 Leona Möller1*
Leona Möller1* Urs Fisch2,3
Urs Fisch2,3 Lena Habermehl1,4
Lena Habermehl1,4 Clara Jünemann1 on behalf of the IGNITE Group and the MuSE Group
Clara Jünemann1 on behalf of the IGNITE Group and the MuSE Group- 1Philipps University Marburg, Department of Neurology, Epilepsy Center Hessen, Marburg, Germany
- 2Department of Neurology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, United States
- 3Department of Neurology, University Hospital Basel, Basel, Switzerland
- 4Epilepsy Center, Neurological Institute, University Hospitals Cleveland Medical Center, Cleveland, OH, United States
Background: Status epilepticus (SE) is a life-threatening neurological emergency, and exhibits significant variability in clinical management despite established guidelines. This study evaluates current practices across German speaking countries.
Methods: A web-based survey (December 2023–May 2024) assessed SE treatment strategies among 83 neurologists and neurointensivists from Germany, Austria, and Switzerland. Cases were presented to analyze diagnostic and therapeutic preferences.
Results: The preferred benzodiazepine for first line treatment was lorazepam, chosen by 71.6% of the respondents. In the case of established SE, 35.4% chose levetiracetam as the preferred ASM. Propofol in combination with sufentanil/fentanyl was the preferred anesthetic of choice in 65.4% of respondents. For super-refractory status epilepticus (SRSE), 41.5% prefer to add further ASM, with valproic acid (67.1%), and lacosamide (64.5%) being the most frequently selected. Only 31.8% reported that their emergency services have a standard operating procedure (SOP) for SE treatment, and the choice of the preferred benzodiazepine varied in the preclinical setting, with midazolam being the most commonly used. 1) First-line therapy: Lorazepam (71.6% in-hospital), midazolam (50% prehospital), 2) Second-line therapy: Levetiracetam (35.4%) and lacosamide (13.4%) were the most common choices, 3) Refractory SE: Propofol with opioids (65.4%) were preferred for anesthesia, 4) Prehospital care: 31.8% of emergency services lacked standardized protocols; midazolam dosing varied widely (2–10 mg).
Diagnostics: Laboratory testing was universal (96.9%), but MR-imaging (10%) and clinical use of prognostic scores (6.2%) were underutilized.
Conclusion: This survey highlights the variability in clinical practice for managing status epilepticus in German-speaking countries. Persistent heterogeneity in SE management underscores the need for standardized protocols, particularly in prehospital care and refractory SE therapy.
Introduction
With an incidence of 10–40 per 100,000 person-years and a 7%–33% mortality, status epilepticus (SE) is one of the most common life-threatening emergencies in neurology and is associated with significant mortality and morbidity (1, 2, 36).
Recommended by international guidelines, the management of SE follows a stepwise approach, starting with the administration of benzodiazepines, as first-line therapy. If SE persists, second-line treatment including anti-seizure medication (ASM) such as levetiracetam, valproate, and lacosamide, should be given within the first 30 min. In cases of refractory or super-refractory SE (SRSE), where seizures continue despite multiple treatments, deeper sedation with anesthetic agents like propofol and even more advanced interventions may be necessary (3–5). SRSE occurs in about 12% of all cases of SE (6). Kantanen et al. (7) identified 75 patients treated in the ICU and under anesthesia, corresponding to an annual incidence of 3.0. Of these, 21% were classified as SRSE, with the annual incidence being 0.6/100,000.
While guidelines advocate benzodiazepines followed by i.v.-ASM and anesthetics, real-world adherence to these guidelines remains inconsistent (8, 9).
Furthermore, new-onset refractory status epilepticus (NORSE), a SE characterised by the occurrence of a refractory SE in a patient without a prior history of epilepsy and without any obvious underlying etiology, poses a particular challenge for intensive care therapy (10). With a mortality rate of 12% and a high risk of survivors developing therapy-resistant epilepsy, the prognosis remains poor despite modern intensive care treatments. The survey also inquired about the usual diagnosis and treatment of NORSE.
To better understand different approaches to SE management in the German-speaking countries (Germany, Austria, Switzerland, DACH), a web-based survey on the treatment of SE was performed among clinicians focusing particularly on ASM choices and dosage and diagnostic procedures. The findings of this survey provide valuable insights into the current state of SE care, offering an opportunity to compare clinical practices and identifying potential areas for improvement in clinical guidelines and research.
Methods
An anonymous web-based survey was conducted from December 2023 until May 2024 among neurologists in Germany, Austria and Switzerland (https://surveymonkey.de, SurveyMonkey Europe UC). The questionnaire consisted of two parts. The first part presented two case-based scenarios addressing escalating SE management from preclinical emergency care of early SE, to established SE, to SRSE. The second part included specific questions on SE management in the prehospital setting and diagnostic procedures. The survey was completed with voluntary demographic information provided by the respondents.
This case-based scenarios and structured questions on SE management was distributed via IGNITE and MuSE networks. The complete questionnaire is available in the Supplementary material. The survey was distributed via the IGNITE (Initiative for German NeuroIntensive Trial Engagement, a section of the German Society for Neurointensive and Emergency Care) and MuSE (Multicentric Studies in Epilepsy, part of the German, Austrian and Swiss epilepsy societies) networks. This is a network of young neurointensive care physicians and epileptologists who are always open to new members, so no specific number of members can be given. In addition, members had the opportunity to pass the survey on to colleagues.
The survey was distributed via email to participants of the different networks, followed by a reminder notification after 2 months.
Descriptive statistical analyses were performed using the SurveyMonkey and jamovi (v2.3.28) software.
Results
A total of 83 clinicians (77.1% attendings/senior physicians, 68.8% university-affiliated, 52.5% EEG-certified, 32.8% board-certified intensivists, 18% board-certified in emergency medicine, 31.2% were epileptologists) completed the survey. A substantial proportion of respondents (68.8%) were affiliated with university hospitals, additional 28.1% reported working in specialized epilepsy centers, while only five participants indicated employment in the outpatient sector. This reflects the target audience of the networks contacted. Furthermore, the questionnaire was completed primarily by specialists and senior physicians (25% specialists, 57.8% senior physicians), which is consistent with the distribution within the networks. The first digit of the postcode was also requested in order to avoid individual areas being overrepresented. Fortunately, there were no significant differences here; all areas were covered. Subgroup analysis did not reveal major systematic differences between countries, although minor numerical trends were observed.
Part 1: therapy escalation management based on a clinical scenario
Case 1
A case describing SE in an early stage was presented first: “A 36-year-old patient (80 kg) is presented to the emergency department. He was given 5 mg diazepam preclinically for generalized convulsive status epilepticus (SE), which did not successfully treat the SE.”
In this presented clinical scenario of convulsive SE, 94% of clinicians administered additional intravenous benzodiazepines, with 57% combining this with levetiracetam as an adjunctive ASM. Other ASM were less frequently chosen at this time. The preferred benzodiazepine of choice here was lorazepam in 71.6%. Diazepam and clonazepam were chosen equally in 11.4%, midazolam in 38.3% (multiple benzodiazepines could be chosen) (Figure 1).
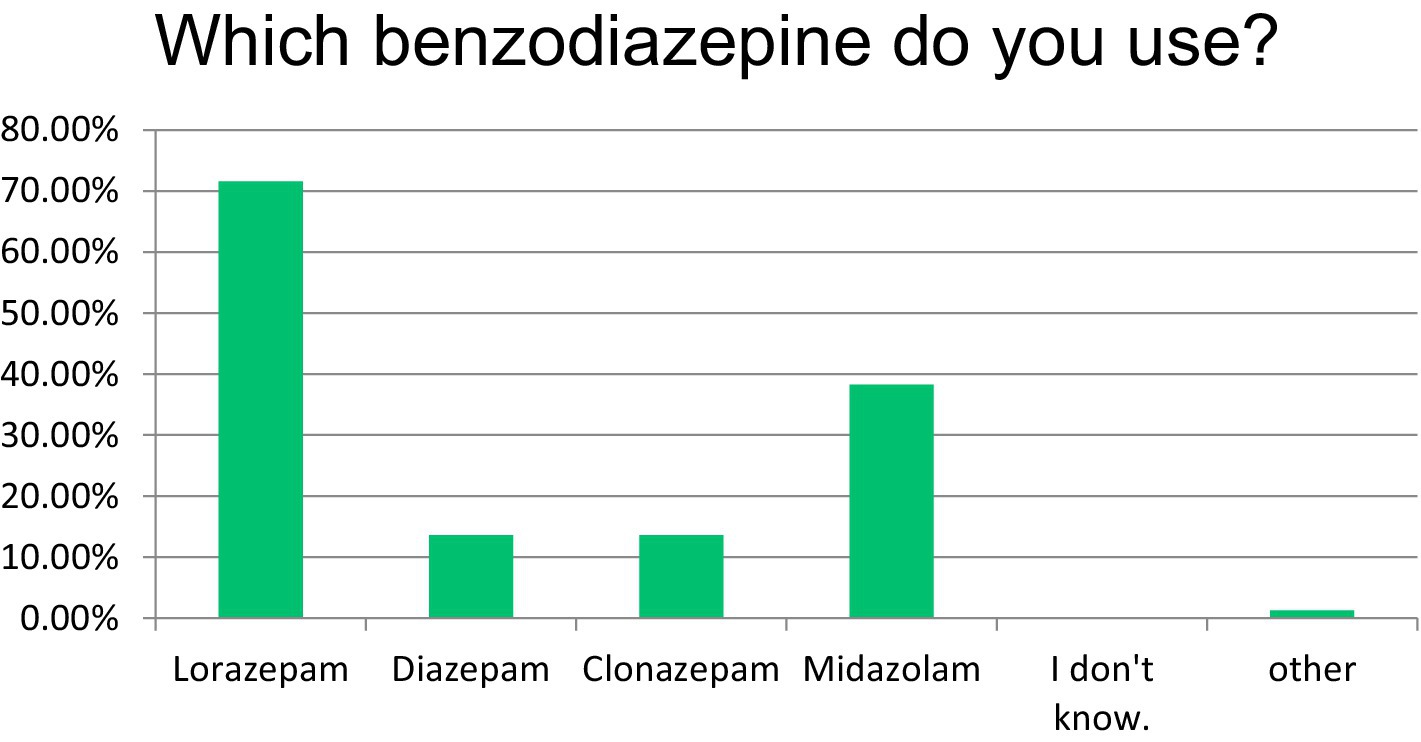
Figure 1. Benzodiazepine chosen for SE therapy stage 1.
The diagnostics chosen at this time (with the possibility of multiple answers) varied between performing a cerebral computer tomography (cCT), cerebral magnetic resonance imaging (cMRI), and cerebrospinal fluid (CSF) diagnostics or no diagnostics at the given time. EEG was reported as being routinely used in 40.24% of cases, whereas long-term (video) EEG monitoring was indicated by only 4.88% of respondents (Table 1). However, the survey did not capture whether EEG facilities were continuously available or restricted to office hours. This limitation prevents a precise evaluation of EEG accessibility across centers.
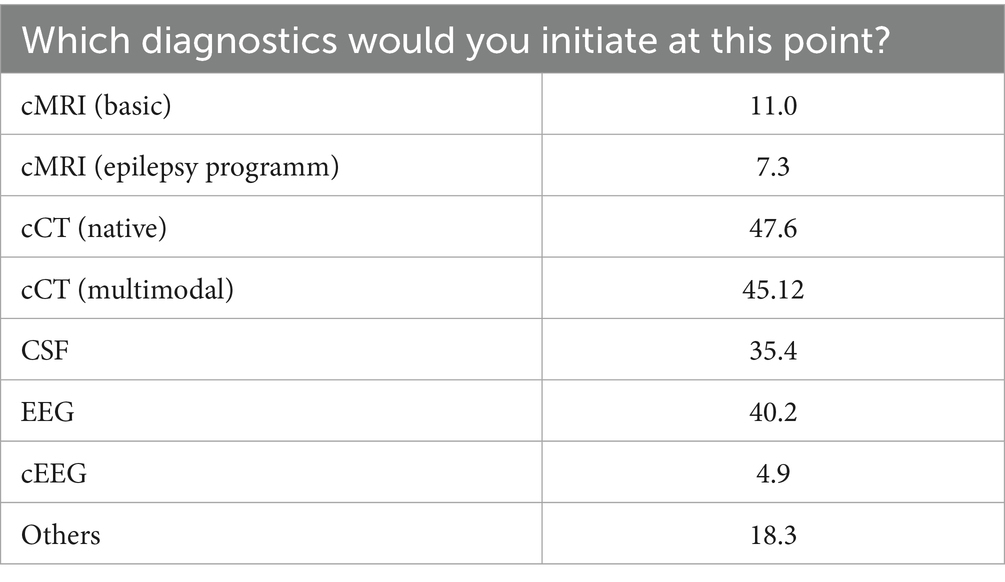
Table 1. Immediate diagnostic procedures after SE onset.
Next, the scenario evolved describing an established convulsive SE. In this setting, 35.4% of the respondents prefer iv-levetiracetam (after prior single administration of benzodiazepines), 13.4% chose lacosamide, and 31.7% had chosen immediate anesthesia. The drug of choice here was propofol monotherapy in 25%, in combination with sufentanil/ fentanyl in 43.2% (Figure 2).
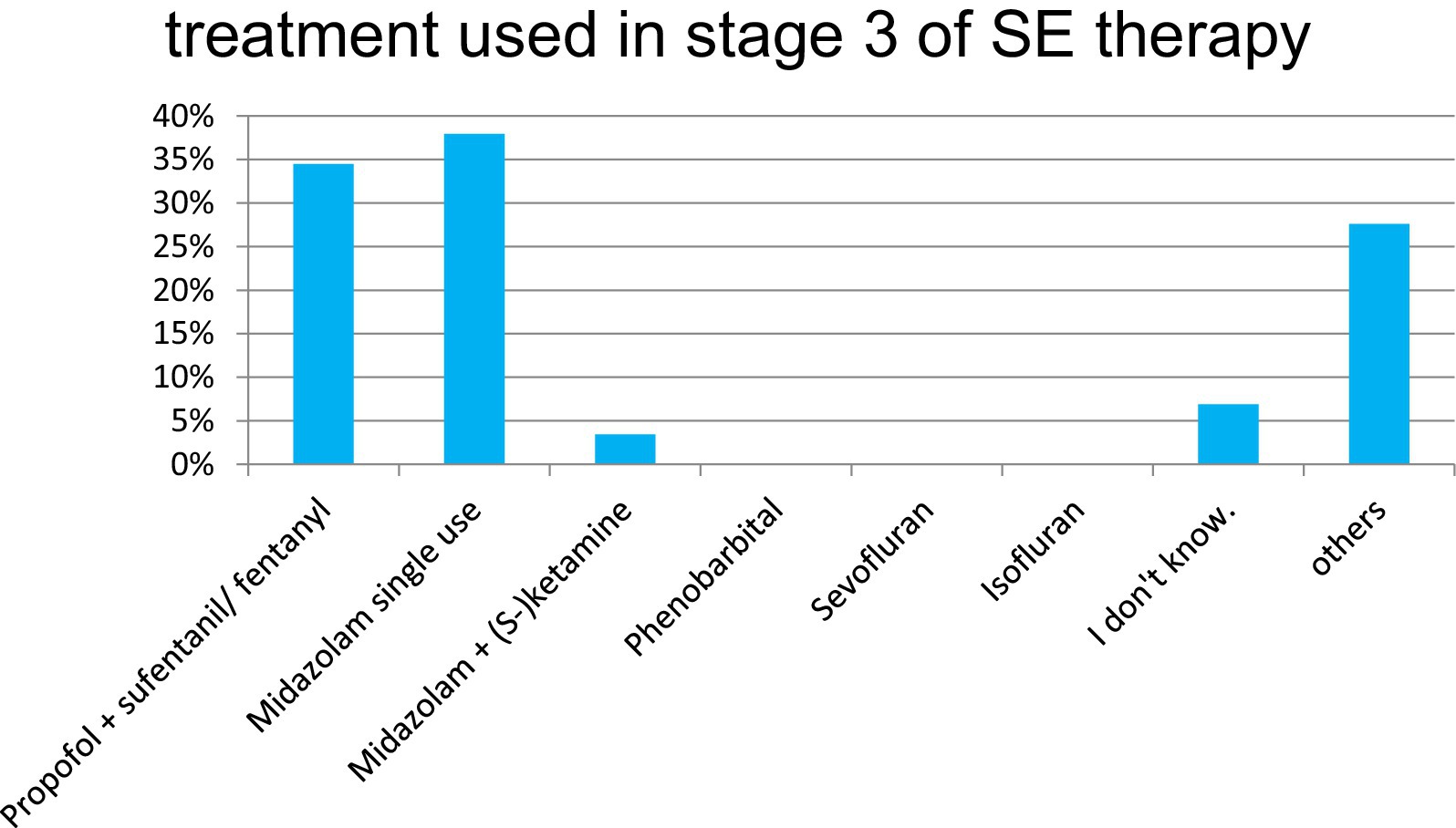
Figure 2. SE therapy, stage 3 (drug escalation).
At the decision point for initiating anesthesia in the case-based scenario, anesthesia was induced with propofol combined with sufentanil or fentanyl in 65.43% of cases, and with propofol monotherapy in 18.5%. The intended duration of anesthesia varied: 32.9% targeted a fixed 24-h period, 28.1% continued for 24 h following the onset of burst suppression, and 19.5% individualized the duration based on clinical assessment (Figure 3).
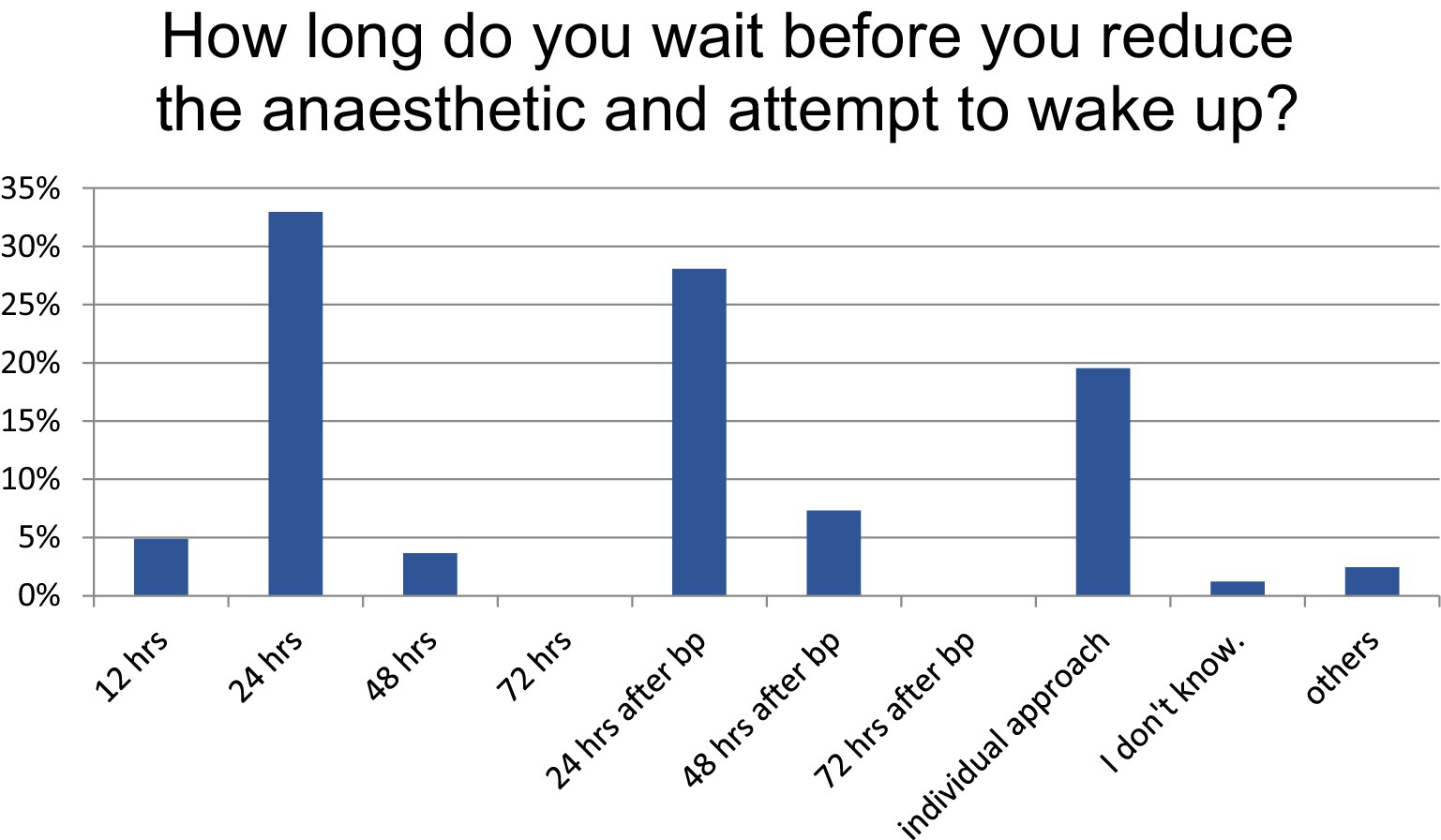
Figure 3. Duration of anesthetic approach, hrs, hours; bp, achieving burst suppression.
If SE persisted and progressed to SRSE, 11% of the respondents opted for a wait-and-see approach, 35% changed the anesthetic agent (with 36% changing PRO to MDZ with S-ketamine, and 19% to a barbiturate.), and 41% escalated treatment by adding an additional ASM.
If additional ASM chosen for escalated treatment at this stage:
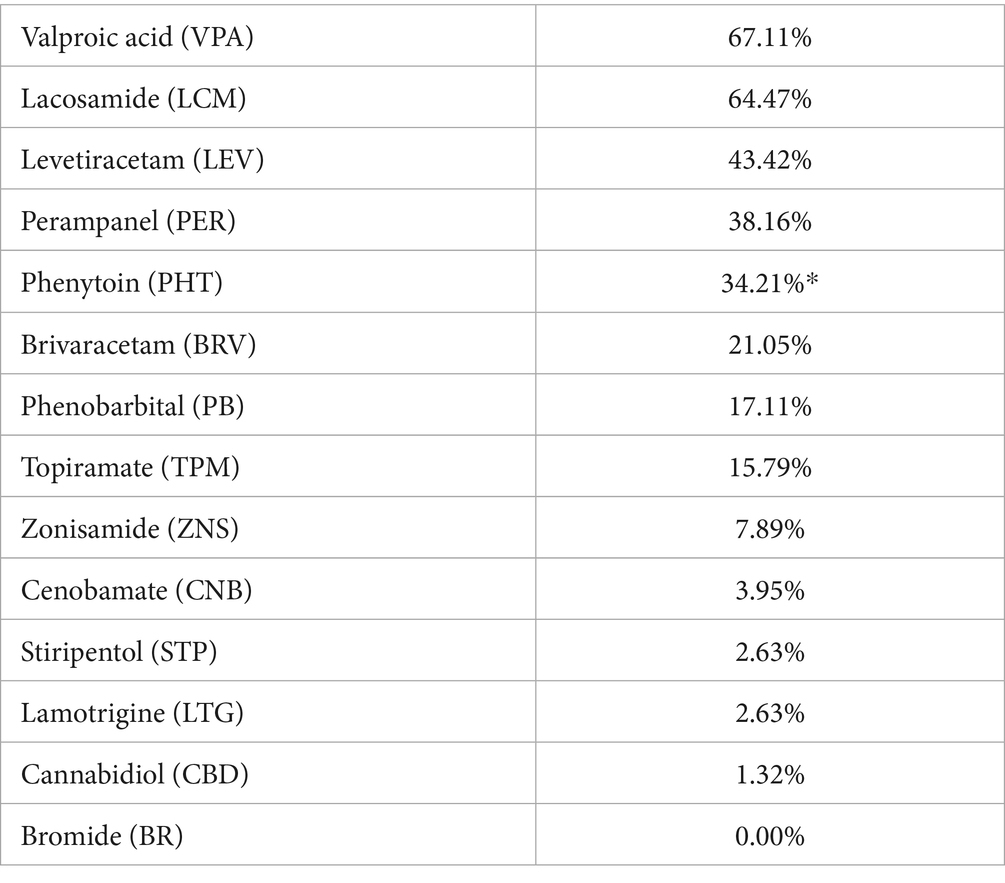
*The survey question did not differentiate between phenytoin and fosphenytoin, as fosphenytoin is approved in Germany and Austria but not marketed, and is not approved in Switzerland. Thus, the reported 34.2% “phenytoin” use in SRSE may have included fosphenytoin, but the authors assume that phenytoin was administered.
Treatment sequencing varied widely. Levetiracetam, lacosamide, and valproic acid were most frequently selected among the first three ASM, although no consistent preference emerged regarding the order. Not all respondents provided dosage information. However, where available, these were within the ranges recommended by the guideline.
Occasionally, stage 3 was also initiated after the administration of a single stage 2 medication.
Similarly, no clear consensus was observed regarding the use of adjunctive therapies such as ketogenic diet or steroids. Beyond the administration of ASM, additional therapeutic strategies were also considered.
These are used in clinical practice with the following frequency:
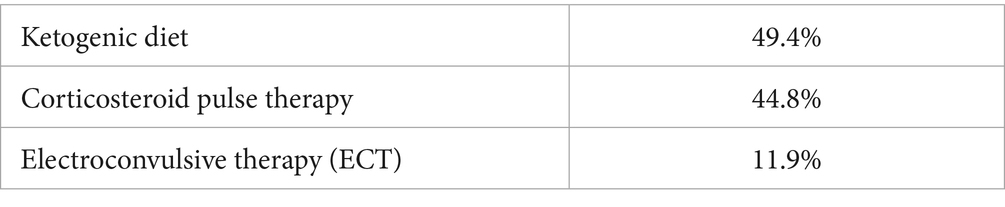
Targeted temperature management (TTM)/hypothermia, deep brain stimulation, transcranial magnetic stimulation (TMS), plasmapheresis and administration of intravenous immunoglobulins (IVIG) were sporadically mentioned.
Case 2
Case 2 described a 63-year-old woman with structural epilepsy treated with 1,500 mg levetiracetam daily, who presented to the emergency department with generalized convulsive status epilepticus. Her last seizure had occurred 6 months ago, prompting levetiracetam dose escalation from 1,000 to 1,500 mg.
This clinical information would not change the therapeutic approach for 65.2% of the respondents.
Part 2: prehospital management and diagnostic procedures
Prehospital management
Prehospital management is critical for the early recognition of SE. The question of whether SE is reliably recognized prehospitally, 74.2% of the respondents indicated that convulsive SE is reliably identified, whereas non-convulsive SE often is not. A standard operating procedure (SOP) or algorithm for SE management was available to 31.8% of emergency services, while 21.2% reported no access to such protocols, while almost half of the participants were unsure.
The prehospital benzodiazepine administration differed by agent: lorazepam was administered in 9.1%, diazepam in 37.9% and others, predominantly midazolam, in 50%. Doses ranged between 2 and 10 mg midazolam (or equivalent dose). Further, 21.2% of the respondents indicated that an anti-seizure medication was administered preclinically, most commonly levetiracetam.
Diagnostic procedures
In addition to pharmacological treatment, the survey assessed diagnostic practices in patients with SE: In patients with known epilepsy, 96.9% would order laboratory test (including electrolytes and infection marker), and 69.2% would order a cranial CT (cCT); only 10% reported performing MRI or CSF analysis. In contrast, patients with NORSE were more comprehensively evaluated: all recommended laboratory testing including electrolytes and infection parameters, 70.8% a cCT, 78.5% a cMRI and almost 80% CSF analysis. Although the results of ASM drug levels are rarely available in the emergency department, it is very important that this is done upon admission, as low levels can explain SE and can also be used to improve compliance subsequently. This was not explicitly asked in the survey.
Use of scores
When used (used by 6% only and by 12% occasionally), the most frequently used score was the STESS (Status epilepticus severity score), while other prognostic scores such as ACD (age at onset, level of consciousness at admission, and duration of status epilepticus), EMSE-EAC (Epidemiology-based Mortality Score in Status Epilepticus—Etiology, Age, level of Consciousness) and END-IT were rarely employed.
In this context, it should be emphasized that the ADAN score proposed by Requena and colleagues (11) is a diagnostic tool designed to support the early recognition of status epilepticus in the emergency medical setting. The ADAN scale was specifically designed for prehospital identification of SE when EEG is not immediately available. It is based on four easily assessable clinical parameters: Abnormal speech, Deviation of gaze (ocular deviation), Automatisms, and Number of seizures. The scale aims to assist EMS and emergency physicians in differentiating SE from other causes of impaired consciousness and to promote earlier recognition and treatment initiation. This tool is, to date, one of the very few diagnostic scores validated for potential use in prehospital and emergency department contexts and does not rely on EEG findings.
Discussion
The findings of this web-based survey among clinicians in Germany, Austria, and Switzerland highlight substantial variability in the management of SE, particularly in treatment strategies and diagnostic approaches. This observed heterogeneity underscores the lack of standardized consensus in key aspects of SE management and care and highlights the complexity and challenges faced by clinicians in managing this neurologic emergency. The development of evidence-based SE guidelines is particularly difficult in intensive care settings where there is little prospective data and a high degree of heterogeneity, for example due to different aetiologies, and requires extensive registry data. The new European registry coordinated by Prof. Nicolas Gaspard represents a unique opportunity to systematically capture treatment and outcome data across centers (12). Such initiatives are an important step toward fact-based rather than consensus-only guidelines.
Medication choices and dosage
The survey confirms a strong preference for benzodiazepines as first-line therapy in status epilepticus (SE), with lorazepam selected by 71.6% of respondents—aligning with guideline recommendations (13).
While lorazepam appears favored in hospital settings, its requirement for cooled storage limits its prehospital use. Following initial benzodiazepine administration, 56.6% of clinicians selected levetiracetam as a second-line agent, consistent with growing evidence supporting its role in early SE management (14). In contrast, ASM such as lacosamide (13.4%) were less commonly used, possibly due to lower familiarity, lack of authorization and contraindications in patients with atrioventricular conduction abnormalities (15).
Third-line therapies for refractory status epilepticus showed greater heterogeneity. Propofol, often used in combination with fentanyl or sufentanil, was the most frequently chosen option, aligning with established recommendations for SRSE management (16).
Decisions regarding the duration of anesthesia varied: 35% targeted 24 h after achieving burst suppression, whereas 19.5% individualized treatment duration based on clinical judgment. Current guidelines remain noncommittal regarding whether burst suppression or seizure cessation should guide anesthetic depth, and available evidence does not clearly favor one strategy over the other (17).
These findings underscore the variability in SE management—particularly in third-line therapy—and reflect both the complexity of clinical decision-making in SRSE and the absence of robust, consensus-driven protocols for anesthetic duration (18). Although established ICU outcome scores such as the simplified acute physiology score (SAPS) and the Acute Physiology and Chronic Health Evaluation (APACHE) as well as the Complication Burden Index (CBI) (19) were not included in this survey, their systematic incorporation in future registry-based studies would provide valuable context for comparing treatment outcomes across centers. These scoring systems are used to assess disease severity (SAPS, APACHE) and to quantify the cumulative burden of medical complications during ICU stay (CBI). Including such standardized outcome metrics in large-scale SE registries could facilitate benchmarking between hospitals, improve the understanding of treatment-related morbidity, and support the development of evidence-based prognostic tools for SE management.
Despite adherence to guideline-recommended agents, the lack of standardized treatment sequencing remains evident.
Prehospital management
The prehospital management remains a critical point in the overall course of SE. A multicenter prospective registry study from Germany, Austria and Switzerland reported that over one-third of SE cases presented initially in the prehospital setting, however, a substantial proportion were treated subtherapeutically inconsistent with established guidelines. The clinical impact of such deviation remains unclear but underscores the need for improved prehospital protocols (9).
The survey revealed that the majority of clinicians (74.2%) felt that convulsive SE was reliably recognized prehospitally, while non-convulsive SE was found frequently missed. This diagnostic gap is concerning, given the potential morbidity associated with NCSE (20, 21). Several diagnostic scoring systems for status epilepticus (SE) have been proposed over the past decade, but few have entered routine clinical use. These include the EMSE-EAC score (37) and the more recent ADAN score, developed specifically for prehospital SE recognition (11). While the EMSE-EAC aims to classify SE subtypes and predict outcomes using EEG, etiology, and comorbidity data, the ADAN score provides an EEG-independent diagnostic tool based purely on clinical parameters. Despite their potential utility, both have seen limited adoption in everyday practice—primarily due to a lack of external validation, complexity of data collection, and limited integration into emergency workflows.
Our findings mirror this gap between research and clinical implementation: most respondents reported not using any structured diagnostic or prognostic scoring system. To bridge this gap, future efforts should focus on validating simplified, time-efficient tools that can be integrated into electronic documentation systems or combined with emerging artificial intelligence based support systems to facilitate rapid and accurate SE diagnosis, especially in prehospital and emergency department settings.
The use of easy to apply, EEG detection systems, potentially supported by artificial intelligence might also offer viable solutions here (22, 23). The availability of EEG, especially in the emergency department and prehospital settings, remains a crucial issue. Continuous EEG is essential for detecting non-convulsive SE and assessing treatment response, as highlighted in recent studies (24, 25). Nevertheless, the lack of round-the-clock EEG coverage in many hospitals and the absence of EEG in most emergency medical services create a diagnostic gap. Early EEG recording—even short, portable or tele-EEG approaches—has been shown to improve early recognition of NCSE and guide timely therapy initiation in emergency settings.
Midazolam was the most frequently administered benzodiazepine in the prehospital setting, in line with current guidelines, (5, 26). However, wide dosing variability (2–10 mg) highlights the lack of standardized administration protocols, and persistent underdosing remains a critical concern (9, 27).
ASMs are often administered preclinically, highlighting concerns about the underdosing of benzodiazepines (8, 27). The use of ASMs prior to hospital arrival was also reported, most commonly levetiracetam. This may reflect inappropriate substitution for first-line benzodiazepines, particularly in elderly patients or those with reduced consciousness, despite a lack of supporting evidence (28, 29). These findings emphasize the need for targeted education, protocol harmonization, and prospective evaluation of prehospital SE interventions to ensure adherence to evidence-based standards.
The limited availability of standard operating procedures (SOPs) for SE management observed in our survey highlights a critical gap in the standardization of emergency care. Only about one-third of respondents reported having access to a defined SE protocol, while almost half were unsure whether such a guideline existed in their institution. The lack of clear, structured algorithms may delay escalation of therapy and contribute to outcome variability between centers. Although our study did not explicitly assess regional differences, anecdotal responses suggest heterogeneity among German-speaking countries, reflecting differences in hospital organization and training structures. The need for unified, evidence-based SOPs extends therefore beyond the German-speaking area. A recent study from Norway highlighted this variability, showing that as many as 18 different emergency protocols for SE were in use within a relatively small country (30). This lack of standardization was associated with delayed treatment escalation and inconsistent use of anesthetics in refractory SE. Developing harmonized European or international protocols—integrating prehospital and in-hospital treatment recommendations—could therefore improve therapeutic consistency and facilitate multicenter research comparability.
The survey did not systematically assess differences between emergency medical service (EMS) structures, which represents a limitation of the present study. However, the existing literature indicates considerable heterogeneity between EMS systems. Benzodiazepines remain the only anti-seizure medication consistently available in most EMS units, serving as the universally recommended first-line treatment for prehospital SE management (31). This has been confirmed in more recent data from the United States, showing that intravenous lorazepam, intravenous or intramuscular diazepam, and intramuscular midazolam are the mainstay of prehospital SE therapy (32).
Across Europe, substantial variability in prehospital SE protocols persists, with inconsistent dosing recommendations, administration routes, and timing.
Second-line ASMs such as levetiracetam or valproate are rarely available in ambulances and are usually administered only after hospital arrival (28, 33). However, several European emergency medical systems—most notably in France and Finland—have integrated the prehospital administration of second-line ASMs, particularly intravenous levetiracetam, into routine practice. The SAMUKeppra study randomised phase 3 trial demonstrated the feasibility and safety of adding levetiracetam to clonazepam in the prehospital treatment of SE (29), and other studies further emphasise that earlier ASM administration and reduced treatment delays are associated with improved outcomes in SE: A study from 2015 found that in children with convulsive status epilepticus (CSE), the administration and escalation of ASM were substantially delayed both before and after hospital arrival, often taking over an hour from seizure onset (34). In addition to that, Kämppi et al. (35) showed that in adults with generalized CSE, treatment delays—especially longer than 2.5 h for diagnosis or escalation of antiseizure therapy—were linked to poorer outcomes, highlighting the need for rapid diagnosis, timely treatment, and prompt transfer to specialized hospitals. These experiences underline that minimising prehospital treatment delays—through protocol adaptation and drug availability—should be a central goal in EMS care for SE.
Overall, these data highlight the wide heterogeneity of prehospital SE treatment capabilities and underscore the urgent need for harmonized EMS protocols and standard operating procedures across regions.
Diagnostic procedures
The survey showed that the variance in diagnostic procedures was significantly smaller than the variance in treatment, indicating good practice in neurological emergencies. Only the initial application of prognostic scores is highly variable and has seen limited integration into clinical routine, in part because their sensitivity and specificity are insufficient for individual clinical decision-making (29). Better validated scoring systems are needed, and artificial intelligence approaches may help to improve future predictive accuracy.
Limitations
The study has several limitations. The sample size was small and predominantly composed of respondents from university hospitals with rapid access to neuro-intensive care units and experience on treating neuro-intensive care patients. In addition, the majority of participants were experienced clinicians; young colleagues, who often provide primary therapy in the emergency department, being underrepresented. Despite the bias in favor of highly experienced respondents, heterogeneity in treatment was reported. The clinical scenarios focused specifically on the management of generalized convulsive SE. It might occur that treatment choices would differ in other contexts, such as focal motor SE or NCSE. However, given that treatment guidelines focus on generalized convulsive SE, the observed heterogeneity underscores the significant variability in clinical practice, even within standardized scenarios.
Conclusion
This survey highlights current practices in the management of SE in the German-speaking countries of Europe. With lorazepam and midazolam being preferred in intra-hospital and pre-hospital settings. From stage 2 of treatment onwards, there are trends, such as the use of levetiracetam for stage 2 and propofol for stage 3. Management of SRSE remains highly variable due to limited guideline evidence. Standardization of prehospital treatment, ICU diagnostics and therapy monitoring is needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
LM: Methodology, Formal analysis, Visualization, Conceptualization, Writing – original draft. UF: Writing – review & editing, Conceptualization. LH: Writing – review & editing. CJ: Writing – review & editing.
Group members of IGNITE Group and the MuSE Group
IGNITE: Initiative of German Neurointensive Trial Engagement, a Section for Clinical Studies within the German Society for Neurointensive and Emergency Care (Deutsche Gesellschaft für NeuroIntensiv- und Notfallmedizin, DGNI). IGNITE Group members are listed in the Supplementary material.
MuSE: multicentric Studies in Epilepsy, part of the German Society for Epilepsy (Deutsche Gesellschaft für Epileptologie, DGfE), Austrian Society for Epilepsy (Österreichische Gesellschaft für Epileptologie, ÖGfE) and Swiss Epilepsy League (Schweizerische Epilepsie-Liga).
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. UF received personal grants from the Gottfried and Julia Bangerter-Rhyner Foundation and the Andre and Michel Bouriez Foundation. LH received a traveling grant from Jazz Pharma and Angelini Pharma, as well as a clinical fellowship from DGfE. CJ states that she has received research support from the ILAE and a fellowship from the DGfE, which had no influence on the present article. Open Access funding provided by the Open Access Publishing Fund of Philipps-Universität Marburg.
Acknowledgments
We would like to take this opportunity to thank everyone who took part in the survey, especially the ignite (Initiative of German Neurointensive Trial Engagement), a Section for Clinical Studies within the German Society for Neurointensive and Emergency Care (Deutsche Gesellschaft für NeuroIntensiv- und Notfallmedizin, DGNI) and MuSE (multicentric Studies in Epilepsy, part of the German Society for Epilepsy (Deutsche Gesellschaft für Epileptologie, DGfE), Austrian Society for Epilepsy (Österreichische Gesellschaft für Epileptologie, ÖGfE) and Swiss Epilepsy League (Schweizerische Epilepsie-Liga) groups, for their support and responses.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. Generative AI was used during the preparation of this work the authors used chat GPT (ChatGPT 4) and DeeplL Write for final checking of grammar and language. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1685993/full#supplementary-material
References
1. Knake, S, Rosenow, F, Vescovi, M, Oertel, WH, Mueller, HH, Wirbatz, A, et al. Incidence of status epilepticus in adults in Germany: a prospective, population-based study. Epilepsia. (2001) 42:714–8. doi: 10.1046/j.1528-1157.2001.01101.x
2. Leitinger, M, Trinka, E, Giovannini, G, Zimmermann, G, Florea, C, Rohracher, A, et al. Epidemiology of status epilepticus in adults: a population-based study on incidence, causes, and outcomes. Epilepsia. (2019) 60:53–62. doi: 10.1111/epi.14607
3. Fisher, RS, Cross, JH, French, JA, Higurashi, N, Hirsch, E, Jansen, FE, et al. Operationale Klassifikation der Anfallsformen durch die Internationale Liga gegen Epilepsie: Positionspapier der ILAE-Klassifikations- und Terminologiekommission. Z Epileptol. (2018) 31:272–81. doi: 10.1007/s10309-018-0216-8
4. Kirmani, BF, Au, K, Ayari, L, John, M, Shetty, P, and Delorenzo, RJ. Super-refractory status epilepticus: prognosis and recent advances in management. Aging Dis. (2021) 12:1097–119. doi: 10.14336/AD.2021.0302
5. Trinka, E, Cock, H, Hesdorffer, D, Rossetti, AO, Scheffer, IE, Shinnar, S, et al. A definition and classification of status epilepticus--report of the ILAE task force on classification of status epilepticus. Epilepsia. (2015) 56:1515–23. doi: 10.1111/epi.13121
6. Tian, L, Li, Y, Xue, X, Wu, M, Liu, F, Hao, X, et al. Super-refractory status epilepticus in West China. Acta Neurol Scand. (2015) 132:1–6. doi: 10.1111/ane.12336
7. Kantanen, A-M, Reinikainen, M, Parviainen, I, and Kälviäinen, R. Long-term outcome of refractory status epilepticus in adults: a retrospective population-based study. Epilepsy Res. (2017) 133:13–21. doi: 10.1016/j.eplepsyres.2017.03.009
8. Guterman, EL, Burke, JF, and Sporer, KA. Prehospital treatment of status epilepticus in the United States. JAMA. (2021) 326:1970–1. doi: 10.1001/jama.2021.15964
9. Kellinghaus, C, Rossetti, AO, Trinka, E, Lang, N, Unterberger, I, Rüegg, S, et al. SENSE registry for status epilepticus. Epilepsia. (2018) 59:150–4. doi: 10.1111/epi.14495
10. Hirsch, LJ, Gaspard, N, van Baalen, A, Nabbout, R, Demeret, S, Loddenkemper, T, et al. Proposed consensus definitions for new-onset refractory status epilepticus (NORSE), febrile infection-related epilepsy syndrome (FIRES), and related conditions. Epilepsia. (2018) 59:739–44. doi: 10.1111/epi.14016
11. Requena, M, Fonseca, E, Olivé, M, Abraira, L, Quintana, M, Mazuela, G, et al. The ADAN scale: a proposed scale for pre-hospital use to identify status epilepticus. Eur J Neurol. (2019) 26:e55:760. doi: 10.1111/ene.13885
12. Damien, C, Leitinger, M, Kellinghaus, C, Strzelczyk, A, De Stefano, P, Beier, CP, et al. Sustained effort network for treatment of status epilepticus/European academy of neurology registry on adult refractory status epilepticus (SENSE-II/AROUSE). BMC Neurol. (2024) 24:19. doi: 10.1186/s12883-023-03505-y
13. Sathe, AG, Underwood, E, Coles, LD, Elm, JJ, Silbergleit, R, Chamberlain, JM, et al. Patterns of benzodiazepine underdosing in the established status epilepticus treatment trial. Epilepsia. (2021) 62:795–806. doi: 10.1111/epi.16825
14. Nakamura, K, Marushima, A, Takahashi, Y, Mochizuki, M, Kimura, A, Fukuda, Y, et al. Levetiracetam versus fosphenytoin as a second-line treatment after diazepam for adult convulsive status epilepticus: a multicentre non-inferiority randomised control trial. J Neurol Neurosurg Psychiatry. (2023) 94:42–8. doi: 10.1136/jnnp-2022-329485
15. Ben-Menachem, E, Dominguez, J, Szász, J, Beller, C, Howerton, C, Jensen, L, et al. Long-term safety and tolerability of lacosamide monotherapy in patients with epilepsy: results from a multicenter, open-label trial. Epilepsia Open. (2021) 6:618–23. doi: 10.1002/epi4.12522
16. Rai, S, and Drislane, FW. Treatment of refractory and super-refractory status epilepticus. Neurotherapeutics. (2018) 15:697–712. doi: 10.1007/s13311-018-0640-5
17. Fisch, Urs, Jünger, Anja L., Baumann, Sira M., Semmlack, Saskia, Marchis, Gian Marcode, Hunziker, Sabina, et al. (2023) Association between induced burst suppression and clinical outcomes in patients with refractory status epilepticus: a 9-year cohort study Neurology 100 e1955–e1966 doi: 10.1212/WNL.0000000000207129
18. Cornwall, CD, Krøigård, T, Kristensen, JSS, Callesen, HE, and Beier, CP. Outcomes and treatment approaches for super-refractory status epilepticus: a systematic review and meta-analysis. JAMA Neurol. (2023) 80:959–68. doi: 10.1001/jamaneurol.2023.2407
19. Kämppi, L, Ritvanen, J, Strbian, D, Mustonen, H, and Soinila, S. Complication burden index-a tool for comprehensive evaluation of the effect of complications on functional outcome after status epilepticus. Epilepsia. (2018a) 59:176–81. doi: 10.1111/epi.14491
20. Maier, S, Godau, J, Bösel, J, and Rösche, J. Recognition and treatment of status epilepticus in the prehospital setting. Seizure. (2021) 86:1–5. doi: 10.1016/j.seizure.2020.12.014
21. Sutter, R, Rüegg, S, and Kaplan, PW. Epidemiology, diagnosis, and management of nonconvulsive status epilepticus: opening Pandora's box. Neurol Clin Practice. (2012) 2:275–86. doi: 10.1212/CPJ.0b013e318278be75
22. Guterman, EL, Mercer, MP, Wood, AJ, Amorim, E, Kleen, JK, Gerard, D, et al. Evaluating the feasibility of prehospital point-of-care EEG: the prehospital implementation of rapid EEG (PHIRE) study. J Am College Emerg Phys Open. (2024) 5:e13303. doi: 10.1002/emp2.13303
23. Welte, TM, Janner, F, Lindner, S, Gollwitzer, S, Stritzelberger, J, Lang, JD, et al. Evaluation of simplified wireless EEG recordings in the neurological emergency room. PLoS One. (2024) 19:e0310223. doi: 10.1371/journal.pone.0310223
24. Bitar, R, Khan, UM, and Rosenthal, ES. Utility and rationale for continuous EEG monitoring: a primer for the general intensivist. Crit Care. (2024) 28:244. doi: 10.1186/s13054-024-04986-0
25. Kozak, R, Gururangan, K, Dorriz, PJ, and Kaplan, M. Point-of-care electroencephalography enables rapid evaluation and management of non-convulsive seizures and status epilepticus in the emergency department. J Am Coll Emerg Phys Open. (2023) 4:e13004. doi: 10.1002/emp2.13004
26. Rosenow, F, and Weber, J. S2k-Leitlinie: Status Epilepticus im Erwachsenenalter: Leitlinie der Deutschen Gesellschaft für Neurologie. Nervenarzt. (2021) 92:1002–30. doi: 10.1007/s00115-020-01036-2
27. Di Vito, L, Matteo, E, Meletti, S, Zenesini, C, Bernabè, G, Bomprezzi, C, et al. Prognostic factors and impact of management strategies for status epilepticus: the STEPPER study in the Emilia-Romagna region, Italy. Epilepsia. (2024) 66:753–67. doi: 10.1111/epi.18227
28. Burghaus, L, Madlener, M, Kohle, F, Bruno, EF, Limmroth, V, Fink, GR, et al. Prehospital levetiracetam use in adults with status epilepticus: results of a multicenter registry. J Clin Neurol. (2023) 19:365–70. doi: 10.3988/jcn.2022.0302
29. Navarro, V, Dagron, C, Elie, C, Lamhaut, L, Demeret, S, Urien, S, et al. Prehospital treatment with levetiracetam plus clonazepam or placebo plus clonazepam in status epilepticus (SAMUKeppra): a randomised, double-blind, phase 3 trial. The Lancet Neurol. (2016) 15:47–55. doi: 10.1016/S1474-4422(15)00296-3
30. Hustad, IA, Horn, M, Rehn, M, Taubøll, E, and Hov, MR. Prehospital seizure management protocols need standardized guidelines. A descriptive study from Norway. Seizure. (2024) 123:92–6. doi: 10.1016/j.seizure.2024.10.002
31. Alldredge, BK, Gelb, AM, Isaacs, SM, Corry, MD, Allen, F, Ulrich, S, et al. A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med. (2001) 345:631–7. doi: 10.1056/NEJMoa002141
32. Silbergleit, R, Durkalski, V, Lowenstein, D, Conwit, R, Pancioli, A, Palesch, Y, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus. N Engl J Med. (2012) 366:591–600. doi: 10.1056/NEJMoa1107494
33. Billington, M, Kandalaft, OR, and Aisiku, IP. Adult status epilepticus: a review of the prehospital and emergency department management. J Clin Med. (2016) 5:74. doi: 10.3390/jcm5090074
34. Sánchez Fernández, I, Abend, NS, Agadi, S, An, S, Arya, R, Brenton, JN, et al. Time from convulsive status epilepticus onset to anticonvulsant administration in children. Neurology. (2015) 84:2304–11. doi: 10.1212/WNL.0000000000001673
35. Kämppi, L, Mustonen, H, Kotisaari, K, and Soinila, S. The essence of the first 2.5 h in the treatment of generalized convulsive status epilepticus. Seizure. (2018b) 55:9–16. doi: 10.1016/j.seizure.2017.12.007
36. Menche, M, Jünemann, C, Reese, JP, Jünemann, M, Teepker, M, Best, C, et al. The impact of revised definitions on the epidemiology of status epilepticus: A population-based study. Epilepsia. (2025) 64. doi: 10.1111/epi.18535
Keywords: epilepsy, status epilepticus, anti-seizure medication, neurocritical care, prehospital management, anesthetic agents
Citation: Möller L, Fisch U, Habermehl L and Jünemann C (2025) Treating status epilepticus in clinical practice—a multi-national survey in Germany, Austria, and Switzerland. Front. Neurol. 16:1685993. doi: 10.3389/fneur.2025.1685993
Edited by:
Ronny Wickstrom, Karolinska Institutet, SwedenReviewed by:
Erik Taubøll, Oslo University Hospital, NorwayLeena Kämppi, Helsinki University Hospital, Finland
Copyright © 2025 Möller, Fisch, Habermehl and Jünemann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leona Möller, bGVvbmEubW9lbGxlckBtZWQudW5pLW1hcmJ1cmcuZGU=