 Davide Cardile1
Davide Cardile1 Chiara Arena1*
Chiara Arena1* Francesco Corallo1
Francesco Corallo1 Giulia Maria Giuffrida2
Giulia Maria Giuffrida2 Andreina Giustiniani1
Andreina Giustiniani1 Maria Grazia Maggio1Carmela Rifici1Angelo Quartarone1,3Francesco Tomaiuolo2Rocco Salvatore Calabrò1
Maria Grazia Maggio1Carmela Rifici1Angelo Quartarone1,3Francesco Tomaiuolo2Rocco Salvatore Calabrò1- 1IRCCS Centro Neurolesi Bonino Pulejo, Messina, Italy
- 2Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy
- 3Department of Biomedical, Dental Sciences, and Morphological and Functional Imaging, University of Messina, Messina, Italy
Background: Virtual reality (VR) has emerged as a promising tool in post-stroke neurorehabilitation, offering immersive and interactive environments capable of enhancing motor and executive function recovery through mechanisms of neuroplasticity. Although various VR modalities—immersive (I), semi-immersive (SI), non-immersive (NI), and mixed (MXD)—have been applied, their relative effectiveness remains unclear.
Objective: This systematic review aimed to evaluate the efficacy of different VR modalities in improving motor or executive functions in post-stroke patients and to explore how the stroke phase and the type of VR system used influence treatment outcomes.
Methods: A comprehensive literature search was conducted across PubMed, Embase, Scopus, and the Cochrane Library, resulting in 46 eligible peer-reviewed studies published between 2014 and 2024. These studies included randomized controlled trials, quasi-experimental designs, and observational studies, with an average sample size of approximately 35 participants. The inclusion criteria focused on studies utilizing VR as a therapeutic modality for motor or executive function recovery in post-stroke populations.
Results: Forty-six studies met the inclusion criteria. Overall, VR interventions yielded positive motor outcomes in 76.3% of cases, with semi-immersive VR (SI-VR) achieving the highest proportion of significant improvements (88.24%), followed by non-immersive VR (NI-VR) (66.67%) and immersive VR (I-VR) (50%). Only 13% of studies assessed executive functions, but SI-VR and I-VR modalities showed more consistent benefits than NI-VR. No statistically significant associations were found between VR typology, the stroke phase (chronic vs. subacute), and motor outcome efficacy.
Conclusion: VR is an effective and versatile adjunct to conventional stroke rehabilitation, with SI-VR showing the most consistent motor benefits and immersive systems offering additional cognitive engagement. The lack of significant differences by stroke phase suggests that VR can be applied across recovery stages. Future research should address the underrepresentation of executive function outcomes and directly compare modalities in well-powered trials.
1 Introduction
Acquired brain injury is the second most common cause of death (62.2%) and the third most common cause of death and disability combined; survivors often suffer severe motor and cognitive impairments that greatly reduce their own and their families’ quality of life (GBD 2019 Stroke Collaborators, 2021).
In these patients, cognitive and motor rehabilitation treatments aim to stimulate neuroplasticity and support the reorganization of damaged brain areas (Einstad et al., 2021).
In recent years, virtual reality (VR) has gained growing interest due to its capacity to deliver engaging, adaptive, and task-oriented environments that simulate real-world scenarios while ensuring patient safety (Massetti et al., 2018). VR enhances motivation, provides real-time feedback, and allows for the repetition of exercises in a controlled setting, which are key factors in effective neurorehabilitation (Rizzo and Koenig, 2017). Depending on the level of immersion, VR environments can be categorized into immersive (I), semi-immersive (SI), non-immersive (NI), or mixed (MXD) reality systems. Immersive VR (I-VR) uses head-mounted displays to fully surround users with a virtual environment, enhancing the presence but sometimes causing side effects such as nausea or disorientation (“VR sickness”) due to sensory conflict between the visual input and signals from the vestibular system (Chang et al., 2020). Roussou et al. (2024) showed that I-VR is safe and usable when basic measures are taken to reduce adverse effects and help users adapt. Semi-immersive VR (SI-VR) allows interaction via screens or robotic interfaces while maintaining partial contact with the real world (Fernández-Vázquez et al., 2022). Non-immersive VR (NI-VR) typically involves standard displays such as TVs or monitors and basic input devices, whereas mixed reality overlays virtual elements onto physical environments, creating hybrid scenarios (Howard, 2017).
Clinically, VR has demonstrated promising effects in post-stroke rehabilitation for both motor and executive function recovery, including improvements in upper and lower limb coordination, strength, and range of motion, enhanced attention, processing speed, and cognitive flexibility (Maier et al., 2019).
Motor and executive functions are closely linked following a stroke, as goal-directed movements require planning, decision-making, and attentional control (Schaefer and Schumacher, 2009). Stroke often affects networks involving both motor and prefrontal regions, leading to concurrent deficits; thus, evaluating these domains together offers a more complete view of recovery and potential cross-domain rehabilitation effects (Cramer et al., 2011). This systematic review aims to bridge this gap by reviewing studies focused on the impact of VR rehabilitative treatments, across all modalities—immersive, semi-immersive, non-immersive, and mixed reality—on both motor and executive functios (or one of them) in post-stroke patients. A secondary objective is to demonstrate the benefits of this innovative therapeutic strategy and its potential role in advancing neurorehabilitation.
2 Materials and methods
We conducted this systematic review to explore the existing evidence on innovative rehabilitation for improving motor and cognitive outcomes in post-stroke patients. This review was registered with a DOI (osf.io/fy3mw) on the Open Science Framework (OSF).
2.1 Search strategy
A review of currently published studies was performed in the following databases: PubMed, Embase, Scopus, and the Cochrane Library. The following search string was used: (((neurorehabilitation [Title/Abstract]) AND (virtual reality [Title/Abstract])) AND (executive functions [Title/Abstract])) OR (motor impairment [Title/Abstract]). All the articles were published between 2014 and 2024.
2.2 Study selection
To minimize bias and ensure a rigorous selection process, three investigators (C.A., D.C., and G.G.) independently reviewed and extracted data from the studies. Full-text articles deemed suitable for the study were then read by these researchers, and any discrepancy in selection was resolved through collaborative discussion, with consultation from a fourth researcher (R.S.C). This multistep approach ensured that at least three research workers independently assessed each article. In cases of persistent disagreement, the final decision involved all authors.
2.3 Inclusion criteria
A study was included if it described or investigated patients with acquired brain injuries who were treated with innovative cognitive or motor rehabilitation approaches. To ensure consistency and quality, only articles written in English and published in peer-reviewed journals were included.
2.4 Exclusion criteria
A study was excluded if it described theoretical models, methodological approaches, algorithms, and basic technical descriptions, along with (i) animal studies, (ii) conference proceedings or reviews, and (iii) studies involving other neurological patients.
2.5 Risk of bias within individual studies
The risk of bias was assessed considering five domains: (i) bias due to the randomization process, (ii) bias due to deviations from the intended interventions, (iii) bias due to missing outcome data, (iv) bias due to the risk of bias in the measurement of post-exposure outcomes, and (v) bias due to the risk of bias in the selection of the reported outcome. A detailed summary of the risk of bias is available in Appendix 1.
3 Results
3.1 Synthesis of evidence
The initial search resulted in 11,153 studies from different databases, such as PubMed, Embase, Scopus, and the Cochrane Library. After screening the titles, abstracts, and full texts of articles against the inclusion and exclusion criteria, 46 studies (Duret et al., 2015; Brunner et al., 2017; Mazzoleni et al., 2018; Mekbib et al., 2021; Zhang et al., 2023; Dahdah et al., 2017; Torrisi et al., 2021; Lam et al., 2022; Gerardin et al., 2022; Valdés and Van der Loos, 2018; Noveletto et al., 2020; Manuli et al., 2020; Norouzi-Gheidari et al., 2020; Johnson et al., 2018; Luo et al., 2023; Schuster-Amft et al., 2018; Colomer et al., 2016; Yuan et al., 2021; Llorens et al., 2021; Paquin et al., 2015; Aşkın et al., 2018; Yao et al., 2020; Saposnik et al., 2016; Kong et al., 2016; Taravati et al., 2022; Jung et al., 2017; Thielbar et al., 2020; Aprile et al., 2021; Patel et al., 2019; Şenocak et al., 2023; Mazzoleni et al., 2014; Rong et al., 2021; Lu et al., 2020; Maistrello et al., 2021; Mugler et al., 2019; Saleh et al., 2017; Ranzani et al., 2020; Sip et al., 2023; Kim et al., 2017; Sale et al., 2014; Lee, 2019; Adams et al., 2023; Abd El-Kafy et al., 2022; Yeh et al., 2017; Thielbar et al., 2014; Palermo et al., 2018) were identified as eligible for this systematic review. The details of the search process are shown in Figure 1.
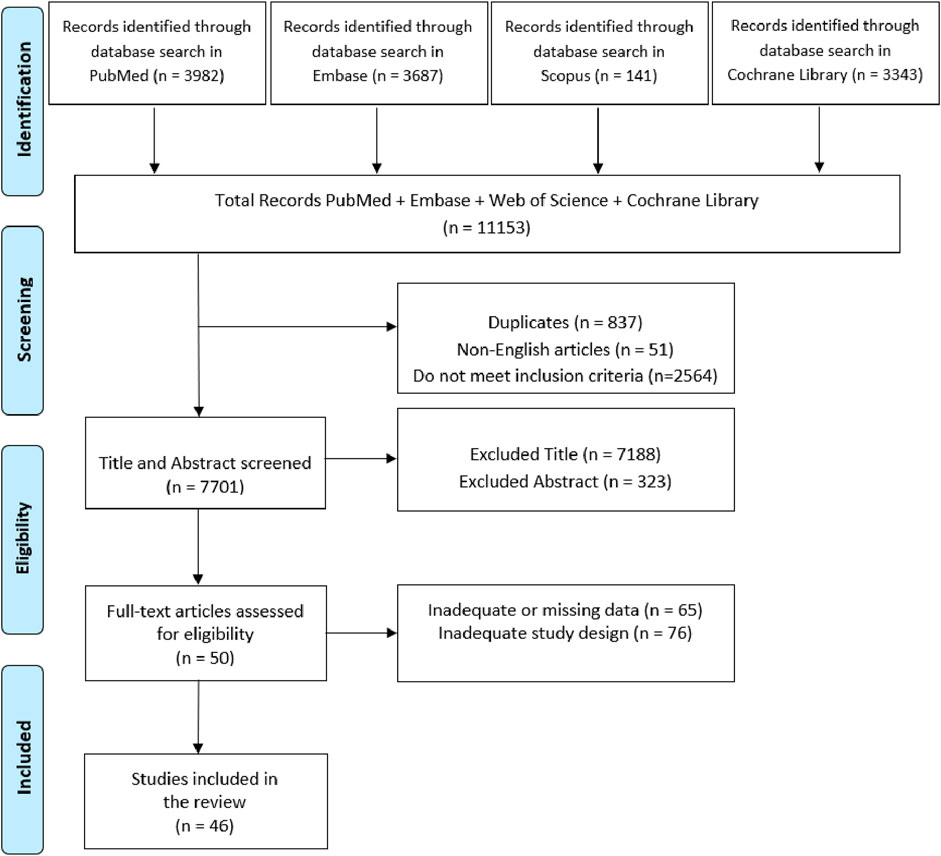
Figure 1. PRISMA flowchart of the current review.
3.2 Description of studies and VR technologies
All studies included in this systematic review were published in English between 2014 and 2024. The main features of the used VR tasks and technologies are summarized in Supplementary Table S1.
Out of the 46 studies reviewed, over two-thirds used robotic devices, either to actively assist limb movement or to provide haptic and motor feedback. Many studies also used assistive elements, such as arm supports, smart gloves or handlebars, designed to facilitate motion or reduce the need for compensatory strategies.
The equipment ranged from head-mounted displays (HMDs) (Mekbib et al., 2021; Dahdah et al., 2017) to robotic exoskeletons (Manuli et al., 2020; Saposnik et al., 2016; Taravati et al., 2022; Rong et al., 2021) and glove-based systems (Jung et al., 2017; Adams et al., 2023; Brunner et al., 2017). Some studies utilized sensor-based tracking systems, such as Kinect sensors (Valdés and Van der Loos, 2018; Aşkın et al., 2018), camera setups (Sip et al., 2023) or motion-tracking gloves (Paquin et al., 2015; Jung et al., 2017; Yeh et al., 2017). Non-robotic equipment was often paired with commercial gaming platforms, particularly the Nintendo Wii (Paquin et al., 2015; Saposnik et al., 2016; Kong et al., 2016) and the Xbox Kinect (Paquin et al., 2015; Saposnik et al., 2016; Kong et al., 2016). These platforms provided cost-effective, engaging environments but generally lacked mechanical assistance.
The software used varied widely: commercial platforms (e.g., WiiMote, Unity3D, and VRRS Evo) (Paquin et al., 2015; Kong et al., 2016; Maistrello et al., 2021), custom-built or proprietary software [such as tyroS with Amadeo (Paquin et al., 2015; Kong et al., 2016; Maistrello et al., 2021), REA software Axinesis with REAplan® (Paquin et al., 2015; Kong et al., 2016; Maistrello et al., 2021) or InMotion Solution Designer (Duret et al., 2015; Mazzoleni et al., 2018)], and hybrid systems, such as those integrated brain–computer interface (BCI) components with functional electrical stimulation (FES) and VR (Zhang et al., 2023; Johnson et al., 2018). Some systems included multimodal inputs, such as EMG signals (Zhang et al., 2023; Johnson et al., 2018), EEG (Zhang et al., 2023; Johnson et al., 2018) or force feedback (Zhang et al., 2023; Johnson et al., 2018), emphasizing motor control precision and adaptability.
All outcomes were measured at baseline and at the end of all interventions. Cognitive outcomes were assessed using the Montreal Cognitive Assessment (MoCA) in five studies (Manuli et al., 2020; Torrisi et al., 2021; Gerardin et al., 2022; Yuan et al., 2021; Taravati et al., 2022). Three studies (Torrisi et al., 2021; Manuli et al., 2020; Ranzani et al., 2020) used the Frontal Assessment Battery (FAB) to evaluate EF. Three studies (Yuan et al., 2021; Schuster-Amft et al., 2018; Ranzani et al., 2020) assessed the cognitive outcomes by the mini-mental state examination. One study (Manuli et al., 2020) used the Trial Making Test (TMT). Two studies (Torrisi et al., 2021; Yuan et al., 2021) used the digit span test. In one study (Torrisi et al., 2021), the attentive matrices test (AMT) was used. Instead, the Rey–Osterrieth complex figure (ROCF) was used to assess cognitive outcomes in one study (Torrisi et al., 2021). Finally, one study (Dahdah et al., 2017) used the Automated Neuropsychological Assessment Metrics (ANAM), in which a Go/No-Go task and the Stroop test are involved as EF outcomes.
Regarding the motor outcomes, the Fugl-Meyer Assessment (FMA) was used in 27 studies (Mekbib et al., 2021; Zhang et al., 2023; Lam et al., 2022; Valdés and Van der Loos, 2018; Noveletto et al., 2020; Norouzi-Gheidari et al., 2020; Luo et al., 2023; Llorens et al., 2021; Aşkın et al., 2018; Yao et al., 2020; Kong et al., 2016; Thielbar et al., 2020; Aprile et al., 2021; Patel et al., 2019; Şenocak et al., 2023; Mazzoleni et al., 2014; Rong et al., 2021; Maistrello et al., 2021; Mugler et al., 2019; Sip et al., 2023; Kim et al., 2017; Sale et al., 2014; Lee, 2019; Adams et al., 2023; Yeh et al., 2017; Thielbar et al., 2014; Mazzoleni et al., 2018). The Wolf Motor Function Test (WMFT) was used by seven studies (Luo et al., 2023; Patel et al., 2019; Şenocak et al., 2023; Mugler et al., 2019; Kim et al., 2017; Adams et al., 2023; Yeh et al., 2017). The Action Research Arm Test (ARAT) was used in five studies (Lam et al., 2022; Yao et al., 2020; Abd El-Kafy et al., 2022; Thielbar et al., 2014; Brunner et al., 2017). Four studies (Mekbib et al., 2021; Yao et al., 2020; Lu et al., 2020; Palermo et al., 2018) used the Barthel Index to assess motor outcome, whereas two studies (Aprile et al., 2021; Rong et al., 2021) used the modified Barthel Index (mBI). Two studies (Adams et al., 2023; Yeh et al., 2017) evaluated the motor outcomes using the Box and Block Test (BBT), and six studies (Saposnik et al., 2016; Kong et al., 2016; Taravati et al., 2022; Palermo et al., 2018; Brunner et al., 2017; Rong et al., 2021) used the Functional Independence Measure. In two studies (Paquin et al., 2015; Saleh et al., 2017), the motor outcome measure used was the Jebsen Hand Function Test (JHFT). Finally, in one study (Şenocak et al., 2023), the Trunk Impairment Scale was used. Moreover, in this case, all outcomes were assessed at baseline and at the end of treatment.
3.3 Description of VR interventions and recipients
The number of participants across the studies varied considerably, ranging from a minimum of three patients (Johnson et al., 2018) to a maximum of 141 patients (Saposnik et al., 2016), with an average sample size of approximately 36 participants per study (Table 1).
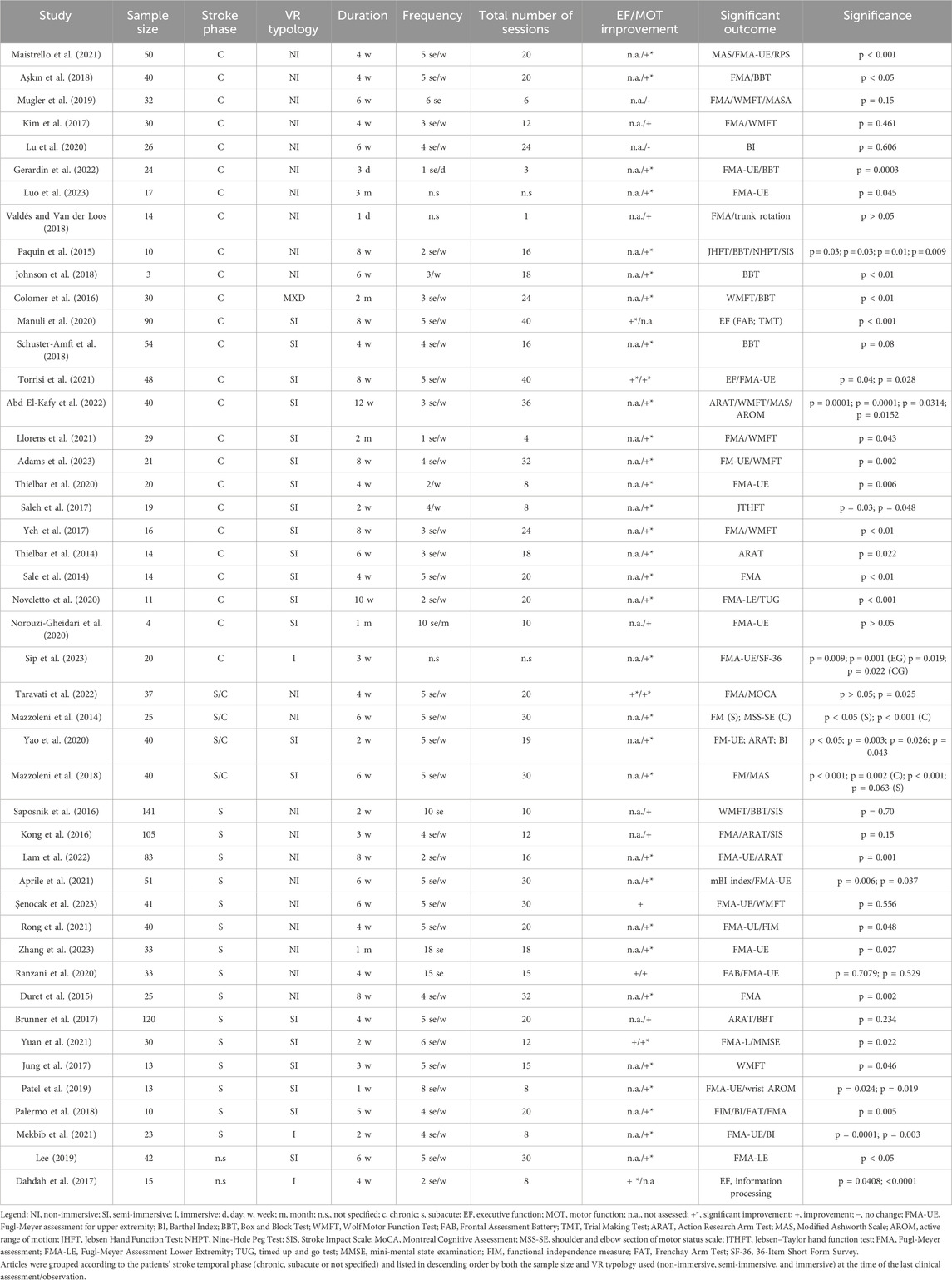
Table 1. Summary of patients’ characteristics, VR features, and outcomes of the studies included in the research.
According to the post-stroke timeframe proposed by Bernhardt et al. (2017), the majority of studies involved individuals in the chronic stage; a total of 25 studies focused on chronic patients (Torrisi et al., 2021; Gerardin et al., 2022; Valdés and Van der Loos, 2018; Noveletto et al., 2020; Manuli et al., 2020; Norouzi-Gheidari et al., 2020; Johnson et al., 2018; Luo et al., 2023; Schuster-Amft et al., 2018; Colomer et al., 2016; Llorens et al., 2021; Paquin et al., 2015; Aşkın et al., 2018; Thielbar et al., 2020; Lu et al., 2020; Maistrello et al., 2021; Mugler et al., 2019; Saleh et al., 2017; Sip et al., 2023; Kim et al., 2017; Sale et al., 2014; Adams et al., 2023; Abd El-Kafy et al., 2022; Yeh et al., 2017; Thielbar et al., 2014). Fifteen studies included individuals in the subacute phase (Mekbib et al., 2021; Zhang et al., 2023; Lam et al., 2022; Yuan et al., 2021; Saposnik et al., 2016; Kong et al., 2016; Jung et al., 2017; Aprile et al., 2021; Patel et al., 2019; Şenocak et al., 2023; Rong et al., 2021; Ranzani et al., 2020; Palermo et al., 2018; Duret et al., 2015; Brunner et al., 2017), whereas four studies involved mixed chronic/subacute samples (Yao et al., 2020; Taravati et al., 2022; Mazzoleni et al., 2014; Mazzoleni et al., 2018). Only two studies did not specify the stroke phase of the participants (Dahdah et al., 2017; Lee, 2019).
In terms of the type of VR used, 21 studies used NI-VR systems (Zhang et al., 2023; Lam et al., 2022; Gerardin et al., 2022; Valdés and Van der Loos, 2018; Johnson et al., 2018; Luo et al., 2023; Paquin et al., 2015; Aşkın et al., 2018; Saposnik et al., 2016; Kong et al., 2016; Taravati et al., 2022; Aprile et al., 2021; Şenocak et al., 2023; Mazzoleni et al., 2014; Rong et al., 2021; Lu et al., 2020; Maistrello et al., 2021; Mugler et al., 2019; Ranzani et al., 2020; Kim et al., 2017; Duret et al., 2015), and another 21 studies used SI-VR systems (Torrisi et al., 2021; Noveletto et al., 2020; Manuli et al., 2020; Norouzi-Gheidari et al., 2020; Schuster-Amft et al., 2018; Yuan et al., 2021; Llorens et al., 2021; Yao et al., 2020; Jung et al., 2017; Thielbar et al., 2020; Patel et al., 2019; Saleh et al., 2017; Sale et al., 2014; Lee, 2019; Adams et al., 2023; Abd El-Kafy et al., 2022; Yeh et al., 2017; Thielbar et al., 2014; Palermo et al., 2018; Brunner et al., 2017; Mazzoleni et al., 2018). Only one study used an MXD approach (Colomer et al., 2016), whereas three studies implemented I-VR systems (Mekbib et al., 2021; Dahdah et al., 2017; Sip et al., 2023). Treatment duration ranged from a minimum of 1 day (Zhang et al., 2023; Johnson et al., 2018) to a maximum of 3 months (Zhang et al., 2023; Johnson et al., 2018). The total number of VR training sessions ranged from a single session (Zhang et al., 2023; Johnson et al., 2018) to a maximum of 40 sessions (Torrisi et al., 2021; Manuli et al., 2020), whereas the frequency varied between a minimum of one session per week (Torrisi et al., 2021; Manuli et al., 2020) to a maximum of daily sessions (i.e., one session per day in consecutive days) (Torrisi et al., 2021; Manuli et al., 2020).
Regarding outcome assessment for executive function (EF) and motor functions (MOTs), only 6 out of 46 studies assessed executive functioning, whereas 44 studies evaluated motor outcomes. Of the studies assessing executive function, four studies reported statistically significant improvements (+) (Dahdah et al., 2017; Torrisi et al., 2021; Manuli et al., 2020; Taravati et al., 2022) and two observed a nonsignificant trend toward improvement (+) (Yuan et al., 2021; Ranzani et al., 2020), with no study reporting null effects (−); the remaining 40 studies did not assess EF at all (n.a.) (Mekbib et al., 2021; Zhang et al., 2023; Lam et al., 2022; Gerardin et al., 2022; Valdés and Van der Loos, 2018; Noveletto et al., 2020; Norouzi-Gheidari et al., 2020; Johnson et al., 2018; Luo et al., 2023; Schuster-Amft et al., 2018; Colomer et al., 2016; Llorens et al., 2021; Paquin et al., 2015; Aşkın et al., 2018; Yao et al., 2020; Saposnik et al., 2016; Kong et al., 2016; Jung et al., 2017; Thielbar et al., 2020; Aprile et al., 2021; Patel et al., 2019; Şenocak et al., 2023; Mazzoleni et al., 2014; Rong et al., 2021; Lu et al., 2020; Maistrello et al., 2021; Mugler et al., 2019; Saleh et al., 2017; Sip et al., 2023; Kim et al., 2017; Sale et al., 2014; Lee, 2019; Adams et al., 2023; Abd El-Kafy et al., 2022; Yeh et al., 2017; Thielbar et al., 2014; Palermo et al., 2018; Duret et al., 2015; Brunner et al., 2017; Mazzoleni et al., 2018). Considering motor function, 34 studies reported statistically significant improvements (+) (Mekbib et al., 2021; Zhang et al., 2023; Torrisi et al., 2021; Lam et al., 2022; Gerardin et al., 2022; Noveletto et al., 2020; Johnson et al., 2018; Luo et al., 2023; Schuster-Amft et al., 2018; Colomer et al., 2016; Yuan et al., 2021; Llorens et al., 2021; Paquin et al., 2015; Aşkın et al., 2018; Yao et al., 2020; Taravati et al., 2022; Jung et al., 2017; Thielbar et al., 2020; Aprile et al., 2021; Patel et al., 2019; Mazzoleni et al., 2014; Rong et al., 2021; Maistrello et al., 2021; Saleh et al., 2017; Sip et al., 2023; Sale et al., 2014; Lee, 2019; Adams et al., 2023; Abd El-Kafy et al., 2022; Yeh et al., 2017; Thielbar et al., 2014; Palermo et al., 2018; Duret et al., 2015; Mazzoleni et al., 2018), 8 studies observed only a nonsignificant improvement trend (+) (Saposnik et al., 2016; Kong et al., 2016; Şenocak et al., 2023; Ranzani et al., 2020; Kim et al., 2017; Brunner et al., 2017; Valdés and Van der Loos et al., 2018; Norouzi-Gheidari et al., 2020), and two studies reported no change (−) (Lu et al., 2020; Mugler et al., 2019); only two studies did not assess motor outcomes (n.a.) (Dahdah et al., 2017; Manuli et al., 2020).
In terms of intervention strategies, the duration of treatment ranged from a minimum of a single session (Valdés and Van der Loos, 2018) to a maximum of 12 weeks (Abd El-Kafy et al., 2022). The mean duration of treatment was 5.3 weeks.
All the interventions involved virtual reality devices in different modalities. In particular, five studies (Mekbib et al., 2021; Dahdah et al., 2017; Sip et al., 2023; Lee, 2019; Palermo et al., 2018) involved patients undergoing rehabilitation treatment in an immersive virtual reality environment. Sixteen studies (Manuli et al., 2020; Norouzi-Gheidari et al., 2020; Schuster-Amft et al., 2018; Yuan et al., 2021; Llorens et al., 2021; Yao et al., 2020; Jung et al., 2017; Thielbar et al., 2020; Patel et al., 2019; Sale et al., 2014; Adams et al., 2023; Abd El-Kafy et al., 2022; Yeh et al., 2017; Thielbar et al., 2014; Brunner et al., 2017; Mazzoleni et al., 2018) based their rehabilitation interventions on sessions of semi-immersive virtual reality. However, 24 studies (Zhang et al., 2023; Torrisi et al., 2021; Lam et al., 2022; Gerardin et al., 2022; Valdés and Van der Loos, 2018; Noveletto et al., 2020; Johnson et al., 2018; Luo et al., 2023; Paquin et al., 2015; Aşkın et al., 2018; Saposnik et al., 2016; Kong et al., 2016; Taravati et al., 2022; Aprile et al., 2021; Şenocak et al., 2023; Mazzoleni et al., 2014; Rong et al., 2021; Lu et al., 2020; Maistrello et al., 2021; Mugler et al., 2019; Saleh et al., 2017; Ranzani et al., 2020; Kim et al., 2017; Duret et al., 2015) based the treatment on a non-immersive virtual reality modality. Finally, one study (Colomer et al., 2016) used a treatment in mixed virtual reality.
To explore potential associations between treatment efficacy and key clinical and technological factors, we conducted chi-square tests of independence. In particular, we examined whether the distribution of motor outcomes [categorized as statistically significant improvement (+*), nonsignificant positive trend (+) or no improvement (−)] varied according to the type of VR applied (non-immersive, semi-immersive, immersive or mixed) and the stroke phase (chronic vs subacute). Motor function outcomes were selected for analysis due to their consistent reporting across studies. The chi-square analysis revealed no statistically significant association between VR typology and motor treatment outcomes [χ2(6) = 5.98; p = 0.425]. Similarly, no significant association was found between the stroke phase and motor outcomes [χ2(2) = 5.46; p = 0.486]. These results suggest that, based on the available data, the efficacy of VR interventions on motor function does not appear to be significantly influenced by either stroke chronicity or the level of immersion of the VR system used.
4 Discussion
4.1 Mechanistic differences across VR modalities
Generally, our findings confirm that VR interventions improve both motor and executive functions in post-stroke rehabilitation, with varying efficacy depending on the degree of immersion. However, as only four studies used I-VR (Mekbib et al., 2021; Dahdah et al., 2017; Sip et al., 2023) or only one use the MXD-VR modality (Colomer et al., 2016), a real comparison was possible only between SI-VR and NI-VR. In particular, SI-VR demonstrated superior motor outcomes (88.24% positive results) compared to NI-VR (66.67%). Although I-VR is typically delivered through head-mounted displays that enhance sensorimotor engagement and presence (Patsaki et al., 2022; Laver et al., 2017), SI systems use large screens or projection setups, and by balancing realism and comfort, they often achieve high adherence and motor outcomes comparable to immersive setups (Hao et al., 2024). The advantages of SI-VR may derive from tasks such as grasping tasks, which improve upper limb movements and cerebral connectivity (Llorens et al., 2021; Yao et al., 2020; Jung et al., 2017; Saleh et al., 2017; Adams et al., 2023; Brunner et al., 2017; Cano-de-la-Cuerda et al., 2015; Laver et al., 2015), along with mirror tasks (Sip et al., 2023), throwing tasks (Mekbib et al., 2021), and hitting or cycling tasks for the lower limbs (Noveletto et al., 2020; Lee, 2019). On the other hand, NI-VR, including BCI-based motor imagery (Zhang et al., 2023) and gaming consoles such as Xbox (Aşkın et al., 2018; Thielbar et al., 2020) and Nintendo Wii (Saposnik et al., 2016; Kong et al., 2016), shows lower efficacy than SI-VR. Nevertheless, NI-VR shows good motor gains, particularly in upper limb recovery, making it preferable to conventional rehabilitation, possibly due to its precise motion tracking and accessible design (Zhang et al., 2025; Molier et al., 2010).
Post-stroke EF impairments (planning, attention, and inhibition) can benefit from VR’s real-world-like challenges (Makmee and Wongupparaj, 2022), enhancing cognitive flexibility and engagement. I-VR and SI-VR modalities lead to significant improvement in the majority of cases (Dahdah et al., 2017; Torrisi et al., 2021; Manuli et al., 2020), with only one study showing just a positive, nonsignificant trend improvement (Yuan et al., 2021). On the other hand, both studies using the NI-VR modality showed nonsignificant improvements (Taravati et al., 2022; Ranzani et al., 2020).
For both motor and executive functions, each VR modality offers unique advantages. I-VR may better stimulate visuospatial and body representation networks, whereas NI-VR systems increase usability and training frequency (Weiss et al., 2004). The current results align with previous reviews, showing that VR, across modalities, supports motor recovery and, to a lesser extent, cognitive improvement post-stroke (Cano-de-la-Cuerda et al., 2015; Lohse et al., 2014). Patsaki et al. (2022) emphasized I-VR’s sensory richness, whereas Zhang et al. (2025) and Molier et al. (2010) highlighted the effectiveness of NI-VR systems, particularly when tasks are gamified and adaptive. Hao et al. (2024) found no consistent superiority of any single modality, suggesting that contextual and patient-related factors such as tolerance, stage of recovery, and resource availability are critical in modality selection. However, considering the significant fine mobility improvements reported by the only study involving a mixed VR modality (Colomer et al., 2016), the comparative efficacy with single-modality treatments (I, SI, and NI) remains an open question.
4.2 Neurophysiological correlates, stroke phase, and VR treatment response
VR promotes neuroplasticity through repetitive, task-specific, multisensory stimulation that engages both motor and cognitive networks (Laver et al., 2015). Functional neuroimaging studies demonstrate that VR tasks can induce neural reorganization, increase cortical excitability, strengthen sensorimotor connectivity, and enhance activity in prefrontal areas during cognitive–motor tasks (Calabrò et al., 2017; Shin et al., 2016; Feitosa et al., 2022). I-VR and SI-VR may more strongly activate visuospatial integration areas, whereas NI-VR can still promote significant reorganization when the feedback is salient and tasks are motivating (Mirelman et al., 2011). These mechanisms likely underlie the dual-domain benefits observed in our review. Our stratified analysis showed VR to be effective in both chronic and subacute phases, with no significant differences in motor outcomes by the stroke stage. However, a study suggested that the subacute stage may offer heightened neuroplastic potential, allowing faster gains in some cases (Hao et al., 2024). Chronic patients, nevertheless, can achieve meaningful improvements when therapy remains intensive and engaging (Patsaki et al., 2022; Laver et al., 2017). The adaptability of VR tasks makes them suitable across recovery stages, with adjustments in difficulty, duration, and feedback tailored to each phase.
4.3 Clinical implications and recommendations
The results of this review highlight the value of VR as an adjunct to conventional rehabilitation for post-stroke patients, yet they also suggest that its effectiveness depends on patient-related factors that should be carefully considered in clinical practice. The stroke stage appears to play an important role. Although our analysis did not identify statistically significant differences in outcomes between subacute and chronic patients, existing evidence suggests that the subacute phase may represent a window of heightened neuroplastic potential in which VR interventions could accelerate functional recovery (Peng et al., 2021). At the same time, patients in the chronic stage are not excluded from potential benefits. Intensive and engaging VR protocols support meaningful gains even several months or years after stroke, indicating that treatment is delivered with sufficient frequency and challenge (Laver et al., 2017). Another determinant of treatment success is the severity of motor impairment. Patients with mild-to-moderate deficits often respond well to non-immersive or semi-immersive VR environments, including commercial gaming platforms or home-based telerehabilitation programs, which combine accessibility with strong motivational components. In contrast, individuals with more severe impairments may require robotic-assisted or sensor-based VR systems that provide physical support, multimodal feedback, and a higher level of guidance to facilitate active participation (Aprile et al., 2021; Mazzoleni et al., 2018). In this sense, tailoring the level of technological assistance to the patient’s motor profile is crucial to maximizing engagement and avoiding frustration. Cognitive status also influences the suitability of different VR modalities. Immersive systems, which demand sustained attention and tolerance of sensory load, may be more appropriate for patients with preserved cognitive and perceptual abilities, whereas simpler non-immersive setups may better serve individuals with cognitive impairments or limited tolerance. Motivation and adherence emerge as additional key factors as VR’s capacity to provide real-time feedback, gamified challenges, and socially meaningful tasks can reinforce patient engagement and ultimately promote functional recovery (Proffitt and Lange, 2015).
From a clinical perspective, these findings suggest that VR cannot be applied indiscriminately but should instead be integrated into individualized rehabilitation plans. Subacute patients with moderate deficits may benefit from early exposure to semi-immersive or non-immersive VR to capitalize on neuroplasticity, whereas chronic patients with severe impairments may still achieve progress when supported by robotic VR systems. Immersive VR may be reserved for those able to tolerate and benefit from enriched environments, whereas home-based VR represents a promising solution for maintaining therapy intensity after discharge, indicating that appropriate monitoring and safety protocols are ensured.
In conclusion, VR should be regarded not as a one-size-fits-all intervention but rather as a flexible therapeutic platform whose modality and intensity can be adapted to stroke stage, impairment severity, cognitive status, and contextual factors. By stratifying patients along these dimensions, clinicians can better determine who is most likely to benefit from VR-based rehabilitation, thereby optimizing outcomes and enhancing the translation of this technology into routine practice.
Author contributions
DC: Conceptualization, Methodology, Supervision, Writing - original draft, Writing - review and editing. CA: Data curation, Resources, Writing - original draft, Writing - review and editing. FC: Resources, Visualization, Writing - review and editing. GG: Data curation, Resources, Writing - review and editing. AG: Data curation, Validation, Writing - review and editing. MM: Supervision, Validation, Writing - review and editing. CR: Resources, Supervision, Writing - review and editing. AQ: Project administration, Resources, Writing - review and editing. FT: Data curation, Investigation, Methodology, Writing - review and editing. RC: Data curation, Supervision, Validation, Writing - review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by Current Research Funds 2025, Ministry of Health, Italy.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2025.1653968/full#supplementary-material
References
Abd El-Kafy, E. M., Alshehri, M. A., El-Fiky, A. A., Guermazi, M. A., and Mahmoud, H. M. (2022). The effect of robot-mediated virtual reality gaming on upper limb spasticity poststroke: a randomized-controlled trial. Games Health J. 11 (2), 93–103. doi:10.1089/g4h.2021.0197
Adams, R. J., Ellington, A. L., Kuccera, K. A., Leaman, H., Smithson, C., and Patrie, J. T. (2023). Telehealth-guided virtual reality for recovery of upper extremity function following stroke. OTJR (Thorofare N J) 43 (3), 446–456. doi:10.1177/15394492231158375
Aprile, I., Guardati, G., Cipollini, V., Papadopoulou, D., Monteleone, S., Redolfi, A., et al. (2021). Influence of cognitive impairment on the recovery of subjects with subacute stroke undergoing upper limb robotic rehabilitation. Brain Sci. 11 (5), 587. PMID: 33946452; PMCID: PMC8147141. doi:10.3390/brainsci11050587
Aşkın, A., Atar, E., Koçyiğit, H., and Tosun, A. (2018). Effects of Kinect-based virtual reality game training on upper extremity motor recovery in chronic stroke. Somatosens. Mot. Res. 35 (1), 25–32. doi:10.1080/08990220.2018.1444599
Bernhardt, J., Hayward, K., Kwakkel, G., Ward, N. S., Wolf, S. L., Borschmann, K., et al. (2017). Agreed definitions and a shared vision for new standards in stroke recovery research: the stroke recovery and rehabilitation roundtable taskforce. Int. J. Stroke 12 (5), 444–450. doi:10.1177/1747493017711816
Brunner, I., Skouen, J. S., Hofstad, H., Aßmus, J., Becker, F., Sanders, A. M., et al. (2017). Virtual reality training for upper extremity in subacute stroke (VIRTUES): a multicenter RCT. Neurology 89 (24), 2413–2421. doi:10.1212/WNL.0000000000004744
Calabrò, R. S., Russo, M., Naro, A., De Luca, R., Leo, A., Tomasello, P., et al. (2017). Robotic gait training in multiple sclerosis rehabilitation: can virtual reality make the difference? Findings from a randomized controlled trial. J. neurological Sci. 377, 25–30. doi:10.1016/j.jns.2017.03.047
Cano-de-la-Cuerda, R., Molero-Sánchez, A., Carratalá-Tejada, M., Alguacil-Diego, I. M., Molina-Rueda, F., Miangolarra-Page, J. C., et al. (2015). Theories and control models and motor learning: clinical applications in neuro-rehabilitation. Neurol. Barc. Spain 30 (1), 32–41. doi:10.1016/j.nrl.2011.12.010
Chang, E., Kim, H. T., and Yoo, B. (2020). Virtual reality sickness: a review of causes and measurements. Int. J. Hum. Comput. Interact. 36, 1658–1682. doi:10.1080/10447318.2020.1778351
Colomer, C., Llorens, R., Noé, E., and Alcañiz, M. (2016). Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke. J. Neuroeng Rehabil. 13 (1), 45. doi:10.1186/s12984-016-0153-6
Cramer, S. C., Sur, M., Dobkin, B. H., O'Brien, C., Sanger, T. D., Trojanowski, J. Q., et al. (2011). Harnessing neuroplasticity for clinical applications. Brain a J. neurology 134 (Pt 6), 1591–1609. doi:10.1093/brain/awr039
Dahdah, M. N., Bennett, M., Prajapati, P., Parsons, T. D., Sullivan, E., and Driver, S. (2017). Application of virtual environments in a multi-disciplinary day neurorehabilitation program to improve executive functioning using the Stroop task. NeuroRehabilitation 41 (4), 721–734. PMID: 29254114. doi:10.3233/NRE-172183
Duret, C., Courtial, O., Grosmaire, A. G., and Hutin, E. (2015). Use of a robotic device for the rehabilitation of severe upper limb paresis in subacute stroke: exploration of patient/robot interactions and the motor recovery process. Biomed. Res. Int. 2015, 1–7. doi:10.1155/2015/482389
Einstad, M. S., Saltvedt, I., Lydersen, S., Ursin, M. H., Munthe-Kaas, R., Ihle-Hansen, H., et al. (2021). Associations between post-stroke motor and cognitive function: a cross-sectional study. BMC Geriatr. 21, 103. doi:10.1186/s12877-021-02055-7
Feitosa, J. A., Fernandes, C. A., Casseb, R. F., and Castellano, G. (2022). Effects of virtual reality-based motor rehabilitation: a systematic review of fMRI studies. J. Neural Eng. 19 (1), 011002. doi:10.1088/1741-2552/ac456e
Fernández-Vázquez, D., Cano-de-la-Cuerda, R., and Navarro-López, V. (2022). Haptic glove systems in combination with semi-immersive virtual reality for upper extremity motor rehabilitation after stroke: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 19 (16), 10378. doi:10.3390/ijerph191610378
GBD 2019 Stroke Collaborators (2021). Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease Study 2019. Lancet Neurol. 20 (10), 795–820. doi:10.1016/S1474-4422(21)00252-0
Gerardin, E., Bontemps, D., Babuin, N. T., Herman, B., Denis, A., Bihin, B., et al. (2022). Bimanual motor skill learning with robotics in chronic stroke: comparison between minimally impaired and moderately impaired patients, and healthy individuals. J. Neuroeng Rehabil. 19 (1), 28. doi:10.1186/s12984-022-01009-3
Hao, J., Crum, G., and Siu, K. C. (2024). Effects of virtual reality on stroke rehabilitation: an umbrella review of systematic reviews. Health Sci. Rep. 7 (9), e70082. doi:10.1002/hsr2.70082
Howard, M. C. (2017). A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput. Hum. Behav. 70, 317–327. doi:10.1016/j.chb.2017.01.013
Johnson, N. N., Carey, J., Edelman, B. J., Doud, A., Grande, A., Lakshminarayan, K., et al. (2018). Combined rTMS and virtual reality brain-computer interface training for motor recovery after stroke. J. Neural Eng. 15, 016009. doi:10.1088/1741-2552/aa8ce3
Jung, H. T., Kim, H., Jeong, J., Jeon, B., Ryu, T., and Kim, Y. (2017). Feasibility of using the RAPAEL Smart Glove in upper limb physical therapy for patients after stroke: a randomized controlled trial. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2017, 3856–3859. doi:10.1109/EMBC.2017.8037698
Kim, G. J., Hinojosa, J., Rao, A. K., Batavia, M., and O'Dell, M. W. (2017). Randomized trial on the effects of attentional focus on motor training of the upper extremity using robotics with individuals after chronic stroke. Arch. Phys. Med. Rehabil. 98 (10), 1924–1931. doi:10.1016/j.apmr.2017.06.005
Kong, K. H., Loh, Y. J., Thia, E., Chai, A., Ng, C. Y., Soh, Y. M., et al. (2016). Efficacy of a virtual reality commercial gaming device in upper limb recovery after stroke: a randomized, controlled Study. Top. Stroke Rehabil. 23 (5), 333–340. doi:10.1080/10749357.2016.1139796
Lam, S. S. L., Liu, T. W., Ng, S. S. M., Lai, C. W. K., and Woo, J. (2022). Bilateral movement-based computer games improve sensorimotor functions in subacute stroke survivors. J. Rehabil. Med. 54, jrm00307. doi:10.2340/jrm.v54.913
Laver, K., George, S., Thomas, S., Deutsch, J. E., and Crotty, M. (2015). Virtual reality for stroke rehabilitation: an abridged version of a Cochrane review. Eur. J. Phys. rehabilitation Med. 51 (4), 497–506.
Laver, K. E., Lange, B., George, S., Deutsch, J. E., Saposnik, G., Crotty, M., et al. (2017). Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2025 (11). doi:10.1002/14651858.cd008349.pub5
Laver, K., George, S., Thomas, S., Deutsch, J., and Crotty, M. (2021). Virtual reality for stroke rehabilitation: an abridged version of a Cochrane review. Eur. J. Phys. Rehabilitation Med. 57 (1), 140–148.
Lee, K. (2019). Speed-Interactive pedaling training using smartphone virtual reality application for stroke patients: Single-Blinded, randomized clinical trial. Brain Sci. 9 (11), 295. doi:10.3390/brainsci9110295
Llorens, R., Fuentes, M. A., Borrego, A., Latorre, J., Alcañiz, M., Colomer, C., et al. (2021). Effectiveness of a combined transcranial direct current stimulation and virtual reality-based intervention on upper limb function in chronic individuals post-stroke with persistent severe hemiparesis: a randomized controlled trial. J. Neuroeng Rehabil. 18 (1), 108. doi:10.1186/s12984-021-00896-2
Lohse, K. R., Hilderman, C. G., Cheung, K. L., Tatla, S., and Van der Loos, H. F. (2014). Virtual reality therapy for adults post-stroke: a systematic review and meta-analysis exploring virtual environments and commercial games in therapy. PloS one 9 (3), e93318. doi:10.1371/journal.pone.0093318
Lu, R. R., Zheng, M. X., Li, J., Gao, T. H., Hua, X. Y., Liu, G., et al. (2020). Motor imagery based brain-computer interface control of continuous passive motion for wrist extension recovery in chronic stroke patients. Neurosci. Lett. 718, 134727. doi:10.1016/j.neulet.2019.134727
Luo, Z., Lim, A. E., Durairaj, P., Tan, K. K., and Verawaty, V. (2023). Development of a compensation-aware virtual rehabilitation system for upper extremity rehabilitation in community-dwelling older adults with stroke. J. Neuroeng Rehabil. 20 (1), 56. doi:10.1186/s12984-023-01183-y
Maier, M., Rubio Ballester, B., Duff, A., Duarte Oller, E., and Verschure, P. F. M. J. (2019). Effect of specific over nonspecific VR-Based rehabilitation on poststroke motor recovery: a systematic meta-analysis. Neurorehabilitation neural repair 33 (2), 112–129. doi:10.1177/1545968318820169
Maistrello, L., Rimini, D., Cheung, V. C. K., Pregnolato, G., and Turolla, A. (2021). Muscle synergies and clinical outcome measures describe different factors of upper limb motor function in stroke survivors undergoing rehabilitation in a virtual reality environment. Sensors (Basel) 21 (23), 8002. doi:10.3390/s21238002
Makmee, P., and Wongupparaj, P. (2022). Virtual reality-based cognitive intervention for enhancing executive functions in community-dwelling older adults. Psychosoc. Interv. 31 (3), 133–144. doi:10.5093/pi2022a10
Manuli, A., Maggio, M. G., Latella, D., Cannavò, A., Balletta, T., De Luca, R., et al. (2020). Can robotic gait rehabilitation plus Virtual Reality affect cognitive and behavioural outcomes in patients with chronic stroke? A randomized controlled trial involving three different protocols. J. Stroke Cerebrovasc. Dis. 29 (8), 104994. doi:10.1016/j.jstrokecerebrovasdis.2020.104994
Massetti, T., da Silva, T. D., Crocetta, T. B., Guarnieri, R., de Freitas, B. L., Bianchi Lopes, P., et al. (2018). The clinical utility of virtual reality in neurorehabilitation: a systematic review. J. Cent. Nerv. Syst. Dis. 27, 1179573518813541. doi:10.1177/1179573518813541
Mazzoleni, S., Puzzolante, L., Zollo, L., Dario, P., and Posteraro, F. (2014). Mechanisms of motor recovery in chronic and subacute stroke patients following a robot-aided training. IEEE Trans. Haptics 7 (2), 175–180. PMID: 24968381. doi:10.1109/TOH.2013.73
Mazzoleni, S., Tran, V. D., Dario, P., and Posteraro, F. (2018). Wrist robot-assisted rehabilitation treatment in subacute and chronic stroke patients: from distal to proximal motor recovery. IEEE Trans. Neural Syst. Rehabil. Eng. 26, 1889–1896. doi:10.1109/TNSRE.2018.2864935
Mekbib, D. B., Debeli, D. K., Zhang, L., Fang, S., Shao, Y., Yang, W., et al. (2021). A novel fully immersive virtual reality environment for upper extremity rehabilitation in patients with stroke. Ann. N. Y. Acad. Sci. 1493 (1), 75–89. doi:10.1111/nyas.14554
Mirelman, A., Maidan, I., Herman, T., Deutsch, J. E., Giladi, N., and Hausdorff, J. M. (2011). Virtual reality for gait training: can it induce motor learning to enhance complex walking and reduce fall risk in patients with Parkinson's disease? journals gerontology. Ser. A, Biol. Sci. Med. Sci. 66 (2), 234–240. doi:10.1093/gerona/glq201
Molier, B. I., Van Asseldonk, E. H., Hermens, H. J., and Jannink, M. J. (2010). Nature, timing, frequency and type of augmented feedback; does it influence motor relearning of the hemiparetic arm after stroke? A systematic review. Disabil. rehabilitation 32 (22), 1799–1809. doi:10.3109/09638281003734359
Mugler, E. M., Tomic, G., Singh, A., Hameed, S., Lindberg, E. W., Gaide, J., et al. (2019). Myoelectric computer interface training for reducing Co-Activation and enhancing arm movement in chronic stroke survivors: a randomized trial. Neurorehabil Neural Repair 33 (4), 284–295. doi:10.1177/1545968319834903
Norouzi-Gheidari, N., Archambault, P. S., and Fung, J. (2020). Changes in arm kinematics of chronic stroke individuals following “Assist-As-Asked” robot-assisted training in virtual and physical environments: a proof-of-concept study. J. Rehabil. Assist. Technol. Eng. 7, 2055668320926054. doi:10.1177/2055668320926054
Noveletto, F., Soares, A. V., Eichinger, F. L. F., Domenech, S. C., Hounsell, M. D. S., and Filho, P. B. (2020). Biomedical serious game System for lower limb motor rehabilitation of hemiparetic stroke patients. IEEE Trans. Neural Syst. Rehabil. Eng. 28 (6), 1481–1487. Epub 2020 Apr 16. PMID: 32305932. doi:10.1109/TNSRE.2020.2988362
Palermo, E., Hayes, D. R., Russo, E. F., Calabrò, R. S., Pacilli, A., and Filoni, S. (2018). Translational effects of robot-mediated therapy in subacute stroke patients: an experimental evaluation of upper limb motor recovery. PeerJ 6, e5544. doi:10.7717/peerj.5544
Paquin, K., Ali, S., Carr, K., Crawley, J., McGowan, C., and Horton, S. (2015). Effectiveness of commercial video gaming on fine motor control in chronic stroke within community-level rehabilitation. Disabil. Rehabil. 37 (23), 2184–2191. doi:10.3109/09638288.2014.1002574
Patel, J., Fluet, G., Qiu, Q., Yarossi, M., Merians, A., Tunik, E., et al. (2019). Intensive virtual reality and robotic based upper limb training compared to usual care, and associated cortical reorganization, in the acute and early sub-acute periods post-stroke: a feasibility study. J. Neuroeng Rehabil. 16, 92. doi:10.1186/s12984-019-0563-3
Patsaki, I., Dimitriadi, N., Despoti, A., Tzoumi, D., Leventakis, N., Roussou, G., et al. (2022). The effectiveness of immersive virtual reality in physical recovery of stroke patients: a systematic review. Front. Syst. Neurosci. 16, 880447. doi:10.3389/fnsys.2022.880447
Peng, Q. C., Yin, L., and Cao, Y. (2021). Effectiveness of virtual reality in the rehabilitation of motor function of patients with subacute stroke: a meta-analysis. Front. neurology 12, 639535. doi:10.3389/fneur.2021.639535
Proffitt, R., and Lange, B. (2015). Considerations in the efficacy and effectiveness of virtual reality interventions for stroke rehabilitation: moving the field forward. Phys. Ther. 95 (3), 441–448. doi:10.2522/ptj.20130571
Ranzani, R., Lambercy, O., Metzger, J. C., Califfi, A., Regazzi, S., Dinacci, D., et al. (2020). Neurocognitive robot-assisted rehabilitation of hand function: a randomized control trial on motor recovery in subacute stroke. J. Neuroeng Rehabil. 17 (1), 115. doi:10.1186/s12984-020-00746-7
Rizzo, A. S., and Koenig, S. T. (2017). Is clinical virtual reality ready for primetime? Neuropsychology 31 (8), 877–899. doi:10.1037/neu0000405
Rong, J., Ding, L., Xiong, L., Zhang, W., Wang, W., Deng, M., et al. (2021). Mirror visual feedback prior to robot-assisted training facilitates rehabilitation after stroke: a randomized controlled Study. Front. Neurol. 12, 683703. doi:10.3389/fneur.2021.683703
Roussou, G., Despoti, A., Patsaki, I., Tzoumi, D., Leventakis, N., Dimitriadi, N., et al. (2024). Suitability, usability and safety of fully immersive Virtual Reality applications for motor and cognitive rehabilitation in stroke patients preliminary data. Health and Res. J. 10 (3), 193–205. doi:10.12681/healthresj.34734
Sale, P., Bovolenta, F., Agosti, M., Clerici, P., and Franceschini, M. (2014). Short-term and long-term outcomes of serial robotic training for improving upper limb function in chronic stroke. Int. J. Rehabil. Res. 37 (1), 67–73. doi:10.1097/MRR.0000000000000036
Saleh, S., Fluet, G., Qiu, Q., Merians, A., Adamovich, S. V., and Tunik, E. (2017). Neural patterns of reorganization after intensive robot-assisted virtual reality therapy and repetitive task practice in patients with chronic stroke. Front. Neurol. 8, 452. doi:10.3389/fneur.2017.00452
Saposnik, G., Cohen, L. G., Mamdani, M., Pooyania, S., Ploughman, M., Cheung, D., et al. (2016). Efficacy and safety of non-immersive virtual reality exercising in stroke rehabilitation (EVREST): a randomised, multicentre, single-blind, controlled trial. Lancet Neurol. 15, 1019–1027. doi:10.1016/S1474-4422(16)30121-1
Schaefer, S., and Schumacher, V. (2009). The interplay between cognitive and motor functioning in healthy older adults: findings from dual-task studies and implications for neurorehabilitation. Neuropsychology 23 (2), 187–199. doi:10.1037/a0014188
Schuster-Amft, C., Eng, K., Suica, Z., Thaler, I., Signer, S., Lehmann, I., et al. (2018). Effect of a four-week virtual reality-based training versus conventional therapy on upper limb motor function after stroke: a multicenter parallel group randomized trial. PLoS One 13 (10), e0204455. doi:10.1371/journal.pone.0204455
Şenocak, E., Korkut, E., Aktürk, A., and Ozer, A. Y. (2023). Is the robotic rehabilitation that is added to intensive body rehabilitation effective for maximization of upper extremity motor recovery following a stroke? A randomized controlled study. Neurol. Sci. 44 (8), 2835–2843. doi:10.1007/s10072-023-06739-3
Shin, J. H., Kim, M. Y., Lee, J. Y., Jeon, Y. J., Kim, S., Lee, S., et al. (2016). Effects of virtual reality-based rehabilitation on distal upper extremity function and health-related quality of life: a single-blinded, randomized controlled trial. J. neuroengineering rehabilitation 13, 17. doi:10.1186/s12984-016-0125-x
Sip, P., Kozłowska, M., Czysz, D., Daroszewski, P., and Lisiński, P. (2023). Perspectives of motor functional upper extremity recovery with the use of immersive virtual reality in stroke patients. Sensors (Basel) 23 (2), 712. doi:10.3390/s23020712
Taravati, S., Capaci, K., Uzumcugil, H., and Tanigor, G. (2022). Evaluation of an upper limb robotic rehabilitation program on motor functions, quality of life, cognition, and emotional status in patients with stroke: a randomized controlled study. Neurol. Sci. 43 (2), 1177–1188. doi:10.1007/s10072-021-05431-8
Thielbar, K. O., Lord, T. J., Fischer, H. C., Lazzaro, E. C., Barth, K. C., Stoykov, M. E., et al. (2014). Training finger individuation with a mechatronic-virtual reality system leads to improved fine motor control post-stroke. J. Neuroeng Rehabil. 11, 171. doi:10.1186/1743-0003-11-171
Thielbar, K. O., Triandafilou, K. M., Barry, A. J., Yuan, N., Nishimoto, A., Johnson, J., et al. (2020). Home-based upper extremity stroke therapy using a multiuser virtual reality environment: a randomized trial. Arch. Phys. Med. Rehabil. 101 (2), 196–203. doi:10.1016/j.apmr.2019.10.182
Torrisi, M., Maggio, M. G., De Cola, M. C., Zichittella, C., Carmela, C., Porcari, B., et al. (2021). Beyond motor recovery after stroke: the role of hand robotic rehabilitation plus virtual reality in improving cognitive function. J. Clin. Neurosci. 92, 11–16. doi:10.1016/j.jocn.2021.07.053
Valdés, B. A., and Van der Loos, H. F. M. (2018). Biofeedback vs game scores for reducing trunk compensation after stroke: a randomized crossover trial. Top. Stroke Rehabil. 25 (2), 96–113. doi:10.1080/10749357.2017.1394633
Weiss, P. L., Rand, D., Katz, N., and Kizony, R. (2004). Video capture virtual reality as a flexible and effective rehabilitation tool. J. neuroengineering rehabilitation 1 (1), 12. doi:10.1186/1743-0003-1-12
Yao, X., Cui, L., Wang, J., Feng, W., Bao, Y., and Xie, Q. (2020). Effects of transcranial direct current stimulation with virtual reality on upper limb function in patients with ischemic stroke: a randomized controlled trial. J. Neuroeng Rehabil. 17 (1), 73. PMID: 32539812; PMCID: PMC7296643. doi:10.1186/s12984-020-00699-x
Yeh, S. C., Lee, S. H., Chan, R. C., Wu, Y., Zheng, L. R., and Flynn, S. (2017). The efficacy of a haptic-enhanced virtual reality System for precision grasp acquisition in stroke rehabilitation. J. Healthc. Eng. 2017, 1–9. doi:10.1155/2017/9840273
Yuan, Z., Peng, Y., Wang, L., Song, S., Chen, S., Yang, L., et al. (2021). Effect of BCI-Controlled pedaling training System with multiple modalities of feedback on motor and cognitive function rehabilitation of early subacute stroke patients. IEEE Trans. Neural Syst. Rehabil. Eng. 29, 2569–2577. doi:10.1109/TNSRE.2021.3132944
Zhang, R., Wang, C., He, S., Zhao, C., Zhang, K., Wang, X., et al. (2023). An adaptive brain-computer interface to enhance motor recovery after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 31, 2268–2278. doi:10.1109/TNSRE.2023.3272372
Keywords: stroke, virtual reality, neurorehabilitation, executive functions, motor recovery, neuroplasticity
Citation: Cardile D, Arena C, Corallo F, Giuffrida GM, Giustiniani A, Maggio MG, Rifici C, Quartarone A, Tomaiuolo F and Calabrò RS (2025) A systematic review on the use of virtual reality in post-stroke patients: exploring when modalities make the difference in executive and motor recovery. Front. Virtual Real. 6:1653968. doi: 10.3389/frvir.2025.1653968
Received: 25 June 2025; Accepted: 26 August 2025;
Published: 01 October 2025.
Edited by:
Marientina Gotsis, University of Southern California, United StatesReviewed by:
Engy BadrEldin Saleh Moustafa, Cairo University, EgyptIrini Patsaki, University of West Attica, Greece
Rita Huan-Ting Peng, University of Illinois at Urbana-Champaign, United States
Copyright © 2025 Cardile, Arena, Corallo, Giuffrida, Giustiniani, Maggio, Rifici, Quartarone, Tomaiuolo and Calabrò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiara Arena, Y2hpYXJhLmFyZW5hQGlyY2NzbWUuaXQ=