 Gonçalo Torrinha1*†Tatiana Gonçalves1,†Maria Sousa2,†
Gonçalo Torrinha1*†Tatiana Gonçalves1,†Maria Sousa2,† Gerrit Högemann3André Goulart1,2,4
Gerrit Högemann3André Goulart1,2,4 Alexandre Fernandes Carvalho1Pedro Leão1,2,4
Alexandre Fernandes Carvalho1Pedro Leão1,2,4
- 1Life and Health Sciences Research Institute (ICVS), Medical School, University of Minho, Braga, Portugal
- 2General Surgery Department, Hospital Privado de Braga, Grupo Trofa Saúde, Braga, Portugal
- 3General Surgery Department, Städtisches Klinikum Karlsruhe, Karlsruhe, Germany
- 4ICVS/3B's – PT – Surgical Science Department, Government Associate Laboratory, Braga/Guimarães, Portugal
Purpose: Haemorrhoids are normal structures in the human body, only seen as pathological when symptomatic. Nowadays, new techniques have surfaced using a diode laser which, after locating the target arteries, blocks the blood flow while hitting and shrinking the local mucosa/submucosa at a depth of 4 mm. Our work aimed to give a broad view over this new technique and its consequences in the post-operative follow-up with a systematic review.
Methods: EMBASE and MEDLINE databases were consulted, retrieving clinical trials, which mentioned the use of 980 nm diode laser on the treatment of haemorrhoids.
Results: Ten clinical trials analyzing the post-operative effects of laser haemorrhoidectomy were selected, including 2 randomized controlled clinical trials and 1 controlled clinical trial. The overall quality of the trials was low, indicating a high risk of bias.
Conclusion: The laser haemorrhoidectomy procedure revealed a high therapeutic potential, considering the reduced number of postoperative complaints (bleeding/pain), the high symptom resolution and the reduced recurrence, albeit the high heterogeneity between the studies in terms of reported results. Future investigations with higher quality and controlled double-blinded studies obtaining better-categorized results should be conducted in order to better evaluate this procedure and compare it to the current paradigm.
Introduction
Description of the condition
Haemorrhoids are normal structures of the human body (1–3). They are usually classified by their location: internal (originates above the dentate line and covered by anal mucosa) and external (originates below the dentate line and covered by anoderm) (2, 4). The internal haemorrhoidal plexus presents itself as anal cushions or sinusoids and consists of arterioles, venules and arteriovenular anastomoses (5).
Generally, haemorrhoids are viewed as a disease when they become symptomatic (6). The most common presentation of hemorrhoidal disease is painless rectal bleeding during defection (3, 6). Pain in patients with haemorrhoids is more likely due to anal fissures and anorectal abscesses (7).
The pathophysiology of internal haemorrhoids is still not fully understood. However, one theory postulates that a chronic rise in intra-abdominal pressure in combination with the absence of valves within rectal veins, can limit venous drainage from sinusoids during defecation, resulting in abnormal dilatation of the sinusoids and, in turn, bleeding due to bursting and/or mucosal damage (2, 8). The Goligher classification is commonly used to grade the severity of haemorrhoids and consequently indicates the modality of surgical treatment (9). Grade I corresponds to non-prolapsing haemorrhoids and grade II to prolapsing haemorrhoids on defecation with spontaneous reduction (10). In advanced stages, the additional disintegration of conjoined longitudinal muscle results in their remaining permanently outside the anus, either manually reversible (3rd degree) or nonreversible (4th degree) (11, 12).
Description of the intervention
The haemorrhoidal laser procedure (HeLP) uses a diode laser, delivered at 980 nm of wavelength (13 W: 5 pulsed shots of 1.2 s each with 0.6 s pause), acting selectively on haemoglobin and causing the closure of the superior hemorrhoidal arteries. No general anesthesia is required for this procedure and, if requested by the patient, analgesic drugs can be administered intraoperatively. A Doppler-transducer (20 Mhz probe of 3 mm diameter) can be used to help identify the terminal branches of the superior hemorrhoidal arteries approximately 3 cm proximal to the dentate line. This device is inserted into the rectum with the patient in lithotomy position, being substituted by the laser after identification of the target artery (13).
How the intervention might work
The laser cuts off the blood supply to the haemorrhoids and causes shrinkage of the mucosa and submucosa, to a depth of 4 mm (14).
Why this review is important
So far, Milligan-Morgan haemorrhoidectomy is the most commonly used technique in Europe (15). However, this technique is invasive and may lead to severe postoperative pain. An ideal procedure for the treatment of haemorrhoids should have the most symptom resolution paired with minimal postoperative pain and complications, as well as demonstrate less recurrence. The procedure should be cheap and cost-effective too.
With this review we aimed to analyze the effects of the laser procedure in terms of post-operative complications and morbidities and access the therapeutic potential of this procedure.
Methods
This review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) norms (16, 17).
Eligibility criteria
All studies regarding the use of diode lasers with a wavelength of 980 nm on the treatment of haemorrhoids were considered.
Only trials conducted in humans, published in English, reporting original results were selected. Conference abstracts, reviews, commentaries, case reports and book chapters were excluded.
Information sources
Studies were identified by searching the electronic databases MEDLINE and EMBASE. This search was last conducted by the authors on 18th of June 2019.
Search
The following setup of search terms was used for MEDLINE: “(‘haemorrhoidectomy’[MeSH Terms] OR ‘haemorrhoidectomy’[All Fields]) AND (‘lasers’[MeSH Terms] OR ‘lasers’[All Fields] OR ‘laser’[All Fields])”; “(‘lasers’[MeSH Terms] OR ‘lasers’[All Fields] OR‘laser’[All Fields]) AND (‘haemorrhoids’[All Fields] OR ‘haemorrhoids’[MeSH Terms] OR ‘haemorrhoids’[All Fields])”.
The following setups of search terms were used for EMBASE: “‘hemorrhoids laser’ OR ((‘hemorrhoids’/exp OR hemorrhoids) AND (‘laser’/exp OR laser))” and “‘hemorrhoidectomy laser’ OR ((‘hemorrhoidectomy’/exp OR hemor- rhoidectomy) AND (‘laser’/exp OR laser))”.
Study selection
The authors performed an eligibility assessment. In case of questionable eligibility, the results were discussed among all authors. All trials were included, regardless of the existence and type of a comparative group. The primary outcome measure was the impact of the laser on pain and bleeding on post-operative follow-up. The secondaries outcomes were: number of arteries affected by laser, mean time of surgery, time until discharge, resolution and recurrence of symptoms after surgery. Articles including participants with previous surgical treatments for haemorrhoids and concomitant anorectal disorders were excluded. Articles that did not use 980 nm diode lasers as a therapeutic approach or used the laser pared with other surgical procedures were also excluded.
Data collection process
We developed a data extraction sheet with the descripted data of each report, adding new parameters throughout the analysis as soon new data was found. All data extracted by the authors was reviewed twice to avoid errors. In cases of uncertain validity, the results were discussed among all authors. Studies from the same research group or group of authors were carefully analyzed to avoid double counting the same data.
Data items
From each study, we extracted the following data items: (1) participant groups (country, sample size, mean age and gender ratio); (2) disorder (haemorrhoid degree); (3) laser procedure (type of anaesthesia/analgesia, number of arteries affected by laser, mean time of surgery and if the laser procedure was or not Doppler-guided) and (4) main outcome measures (bleeding, pain, time until discharge, resolution and recurrence of symptoms after surgery).
Risk of bias in individual studies
To ascertain the risk of bias of the eligible studies, the authors determined the quality of each study using the critical appraisal skills programme (CASP) checklist for randomized controlled trials (18).
In the case of trials, which did not have a comparison/control group, the methodological quality assessment was established by using the Quality Assessment Tool for Before-After Studies with No Control Group (National Heart Lung and Blood Institute).
Synthesis of results
In order to extract data regarding the outcome variable bleeding, we focused our attention on the occurrence of bleeding after the surgery, only extracting the number of patients with bleeding after laser procedure up to 1 month after surgery.
Concerning the outcome variable “pain”, we extracted “early post-operative pain” data expressed using a visual analogue scale (VAS), as well as the maximum percentage of patients with pain up to 12 months of follow-up. The mean and range values for early post-operative pain data was selected and pulled out according to the following time parameters: first 24 h, 1–3 days and 4–14 days. If the mean value wasn't available, the proportion of patients per VAS score was retrieved; if the range value wasn't available, standard deviation was extracted instead. Each time the percentage of patients with pain was presented as divided between “pain during defecation” and “pain at rest”—we considered “pain” as the sum of these two variables.
Other outcome variables observed were the time until discharge (mean hours and standard deviation, when available), the percentage of patients with complete resolution of symptoms and the percentage of patients with recurrence after 12 months of follow-up.
Results
Study selection
Figure 1 shows the flow diagram representative of the process of study selection. We retrieved 338 potentially relevant reports from our electronic searches. From these, 51 studies were elected to be included in the review after reading the abstract and removing duplicates. From those, 6 articles were discarded due to full text unavailability, as well as 2 reviews and 21 conference abstracts. Twelve studies did not meet the inclusion criteria: no use 980 nm diode lasers (n = 1). no description of the employed laser (n = 7) and no use of diode lasers at all (n = 4).
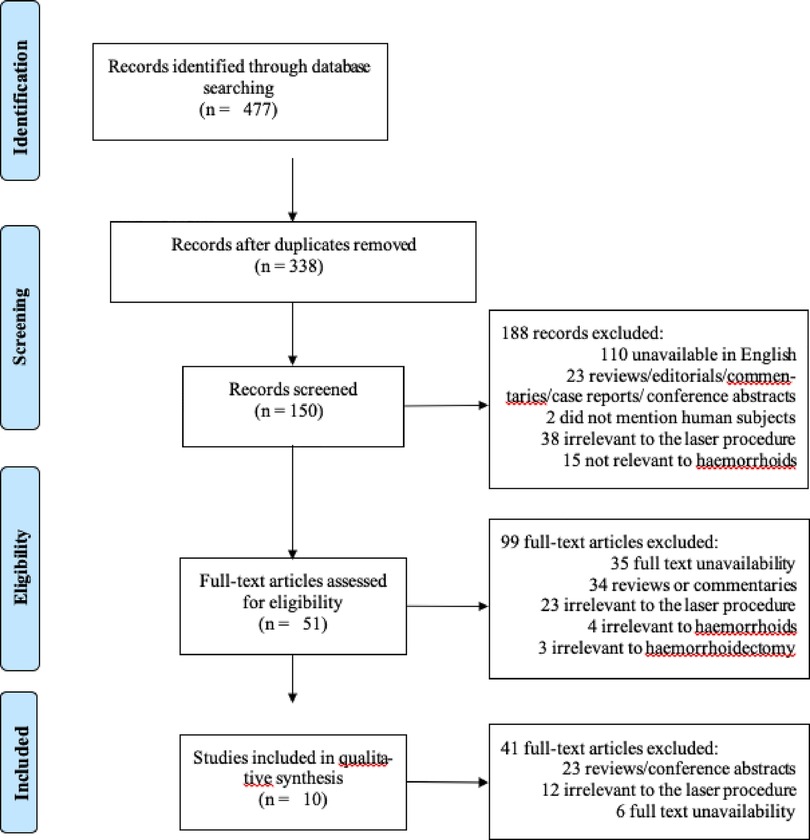
Figure 1. Summary of data collection process.
Study characteristics
All studies included in the systematic review (n = 10) involved the hemorrhoidal laser procedure and were published between 2009 and 2018.
We analyzed three randomized controlled trials; one was performed in Italy (19), one in Kosovo (20), and the other in Iran (21). Two prospective clinical trials were included in our search: one multicentric (22) and another not multicentric (23), both conducted in Italy. Five remaining studies were all clinical trials performed in Italy (13, 24, 25), Israel (15) and Iran (26). Table 1 shows a summary of the studies included in the systematic review. The mean age of the participants for each study ranges between 41.5 and 47.5 years of age [2 articles didn't report mean age (19, 26)]. The sample size ranges between 20 and 341; predominance in male subjects can be observed in most trials, except for two reports (13, 25).
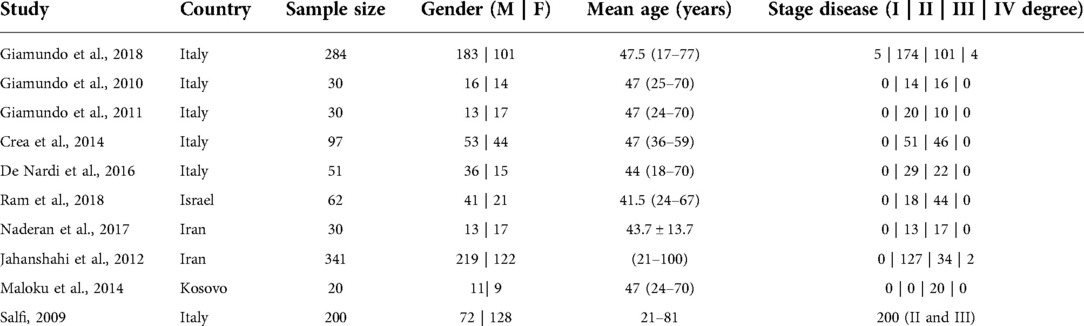
Table 1. Summary of demographic and clinical information of the studies included for systematic reviewing.
Table 2 shows the inclusion and exclusion criteria used by each study. All studies included symptomatic patients, II/III degree, minimal prolapse and failure of conservative treatment. Five full-texts excluded previous surgical treatment, severe prolapse, previous surgical anastomosis less than 3 cm from the dentate line, anal stenosis, fissures and fistulas, and patients under treatment with anticoagulants (15, 19, 21–23). One study included patients taking Low Molecular Weight Heparin (LMWH) and patients with first and fourth degree hemorrhoids (24), and one study included patients with fourth degree hemorrhoids (26). Some articles didn't specify a great number of criteria (20, 25, 26). However, since they followed the HeLP protocol (13) which stated specific guidelines, the assumption was made that inclusion/exclusion criteria were similar.
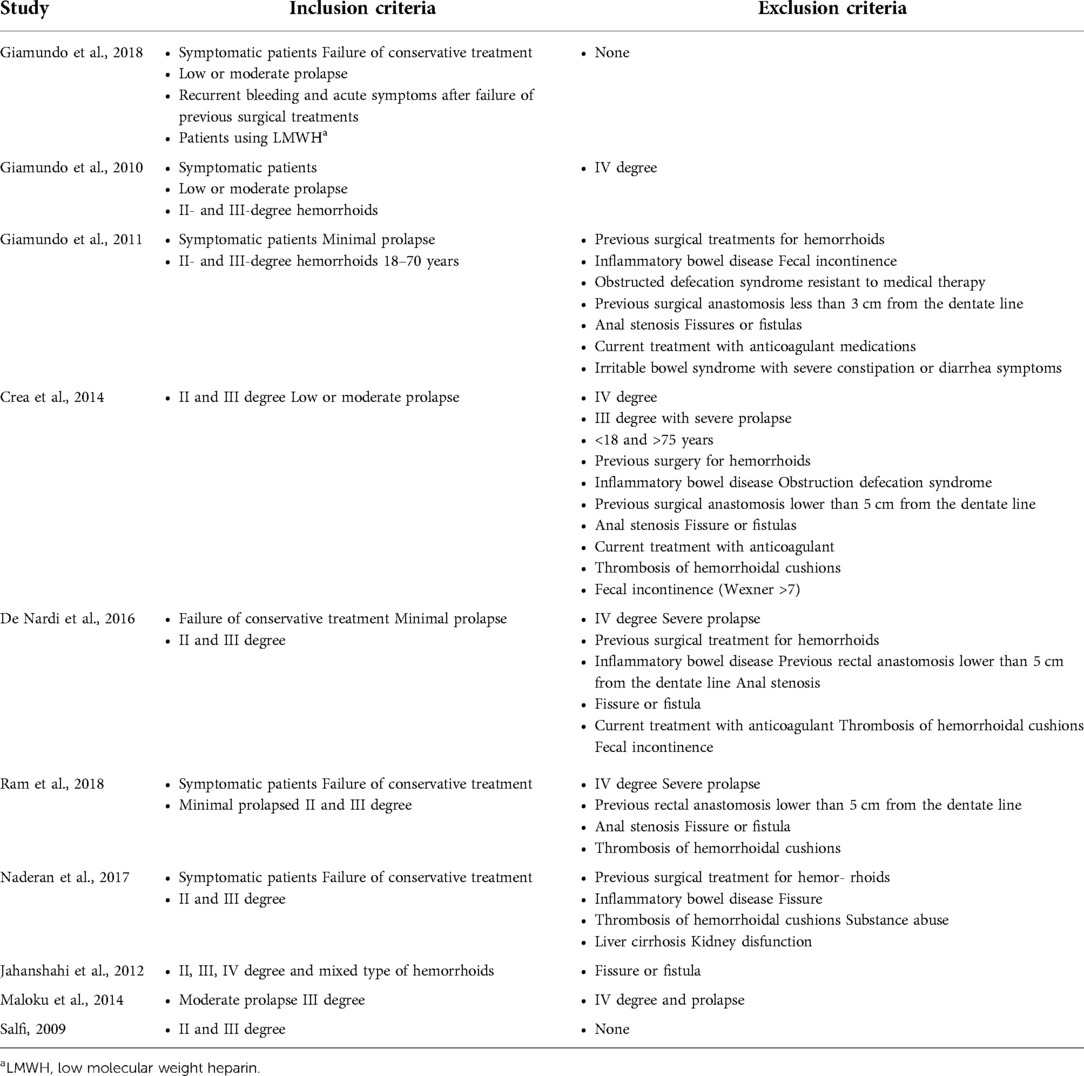
Table 2. Summary of the inclusion and exclusion criteria of the studies included for systematic reviewing.
Table 3 summarizes the surgical procedure information of each study. Out of the 10 studies, two didn't use any anesthesia throughout the procedure (19, 25), two refer some use of topical anesthesia (22, 24), and one mentioned the use of general anesthesia in all patients (21). The overall number of arteries that have undergone the procedure ranged between 8 and 15. The mean surgery duration time ranged between 9.5 and 33.1 min. Almost all studies performed the doppler-guided laser procedure, except for three: Jahanshashi et al., 2012 (26) and Maloku et al., 2014 (20) and Naderan et al., 2017 (21).
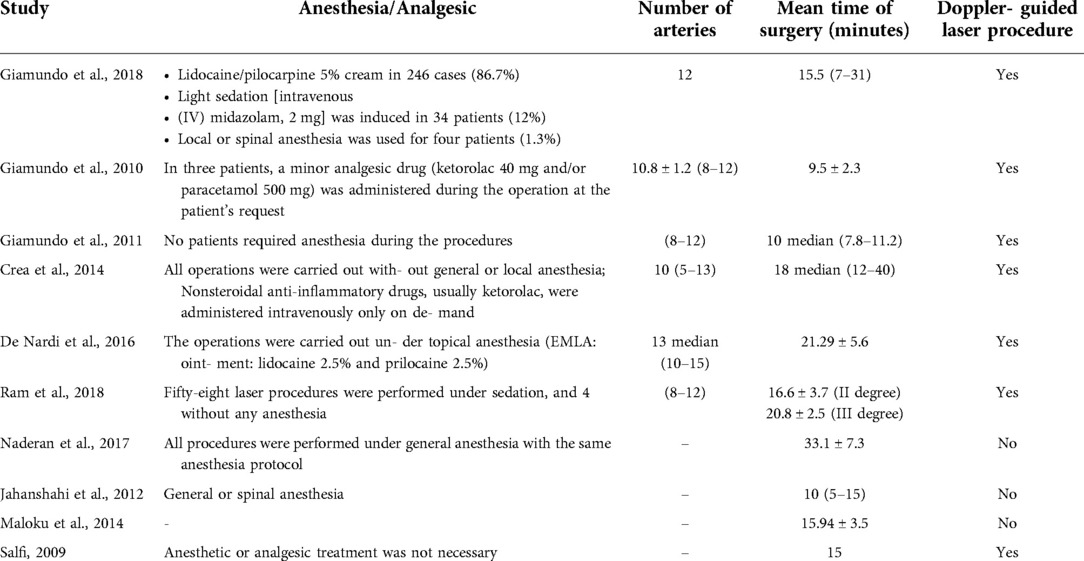
Table 3. Summary of the surgical procedure information of each study by employed anaesthetics, number of arteries implied, procedure time and Doppler assistance.
Risk of bias within studies
Tables 4, 5 compile the information regarding the quality of the studies included in the systematic review.
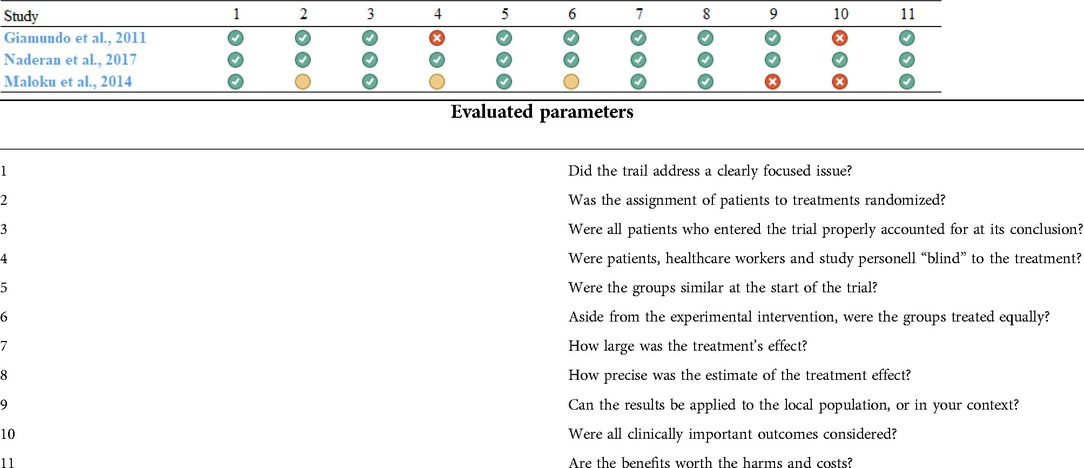
Table 4. Summary of the results of the CASP appraisal list.
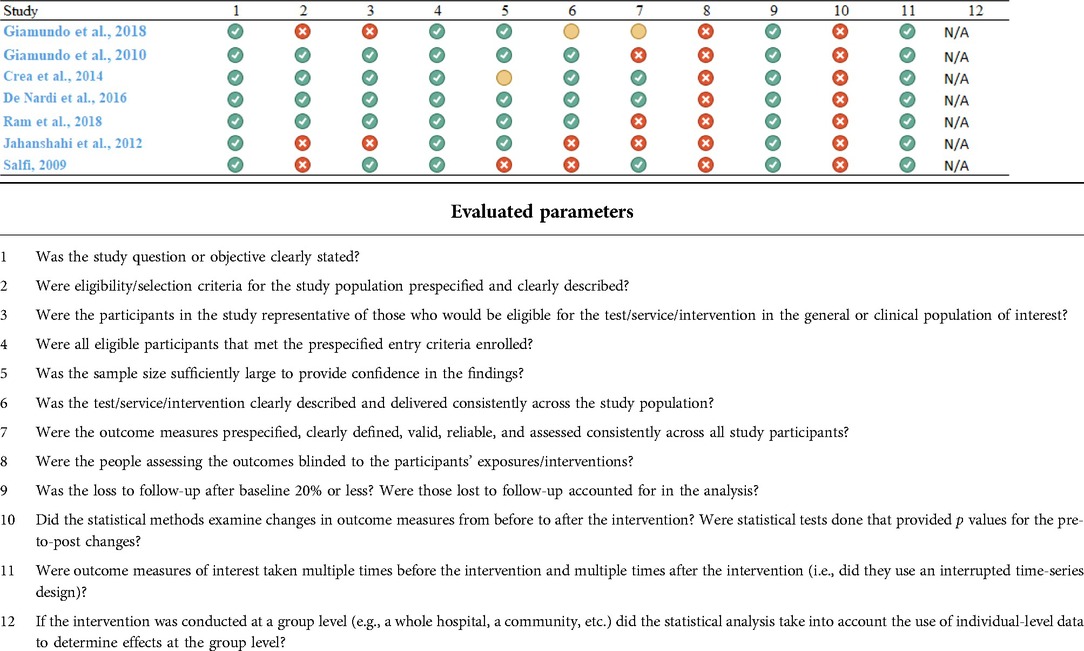
Table 5. Quality assessment tool for before-after studies with no control group (national heart lung and blood institute).
Based on the results, we considered 1 paper of good quality (21), 3 of medium (19, 22, 23) and 5 of low quality (13, 15, 20, 24–26).
From the 3 controlled trials, only Naderan et al. 2017 (21) proved to be effectively double blind and randomized; Giamundo et al. 2011 (19) didn't properly ensure investigator blindness and Maloku et al. 2014 (20) didn't provide any information about the control given over the groups, whether they were randomized or if the participants were “blinded”, both acquiring a substantial degree of bias from these blunders. When evaluating the 7 clinical trials, we faced with no blindness (Parameter 8) and no little to no comparison between the before-after status of the participants (Parameter 10) throughout the different studies. Since the intervention was applied at an individual patient level, the 12th parameter was coded as NA (not applicable). Apart from these bias inducing flaws, the parameter with the least positive mark was the 7th, attaining to the outcome measures, accentuating the same problem observed in the 3 randomized controlled trials of heterogenicity between studies in respect to variables extracted and units of expression of those same variables. Only 4 trials in total expressed an acceptable number of different variables in clinically relevant units of measure (21–23, 25).
Results of individual studies
Table 6 represents a summary of the main outcomes extracted of the studies included. The prospective study by Crea et al. (23) presented with the largest proportion of number of patients with bleeding immediately after the laser procedure up to 1 month post-surgery (25/97) in contrast with the clinical trial by Salfi (25) (1/200). The analysis of the results concerning the early postoperative pain at 24h shows that almost 80% (49/62) of patients presents values of pain between 0 and 1 in Ram et al. (15), in contrast with Maloku et al. (20) where the pain between 0 and 1 is present only in 25% of patients. The maximum mean value of pain after 24 h of surgery until 2 weeks after surgery is 1,4 in Giamundo et al. (19). The percentage of patients with pain until 12 months of follow-up in the different studies mostly ranged between 13.2% and 16.7%. However, Salfi (25) shows 0% of patients with pain until 12 months of follow-up. Naderan et al. (21) and Jahanshahi et al. (26) present a larger time until discharge compared to the other studies (24 and 18 h, respectively). Naderan et al. (21) was the study with the smallest percentage of patients with complete resolution of symptoms (70%), while in the other reports this value ranged between 86.3% and 95%. The percentage of patients with hemorrhoid recurrence did not exceed 9.7%.

Table 6. Main outcomes of the selected studies.
Discussion
Our work aimed to give a broad view over laser haemorrhoidplasty and its post-operative follow up consequences.
The HeLP technique is ineffective in resolving the prolapse, as can be evaluated in the studies of Giamundo and De Nardi (22, 24). For this reason, in case of important prolapses, Giamundo recently introduced the HeLPexx procedure.
Accounting for the results previously described, we can see that in the few trials that report information regarding the same issue there appears to be a pattern between most of the trials. The results from the trials are consensual in terms of the reduced mean time of surgery, which, when taking into account the direct approach to the intended arteries, may direct to possible advantages of this procedure over more traditional techniques.
By analyzing the “bleeding” and “pain” parameters, one can see that the data is somewhat concordant, revealing a tendency of producing low number of symptoms, albeit the small differences in follow-up and the procedure itself within the trials. This could contribute to a good patient response regarding the treatment. When comparing the response to the treatment in terms of early post-operative pain, for the few trials which reported data the same way, the results were consistent, reporting mean values which could translate to a better patient response. However, these symptoms may not derive from the procedure itself but from non-resolved hemorrhoidal issues, though the symptoms and the non-complete resolution of symptoms being both sporadic.
When comparing with the literature on the Milligan-Morgan procedure, the trials that we described seemed to have an overall shorter operative time (27–29), shorter times until discharge (29, 30), lower rates of post-operative pain related complaints (31), higher symptom control rates (32) and lower rates of major complication (our papers reported no major complications) (33).
However, the same literature reported lower bleeding related complaints (30) and lower recurrence at 1 year follow-up (31, 33) for the Milligan-Morgan procedure. This information should be confirmed with posterior investigation with comparative trials between these two techniques.
The fact that the studies which did not use the doppler assisted technique had higher times until discharge is something of interest and could potentially be something worth looking to in future research.
In short, all of the trials concur that the laser, partly because it's a minimally invasive technique, can only bring benefits in terms of resolution of symptoms and absence of major complications.
Limitations
One of the major limitations that we found within our analysis of the different papers was the difference of reported outcomes and the uncategorized nature of the different comorbidities reported. In this review, the authors agreed to only report about bleeding and pain, as these were not only the main symptoms but also the only ones that were systematically reported through the different trials. This proved to be a limitation of our study, since many other symptoms could have gone unnoticed and escaped our analysis, biasing any conclusions made in this review.
The heterogeneity between studies where different papers presented the same variable with different units was another of our major limitations. For example, two different papers presented the results of bleeding after the laser procedure in different ways comparing with the remaining articles: Giamundo et al. 2018 (24) referred to the bleeding in the form of a “bleeding score” using VAS, on the other hand, Giamundo et al. 2010 (13) didn't mention the number of patients with bleeding immediately after laser procedure up to 1 month post-surgery, but only the number of patients with bleeding intraoperatively, invalidating the data collection and possible comparison with the others articles.
The comparison of the outcome variable pain was also difficult since the values of early post-operative pain using VAS in the different studies weren't obtained at the same time after the procedure and Ram et al. 2018 (15) and Maloku et al. 2014 (20) didn't present mean values of pain in VAS. The short follow-up at which these symptoms were evaluated may also contribute to biased results.
The unavailability of some articles found in our electronic search and the fact that no reference list research was preformed may also prove to be a limitation. Some relevant studies could have been missed and could enrich our systematic review. The publication bias may also have influenced our results.
Other potential bias sources could be the anaesthesia (general anesthesia is not needed although some articles mention the use of it, which could be impacting their results, especially when attaining to early post-operative pain values) and the fact that some papers considered patients with first- and fourth-degree haemorrhoids (could influence post-operative complications values). Treatment at grade IV is advisable only in fragile patients with major comorbidities to reduce bleeding, the HeLP alone does not correct prolapse. For this reason, the inclusion of patients with grade IV hemorrhoids may represent a bias in the analysis of complications and relapses.
Brusciano et al. show (34) that the postoperative pain score was extremely low, the presence of slightly signifcant peri-anal wounds, no special anal hygienic measures and low surgical time using HeLP. In this study, the 100% of their population came back to daily activity 2 days after surgery. At a mean follow-up period of 8.6 months, existed a recurrence rate of 0%. Thus, resulting in a negligible postoperative discomfort, HeLP could be considered a painless and minimal invasive technique in the treatment of hemorrhoids disease.
Conclusion
In summary, the laser haemorrhoidplasty procedure revealed a high therapeutic potential and a high beneficial impact on recuperation from the haemorrhoidplasty procedure, considering the reduced number of post-operative complications and comorbidities, the high symptom resolution and the reduced recurrence.
However, the limitations found within the studies must be taken into account and are the main reason that made impossible to proceed with a meta-analysis. Future high-quality investigations, with randomized studies are needed to compare HeLP technique with other dearterialization techniques in patients with Grade II and III haemorrhoids, obtaining better categorized results and complications, with a longer follow-up period.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Acknowledgments
We would like to thank Pedro Teixeira and Filipa Pinto-Ribeiro for the help with the trial analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Ganz RA. The evaluation and treatment of hemorrhoids: a guide for the gastroenterologist. Clin Gastroenterol Hepatol. (2013) 11(6):593–603. doi: 10.1016/j.cgh.2012.12.020
3. Jacobs D. Clinical practice. Hemorrhoids. N Engl J Med. (2014) 371(10):944–51. doi: 10.1056/NEJMcp1204188
5. Neves Jorge JM, Habr-Gama A, David BE, Steven WD, Tracy HL, et al. Anatomy and embryology of the colon, rectum, and anus. In: Beck DE, Wexner SD, Hull TL, editors. The ASCRS manual of colon and rectal surgery. 2nd ed. New York: Springer (2011). p. 1–22.
6. Sun Z, Migaly J. Review of hemorrhoid disease: presentation and management. Clin Colon Rectal Surg. (2016) 29(1):022–9. doi: 10.1055/s-0035-1568144
7. Lohsiriwat V. Treatment of hemorrhoids: a coloproctologist's view. World J Gastroenterol. (2015) 21(31):9245–52. doi: 10.3748/wjg.v21.i31.9245
8. Fox A, Tietze PH, Ramakrishnan K. Anorectal conditions: hemorrhoids. FP Essent. (2014) 419:11–9.24742083
9. Goligher J. Haemorrhoids or piles. In: Goligher JC, editors. Surgery of the anus rectum and colon. 4th ed. London: Bailliere Tindall (1980). p. 96.
10. Clinical Practice Committee AGA. American Gastroenterological association medical position statement: diagnosis and treatment of hemorrhoids. Gastroenterology. (2004) 126(5):1461–2. doi: 10.1053/j.gastro.2004.03.001
11. Yang HK. The pathology of hemorrhoids. In: Yang HK, editors. Hemorrhoids. Berlin Heidelberg: Springer-Verlag (2014). p. 15–24.
12. Yang HK, Yang HK. Anal anatomy. In: Yang HK, editors. Hemorrhoids. Berlin Heidelberg: Springer-Verlag (2014). p. 5–13.
13. Giamundo P, Cecchetti W, Esercizio L, Walter C, Luigi E, Giovanni F, et al. Doppler-guided hemorrhoidal laser procedure for the treatment of symptomatic hemorrhoids: experimental background and short-term clinical results of a new mini- invasive treatment. Surg Endosc. (2011) 25(5):1369–75. doi: 10.1007/s00464-010-1370-x
14. Giamundo P. Advantages and limits of hemorrhoidal dearterialization in the treatment of symptomatic hemorrhoids. World J Gastrointest Surg. (2016) 8(1):1–4. doi: 10.4240/wjgs.v8.i1.1
15. Ram E, Bachar GN, Goldes Y, Joubran S, Rath-Wolfson L. Modified Doppler-guided laser procedure for the treatment of second- and third-degree hemorrhoids. Laser Ther. (2018) 27(2):137–42. doi: 10.5978/islsm.18-or-14
16. Liberati A, Altman DG, Tetzlaff J, Devereaux PJ, Kleijnen J, Moher D, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62(10):e1–e34. doi: 10.1016/j.jclinepi.2009.06.006
17. Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6(6):e1000097. doi: 10.1371/journal.pmed.1000097
18. CASP. Critical appraisal skills programme (randomised controlled trial). Crit Apprais Ski Program. (2017) 4:1–4.
19. Giamundo P, Salfi R, Geraci M, Tibaldi L, Murru L, Valente M. The hemorrhoid laser procedure technique vs rubber band ligation: a randomized trial comparing 2 mini- invasive treatments for second- and third- degree hemorrhoids. Dis Colon Rectum. (2011) 54(6):693–8. doi: 10.1007/DCR.0b013e3182112d58
20. Maloku H, Gashi Z, Lazovic R, Islami H, Juniku-Shkololli A. Laser hemorrhoidoplasty procedure vs open surgical hemorrhoidectomy: a trial comparing 2 treatments for hemorrhoids of third and fourth degree. Acta Inform Medica. (2014) 22(6):365–7. doi: 10.5455/aim.2014.22.365-367
21. Naderan M, Shoar S, Nazari M, Elsayed A, Mahmoodzadeh H, Khorgami Z. A randomized controlled trial comparing laser intra-hemorrhoidal coagulation and milligan–morgan hemorrhoidectomy. J Investig Surg. (2017) 30(5):325–31. doi: 10.1080/08941939.2016.1248304
22. De Nardi P, Tamburini AM, Gazzetta PG, Lemma M, Pascariello A, Asteria CR. Hemorrhoid laser procedure for second- and third-degree hemorrhoids: results from a multicenter prospective study. Tech Coloproctol. (2016) 20(7):455–9. doi: 10.1007/s10151-016-1479-6
23. Crea N, Pata G, Lippa M, Chiesa D, Gregorini ME, Gandolfi P. Hemorrhoidal laser procedure: short- and long-term results from a prospective study. Am J Surg. (2014) 208(1):21–5. doi: 10.1016/j.amjsurg.2013.10.020
24. Giamundo P, Braini A, Calabro’ G, Crea N, De Nardi P, Fabiano F, et al. Doppler-guided hemorrhoidal dearterialization with laser (HeLP): a prospective analysis of data from a multicenter trial. Tech Coloproctol. (2018) 22(8):635–43. doi: 10.1007/s10151-018-1839-5
25. Salfi R. A new technique for ambulatory hemorrhoidal treatment: doppler-guided laser photocoagulation of hemorrhoidal arteries. Coloproctology. (2009) 31(2):99–103. doi: 10.1007/s00053-009-0009-7
26. Jahanshahi A, Mashhadizadeh E, Sarmast MH. Diode laser for treatment of symptomatic hemorrhoid: a short term clinical result of a mini invasive treatment, and one year follow up. Pol Przegl Chir. (2012) 84(7):329–32. doi: 10.2478/v10035-012-0055-7
27. Bakhtiar N, Moosa FA, Jaleel F, Qureshi NA, Jawaid M. Comparison of hemorrhoidectomy by ligasure with conventional milligan morgan’s hemorrhoidectomy. Pakistan J Med Sci. (2016) 5:1–5. doi: 10.12669/pjms.323.9976
28. Tjandra JJ, Chan MKY. Systematic review on the procedure for prolapse and hemorrhoids (stapled hemorrhoidopexy). Dis Colon Rectum. (2007) 50(6):878–92. doi: 10.1007/s10350-006-0852-3
29. Panarese A, Pironi D, Vendettuoli M, Arcieri S, Conversi A, Romani AM, et al. Stapled and conventional milligan-morgan haemorrhoidectomy: different solutions for different targets. Int J Colorectal Dis. (2012) 5:1–5. doi: 10.1007/s00384-011-1342-1
30. Shaikh AR, Dalwani AG, Soomro N. An evaluation of milligan-morgan and ferguson procedures for haemorrhoidectomy at Liaquat University Hospital Jamshoro, Hyderabad, Pakistan. Pakistan J Med Sci. (2012) 7:1–7. doi: 10.12669/pjms.291.2858
31. Towliat Kashani SM, Mehrvarz S, Mousavi Naeini SM, Erfanian R. Milligan-Morgan hemorrhoidectomy vs stapled hemorrhoidopexy. Trauma Mon. (2011) 3:1–3. doi: 10.5812/kowsar.22517464.3363
32. Lumb KJ, Colquhoun PHD, Malthaner R, Jayaraman S. Stapled versus conventional surgery for hemorrhoids. Cochrane Database Syst Rev. (2006) 54:9. doi: 10.1002/14651858.CD005393.pub2
33. Buntzen S, Christensen P, Khalid A, Ljungmann K, Lindholt J, Lundby L, et al. Diagnosis and treatment of hemorrhoids. Dan Med J. (2013) 60:B4754.
34. Brusciano L, Gambardella C, Terracciano G, Gualtieri G, di Visconte MS, Tolone S, et al. Postoperative discomfort and pain in the management of hemorrhoidal disease: laser hemorrhoidoplasty, a minimal invasive treatment of symptomatic hemorrhoids. Updates Surg. (2020) 72(3):851–7. doi: 10.1007/s13304-01900694-5
Keywords: haemorrhoids, diode laser, haemorrhoidectomy, haemorrhoidplasty, HeLP
Citation: Torrinha G, Gonçalves T, Sousa M, Högemann G, Goulart A, Carvalho AF and Leão P (2022) The effects of laser procedure in symptomatic patients with haemorrhoids: A systematic review. Front. Surg. 9:1050515. doi: 10.3389/fsurg.2022.1050515
Received: 21 September 2022; Accepted: 10 November 2022;
Published: 12 December 2022.
Edited by:
Enrico Fiori, Sapienza University of Rome, ItalyReviewed by:
Emir Çapkınoğlu, Acıbadem University, TurkeyRossella Palma, Sapienza University of Rome, Italy
Marco Bononi, Sapienza University of Rome, Italy
© 2022 Torrinha, Gonçalves, Sousa, Högemann, Goulart, Carvalho and Leão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gonçalo Torrinha Z29uY2Fsb3RlaXhlaXJhYWx2ZXNAZ21haWwuY29t
†These authors share first authorship
Specialty section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery