 Richelle L. Clifton
Richelle L. Clifton Tamika C. B. Zapolski
Tamika C. B. Zapolski- 1Department of Pediatrics, University of Washington School of Medicine, Seattle, WA, United States
- 2Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, United States
Introduction: Racial microaggressions are associated with multiple negative health outcomes, including increased distress, anxiety, and substance use. One factor that may impact this relationship and has received considerable attention in the literature is racial identity. Moreover, recent studies have employed the use of racial identity profiles to provide a more nuanced understanding of racial identity's impact on health outcomes. However, to date, few studies have explored the existence of racial identity profiles among adolescents or variability in risk pathways between racial microaggressions and health outcomes based on racial identity profiles among adolescents.
Methods: For the current study, 48 Black adolescents (79.2% girls; Mage= 17.13) completed measures of racial identity at baseline and daily diary measures of racial microaggressions, depression, anxiety, aggression, and substance use for 14 days.
Results: Four racial identity profiles were identified (labeled race-focused, undifferentiated, integrationist, and multiculturalist), with evidence to suggest reduced risk for aggression among youth within the race-focused profile but that these youth remain at risk for depression and cannabis use.
Discussion: The current study helps to inform the field of adolescent health, highlighting several areas for future research and intervention for mental and behavioral health outcomes among Black adolescents experiencing racial microaggressions.
1. Introduction
As Black children enter adolescence (i.e., beginning around age 10), their experiences of racial discrimination increase (1, 2). In a study conducted among Black adolescents aged 14–18, 97% of participants reported at least one instance of racial discrimination in the past two weeks, with a daily average of 2.5 discriminatory events experienced every day (3). Moreover, racial microaggressions, which are commonplace verbal, behavioral, or environmental slights and insults toward people of color (4), are a more covert form of racial discrimination that have been found to occur more frequently than overt forms of racial discrimination (5). Racial microaggressions have been associated with a number of negative psychological consequences among racial/ethnic minority youth, including elevated depressive and somatic symptoms (6), poorer sleep quality and shorter sleep duration the following day (7), and past-year cigarette use and alcohol-related consequences in the last three months (8). Further, studies conducted specifically among Black adolescents have also demonstrated that racial microaggressions are associated with increased externalizing (9) and depression symptoms (10).
Given the impact of racial microaggressions on negative health outcomes among Black adolescents, it is critical to examine factors that might impact this risk pathway. Of note, a body of literature has developed, identifying protective factors that could buffer against these stressors and mitigate risk for associated negative physical, mental, and behavioral health consequences (11, 12). Within this literature, one factor that has received a considerable amount of attention is racial identity, as it has been shown to not only mitigate risk for health outcomes as a consequence of racial discrimination (13, 14) but also has direct promotive effects on positive mental and behavioral health outcomes among Black individuals (15, 16).
However, there has also been a separate body of research that has documented that there are some aspects of racial identity that may heighten risk for negative health outcomes [e.g. (17),]. For instance, in a study among a sample of 103 Black adolescents, researchers found that different components of racial identity differentially moderated associations between experiences of racial discrimination and daily depressive symptoms. Specifically, neither racial centrality (i.e., the importance of one's race to their self-concept) nor private regard (i.e., how an individual views their race) moderated the same-day or lagged associations between daily racial discrimination experiences and daily depressive symptoms. However, low public regard (i.e., believing that others view your race negatively) exacerbated the lagged day relation between daily racial discrimination experiences and daily depressive symptoms (18).
Given the differential impact of racial identity components on health outcomes, researchers have called to examine profiles of racial identity among Black individuals (19–21). While it is useful and informative to look at particular components of racial identity, a profile approach allows for the analysis of patterns of racial identity, as well as how racial identity might look on the individual level with many interacting patterns. Several different models of Black racial identity have been proposed over the past several decades. One of the most recent multidimensional models of racial identity was developed by Sellers et al. (12) who proposed the Multidimensional Model of Racial Identity (MMRI). The MMRI proposes four distinct dimensions of racial identity: racial salience, racial centrality, racial regard (includes two sub-dimensions: private and public regard), and racial ideology (includes four subdimensions: assimilationist, humanist, oppressed minority, and nationalist) (12). The measure that operationalizes the MMRI and allows for the creation of these profiles is the Multidimensional Inventory of Black Identity [MIBI; (22)].
Since the development of the MIBI, an emerging body of research has been published examining racial identity profiles among Black college students and adults utilizing all seven subscales of the MIBI measure (23–28). Across the studies, different numbers of profiles have been produced, with two studies identifying three profiles (27, 28), three studies identifying four racial identity profiles (23–25), and one study identifying five profiles (26). The methodology utilized to create profiles or clusters of racial identity varies across studies, but many researchers prefer utilizing latent class or latent profile analysis, because these methods have strong theoretical bases and have the ability to deal with different types of data (e.g., combinations of categorical, numerical, and continuous data) and missing data in a comprehensive manner (29).
Commonly identified profiles in these studies include an undifferentiated profile (i.e., individuals who might be described as not having a race-based worldview), a race-focused profile (i.e., individuals who hold race central to their identity, feel positive about being Black, and believe that others hold more negative beliefs about Black Americans), a multiculturalist profile (i.e., individuals focused on the commonalities among all humans, Americans, and marginalized groups), and an integrationist profile (i.e., individuals with goals of blending with the mainstream and a focus on shared human qualities rather than perceiving race to be a core self-concept).
Previous studies have examined the direct effect of racial identity profiles (based on the full MIBI measure) among Black adults on psychological and health outcomes. Among other findings, researchers have found that a profile similar to the integrationist profile is associated with increased imposter phenomenon (24), a profile similar to the undifferentiated profile was associated with increased hopelessness compared to other profiles (26), and a multiculturalist profile is associated with increased cannabis use and depressive symptoms (25).
Further, researchers have examined the impact of racial identity profiles on the relationship between racial discrimination and various psychological and health outcomes among Black adults. Researchers have found that the integrationist profile introduced the most risk in the relationship between racial discrimination and depressive symptoms (23), the race-focused profile exacerbated the negative impact of racial discrimination on obsessive-compulsive distress one year later but the multiculturalist profile and humanist profile buffered this risk (28), and no profile differences in the relationship between racial discrimination and imposter phenomenon (24). Further, one study found that for individuals in the race-focused profile and undifferentiated profiles, racial discrimination led to increased alcohol and cannabis use but for individuals in the integrationist and multiculturalist profile, racial discrimination had a significant negative relationship with cannabis use (25). Although important information has been gained from these studies, they have only been conducted among adult samples limiting our understanding of racial identity profiles on health outcomes among Black youth.
There have also been methodological advancements in this body of work that warrant further investigation. Intensive longitudinal studies have been utilized to examine how racial identity influences daily risk and protective processes [e.g., (30)]. Intensive longitudinal study designs are important, as they increase the precision with which rapidly changing processes are characterized, minimize retrospection bias, and strengthen causal inference by establishing temporal precedence (31). Importantly, time-intensive designs allow researchers to simultaneously account for within- and between-person sources of variation in data.
There is a small body of literature examining the moderating role of racial identity variables in the relationship between racial discrimination and health outcomes using daily diary methodology. Burrow and Ong (32) conducted a 2-week daily diary study among 174 Black doctoral students and graduates, examining the moderating role of racial identity in the relationship between daily racial discrimination and daily psychological distress (depression, anxiety, negative affect). Racial identity was assessed at baseline using the MIBI and discrimination and psychological distress every day of their 2-week protocol. Results indicated that racial centrality exacerbated the effects of daily racial discrimination on negative affect and depression, and neither private nor public regard moderated this association (32). Further, Hoggard et al. (33) conducted a 20-day daily diary study among 225 Black college students, examining the moderating role of racial identity in the relationship between racial (and non-racial) stressors and depressive symptoms. Racial identity was assessed once during an annual survey using the MIBI and measures examining racial stressors and depressive symptoms were assessed every day for 20 days. The researchers found that racial identity variables (racial centrality, private regard, public regard) did not moderate the same-day relationship between racial stress and depression. However, high racial centrality exacerbated the impact of racial stressors and depressive symptoms over time (slope), and high public regard and low public regard buffered the impact of racial stressors on depressive symptoms over time (slope) (33). Finally, Seaton and Iida (18) conducted a 2-week daily diary study among 103 Black adolescents, examining the moderating role of daily racial identity in the relationship between daily racial discrimination and daily depressive symptoms. The researchers measured all variables on each day of their 2-week protocol. Findings indicated that neither racial centrality nor private regard moderated the same-day or lagged associations between daily racial discrimination experiences and daily depressive symptoms. However, when Black youth experienced lower levels of public regard compared to their average levels, previous-day racial discrimination experiences were associated with an increase in depressive symptoms (18). While these studies have made an important contribution to the racial identity literature, no studies have examined the moderating role of racial identity profiles in the relationship between daily racial microaggressions and health outcomes.
The aims of the current study were to explore the existence of racial identity profiles among Black adolescents, and to explore variability in the relationship between daily experiences of racial microaggressions and health outcomes based on racial identity profiles identified among Black adolescents. We hypothesized that, based on the existing literature, four racial identity profiles would emerge, similar to the profiles commonly found in previous studies [i.e., (23–28)]. We also hypothesized that those racial identity profiles characterized by a high connection to one's race, positive views of one's race, and beliefs that others view one's race positively would be protective against negative health outcomes as a consequence of racial microaggressions. Conversely, we hypothesized that profiles characterized by a low connection to one's race, negative views of one's race, and beliefs that others view one's race negatively would elevate risk. These hypotheses were based on a body of literature documenting the protective nature of a strong, positive connection to one's race against racial discrimination [e.g., (34)] and research documenting the exacerbating impact of low public regard on the relationship between racism and racism-related stress [e.g., (35)].
2. Materials and methods
2.1. Participants
Participants were African American/Black adolescents ages 10–19 recruited from locations in and around a large mid-western city. Participants were recruited through flyering (online and in person) and in-person recruitment efforts utilizing verbal advertisement scripts. Recruitment locations included local schools, after-school programs, and youth-serving organizations. Additionally, participants were recruited through unpaid social media advertisements. Eligible participants were those who had a cell phone for exclusive personal use with SMS capabilities, informed parental consent (for those under 18), and active youth assent/consent.
2.2. Procedures
Following institutional review board approval, eligible participants completed assent (or consent for those over 18) procedures. After assent/consent was obtained, participants were oriented to the text-message protocol and completed self-report baseline measures. Participants who completed the orientation and took the baseline survey earned a $10 incentive. Participants were paid an additional $10 to offset the costs of SMS messaging and data on their personal phones.
The daily diary protocol began two days after completion of the baseline survey and lasted for 14 consecutive days. Each day of the protocol, participants received an SMS prompt at 3:00 pm with a link to the daily survey. Participants could initiate the day's survey until 11:59 pm local time, after which time entries were no longer recorded. The initial prompt indicated that questions referred to their experiences with racial microaggressions, mood, and health behavior on the previous day (i.e., “These questions are about yesterday from the time you woke up until the time you went to sleep”). Participants were also delivered a follow-up reminder prompt via SMS at 7:00 pm local time. Participants were awarded $2 per daily survey and a $5 bonus for completing 6 out of 7 surveys in a week. Participants who completed more than 85% (at least 12) of surveys received an additional $10. The maximum compensation for participation was $68 per participant.
2.3. Baseline measures
2.3.1. Demographics
During the baseline survey, participants were asked about demographics including their age and gender. They were also asked for the highest level of education that their parent(s)/guardian(s) had completed. Options included some high school, high school degree or GED, technical or trade school degree/certificate, some college or associate degree, 4-year college degree, advanced degree (i.e., Master's, Ph.D., JD, MD), and other/unknown.
2.3.2. Racial identity
Racial identity was measured using the Multidimensional Inventory of Black Identity-Teen Version [MIBI-T; (36)]. Three domains measured by seven subscales of the MIBI were utilized. These seven subscales were: Racial Centrality, Private Regard, Public Regard, Assimilationist Ideology, Humanist Ideology, Oppressed Minority Ideology, and Nationalist Ideology. Items included statements like, “I have a strong sense of belonging to other Black people” and “Blacks should think of themselves as individuals, not as Black.” Responses were rated on a 5-point Likert scale with potential responses ranging from 1 (strongly disagree) to 5 (strongly agree). A total score was calculated from a sum of all item scores for each subscale. For the current study, the internal consistency for each subscale was poor to acceptable (racial centrality = 0.464, private regard = 0.674, public regard = 0.813, assimilationist = 0.780, humanist = 0.725, oppressed minority = 0.606, nationalist = 0.641). These internal consistency scores are comparable to what has been found in some previous studies using the MIBI, with scores ranging from.55 to.85 (23, 24, 37).
2.4. Daily measures
2.4.1. Racial microaggressions
Racial Microaggressions were measured using the Revised 28-Item Racial and Ethnic Microaggressions Scale, checklist version [REMS-Checklist; (38, 39)]. The measure consists of 28 items, including items like, “I was ignored at school or at work because of my race” and “someone assumed that I would not be intelligent because of my race.” Participants were asked to indicate whether or not they experienced each of the 28 events described in the scale on the previous day. Response options were on a yes/no scale, and scores ranged from 0 (I did not experience this event) to 1 (I experienced this event). For the current study, a total score was created from the sum of all item scores. The internal consistency for this measure was good (Cronbach's alpha = 0.899).
2.4.2. Symptoms of depression
Symptoms of depression were measured using the Patient Health Questionnaire, 8-item [PHQ-8; (40)]. This measure was modified to ask about symptoms on the day prior. Participants were asked how often during the day they were bothered by particular symptoms of depression, with items including statements like “little interest or pleasure in doing things” and “feeling down, depressed, or hopeless.” Response options were a 4-point Likert scale, ranging from 0 (not at all) to 4 (nearly all day). A total score was calculated from a sum of all item scores. The internal consistency for this measure was good (Cronbach's alpha = 0.895).
2.4.3. Symptoms of anxiety
Symptoms of depression were measured using the Generalized Anxiety Disorder scale, 7-item [GAD-7; (41)]. This measure was modified to ask about symptoms on the day prior. Participants were asked how often during the day they were bothered by particular symptoms of anxiety, with items including statements like “feeling nervous, anxious, or on edge” and “not being able to stop or control worrying.” Response options were a 4-point Likert scale, ranging from 0 (not at all) to 4 (nearly all day). A total score was calculated from a sum of all item scores. The internal consistency for this measure was good (Cronbach's alpha = 0.891).
2.4.4. Aggression
Aggression was measured using the Aggression Experience Sampler [Aggression-ES; (42)] which assesses physical, indirect, reactive, and proactive aggression. The measure consists of 12 items designed specifically for EMA research. Questions were used to assess aggression on the day prior, with items including statements like, yesterday I “lost my temper” or “physically attacked someone.” Response options were a 5-point Likert scale, ranging from 0 (not at all true) to 4 (extremely true). A total score was calculated from a sum of all item scores. The internal consistency for this measure was good (Cronbach's alpha = 0.873).
2.4.5. Substance Use
Substance use was assessed using 3 questions regarding whether or not participants used cannabis, alcohol, and/or tobacco on the day prior (yes/no). Due to low endorsement of alcohol and tobacco among participants, only the cannabis use outcome is reported in the current study.
2.5. Data analysis
Preliminary analyses examined scale reliability, missing data, and descriptive statistics. There was no missing data on baseline measures. Person-mean imputation (MI) was used to replace partially missing daily diary data. Fully missing diary occasions were accounted for with maximum likelihood (ML) estimation using the MIXED command in SPSS. A combination of MI and ML procedures for missingness in intensive longitudinal studies has been recommended by researchers, particularly since ML methods do not accurately account for partial missingness (43).
To examine racial identity profiles, a latent profile analysis (LPA) was performed in Mplus, with a robust maximum likelihood (MLR) estimator used to estimate the optimal number of profiles. We examined a range of one to six potential profiles based on previous studies utilizing LPA with the MIBI-T (24). To determine the best number of profiles, we relied on the following criteria: Akaike's Information Criterion [AIC; (44)], the Constant AIC (CAIC), the Bayesian Information Criterion [BIC; (45)], the sample-size adjusted BIC (SSA-BIC), and the Bootstrapped Likelihood Ratio Test [BLRT; (46, 47)], as suggested by previous research (48). Entropy was also assessed. The optimal model was chosen based on goodness-of-fit and parsimony as well as theoretical expectations. After the number of profiles was determined, the standardized means (indexed by z scores) of each racial identity variable was used to describe and label each profile.
To examine whether the impact of racial microaggressions on outcomes of interest varied within racial identity profiles, stratified multilevel models (MLM) were examined using SPSS version 29. For continuous outcomes (depression, anxiety, and aggression), two-level (days within persons) linear multilevel models were run, examining the concurrent relationships between daily experiences of racial microaggressions and outcomes. For substance use, a two-level (days within persons) logistic model was used to examine the concurrent relationship between microaggressions and substance use (no use vs. use).
For all models, daily racial microaggressions were person-mean centered and individuals’ mean level of microaggressions were grand-mean centered; these variables were simultaneously entered into the models (49). Gender, age, and parental education were included as covariates. These variables were included as covariates because all three are associated with differences in mental health and substance use outcomes among adolescents [e.g., (50–55)].
3. Results
The final sample size included 48 participants who mostly identified as girls (79.2%) with a smaller minority of individuals identifying as boys (20.8%). For the current study, gender was examined as a binary category given that all participants indicated identifying with one of these two categories (boy/girl). However, it is important to note that some individuals also identified with additional gender categories, including non-binary and/or other gender (n = 3; 6.3%). There was some diversity in the highest level of reported parent education (high school or less = 6.25%, some college = 25.0%, 4-year college degree = 37.5%, advanced college degree = 31.25%). The average age of participants was 17.13 (SD = 1.86).
Regarding study variables, all participants reported at least one instance of experiencing a racial microaggression across the 14-day protocol, with an average of 5.56 reported experiences of racial microaggressions per day across 28 daily items. Participants also had mild average daily levels of anxiety (M = 3.90, SD = 4.41) and depression (M = 4.55, SD = 5.01) with the average daily score on the aggression measure being 2.80 (SD = 5.56). Cannabis use was reported by 14.6% of participants during the 14-day protocol. An association between daily racial microaggressions and aggression (estimate = 0.345, SE = 0.138, t = 2.495, p = 0.016) and cannabis use [OR = 1.524, 95% CI (0.103, 0.740), p = 0.010] was observed, with nonsignificant associations found for anxiety and depression.
3.1. Profile identification
Using the data from the seven subscales of the MIBI, of the six models estimated, the four-profile model was determined to be the most appropriate solution. It had the lowest Akaike information criterion (AIC = 1,463.402), and the Bootstrapped likelihood ratio test (BLRT) had a significant p-value, suggesting that the four-profile solution was better fitting compared to the three-profile solution (value = 27.949, p = 0.0400). The four-profile model also fits the theoretical expectations for this study. See Table 1 for a summary of all fit statistics for all six latent class models.
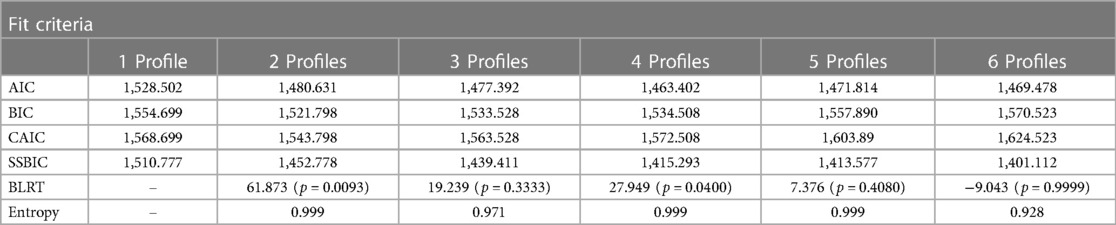
Table 1. Measures of model Fit for latent profile analysis.
Standardized means (z scores) of each racial identity variable were taken together with theoretical expectations, and used to describe and label the profiles (see Figure 1). The first and largest profile was labeled Race-Focused (n = 37; 77% of sample; 16.2% boys, 83.8% girls). This profile was characterized by scores near/slightly above the sample mean on the subscales measuring centrality, private regard, oppressed minority ideology and nationalist ideology. This profile also had scores slightly below the mean on the subscales measuring public regard, assimilationist and humanist ideologies. These individuals might be described as being reasonably connected to Black culture and are aware of racism specific to Black people.
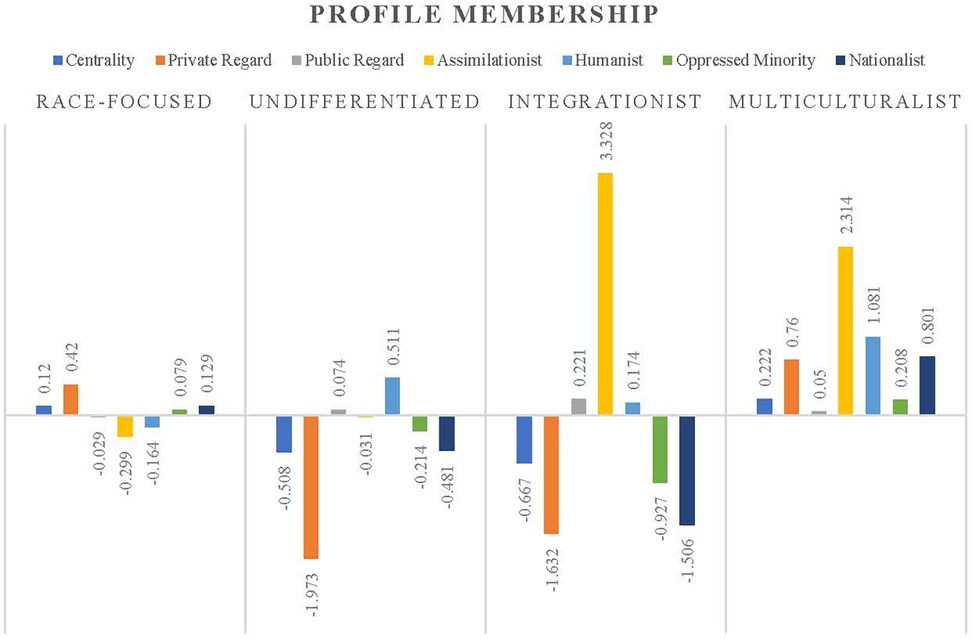
Figure 1. MIBI-teen subscale Z-scores illustrating profile membership.
Three other profiles were also identified within the dataset, however cell size was considerably smaller than the race-focused profile. The second profile was labeled Undifferentiated (n = 7; 14.6% of sample; 28.6% boys, 71.4% girls) and had scores below the mean (∼0.5 SD below the mean) on subscales measuring centrality and nationalist ideology, and scores well below the mean (∼2 SD below the mean) on a subscale measuring private regard. Individuals in this profile had scores above the mean (∼0.5 SD above the mean) on a subscale measuring humanist ideology. This profile also had scores near the mean on the public regard, assimilationist ideology, and oppressed minority subscales. Thus, this group does not hold race central to their identity and also tends to place more of an emphasis on shared human qualities, feeling negatively in general about being Black themself. This group might be described as trying not to have a strong race-based worldview.
The third profile was labeled Integrationist (n = 2; 4.2% of sample; 100% boys) and was characterized by low standardized scores (∼0.25–2 SD below the mean) on centrality, private regard, oppressed minority ideology and nationalist ideology subscales and scores near/slightly above the mean on public regard humanist subscales. These individuals had scores well above the mean (∼3 SD above the mean) on the assimilationist ideology subscale. Thus, this group tends to not see race as central to their identity, focusing more on shared qualities between many different groups (i.e., minorities, humans), and placing an emphasis on Black people integrating/assimilating into mainstream American culture.
The fourth profile was labeled Multiculturalist (n = 2; 4.2% of sample; 100% girls) and had scores above the mean on all subscales. Most notably, this profile was made up of individuals above the mean (∼0.25–2 SD above the mean) on subscales measuring private regard, assimilationist ideology, humanist ideology, and nationalist ideology. Thus, this group generally feels positively about being Black, believes others hold positive beliefs about Black people, and while believing in the uniqueness of Black people, believes that all Americans and humans in general are similar.
3.2. Variability in the relationship between racial microaggressions and anxiety, depression and aggression by racial identity profile
Mixed-effects (i.e., multilevel) models were used to examine the effect of the interaction of racial identity profiles and the between- and within-person effects of daily experiences of racial microaggressions on anxiety, depression, and aggression. These models also controlled for age, gender, and parental education (at the person-level). Results of the omnibus test suggested that the relationship between daily racial microaggressions and anxiety differed significantly by racial identity profile membership at both the within- [F(3,1600.80)= 3.76, p = 0.010] and between-person [F(3,1474.12)= 4.02, p = 0.007] levels. Similar results were found for depression outcomes (within-person: F(3,39.67)= 3.28, p = 0.031; between-person: F(3,30.44)3.35, p = 0.032). For aggression outcomes, results suggested that the relationship between daily racial microaggressions and aggression differed significantly by racial identity profile membership at the between-person [F(3,1078.78)= 3.38, p = 0.018] but not the within-person level [F(3,1013.04) = 1.48, p = 0.219]. Given these results, stratified analyses were conducted to further explore the relationship between racial microaggressions and these outcomes within each racial identity profile. We are reporting the findings from the stratified models, but acknowledge that due to the extremely small cell sizes for most profiles, caution should be taken with interpretation of findings.
For individuals in the race-focused profile, there were no significant effects of racial microaggressions on anxiety or aggression at the between- or within-person level. However, there was a significant positive within-person effect of racial microaggressions on depression for individuals in the race-focused profile (effect = 0.332, SE = 0.151, t = 2.202, p = 0.030).
For individuals in the undifferentiated profile, there were no significant effects of racial microaggressions on aggression. However, there was a significant positive between-person effect of racial microaggressions on anxiety (effect = .872, SE = 0.307, t = 2.837, p = 0.015) and depression (effect = 1.364, SE = 0.430, t = 3.173, p = 0.010). Additionally, there was a significant negative (buffering) within-person effect of racial microaggressions on depression for individuals in the undifferentiated profile (effect = −1.375, SE = 0.459, t = −2.994, p = 0.011).
For individuals in the integrationist profile, there were no significant effects of racial microaggressions on depression. However, there was a significant positive between-person effect of racial microaggressions on anxiety (effect = 1.211, SE = 0.312, t = 3.881, p = 0.002) and aggression (effect = 2.151, SE = 0.782, t = 2.750, p = 0.047). Additionally, there was a significant negative (buffering) within-person effect of racial microaggressions on anxiety for individuals in the integrationist profile (effect = −1.079, SE = 0.406, t = −2.658, p = 0.024).
Finally, for individuals in the multiculturalist profile, there were significant between- and within-person effects or racial microaggressions on anxiety, depression, and aggression outcomes. For anxiety, the between-person effect was negative (buffering; effect = 2.948, SE = 0.627, t = −4.071, p = 0.019) and the within-person effect was positive (effect = 3.228, SE = 0.644. t = 5.016, p = 0.014). For depression, the pattern was similar, with the between-person effect being negative (buffering; effect = −1.651, SE = 0.559, t = −2.955, p = 0.030) and within-person effect being positive (effect = 1.841, SE = 0.584, t = 3.153, p = 0.022). For aggression, the pattern was opposite, with a positive between-person effect (effect = 0.885, SE = 0.305, t = 2.899, p = 0.019) and a negative (buffering) within-person effect (effect = −0.753, SE = 0.323, t = −2.328, p = 0.045). See Table 2 for complete results for stratified analyses examining the effects of racial microaggressions on anxiety, depression, and aggression by racial identity profile.
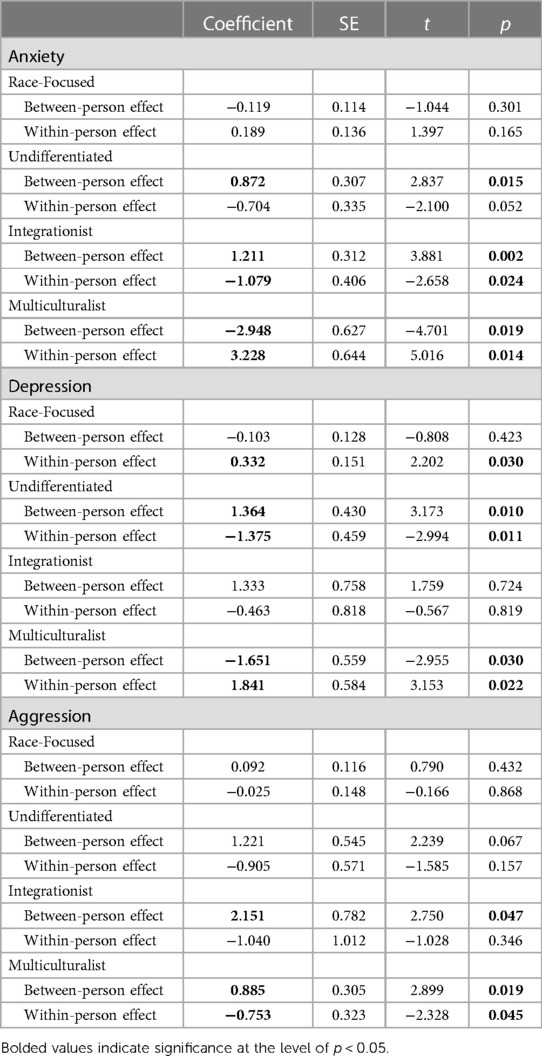
Table 2. Effects of daily experiences with microaggressions by racial identity profile on anxiety, depression, and aggression.
3.3. Variability in the relationship between racial microaggressions and cannabis use by racial identity profile
Mixed-effects (i.e., multilevel) binomial logistic models were used to examine the effect of the interaction of racial identity profiles and the between- and within-person effects of daily experiences of racial microaggressions on cannabis use (0 = no use, 1 = use). These models also controlled for age, gender, and parental education (at the person-level). Results of the omnibus likelihood ratio test (LRT) suggested that the relationship between daily racial microaggressions and cannabis use differed significantly by racial identity profile membership at both the within- [X2(df = 3) = 23.83], p = 0.000) and between-person [X2(df = 3)= 27.63, p = 0.000] levels. Given these results, stratified analyses were conducted to further explore the relationship between racial microaggressions and cannabis use within each racial identity profile.
For individuals in the race-focused profile, there was a significant within-person effect, where individuals who experienced more racial microaggressions had greater odds of endorsing cannabis use [OR = 1.324, 95% CI (1.000, 1.802), p = 0.050]. There were no other significant relationships between racial microaggressions and cannabis use for other racial identity profiles. Moreover, these stratified analyses could not be conducted for individuals in the integrationist or multicultural profiles because the individuals in these profiles did not endorse cannabis use on any days of the daily diary protocol. See Table 3 for complete results for stratified analyses examining the effect of racial microaggressions on cannabis use by racial identity profile.
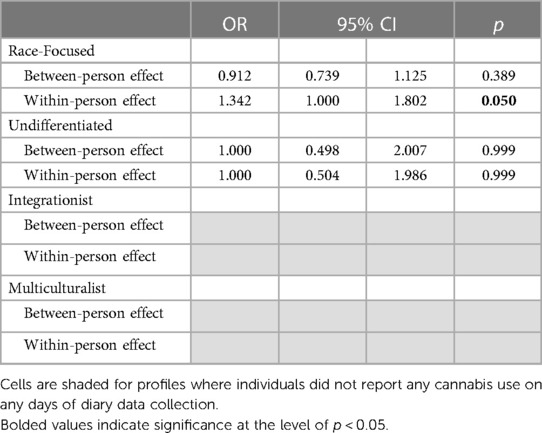
Table 3. Effects of daily experiences with microaggressions by racial identity profile on cannabis use.
4. Discussion
Experiences of racism among Black youth are ubiquitous and have significant impacts on their well-being and development [García (56)]. Thus, it is critical to examine factors that might buffer or exacerbate the relationship between experiences with racial discrimination and health outcomes among Black adolescents. The aims of the current study were to explore the existence of racial identity profiles among Black adolescents and to explore variability in the relationship between daily experiences of racial microaggressions and health outcomes within racial identity profiles among Black adolescents. We hypothesized that we would identify four racial identity profiles in the data, and further, that racial identity profiles characterized by high connection to one's race, positive views of one's race, and beliefs that others view one's race positively would be protective against negative health outcomes as a consequence of racial discrimination. Conversely, we hypothesized that profiles characterized by low connection to one's race, negative views of one's race, and beliefs that others view one's race negatively would elevate risk.
In support of our hypothesis, four racial identity profiles were identified within the dataset, representing youth who were reasonably well-connected to Black culture and aware of racism specific to Black people (i.e., race-focused), those who do not have a strong race-based worldview (i.e., undifferentiated), youth focused on shared qualities between many different groups and placing an emphasis on Black people integrating/assimilating into mainstream American culture (i.e., integrationist), and those who believed that all Americans and humans in general are similar (i.e., multiculturalist). This finding was largely consistent with previous studies using the full MIBI to identify racial identity profiles [e.g., (23–25)]. Of note, the largest profile found in this sample was the race-focused profile, which is similar to distributions of corresponding profiles found in other studies [e.g., (25)]. Further, while several profiles in this study had small cell sizes due to the limited sample size, each profile was described here, as other previous studies have also retained profiles with very small sample sizes [e.g., n = 5; (26)] and have called for the inclusion rather than the removal of these profiles as they may be representative of actual groups of individuals in a given population. However, we will not interpret the findings for the other three profiles given the low cell count, but provide them as evidence of their existence and to highight the need for more work in this area to validate their relationship with health outcomes among Black adolescents.
For individuals in the race-focused profile, there were no significant effects of racial microaggressions on anxiety or aggression for individuals in this profile. Regarding the aggression outcome, this may suggest a buffering effect of race-focused profiles, given that an association was observed between racial microaggressions and aggression across participants. This is in line with our stated hypotheses and research documenting the protective nature of a strong, positive connection to one's race against racial discrimination [e.g., (34)]. Furthermore, researchers have found that for Black young adult males, the relationship between racial discrimination and violent behavior is buffered by high race centrality (57). These researchers suggest that perhaps an internalization of a strong sense of one's racial identity and group affiliation may offset the stigmatization and marginalization that being Black in society involves. However, without a strong racial identity, Black adolescents may feel more disrupted when experiencing what they perceive as the negative effects of being Black (57).
Additionally, there were some significant effects observed within the race-focused profile, such that for those in this profile, on days when an individual experienced more racial microaggressions than usual for themself, they also reported greater depression as well as greater cannabis use (within-person effects). These findings were partially in opposition to our hypotheses because we expected that profiles characterized by a high connection to one's race and positive views of one's race would introduce less risk in the relationship between racial discrimination and outcomes. These findings also contradict some previous findings where individuals with a strong, positive connection to their race have more positive outcomes [e.g., (58)]. However, the race-focused profile is also characterized by relatively low public regard compared to other profiles (i.e., the belief that others view your race negatively). Indeed, we did hypothesize that profiles characterized by beliefs that others view one's race negatively would elevate risk, which was supported.
This multidimensional understanding of racial identity allows us to gain a deeper understanding of why individuals in particular profiles might have certain outcomes. Individuals in the race-focused profile are not only highly connected to their race, but also highly aware of racism specific to Black Americans. Perhaps this combination creates scenarios in which these individuals are more likely to pick up on negative race-related cues in more ambiguous situations (59, 60), and thus might be more likely to have worse mental and behavioral health outcomes following experiences of racial discrimination compared to other profiles that might not be as tuned in to these negative cues. Further, in an intensive longitudinal study of racial discrimination on depression among Black adolescents, researchers found that neither racial centrality nor private regard moderated the same-day or lagged associations between racial discrimination experiences and daily depressive symptoms. However, low public regard exacerbated the relationship between racial discrimination experiences and daily depressive symptoms (18). The finding from the current study is in line with these results and builds on them, suggesting that even in combination with high centrality and high private regard, low public regard introduces risk. Further, previous cross-sectional studies have found that individuals in the race-focused profile are at increased risk for substance use as a consequence of racial discrimination compared to those in other profiles (25). Taken together, individuals in the race-focused profile may be at greater risk for depression and cannabis use on days when they experience greater racial microaggressions.
Another factor to consider when examining the results of this study is the gender of participants within each profile. Previous research utilizing all seven subscales of the MIBI to construct and examine racial identity profiles have had samples that were majority female/woman identifying, with samples ranging from 66% to 100% female/woman identifying (23–28). This study was no exception, with 79.2% of the sample identifying as girls. While it is a strength of the study that we were able to recruit and retain a sample of Black girls, a group historically underrepresented in research [e.g., (61)], it limits our understanding of how these profiles might look or impact outcomes among other genders. Of these previous studies, most have identified no cluster/profile differences by gender (24, 27, 28), or have not examined differences by gender (25, 26). However, Banks and Kohn-Wood (23) did find significant profile differences by gender, and reported that their undifferentiated and race-focused profiles mirrored the total sample in terms of gender makeup, the multiculturalist profile had roughly equal numbers of male and female participants, and their integrationist profile was made up of mostly females (82.5%). Interestingly, for the current study, the multiculturalist profile was made up entirely of girls (100%) and the integrationist profile was made up entirely of boys (100%). However, there were only two participants within each profile, thus findings must be interpreted with caution. Yet, these findings highlight the need for more research in this area to better understand how racial identity profiles may or may not differ by gender. This will require recruiting samples with appropriate representation of different gender categories given that much of the research to date has been done on samples that are predominantly female or woman-identifying.
4.1. Limitations
Despite the strengths of the current investigation, including advanced, person-centered methodology, the current study has several limitations that should be considered during its interpretation. First, the study used community-based sampling methods in a mid-sized Midwestern city and surrounding areas, limiting the generalizability of the study. Second, measurement in the current study spanned over two weeks but racial identity was only assessed at baseline rather than daily. While some researchers propose that racial identity is relatively stable over time [e.g., (12)], some research suggests that racial identity can change significantly over time, particularly among Black adolescents and young adults [e.g., (18)]. Third, the small sample size, while on par with previous studies utilizing EMA methodology among children, which have ranged from 5 to 562 [in a meta-analysis of 36 studies with an average of 98.81 participants; see (62)], provides limited power to detect effects, particularly when stratifying based on racial identity profiles. Fourth, the internal consistency on a particular subscale on the MIBI-T racial identity measure was poor (racial centrality = 0.464). Low internal consistency may suggest that items on this particular subscale may not be measuring the construct consistently or reliably in the current study (63). Low Cronbach's alpha values could be due to a low number of questions, poor inter-relatedness between items or heterogeneous constructs. The MIBI-T centrality subscale only has 3 questions, but previous studies have still found alpha values for this subscale that are closer to the acceptable range [e.g., 0.58; (64)]. Further investigation of the data illustrated that one item in this subscale (“If I were to describe myself to someone, one of the first things that I would say is that I’m Black”) was not significantly correlated with the other two items (“I feel close to other Black people” and “I have a strong sense of belonging to other Black people”). It may be that participant characteristics in the current study were related to differential endorsement of the uncorrelated item compared to the other subscale items. If the uncorrelated item is removed from the scale, Cronbach's alpha increases to 0.818. However, latent profile analyses still suggested a 4-profile model fit the data best and all 48 participants’ racial identity profile membership remained the same when this item was removed. Thus, we elected to leave the item in for the current study; however, it will be important for future studies to examine the items within this particular measure to ensure they are accurately loading onto the proposed factors. Further, perhaps stronger measures are needed to examine racial identity more accurately among Black adolescents.
4.2. Implications
There are several implications of the current study for future research and prevention efforts. These results continue to support racial identity as an important developmental factor to assess and measure among Black youth. Further, a more multidimensional view of racial identity can provide clinicians with even more areas for intervention for individuals who may be at risk for negative outcomes. However, more research is needed regarding the impact of racial identity profiles on the health and well-being of Black children and youth. More specifically, racial identity profiles help us to better understand those youth who may be the most at risk for negative internalizing and externalizing outcomes as a result of racial microaggressions and constitute an important area of intervention. In particular, researchers have found that racial socialization that Black youth receive can not only help shape and solidify racial identity but can work together with elements of racial identity to protect these youth from the damaging impact of racism [e.g., (65)]. Racial socialization interventions exist, focused on bolstering the socialization skills and strategies among Black parents to help Black youth develop strong, protective racial identities and racially-specific coping strategies (e.g., Engaging, Managing, and Bonding through Race (EMBRace) intervention; (66)).
Future research should continue to explore and report on Black youths’ experiences with racism and factors that might buffer or exacerbate its impact on health outcomes utilizing EMA approaches like the ones utilized in the current study. Additional studies are needed to replicate or further elucidate these effects, and as previously mentioned, additional studies are needed with more frequent data collection of racial identity measures to better understand possible shorter-term changes and processes that may be taking place. In sum, this study represents a crucial step in advancing our understanding of the impact of racial identity in the risk pathway between racial microaggressions and health outcomes among Black adolescents on a daily level.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Indiana University Purdue University Indianapolis. The studies were conducted in accordance with the local legislation and institutional requirements. Verbal informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
RC: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Writing – original draft. TZ: Conceptualization, Funding acquisition, Investigation, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported in part by the American Psychological Association (APA), Division 38 Graduate Student Research in General Health Psychology Award (Clifton) and NIH/NIDA K01DA043654 (Zapolski).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Seaton EK, Caldwell CH, Sellers RM, Jackson JS. The prevalence of perceived discrimination among African American and Caribbean black youth. Dev Psychol. (2008) 44(5):1288–97. doi: 10.1037/a0012747
2. Umaña-Taylor AJ. A post-racial society in which ethnic-racial discrimination still exists and has significant consequences for youths’ adjustment. Curr Dir Psychol Sci. (2016) 25(2):111–8. doi: 10.1177/0963721415627858
3. Seaton EK, Douglass S. School diversity and racial discrimination among African-American adolescents. Cultur Divers Ethnic Minor Psychol. (2014) 20(2):156–65. doi: 10.1037/a0035322
4. Sue DW, Capodilupo CM, Torino GC, Bucceri JM, Holder AMB, Nadal KL, et al. Racial microaggressions in everyday life: implications for clinical practice. American Psychologist. (2007) 62(4):271–86. doi: 10.1037/0003-066X.62.4.271
5. Wong G, Derthick AO, David EJR, Saw A, Okazaki S. The what, the why, and the how: a review of racial microaggressions research in psychology. Race Soc Probl. (2014) 6(2):181–200. doi: 10.1007/s12552-013-9107-9
6. Huynh VW. Ethnic microaggressions and the depressive and somatic symptoms of latino and Asian American adolescents. J Youth Adolesc. (2012) 41:831–46. doi: 10.1007/s10964-012-9756-9
7. Ong AD, Cerrada C, Lee RA, Williams DR. Stigma consciousness, racial microaggressions, and sleep disturbance among Asian Americans. Asian Am J Psychol. (2017) 8(1):72–81. doi: 10.1037/aap0000062
8. Dickerson DL, Brown RA, Klein DJ, Agniel D, Johnson C, D'Amico EJ. Overt perceived discrimination and racial microaggressions and their association with health risk behaviors among a sample of urban American Indian/Alaska native adolescents. J Racial Ethn Health Disparities. (2019) 6(4):733–42. doi: 10.1007/s40615-019-00572-1
9. Loyd AB, Kürüm E, Crooks N, Maya A, Emerson E, Donenberg GR. Investigating longitudinal associations between racial microaggressions, coping, racial/ethnic identity, and mental health in black girls and women. J Res Adolesc. (2022) 32(1):69–88. doi: 10.1111/jora.12710
10. English D, Lambert SF, Tynes BM, Bowleg L, Zea MC, Howard LC. Daily multidimensional racial discrimination among black U.S. American adolescents. J Appl Dev Psychol. (2020) 66:101068. doi: 10.1016/j.appdev.2019.101068
11. Paradies Y. A systematic review of empirical research on self-reported racism and health. Int J Epidemiol. (2006) 35(4):888–901. doi: 10.1093/ije/dyl056
12. Sellers RM, Smith MA, Shelton JN, Rowley SAJ, Chavous TM. Multidimensional model of racial identity: a reconceptualization of African American racial identity. Pers Soc Psychol Rev. (1998) 2(1):18–39. doi: 10.1207/s15327957pspr0201_2
13. Lee DL, Ahn S. The relation of racial identity, ethnic identity, and racial socialization to discrimination–distress: a meta-analysis of black Americans. J Couns Psychol. (2013) 60(1):1–14. doi: 10.1037/a0031275
14. Sellers RM, Copeland-Linder N, Martin PP, Lewis RL. Racial identity matters: the relationship between racial discrimination and psychological functioning in African American adolescents. J Res Adolesc. (2006) 16(2):187–216. doi: 10.1111/j.1532-7795.2006.00128.x
15. Rivas-Drake D, Seaton EK, Markstrom C, Quintana S, Syed M, Lee RM, et al. Ethnic and racial identity in adolescence: implications for psychosocial, academic, and health outcomes. Child Dev. (2014) 85(1):40–57. doi: 10.1111/cdev.12200
16. Smith TB, Silva L. Ethnic identity and personal well-being of people of color: a meta-analysis. J Couns Psychol. (2011) 58(1):42. doi: 10.1037/a0021528
17. Yip T. Ethnic/racial identity—a double-edged sword? Associations with discrimination and psychological outcomes. Curr Dir Psychol Sci. (2018) 27(3):170–5. doi: 10.1177/0963721417739348
18. Seaton EK, Iida M. Racial discrimination and racial identity: daily moderation among black youth. American Psychologist. (2019) 74(1):117. doi: 10.1037/amp0000367
19. Bradby D, Helms JE. Black racial identity attitudes and white therapist cultural sensitivity in cross-racial therapy dyads: An exploratory study. In: Helms JE, editor. Black and White Racial Identity: Theory, Research, and Practice. Westport, Connecticut: Greenwood Press (1990). p. 165–75.
20. Helms JE. Toward a theoretical explanation of the effects of race on counseling a black and white model. Couns Psychol. (1985) 12(4):153–65. doi: 10.1177/0011000084124013
21. Parham TA, Helms JE. Relation of racial identity attitudes to self-actualization and affective states of black students. J Couns Psychol. (1985) 32:307–22. doi: 10.1037/0022-0167.32.3.431
22. Sellers RM, Rowley SA, Chavous TM, Shelton JN, Smith MA. Multidimensional inventory of black identity: a preliminary investigation of reliability and constuct validity. J Pers Soc Psychol. (1997) 73(4):805. doi: 10.1037/0022-3514.73.4.805
23. Banks KH, Kohn-Wood LP. The influence of racial identity profiles on the relationship between racial discrimination and depressive symptoms. J Black Psychol. (2007) 33(3):331–54. doi: 10.1177/0095798407302540
24. Bernard DL, Hoggard LS, Neblett EW Jr. Racial discrimination, racial identity, and impostor phenomenon: a profile approach. Cultur Divers Ethnic Minor Psychol. (2018) 24(1):51. doi: 10.1037/cdp0000161
25. Clifton RL. The promotive and protective role of racial identity profiles [Unpublished master’s thesis]. Indianapolis: Indiana University Purdue University (2020).
26. Mekawi Y, Lewis CB, Watson-Singleton NN, Jatta IF, Ander L, Lamis D, et al. Racial identity profiles among suicidal black women: a replication and extension study. J Black Stud. (2020) 51(7):685–704. doi: 10.1177/0021934720935601
27. Jr N, & Carter EW, E S. The protective role of racial identity and africentric worldview in the association between racial discrimination and blood pressure. Psychosom Med. (2012) 74(5):509–16. doi: 10.1097/PSY.0b013e3182583a50
28. Willis HA, Neblett EW Jr. OC symptoms in African American young adults: the associations between racial discrimination, racial identity, and obsessive-compulsive symptoms. J Obsessive Compuls Relat Disord. (2018) 19:105–15. doi: 10.1016/j.jocrd.2018.09.002
29. Vermunt JK, Lewis-Beck M, Bryman A, Liao T. Latent profile model. In: Lewis-Beck MS, Bryman A, Liao TF, editors. The sage encyclopedia of social sciences research methods. Thousand Oaks, California: Sage (2004). p. 554–5.
30. Bolger N, Zuckerman A. A framework for studying personality in the stress process. J Pers Soc Psychol. (1995) 69:890–902. doi: 10.1037/0022-3514.69.5.890
31. Affleck G, Zautra A, Tennen H, Armeli S. Multilevel daily process designs for consulting and clinical psychology: a preface for the perplexed. J Consult Clin Psychol. (1999) 67(5):746. doi: 10.1037/0022-006X.67.5.746
32. Burrow AL, Ong AD. Racial identity as a moderator of daily exposure and reactivity to racial discrimination. Self Identity. (2010) 9(4):383–402. doi: 10.1080/15298860903192496
33. Hoggard LS, Byrd CM, Sellers RM. Comparison of African American college students’ coping with racially and nonracially stressful events. Cultur Divers Ethnic Minor Psychol. (2012) 18(4):329–39. doi: 10.1037/a0029437
34. Haeny AM, Gibbons FX, Fleischli ME, Gerrard M, Lopez J, Beach SR. Racial centrality mediates the association between adolescent racial discrimination and adult cigarette smoking outcomes among black Americans. Soc Sci Med. (2023) 316:115225. doi: 10.1016/j.socscimed.2022.115225
35. Hope EC, Brinkman M, Hoggard LS, Stokes MN, Hatton V, Volpe VV, et al. Black adolescents’ anticipatory stress responses to multilevel racism: the role of racial identity. Am J Orthopsychiatry. (2021) 91(4):487. doi: 10.1037/ort0000547
36. Scottham KM, Sellers RM, Nguyên HX. A measure of racial identity in African American adolescents: the development of the multidimensional inventory of black identity–teen. Cultur Divers Ethnic Minor Psychol. (2008) 14(4):297–306. doi: 10.1037/1099-9809.14.4.297
37. Chavous TM, Bernat DH, Schmeelk-Cone K, Caldwell CH, Kohn-Wood L, Zimmerman MA. Racial identity and academic attainment among African American adolescents. Child Dev. (2003) 74(4):1076–90. doi: 10.1111/1467-8624.00593
38. Forrest-Bank S, Jenson JM, Trecartin S. The revised 28-item racial and ethnic microaggressions scale (R28REMS): examining the factorial structure for black, latino/hispanic, and Asian young adults. J Soc Serv Res. (2015) 41(3):326–44. doi: 10.1080/01488376.2014.987944
39. Nadal KL. The racial and ethnic microaggressions scale (REMS): construction, reliability, and validity. J Couns Psychol. (2011) 58(4):470. doi: 10.1037/a0025193
40. Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. (2009) 114(1-3):163–73. doi: 10.1016/j.jad.2008.06.026
41. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166(10):1092. doi: 10.1001/archinte.166.10.1092
42. Borah TJ, Murray AL, Eisner M, Jugl I. Developing and validating an experience sampling measure of aggression: the aggression-ES scale. J Interpers Violence. (2021) 36(11-12):NP6166–82. doi: 10.1177/0886260518812068
43. Nooraee N, Molenberghs G, Ormel J, Van den Heuvel ER. Strategies for handling missing data in longitudinal studies with questionnaires. J Stat Comput Simul. (2018) 88(17):3415–36. doi: 10.1080/00949655.2018.1520854
44. Akaike H. A new look at the statistical model identification. IEEE Transactions on Automatic Control. (1974) 19(6):716–23. doi: 10.1109/TAC.1974.1100705
45. Schwarz G. Estimating the dimension of a model. Ann Stat. (1978) 6(2):461–4. doi: 10.1214/aos/1176344136
48. Marsh HW, Lüdtke O, Trautwein U, Morin AJ. Classical latent profile analysis of academic self-concept dimensions: synergy of person-and variable-centered approaches to theoretical models of self-concept. Struct Equ Modeling. (2009) 16(2):191–225. doi: 10.1080/10705510902751010
49. Curran PJ, Bauer DJ. The disaggregation of within-person and between-person effects in longitudinal models of change. Annu Rev Psychol. (2011) 62:583–619. doi: 10.1146/annurev.psych.093008.100356
50. Campbell OL, Bann D, Patalay P. The gender gap in adolescent mental health: a cross-national investigation of 566,829 adolescents across 73 countries. SSM-population Health. (2021) 13:100742. doi: 10.1016/j.ssmph.2021.100742
51. Young SE, Corley RP, Stallings MC, Rhee SH, Crowley TJ, Hewitt JK. Substance use, abuse and dependence in adolescence: prevalence, symptom profiles and correlates. Drug Alcohol Depend. (2002) 68(3):309–22. doi: 10.1016/S0376-8716(02)00225-9
52. McHugh RK, Votaw VR, Sugarman DE, Greenfield SF. Sex and gender differences in substance use disorders. Clin Psychol Rev. (2018) 66:12–23. doi: 10.1016/j.cpr.2017.10.012
53. Alcover KC, Thompson CL. Patterns of mean age at drug use initiation among adolescents and emerging adults, 2004-2017. JAMA Pediatr. (2020) 174(7):725–7. doi: 10.1001/jamapediatrics.2019.6235
54. McLaughlin KA, Costello EJ, Leblanc W, Sampson NA, Kessler RC. Socioeconomic status and adolescent mental disorders. Am J Public Health. (2012) 102(9):1742–50. doi: 10.2105/AJPH.2011.300477
55. Andrabi N, Khoddam R, Leventhal AM. Socioeconomic disparities in adolescent substance use: role of enjoyable alternative substance-free activities. Soc Sci Med. (2017) 176:175–82. doi: 10.1016/j.socscimed.2016.12.032
56. Coll G, Crnic C, Lamberty K, Wasik G, Jenkins BH, Garcia R, et al. An integrative model for the study of developmental competencies in minority children. Child Dev. (1996) 67(5):1891–914. doi: 10.2307/1131600
57. Caldwell CH, Kohn-Wood LP, Schmeelk-Cone KH, Chavous TM, Zimmerman MA. Racial discrimination and racial identity as risk or protective factors for violent behaviors in African American young adults. Am J Community Psychol. (2004) 33:91–105. doi: 10.1023/B:AJCP.0000014321.02367.dd
58. Mandara J, ., Gaylord-Harden NK, Richards MH, Ragsdale BL. The effects of changes in racial identity and self-esteem on changes in African American adolescents’ mental health. Child Dev. (2009) 80(6):1660–75. doi: 10.1111/j.1467-8624.2009.01360.x
59. Operario D, Fiske ST. Ethnic identity moderates perceptions of prejudice: judgments of personal versus group discrimination and subtle versus blatant bias. Pers Soc Psychol Bull. (2001) 27(5):550–61. doi: 10.1177/0146167201275004
60. Sellers RM, Shelton JN. The role of racial identity in perceived racial discrimination. J Pers Soc Psychol. (2003) 84(5):1079. doi: 10.1037/0022-3514.84.5.1079
61. Bierer BE, Meloney LG, Ahmed HR, White SA. Advancing the inclusion of underrepresented women in clinical research. Cell reports. Medicine (Baltimore). (2022) 3(4):100553. doi: 10.1016/j.xcrm.2022.100553
62. Wen CKF, Schneider S, Stone AA, Spruijt-Metz D. Compliance with mobile ecological momentary assessment protocols in children and adolescents: a systematic review and meta-analysis. J Med Internet Res. (2017) 19(4):e132. doi: 10.2196/jmir.6641
63. Tavakol M, Dennick R. Making sense of cronbach’s alpha. Int J Med Educ. (2011) 2:53. doi: 10.5116/ijme.4dfb.8dfd
64. Butler-Barnes ST, Leath S, Williams A, Byrd C, Carter R, Chavous TM. Promoting resilience among African American girls: racial identity as a protective factor. Child Dev. (2018) 89(6):e552–71. doi: 10.1111/cdev.12995
65. Gibson SM, Bouldin BM, Stokes MN, Lozada FT, Hope EC. Cultural racism and depression in black adolescents: examining racial socialization and racial identity as moderators. J Res Adolesc. (2022) 32(1):41–8. doi: 10.1111/jora.12698
Keywords: racial identity profiles, Black adolescents, racial microaggressions, depression, anxiety, aggression, substance use
Citation: Clifton RL and Zapolski TCB (2023) Racial identity profiles among Black adolescents: impact on the relationship between daily racial microaggressions and health outcomes. Front. Adolesc. Med. 1:1283373. doi: 10.3389/fradm.2023.1283373
Received: 25 August 2023; Accepted: 20 October 2023;
Published: 20 November 2023.
Edited by:
Anita Cservenka, Oregon State University, United StatesReviewed by:
Elizabeth Culatta, Augusta University, United StatesMiesha Marzell, Binghamton University, United States
© 2023 Clifton and Zapolski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Richelle L. Clifton cmNsaWZ0b0B1dy5lZHU=