 Guadalupe Lizzbett Luna-Rodríguez1
Guadalupe Lizzbett Luna-Rodríguez1 Viridiana Peláez-Hernández1*
Viridiana Peláez-Hernández1* Arturo Orea-Tejeda1Celia Deyanira Ledesma-Ruíz1Fernando Casarín-López1Adrían Rosas-Trujillo1Benjamín Domínguez-Trejo2
Arturo Orea-Tejeda1Celia Deyanira Ledesma-Ruíz1Fernando Casarín-López1Adrían Rosas-Trujillo1Benjamín Domínguez-Trejo2 Li Erandi Tepepa-Flores2
Li Erandi Tepepa-Flores2- 1Cardiology Service of the Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City, Mexico
- 2Faculty of Psychology, Universidad Nacional Autónoma de México, Mexico City, Mexico
Introduction: Among the different psychological sequelae of post-COVID syndrome are symptoms related to emotional impairment, mostly depression, anxiety, and post-traumatic stress disorder (PTSD).
Objective: To describe and compare the prevalence and severity of PTSD, anxiety, depression, and fear of COVID-19 in survivors 3 months after discharge from the hospital.
Methods: A cross-sectional descriptive study was conducted, a total of 227 survivors of COVID-19 participated; they were assessed 3 months after being discharged from the hospital. A psychological evaluation focused on anxiety, depression, PTSD, and fear was conducted. Statistical analysis through the t-test for independent samples was performed.
Results: Of the patients, 64.5% were men, 60.9% required invasive mechanical ventilation (IMV) during hospitalization, and the average age was about 48.23 ± 14.33 years. Also, 40% showed symptoms associated with PTSD, 38.4% exhibited anxiety, 36.6% depression, and 36.12% exhibited fear of COVID-19. There were statistically significant differences between men and women, in PTSD (t = -3.414, df = 224, p = 0.001, x̅m = 5.10, x̅w = 6.32), depression (t = -4.680, df = 225, p = 0.000, x̅m = 3.64, x̅w = 7.18), anxiety (t = -3.427, df = 152.53, p = 0.001, x̅m = 3.78, x̅w = 6.20), and fear of COVID-19 (t = -3.400, df = 224, p = 0.001, x̅m = 11.88, x̅w = 15.19). Furthermore, there were also statistically significant differences between the type of treatment during hospitalization (IMV vs. without IMV), in PTSD (t = 2.482, df = 223, p = 0.014, x̅IMV = 5.21, x̅WIMV = 6.08) and anxiety (t = -2.006, df = 223, p = 0.046, x̅IMV = 4.05, x̅WIMV = 5.44).
Conclusion: Survivors of COVID-19 experience a high prevalence of PTSD, anxiety, depression, and fear, even 3 months after discharge from the hospital. Females and patients who did not require IMV during hospitalization are the most affected population, presenting more severe symptoms of these psychological alterations. More research is required to know and observe the long-term evolution of these psychological alterations in this population.

1 Introduction
The SARS-CoV-2 coronavirus outbreak in China spread rapidly around the world, generating a major health emergency (Velavan and Meyer, 2020). At the time of writing this article, 496 million confirmed cases and 6.17 million deaths have been reported worldwide. COVID-19 is a condition caused by the coronavirus SARS-CoV-2, and this infection present symptoms such as fever, cough, and shortness of breath (Ciotti et al., 2020).
Throughout the course of the pandemic, it has been observed that some of the patients who had recovered from the acute phase of the infection began to present persistent symptoms, which constitute a new post-infectious syndrome called “post-COVID-19 syndrome,” which is defined as a set of signs and symptoms that develop after an infection compatible with COVID-19, persisting beyond 12 weeks and are not explained by an alternative diagnosis (Bender del Busto, 2022). This has also been observed in other infections such as Epstein–Bar, Coxiella Burnetti, or Lyme disease (Boix and Merino, 2022).
The incidence of this syndrome has been reported mostly in patients with mild or severe COVID-19, regardless of the severity of symptoms in the acute phase. Between 10 and 65% of survivors who suffered mild or moderate COVID-19 present symptoms of post-COVID-19 syndrome for 12 weeks or more (Carod-Artal, 2018), in addition, more than 80 long-term symptoms have been identified, with duration and severity still unknown, but producing a negative impact on the health and quality of life at short and long-term (Bender del Busto, 2022; Boix and Merino, 2022).
Among the most frequently reported symptoms are physical, psychological, cognitive, and neurological alterations, such as chronic illness, fatigue, dyspnea, pain, cough, dysphagia, anxiety, depression, post-traumatic stress disorder (PTSD), obsessive compulsive disorder (OCD), concentration problems, memory loss, sleep disorders, and headache (Halpin et al., 2021; Mazza et al., 2020; Moreno-Pérez et al., 2021; Nalbandian et al., 2021; Xiong et al., 2021). On the other hand, it is estimated that 75% of survivors experienced at least one physical or psychological symptom 6 months after hospital discharge, where 23% reported feeling fatigue or muscle weakness, 23% reported depression or anxiety, and 26% reported sleep problems (Huang et al., 2021). A similar prevalence of psychological symptoms has been observed in the aftermath of other coronavirus infections, where nearly 40% of survivors of SARS and MERS epidemics in Asian and Middle Eastern countries reported symptoms associated with anxiety, depression, OCD, and PTSD after 1 month of the acute period of infection and even during follow-up 50 months later (Cheng et al., 2004; Lam et al., 2009; Moldofsky and Patcai, 2011; Du et al., 2020; Rogers et al., 2020).
Hospitalization due to COVID-19 is an event that generates an elevated level of stress, and the experience could even become traumatic. One of the prevalent psychological disorders among survivors is PTSD (Chen et al., 2021), which is caused mainly by exposure to a highly stressful or traumatic situation (Brady et al., 2000; Carvajal, 2002); it is commonly developed in the short or long term, and even in other infectious epidemics caused by SARS and MERS (Mak et al., 2009; Mak et al., 2010), survivors reported presenting symptoms associated with PTSD. Furthermore, comorbidities are frequently observed, especially in anxiety and depression, where comorbidity rates range from 21–94% for depression and 39–97% for anxiety (Ginzburg et al., 2010; Mak et al., 2009). The presence of comorbidities increases symptoms, aggravating the alterations and increasing the difficulties associated with psychological treatment (Chen et al., 2021).
The etiology related to post-COVID-19 syndrome includes a set of immunological alterations triggered during the acute period of infection. The exacerbated cellular inflammatory process increases the probability of developing psychological disorders such as PTSD, anxiety, or depression (Najjar et al., 2013; Miller and Raison, 2016), which when coupled with psychosocial vulnerability factors during recovery such as a continued fear of illness, contagion, uncertain future, stigma, discrimination, and traumatic memories of hospitalization and social isolation (Brooks et al., 2020; Carvalho et al., 2020; Mazza et al., 2020), could play a fundamental role within the onset, severity, and maintenance duration of psychological diseases associated with post-COVID-19 syndrome.
The duration and prevalence of the psychological symptoms of post-COVID-19 syndrome are not yet known (Table 1). Thus, the aim of our study was to describe and compare the prevalence and severity of PTSD, anxiety, depression, and fear of COVID-19 in COVID-19 survivors, 3 months after hospital discharge in a Latin American context.
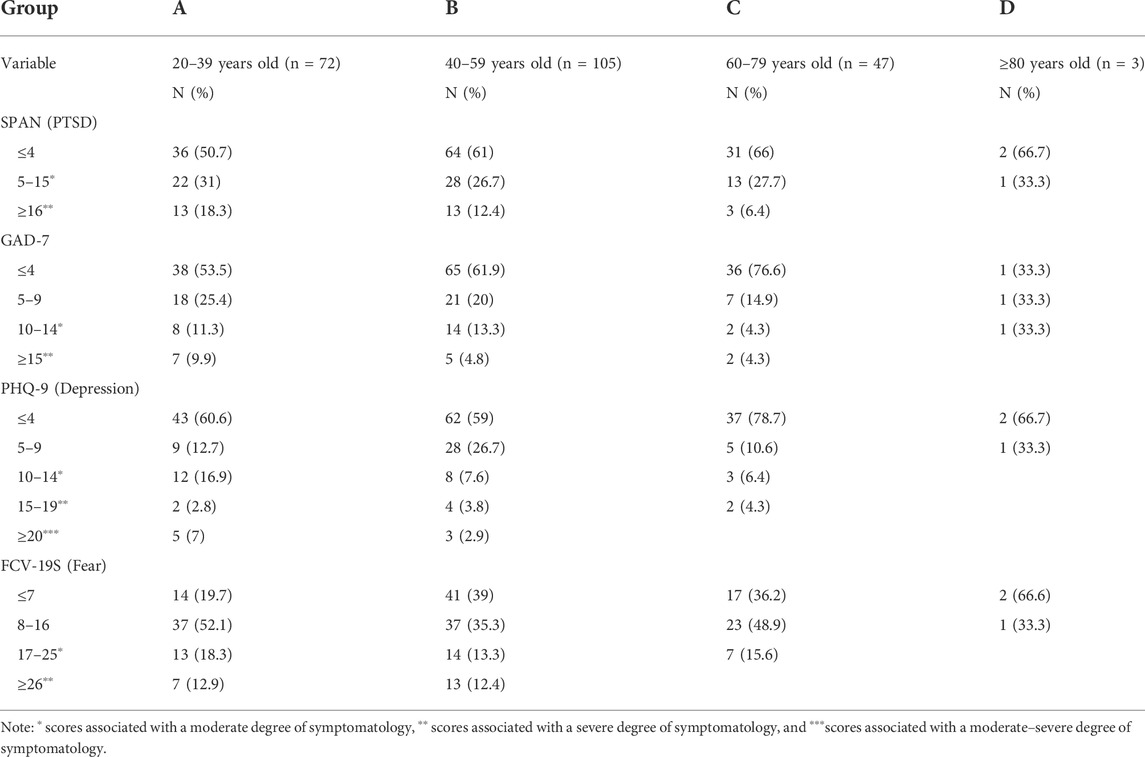
TABLE 1. Prevalence of PTSD, anxiety, depression, and fear according to age group.
2 Methods and materials
2.1.1 Participants
A total of 227 COVID-19 survivors, 3 months after discharge from hospitalization, participated in the study. The participants are part of a prospective cohort study in COVID-19 survivors conducted by the Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas. The psychological assessments were conducted from August 2021 to January 2022. Previously, each patient was given informed consent, detailing the characteristics and objectives of the study. The present study was approved by the Institutional Ethics Committee in accordance with the principles of the Declaration of Helsinki.
2.2 Data collection and measurement
Sociodemographic and clinical data were obtained from each patient’s clinical record and from a structured interview during the psychological assessment. Psychological assessment was performed by trained and qualified psychologists using the following psychometric tests.
The Davidson Brief Trauma Scale (SPAN) (Meltzer-Brody et al., 1999), an abbreviated version of the Davidson Trauma Scale, focused on assessing physiological and cognitive components present in PTSD symptomatology. It consists of four items, with a Likert-type response scale ranging from 1–5, obtaining a minimum final score of 4 and a maximum of 20. Final scores higher than 5 show a sensitivity of 0.69 and specificity of 0.95 for the diagnosis of PTSD (Meltzer-Brody et al., 1999). The validity and reliability in the Spanish-speaking population (Campo-Arias et al., 2020), obtained a Kaiser–Meyer–Olkin index of 0.714, Bartlett’s chi square = 783.3 (gl = 6; p = 0.001), α = 0.66, and eigenvalue of 1.99, explained about 49.7% of the variance. In the confirmatory factor analysis was obtained x2 = 5.921, df = 2, p = 0.052, RMSEA = 0.037 [CI 90% 0.000-0.072], CFI = 0.955, Tucker–Lewis Index = 0.985, SMRM = 0.011, a Cronbach’s α = 0.66, and an Omega coefficient = 0.69.
The Generalized Anxiety Scale (GAD-7) (Spitzer et al., 2006) is based on seven items that evaluate the presence and frequency of symptoms associated with anxiety. The response options are offered on a Likert-type scale with values from 0–3, with the total score ranging from 0–3. The total score ranges from minimum values of zero to maximum values of 21 points. Scores of 10–14 are associated with a moderate level of anxious symptomatology and values greater than or equal to 15 with severe symptomatology (Table 1). The validation in the Mexican population (Gutiérrez-Velilla et al., 2022) obtained a Cronbach´s α = 0.82, a single factor explained 48.8% of variance, and the confirmatory analysis showed a model fit adequately (CFI = 0.0991, CMIN/DF = 1.924, RMSEA = 0.042, and SMRMR = 0.026).
The Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001) is an abbreviated version of the Patient Health Questionnaire. It consists of nine items aimed to assess the presence and frequency of symptoms associated with depression. The responses are based on a Likert-type scale with values from 0–3, allowing a minimum total score of 0 and a maximum of 27. Scores of 10–14 are associated with a moderate level of depressive symptomatology, from 15 to 19 with moderate–severe levels, and scores greater than or equal to 20 with severe symptoms. Validation in the Mexican population (Arrieta et al., 2017) obtained a Cronbach´s α = 0.80 and showed a model fit adequately (CFI = 0.91, Bentler–Bannet non-normed index = 0.88, RMSEA = 0.09, and ROC = 0.85 (95% CI [0.84-0.94]).
The COVID-19 Fear Scale (FCV-19S) (Ahorsu et al., 2020): Mexican version of the COVID-19 Fear Scale (García-Reyna et al., 2022). It is composed of seven items that assess the severity, presence, and frequency of physiological, emotional, and behavioral responses associated with the fear of COVID-19. The response options are through a Likert-type scale with values from 1–5, obtaining total scores of a minimum of 7 and a maximum of 35. High scores are related to a more severe fear response (Table 2). The internal reliability showed a Cronbach´s alpha of 0.90 and the confirmatory factor analysis showed a good model fit (x2 (7) = 29.40, p < 0.001; CFI = 0.99; TLI = 0.99; RMSEA = 0.03; SRMR = 0.010; and AIC = 71.40).
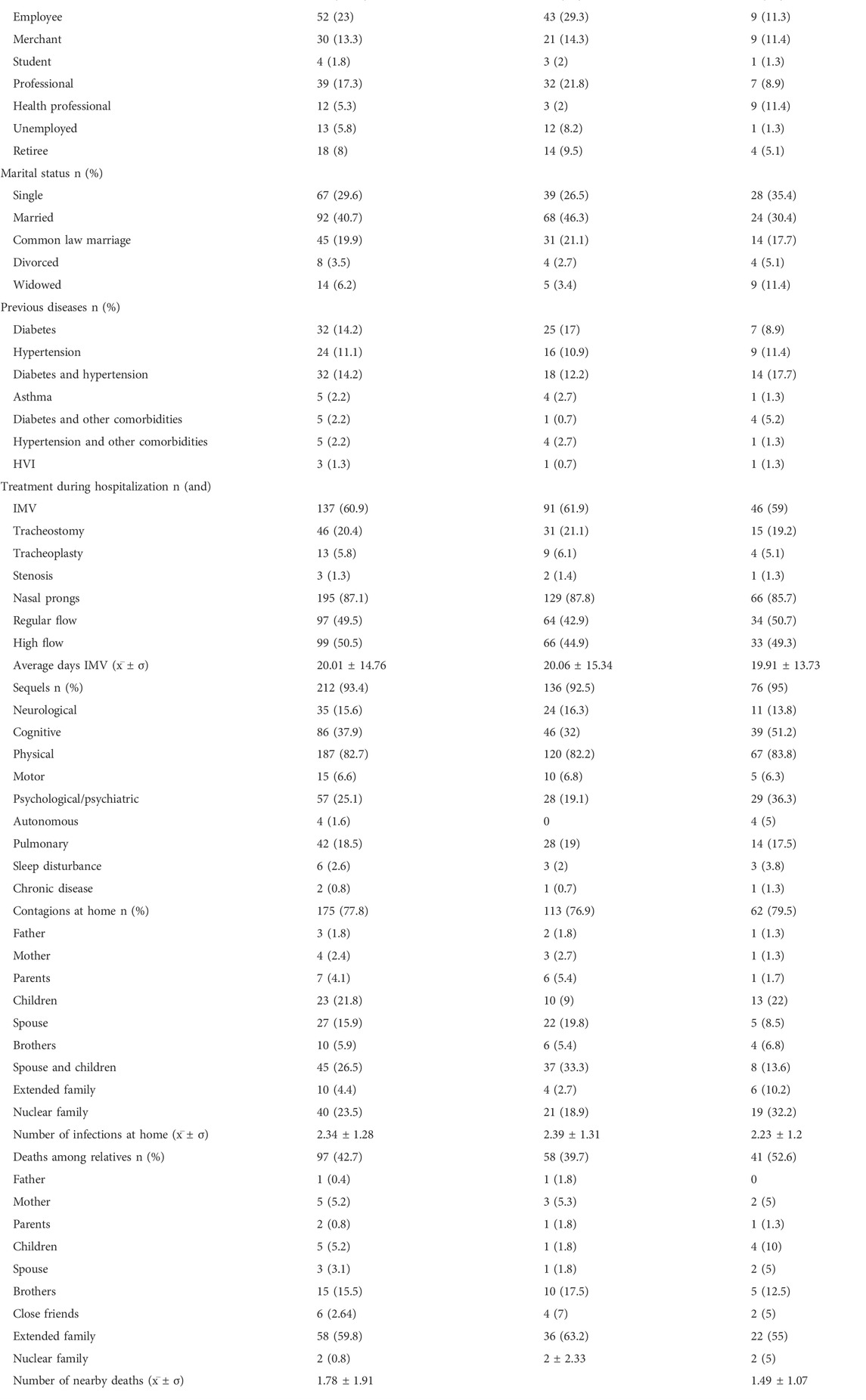
TABLE 2. Sociodemographic and clinical characteristics of surviving COVID-19 patients.
2.3 Statistical analysis
The clinical and sociodemographic characteristics of the patients were analyzed by descriptive analysis. The Kolmogorov–Smirnoff statistical test was used to verify the normal distribution of the data, finding in all analyzed variables, values p > 0.05; for this reason, we decided to use parametric tests for the comparative statistical analysis and to determine the prevalence of PTSD symptoms, anxiety, depression, and fear in men and women according to the type of treatment received during hospitalization. Descriptive and statistical analyses were performed to determine whether there were statistically significant differences in the presence of symptoms associated with PTSD, anxiety, depression, and fear between men and women, in the type of treatment received in hospitalization, and by age group. Student’s t-test for independent samples and a variance test (ANOVA) were performed, in addition to calculating the effect size and statistical power. The analyses were performed using SPSS version 26 and G power version 3.1 statistical software. Statistical significance was established at p < 0.05.
3 Results
The mean age of COVID-19 survivor patients was 48.23 ± 14.33 years, 64.75% were male, and a smaller percentage was composed of female patients (35.24%). Most patients had an education of the basic level (24.3%) or at least a bachelor’s degree (28.8%). It was observed that men had a higher unemployment rate than women (8.2 vs 1.3%). Most of the patients were married (40.7%) or single (29.6%); men were mostly married (46.3%) while women were mostly single (35.4%). Medical history indicates that among the chronic diseases previously diagnosed are diabetes (14.2%), hypertension (11.1%), and diabetes and hypertension (14.2%) affecting more men than women. Invasive mechanical ventilation (IMV) was required by 60.9% of the patients, with similar percentages in both sexes. Physical (82.7%), cognitive (37.9%), and psychological or psychiatric (25.1%) alterations were the most prevalent, with cognitive and psychological sequelae affecting mostly women (5.2 and 36.3%, respectively). Among the rate of infection and mortality in the patients’ families, it was found that 77.8% reported having close relatives infected with COVID-19 during the same time they became ill, with an average of 2.34 ± 1.28 contagions, with their respective partners and children (26.5%) being the ones who were mostly infected; however, men referred that their partners were the ones who were mostly infected (19.8%) and women referred that their nuclear family members were the ones who were most frequently infected (32.2%). Meanwhile, 42.73% of patients reported the loss of a close family member or friend, with an average of 1.78 ± 1.91 close deaths. The losses affected more women (55.6%). Deaths of close extended family members were the most reported (59.8%), which were mostly present in men (63.2%).
To determine the prevalence of symptom severity for each of the psychological variables evaluated, percentages were analyzed based on score ranges associated with moderate to severe symptomatology both in the overall sample and the differences between sexes and based on inpatient treatment (Table 3). Mean scores associated with PTSD indicated that mild to moderate symptoms were found in 40.2% of patients, affecting mostly women (51.9%) and patients who did not require IMV (48.9%), while severe symptoms were found in only 0.9%, affecting only women (2.5%). Moderate anxiety symptoms affected 11.5% of the patients, with a similar prevalence in men and women and in the type of treatment during hospitalization, while severe symptoms affected 6.2% of the population, occurring more in patients without IMV (10.2%). The prevalence of moderate depressive symptomatology was found in 10.6% of patients, affecting mostly women (17.5%), with no apparent differences between the types of inpatient treatment; moderate–severe levels affect 4%, mostly men (4.1%) and patients without IMV (8%). Clinically severe depressive symptoms affect about 3.5% of patients, continuing with a higher presence in women (7.5%) with no differences from inpatient treatment. The prevalence of symptoms associated with fear produced by COVID-19 indicates that moderate levels are found in 17.3% of patients, where the percentages are similar for both sexes (19% in men and 17.5% in women) and in hospital treatment (17.5% for patients with IMV and 17% for patients without IMV); severe symptoms were present in 8.84% of patients, affecting mostly women (16.13%), but without important differences after inpatient treatment. In addition, the prevalence of PTSD, anxiety, depression, and fear symptoms according to the age group (Table 4) showed that the younger group (A) presented a high percentage of moderate and clinically severe PTSD symptoms (31 and 18.3% respectively) compared with the other group age, while moderate anxiety symptoms were more prevalent in group B (13.3%). In addition, clinically severe anxiety symptoms affect about 10% of the younger patients (group A). The prevalence of moderate and clinically severe depressive symptomatology was found in 17 and 7% of the younger patients, compared with the other group age. The prevalence of symptoms associated with fear produced by COVID-19 indicates that moderate levels are found between 12 and 18.3%, where the percentages are similar in groups A, B, and C.
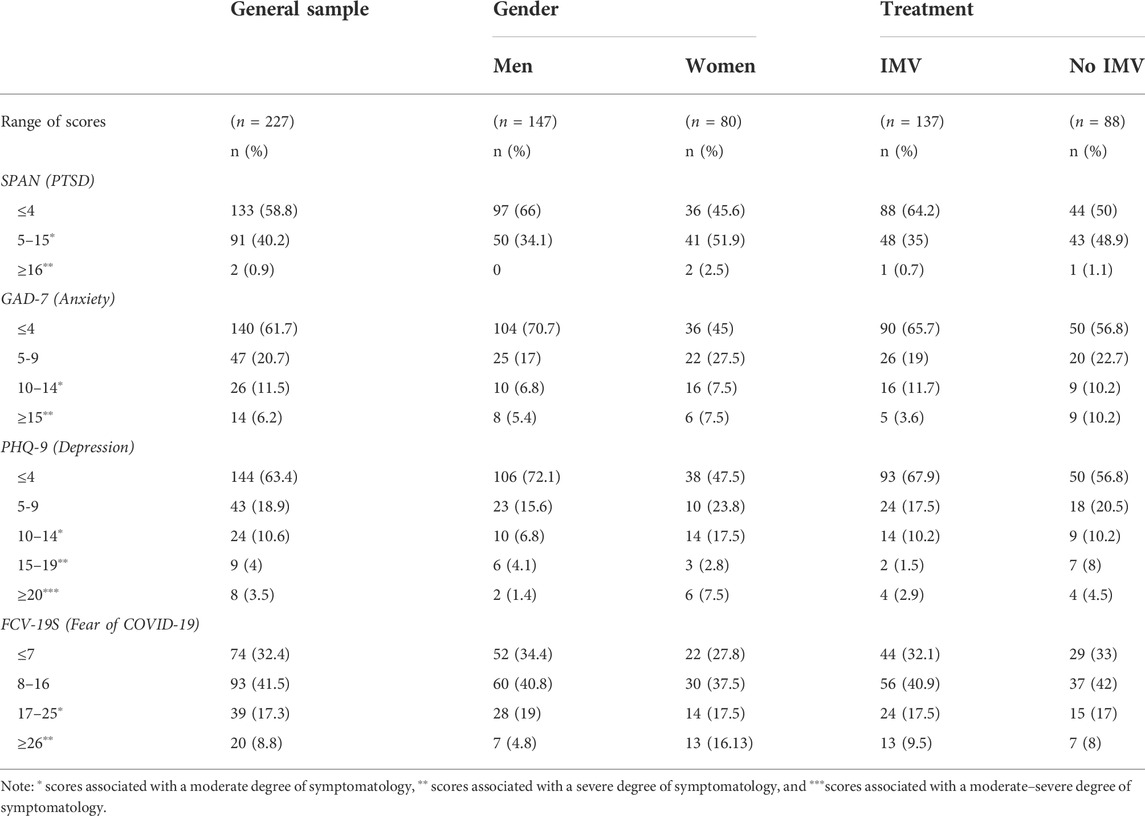
TABLE 3. Prevalence of PTSD, anxiety, depression, and fear according to sex and type of treatment used in hospitalization.
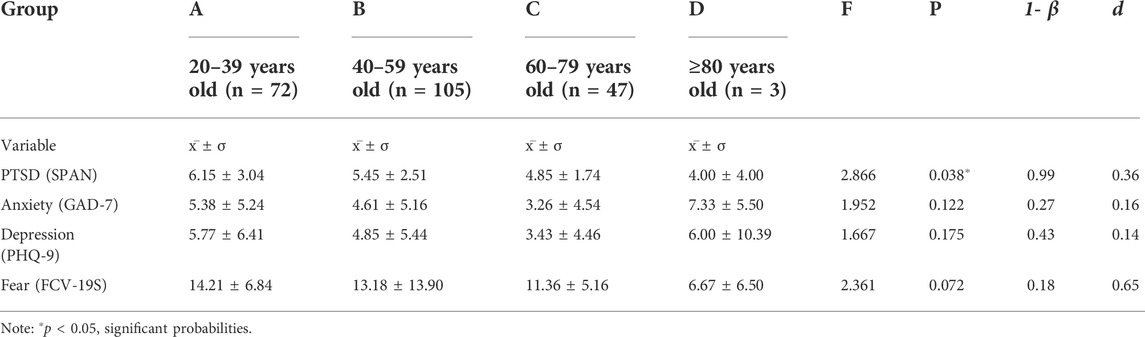
TABLE 4. Differences between age groups in the PTSD, anxiety, depression, and fear to covid-19 scores.
We analyzed whether there were statistically significant differences in PTSD, anxiety, depression, and fear scores between sexes and type of hospital treatment (Tables 2, 5), finding statistically significant differences between men and women in PTSD (t (111.58) = -2.08 p =0 .003, CI 95% [-2.020, -0.409]), 1-β =0 .45, d = 0.44) with a mean for men of 5.10 ± 2.05 and a mean for women of 6.32 ± 3.28, in anxiety (t (225) = -3.50 p =.001, 95% CI [-3.789, -1.060]), 1-β =0 .54, d = 0.48) with a mean for men of 3.78 ± 4.85 and a mean for women of 6.20 ± 5.21, in depression (t (133.01) = -4.36, p < 0.001, 95% CI [-5.138, -1.933]), 1- β =0 .87, d = 0.62) with a mean for men of 3.64 ± 4.93 and a mean for women of 7.18 ± 6.26 and in fear (t (123.85) = -3.10, p=.002, CI 95% [-5.415, -1.196]), 1-β =0 .46, d = 0.45) with a mean for men of 11.88 ± 6.10 and a mean for women of 15.19 ± 8.34.
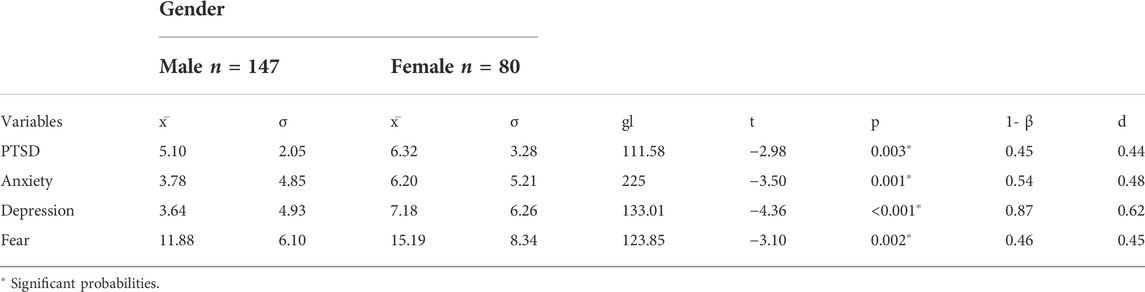
TABLE 5. Gender differences in PTSD, anxiety, depression, and fear scores.
Statistically significant differences were also observed between the type of inpatient treatment used (Table 5) in PTSD (t (145.93) = -2.32, p=.022, 95% CI [-1.607, -0.129]), 1-β =0 .53, d = 0.32) with a mean for patients requiring IMV of 5.21 ± 2.21 and a mean for patients without IMV of 6.08 ± 3.02 and anxiety (t (223) = -2.00, p=0.046, 95% CI [-2.759, -0.025]), 1-β =0 .89, d = 0.26) with a mean for patients requiring IMV of 4.05 ± 4.71 and a mean for patients without IMV of 5.44 ± 5.59.
The patients were divided into four groups based on their age: group A (20–39 years old), group B (40–59 years old), group C (60–79 years old), and group D (≥80 years old). The objective was to determine if there were statistically significant differences with respect to age in the PTSD, anxiety, depression, and fear scores (Table 6). Statistically significant differences (p < 0.05) were only found between group A (6.15 ± 3.04) and group C (4.85 ± 1.74) in the PTSD scores; for verifying this difference, a post-hoc analysis showed that group A had a higher score than group C ((p < 0.05) CI 95% [0.05, 2.66]).
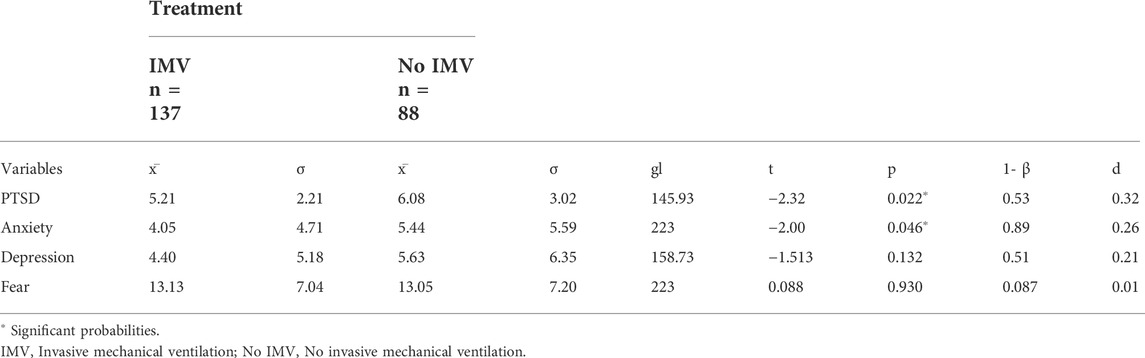
TABLE 6. Differences between the type of treatment required in hospitalization in PTSD, anxiety, depression, and fear scores.
4 Discussion
The aim of our study was to determine the prevalence and severity of PTSD, anxiety, depression, and fear in COVID-19 survivors 3 months after hospital discharge. Our results initially show that 93.4% of the survivors reported having at least one symptom associated with post-COVID-19 syndrome after their recovery, the most frequent of which were physical (82.7%), cognitive (37.9%), and psychological (25.1%). These observations are similar to those reported in other studies, where between 40 and 90% of patients with moderate to severe COVID-19 presented at least one symptom associated with post-COVID-19 syndrome within the first 6 months after recovery (Huang et al., 2021; Nalbandian et al., 2021; Peghin et al., 2021).
Within the psychological aspect, symptoms associated with PTSD were observed in 40.2% of the survivors, 38.4% reported anxiety, 36.6% depression, and 36.12% fear of different aspects related to COVID-19. These results agree with those reported by other research studies where it was found that the prevalence of PTSD ranges from 30–40%, depression 20–40%, and anxiety 25–40% (Liu et al., 2020; Sun et al., 2021; Huang et al., 2021; Huilca Sergo, 2021; Nalbandian et al., 2021). Our study provides and complements information to address post-COVID psychological sequelae, which is a very important subject of study in the field of mental health.
Statistically significant differences were found between men and women (p = 003), showing that women have a higher prevalence of severe symptoms associated with PTSD (2.5%), anxiety (7.5%), depression (7.5%), and fear (16.13%). These findings are related to what is found in the literature, where women tend to have a higher prevalence of psychological and emotional disorders (Lee et al., 2019; Huang et al., 2021), for example, the likelihood of developing PTSD increases and occurs mostly in women (Schein et al., 2021). In addition, being female has also been associated as one of the predictors for higher PTSD symptom severity in COVID-19 survivors, in conjunction with other factors such as past traumatic events, prolonged symptoms, stigmatization, and a negative perspective of the COVID-19 pandemic (Huilca Sergo, 2021; Poyraz et al., 2021).
Another important aspect for the development of psychological alterations is related to the severity of the patients and hospitalization (Chen et al., 2021), when analyzing the presence of PTSD, anxiety, depression, and fear symptoms between patients who required IMV and those who only needed oxygenation during their hospitalization. Statistically significant differences were found in PTSD (p < 0.05) and anxiety (p < 0.05). Our results showed that the prevalence of symptoms associated with PTSD is higher in patients who did not require IMV (48.9%) and in patients with anxiety symptoms considered severe (10.2%), while depression scores associated with a moderate–severe level were higher in these patients (8%), and the scores associated with fear before COVID-19 were very similar in both groups (9.5% in patients with IMV and 8% in patients without IMV). The percentages of symptoms associated with PTSD, anxiety, and depression present in those patients who did not require IMV during their hospitalization are in agreement with those obtained by Chen et al. (2021), who observed that hospitalized patients who reported greater symptoms of PTSD are those who, during their hospital stay, were exposed to negative news and that they are mostly patients who did not require IMV, being aware of disease processes such as delusions, agitation, persistent medical symptoms, and psychosocial factors such as constant concern for their own and family members’ health (Janiri et al., 2021), and that during recovery, there could be factors for developing traumatic memories, compared to patients requiring IMV, who for most of their hospital stay are sedated. Our results also agree with those reported by Abdelghani et al. (2021) and Huilca Sergo, (2021) who found that patients with moderate to severe symptoms and who required hospitalization had a higher prevalence of moderate to severe PTSD symptoms 1 month after hospitalization, and with the findings of Liu et al. (2020), who reported that patients who were admitted to the Intensive Care Unit during hospitalization had no severe symptoms of PTSD, but moderate to severe symptoms of depression.
Age is another important factor associated with the development of PTSD, anxiety, and depressive symptoms. We found that PTSD symptoms affected most frequently younger patients compared with other age groups (p < 0.05). The prevalence of clinically severe PTSD symptoms affected about 18.3% of the younger patients, clinically severe anxiety symptoms was present in 10% of these patients, while 7% presented symptoms related to clinically severe depression. Our results are related to what is found in the literature, where stressful events affect young people more than old people (Cai et al., 2020). It has been observed that old people present a lower level of acute stress during stressful events than young people (Reynolds et al., 2016). In the COVID-19 context, the patron is the same (Cai et al., 2020; Tang et al., 2022). On the other hand, anxiety and depressive symptoms are also most common in young people (Gambin et al., 2021; Solomou and Constantinidou, 2020). Age, along with other factors such as being female, and the severity of COVID-19 symptoms have been identified as risk factors for the development of PTSD, anxiety, depression, or other mental comorbidities (Chen et al., 2020, Nie et al., 2020, Ochnik et al., 2022; Tang et al., 2022).
One of the factors associated with the development of PTSD and other psychological disorders such as anxiety and depression is related to the loss of a family member or loved one (Huilca Sergo, 2021). In our study, about 42.7% of COVID-19 survivors reported having lost one or more family members due to COVID-19, being more frequent in women (52.6%). This is one limitation of our study, not exploring the association between the loss of a family member and the severity of PTSD symptoms, anxiety, depression, and fear. According to what is reported in the literature, it is hypothesized that it could be a risk factor for the onset and modulation of these alterations (Liu et al., 2020; Sun et al., 2021; Huilca Sergo, 2021).
Another limitation of our study is that we do not have a control group that allows us to compare the results in a retrospective study, as many others have done (e.g., Taquet et al., 2021). However, our results are in accordance with those previously reported throughout the course of the COVID-19 pandemic and other infectious epidemics, allowing us to provide more data that demonstrate the impact that post-COVID-19 syndrome has on the mental health of survivors, and contributing information to those already existing in the Latin American context. However, more research is needed to understand the long-term development of these symptoms.
5 Conclusion
Psychological symptoms are observed within post-COVID-19 syndrome in about 25% of COVID-19 survivors even after hospital discharge. Symptomatology associated with PTSD, depression, anxiety, and fear tends to affect more women, while those survivors who did not require IMV during their hospitalization and the stressful experience that this involves tend to be more affected by PTSD and anxiety symptoms compared to those patients who required IMV. Knowing the prevalence and incidence of psychological disturbances such as anxiety, depression, and PTSD, allows prevention plans to be implemented before patients present a severe case of COVID-19, providing tools that successfully help in coping due to adaptive behavior after the acute period of infection. In addition, knowing the prevalence of these symptoms also makes it possible to design and implement cognitive and behavioral treatments for survivors who are mostly affected by symptoms associated with PTSD, anxiety, or depression, access more efficient treatments, reduce comorbidity, and even decrease associated risk factors such as suicide and addictions.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the ethics and research committee of the Instituto Nacional de Enfermedades Respiratorias, Ismael Cosío Villegas.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This work was supported by economic funds granted by the Secretary of Health of the Mexican government.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor RD and the Reviewer JS declared a shared affiliation with the authors BD and LT at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abdelghani, M., Hassan, M. S., Alsadik, M. E., Abdelmoaty, A. A., Said, A., and Atwa, S. A. (2021). Post-traumatic stress symptoms among an Egyptian sample of post-remission COVID-19 survivors: Prevalence and sociodemographic and clinical correlates. Middle East Curr. Psychiatry 28 (1), 20–28. doi:10.1186/s43045-021-00102-y
Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., and Pakpour, A. H. (2020). The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 20, 1537–1545. doi:10.1007/s11469-020-00270-8
Arrieta, J., Aguerrebere, M., Raviola, G., Flores, H., Elliott, P., Espinosa, A., et al. (2017). Validity and utility of the patient health Questionnaire (PHQ)-2 and PHQ-9 for screening and diagnosis of depression in rural chiapas, Mexico: A cross-sectional study. J. Clin. Psychol. 73 (9), 1076–1090. doi:10.1002/jclp.22390
Bender del Busto, J. E. (2022). Algunas consideraciones con relación al síndrome post-COVID-19. Rev. Electrónica Medimay 29 (1), 1–6.
Boix, V., and Merino, E. (2022). Post-COVID syndrome. The never ending challenge. Med. Clin. 158 (4), 178–180. doi:10.1016/j.medcle.2021.10.005
Brady, K. T., Killen, T. K., Brewerton, T., and Lucerini, S. (2000). Comorbidity of psychiatric disorders and posttraumatic stress disorder. J. Clin. Psychiatry 61 (7), 22–32.
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 395, 912–920. doi:10.1016/s0140-6736(20)30460-8
Cai, X., Hu, X., Ekumi, I. O., Wang, J., An, Y., Li, Z., et al. (2020). Psychological distress and its correlates among COVID-19 survivors during early convalescence across age groups. Am. J. Geriatric Psychiatry 28 (10), 1030–1039. doi:10.1016/j.jagp.2020.07.003
Campo-Arias, A., Herazo, E., Caballero-Domínguez, C. C., Campo-Arias, A., Herazo, E., and Caballero-Domínguez, C. C. (2020). Dimensionalidad, validez nomológica y consistencia interna de la escala breve de Davidson para estrés postraumático en estudiantes de Santa Marta, Colombia. Rev. Fac. Nac. Salud Publica 38 (3), 1–8. doi:10.17533/UDEA.RFNSP.E339851
Carod-Artal, F. (2018). Infectious diseases causing autonomic dysfunction. Clin. Auton. Res. 28 (1), 67–81. doi:10.1007/s10286-017-0452-4
Carvajal, C. (2002). Trastorno por estrés postraumático: Aspectos clínicos. Rev. Chil. Neuro-psiquiatr. 40 (2), 20–34. doi:10.4067/s0717-92272002000600003
Carvalho, P. M. de M., Moreira, M. M., de Oliveira, M. N. A., Landim, J. M. M., and Neto, M. L. R. (2020). The psychiatric impact of the novel coronavirus outbreak. Psychiatry Res. 286, 112902. doi:10.1016/j.psychres.2020.112902
Chen, Y., Huang, X., Zhang, C., An, Y., Liang, Y., Yang, Y., et al. (2021). Prevalence and predictors of posttraumatic stress disorder, depression and anxiety among hospitalized patients with coronavirus disease 2019 in China. BMC Psychiatry 21 (1), 80–88. doi:10.1186/s12888-021-03076-7
Cheng, S. K. W., Wong, C. W., Tsang, J., and Wong, K. C. (2004). Psychological distress and negative appraisals in survivors of severe acute respiratory syndrome (SARS). Psychol. Med. 34 (7), 1187–1195. doi:10.1017/s0033291704002272
Ciotti, M., Ciccozzi, M., Terrinoni, A., Jiang, W. C., Wang, C., and Bernardini, S. (2020). The COVID-19 pandemic”, critical reviews in clinical laboratory sciences. Taylor Francis 57, 365–388. doi:10.1080/10408363.2020.1783198
Du, L., Chen, Y. M., Li, Y., Yuan, W., and Wang, J. S. (2020). Prevalence of depression during the SARS, MERS, and COVID-19 pandemics: A protocol for overview of systematic reviews. Medicine 99 (38), e22235. doi:10.1097/md.0000000000022235
Gambin, M., Sękowski, M., Woźniak-Prus, M., Wnuk, A., Oleksy, T., Cudo, A., et al. (2021). Generalized anxiety and depressive symptoms in various age groups during the COVID-19 lockdown in Poland. Specific predictors and differences in symptoms severity. Compr. Psychiatry 105, 152222. doi:10.1016/j.comppsych.2020.152222
García-Reyna, B., Castillo-García, G. D., Barbosa-Camacho, F. J., Cervantes-Cardona, G. A., Cervantes-Pérez, E., Torres-Mendoza, B. M., et al. (2022). International journal of mental health and addiction. Fear COVID-19 Scale Hosp. Staff Regional Hosp. Mexico A Brief Report” 20 (2), 895–906.
Ginzburg, K., Ein-Dor, T., and Solomon, Z. (2010). Comorbidity of posttraumatic stress disorder, anxiety and depression: A 20-year longitudinal study of war veterans. J. Affect. Disord. 123 (1–3), 249–257. doi:10.1016/j.jad.2009.08.006
Gutiérrez-Velilla, E., Barrientos-Casarrubias, V., Cruz-Maycott, R., Perrusquia-Ortiz, L. E., Alvarado-de la Barrera, C., Ávila-Ríos, S., et al. (2022). Assessment of anxiety in Mexican persons living with HIV using a culturally-adapted version of the GAD-7 test”. London, England: SAGE Publications Sage UK.
Halpin, S. J., McIvor, C., Whyatt, G., Adams, A., Harvey, O., McLean, L., et al. (2021). Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 93 (2), 1013–1022. doi:10.1002/jmv.26368
Huang, C., Huang, L., Wang, Y., Li, X., Ren, L., Gu, X., et al. (2021). 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 397 (10270), 220–232. doi:10.1016/s0140-6736(20)32656-8
Huilca Sergo, K. (2021). Factores asociados a síntomas del trastorno de estrés postraumático en pacientes con COVID-19 DADOS DE ALTA del Hospital Regional del Cusco, 2021. Cusco, Perú: Universidad Nacional de San Antonio Abad del Cusco.
Janiri, D., Carfì, A., Kotzalidis, G. D., Bernabei, R., Landi, F., and Sani, G. (2021). Posttraumatic stress disorder in patients after severe COVID-19 infection. JAMA Psychiatry 78 (5), 567–569. doi:10.1001/jamapsychiatry.2021.0109
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). “The PHQ-9”, validity of a brief depression severity measure. Journal of general internal medicine 16 (9), 606–613. doi:10.1046/j.1525-1497.2001.016009606.x
Lam, M. H. B., Wing, Y. K., Yu, M. W. M., Leung, C. M., Ma, R. C. W., Kong, A. P. S., et al. (2009). Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors long-term follow-up. Arch. Intern. Med. 169 (22), 2142–2147. doi:10.1001/archinternmed.2009.384
Lee, S. H., Shin, H. S., Park, H. Y., Kim, J. L., Lee, J. J., Lee, H., et al. (2019). Depression as a mediator of chronic fatigue and post-traumatic stress symptoms in Middle East respiratory syndrome survivors. Psychiatry Investig. 16 (1), 59–64. doi:10.30773/pi.2018.10.22.3
Liu, D., Baumeister, R. F., Veilleux, J. C., Chen, C., Liu, W., Yue, Y., et al. (2020). Risk factors associated with mental illness in hospital discharged patients infected with COVID-19 in Wuhan, China. Psychiatry Res. 292, 113297. doi:10.1016/J.PSYCHRES.2020.113297
Mak, I. W. C., Chu, C. M., Pan, P. C., Yiu, M. G. C., and Chan, V. L. (2009). Long-term psychiatric morbidities among SARS survivors. General Hosp. Psychiatry 31 (4), 318–326. doi:10.1016/j.genhosppsych.2009.03.001
Mak, I. W. C., Chu, C. M., Pan, P. C., Yiu, M. G. C., Ho, S. C., and Chan, V. L. (2010). Risk factors for chronic post-traumatic stress disorder (PTSD) in SARS survivors. Gen. Hosp. Psychiatry 32 (6), 590–598. doi:10.1016/j.genhosppsych.2010.07.007
Mazza, M. G., de Lorenzo, R., Conte, C., Poletti, S., Vai, B., Bollettini, I., et al. (2020). Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors”, Brain, Behavior, and Immunity, 89. Academic Press, 594–600. doi:10.1016/j.bbi.2020.07.037
Meltzer-Brody, S., Churchill, E., and Davidson, J. R. (1999). Derivation of the SPAN, a brief diagnostic screening test for post-traumatic stress disorder. Psychiatry res. 88 (1), 63–70. doi:10.1016/s0165-1781(99)00070-0
Miller, A. H., and Raison, C. L. (2016). The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 16 (1), 22–34. doi:10.1038/nri.2015.5
Moldofsky, H., and Patcai, J. (2011). Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. 11, 37. doi:10.1186/1471-2377-11-37
Moreno-Pérez, O., Merino, E., Leon-Ramirez, J. M., Andres, M., Ramos, J. M., Arenas-Jiménez, J., et al. (2021). Post-acute COVID-19 syndrome. Incidence and risk factors: A mediterranean cohort study. J. Infect. 82 (3), 378–383. doi:10.1016/j.jinf.2021.01.004
Najjar, S., Pearlman, D. M., Alper, K., Najjar, A., and Devinsky, O. (2013). Neuroinflammation and psychiatric illness. J. Neuroinflammation 10 (1), 8161–8224. doi:10.1186/1742-2094-10-43
Nalbandian, A., Sehgal, K., Gupta, A., Madhavan, M. v., McGroder, C., Stevens, J. S., et al. (2021). Post-acute COVID-19 syndrome. Nat. Med. 2727 (4), 4601–4615. doi:10.1038/s41591-021-01283-z
Nie, X. D., Wang, Q., Wang, M. N., Zhao, S., Liu, L., Zhu, Y. L., et al. (2020). Anxiety and depression and its correlates in patients with coronavirus disease 2019 in Wuhan. Int. J. Psychiatry Clin. Pract. 25 (2), 109–114. doi:10.1080/13651501.2020.1791345
Ochnik, D., Rogowska, A. M., Arzenšek, A., and Benatov, J. (2022). Longitudinal predictors of coronavirus-related PTSD among young adults from Poland, Germany, Slovenia, and Israel. Int. J. Environ. Res. Public Health 2022 (12), 7207. doi:10.3390/ijerph19127207
Peghin, M., Palese, A., Venturini, M., de Martino, M., Gerussi, V., Graziano, E., et al. (2021). Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 27 (10), 1507–1513. doi:10.1016/j.cmi.2021.05.033
Poyraz, B. Ç., Poyraz, C. A., Olgun, Y., Gürel, Ö., Alkan, S., Özdemir, Y. E., et al. (2021). Psychiatric morbidity and protracted symptoms after COVID-19. Psychiatry Res. 295, 113604. doi:10.1016/J.PSYCHRES.2020.113604
Reynolds, K., Pietrzak, R. H., Mackenzie, C. S., Chou, K. L., and Sareen, J. (2016). Post-traumatic stress disorder across the adult lifespan: Findings from a nationally representative survey. Am. J. Geriatric Psychiatry 24 (1), 81–93. doi:10.1016/j.jagp.2015.11.001
Rogers, J. P., Chesney, E., Oliver, D., Pollak, T. A., McGuire, P., Fusar-Poli, P., et al. (2020). Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 7 (7), 611–627. doi:10.1016/s2215-0366(20)30203-0
Schein, J., Houle, C., Urganus, A., Cloutier, M., Patterson-Lomba, O., Wang, Y., et al. (2021). Prevalence of post-traumatic stress disorder in the United States: A systematic literature review. Curr. Med. Res. Opin. 37 (12), 2151–2161. doi:10.1080/03007995.2021.1978417
Solomou, I., and Constantinidou, F. (2020). Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health Vol. 1717 (14), 49244924. doi:10.3390/ijerph17144924
Spitzer, R. L., Kroenke, K., Williams, J. B., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166 (10), 1092–1097. doi:10.1001/archinte.166.10.1092
Sun, L., Sun, Z., Wu, L., Zhu, Z., Zhang, F., Shang, Z., et al. (2021). Prevalence and risk factors for acute posttraumatic stress disorder during the COVID-19 outbreak. J. Affect. disord.. 283, 123–129. doi:10.1016/j.jad.2021.01.050
Tang, L., Gao, Y., Qi, S., Cui, J., Zhou, L., and Feng, Y. (2022). Prevalence of post-traumatic stress disorder symptoms among patients with mental disorder during the COVID-19 pandemic. BMC Psychiatry. 22, 156. doi:10.1186/S12888-022-03790-W
Taquet, M., Geddes, J. R., Husain, M., Luciano, S., and Harrison, P. J. (2021). 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospective cohort study using electronic health records. Lancet Psychiatry. 8, 416–427. doi:10.1016/S2215-0366(21)00084-5
Velavan, T. P., and Meyer, C. G. (2020). The COVID-19 epidemic. Trop. Med. Int. Health 25 (3), 278–280. doi:10.1111/tmi.13383
Keywords: post-traumatic stress disorder (PTSD), anxiety, depression, fear, SARS- CoV-2
Citation: Luna-Rodríguez GL, Peláez-Hernández V, Orea-Tejeda A, Ledesma-Ruíz CD, Casarín-López F, Rosas-Trujillo A, Domínguez-Trejo B and Tepepa-Flores LE (2022) Prevalence of post-traumatic stress disorder, emotional impairments, and fear in COVID-19 surviving patients. Front. Virtual Real. 3:927058. doi: 10.3389/frvir.2022.927058
Received: 23 April 2022; Accepted: 29 July 2022;
Published: 20 October 2022.
Edited by:
Raúl Duron-Figueroa, National Autonomous University of Mexico, MexicoReviewed by:
José Manuel Sanchez Sordo, National Autonomous University of Mexico, MexicoEdwin Oliveros, Universidad de San Buenaventura, Colombia
Copyright © 2022 Luna-Rodríguez, Peláez-Hernández, Orea-Tejeda, Ledesma-Ruíz, Casarín-López, Rosas-Trujillo, Domínguez-Trejo and Tepepa-Flores. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viridiana Peláez-Hernández, dnBlbGFlemhAZ21haWwuY29t