 Helle Bøgard1*
Helle Bøgard1* Signe Green Knakkergaard1,2Charlotte Simonÿ1,2Lars Hermann Tang1,2
Signe Green Knakkergaard1,2Charlotte Simonÿ1,2Lars Hermann Tang1,2 Jeanette Reffstrup Christensen3,4,5Anne Dalhoff Pedersen1Alexander Luijk1,6Stine Gundtoft Roikjær1,7
Jeanette Reffstrup Christensen3,4,5Anne Dalhoff Pedersen1Alexander Luijk1,6Stine Gundtoft Roikjær1,7
- 1The Research and Implementation Unit PROgrez, Department of Physiotherapy and Occupational Therapy, Næstved-Slagelse-Ringsted Hospitals, Slagelse, Denmark
- 2The Department of Regional Health Research, University of Southern Denmark, Odense, Denmark
- 3Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark
- 4Research Unit for General Practice, Aarhus, Denmark
- 5DRIVEN – Danish Centre for Motivational and Behavior Science, Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark
- 6Centre for Health Research, Zealand University Hospital, Nykøbing Falster, Denmark
- 7Center for Health, University College Absalon, Roskilde, Denmark
Introduction: Rehabilitation needs are rising in the Nordic countries due to an aging population and declining health profiles. Nordic healthcare systems share common features, including universal access, organization, and substantial tax-based financing. Due to the organization of the healthcare system, patients often experience transitions between sectors as part of the rehabilitation program. This fragmented setup undermines the continuity and quality of rehabilitation, making implementation more difficult. To inform future implementation processes, this scoping review examines the factors that influence cross-sectoral rehabilitation in settings with comparable healthcare systems.
Methods: This Scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews. The search strategy aimed to identify published, peer-reviewed primary studies on interventions implemented in adult rehabilitation within Nordic countries. Data were charted following Levac et al.'s framework and analyzed using Elo & Kyngäs' content analysis to identify factors influencing implementation. Key study characteristics and implementation approaches were synthesized narratively and in tables.
Results: Thirty-six papers were identified. Most studies described the implementation of rehabilitation transitioning from the secondary to the primary sector. A top-down implementation approach was predominantly reported and appears more facilitating than a bottom-up approach. Implementation of rehabilitation across sectors is influenced by an interplay of factors: (1) Organization & Resources: alignment of context with intervention, involvement from front-line personnel, time & resources, the workplace itself, and managers, and (2) Collaboration & Communication, including knowledge and competence, attitudes, communication, patients, and families.
Conclusion: While this scoping review conveys that collaboration, communication, resources, and organization have a central role affecting the implementation of cross-sectoral rehabilitation, it further identifies knowledge gaps, such as the lack of the patients' perspective, the use of a framework or other systematic approach to ensure the success of the implementation.
Introduction
The population in the Nordic countries is aging rapidly (1), with over 20% now aged 65 years and older (2). Accompanying this increasing age brings a growing burden of chronic -and mental conditions, along with functional limitations. These issues often require complex journeys across multiple healthcare sectors (3). In this process, rehabilitation services become critical. They support individuals in regaining function, independence, and quality of life (4–6).
Nordic healthcare systems share features such as universal access, decentralization, and substantial tax-based financing. These systems cover the majority of healthcare expenditures (3). The healthcare services in Nordic countries are organized across primary, secondary, and sometimes, tertiary sectors. This structure leads to patient transitions between sectors and settings during rehabilitation (3). These transitions have challenged the continuity and quality of rehabilitation (7).
Current implementation research in Nordic countries and other comparable healthcare contexts has often focused on specific areas. These include transitional care for older adults (7), improvements in primary care (8) and mental health interventions (9, 10). Some studies have also focused the roles of particular professional groups, such as nurses (11). Although valuable, these studies do not fully capture the complexity of implementing cross-sectoral rehabilitation for the general adult population. A notable gap remains in understanding how to implement interventions that span multiple organizations. Such efforts often require collaboration among diverse professional groups across sectors. Implementation science recognizes that successfully integrating interventions into real-world settings is an iterative and dynamic process. It is also influenced by a range of ever-changing determinants (12). Defining and understanding these determinants is challenging, especially when interventions are not confined to a single context or profession. Successful cross-sectoral implementation may depend upon various fundamental components. These include stakeholder engagement, alignment of organizational missions, and use of an implementation framework. Interprofessional collaboration, and cultural adaptability within and across different healthcare settings are also essential (13–17). Contextual factors, such as institutional structures, resource availability, and normative values, can significantly shape the uptake, sustainability, and scalability of rehabilitation (7, 18, 19).
To advance implementation, it is crucial to investigate how these factors converge and influence cross-sectoral rehabilitation in settings where healthcare systems, financing models, and sociocultural values are relatively comparable (1, 2, 20). By focusing on the Nordic countries, we can explore processes and outcomes within similar welfare-based health systems and populations. This shared context provides a more controlled environment to identify factors that either facilitate or hinder successful implementations. Such insights can guide the design, adaptation, and evaluation of future interventions, ultimately optimizing the delivery of cross-sectoral rehabilitation services.
In light of these considerations, our scoping review aims to illuminate the factors, including both facilitators and barriers, that influence the implementation of cross-sectoral rehabilitation in Nordic healthcare settings. By synthesizing the available evidence, we seek to address current knowledge gaps, improve clarity on implementation strategies, and stimulate further development of context-specific implementation strategies. This endeavor enriches our understanding within the Nordic context. It also contributes broadly to the field of implementation science, offering transferable insights. These insights can support effective translation of evidence-based interventions across diverse healthcare systems and populations.
Aim
This scoping review aims to systematically examine and synthesize existing research on the cross-sectoral implementation of rehabilitation in Nordic health systems, focusing on factors that influence implementation processes to inform and support future implementation efforts.
Methods
A scoping review was chosen to examine the extent, nature, and range of existing peer-reviewed research literature on the implementation of rehabilitation (21). The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta- Analyses Extension for Scoping Reviews (PRISMA-ScR) (22). HB and SGR developed an initial study protocol (https://doi.org/10.17605/OSF.IO/XF6G2) to address the review objectives. A preliminary search was carried out to assess the available literature and refine the search strategy, aligning with the iterative process of the scoping review, which allows for revisiting earlier stages in response to unexpected findings and emerging insights. The scoping review study is not subject to ethical restrictions.
Eligibility criteria
To be eligible for inclusion in this review, the studies had to:
• Target an adult population aged 18 years or older
• Be conducted within a rehabilitative context
• Report on the implementation of an intervention
• Be located in a Nordic country
Rehabilitative intervention: The World Health Organization (WHO) (23) defines a rehabilitative intervention as “a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment”. These interventions were focused on care, physical, mental, and/or social outcomes and were either directed towards patients or aimed at the development and support of healthcare professionals or organizations (23).
Implementation
The included studies must evaluate the process and outcomes of implementation. Implementation was defined as the adoption and integration of evidence-based health interventions into routine practice within specific settings (24). This implementation of a rehabilitative intervention must occur in a cross-sectoral setting, meaning it was implemented across or within multiple sectors of the health system. The health system encompasses both public and private entities, including hospitals, municipalities, clinics, general practitioners, nursing homes, and rehabilitation centers.
Studies were excluded if they were: protocols, reviews, opinion pieces, editorials, conference proceedings, or published only as an abstract.
Data sources
The following databases were searched to identify relevant studies: MEDLINE (via OVID), EMBASE (via OVID), CINAHL (via EBSCOhost), Physiotherapy Evidence Database (PEDro), Occupational Therapy Systematic Evaluation of Evidence (OTseeker), Klinisk Sygepleje (via Idunn) and Web of Science. No limitations or restrictions were applied regarding language or date of publication. All databases were systematically searched in November 2023. The final search strategies can be found in Supplementary File S1. In addition, the full-text articles were hand-screened for additional records as well as run through Web of Science, adding a snowballing effect to the database search. All studies identified through the search strategy were uploaded into Covidence for study selection. Here, all duplicates were excluded.
Search strategy
The search strategy aimed to identify published, peer-reviewed primary studies. Grey literature was excluded to keep the scope of the review manageable and to ensure a transparent and reproducible search process. An initial search in Cochrane was conducted to expand the search and index terms. These keywords and index terms were tailored to each information source. Two information specialists peer-reviewed the search strategy in accordance with the PRESS guidelines (25).
A four-part PICO model consisting of Population, Intervention, Context/Setting, and Outcome (26) inspired and guided our search. For each component of the PICO model, a combination of Medical Subject Headings (MeSH), keywords, free-text terms, and word variants was employed to ensure comprehensive coverage. For the Population component, the focus was on adults aged 18 years and older residing in the Nordic countries, with country-specific identifiers such as Denmark, Danish, Sweden, Swedish, Norway, Norwegian, Finland, Finnish, Iceland, Icelandic. The Intervention component targeted rehabilitation-related concepts, including terms such as rehabilitation, exercise, physical activity, activities of daily living, leisure activities, recreational therapy. For the Context/Setting, the emphasis was on cross-sectoral care and transitional processes, with terms such as cross-sector, hospital discharge, continuity of patient care. Finally, the Outcome component focused on implementation processes and evaluations, with terms including implementation, outcome assessment, program development, quality control, delivery of health. This comprehensive search strategy was designed to capture relevant literature addressing the implementation and evaluation of rehabilitation interventions across sectors in Nordic adult populations (Supplementary File S1).
Study selection
To enhance consistency among reviewers, each reviewer initially screened 20 papers to become familiar with the inclusion and exclusion criteria and then discussed any questions or concerns regarding the screening process with HB. Following this, the inclusion and exclusion criteria were refined, particularly regarding the definitions of rehabilitative interventions and implementation evaluations. The exclusion criteria encompassed protocols, opinion papers, conference proceedings or similar, abstract-only and reviews and palliative rehabilitation articles. At least two reviewers independently (HB, AL, IU, TGH, SGK, SFH) screened titles and abstracts for eligible studies. Any disagreements were resolved by consensus between the two reviewers. If consensus could not be achieved, a third reviewer was consulted. Studies that passed the initial screening were then reviewed in full text by two reviewers (HB, SGK), who independently decided whether the study should be included. Disagreements were resolved by consensus between the two reviewers. Decisions were discussed and resolved with SGR if consensus could not be achieved.
Data extraction
The authors followed Levac et al.'s (26) recommendations for advancing scoping methodology to chart the data. A data charting form was developed to extract data from the studies included (Supplementary File S2). The items selected for extraction were chosen to give a thorough insight into each study on design, characteristics, and results and enable a basis for comparison between studies. Items for extraction are country of origin, year of publication, aim, study participants, sectors included, setting, methods, main conclusion, framework, top-down or bottom-up approach, intervention description and the implementers. Two reviewers (HB, SGK) independently charted the data, and then each reviewer verified the other's charting. Disagreements were discussed, and if consensus could not be reached, a third reviewer (SGR) was consulted. The charting process was iterative, and when it became evident that the organizational approach was an element of importance, an additional column with “Top-down, Bottom-up” was added. “Top-down” or “Bottom-up” referred to the implementation process' origin and lead, as to who decided and initiated the implementation. A top-down implementation is decided upon and administered from the top of an organization, for example a national cancer reform (27). A bottom-up implementation is driven and co-designed by the front line healthcare e.g., a patient trajectory where the healthcare professionals define challenges and propose solutions (28).
The charted characteristics are synthesized and presented narratively and in tables. All decisions were discussed between HB and SGK, and if there were any disagreements, SGR was consulted.
Data analysis
The content analysis with a deductive-inductive approach inspired by Elo & Kyngäs (29) was applied. The analysis was divided into three phases: preparation, organizing, and reporting. See Figure 1. The content analysis aims to attain a condensed and broad description of factors influencing the implementation, with categories describing this (29). During the preparation phase, reading the papers, it became evident that factors influencing the implementations process were distributed across various sections in each paper. These factors were identified as either facilitators, barriers or factors with an unspecified impact. All relevant factors were extracted grouped into subcategories. These subcategories were then refined into main categories. To ensure validity, the categorization process involved iterative comparison between individual factors and the emerging categories. Factors that were not clearly labeled in terms of their influence on the implementation were excluded from the results, as their impact remains unclear. The main categories for the factors acting as facilitators or barriers are depicted in the “results” section.
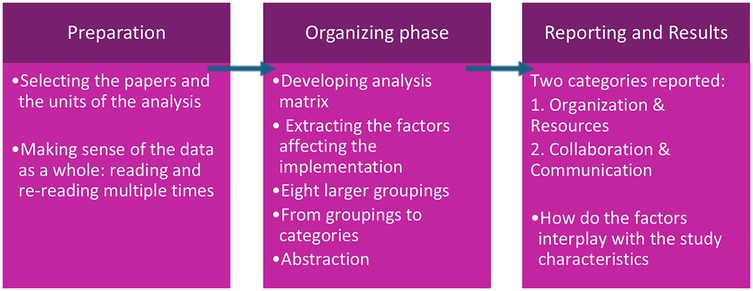
Figure 1. Phases in the content analysis.
Results
The presentation of the results is as follows: a description of the study characteristics, including study selection, design, organizational approach, population, setting, and framework. This will be followed by a presentation of the factors influencing implementation in two categories: Organization & Resources and Collaboration & Communication.
Study selection
The search took place on November 1, 2023. Initially, 4,630 citations were screened, with 4,425 deemed ineligible. We conducted full-text screening on 205 papers, of which 169 were excluded. Ultimately, 36 papers were included in the final stage (27, 28, 30–63). The primary reason for exclusion at this stage was that the studies were either only abstracts, only focused on one sector, or the studies lacked a focus on implementation. See Figure 2 The PRISMA flow chart.
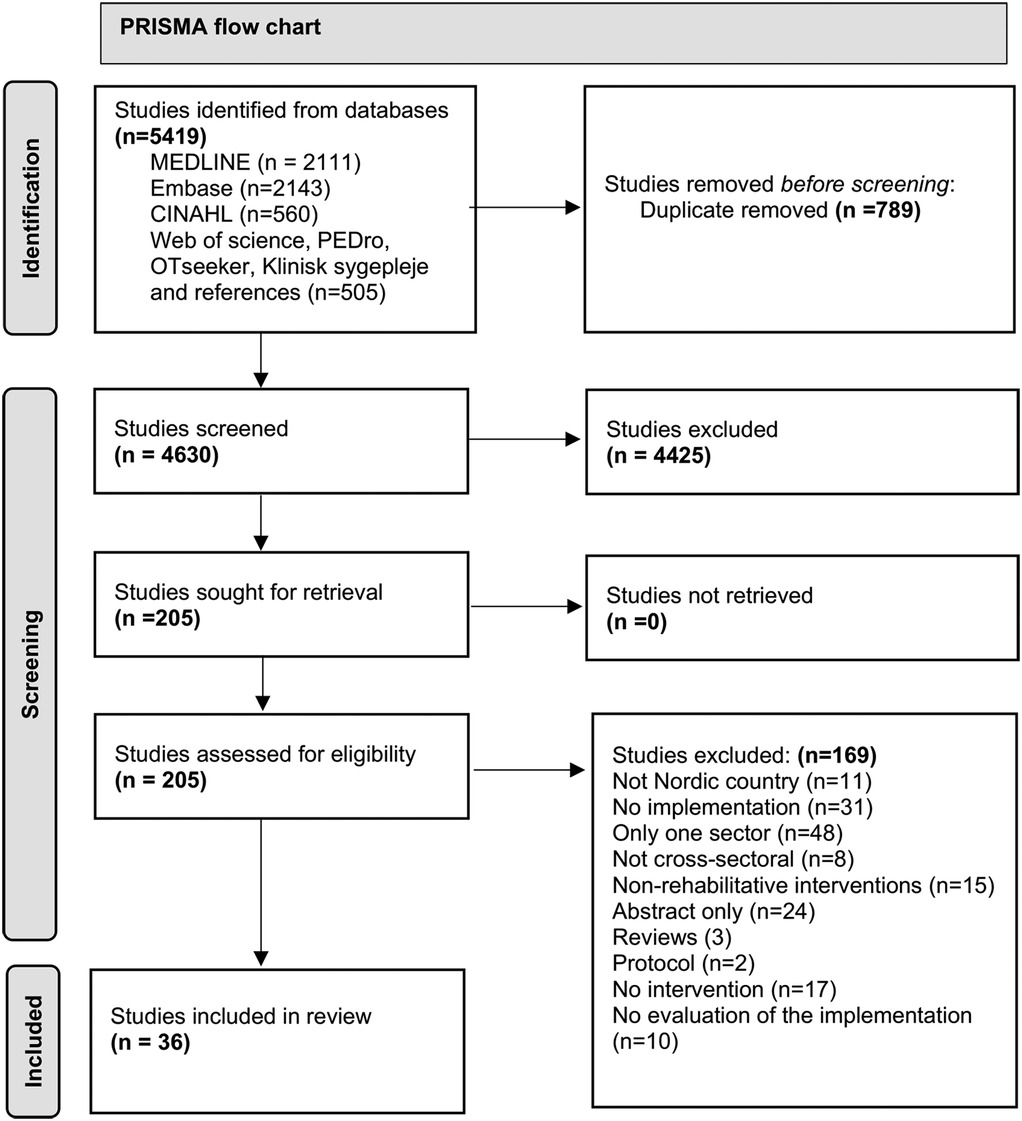
Figure 2. The PRISMA flow chart.
Study characteristics and design
The 36 papers included were published from 2000 to 2023, with 28 published from 2014 and onwards. Interventions were allocated across four of the five Nordic countries. Denmark (n = 15) (32, 33, 36, 39, 41, 45, 48–50, 56–58, 61–63), Sweden (n = 13) (27, 31, 34, 35, 37, 38, 40, 42, 44, 46, 47, 51, 54), Norway (n = 7) (28, 43, 52, 53, 55, 59, 60), and Finland (n = 1) (30). No studies were identified from Iceland. In terms of study design, six were quantitative, twenty qualitative, and ten employed mixed methods. Some papers reported results from the same original intervention but with different aims (37, 38, 46, 47, 59, 60).
Characteristics of the study participants
All interventions ultimately aimed to improve patient outcomes, but the interventions targeted various professions, which then influenced patient rehabilitation. In 28 studies, healthcare workers performed the implementation. The healthcare workers included were physiotherapists, occupational therapists, dieticians, psychologists, nurses, and nurses' assistants. A broad variation of other professions involved in implementation were physicians, general practitioners, pharmacists, managers/leaders, employment specialists, social insurance officers, discharge planning coordinators and researchers. Few studies included the patient as a part of the implementation process. Six studies included patient interviews as part of the evaluation (44, 48, 50, 59, 62), and two studies used questionnaires for patient evaluation (39, 41). A total of 29 studies did not ask for patients' opinions on how they were affected. See supplementary File S2.
Description of sectors for the implementation
Twenty-two papers (28, 32, 35, 39, 41, 43–51, 55, 56, 58–63) described interventions moving from the secondary sector to the primary sector, while only one paper described an intervention moving from the primary sector to the secondary sector (27). The secondary sector refers to hospitals of varying sizes, often involving one or more wards. The primary sector encompasses a wide range of settings, including in- and outpatient rehabilitation units, home care, and specialized units.
Thirteen papers described an intervention with more parallel characteristics, implemented in either two sectors (30, 33, 37, 38, 40, 42, 52, 54, 57) or within two entities of a single sector (31, 34, 36, 53). The implementation was presented as more parallel than integrated across sectors, without any obvious element bridging them. Eight of the 13 papers described parallel interventions in the primary and secondary sectors (30, 33, 37, 38, 40, 52, 54, 57), e.g., a screening tool for anxiety and depression being implemented simultaneously in both a hospital and a municipality setting (33). Five of the 13 papers described interventions implemented only within the primary sector (31, 34, 36, 42, 53), but from one entity to another within the sector, for example in a municipality setting between a mental health care unit and a vocational service unit (42).
Organizational approach to the implementation process
In 12 papers, the organizational approach to the implementation process was described as top-down (27, 30–32, 37, 39–42, 46, 52, 62). Three papers described a bottom-up approach (28, 44, 51), while two papers combined the two approaches (38, 54). Nineteen papers did not specify the approach (33–36, 43, 45, 47–50, 53, 55–61, 63). With regard to which organizational approach facilitates more successful implementation, all three papers employing a bottom-up approach report only limited success (28, 44, 51). As one paper highlights, “bottom-up process and enthusiasm are not enough” (p.8, Røsstad, 2015) (28). Conversely, top-down approaches appear to support the achievement of greater implementation success (27, 31, 32, 39, 41).
Frameworks
To examine whether utilizing a framework facilitates implementation, we searched the papers for the use of frameworks. Seventeen papers utilize implementation frameworks considering both context and individual perspectives. See supplementary File S2—data extraction chart. The frameworks are RE-AIM (30, 56), PARiHS (35, 49), Normalization Process Theory (28, 33), ERIC (38), CFIR (37), Model of strategic change management developed by Pettigrew and Whipp (31), Realistic Evaluation (63), Framework by Nielsen et al. (47), implementation outcomes described by Proctor et al. (40, 52), The Theoretical Domains Framework (61), Process evaluation by Saunders et al. (34, 62) and Process evaluation by Thorne (36).
Only one of the papers described using an implementation framework for both planning and evaluating the intervention (56). The majority of the papers employ a framework for evaluation only (30, 33, 35, 36, 40, 63) or for data analysis (28, 37, 38, 47, 61, 62). The remaining papers utilize the implementation framework for a theoretical framework (31, 49) or to structure or inspire the interview guide (34, 52). A search through the 36 papers' results and conclusions sections did not convey more success using a framework.
Factors influencing implementation
Factors reported as facilitators, barriers, or both were grouped into subcategories during analysis and later organized into two main categories: Organization & Resources and Collaboration & Communication (see Figure 3). Only the main categories are described narratively, while subcategories are shown in Figure 3 to illustrate the analytical process.

Figure 3. Categories and sub-categories of factors influencing the implementation.
The category of Organization & Resources encompasses factors that affect the implementation within the organizations, such as organizational structure, the teams and leadership roles, the operational procedures, and human resources, such as staffing and management. Financial resources, IT systems, and resource allocation are also in this category. As are the more evaluating factors.
Collaboration & Communication encompasses how teams, departments, and sectors work together, internal and external communication, and interaction with other stakeholders in the implementation. It also includes structures for discussions and decision-making, as well as other tools and strategies for a collaborative work environment.
Organization & resources
The alignment or especially misalignment of the intervention within the context is a frequently mentioned hindering factor. It is attributed to, e.g., inflexible policies, the structure of the intervention, the size of the workplaces, a patient population that differs from what the intervention requires (27, 30, 31, 33–36, 39, 42, 44, 49, 52, 53, 63) or the organizations working together differing in aims and perspectives (43, 45, 50, 62). A facilitator that can affect this factor is pilot testing or trialability, mentioned by several papers as part of the pre-implementation phases (30, 37). Additionally, involvement from the frontline personnel at all stages is a crucial facilitating factor for the implementation and for the intervention to be integrated and contextually appropriate (32, 33, 38, 46, 49, 50, 53, 56, 57, 61).
Time & Resources are factors of great influence, both acting as barriers and facilitators to the implementation process. Commonly cited barriers arise in the form of a lack of resources, high staff turnovers, and time-consuming tasks like forming new teams or recruiting new staff (28, 31, 37, 40, 44, 51, 54, 56, 57, 62). Facilitators are commonly seen in the form of management engagement, where management is often responsible for providing additional resources, such as adjusting task lists, supporting staff in dedicating the required time, and allocation and helping to prioritize time (28, 37, 56, 61, 62).
The time factor can act as a facilitator when there is sufficient time for planning and conducting the implementation (48, 61, 63) and as a barrier when time is perceived as insufficient (27, 28, 30, 31, 35, 36, 39, 40, 46–49, 52). Insufficient time can lead to a feeling of inadequate preparation among implementers and uncertainty about what to expect (28, 34, 36, 46, 53, 55) and can impact the ability to reflect on challenges, causing feelings of professionalism to be compromised (35, 36).
The workplace itself is a factor. A barrier is a workplace culture resistant to change (34, 36, 39, 42, 49). Support or encouragement from the workplace, including project leads, leaders, and colleagues, can act as a barrier when absent (35, 36, 60) and as a facilitator when present (47, 63). Additional facilitating support encompasses technical, organizational, and emotional assistance (47, 48). Having a person designated as the facilitator on-site (49) can aid in creating the sense of being part of a larger common agenda (49). Researchers can facilitate implementation by providing the right research evidence that aligns with the clinical practice needs (35). Project leads or trainers contribute to a barrier through insufficient informal workplace training, insufficient continuous support, and a lack of follow-up (33, 63).
Managers play a key role in the implementation process. They can be a barrier in the form of lack of support, due to absence from daily practice, or failing in providing leadership (33, 39, 46, 53, 62, 63). On the other hand, managers are frequently mentioned as facilitators (28, 33–35, 49, 53, 54, 56, 60–63). Facilitating management involves showing commitment and drive, being encouraging and responsive, as well as being realistic and concise. Formal requirements and mandatory participation facilitate implementation (33, 62). The factors and the number of papers that include each factor are depicted in Figure 4.
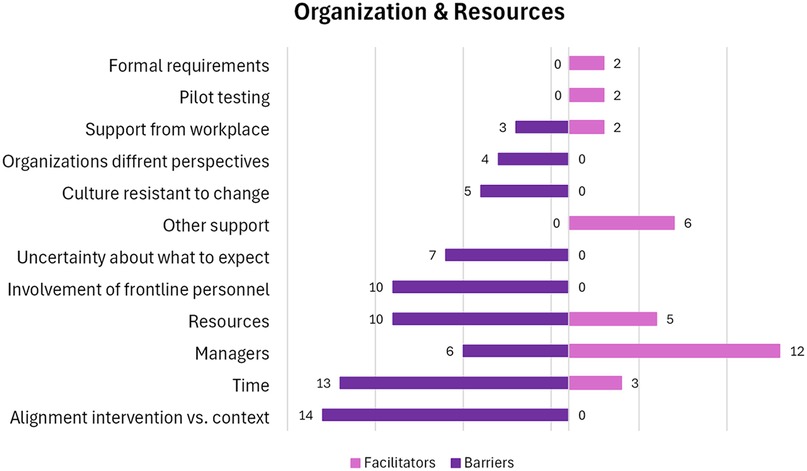
Figure 4. Number of papers within each factor in the category “Organization & Resources”. A visual presentation of the number of papers that holds facilitators and barriers within each factor.
Collaboration & communication
Knowledge and competence among staff regarding the intervention are identified as a factor that is a barrier to implementation when there is a lack of knowledge and a feeling of lack of competence towards the intervention (31–33, 37, 44, 49, 55) or lack of knowledge of each other's work (42, 56, 62). However, it can be a facilitator through educational activities (33–35, 38, 52, 54, 62, 63), including workshops, meetings, and education on relevant evidence. Knowledge sharing between staff at meetings or audits was a valuable resource; discussions and communication made the interventions meaningful for staff (31, 34, 35, 39, 49, 53, 56, 57, 59, 61), as well as training in a real environment (35, 47, 52, 63), and learning through their own experience (33, 35, 55, 63). These activities helped staff feel prepared to implement the intervention.
Attitudes among staff are a factor that holds both barriers and facilitators. Attitudes can be a barrier when there is a lack of motivation, a perception of no need for change or resistance towards change, and skepticism towards other professions and their capabilities that complicate collaboration (31, 34, 39, 42, 44, 45, 50, 54). Attitude is a facilitating factor when it includes mutual interest, active engagement from all parties, increasing awareness, positive expectations, respect towards the practitioners’ roles from managers and researchers, and a sense of responsibility towards practicing improvement (31, 33–36, 41, 46, 54, 56, 57, 61, 62).
Communication is a factor that can facilitate collaboration (36, 39, 45–47, 54, 60, 62). This includes more structured communication, guidelines, and communication at all levels within and across organizations. The setting for communication must be developed in the specific context of cross-sectoral work. This is also the case for documentation flow and systematic processes, such as referrals that were a facilitator when functioning (34, 35, 39, 41, 43, 44, 52, 53, 62) and an important factor for cross-sectoral communication. Working towards a shared goal can be both facilitating when it occurs (34, 39) and a barrier when not (44, 45, 50, 54). Communication can be a barrier when respect is lacking, e.g., researchers have to respect stakeholders' knowledge and expertise in their respective fields (35, 59).
Patients and their families can be a factor that serves as a barrier when they are dissatisfied with the information provided, as it was either repetitive or contradictory to previous information received (33, 63). The factors and the number of papers that include each factor are depicted in Figure 5.
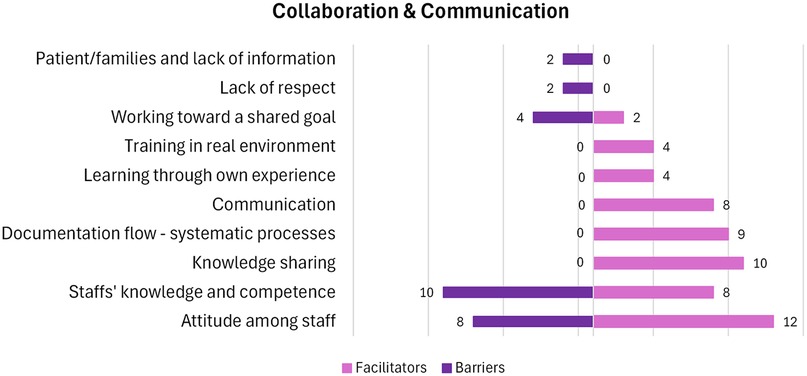
Figure 5. Number of papers within each factor in the category “Collaboration & Communication”. A visual presentation of the number of papers that hold facilitators and barriers within each factor.
Discussion
This scoping review examined existing research on the cross-sectoral implementation of rehabilitation in Nordic health systems, focusing on barriers and facilitators that influence the implementation processes. Synthesizing the research reveals that most interventions reported took place during patients' transitions from hospital to primary care in Denmark, Sweden, and Norway. Results consist of a) the characteristics of the studies as to the country, implementers, sectors, organizational approach and frameworks and b) categories of factors that can affect the implementation process: Organization & Resources and Collaboration & Communication.
Considering the PICO elements guiding the review, the included studies addressed broad Populations, typically adults with varying rehabilitation needs, though details on diagnosis and impairments were inconsistently reported. The Interventions ranged from exercise and person-centered care to discharge planning, screening tools, and structured rehabilitation programs. Most were implemented in cross-sectoral Contexts/Settings, particularly transitions from secondary (hospital) to primary or community care, while others described more parallel sectoral initiatives. The Outcomes most often reported related to implementation processes—such as feasibility, staff engagement, and organizational alignment, whereas direct patient outcomes and perspectives were less frequently included. This imbalance suggests that while organizational and professional experiences are well-documented, patients' needs, goals, and barriers to service use remain underexplored (64).
Several findings warrant further discussion. Notably, most of the studies included were published from 2014 onwards. This trend aligns with a corresponding increase in the scholarly use of the term implementation, as evidenced by a PubMed search (65) showing a doubling of such articles between 2014 and 2024. This trend may be interpreted in light of the growing focus in implementation research in general, an emphasis on rehabilitation service's needs, and the recognition of persistent challenges in translating evidence into clinical practice (66). Bunger et al. (67) similarly underscore the necessity for more precise and systematic reporting of implementation strategies to facilitate replicability and cumulative knowledge development within the field. Surprisingly, our review did not identify a common or standardized framework for conducting or reporting implementation processes across the included papers. The absence of such structured approaches further highlights the pressing need for the establishment of standardized methodologies to enhance comparability, rigor, and transparency in future research endeavors.
Our findings show a top-down organizational approach to implementation is most frequently applied and appears to be more facilitating than a bottom-up approach. Top-down processes seem to succeed particularly when they involve mandatory participation or strong leadership characterized by visible support, commitment, and realistic goal setting, while also ensuring the involvement of front-line personnel and stakeholders. This reliance on top-down strategies has important implications for policy design. It suggests that centralized leadership and formal structures may provide the necessary authority and resources to drive cross-sectoral implementation but also raises concerns about flexibility and ownership at the local level. Bottom-up approaches, although less frequently reported as successful, may still be viable under conditions where front-line staff are well-prepared, supported, and empowered to adapt interventions to local contexts. Co-designing strategies, as highlighted by Manalili et al. (68), or a more inclusive approach that engage front-line personnel early (65, 66), may help bridge the gap between top-down directives and bottom-up ownership. Without adequate preparation however, involvement of front-line personnel can hinder rather than support implementation, as shown when healthcare professionals are unprepared for new roles and transitions (67). The focus on context during implementation is highlighted by Skivington et al. in the Medical Research Council (MRC) framework of complex interventions (14), by van Scherpenseel et al. (69), and in The Implementation in Context (ICON) framework by Squires et al., which has a specific focus on the importance of analyzing the context of the intervention (17). Unexpectedly, when a comparison of the results of this scoping review was made with the core elements in the MRC (14) and ICON frameworks (17), we found that there was a lack of focus on adapting or refining the implementation throughout the implementation period. Although the results in this scoping review do highlight some importance of interorganizational relationships, these relationships should play an even greater role in cross-sectoral implementation according to the ICON framework (18).
Another major gap identified in the comparison was the limited involvement of stakeholders, particularly patients. Consequently, most studies included in this scoping review concentrate on the intervention and evaluation of healthcare personnel, with only a few incorporating the patients' perspectives. Patient involvement is widely recognized as essential across all research settings (70, 71). Therefore, it is a significant limitation that these studies do not report on patient involvement, and the potential impact on the implementations remains unexplored. The lack of patient involvement contradicts the more inclusive practice by the MRC, the ICON framework and Eskerod et al.'s (72) project management theory. The last which holds the concept of 'stakeholder inclusiveness', which entails recognizing and addressing the needs and concerns of all stakeholders, regardless of their level of influence or potential impact on the project (72).
Aligning with Proctor et al. (73), who argue that the strategic application of frameworks or other systematic approaches can enhance implementation success, we searched the papers for the use of implementation frameworks. Notably, the seventeen interventions which employed an implementation framework that accounted for both contextual factors and individual perspectives, primarily used it for evaluation purposes rather than for planning or guiding the implementation process. This limited use may be attributed to the wide variety of available frameworks and the lack of consensus on which to apply (17, 74). An emphasis on the early phases of implementation is advocated by Alley et al. (75), as to a thorough investigation of stakeholder engagement, feasibility, and organizational readiness during the pre-implementation phase, factors that according to Alley et al. (75) will significantly enhance the likelihood of successful implementation. There should be a focus on strengthening this in future implementation processes.
Strengths and limitations
We consider the broad scope of rehabilitation focused on care, physical, mental, and/or social outcomes a strength in our effort to identify factors affecting cross-sectoral implementation. The papers in this scoping review, although covering various rehabilitative areas, all contribute to valuable knowledge for future implementations efforts. A strength of this study is that we not only searched in the larger databases but also in databases targeted at rehabilitation, such as PEDro, OTseeker, and journal of Klinisk Sygepleje (Clinical Nursing), and in the search for relevant papers, included a citation search in Web of Science. Also, we adhere to the PRISMA-ScR recommendations and reporting standards, the consultation with information specialists in deciding the search strategy, and the use of multiple reviewers in all phases.
This review has limitations. Firstly, despite using an extensive search strategy, we may have missed some publications as the research papers do not always clearly describe the setting or focus on implementation and a more precise and established terminology could have increased the number of relevant studies found. However, the potential loss of relevant studies was minimized by hand-screening for additional records as well as by using Web Of Science. Secondly, only published studies were included, and grey literature and unpublished studies were excluded. While this decision supported feasibility and transparency of the review process, it may have biased the findings toward academic and clinical perspectives, underrepresenting practice-based or policy-level insights. Thirdly, sector-specific studies were excluded, which means that contextual factors unique to single-sector settings were not captured. Whether these differ substantially from those influencing cross-sectoral implementation is unknown and warrants further research. Fourthly, a third of the included studies, despite having a cross-sectoral design, described a more parallel implementation without a clear element bridging sectors. These studies are presented and included. Thus, the facilitators and barriers for cross-sectorial implementation are still experienced in a multiple-sector setting. Several factors that seem to affect the implementation were not labelled or distinguished by the authors as to what effect they had on the implementation and could possibly hold valuable knowledge. Finally, consistent with scoping review methodology, we did not appraise the quality of the studies included. This lack of critical appraisal means the strength of evidence underlying individual findings cannot be assessed within this review. Readers interested in evaluating the robustness of particular studies are therefore encouraged to explore the articles included independently.
Conclusion
Evidence from this scoping review shows that the two most reported factors influencing implementation are lack of time and resources (Organization & Resources) and staff attitudes and competencies (Collaboration & Communication). Other barriers include poor alignment between interventions and context, limited frontline involvement, negative staff attitudes, and lack of knowledge. Facilitators include strong managerial support, engaged stakeholders, knowledge sharing, and effective communication and documentation flows. The knowledge presented in this review is drawn from studies conducted in Denmark, Sweden, and Norway, with no eligible studies identified from Finland or Iceland.
Based on these findings, four key recommendations for implementing cross-sectoral rehabilitation can be made:
1. Allocate resources and time to adequately prepare for implementation and support sustainability.
2. Ensure strong and committed leadership, ideally with clear top-down support, to drive and coordinate the process.
3. Involve stakeholders early, including frontline personnel, to build engagement, competence, and shared ownership.
4. Foster adaptive and context-sensitive processes, including systematic communication, shared documentation, and opportunities for dialogue and refinement.
Author contributions
HB: Conceptualization, Writing – original draft, Writing – review & editing, Formal analysis, Methodology, Data curation. SG: Formal analysis, Writing – original draft, Writing – review & editing, Data curation. CS: Conceptualization, Writing – review & editing. LT: Writing – review & editing. JC: Supervision, Writing – review & editing. AD: Conceptualization, Project administration, Writing – review & editing. AL: Data curation, Writing – review & editing. SG: Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The research is funded by a grant from Region Zealand (Project: Exercise First).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2025.1662230/full#supplementary-material
References
1. Jørgensen TSH, Fors S, Nilsson CJ, Enroth L, Aaltonen M, Sundberg L, et al. Ageing populations in the nordic countries: mortality and longevity from 1990 to 2014. Scand J Public Health. (2019) 47(6):611–7. doi: 10.1177/1403494818780024
2. Nordic Co-operation. The population of the Nordic Region (2024). Available online at: https://www.norden.org/en/information/population-nordic-region (Accessed December 3, 2024).
3. Laugesen K, Ludvigsson JF, Schmidt M, Gissler M, Valdimarsdottir UA, Lunde A, et al. Nordic health registry-based research: a review of health care systems and key registries. Clin Epidemiol. (2021) 19(13):533–54. doi: 10.2147/CLEP.S314959
4. European Observatory on Health Systems and Policies. Norway: Health System Summary. Copenhagen: WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (2022). Available online at: https://eurohealthobservatory.who.int/publications/i/norway-health-system-summary (Accessed October 1, 2024).
5. The Ministry of Health. Healthcare in Denmark: an overview (2017). Available online at: https://sum.dk/Media/C/A/Healthcare-in%20denmark%20an%20overview%20english-V16-dec.pdf (Accessed September 12, 2023).
6. Larsen AT. Primary Health Care in the Nordic Countries – Comparative Analysis and Identification of Challenges.
7. Fakha A, Groenvynck L, de Boer B, van Achterberg T, Hamers J, Verbeek H. A myriad of factors influencing the implementation of transitional care innovations: a scoping review. Implement Sci. (2021) 16:21. doi: 10.1186/s13012-021-01087-2
8. McGilton KS, Vellani S, Krassikova A, Robertson S, Irwin C, Cumal A, et al. Understanding transitional care programs for older adults who experience delayed discharge: a scoping review. BMC Geriatr. (2021) 21(1):210. doi: 10.1186/s12877-021-02099-9
9. Khatri R, Endalamaw A, Erku D, Wolka E, Nigatu F, Zewdie A, et al. Continuity and care coordination of primary health care: a scoping review. BMC Health Serv Res. (2023) 23(1):750. doi: 10.1186/s12913-023-09718-8
10. Jørgensen K, Rasmussen T, Hansen M, Andreasson K. Recovery-oriented intersectoral care between mental health hospitals and community mental health services: an integrative review. Int J Soc Psychiatry. (2021) 67(6):788–800. doi: 10.1177/0020764020966634
11. Lemetti T, Stolt M, Rickard N, Suhonen R. Collaboration between hospital and primary care nurses: a literature review. Int Nurs Rev. (2015) 62(2):248–66. doi: 10.1111/inr.12147
12. Powell BJ, Fernandez ME, Williams NJ, Aarons GA, Beidas RS, Lewis CC, et al. Enhancing the impact of implementation strategies in healthcare: a research agenda. Front Public Health. (2019) 22(7):3. doi: 10.3389/fpubh.2019.00003
13. Fernandez ME, Ruiter RAC, Markham CM, Kok G. Intervention mapping: theory- and evidence-based health promotion program planning: perspective and examples. Front Public Health. (2019) 14(7):209. doi: 10.3389/fpubh.2019.00209
14. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of medical research council guidance. Br Med J. (2021) 30:n2061. doi: 10.1136/bmj.n2061
15. Petersen HV, Foged S, Nørholm V. “It is two worlds” cross-sectoral nurse collaboration related to care transitions: a qualitative study. J Clin Nurs. (2019) 28(9–10):1999–2008. doi: 10.1111/jocn.14805
16. Bryson J, Crosby B, Stone M. The design and implementation of cross-sector collaborations: propositions from the literature. Public Adm Rev. (2006) 1(66):44–55. doi: 10.1111/j.1540-6210.2006.00665.x
17. Squires JE, Graham ID, Santos WJ, Hutchinson AM, The ICON Team. The implementation in context (ICON) framework: a meta-framework of context domains, attributes and features in healthcare. Health Res Policy Sys. (2023) 21(1):81. doi: 10.1186/s12961-023-01028-z
18. Lengnick-Hall R, Willging CE, Hurlburt MS, Aarons GA. Incorporators, early investors, and learners: a longitudinal study of organizational adaptation during EBP implementation and sustainment. Implement Sci. (2020) 15(1):74. doi: 10.1186/s13012-020-01031-w
19. Fakha A, Leithaus M, de Boer B, van Achterberg T, Hamers JP, Verbeek H. Implementing four transitional care interventions for older adults: a retrospective collective case study. Gerontologist. (2022) 63(3):451–66. doi: 10.1093/geront/gnac128
20. Kristiansen IS, Pedersen KM. Health care systems in the nordic countries–more similarities than differences? Tidsskr Nor Laegeforen. (2000) 120(17):2023–9. Available online at: https://pubmed.ncbi.nlm.nih.gov/11008540/11008540
21. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
22. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169(7):467–73. doi: 10.7326/M18-0850
23. WHO. Rehabilitation (2025). Available online at: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (Accessed September 12, 2023).
24. Wolfenden L, Goldman S, Stacey FG, Grady A, Kingsland M, Williams CM, et al. Strategies to improve the implementation of workplace-based policies or practices targeting tobacco, alcohol, diet, physical activity and obesity. Cochrane Database Syst Rev. (2018) 2018(11):CD012439. doi: 10.1002/14651858.CD012439.pub2
25. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. (2016) 75:40–6. doi: 10.1016/j.jclinepi.2016.01.021
26. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5(1):69. doi: 10.1186/1748-5908-5-69
27. Schmidt I, Thor J, Davidson T, Nilsson F, Carlsson C. The national program on standardized cancer care pathways in Sweden: observations and findings half way through. Health Policy. (2018) 122(9):945–8. doi: 10.1016/j.healthpol.2018.07.012
28. Røsstad T, Garåsen H, Steinsbekk A, Håland E, Kristoffersen L, Grimsmo A. Implementing a care pathway for elderly patients, a comparative qualitative process evaluation in primary care. BMC Health Serv Res. (2015) 15(1):86. doi: 10.1186/s12913-015-0751-1
29. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. (2008) 62(1):107–15. doi: 10.1111/j.1365-2648.2007.04569.x
30. Aittasalo M, Miilunpalo S, Ståhl T, Kukkonen-Harjula K. From innovation to practice: initiation, implementation and evaluation of a physician-based physical activity promotion programme in Finland. Health Promot Int. (2007) 22(1):19–27. doi: 10.1093/heapro/dal040
31. Brämberg EB, Klinga C, Jensen I, Busch H, Bergström G, Brommels M, et al. Implementation of evidence-based rehabilitation for non-specific back pain and common mental health problems: a process evaluation of a nationwide initiative. BMC Health Serv Res. (2015) 15(1):79. doi: 10.1186/s12913-015-0740-4
32. Douw K, Nielsen CP, Pedersen CR. Centralising acute stroke care and moving care to the community in a Danish health region: challenges in implementing a stroke care reform. Health Policy. (2015) 119(8):1005–10. doi: 10.1016/j.healthpol.2015.05.007
33. Egholm CL, Helmark C, Rossau HK, Munkehøj P, Brøndum S, Pedersen SS, et al. Implementation of systematic screening for anxiety and depression in cardiac rehabilitation: real world lessons from a longitudinal study. J Psychosom Res. (2022) 158:110909. doi: 10.1016/j.jpsychores.2022.110909
34. Eklund M, Argentzell E. Implementing an occupational therapy specific mental health intervention in a multi-professional context—the case of balancing everyday life (BEL). Scand J Occup Ther. (2023) 30(2):182–94. doi: 10.1080/11038128.2021.1998608
35. Eriksson C, Eriksson G, Johansson U, Guidetti S. Occupational therapists’ perceptions of implementing a client-centered intervention in close collaboration with researchers: a mixed methods study. Scand J Occup Ther. (2020) 27(2):142–53. doi: 10.1080/11038128.2019.1573917
36. Faymonville L, Schmidt AM, Handberg C. Implementation of a multidisciplinary rehabilitation program for patients with chronic low back pain—experiences and perspectives of rehabilitation team members. J Eval Clin Pract. (2021) 27(2):377–84. doi: 10.1111/jep.13441
37. Fridberg H, Wallin L, Tistad M. The innovation characteristics of person-centred care as perceived by healthcare professionals: an interview study employing a deductive-inductive content analysis guided by the consolidated framework for implementation research. BMC Health Serv Res. (2021) 21(1):904. doi: 10.1186/s12913-021-06942-y
38. Fridberg H, Wallin L, Tistad M. Tracking, naming, specifying, and comparing implementation strategies for person-centred care in a real-world setting: a case study with seven embedded units. BMC Health Serv Res. (2022) 22(1):1409. doi: 10.1186/s12913-022-08846-x
39. Frølich A, Høst D, Schnor H, Nørgaard A, Ravn-Jensen C, Borg E, et al. Integration of healthcare rehabilitation in chronic conditions. Int J Integr Care. (2010) 10:e033. doi: 10.5334/ijic.507
40. Gyllensten H, Tistad M, Fridberg H, Wallin L. Analysis on personnel costs and working time for implementing a more person-centred care approach: a case study with embedded units in a Swedish region. BMJ Open. (2023) 13(10):e073829. doi: 10.1136/bmjopen-2023-073829
41. Hansen VB, Haslev VP, Kring A, Buch MS. [Inter-sectoral coordination of rehabilitation can reduce the number of dropouts from chronic heart disease courses]. Ugeskr Laeger. (2014) 176(5):V10120632.25096009
42. Hasson H, Andersson M, Bejerholm U. Barriers in implementation of evidence-based practice: supported employment in Swedish context. J Health Organ Manag. (2011) 25(3):332–45. doi: 10.1108/14777261111143563
43. Henriksen BT, Krogseth M, Andersen RD, Davies MN, Nguyen CT, Mathiesen L, et al. Clinical pharmacist intervention to improve medication safety for hip fracture patients through secondary and primary care settings: a nonrandomised controlled trial. J Orthop Surg Res. (2023) 18(1):434. doi: 10.1186/s13018-023-03906-2
44. Henriksen E, Rosenqvist U. Understanding and practice: a 7-year follow-up study on implementation of a cardiac rehabilitation program. Qual Health Res. (2002) 12(5):671–84. doi: 10.1177/104973202129120179
45. Hjelmar U, Hendriksen C, Hansen K. Motivation to take part in integrated care—an assessment of follow-up home visits to elderly persons. Int J Integr Care. (2011) 11:e122. doi: 10.5334/ijic.649
46. Hofflander M, Nilsson L, Eriksén S, Borg C. Healthcare Managers’ experiences of leading the implementation of video conferencing in discharge planning sessions: an interview study. CIN: Comput Inform Nurs. (2016) 34(3):108–15. doi: 10.1097/CIN.0000000000000217
47. Hofflander M, Nilsson L, Eriksén S, Borg C. Framing the implementation process of video conferencing in discharge planning–according to staff experience. Inform Health Soc Care. (2016) 41(2):192–209. doi: 10.3109/17538157.2015.1008484
48. Juncher AE, Hansen N, Jürgensen KSL, Frølund B, Jørgensen LM. [Functional training of enfeebled elderly in their own homes. A cross-disciplinary and cross-sectorial model]. Ugeskr Laeger. (2002) 164(20):2623–7.12043406
49. Kristensen HK, Hounsgaard L. Implementation of coherent, evidence-based pathways in Danish rehabilitation practice. Disabil Rehabil. (2013) 35(23):2021–8. doi: 10.3109/09638288.2013.768301
50. Ladekjær Larsen E, Jensen JM, Pedersen KMH. Cross-sectorial collaboration in return to work interventions: perspectives from patients, mental health care professionals and case managers in the social insurance sector. Disabil Rehabil. (2022) 44(11):2317–24. doi: 10.1080/09638288.2020.1830310
51. Lilja M, Nygård L, Borell L. The transfer of information about geriatric clients in the occupational therapy chain of care: an intervention study. Scand J Occup Ther. (2000) 7(2):51–9. doi: 10.1080/110381200750018841
52. Mathisen TS, Eilertsen G, Ormstad H, Falkenberg HK. ‘If we don’t assess the patient’s vision, we risk starting at the wrong end’: a qualitative evaluation of a stroke service knowledge translation project. BMC Health Serv Res. (2022) 22(1):351. doi: 10.1186/s12913-022-07732-w
53. Moe C, Brinchmann B, Rasmussen L, Brandseth OL, McDaid D, Killackey E, et al. Implementing individual placement and support (IPS): the experiences of employment specialists in the early implementation phase of IPS in northern Norway. The IPSNOR study. BMC Psychiatry. (2021) 21(1):632. doi: 10.1186/s12888-021-03644-x
54. Moore L, Britten N, Lydahl D, Naldemirci Ö, Elam M, Wolf A. Barriers and facilitators to the implementation of person-centred care in different healthcare contexts. Scand J Caring Sci. (2017) 31(4):662–73. doi: 10.1111/scs.12376
55. Netteland G. Improving handovers between hospitals and primary care: implementation of E-messages and the importance of training. Stud Health Technol Inform. (2017) 235:564–8. doi: 10.3233/978-1-61499-753-5-564
56. Poulsen LK, Ilvig PM, Brendstrup L, Rasmussen CL, Pedersen KA, Ditlevsen P, et al. Development, implementation and evaluation of an optimized cross-sectoral rehabilitation program after acute hip fracture surgery: a mixed-methods study. Eval Program Plann. (2022) 91:102021. doi: 10.1016/j.evalprogplan.2021.102021
57. Stenov V, Wind G, Vallis M, Reventlow S, Hempler NF. Group-based, person-centered diabetes self-management education: healthcare professionals’ implementation of new approaches. BMC Health Serv Res. (2019) 19(1):368. doi: 10.1186/s12913-019-4183-1
58. Villumsen M, Livbjerg AE, Grarup B, Kjeldal Skram C, Laessoe U. Implementation of a municipality-based rehabilitation program for patients with neuritis vestibularis: lessons learned and derived snowball effects. Physiother Theory Pract. (2023) 39(4):761–71. doi: 10.1080/09593985.2022.2030829
59. Worum H, Lillekroken D, Ahlsen B, Roaldsen KS, Bergland A. Bridging the gap between research-based knowledge and clinical practice: a qualitative examination of patients and physiotherapists’ views on the Otago exercise programme. BMC Geriatr. (2019) 19(1):278. doi: 10.1186/s12877-019-1309-6
60. Worum H, Lillekroken D, Ahlsen B, Roaldsen KS, Bergland A. Otago exercise programme—from evidence to practice: a qualitative study of physiotherapists’ perceptions of the importance of organisational factors of leadership, context and culture for knowledge translation in Norway. BMC Health Serv Res. (2020) 20(1):985. doi: 10.1186/s12913-020-05853-8
61. Petersen HV, Sivertsen DM, Jørgensen LM, Petersen J, Kirk JW. From expected to actual barriers and facilitators when implementing a new screening tool: a qualitative study applying the theoretical domains framework. J Clin Nurs. (2023) 32(11–12):2867–79. doi: 10.1111/jocn.16410
62. Martin MHT, Moefelt L, Nielsen MBD, Rugulies R. Barriers and facilitators for implementation of a return-to-work intervention for sickness absence beneficiaries with mental health problems: results from three Danish municipalities. Scand J Public Health. (2015) 43(4):423–31. doi: 10.1177/1403494814568484
63. Eriksen S, Dahler AM, Øye C. The informal way to success or failure? Findings from a comparative case study on video consultation training and implementation in two Danish hospitals. BMC Health Serv Res. (2023) 23(1):1135. doi: 10.1186/s12913-023-10163-w
64. Doyle C, Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open. (2013) 3(1):e001570. doi: 10.1136/bmjopen-2012-001570
65. Churruca K, Ludlow K, Taylor N, Long JC, Best S, Braithwaite J. The time has come: embedded implementation research for health care improvement. J Eval Clin Pract. (2019) 25(3):373–80. doi: 10.1111/jep.13100
66. Simonÿ C, Riber C, Bodtger U, Birkelund R. Striving for confidence and satisfaction in everyday life with chronic obstructive pulmonary disease: rationale and content of the tele-rehabilitation programme > C☺PD-Life>>. Int J Environ Res Public Health. (2019) 16(18):3320. doi: 10.3390/ijerph16183320
67. Sterling MR, Dell N, Tseng E, Okeke F, Cho J, Piantella B, et al. Home care workers caring for adults with heart failure need better access to training and technology: a role for implementation science. J Clin Transl Sci. (2020) 4(3):224–8. doi: 10.1017/cts.2020.36
68. Manalili K, Scott CM, Hemmelgarn B, O’Beirne M, Bailey AL, Haener MK, et al. Co-designing person-centred quality indicator implementation for primary care in Alberta: a consensus study. Res Involve Engage. (2022) 8(1):59. doi: 10.1186/s40900-022-00397-z
69. van Scherpenseel MC, te Velde SJ, Veenhof C, Emmelot-Vonk MH, Barten JA. Contextual determinants influencing the implementation of fall prevention in the community: a scoping review. Front Health Serv. (2023) 3:1138517. doi: 10.3389/frhs.2023.1138517
70. Smits DW, van Meeteren K, Klem M, Alsem M, Ketelaar M. Designing a tool to support patient and public involvement in research projects: the involvement matrix. Res Involve Engage. (2020) 6(1):30. doi: 10.1186/s40900-020-00188-4
71. de Wit M, Beurskens A, Piškur B, Stoffers E, Moser A. Preparing researchers for patient and public involvement in scientific research: development of a hands-on learning approach through action research. Health Expect. (2018) 21(4):752–63. doi: 10.1111/hex.12671
72. Eskerod P, Huemann M, Ringhofer C. Stakeholder inclusiveness: enriching project management with general stakeholder theory. Proj Manag J. (2015) 46(6):42–53. doi: 10.1002/pmj.21546
73. Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. (2011) 38(2):65–76. doi: 10.1007/s10488-010-0319-7
74. Waltz TJ, Powell BJ, Fernández ME, Abadie B, Damschroder LJ. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. (2019) 14(1):42. doi: 10.1186/s13012-019-0892-4
Keywords: cross-sectoral, implementation, rehabilitation, Nordic welfare systems, organization
Citation: Bøgard H, Green Knakkergaard S, Simonÿ C, Tang LH, Christensen JR, Dalhoff Pedersen A, Luijk A and Gundtoft Roikjær S (2025) Implementation of cross-sectoral rehabilitation in the Nordic countries: a scoping review. Front. Health Serv. 5:1662230. doi: 10.3389/frhs.2025.1662230
Received: 8 July 2025; Accepted: 2 September 2025;
Published: 19 September 2025.
Edited by:
Martina Giusti, University of Florence, ItalyReviewed by:
Stefano Doronzio, IRCCS Don Carlo Gnocchi Firenze, ItalyTuğba Aksakal, Witten/Herdecke University, Germany
Copyright: © 2025 Bøgard, Green Knakkergaard, Simonÿ, Tang, Christensen, Dalhoff Pedersen, Luijk and Gundtoft Roikjær. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helle Bøgard, aGJvZ2FAcmVnaW9uc2phZWxsYW5kLmRr