the data for all causes of CSVD (47, 48). Other features may be important for non-arteriosclerosis causes of CSVD. Superficial siderosis, for instance, is relevant to evaluate the burden of cerebral amyloid angiopathy but is not included in the tSVD score (49). The tSVD score does not consider differences in the distribution of CSVD lesions among causes of CSVD. For example, in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), WMH affect the extreme capsule and anterior temporal poles, uncommon in other causes of CSVD (50). All studies in the inter-rater and intra-rater analyses focused on populations with arteriolosclerosis as the primary cause of CSVD, restricting reliability and validity assessment to sporadic SVD.
The reliabilities of all tSVD features were substantial or almost perfect, while reliabilities of the periventricular and deep Fazekas scale were substantial (51). The tSVD score addresses the limitations of current methods for assessing CSVD burden on brain MRI. While the Fazekas scale addresses only WMH (51), the tSVD score integrates multiple CSVD markers – LAC, CMB, and EPVS.
The tSVD score provides a simple and practical measure of CSVD burden on brain MRI, in contrast with automatic segmentation tools that may offer greater precision but necessitates additional imaging acquisitions and processing (52). These requirements limit the widespread use of these techniques, particularly in retrospective studies that use routine clinical MRI data.
The tSVD score exhibits an evolving nature, leading to adaptations such as a simplified version that excludes EPVS, which are associated with dementia (53). Another adaptation incorporates centrum semiovale EPVS and cortical superficial siderosis, both of which correlate with pathological evidence of amyloid angiopathy (49). Other modifications include raising the EPVS threshold and refining the scoring for microbleeds and WMH burden based on their count and severity (54). This study focused on the original tSVD score, and future research should examine how its ongoing adaptations may affect the tool’s reliability and validity.
This meta-analysis relied solely on aggregated data; therefore, individual patient data were not available to assess other neuroimaging patterns of CSVD. Future studies in the field of CSVD should evaluate the tSVD score in subjects with non-atherosclerotic causes of CSVD, as well as its responsiveness to change over time.
The present study was limited to the two most used properties of a neuroimaging score: validity and reliability. Another relevant characteristic - responsiveness to change (55) - was not evaluated. Responsiveness to change is a concern for the tSVD score because LAC and CMB are scored according to their presence rather than their number. Hence, the tSVD score may carry a potential risk of a ceiling effect, as an increase in the number of LAC or CMB might not lead to a corresponding increase in the score. Moreover, the results of this systematic review suggest that higher median tSVD scores may be linked to higher inter-rater agreement for CMB. The tSVD score might be limited in at the extremes of the CSVD burden.
No longitudinal studies evaluating successive tSVD scores over time and its association with clinical symptoms were identified. Future longitudinal studies, particularly those leveraging big data and open science, should assess changes in the tSVD score over time and evaluate the impact of its increase on stroke and dementia risk. Additionally, adaptations of the tSVD score could include adjustments for the total number of lacunes and microbleeds, rather than just their presence, as a strategy to mitigate the risk of a ceiling effect.
Conclusion
The tSVD score features are reliable and valid measures of CSVD, supporting its application in research. However, the inter-rater reliability of these features may be influenced by factors such as rater type, median tSVD score, and participant age. Future research should address several knowledge gaps, including the overall reliability of the tSVD score rather than just its individual features; the reliability and potential need for additional features in cases of CSVD unrelated to age and hypertension; and the optimal approach for longitudinal application of the tSVD score, particularly in light of potential ceiling effects.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
GS: Visualization, Project administration, Writing – original draft, Data curation, Methodology, Formal analysis, Software, Conceptualization. JT: Writing – original draft, Data curation, Methodology. CR: Methodology, Writing – review & editing. GV: Methodology, Writing – review & editing. EY: Methodology, Writing – review & editing. RA: Methodology, Writing – review & editing. GT: Writing – review & editing, Methodology. LL: Methodology, Writing – review & editing, Investigation. RP: Writing – review & editing, Conceptualization, Writing – original draft. AC: Validation, Supervision, Writing – review & editing, Project administration, Methodology, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
In Memoriam
RP passed away during the development of this work. She made significant contributions to the conceptualization and methodology of the study. In recognition of her contributions, she is included as an author posthumously.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. We authors verify we used ChatGPT to improve readability and detect grammatical errors in the manuscript. We authors take full responsibility for the use of generative AI in the preparation of the manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1593402/full#supplementary-material
References
1. Wardlaw, JM, Smith, EE, Biessels, GJ, Cordonnier, C, Fazekas, F, Frayne, R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. (2013) 12:822–38. doi: 10.1016/S1474-4422(13)70124-8
2. Gurol, ME, Biessels, GJ, and Polimeni, JR. Advanced neuroimaging to unravel mechanisms of cerebral small vessel diseases. Stroke. (2020) 51:29–37. doi: 10.1161/STROKEAHA.119.024149
3. van der Flier, WM, van Straaten, ECW, Barkhof, F, Verdelho, A, Madureira, S, Pantoni, L, et al. Small vessel disease and general cognitive function in nondisabled elderly: the LADIS study. Stroke. (2005) 36:2116–20. doi: 10.1161/01.STR.0000179092.59909.42
4. Duering, M, Biessels, GJ, Brodtmann, A, Chen, C, Cordonnier, C, de Leeuw, F-E, et al. Neuroimaging standards for research into small vessel disease-advances since 2013. Lancet Neurol. (2023) 22:602–18. doi: 10.1016/S1474-4422(23)00131-X
5. Klarenbeek, P, van Oostenbrugge, RJ, Rouhl, RPW, Knottnerus, ILH, and Staals, J. Ambulatory blood pressure in patients with lacunar stroke: association with total MRI burden of cerebral small vessel disease. Stroke. (2013) 44:2995–9. doi: 10.1161/STROKEAHA.113.002545
6. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. (2021) 134:178–89. doi: 10.1016/j.jclinepi.2021.03.001
7. Lucas, NP, Macaskill, P, Irwig, L, and Bogduk, N. The development of a quality appraisal tool for studies of diagnostic reliability (QAREL). J Clin Epidemiol. (2010) 63:854–61. doi: 10.1016/j.jclinepi.2009.10.002
8. Kottner, J, Audige, L, Brorson, S, Donner, A, Gajewski, BJ, Hróbjartsson, A, et al. Guidelines for reporting reliability and agreement studies (GRRAS) were proposed. Int J Nurs Stud. (2011) 48:661–71. doi: 10.1016/j.ijnurstu.2011.01.016
9. Balshem, H, Helfand, M, Schünemann, HJ, Oxman, AD, Kunz, R, Brozek, J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
10. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
11. Chmura Kraemer, H, Periyakoil, VS, and Noda, A. Kappa coefficients in medical research. Stat Med. (2002) 21:2109–29. doi: 10.1002/sim.1180
12. Hanley, JA. Standard error of the kappa statistic. Psychol Bull. (1987) 102:315–21. doi: 10.1037//0033-2909.102.2.315
13. Del Brutto, VJ, Mera, R, Recalde, BY, Rumbea, DA, Costa, AF, and Del Brutto, OH. Total cerebral small vessel disease score and all-cause mortality in older adults of Amerindian ancestry: the Atahualpa project. Eur Stroke J. (2021) 6:412–9. doi: 10.1177/23969873211060803
14. de Heus, RAA, Reumers, SFI, van der Have, A, Tumelaire, M, Tully, PJ, and Claassen, JAHR. Day-to-day home blood pressure variability is associated with cerebral small vessel disease burden in a memory clinic population. J Alzheimers Dis. (2020) 74:463–72. doi: 10.3233/JAD-191134
15. Fan, Y, Xu, Y, Shen, M, Guo, H, and Zhang, Z. Total cerebral small vessel disease burden on MRI correlates with cognitive impairment in outpatients with amnestic disorders. Front Neurol. (2021) 12:747115. doi: 10.3389/fneur.2021.747115
16. Du, H, Wu, S, Lei, H, Ambler, G, Werring, DJ, Li, H, et al. Total cerebral small vessel disease score and cerebral bleeding risk in patients with acute stroke treated with intravenous thrombolysis. Front Aging Neurosci. (2022) 14:790262. doi: 10.3389/fnagi.2022.790262
17. Hara, M, Yakushiji, Y, Suzuyama, K, Nishihara, M, Eriguchi, M, Noguchi, T, et al. Synergistic effect of hypertension and smoking on the total small vessel disease score in healthy individuals: the Kashima scan study. Hypertens Res. (2019) 42:1738–44. doi: 10.1038/s41440-019-0282-y
18. Liang, Y, Chen, Y-K, Mok, VC-T, Wang, D-F, Ungvari, GS, Chu, WC-W, et al. Cerebral small vessel disease burden is associated with poststroke depressive symptoms: a 15-month prospective study. Front Aging Neurosci. (2018) 10:46. doi: 10.3389/fnagi.2018.00046
19. Liu, D, Cai, X, Yang, Y, Wang, S, Yao, D, Mei, L, et al. Associations of life’s simple 7 with cerebral small vessel disease. Stroke. (2022) 53:2859–67. doi: 10.1161/STROKEAHA.122.038838
20. Song, TJ, Kim, J, Song, D, Yoo, J, Lee, HS, Kim, YJ, et al. Total cerebral small-vessel disease score is associated with mortality during follow-up after acute ischemic stroke. J Clin Neurol. (2017) 13:187–95. doi: 10.3988/jcn.2017.13.2.187
21. Umeno, T, Yamashita, A, Mizota, T, Uramatsu, T, and Matsuo, T. Predictive value of total small-vessel disease score for recurrent stroke in patients undergoing maintenance hemodialysis. J Stroke Cerebrovasc Dis. (2022) 31:106400. doi: 10.1016/j.jstrokecerebrovasdis.2022.106400
22. Wang, T, Jin, A, Fu, Y, Zhang, Z, Li, S, Wang, D, et al. Heterogeneity of white matter Hyperintensities in cognitively impaired patients with cerebral small vessel disease. Front Immunol. (2021) 12:803504. doi: 10.3389/fimmu.2021.803504
23. Wei, C, Liu, J, Li, J, and Liu, M. A non-linear association between Total small vessel disease score and hemorrhagic transformation after ischemic stroke with atrial fibrillation and/or rheumatic heart disease. Front Neurol. (2019) 10:769. doi: 10.3389/fneur.2019.00769
24. Yang, X, Zhang, S, Dong, Z, Zi, Y, Luo, Y, Jin, Z, et al. Insulin resistance is a risk factor for overall cerebral small vessel disease burden in old nondiabetic healthy adult population. Front Aging Neurosci. (2019) 11:127. doi: 10.3389/fnagi.2019.00127
25. Zhang, K, Jiang, Y, Wang, Y, Suo, C, Xu, K, Zhu, Z, et al. Associations of arterial stiffness and carotid atherosclerosis with cerebral small vessel disease in a rural community-based population. J Atheroscler Thromb. (2020) 27:922–33. doi: 10.5551/jat.52530
26. Lau, KK, Pego, P, Mazzucco, S, Li, L, Howard, DP, Küker, W, et al. Age and sex-specific associations of carotid pulsatility with small vessel disease burden in transient ischemic attack and ischemic stroke. Int J Stroke. (2018) 13:832–9. doi: 10.1177/1747493018784448
27. Lau, KK, Li, L, Schulz, U, Simoni, M, Chan, KH, Ho, SL, et al. Total small vessel disease score and risk of recurrent stroke: validation in 2 large cohorts. Neurology. (2017) 88:2260–7. doi: 10.1212/WNL.0000000000004042
28. Dobrynina, LA, Shamtieva, KV, Kremneva, EI, Zabitova, MR, Akhmetzyanov, BM, Gnedovskaya, EV, et al. Daily blood pressure profile and blood–brain barrier permeability in patients with cerebral small vessel disease. Sci Rep. (2022) 12:1–10. doi: 10.1038/s41598-022-11172-1
29. Goldstein, ED, Badi, MK, Hasan, TF, Lesser, ER, Hodge, DO, Lin, MP, et al. Cerebral small vessel disease burden and all-cause mortality: Mayo Clinic Florida familial cerebrovascular diseases registry. J Stroke Cerebrovasc Dis. (2019) 28:104285. doi: 10.1016/j.jstrokecerebrovasdis.2019.07.001
30. Staals, J, Makin, SDJ, Doubal, FN, Dennis, MS, and Wardlaw, JM. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology. (2014) 83:1228–34. doi: 10.1212/WNL.0000000000000837
31. Wiseman, SJ, Bastin, ME, Jardine, CL, Barclay, G, Hamilton, IF, Sandeman, E, et al. Cerebral small vessel disease burden is increased in systemic lupus erythematosus. Stroke. (2016) 47:2722–8. doi: 10.1161/STROKEAHA.116.014330
32. Yakushiji, Y, Charidimou, A, Noguchi, T, Nishihara, M, Eriguchi, M, Nanri, Y, et al. Total small vessel disease score in neurologically healthy Japanese adults in the Kashima scan study. Intern Med. (2018) 57:189–96. doi: 10.2169/internalmedicine.8393-16
33. Del Brutto, OH, Mera, RM, Del Brutto, VJ, Costa, AF, Zambrano, M, and Brorson, J. Basilar artery Dolichoectasia: prevalence and correlates with markers of cerebral small vessel disease in community-dwelling older adults. J Stroke Cerebrovasc Dis. (2017) 26:2909–14. doi: 10.1016/j.jstrokecerebrovasdis.2017.07.014
34. Guo, X, Zhu, Y, Li, X, Lu, Z, Cao, Z, Yi, X, et al. Increased insulin resistance is associated with vascular cognitive impairment in Chinese patients with cerebral small vessel disease. Psychogeriatrics. (2021) 21:342–9. doi: 10.1111/psyg.12675
35. Han, F, Zhang, D-D, Zhai, F-F, Xue, J, Zhang, J-T, Yan, S, et al. Association between large artery stenosis, cerebral small vessel disease and risk of ischemic stroke. Sci China Life Sci. (2021) 64:1473–80. doi: 10.1007/s11427-020-1849-x
36. Liu, C, Roth, DL, Gottesman, RF, Sheehan, OC, Blinka, MD, Howard, VJ, et al. Change in life’s simple 7 measure of cardiovascular health after incident stroke. Stroke. (2021) 52:878–86. doi: 10.1161/STROKEAHA.120.030836
37. Pasi, M, Sugita, L, Xiong, L, Charidimou, A, Boulouis, G, Pongpitakmetha, T, et al. Association of Cerebral Small Vessel Disease and Cognitive Decline after Intracerebral Hemorrhage. Neurology. (2021) 96:e182–92. doi: 10.1212/WNL.0000000000011050
38. Shen, Y, Dong, Z, Zhong, J, Pan, P, Xu, G, Zhang, Z, et al. Effect of cerebral small vessel disease on cognitive impairment in Parkinson’s disease. Acta Neurol Belg. (2022) 123:487–95. doi: 10.1007/s13760-022-02078-w
39. Suzuyama, K, Yakushiji, Y, Ogata, A, Nishihara, M, Eriguchi, M, Kawaguchi, A, et al. Total small vessel disease score and cerebro-cardiovascular events in healthy adults: the Kashima scan study. Int J Stroke. (2020) 15:973–9. doi: 10.1177/1747493020908144
40. Xiang, L, Zhang, T, Zhang, B, Zhang, C, Hou, S, and Yue, W. The associations of increased cerebral small vessel disease with cognitive impairment in neurosyphilis presenting with ischemic stroke. Brain Behav. (2021) 11:e02187. doi: 10.1002/brb3.2187
41. Xie, H, Zhang, N, Xia, C, Ding, Y, Zhao, H, and Huang, Y. The clinical characteristics of cerebral small vessel disease patients with motoric cognitive risk syndrome during single- and dual-task walking. Heliyon. (2024) 10:e30007. doi: 10.1016/j.heliyon.2024.e30007
42. Xu, Z, Li, F, Xing, D, Song, H, Chen, J, Duan, Y, et al. A novel imaging biomarker for cerebral small vessel disease associated with cognitive impairment: the deep-medullary-veins score. Front Aging Neurosci. (2021) 13:720481. doi: 10.3389/fnagi.2021.720481
44. Mok, V, Srikanth, V, Xiong, Y, Phan, TG, Moran, C, Chu, S, et al. Race-ethnicity and cerebral small vessel disease--comparison between Chinese and white populations. Int J Stroke. (2014) 9 Suppl A100:36–42. doi: 10.1111/ijs.12270
45. Shahjouei, S, Tsivgoulis, G, Singh, M, McCormack, M, Noorbakhsh-Sabet, N, Goyal, N, et al. Racial difference in cerebral microbleed burden among ischemic stroke patients. J Stroke Cerebrovasc Dis. (2017) 26:2680–5. doi: 10.1016/j.jstrokecerebrovasdis.2017.06.040
46. Castello, JP, Pasi, M, Abramson, JR, Rodriguez-Torres, A, Marini, S, Demel, S, et al. Contribution of racial and ethnic differences in cerebral small vessel disease subtype and burden to risk of cerebral hemorrhage recurrence. Neurology. (2021) 96:e2469–80. doi: 10.1212/WNL.0000000000011932
47. Pantoni, L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. (2010) 9:689–701. doi: 10.1016/S1474-4422(10)70104-6
48. Silva, GD, Vieira, GT, Rimkus, C d M, Neves Yuki, EF, Azevedo, RS, Tinone, G, et al. Distinctive cerebral small vessel disease patterns are associated with ischemic stroke in systemic lupus erythematosus. Lupus. (2025) 34:348–57. doi: 10.1177/09612033251322930
49. Charidimou, A, Martinez-Ramirez, S, Reijmer, YD, Oliveira-Filho, J, Lauer, A, Roongpiboonsopit, D, et al. Total magnetic resonance imaging burden of small vessel disease in cerebral amyloid Angiopathy: an imaging-pathologic study of concept validation. JAMA Neurol. (2016) 73:994–1001. doi: 10.1001/jamaneurol.2016.0832
50. Bersano, A, Bedini, G, Markus, HS, Vitali, P, Colli-Tibaldi, E, Taroni, F, et al. The role of clinical and neuroimaging features in the diagnosis of CADASIL. J Neurol. (2018) 265:2934–43. doi: 10.1007/s00415-018-9072-8
51. Kapeller, P, Barber, R, Vermeulen, RJ, Adèr, H, Scheltens, P, Freidl, W, et al. Visual rating of age-related white matter changes on magnetic resonance imaging. Stroke. (2003) 34:441–5. doi: 10.1161/01.STR.0000049766.26453.E9
52. Xu, B, Zhang, X, Tian, C, Yan, W, Wang, Y, Zhang, D, et al. Automatic segmentation of white matter hyperintensities and correlation analysis for cerebral small vessel disease. Front Neurol. (2023) 14:1242685. doi: 10.3389/fneur.2023.1242685
53. Amin Al Olama, A, Wason, JMS, Tuladhar, AM, van Leijsen, EMC, Koini, M, Hofer, E, et al. Simple MRI score aids prediction of dementia in cerebral small vessel disease. Neurology. (2020) 94:e1294–302. doi: 10.1212/WNL.0000000000009141
54. Zhi, N, Zhang, L, Wang, Y, Bai, S, Geng, J, Yu, L, et al. Modified cerebral small vessel disease score is associated with vascular cognitive impairment after lacunar stroke. Aging (Albany NY). (2021) 13:9510–21. doi: 10.18632/aging.202438
Keywords: cerebral small vessel disease, score, reliability, validity, systematic review, meta-analysis, white matter hyper intensities, cerebral microbleed
Citation: Silva GD, Telles JPM, Rimkus CdM, Vieira GT, Yuki EFVN, Azevedo RS, Tinone G, Lucato LT, Pereira RM and Conforto AB (2025) Reliability and validity of the total cerebral small vessel disease score: a systematic review and meta-analysis. Front. Neurol. 16:1593402. doi: 10.3389/fneur.2025.1593402
Edited by:
Rafael Rehwald, University College London, United KingdomReviewed by:
Maria Del Carmen Valdés Hernández, University of Edinburgh, United KingdomLuis Rafael Moscote-Salazar, Colombian Clinical Research Group in Neurocritical Care, Colombia
Copyright © 2025 Silva, Telles, Rimkus, Vieira, Yuki, Azevedo, Tinone, Lucato, Pereira and Conforto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guilherme Diogo Silva, Z3VpbGhlcm1lLmRpb2dvQGhjLmZtLnVzcC5icg==
†Deceased