 Alexandre Hudon1,2,3,4*
Alexandre Hudon1,2,3,4*- 1Centre de recherche de l’Institut universitaire en santé mentale de Montréal, Montreal, QC, Canada
- 2Department of Psychiatry, Institut universitaire en santé mentale de Montréal, Montreal, QC, Canada
- 3Department of Psychiatry, Institut national de psychiatrie légale Philippe-Pinel, Montreal, QC, Canada
- 4Department of Psychiatry and Addictology, Université de Montréal Faculty of Medicine, Montreal, QC, Canada
Background: Decisions surrounding involuntary psychiatric treatment orders often involve complex clinical, legal, and ethical considerations, especially when patients lack decisional capacity and refuse treatment. In Quebec, these orders are issued by the Superior Court based on a combination of medical, legal, and behavioral evidence. However, no transparent, evidence-informed predictive tools currently exist to estimate the likelihood of full treatment order acceptance. This study aims to develop and evaluate a hybrid fuzzy logic–machine learning model to predict such outcomes and identify important influencing factors.
Methods: A retrospective dataset of 176 Superior Court judgments rendered in Quebec in 2024 was curated from SOQUIJ, encompassing demographic, clinical, and legal variables. A Mamdani-type fuzzy inference system was constructed to simulate expert decision logic and output a continuous likelihood score. This score, along with structured features, was used to train a Random Forest classifier. Model performance was evaluated using accuracy, precision, recall and F1 score. A 10-fold stratified cross-validation was employed for internal validation. Feature importance was also computed to assess the influence of each variable on the prediction outcome.
Results: The hybrid model achieved an accuracy of 98.1%, precision of 93.3%, recall of 100%, and a F1 score of 96.6. The most influential predictors were the duration of time granted by the court, duration requested by the clinical team, and age of the defendant. Fuzzy logic features such as severity, compliance, and a composite Burden_Score also significantly contributed to prediction accuracy. Only one misclassified case was observed in the test set, and the system provided interpretable decision logic consistent with expert reasoning.
Conclusion: This exploratory study offers a novel approach for decision support in forensic psychiatric contexts. Future work should aim to validate the model across other jurisdictions, incorporate more advanced natural language processing for semantic feature extraction, and explore dynamic rule optimization techniques. These enhancements would further improve generalizability, fairness, and practical utility in real-world clinical and legal settings.
1 Introduction
In psychiatric care, particularly in acute and forensic contexts, there are situations in which patients are incapable of consenting to treatment and simultaneously refuse all interventions, including psychotropic medication. These scenarios present complex clinical and ethical challenges, as the refusal of care may result in self-harm, deterioration of mental status, or threats to others. In such cases, legal mechanisms like treatment orders become essential tools to ensure continuity of care while safeguarding civil liberties (Saya et al., 2019; Szmukler and Holloway, 1998). These orders permit the administration of treatment without full consent when patients are found to lack decisional capacity due to psychiatric illness such as schizophrenia, bipolar disorder with psychotic features, or severe depressive episodes with psychosis (Pons et al., 2020; Owen et al., 2008). The use of treatment orders reflects a delicate balance between patient autonomy and the necessity for care in the face of incapacity (Bergamin et al., 2022).
In Quebec, treatment orders are issued under the jurisdiction of the Superior Court, following legal frameworks established in the Civil Code of Quebec and applicable jurisprudence. The legal process typically begins when a treating psychiatrist summons the court, supported by documentation that the patient lacks capacity and that treatment is urgently required (O'Reilly et al., 2019). The patient is afforded the right to contest the application and is often represented by legal aid counsel. The judge considers expert testimony, diagnostic assessments, and social context before determining whether to authorize the treatment order, in part or in full (Frank et al., 2020). The decision itself is not a simple clinical translation. It reflects a legal interpretation of psychiatric risk, patient history, compliance patterns, and the proportionality of the request. As such, decisions can vary significantly across judges and institutions despite similar clinical contexts (Rugkåsa, 2016; Weich et al., 2020).
Given the subjective, cross-disciplinary, and time-sensitive nature of these legal decisions, identifying the important variables that influence a judge’s decision to fully accept a treatment order is both clinically and legally relevant. However, the semi-structured nature of psychiatric records and the complex language of legal documentation pose barriers to standard predictive modeling (London, 2019). Furthermore, traditional machine learning models often lack interpretability, making them less suited for ethically sensitive applications in mental health law (Goktas and Grzybowski, 2025; Ennab and Mcheick, 2024). Fuzzy logic systems, by contrast, allow for expert rule-based reasoning that accommodates uncertainty and vagueness which are common characteristics in psychiatric data (Torres and Nieto, 2006; Shoaip et al., 2024; Modai et al., 2004). When combined with Random Forests, an ensemble-based machine learning method known for handling non-linear relationships and high-dimensional data, fuzzy logic can enhance model performance without sacrificing interpretability (Hao et al., 2022; Shoaip et al., 2024).
The objective of this proof-of-concept, exploratory study is twofold. First, it aims to build a predictive model that accurately estimates the probability that a Superior Court in Quebec will accept a psychiatric treatment order as requested by the treating team. Second, it seeks to identify the most influential features contributing to that outcome, including demographic variables, legal context, clinical diagnosis, and behavioral compliance. It is hypothesized that features such as diagnosis severity, time requested by the treating team, non-compliance behaviors, and substance use history will emerge as significant predictors. By integrating expert-driven rule logic with empirical learning, the model aims to support clinicians, legal professionals, and policymakers in making more transparent, equitable, and evidence-informed decisions.
2 Materials and methods
2.1 Description of the dataset
This study draws on a manually curated dataset titled TreatmentOrderQuebec2024, comprising real-world data on mental health treatment order requests rendered in Quebec during the year 2024 from January 1st to December 31st. More specifically, it comprises the 176 judgments from the Superior Court that were identified in the publicly sponsored legal information service in Quebec, Société québécoise d’information juridique (SOQUIJ) (Société québécoise d'information juridique, n.d.). It is important to note that SOQUIJ anonymizes each case reported publicly in their database. Each entry represents a legal case evaluated by the Superior Court and includes both structured variables and semi-structured clinical text. The dataset contains several variables encompassing demographic characteristics (such as the age and sex of the defendant), legal context (including whether the defendant had legal representation or was assisted by legal aid), and clinical indicators (such as primary and secondary diagnoses, behavioral symptom descriptions, and substance use history). It also captures procedural information, notably the duration of treatment requested by the clinical team, the duration granted by the court, and the outcome: specifically, whether the order was accepted in full or only partially granted. The characteristic reported in the dataset are found in Table 1. The main outcome variable used for model training and evaluation is a binary indicator reflecting the court’s decision to either entirely or partially accept the treatment order. To ensure validation, the dataset was split into training and testing subsets using a 70/30 ratio, with 70% of the data reserved for model development and 30% held out for independent performance assessment (Collins et al., 2024). The dataset is available as Supplementary Material 1.
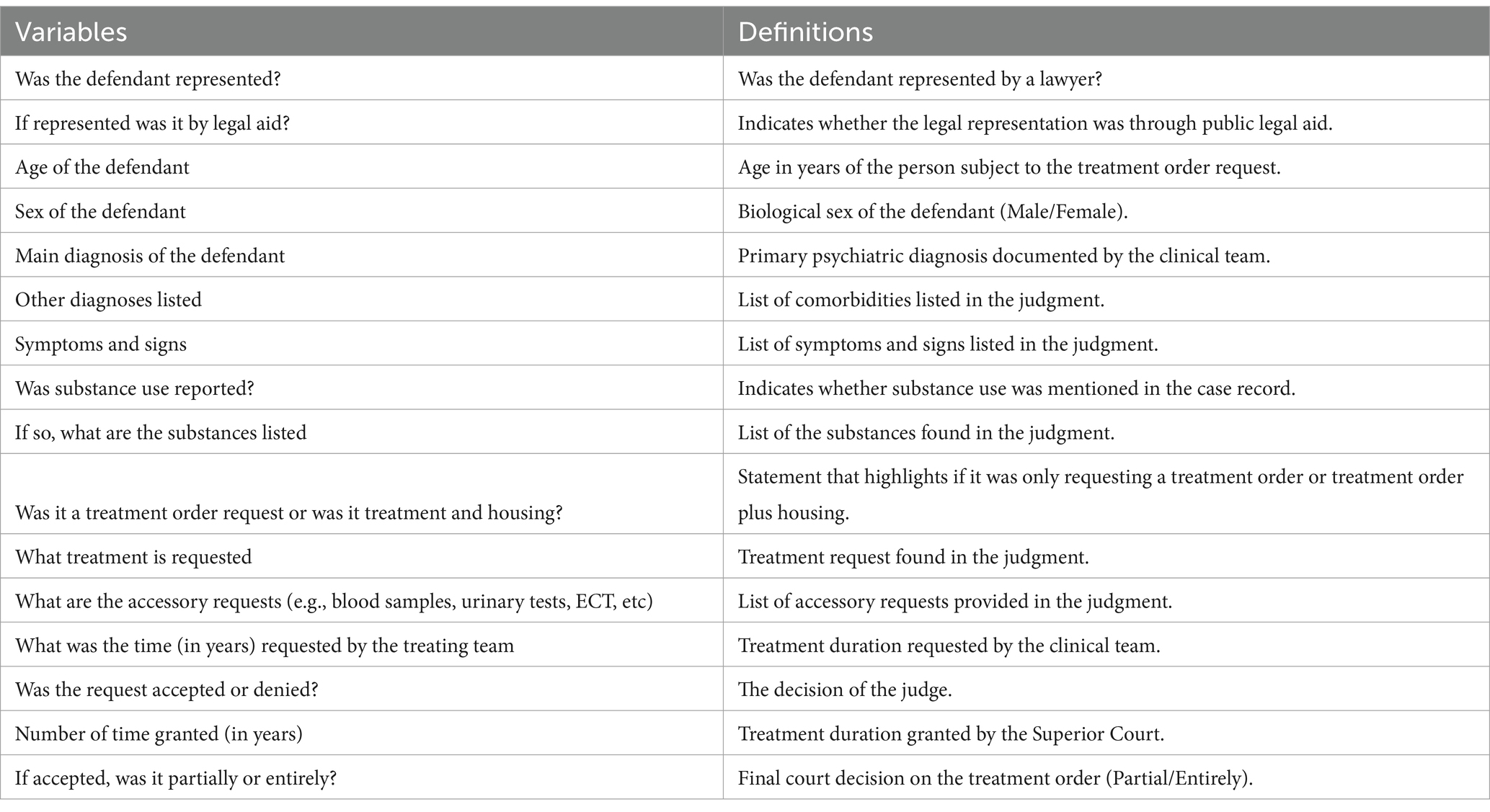
Table 1. Summary of the variables and their definitions.
2.2 Fuzzy logic modeling
A fuzzy inference system (FIS) was developed using a Mamdani-type architecture to encode expert reasoning and produce interpretable predictions regarding the outcome of psychiatric treatment order requests (Guillaume and Charnomordic, 2012). Implemented in Python 3.11, this system was designed to output a continuous score, known as the fuzzy score, between 0 and 1 that represents the likelihood that a treatment order would be entirely accepted by the court. The system was created to mirror the reasoning patterns of mental health and legal experts, translating qualitative assessments (e.g., severity, compliance, context) into a structured, explainable logic model. This approach allowed for both nuanced classification and transparency in decision-making.
The fuzzy model was implemented using a combination of widely recognized Python libraries. Specifically, pandas and numpy were used for data handling and transformation, while scikit-learn supported preprocessing, scaling, and integration into the broader machine learning pipeline (Harris et al., 2020; The pandas development team, 2020). Fuzzy logic inference was handled via the scikit-fuzzy (skfuzzy) library, which provided tools for defining fuzzy variables, membership functions, and rule application (Pedregosa et al., 2011).
To enable fuzzification of key features, numerical variables were normalized to a common [0, 1] scale using Min-Max scaling. Triangular membership functions were then defined for core fuzzy inputs. For example, the “Age of the Defendant” variable was fuzzified into three linguistic categories: Young ([0.0, 0.0, 0.3]), Middle-aged ([0.2, 0.5, 0.7]), and Older ([0.8, 1.0, 1.0]). Similarly, both requested and granted treatment durations were described as Short ([0.0, 0.0, 0.3]), Medium ([0.2, 0.5, 0.7]), or Long ([0.6, 1.0, 1.0]). The fuzzy output variable, representing the Likelihood of Entire Acceptance, was categorized into three fuzzy sets: Low ([0.0, 0.0, 0.4]), Medium ([0.3, 0.5, 0.7]), and High ([0.6, 1.0, 1.0]).
Semantic features were derived through natural language processing of textual case data. Two binary flags were introduced to capture clinically meaningful patterns. The Severity_Flag was set to 1 if the main diagnosis field contained terms like “schizophrenia,” “psychosis,” or “bipolar disorder,” reflecting high diagnostic severity. The Compliance_Flag was similarly set to 1 if the behavioral description included language such as “non-compliance,” “refused,” or “discontinued,” indicating potential treatment resistance. These semantic flags played an important role in the fuzzy rule base, in order to offer binary anchors for more complex rule conditions.
Rather than assigning fixed classifications, the system employed a weighted rule-based approach to produce a fuzzy score. Each rule contributed a weighted score to the final output, allowing for partial activation across multiple rules. For instance, the rule “Severe + Non-compliant → High” carried a full weight of 1.0, whereas “Older + Severe + Compliant → Medium” was assigned a weight of 0.7. Other rules included “Low Severity + Compliance → Low” (weight: 1.0), “Young Male + Substance Use + Long Duration → High” (weight: 0.8), and “Female + High Burden Score → Medium-High” (weight: 0.6). This weighted logic allowed for dynamic blending of rule contributions based on individual case profiles, increasing both predictive power and interpretability. The ten rules implemented in this model are reported in Table 2.
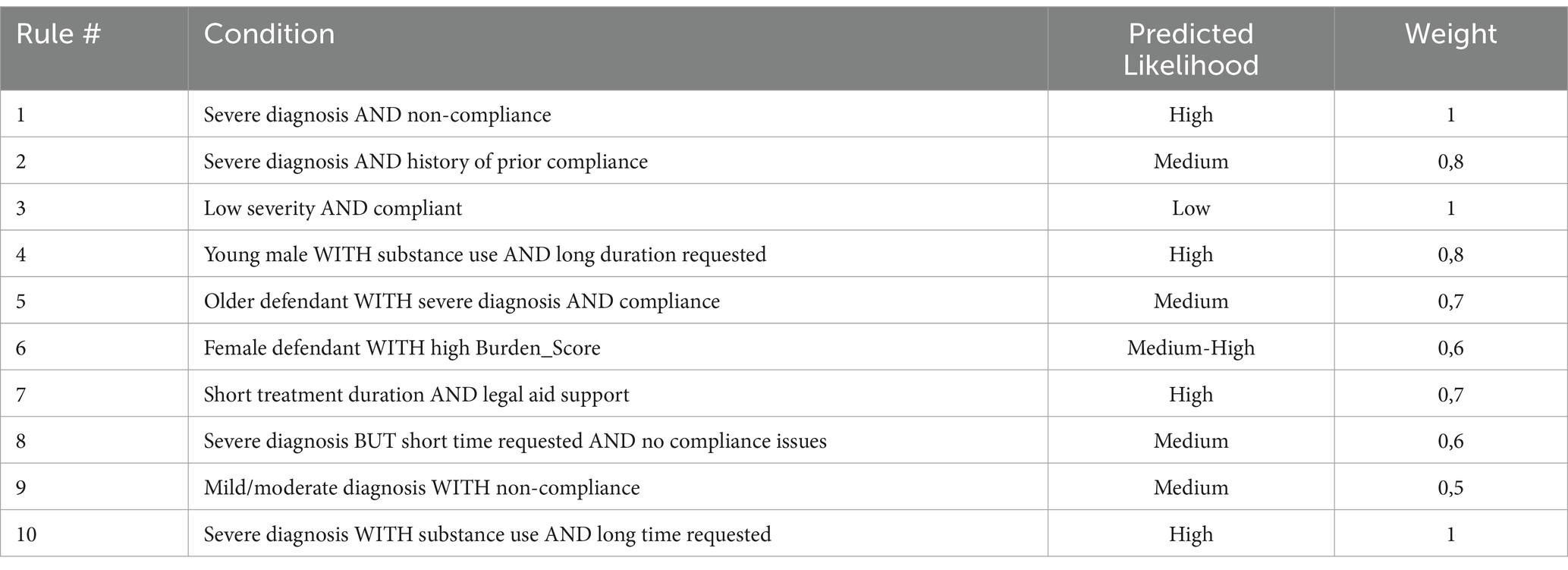
Table 2. Rules of the fuzzy inference system.
To further capture the multidimensional burden of each case, a Burden_Score was calculated as a weighted composite of the features. The weights were chosen based on clinical relevance and empirical signal strength: Severity (35%), Compliance (30%), Time Requested (20%), and Substance Use (15%). The resulting Burden_Score offered a normalized index of clinical and legal complexity, which could then be used directly in rules or passed downstream into machine learning classifiers.
The fuzzy inference system produced a continuous output referred to as the Expanded_Score, representing the degree of likelihood that the court would grant a treatment order in full. This score was derived by averaging the outputs of all activated rules, weighted by their respective importance. For interpretability, the Expanded_Score was categorized into three final risk levels using defuzzification thresholds: Low (< 0.4), Medium (0.4 to 0.7), and High (> 0.7). This final output served as a key input into the hybrid modeling stage, where it was integrated with structured features for supervised classification. The pseudocode for the implementation is found in Supplementary Material 2.
2.3 Random Forest classifier
The second stage involved training a Random Forest classifier using the combined dataset, which included both raw features and the fuzzy-derived Expanded_Score. The model was implemented using the RandomForestClassifier class from the sklearn.ensemble library, with the parameter class_weight = ‘balanced’ to address potential class imbalance between cases that were entirely versus partially accepted (Pedregosa et al., 2011). The input features used for training included: age of the defendant, time requested by the treating team, time granted by the court, legal aid representation, sex, substance use status, semantic flags (severity and compliance), the Burden_Score, and the fuzzy Expanded_Score. The model was trained on 70% of the dataset and evaluated on the remaining 30% using both predicted labels and prediction probabilities.
To assess model interpretability and understand the relative influence of each variable, feature importance analysis was conducted using the Random Forest model’s feature_importances_ attribute. This function computes the mean decrease in Gini impurity contributed by each feature, normalized across all predictors. A Gini impurity is a measure used in decision tree algorithms to quantify how often a randomly chosen element from a set would be incorrectly labeled if it were randomly assigned a label according to the distribution of labels in that set (Das et al., 2018).
2.4 Data analysis
Model performance was assessed through a suite of supervised classification evaluation techniques designed to measure predictive accuracy, class discrimination, and reliability. Class probabilities generated with predict() and predict_proba() from sklearn.ensemble. RandomForestClassifier (Pedregosa et al., 2011). The binary classification outcome (entirely vs. partially accepted treatment orders) was compared to the ground truth labels using four standard evaluation metrics: accuracy, precision, recall and the F1 score (Hicks et al., 2022). Accuracy measured the overall proportion of correct classifications, while precision focused on how many of the cases predicted as fully accepted were actually accepted in full, minimizing false positives. Recall assessed the model’s ability to correctly identify all truly accepted cases, ensuring no eligible cases were missed. The F1 score provided a balanced metric that accounts for both precision and recall, particularly useful in slightly imbalanced datasets.
To further analyze prediction patterns and error distribution, a confusion matrix was generated using confusion_matrix() and visualized with seaborn providing an intuitive view of true positives, false positives, and other classifications across the binary decision space (Waskom, 2021). Additionally, a correlation heatmap was computed using pandas and displayed with seaborn to explore linear relationships among relevant features, including the fuzzy output (Expanded_Score), Burden_Score, and the durations of treatment requested and granted. The choice of these variables was based on the fact that only numeric, monotonic predictors were eligible for a bivariate correlation table. All other predictors (e.g., sex, representation status, diagnosis categories) are nominal or ordinal and would have required point-biserial or rank-based statistics that complicate a single, readable table. With only 176 cases, adding many low-variance or categorical features to a correlation matrix inflates the familywise Type I error without providing interpretable effect sizes.
2.5 Cross-validation
A 10-fold stratified cross-validation procedure was employed during development (Jung and Hu, 2015). This method involved partitioning the training dataset into ten equally sized subsets, or folds, while maintaining the original distribution of the binary outcome (entirely versus partially accepted treatment orders). For each iteration, the model was trained on nine folds and validated on the remaining one, cycling through all combinations. Stratification ensured that class imbalance did not affect any fold disproportionately, thus preserving the fairness and reliability of the evaluation.
2.6 Ethical considerations
All ethical principles were upheld throughout this study. In terms of data privacy, all personal identifiers were removed in accordance with SOQUIJ’s database, and the dataset was processed in full compliance with applicable privacy standards. According to Tri-Council Policy Statement 2 on Ethical Conduct for Research Involving Humans, ethics approval was not required because all the material used to construct the dataset is publicly available (Conseil de recherches en sciences humaines du Canada, n.d.).
Finally, the model is intended strictly as an exploratory decision support tool rather than a substitute for professional judgment. Its use is to provide a proof-of-concept for enhancing risk stratification, guiding policy evaluation, and supporting procedural transparency in complex mental health adjudication contexts.
3 Results
3.1 Fuzzy logic output and categorization
Each sample in the dataset was first evaluated using the fuzzy logic layer, which implemented 10 expert-defined rules with weighted scoring. The top 5 diagnosis identified in the judgments are reported in Figure 1. These rules assessed key variables such as diagnosis severity, treatment compliance, the duration of treatment requested, patient age, sex, substance use, and legal aid involvement. The resulting fuzzy outputs (Expanded_Score) ranged between 0.3 and 0.85 and were defuzzified using the centroid method. Among the 53 cases in the test set, 56.6% were categorized as Medium and 43.4% as High, with no cases falling into the Low category.
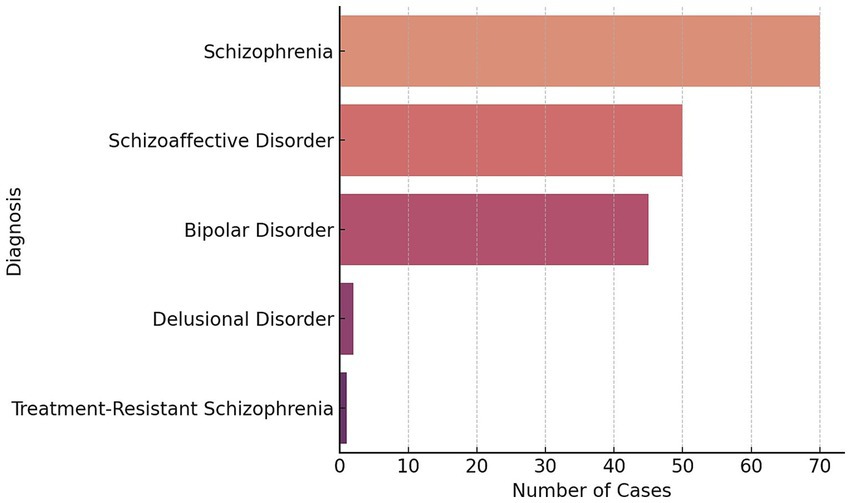
Figure 1. Top 5 diagnosis identified in the judgments.
3.2 Combined model performance
The model achieved an accuracy of 98.1% (95% CI: 92.3–100%), precision of 93.3% (95% CI: 85.7–100%), recall of 100% (95% CI: 94.9–100%), and F1 score of 96.6% (95% CI: 91.2–100%). The confusion matrix revealed only one misclassified case among the 53 test instances which can be found in Figure 2. This indicates a strong alignment between predicted outcomes and actual court decisions.
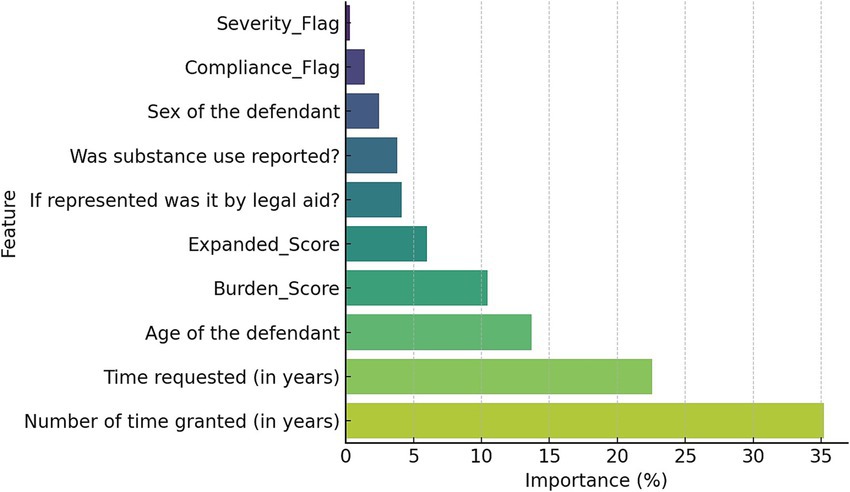
Figure 2. Importance of the combined model’s features.
The most influential predictor was the duration of time granted by the court (35.2%), followed by the duration requested by the treating team (22.6%) and the age of the defendant (13.7%). The Burden_Score contributed 10.4%, and the fuzzy system’s Expanded_Score added 6.0% to the overall model prediction. Semantic flags also played nontrivial roles. Features like legal aid, substance use, and sex were less predictive individually (<2%), but contributed contextually to the model’s overall structure. The importance of features is reported in Figure 3.

Figure 3. Confusion matrix of the hybrid model predictions.
The correlation heatmap revealed several meaningful relationships between the variables in the hybrid model. A strong correlation (r = 0.87) between the Expanded_Score and the Burden_Score suggests that the fuzzy system’s outputs are closely aligned with the composite clinical and legal complexity captured by the Burden_Score, which integrates inputs such as severity, compliance, substance use, and treatment duration. Similarly, a strong correlation (r = 0.77) between time requested and time granted indicates that judicial decisions tend to reflect the duration recommended by the clinical team. In contrast, the Expanded_Score showed very weak correlations with time requested (r = 0.07) and time granted (r = 0.09), suggesting that the fuzzy system operates independently of duration-based inputs and is more heavily influenced by rule-based clinical and behavioral features. The Burden_Score showed only modest correlations with time requested (r = 0.28) and time granted (r = 0.21), indicating that while duration contributes to the burden calculation, it does not dominate it which reinforces the multidimensional nature of the composite score. The heatmap is found in Figure 4.
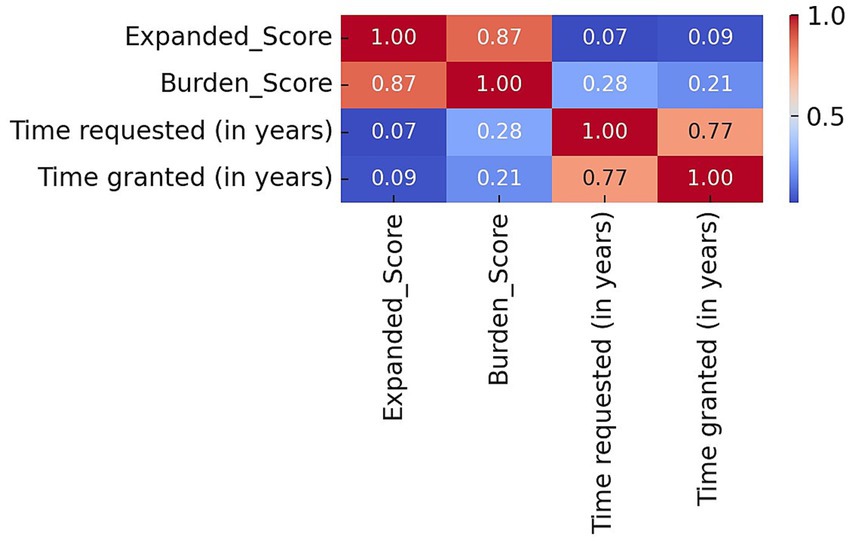
Figure 4. Correlation heatmap of fuzzy and model features.
3.3 Case-based reasoning and interpretability
To assess how the model performs on individual profiles, two illustrative cases were examined. In the first example, a patient diagnosed with schizophrenia who was non-compliant with treatment and recommended for a long treatment duration under legal aid received a fuzzy score of 0.85 and was correctly predicted to be entirely accepted. In the second case, a compliant patient with a mood disorder, a short treatment request, and legal aid representation received a fuzzy score of 0.45 and was correctly classified as partially accepted. These examples highlight how the model’s reasoning aligns with typical clinical and legal expectations.
4 Discussion
This study demonstrates the feasibility and potential utility of combining fuzzy logic with supervised machine learning to predict judicial decisions regarding psychiatric treatment orders. By integrating clinical, legal, and semantic information within a hybrid fuzzy–Random Forest framework, the model achieved strong predictive performance and offered interpretable outputs aligned with expert reasoning. These findings suggest that decision support tools grounded in hybrid modeling can offer value in ethically sensitive, cross-disciplinary contexts such as involuntary psychiatric treatment.
The high predictive performance observed suggests that the hybrid model is highly capable of distinguishing between cases that will be entirely versus partially accepted by the court. These results are important given the complexity and subjectivity of such decisions. Prior work in clinical decision support and mental health law has emphasized the limitations of purely statistical or black-box models in capturing the ambiguity of psychiatric documentation and judicial interpretation (Chekroud et al., 2021; McCradden et al., 2023). Traditional machine learning approaches often struggle to accommodate the vagueness and semantic variability inherent in mental health records (Holzinger et al., 2019). Fuzzy logic, by contrast, provides a formal framework to model uncertainty and expert knowledge, which is especially valuable in psychiatric decision-making (Torres and Nieto, 2006). In this study, the use of expert-defined fuzzy rules attempted to allow for transparent reasoning processes that mirror how judges and clinicians synthesize narrative and structured data.
The use of interpretability-focused AI is especially relevant in legal-medical settings, where decision accountability and traceability are essential. Several researchers have highlighted the importance of explainability in clinical AI to ensure trust and fairness, particularly in high-stakes domains (Abgrall et al., 2024; Asan et al., 2020). Sirocchi et al. emphasize that models used in medicine must not only be accurate but also interpretable by domain experts (Sirocchi et al., 2024). Similarly, Rama et al. advocate for hybrid models that balance statistical rigor with symbolic reasoning to ensure stakeholder acceptance (Raman et al., 2025). In the present study, the fuzzy inference layer played a role in ensuring model transparency. By encoding rules such as “Severe + Non-compliant → High likelihood of acceptance” the system provided logic paths that could be validated or critiqued by legal or clinical stakeholders, enhancing the model’s usability and trustworthiness.
In addition to predictive performance, the study contributes to a growing body of literature supporting hybrid symbolic-statistical models in healthcare and law. Holzinger et al. argue that hybrid approaches allow for “augmented intelligence” by integrating domain expertise into data-driven models (Holzinger et al., 2019). This is relevant in psychiatric contexts, where machine learning alone may miss important context-specific information that clinicians routinely interpret (Torres and Nieto, 2006). The present model’s ability to integrate fuzzy outputs with structured variables (e.g., age, treatment duration, legal aid status) and semantic indicators (e.g., compliance, severity) reflects this “augmented” approach. Importantly, the inclusion of the Burden_Score also aligns with literature advocating for holistic, multi-dimensional indicators in forensic psychiatry (Raharjanti et al., 2021).
Although legal frameworks may vary internationally, the core challenges (balancing patient autonomy, clinical risk, and procedural fairness) are widely shared (Mikellides et al., 2019). The decision-making process in Quebec’s Superior Court is informed not only by medical evaluations but also by judicial discretion shaped by case law and social values. Thus, modeling approaches must reflect both the evidence-based nature of psychiatry and the normative reasoning of law in the specific jurisdiction. The hybrid fuzzy–Random Forest model presented here offers a promising approach to capturing that intersection.
It is also important to note that the fuzzy inference system was explicitly designed to enhance interpretability via rule-based logic, the study did not include a formal expert evaluation of interpretability. Future work should engage legal and psychiatric professionals to assess whether the system’s explanations are clinically meaningful, cognitively accessible, and ethically appropriate for real-world decision support.
Finally, while the findings of this study are promising, several limitations must be acknowledged. The dataset was limited to 176 cases from Quebec’s Superior Court in 2024, which may constrain the generalizability of the model to other jurisdictions or legal systems with differing criteria for involuntary treatment. Furthermore, not all the treatment orders that took place in Quebec in 2024 were reported in the SOQUIJ’s database which may underrepresent certain areas. The dataset also lacked temporal or longitudinal data, such as prior treatment history or recidivism, which could enhance predictive accuracy. Also, the construction of semantic features such as severity and compliance flags relied on keyword matching from clinical narratives, which may not fully capture the nuance of psychiatric assessments and could introduce misclassification bias. Furthermore, although the fuzzy logic system was based on expert-informed rules, the weighting of those rules was manually tuned rather than optimized through formal learning algorithms, potentially limiting the model’s scalability and introduce overfitting. While the model achieved a recall rate of 100% in the held-out test set, this result should be interpreted in light of the relatively small sample size and the potential for overfitting. With only 53 cases in the test set, even a single misclassified instance would have led to a marked reduction in recall. As such, the recall score likely reflects model performance on this specific dataset and may not generalize to future or out-of-distribution cases. Future work should prioritize external validation with larger and more diverse datasets to confirm the model’s robustness across settings. Also, the study used retrospective data and did not include external validation across multiple sites or years, limiting its ability to predict future or out-of-distribution cases. Future studies on this topic should also explore adaptive rule learning, richer natural language processing pipelines, and multi-jurisdictional validation to strengthen the model’s reliability and fairness.
5 Conclusion
This study demonstrates the successful implementation of a hybrid fuzzy logic–Random Forest model to predict the outcome of psychiatric treatment orders in Quebec’s Superior Court. By integrating structured demographic and legal variables with expert-informed semantic features and rule-based reasoning, the model achieved high predictive accuracy while preserving interpretability. The fuzzy inference system provided a transparent layer that mirrored clinical and legal judgment processes, while the machine learning classifier captured non-linear relationships and enhanced overall performance. The ability of the model to accurately distinguish between fully and partially accepted orders (while simultaneously offering an interpretable rationale for its predictions) addresses a need in both forensic psychiatry and legal medicine. Furthermore, the creation of the Burden_Score and Expanded_Score allowed for meaningful integration of clinical, behavioral, and procedural data, reinforcing the value of multidimensional modelling in such contexts. As health systems and courts increasingly turn to data-driven tools for support, this hybrid architecture offers a blueprint for responsible and context-sensitive AI deployment. Future research should aim to expand the dataset to include broader geographical coverage, refine semantic feature extraction with more sophisticated natural language processing techniques, and explore dynamic tuning of fuzzy rules through machine learning. With such advancements, hybrid models can serve not only as predictive tools but also as frameworks for dialogue between clinical judgment, legal reasoning, and artificial intelligence. This exploratory study paves the way for future research to enhance and deploy such models to verify their use in a real-world environment.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AH: Funding acquisition, Writing – original draft, Software, Formal analysis, Data curation, Resources, Project administration, Validation, Methodology, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study has been funded indirectly by the Foundation de l’Institut universitaire en santé mentale de Montréal.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author declares that Gen AI was used in the creation of this manuscript. The author(s) declare that Gen AI was used to proof read this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frai.2025.1606250/full#supplementary-material
References
Abgrall, G., Holder, A. L., Chelly Dagdia, Z., Zeitouni, K., and Monnet, X. (2024). Should AI models be explainable to clinicians? Crit. Care 28:301. doi: 10.1186/s13054-024-05005-y
Asan, O., Bayrak, A. E., and Choudhury, A. (2020). Artificial intelligence and human trust in healthcare: focus on clinicians. J. Med. Internet Res. 22:e15154. doi: 10.2196/15154
Bergamin, J., Luigjes, J., Kiverstein, J., Bockting, C. L., and Denys, D. (2022). Defining autonomy in psychiatry. Front. Psych. 13:801415. doi: 10.3389/fpsyt.2022.801415
Chekroud, A. M., Bondar, J., Delgadillo, J., Doherty, G., Wasil, A., Fokkema, M., et al. (2021). The promise of machine learning in predicting treatment outcomes in psychiatry. World Psychiatry 20, 154–170. doi: 10.1002/wps.20882
Collins, G. S., Dhiman, P., Ma, J., Schlussel, M. M., Archer, L., van Calster, B., et al. (2024). Evaluation of clinical prediction models (part 1): from development to external validation. BMJ 384:e074819. doi: 10.1136/bmj-2023-074819
Conseil de recherches en sciences humaines du Canada. Énoncé de politique des trois Conseils: Éthique de la recherche avec des êtres humains, décembre 2022. Available online at: https://ethics.gc.ca (Accessed January 12, 2025).
Das, S., Sural, S., Vaidya, J., and Atluri, V. Poster: using Gini impurity to mine attribute-based access control policies with environment attributes. Proceedings of the 23nd ACM symposium on access control models and technologies. (2018): 213–215.
Ennab, M., and Mcheick, H. (2024). Enhancing interpretability and accuracy of AI models in healthcare: a comprehensive review on challenges and future directions. Front. Robot AI 11:1444763. doi: 10.3389/frobt.2024.1444763
Frank, D., Fan, E., Georghiou, A., and Verter, V. (2020). Community treatment order outcomes in Quebec: a unique jurisdiction. Can. J. Psychiatr. 65, 484–491. doi: 10.1177/0706743719892718
Goktas, P., and Grzybowski, A. (2025). Shaping the future of healthcare: ethical clinical challenges and pathways to trustworthy AI. J. Clin. Med. 14:1605. doi: 10.3390/jcm14051605
Guillaume, S., and Charnomordic, B. (2012). Fuzzy inference systems: an integrated modeling environment for collaboration between expert knowledge and data using FisPro. Expert Syst. Appl. 39, 8744–8755. doi: 10.1016/j.eswa.2012.01.206
Hao, J., Luo, S., and Pan, L. (2022). Rule extraction from biased random forest and fuzzy support vector machine for early diagnosis of diabetes. Sci. Rep. 12:9858 2022. doi: 10.1038/s41598-022-14143-8
Harris, C. R., Millman, K. J., van der Walt, S. J., Gommers, R., Virtanen, P., Cournapeau, D., et al. (2020). Array programming with NumPy. Nature 585, 357–362. doi: 10.1038/s41586-020-2649-2
Hicks, S. A., Strümke, I., Thambawita, V., Hammou, M., Riegler, M. A., Halvorsen, P., et al. (2022). On evaluation metrics for medical applications of artificial intelligence. Sci. Rep. 12:5979. doi: 10.1038/s41598-022-09954-8
Holzinger, A., Langs, G., Denk, H., Zatloukal, K., and Müller, H. (2019). Causability and explainability of artificial intelligence in medicine. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 9:e1312. doi: 10.1002/widm.1312
Jung, Y., and Hu, J. (2015). A K-fold averaging cross-validation procedure. J. Nonparametr. Stat. 27, 167–179. doi: 10.1080/10485252.2015.1010532
London, A. J. (2019). Artificial intelligence and black-box medical decisions: accuracy versus explainability. Hast. Cent. Rep. 49, 15–21. doi: 10.1002/hast.973
McCradden, M., Hui, K., and Buchman, D. Z. (2023). Evidence, ethics and the promise of artificial intelligence in psychiatry. J. Med. Ethics 49, 573–579. doi: 10.1136/jme-2022-108447
Mikellides, G., Stefani, A., and Tantele, M. (2019). Community treatment orders: international perspective. BJPsych Int. 16, 83–86. doi: 10.1192/bji.2019.4
Modai, I., Kuperman, J., Goldberg, I., Goldish, M., and Mendel, S. (2004). Fuzzy logic detection of medically serious suicide attempt records in major psychiatric disorders. J. Nerv. Ment. Dis. 192, 708–710. doi: 10.1097/01.nmd.0000142020.20038.dd
O'Reilly, R. L., Hastings, T., Chaimowitz, G. A., Neilson, G. E., Brooks, S. A., and Freeland, A. (2019). Community treatment orders and other forms of mandatory outpatient treatment. Can. J. Psychiatr. 64, 356–374. doi: 10.1177/0706743719845906
Owen, G. S., Richardson, G., David, A. S., Szmukler, G., Hayward, P., and Hotopf, M. (2008). Mental capacity to make decisions on treatment in people admitted to psychiatric hospitals: cross sectional study. BMJ 337:a448. doi: 10.1136/bmj.39580.546597.BE
Pedregosa, F., Varoquaux, G., Gramfort, A., Michel, V., Thirion, B., Grisel, O., et al. (2011). Scikit-learn: machine learning in Python. J. Mach. Learn. Res. 12, 2825–2830.
Pons, E. V., Salvador-Carulla, L., Calcedo-Barba, A., Paz, S., Messer, T., Pacciardi, B., et al. (2020). The capacity of schizophrenia and bipolar disorder individuals to make autonomous decisions about pharmacological treatments for their illness in real life: a scoping review. Health Sci. Rep. 3:e179. doi: 10.1002/hsr2.179
Raharjanti, N. W., Wiguna, T., Purwadianto, A., Soemantri, D., Bardosono, S., Poerwandari, E. K., et al. (2021). Clinical reasoning in forensic psychiatry: concepts, processes, and pitfalls. Front. Psych. 12:691377. doi: 10.3389/fpsyt.2021.691377
Raman, R., Kowalski, R., Achuthan, K., Iyer, A., and Nedungadi, P. (2025). Navigating artificial general intelligence development: societal, technological, ethical, and brain-inspired pathways. Sci. Rep. 15:8443. doi: 10.1038/s41598-025-92190-7
Rugkåsa, J. (2016). Effectiveness of community treatment orders: the international evidence. Can. J. Psychiatr. 61, 15–24. doi: 10.1177/0706743715620415
Saya, A., Brugnoli, C., Piazzi, G., Liberato, D., Di Ciaccia, G., Niolu, C., et al. (2019). Criteria, procedures, and future prospects of involuntary treatment in psychiatry around the world: a narrative review. Front. Psych. 10:271. doi: 10.3389/fpsyt.2019.00271
Shoaip, N., el-Sappagh, S., Abuhmed, T., and Elmogy, M. (2024). A dynamic fuzzy rule-based inference system using fuzzy inference with semantic reasoning. Sci. Rep. 14:4275. doi: 10.1038/s41598-024-54065-1
Sirocchi, C., Bogliolo, A., and Montagna, S. (2024). Medical-informed machine learning: integrating prior knowledge into medical decision systems. BMC Med. Inform. Decis. Mak. 24:186. doi: 10.1186/s12911-024-02582-4
Société québécoise d'information juridique. Trouver une décision. Available online at: https://citoyens.soquij.qc.ca/ (Accessed November 02, 2025).
Szmukler, G., and Holloway, F. (1998). Mental health legislation is now a harmful anachronism. Psychiatr. Bull. 22, 662–665. doi: 10.1192/pb.22.11.662
Torres, A., and Nieto, J. J. (2006). Fuzzy logic in medicine and bioinformatics. J. Biomed. Biotechnol. 2006:91908. doi: 10.1155/JBB/2006/91908
Waskom, M. L. (2021). Seaborn: statistical data visualization. J. Open Source Softw. 6:3021. doi: 10.21105/joss.03021
Keywords: fuzzy logic, Random Forest, psychiatric treatment orders, legal decision support, forensic psychiatry, machine learning, interpretability, law
Citation: Hudon A (2025) A hybrid fuzzy logic–Random Forest model to predict psychiatric treatment order outcomes: an interpretable tool for legal decision support. Front. Artif. Intell. 8:1606250. doi: 10.3389/frai.2025.1606250
Edited by:
Kim Tan, University of Nottingham, United KingdomReviewed by:
Shuai Xie, Changjiang River Scientific Research Institute (CRSRI), ChinaC. P. Lim, Swinburne University of Technology, Australia
Copyright © 2025 Hudon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Hudon, YWxleGFuZHJlLmh1ZG9uLjFAdW1vbnRyZWFsLmNh