 Martina Sombetzki1
Martina Sombetzki1 Petra Lücker2
Petra Lücker2 Manja Ehmke1Sabrina Bock3Martina Littmann3
Manja Ehmke1Sabrina Bock3Martina Littmann3 Emil C. Reisinger1Wolfgang Hoffmann2
Emil C. Reisinger1Wolfgang Hoffmann2 Anika Kästner2*
Anika Kästner2*- 1Department of Tropical Medicine and Infectious Diseases, University Medical Center Rostock, Rostock, Germany
- 2Department for Epidemiology of Health Care and Community Health, Institute for Community Medicine, University Medicine Greifswald, Greifswald, Germany
- 3Landesamt für Gesundheit und Soziales Mecklenburg-Vorpommern State Office for Health and Social Affairs, Rostock, Germany
Introduction: With the increased emergence of SARS-CoV-2 variants, the impact on schools and preschools remains a matter of debate. To ensure that schools and preschools are kept open safely, the identification of factors influencing the extent of outbreaks is of importance.
Aim: To monitor dynamics of COVID-19 infections in schools and preschools and identify factors influencing the extent of outbreaks.
Methods: In this prospective observational study we analyzed routine surveillance data of Mecklenburg-Western Pomerania, Germany, from calendar week (CW) 32, 2020 to CW19, 2021 regarding SARS-CoV-2 infection events in schools and preschools considering changes in infection control measures over time. A multivariate linear regression model was fitted to evaluate factors influencing the number of students, teachers and staff tested positive following index cases in schools and preschools. Due to an existing multicollinearity in the common multivariate regression model between the variables “face mask obligation for children” and “face mask obligation for adults”, two further separate regression models were set up (Multivariate Model Adults and Multivariate Model Children).
Results: We observed a significant increase in secondary cases in preschools in the first quarter of 2021 (CW8 to CW15, 2021), and simultaneously a decrease in secondary cases in schools. In multivariate regression analysis, the strongest predictor of the extent of the outbreaks was the teacher/ caregiver mask obligation (B = −1.9; 95% CI: −2.9 to −1.0; p < 0.001). Furthermore, adult index cases (adult only or child+adult combinations) increased the likelihood of secondary cases (B = 1.3; 95% CI: 0.9 to 1.8; p < 0.001). The face mask obligation for children also showed a significant reduction in the number of secondary cases (B = −0.6; 95% CI: −0.9 to −0.2; p = 0.004.
Conclusion: The present study indicates that outbreak events at schools and preschools are effectively contained by an obligation for adults and children to wear face masks.
Introduction
Since the emergence of the coronavirus SARS-CoV-2 and the subsequent global COVID-19 pandemic, the role of children and adolescents, and in particular the role of schools and pre-schools in the infection process remains unclear. Preliminary results suggest that children younger than 10–14 years have a lower susceptibility to SARS-CoV-2 infection compared to adults (1–4). In addition, children have lower rates of severe COVID-19 courses compared to other age groups and present fewer and milder symptoms compared to adults (5–7).
Although the closure of general and private schools, as well as pre-schools, has become a common approach in containing the COVID-19 pandemic, the contribution of school and pre-school openings to the dynamics of the pandemic is unclear. On the one hand, it has been shown that schools play a rather minor role in virus spreading and that infections occurring in schools largely reflect the incidence of the surrounding area (8, 9). On the other hand, it has been shown that school closures can have a significant effect on the trend reversal of case numbers (10, 11). Nevertheless, early modeling studies of COVID-19 suggested that school closures alone would prevent only 2–4% of overall COVID-19-associated deaths (12). Children and adolescents represent a vulnerable group that is particularly at risk due to the social deprivation and constraints imposed by school closures, with consequent negative physical, psychological, and educational effects (13, 14).
To date, there is only insufficient evidence to definitively rule out schools as a source of infection. It remains undisputed that children and adolescents can be infected with SARS-CoV-2 and can spread the infection possibly as asymptomatic carriers. However, studies in schools suggest that infections are predominantly brought into schools by adults and that a child-to-child transmission in schools is rare and probably not the primary cause of SARS-CoV-2 infections in children collectives (15, 16). An analysis of laboratory-confirmed COVID-19 cases in children and adolescents in Germany from January to August 2020 showed that affected schools had few cases per outbreak and that older age groups were affected more frequently (17). Actual COVID-19 outbreaks in schools, i.e., infection events with more than one person infected are rare (8, 17).
Because new virus variants with altered infection dynamics emerge, it is crucial to closely monitor infection events in schools and pre-schools. In a study by Loenenbach et al. children and adolescents showed a comparable secondary attack rate (SAR) upon infections with SARS-CoV-2 variant B.1.1.7 to adults, with consequent evidence for increased susceptibility and infectiousness of the viral mutant in children and adolescents (18). In addition, the delta variant of SARS-CoV-2 is spreading rapidly worldwide. Analyses of self-administered RT-PCR swab samples tested for SARS-CoV-2 positivity as well as viral genome sequencing suggest that children may be infected with the delta variant of the virus more frequently than adults (19, 20). In the absence of pre-existing conditions, however, there is currently no evidence of a higher risk of severe disease progression in this age group. Nevertheless, there is some evidence suggesting that a relevant proportion of children may experience long-term effects similar to adults after clinical COVID-19 infection (Long COVID) (21).
The aim of this prospective observational study was to monitor the dynamics of infection events at schools and pre-schools, taking into account the hygiene regulations in force in Mecklenburg-Western Pomerania at the time, and to identify factors influencing the extent of outbreaks.
Methods
The following evaluations are based on data from the routine surveillance of the State Office for Health and Social Affairs Mecklenburg-Western Pomerania (Landesamtes für Gesundheit und Soziales M-V, LAGuS). We analyzed information of school-related infections from calendar week (CW) 32 in 2020 to CW 19 in 2021 at general and private schools and pre-schools. Local health offices identified school-related cases through contact tracing and reported them to the LAGuS. All vocational schools were excluded due to the special regulations with regard to hygiene measures and heterogeneity compared to the other types of schools. The primary objective of the study was to investigate the dynamics of COVID-19 infections in schools and pre-schools in dependence on pandemic-related changes in hygiene measures and to investigate the influence of hygiene measures on the extent of outbreaks. The ethics committee at the University Medical Center Rostock gave a positive vote on this study (Registration Number: A2020-0090).
Study Population
Cases with SARS-CoV-2 positive results were identified by laboratory-based RT-PCR testing. Then, the positive test results were forwarded to the LAGuS by physicians or laboratory staff. Federal health authorities categorized the infections as index or secondary cases by identifying contact persons and the onset of symptoms. Furthermore, infected individuals were indicated as children or adults. The number of infections that occurred at each school/pre-school were listed according to the respective CW.
Information on the affected institution for this study were provided by the LAGuS. These included name and location, the number of infections among adults and children, their classification into index and secondary cases as well as the prescribed measures. The information was anonymized and did not convey personal data. In a few cases, it was either not possible to identify the first person infected, or infection events occurred simultaneously, so two individuals may be listed as the index case.
An infection event in schools/pre-schools was defined by the LAGuS as one person tested positive by PCR testing (index case) and, in temporal (maximum 10 days) and spatial relation (same institution) to this, the occurrence of another person tested positive by PCR testing (secondary case). The R-factor (R-F) was calculated by dividing the number of secondary cases by the number of index cases.
Infection Control Measures and Timeline
Hygiene measures applicable in Mecklenburg-Western Pomerania were listed on the basis of the information letters and corona ordinances issued by the Ministry of Education, Science and Culture and the Ministry of Social Affairs, Integration and Equality in collaboration with the LAGuS (22, 23). The applicable hygiene measures were documented chronologically by date for schools and pre-schools (Table 1).
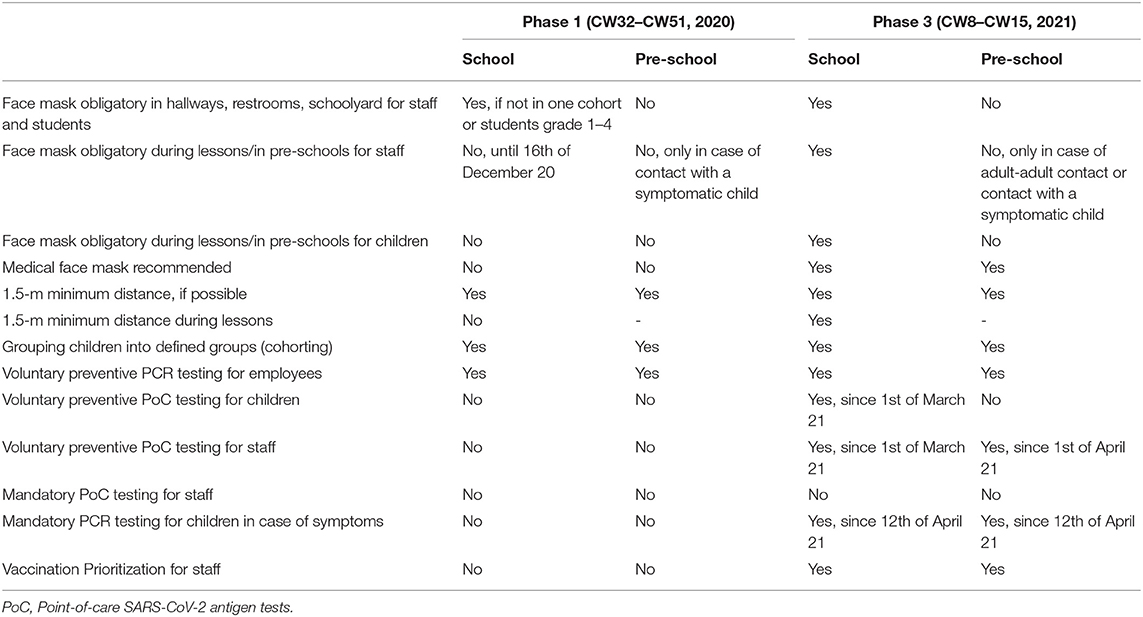
Table 1. Applicable hygiene measures in schools (Ministry of Education, Science and Culture) and pre-schools (Ministry of Social Affairs, Integration and Equality) in Mecklenburg-Western Pomerania comparing phase 1 with phase 3.
To capture the impact of hygiene measures, we divided infection events throughout the school year 2020/2021 into four phases. In phase 1, both schools and pre-schools were open on a regular basis and in usual operation, subject to conditions such as maintaining a minimum distance of 1.5 m, wherever possible. In the second phase, schools and pre-schools were closed. In the third phase, schools and pre-schools were gradually opened with modified hygiene measures, depending on the local incidence levels (see Table 1). In the fourth phase, there was another lockdown. During the lockdown, schools and pre-schools were primarily closed. Pupils were instructed from the distance to self-study at home. Emergency care was provided for children from pre-school until 6th grade, if parents could prove to have system-relevant jobs (such as hospital employees, etc.) and were not able to organize other forms of childcare. Furthermore, all graduating classes were allowed to be taught in presence in the school building.
The study period was divided into the following time phases depending on the infection control measures in place:

Statistical Analysis
Continuous variables were reported as median (range), and categorical data as counts and percentages. In addition, the mean value per infection event was reported for the following variables: overall cases, index cases, secondary cases, index cases children, index cases adults, secondary cases children and secondary cases adults. Univariate analysis for categorical variables was performed by using Chi2-test or Fisher's exact-test and for continuous variables with Student's t-Test or Mann-Whitney-U test depending on the normal distribution (tested with Shapiro-Wilk test). To evaluate the impact of associated variables on the number of secondary cases, a multivariate analysis was conducted.
For multivariate analysis a common linear regression model was set up with the number of secondary cases as the dependent variable and as independent variables the total number of index cases, type of index case [Child (1)/Adult (2)/Child + Adult (3)], Mask obligation for adults [No (0)/Yes, conditionally (1)/Yes, everywhere in school building/pre-school (2)], mask obligation for children {No (0)/[No/Yes, conditionally (1)]/Yes, conditionally (2)/Yes, everywhere in the school building/pre-school (3)} and setting [school (0)/pre-school (1)]. For the variable “affected person as index case,” it occurred that more than one person was documented as an index case. This means that it was not possible to distinguish which person was infected first, e.g., because symptoms occurred simultaneously or two outbreaks occurred at the same time. When a child and an adult were documented as index cases, they were assigned to the “child + adult” category. With respect to the variables “face mask mandatory for adults” and “face mask mandatory for children,” “Yes, under certain circumstances” was selected if the mask obligation existed only under certain circumstances but not during the entire time spent in the school building/pre-school (Table 1). For schools, for example, this applies if there was no mask obligation during lessons and in pre-schools if there was no mask obligation for adults during pedagogical work with the children. Furthermore, the “No/Yes, conditionally” category was applied when the school consisted of a primary and secondary part, due to different applicable hygiene measures for children among different age groups. Time and location were considered by CW and county of the school/pre-school and were dummy-coded in the model to avoid temporal and spatial associations. Due to multicollinearity between the variables mask obligation for children and mask obligation for adults, two further multivariate linear regression models were set up, whereby in the “Multivariate Model Adults” the mask obligation for children was not taken into account and in the “Multivariate Model Children” the mask obligation for adults was not considered. Regression coefficients (B) are presented with 95% confidence intervals (CI). The goodness of fit of the model was determined using R2 and the corrected R2. Cohen's f2 was calculated with the formula f2 = [corrected R2/(1-corrected R2)].
A p-value < 0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics version 27. The figures were created using Microsoft® Excel (Microsoft® Excel for Mac, Version 16.51 (21071101).
Results
Hygiene Measures in Schools and Pre-schools
The specifications for hygiene measures to contain the COVID-19 pandemic in schools and pre-schools were continually adapted and changed throughout the study period from August 2020 until May 2021. Since schools and pre-schools were open in phase 1 and phase 3, we particularly compared the hygiene measures in those periods. Table 1 provides an overview of the hygiene measures that were in place in schools and pre-schools during each phase. General hygiene measures such as keeping a minimum distance (at least 1.5 m), proper coughing, sneezing and thorough hand washing, wearing a mask and frequent ventilation were persistent throughout the study period and are therefore neglected in the overview.
Regulations differed between schools and pre-schools in Mecklenburg-Western Pomerania, particularly regarding the obligation to wear a mask covering mouth and nose. A differentiation between staff (educators and teachers) and children is relevant. Face masks became mandatory on school grounds and within school buildings at the 4th of August 2020. Defined exceptions applied, e.g., during lessons; for pupils from 1st til 4th grade; if a distance of at least 1.5-m was kept or while drinking and eating.
The mask obligation during lessons was introduced for teachers at schools on 16th of December 2020, whereas this obligation for children was issued 8th of January 2021. Children in pre-schools were not required to wear a mask at any time of our study period. Educators in pre-schools are exempt from the mask requirement during their pedagogical work with children.
Other hygiene measures, such as maintaining the 1.5 m minimum distance, building defined cohorts, and offering vaccination to staff members, did not differ between the settings in the respective phases.
Infection Events in Schools
A total of 956 infection events occurred during the study period, of which n = 43 infection events were excluded from the analyses because they occurred at vocational schools. Of the included n = 913 infections, n = 475 occurred in schools and n = 438 in pre-schools. A summary of the total number of SARS-CoV-2 cases at schools and pre-schools during the study period is provided in Figure 1.
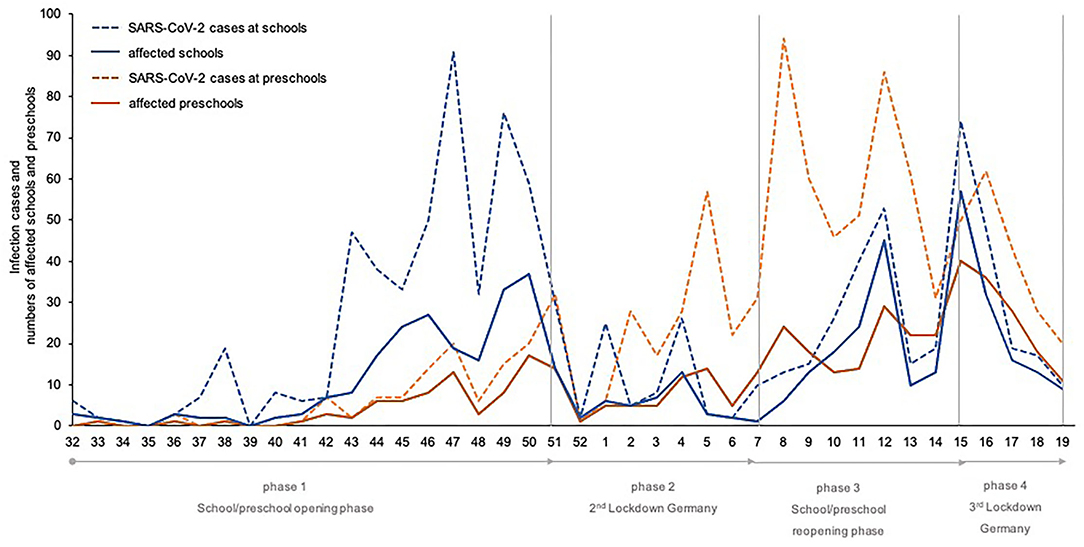
Figure 1. Total number of SARS-CoV-2 cases at schools and pre-schools in the study period (week 32/20–19/21) divided into the different phases of infection control measures in Mecklenburg-Western Pomerania.
In phases 1 (CW32-CW51, 2020) and 3 (CW8–CW15, 2021), the schools were open under different restrictions (Table 2). In phase 1, a total of n = 189 schools were affected by at least one infection. A total of n = 225 index cases and n = 236 secondary cases were identified (R-F = 1.05). Most frequently regional schools (n = 67) were affected, followed by elementary schools (n = 41) and integrated/cooperative, comprehensive schools (n = 35), grammar schools (n = 30), or special schools (n = 15).
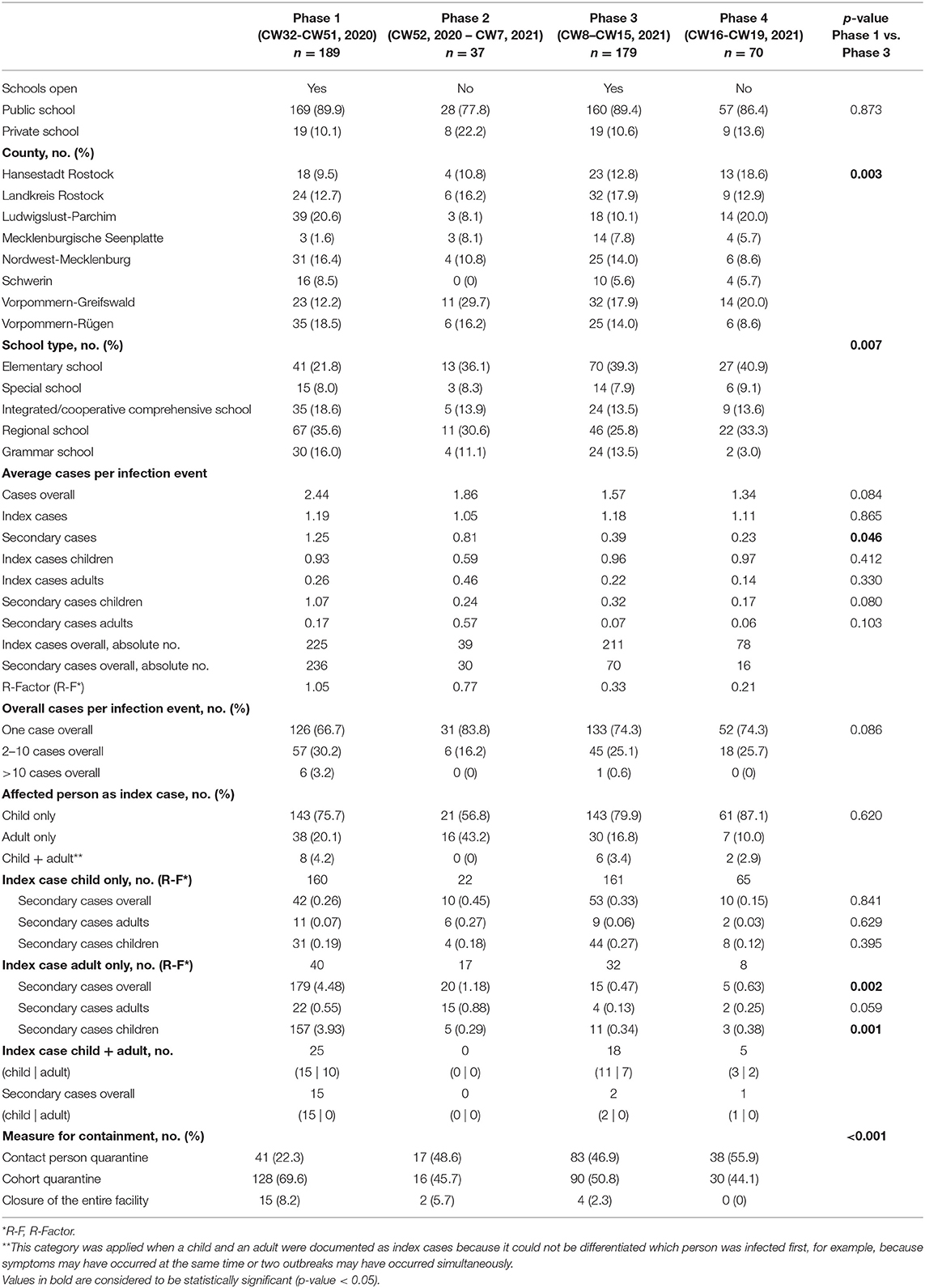
Table 2. Infection incidence in schools in Mecklenburg-Western Pomerania subdivided by time phases depending on infection control measures in place, N = 475.
In phase 3 (CW8-CW15 2021, open schools), a comparable number of schools was affected (n = 179) as in phase 1, but the incidence shifted to younger school cohorts (elementary schools n = 70, regional Schools n = 46, grammar schools n = 24, integrated/cooperative, comprehensive schools n = 24, special schools n = 14. A total of n = 211 index and n = 70 secondary cases (R-F = 0.33) were identified in phase 3.
In both phases 1 and 3, children were identified more frequently as index cases (phase 1: n = 160 and phase 3: n = 161) compared to adults (phase 1: n = 40 and phase 3: n = 32). The number of secondary cases caused by the index case “child only” was also comparable in both phases (phase 1: R-F = 0.26 and phase 3: R-F = 0.33), whereby children became infected more frequently (phase 1: R-F = 0.19 and phase 3: R-F = 0.27) than adults (phase 1: R-F = 0.07, and phase 3: R-F = 0.06).
Differences in the two phases became evident when considering the index case “adult only” and the resulting secondary infections. In total, n = 40 adults were identified as index cases in phase 1 and n = 32 in phase 3. These infections resulted in a total of 179 secondary infections (R-F = 4.48) in phase 1 and 15 secondary infections in phase 3 (R-F = 0.47, p = 0.002). Just as in the case of “child only” as index, more children (phase 1: R-F = 3.93 and phase 3: R-F = 0.34, p = 0.001) than adults (phase 1: R-F = 0.55 and phase 3: R-F = 0.13) became infected by positive adults.
With comparable numbers of affected schools and index cases, the number of subsequent cases decreases significantly from phase 1 to phase 3. This becomes particularly obvious when looking at the transmission from adults to children. An average of 2.44 cases was reported per infection event in phase 1, of these n = 1.19 were classified as index cases and n = 1.25 as secondary cases. In phase 3, an average of 1.57 cases occurred per infection event, of which 1.18 were index cases and 0.39 were secondary cases (p = 0.046).
Infection Events in Pre-schools
An overview of the COVID-19 infection events at pre-schools subdivided into phases during the study period is given in Table 3.
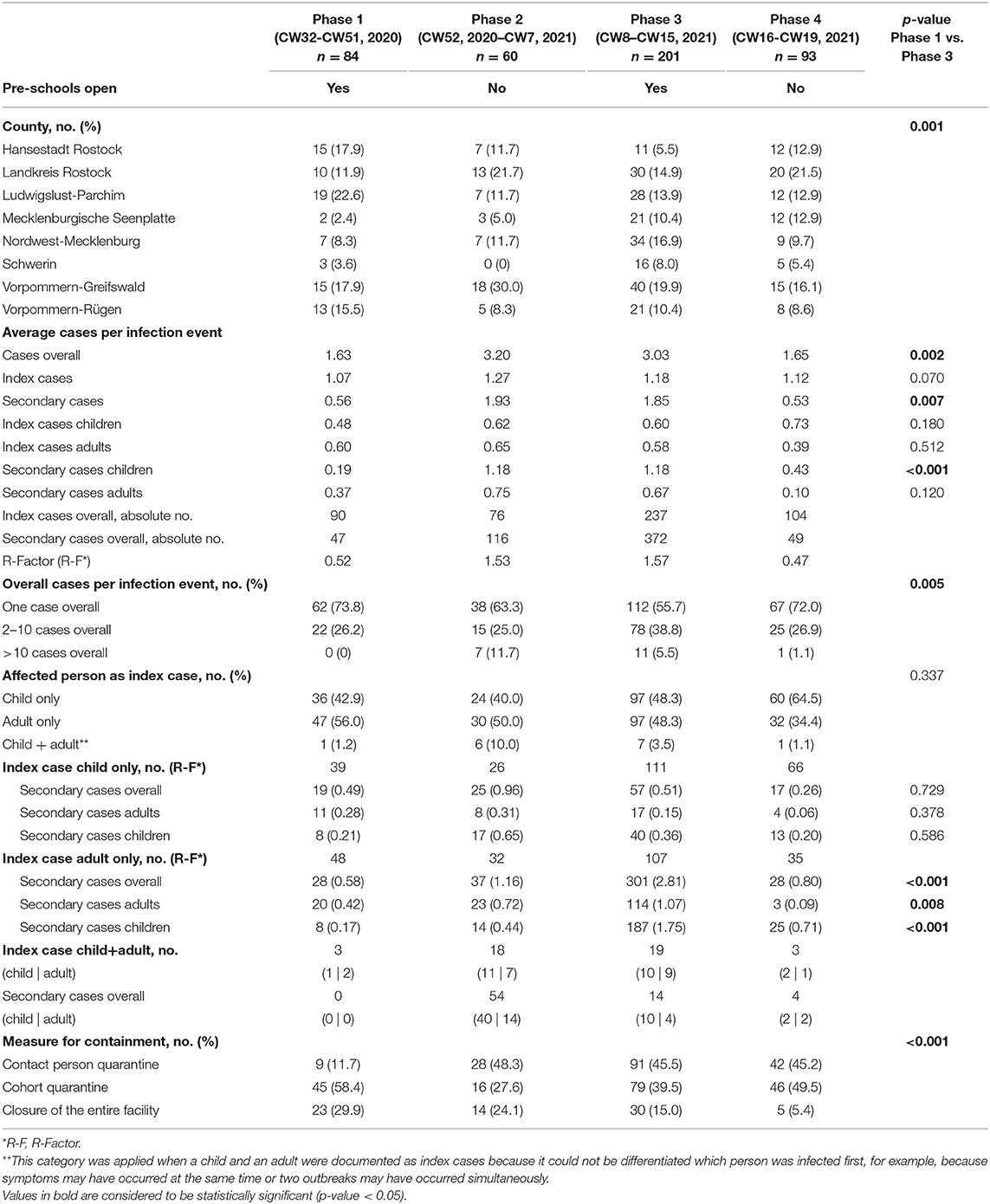
Table 3. Infection incidence in pre-schools in Mecklenburg-Western Pomerania subdivided into phases subdivided by time phases depending on infection control measures in place, N = 438.
In phase 1, n = 84 infection events occurred overall in pre-schools, with n = 90 index cases leading to n = 47 secondary cases (R-F = 0.52). Whereas, in phase 3 n = 201 infection events occurred, whereby n = 237 index cases led to n = 372 secondary cases (R-F = 1.57). Comparing phase 1 to phase 3 (pre-schools were open), significantly more cases overall occurred in phase 3 with significantly more secondary cases (p = 0.002; p = 0.007). When comparing the two phases, there were no significant differences in the distribution between children and adults as index cases. In terms of secondary cases, significantly more children were affected in phase 3 compared to phase 1 (p < 0.001), whereas no differences were seen in adults (p = 0.120).
If the index case was a child, there were no differences in the number of secondary cases and the individuals affected between the two phases. In the first phase infections in children in pre-schools caused an average of 0.49 secondary cases and the corresponding number in the third phase was 0.51 secondary cases.
If the index case was an adult, there were significantly more secondary cases in the 3rd phase compared to the first phase (1st phase, R-F = 0.58; 3rd phase R-F = 2.81; p < 0.001), with more secondary cases among adults (p = 0.008), as well as among children (p < 0.001). Infections in adults in pre-schools caused an average of 0.42 secondary cases in adults and 0.17 secondary cases in children in the first phase, whereas infections in adults in the third phase caused 1.07 secondary cases in adults and 1.75 secondary cases in children. Accordingly, in the third phase the probability of transmission of adults as index case was five times higher compared to children.
Impact of Hygiene Measures in Schools and Pre-schools on Extent of Outbreak Occurrence
To examine the impact of hygiene measures on the magnitude of outbreak occurrence, a linear regression model was set up with the number of total secondary cases per infection event as the dependent variable. The linear regression model is presented in Table 4. The wearing of face masks by children and adults was included in the model, as these hygiene measures differed between schools and pre-schools.
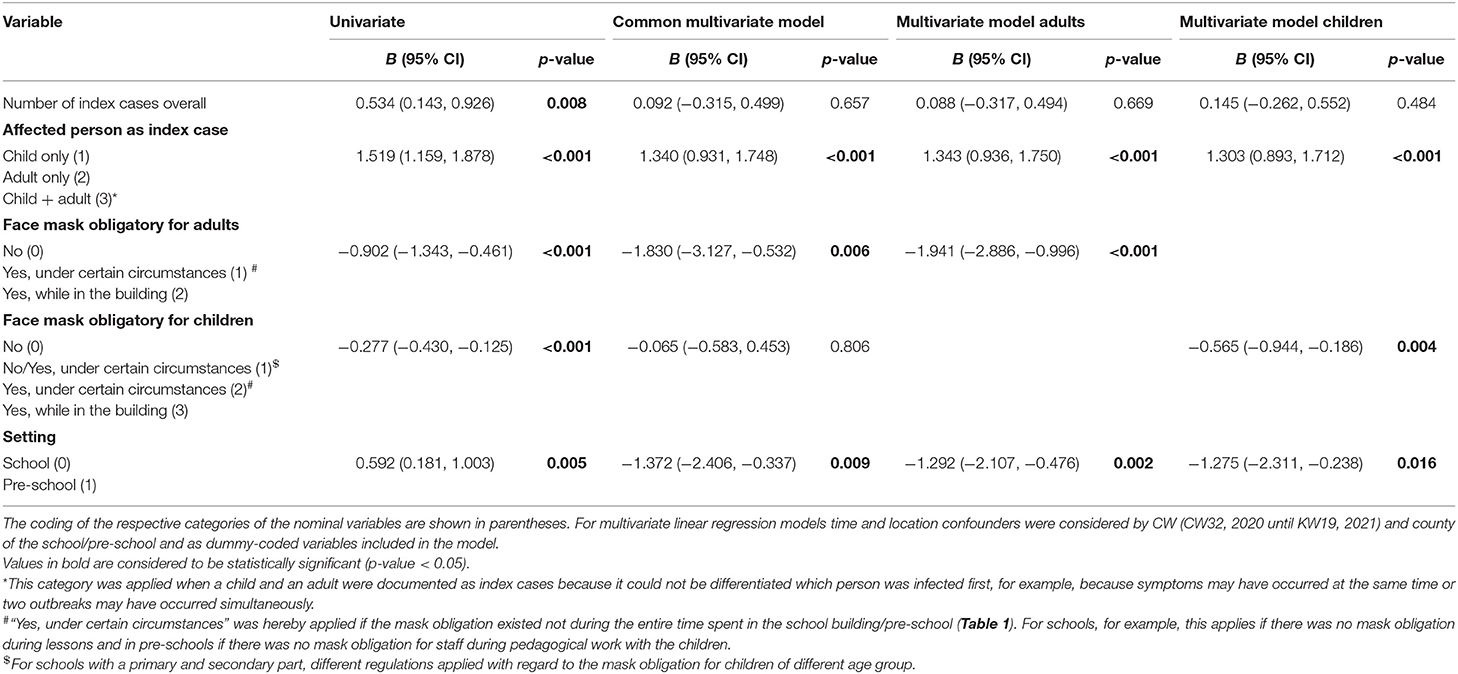
Table 4. Linear regression models with dependent variable number of secondary cases, N = 913.
In univariate analysis, mandatory masking of adults (B = −0.9; p < 0.001) and mandatory masking of children (B = −0.3; p < 0.001) each resulted in a significant reduction in the number of secondary cases. An increasing number of index cases leads to an increase in secondary cases (B = 0.5; p = 0.008). Infections of adults and adults + children as index cases were positively associated with more secondary cases (B = 1.5; p < 0.001) (Table 4).
Due to an existing multicollinearity in the common multivariate regression model between the variables face mask obligation for children and face mask obligation for adults, two further separate regression models were set up (Table 4, Multivariate Model Adults and Multivariate Model Children). Requiring adults and children to wear masks significantly reduced the likelihood of secondary cases (Model Adults: B = −1.9; p < 0.001; Model Children: B = −0.6; p = 0.004) and having an adult or child+adult as index case increased the likelihood of secondary cases (B = 1.3; p < 0.001); Model Adults: R2 = 0.152, corrected R2 = 0.106; Model Children: R2 = 0.145, corrected R2 = 0.099. Cohens f2 = 0.12 (Model Adults) and Cohens f2 = 0.11 (Model Children) represent a small effect size of the multivariate linear regression models.
Discussion
Due to the highly dynamic nature of the COVID-19 pandemic, especially during the winter season in 2020/2021, and due to the simultaneous start of COVID-19 vaccination, there were repeated adjustments of Corona hygiene regulations for schools and pre-schools in Mecklenburg-Western Pomerania, Germany. This prospective observational study aimed to map the dynamic changes in infection events at schools and pre-schools and to highlight factors influencing the extent of an outbreak while taking hygiene measures into account.
To date, several studies provide evidence that schools are not drivers of the pandemic, but may contribute to the reduction of the reproduction number, depending on other hygiene measures in the population (24–26). Consistent with others, our data from schools and pre-schools in Mecklenburg-Western Pomerania suggest that the risk of a COVID-19 outbreak in these institutions increases if the index case is an adult (26).
In schools, outbreaks with secondary cases occurred more frequently in the first phase, whereas outbreaks in pre-schools occurred more frequently in the third phase. A recently published study by Loenenbach et al. provides preliminary evidence that as SARS-CoV-2 variant B.1.1.7 has become more widespread; the susceptibility and infectivity of children and adolescents has increased (18). Similar data are shown in the REACT_r12 study in England (19) and in a study from Scotland (20). The delta variant (B.1.617.2) of SARS-CoV-2 is spreading rapidly worldwide, and as of the end of June 2021, is the dominant virus variant in Germany, accounting for 59% of the total in Germany (27). Initial studies indicate that children were more likely to be infected with the delta variant of the virus than adults (19, 20). An increased risk of severe disease progression was not observed. As with the previous variants, the risk of severe disease progression in children and adolescents without previous illness is very low.
We could observe a comparable trend in pre-schools, but not in schools. However, an increase in infection cases in elementary schools in phase 3 suggests a shift of infections toward the age group <12. It should be emphasized that there were comprehensive adaptations of hygiene concepts in schools e.g., incidence-dependent alternating lessons, as well as an obligation to wear face masks during lessons in the third phase—possibly reducing outbreak events. On the other hand, voluntary point-of-care (PoC) testing has been implemented in schools since 03/21, increasing the likelihood of detecting asymptomatic cases. Mandatory PoC testing at schools did not begin until the end of April 2021, CW17. No mandatory PoC testing was conducted in pre-schools. In our study, we did not see an increase in the number of cases in schools since March 2021. In both schools and pre-schools, symptomatic children and adults had to stay at home. In Mecklenburg-Western Pomerania, both teachers and pedagogical staff were offered vaccinations from the beginning of March 2021. However, the acceptance rate of the offers cannot be verified as there is no consistent vaccination surveillance in Germany.
Interestingly, the strongest predictor of the extent of the outbreak in our study was found to be the teacher/caregiver mask obligation. Furthermore, requiring children to wear masks may also reduce the number of secondary cases. The existing multicollinearity between the variables face mask obligation for children and face mask obligation for adults in the multivariate regression model leads to the fact that not both variables should be considered in one regression model, and even after separation into two regression models, the estimates should be considered with caution since estimates for children may be at least partially explained by adult mask-wearing and vice-versa. Nevertheless, since adults were more often the index case, adult mask-wearing is particularly effective. Of course, children wearing face masks reduces the risk of infection and consequently the number of secondary cases, but mask-wearing is not recommended in young children under 6 years of age, as they cannot use it properly.
When comparing the hygiene measures between schools and pre-schools, an important difference emerges. In pre-schools, masks were not mandatory at any time during the educational work, i.e., the interaction between staff and child. Other hygiene measures were largely comparable between schools and pre-schools. The implementation of hygiene measures following the regulations can only be assumed here. As part of another project, we carried out school inspections, whereby we monitor infection events at schools and the compliance to hygiene regulations. In these inspections we have so far not been able to detect any gross violations (unpublished data). An analysis by Philipps et al. showed that outbreak size in pre-schools and primary schools may be reduced by smaller group sizes and grouping of siblings (28).
It is important to highlight that the temporal subdivision of the phases is simplified and the containment measures were heterogeneous and complex, depending on the incidence of each county, especially in the 3rd phase (school and pre-school opened). Therefore, time and location were included as potential confounders in our model. Another important aspect is, that further to the different age distribution of children in schools and pre-schools, the staff-child interactions are not comparable between these two settings. Therefore, univariate analyses of the infection events were performed separately and in the multivariate regression model the setting (school/pre-school) was considered.
Nevertheless, the presented data on the incidence of infections in pre-schools in the third phase is of concern and should receive more focus in the public debate—especially in light of the fact that new virus mutations may lead to altered transmission and infectiousness in children and adolescents.
In our opinion, a mask requirement for caregivers in pre-schools should be considered. For example, instead of medical masks, colorful fabric masks could be recommended to make children feel more comfortable. The educational work could be impaired by such a measure, yet mouth-nose covering is one effective preventive method to contain the COVID-19 pandemic (29, 30). Given that educational professionals and teaching staff in Germany have been prioritized for vaccination, a reduction in the incidence of infection in schools and pre-schools can be assumed. However, verification of vaccination status is not permissible, so that a mask requirement should be reconsidered.
Limitations of this study are especially the insufficient information on SARS-CoV-2 positive tested persons at schools and pre-schools, such as demographics, medical history, number of contact persons and symptoms since illness onset to further specify the factors influencing the extent of the outbreaks. Furthermore, it must be emphasized that contact persons of infected persons have not been tested consistently, but have often been quarantined based on contact only, so that the number of SARS-CoV-2 positive cases may be underestimated. In particular, children and adolescents are often asymptomatic, so that cases may go undetected. As mentioned above, the temporal breakdown into phases is simplified and based on the guidelines of the state of Mecklenburg-Western Pomerania, Germany. Furthermore, during phase 1 the hygiene measures were partly different at one school, for example, primary school students did not have to wear a mask, whereas secondary school students had to wear a mask e.g., in the corridors and during breaks. This was therefore considered in the multivariate analysis.
With the start of the new school year 2021/2022, children and adolescents will be among the age groups with the lowest vaccination coverage for COVID-19. Therefore, in the absence of strict adherence to hygiene measures, a concentrated spread of COVID-19, including outbreaks, might be expected in these age groups.
In principle, however, it can be assumed that the established hygiene rules (distance, frequent handwashing, wearing a mask) will also protect against new variants of SARS-CoV-2. Due to the possible increased susceptibility of children, these measures must be implemented even more consistently, especially in the age group <12 years. A focus should therefore be placed on effective protection concepts in pre-school and elementary school settings and in after-school care centers.
In conclusion, the dynamics of infection events differ between schools and pre-schools over time. Considering the respective applicable hygiene measures in schools and pre-schools in the study region, as well as temporal and spatial factors, the present study indicates that outbreak events at pre-schools and schools are particularly potentiated when an adult is the index case. Thus, an obligation for adults to wear face masks might be an important measure to contain outbreaks, particularly in pre-schools during educational work.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
MS, PL, WH, ER, and AK: conceptualization. MS, PL, ME, and AK: methodology. MS, ME, PL, WH, and AK: investigation. SB and ML: resources. MS and AK: writing—original draft preparation. MS, PL, ME, WH, and ER: writing—review and editing. MS, WH, AK, and ER: funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This study was financially supported by the Ministry of Economic Affairs, Labor and Health Mecklenburg-Western Pomerania.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Davies NG, Klepac P, Liu Y, Prem K, Jit M, Eggo RM. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat Med. (2020) 26:1205–11. doi: 10.1038/s41591-020-0962-9
2. Goldstein E, Lipsitch M, Cevik M. On the effect of age on the transmission of SARS-CoV-2 in households, schools, and the community. J Infect Dis. (2021) 223:362–9. doi: 10.1093/infdis/jiaa691
3. Viner RM, Mytton OT, Bonell C, Melendez-Torres GJ, Ward J, Hudson L, et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: a systematic review and meta-analysis. JAMA Pediatr. (2021) 175:143–56. doi: 10.1001/jamapediatrics.2020.4573
4. Gudbjartsson DF, Helgason A, Jonsson H, Magnusson OT, Melsted P, Norddahl GL, et al. Spread of SARS-CoV-2 in the icelandic population. N Engl J Med. (2020) 382:2302–15. doi: 10.1056/NEJMoa2006100
5. Götzinger F, Santiago-García B, Noguera-Julián A, Lanaspa M, Lancella L, Calò Carducci FI, et al. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Health. (2020) 4:653–61. doi: 10.1016/S2352-4642(20)30177-2
6. Laws RL, Chancey RJ, Rabold EM, Chu VT, Lewis NM, Fajans M, et al. Symptoms and transmission of SARS-CoV-2 among children - Utah and Wisconsin, March-May 2020. Pediatrics. (2021) 147:268. doi: 10.1542/peds.2020-027268
7. Bhuiyan MU, Stiboy E, Hassan MZ, Chan M, Islam MS, Haider N, et al. Epidemiology of COVID-19 infection in young children under five years: a systematic review and meta-analysis. Vaccine. (2021) 39:667–77. doi: 10.1016/j.vaccine.2020.11.078
8. Ismail SA, Saliba V, Lopez Bernal J, Ramsay ME, Ladhani SN. SARS-CoV-2 infection and transmission in educational settings: a prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect Dis. (2021) 21:344–53. doi: 10.1016/S1473-3099(20)30882-3
9. Sombetzki MHW, Lücker P, Littmann M, Bock S, Reisinger EC. Kein erhöhtes SARS-CoV-2-Infektionsrisiko in Schulen. Schulöffnung in Mecklenburg-Vorpommern unter Pandemiebedingungen. Rostock: ÄRZTEBLATT MECKLENBURG-VORPOMMERN (2021).
10. Brauner JM, Mindermann S, Sharma M, Johnston D, Salvatier J, Gavenčiak T, et al. Inferring the effectiveness of government interventions against COVID-19. Science. (2021) 371:eabd9338. doi: 10.1126/science.abd9338
11. Baier L, Kühl N, Schöffer J, Satzger G. Utilizing Concept Drift for Measuring the Effectiveness of Policy Interventions: The Case of the COVID-19 Pandemic. Karlsruhe: Karlsruher Institut für Technologie (KIT) (2020).
12. Viner RM, Russell SJ, Croker H, Packer J, Ward J, Stansfield C, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health. (2020) 4:397–404. doi: 10.1016/S2352-4642(20)30095-X
13. Patrick SW, Henkhaus LE, Zickafoose JS, Lovell K, Halvorson A, Loch S, et al. Well-being of parents and children during the COVID-19 pandemic: a national survey. Pediatrics. (2020) 146:824. doi: 10.1542/peds.2020-016824
14. Ravens-Sieberer U, Kaman A, Otto C, Adedeji A, Devine J, Erhart M, et al. Mental health and quality of life in children and adolescents during the COVID-19 pandemic-results of the copsy study. Dtsch Arztebl Int. (2020) 117:828–9. doi: 10.3238/arztebl.2020.0828
15. Ehrhardt J, Ekinci A, Krehl H, Meincke M, Finci I, Klein J, et al. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020. Baden-Württemberg, Germany. Euro Surveill. (2020) 25:2001587. doi: 10.2807/1560-7917.ES.2020.25.36.2001587
16. Willeit P, Krause R, Lamprecht B, Berghold A, Hanson B, Stelzl E, et al. Prevalence of RT-qPCR-detected SARS-CoV-2 infection at schools: first results from the Austrian School-SARS-CoV-2 prospective cohort study. Lancet Regional Health Europe. (2021) 5:86. doi: 10.1016/j.lanepe.2021.100086
17. Otte Im Kampe E, Lehfeld AS, Buda S, Buchholz U, Haas W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Euro Surveill. (2020) 25:1645. doi: 10.2807/1560-7917.ES.2020.25.38.2001645
18. Loenenbach A, Markus I, Lehfeld AS, An der Heiden M, Haas W, Kiegele M, et al. SARS-CoV-2 variant B.1.1.7 susceptibility and infectiousness of children and adults deduced from investigations of childcare centre outbreaks, Germany, 2021. Euro Surveill. (2021) 26:433. doi: 10.2807/1560-7917.ES.2021.26.21.2100433
19. Riley S, Wang H, Eales O, Haw D, Walters CE, Ainslie KEC, et al. REACT-1 round 12 report: resurgence of SARS-CoV-2 infections in England associated with increased frequency of the Delta variant. medRxiv. doi: 10.1101/2021.06.17.21259103
20. Sheikh A, McMenamin J, Taylor B, Robertson C. SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness. Lancet (London, England). (2021) 397:2461–2. doi: 10.1016/S0140-6736(21)01358-1
21. Danilo Buonsenso FEP, Munblit D, Mcfarland S, Simpson F. Clinical characteristics, activity levels and mental health problems in children with long COVID: a survey of 510 children. Preprints. (2021) 2021030271 doi: 10.20944/preprints202103.0271.v1
22. Regierungsportal, Mecklenburg-Vorpommern, Ministerium für, Bildung, Wissenschaft und, Kultur,. Coronavirus. Available online at: https://www.regierung-mv.de/Landesregierung/bm/Blickpunkte/Coronavirus/Coronavirus-%E2%80%93-Informationen-f%C3%BCr-schule/ (accessed June 30, 2021).
23. Regierungsportal, Mecklenburg-Vorpommern, Ministerium für, Soziales,. Integration und Gleichstellung, Informationen zu Corona, Informationen zur Kindertagesförderung. Available online at: https://www.regierung-mv.de/Landesregierung/sm/Service/Corona/Kindertagesf%C3%B6rderung/ (accessed June 30, 2021).
24. Rozhnova G, van Dorp CH, Bruijning-Verhagen P, Bootsma MCJ, van de Wijgert J, Bonten MJM, et al. Model-based evaluation of school- and non-school-related measures to control the COVID-19 pandemic. Nat Commun. (2021) 12:1614. doi: 10.1038/s41467-021-21899-6
25. Brandal LT, Ofitserova TS, Meijerink H, Rykkvin R, Lund HM, Hungnes O, et al. Minimal transmission of SARS-CoV-2 from paediatric COVID-19 cases in primary schools, Norway, August to November 2020. Euro Surveill. (2021) 26:2011. doi: 10.2807/1560-7917.ES.2020.26.1.2002011
26. Gandini S, Rainisio M, Iannuzzo ML, Bellerba F, Cecconi F, Scorrano L, et al. cross-sectional and prospective cohort study of the role of schools in the SARS-CoV-2 second wave in Italy. Lancet Regional Health Eur. (2021) 5:100092. doi: 10.1016/j.lanepe.2021.100092
27. Robert Koch Institut (RKI). Bericht zu Virusvarianten von SARS-CoV-2 in Deutschland Stand. Berlin: Robert Koch Institut (RKI) (2021).
28. Phillips B, Browne DT, Anand M, Bauch CT. Model-based projections for COVID-19 outbreak size and student-days lost to closure in Ontario childcare centres and primary schools. Sci Rep. (2021) 11:6402. doi: 10.1038/s41598-021-85302-6
29. Leung NHL, Chu DKW, Shiu EYC, Chan KH, McDevitt JJ, Hau BJP, et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. (2020) 26:676–80. doi: 10.1038/s41591-020-0843-2
Keywords: schools and pre-schools, routine surveillance data, control measures, multivariate regression analysis, SARS-CoV-2 infections
Citation: Sombetzki M, Lücker P, Ehmke M, Bock S, Littmann M, Reisinger EC, Hoffmann W and Kästner A (2021) Impact of Changes in Infection Control Measures on the Dynamics of COVID-19 Infections in Schools and Pre-schools. Front. Public Health 9:780039. doi: 10.3389/fpubh.2021.780039
Received: 20 September 2021; Accepted: 23 November 2021;
Published: 20 December 2021.
Edited by:
Guodong Ding, Shanghai Children's Hospital, ChinaReviewed by:
Mohammad Alseaidan, Ministry of Health, KuwaitArmelia Sari Widyarman, Trisakti University, Indonesia
Copyright © 2021 Sombetzki, Lücker, Ehmke, Bock, Littmann, Reisinger, Hoffmann and Kästner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anika Kästner, anika.kaestner@med.uni-greifswald.de