 Ahmet Furkan Sarıkaya1*
Ahmet Furkan Sarıkaya1* Kayhan Tarım1Ersin Köseoğlu1Arif Özkan1İbrahim Can Aykanat1
Kayhan Tarım1Ersin Köseoğlu1Arif Özkan1İbrahim Can Aykanat1 Baris Esen1Umut Can Karaarslan1Mustafa Müdüroğlu1Şevval Kanlı1Murat Can Kiremit1Yakup Kordan1Mevlana Derya Balbay1
Baris Esen1Umut Can Karaarslan1Mustafa Müdüroğlu1Şevval Kanlı1Murat Can Kiremit1Yakup Kordan1Mevlana Derya Balbay1 Tarık Esen1Serdar Aydın2,3Abdullah Erdem Canda1,4
Tarık Esen1Serdar Aydın2,3Abdullah Erdem Canda1,4
- 1Department of Urology, Koç University, Istanbul, Türkiye
- 2Department of Obstetrics and Gynecology, Koç University, Istanbul, Türkiye
- 3Research Center for Translational Medicine, Koç University, Sarıyer, Türkiye
- 4RMK AIMES, Rahmi M. Koc Academy of Interventional Medicine, Education, and Simulation, Istanbul, Türkiye
Background: Traditional surgical training relies on a master-apprentice model, but limitations such as restricted working hours and evolving surgical techniques have led to the integration of simulation-based training. Three-dimensional (3D) printing has emerged as a valuable tool for enhancing surgical education, offering patient-specific anatomical models that improve skill acquisition. Additionally, personalized video feedback may further refine training outcomes. This study investigates the impact of 3D-printed renal models and video-based feedback on skill acquisition in robotic partial nephrectomy training.
Methods: Forty urology residents without prior robotic surgery experience participated in this study. After completing a standardized theoretical and simulation-based training program, they performed partial nephrectomy on 3D-printed kidney models. The participants were randomly assigned to two groups: one received personalized video feedback based on their recorded surgical performances, while the other proceeded without feedback. Their surgical performance was evaluated based on dissection time, renorrhaphy time, total console time, and the amount of healthy renal parenchyma removed. Statistical analysis was conducted to compare improvements between the groups and assess the impact of video feedback on skill development.
Results: Initial comparisons between junior and senior residents showed no significant differences in their first operations, demonstrating that e-learning and proficiency-based simulation training effectively equalized skill levels before transitioning to realistic 3D model-based training. This suggests that structured preparatory training with objective performance targets can enhance learning outcomes in surgical simulation. Additionally, 3D-printed models provide a significantly more cost-effective alternative to cadaveric and animal-based training, making high-quality surgical education more accessible and scalable. Residents who received video feedback demonstrated a greater percentage improvement in dissection time compared to the control group (46.63% vs. 23.62%, p = 0.043). The amount of healthy renal parenchyma removed significantly decreased in the video feedback group (p = 0.048), indicating improved surgical precision. No significant differences were observed in renorrhaphy times between the two groups, suggesting that video feedback primarily enhanced dissection skills.
Conclusion: The integration of 3D-printed anatomical models with personalized video feedback enhances skill acquisition in robotic partial nephrectomy training. Video feedback significantly improves surgical precision by reducing unnecessary parenchymal removal and accelerating dissection time. These findings support the use of patient-specific 3D models and targeted feedback as cost-effective and scalable strategies to optimize surgical education and shorten the learning curve for complex procedures.
1 Introduction
The traditional surgical education model has long been grounded in the master-apprentice relationship, yet modern educational approaches began emerging in the late 19th century. This model, largely based on the progressive responsibility system initiated by William Stewart Halsted at Johns Hopkins Hospital, has been a cornerstone in training surgeons for decades (1, 2). Nevertheless, evolving challenges have necessitated the development of new approaches in surgical education. Legal limitations on weekly working hours, an increasing bureaucratic burden, and the diversification of surgical techniques and equipment have all contributed to diminishing the effectiveness of traditional training methods.
In response, simulation technologies and three-dimensional (3D) printing have emerged as -innovative and ethical alternatives for acquiring surgical skills. Anatomical models created through 3D printing not only enhance surgical practice but also facilitate patient-specific surgical planning. While traditional training methods demand significant time and resources over the long term, simulation-based models and 3D printing technologies offer the potential to provide more efficient and cost-effective education. Furthermore, the integration of technologies such as virtual reality (VR) and augmented reality (AR) is expanding opportunities for hands-on training while creating a safer learning environment that minimizes errors.
Recent studies (3–7) have demonstrated that incorporating 3D printing technology into surgical education accelerates skill acquisition and improves understanding of complex anatomical structures. Individually customized models enable trainees to better appreciate patient-specific conditions and experience realistic surgical procedures. Additionally, training processes enhanced by personalized video feedback not only reduce surgical errors but also shorten the learning curve. By analyzing past performances to identify areas for improvement, this targeted approach further refines the training process.
This study aims to evaluate the impact of 3D printing technology on surgical education, examine the role of personalized video feedback in skill acquisition, and assess the integration of simulation-based training with traditional educational models across various surgical disciplines. The broader adoption of these innovative approaches may significantly enhance surgical training, ultimately contributing to the development of more competent and well-equipped surgeons.
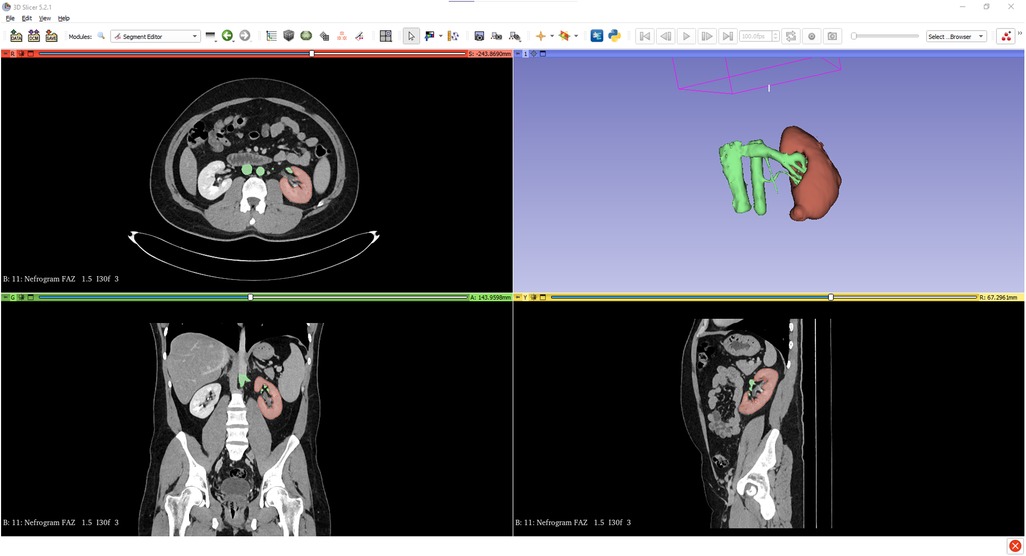
Figure 1. Segmentation images of the kidney tumor generated from CT scans using 3D Slicer software.
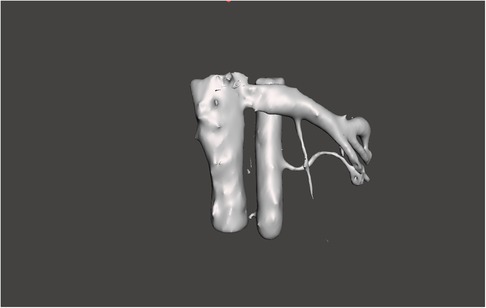
Figure 2. 3D reconstruction of segmented renal artery and vein, post-processed using Meshmixer software.
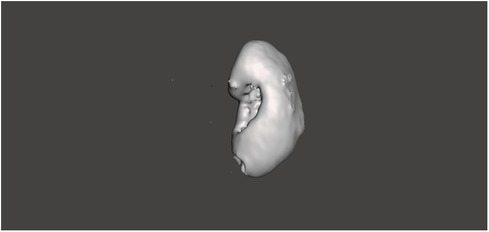
Figure 3. 3D model of the renal parenchyma (excluding tumor), segmented and refined using Meshmixer software.
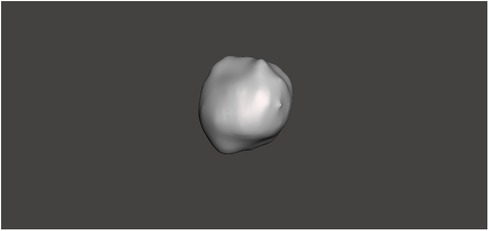
Figure 4. 3D model of the renal tumor, segmented and refined using Meshmixer software.
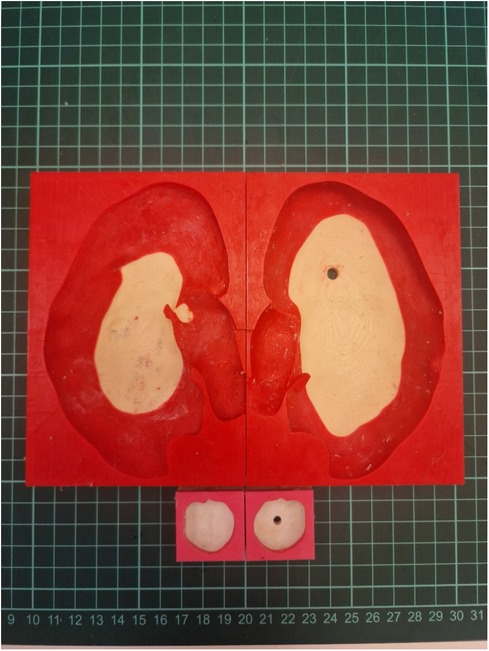
Figure 5. Negative molds and tumor components prepared for final model assembly.

Figure 6. Finalized 3D-printed kidney models prepared for surgical simulation.
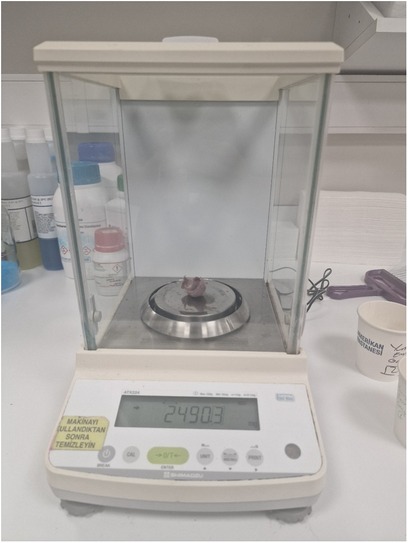
Figure 7. Measurement of resected healthy parenchyma using a precision laboratory scale.
2 Materials and methods
2.1 Study population and design
A total of 40 urology residents with no prior experience in robotic, open, or laparoscopic partial nephrectomy were invited from seven different centers to participate in this study.
Following successful completion of the European Basic Robotic Urological Skills (E-BRUS) theoretical course, developed by the European Association of Urology (EAU), participants proceeded to robotic simulation training in groups.
The simulation training incorporated the da Vinci Skills Simulator (dVSS; Intuitive Surgical, Sunnyvale, CA) with modules including Sea Spikes, Camera Targeting, and Needle Targeting (dV-Trainer, Mimic Technologies, Seattle, WA), as well as the Vertical Defect Suturing module (Simbionix, currently, both Mimic Technologies and Simbionix have been acquired by Surgical Science. An instructor guided each participant during the training sessions, continuing until proficiency was demonstrated in all simulator subsections. To ensure competency, participants were required to successfully complete each component of the assessment, including economy of motion and instrument collision evaluations.
After completing the structured training, participants were given additional time for unrestricted practice on the simulator, allowing them to practice freely without any time limitations.
Among the 40 participants, 20 residents were randomly selected to receive video-based feedback using recordings of their own surgical performances. The remaining 20 participants did not receive any feedback. Randomization was performed according to the order of arrival. One participant was unable to complete the final stage of the training and was therefore excluded from the study.
The primary parameters evaluated in this study included:
• Dissection time of the renal mass
• Repair time of the renal parenchyma defect (renorraphy)
• Total console time
• Amount of healthy renal parenchyma remaining following tumor excision from the removed specimen
Additionally, the duration of residency experience for each participant was recorded and analyzed.
The video feedback group included 11 junior and 9 senior residents, while the control group included 8 junior and 11 senior residents. Fisher's exact test indicated no statistically significant difference between the groups in baseline residency level (p = 0.527), confirming that they were comparable at baseline.
2.2 Material preparation
A renal mass with a low level of robotic surgical removal difficulty (low complexity) according to the R.E.N.A.L. Nephrometry Score (score 4a), was initially selected for this study (8). DICOM images of the renal mass were acquired and transferred to the 3D Slicer software. At this stage, segmentation, the process of defining the boundaries of the organs, was completed. For example, the mass and vascular structure in the lower pole were clearly delineated in the relevant sections.
Subsequently, the data were prepared for the negative printing technique using TinkerCad software. This technique involves injecting a prepared solution into a mold and then removing the solidified material from the mold, allowing for the mass production of identical models. Studies suggest that this method is the most effective approach currently available for producing tissue-like materials with realistic properties (9). Utilizing this injection molding method, a total of 80 identical models were produced. Molds were designed using TinkerCad and then fabricated with a Bambulab P1P model 3D printer.
For model construction, RTV (Room Temperature Vulcanizing) silicone was used with varying hardness levels. RTV type 10 Shore silicone, mixed with a silicone thinning agent, was used for the renal parenchyma, while RTV type 20 Shore silicone was used for the renal mass. A third mold facilitated the integration of the renal parenchyma and mass. During the curing process of the renal parenchyma molds, tissue representing the renal pelvis was incorporated. Polylactic Acid (PLA) filaments were used to create these molds, while PolyVinyl Alcohol (PVA) filaments were selected for the renal pelvis, offering the necessary flexibility.
All software utilized in this process was free and, where possible, open-source, significantly reducing costs by eliminating software licensing fees. Two models were produced for each participant, ensuring ample opportunity for hands-on practice.
Optional hilar structures, including the renal artery, renal vein, and ureter, could be added to the models based on 3D Slicer drawings. The inclusion of these structures incurred an additional cost of $0.50 to $2.00, depending on the materials used. During the production process, custom colors were applied to each structure using specialized paints, with an approximate paint cost of $0.056 per model.
The total production cost of a single kidney model was $2.06, with an additional electricity cost of $0.077, bringing the total cost to $2.14 per model. The initial cost of the molds was $4.63, and the PLA filament required for one-time mold production cost approximately $4.45. Over the course of the study, 80 models were produced, and participants had the option to request additional models if needed. Two participants utilized this option and received extra models during the study.
2.3 Operations and video feedback
The participants attended the first phase of the study at RMK Academy of Interventional Medicine, Education, and Simulation (RMK AIMES), where they observed a partial nephrectomy procedure performed by an experienced surgeon (AEC). Following this observation, they conducted a partial nephrectomy themselves using the Intuitive Da Vinci X model robotic system. The setup included one camera and robotic arms, operating within an abdomen model prepared using 3D printing technology.
All procedures were recorded using the Stryker InSITE Centre system. These recordings were later evaluated by a single experienced robotic surgeon (AEC) to ensure consistency in assessment. The primary focus of the evaluation was the tumor enucleation step during renal mass excision, where participants were encouraged to follow a true enucleation plane. In addition, technical deficiencies observed during renorrhaphy—such as improper needle angulation or failure to achieve the correct clip placement angle—were also identified. Personalized video feedback was created using these observations. Instructional annotations and verbal comments were added to each participant's surgical recording, emphasizing areas for improvement and reinforcing correct techniques. When participants returned to RMK AIMES within two weeks, the experimental group was shown their individualized feedback videos prior to the second attempt. The control group did not receive any feedback.
The video feedback provided to the experimental group included targeted instructional messages, such as:
• Guiding enucleation attempts when enucleation was required.
• Adjusting needle grip position, offering specific guidance on achieving the most accurate positioning.
• Confirming correct positioning, reinforcing positive behaviors.
• Providing optimal angles for ML sized (544,230) hem-o-lok clip (Teleflex Medical, Westmeath, Ireland) placement during renorrhaphy.
The primary outcome measures included:
• Dissection time
• Renorrhaphy time
• Total console time
• Amount of healthy parenchyma removed along with tumors
These parameters were compared between participants who received video feedback and those who did not.
To account for the varying stages of residency training among participants, the study initially evaluated the first operation parameters. This approach aimed to ensure that the pre-study training on 3D models placed all participants under comparable conditions before further evaluation.
During the study, a stopwatch was used to precisely measure the duration of each operational step. After each procedure, the tumoral formation was isolated from the excised mass, and the tissue representing the healthy parenchyma was weighed using the Shimadzu ATX224 precision balance (precision: 0.1 mg). This method enabled an accurate assessment of the effectiveness of nephron-sparing surgery performed by each participant.
2.4 Statistical analysis
SPSS version 28.0.0.0 (IBM, Chicago, USA) was used for statistical analysis. All numerical parameters were tested for normality using appropriate statistical methods. Comparisons between groups were performed using either the Mann–Whitney U test or the Student's t-test, depending on the distribution of the data. A p-value < 0.05 was considered statistically significant.
3 Results
Table 1 compares the first operations of junior and senior residents on 3D models after theoretical and simulation training. Since residency duration in Turkish urology programs is five years, participants were categorized as junior (<2.5 years of training) or senior (>2.5 years of training).

Table 1. Comparison of surgical performance parameters between junior and senior residents in their first operation on 3D kidney models after theoretical and simulation-based training.
The results analyzed in Table 1 are important because they show that simulation training with success condition after theoretical training eliminates the importance of the training time between the residents. These results showed us that having the success rates of the preparatory training to be done before the training to be done on 3D models can provide more accurate results. Here, there was no difference between the two groups in the first operations performed, which gives us a better starting point to examine the contribution of video feedback.
Table 2 compares the operative data of residents in the video feedback group and the control group.
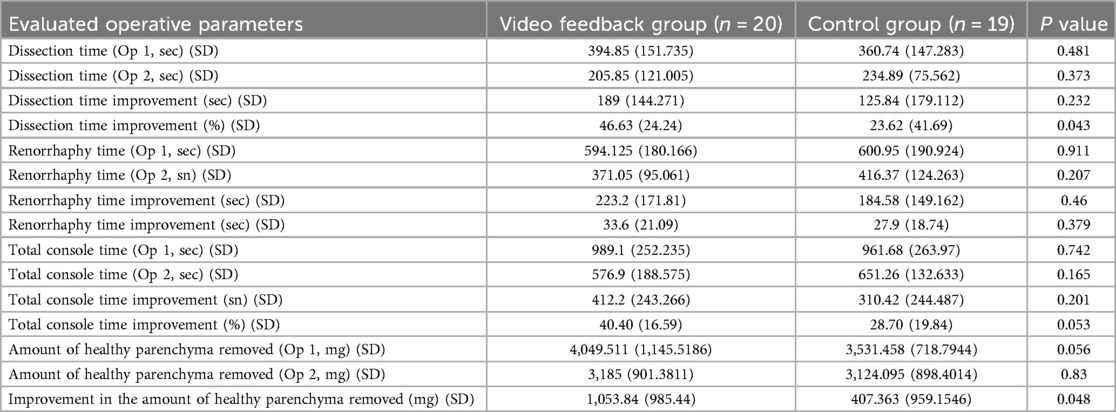
Table 2. Comparison of surgical performance parameters between the video feedback group and the control group, including changes between the first and second operations on 3D kidney models.
In Table 2, the contribution of video feedback to training was analyzed. A statistically significant improvement was seen in the renal mass dissection time when examined in percentage of those who received a personalized video feedback during the surgical training process. This improvement did not reach statistical significance when analyzed in seconds, but when the pattern was carefully examined, improvement was also evident here. Again, during tumor removal, healthy parenchymal tissue, which was inadvertently removed, also showed a significant improvement after video feedback.
4 Discussion
The use of three-dimensional (3D) materials in medical education, particularly in anatomy training, has been extensively studied. Numerous studies have demonstrated that 3D models enhance anatomical understanding more effectively than traditional methods (3). Melnyk et al. further emphasized that 3D models provide more detailed information in a shorter time with reduced cognitive effort compared to CT scans (4). Beyond anatomy education, the application of 3D materials in surgical training is increasingly gaining attention, highlighting the importance of the properties of the 3D models used.
Conventional 3D printers primarily produce rigid materials, which, while adequate for anatomical education, may be less effective for surgical skill development. To address this limitation, our study employed silicone casting techniques using molds created via 3D printing. This method ensured that all training models were identical, providing a standardized platform for skill acquisition among participants.
The experience level of participants may also influence surgical performance. Since residency duration in Turkish urology programs is five years, participants were categorized as junior (<2.5 years of training) or senior (>2.5 years of training). Table 1 presents the procedural outcomes from the first attempt, showing no statistically significant differences between the two groups. This finding indicates that the e-learning module and proficiency-based simulation training provided at the beginning of the study effectively equalized the preparation level of participants, ensuring comparable performance regardless of residency duration.
Furthermore, the structured nature of the proficiency-based progression model used in this study may have contributed to the comparable baseline performance observed across participants. Unlike time-based simulation, where duration of exposure is fixed, our model required residents to demonstrate competency in each technical parameter before progressing (10). This ensured that all participants entered the surgical phase with a uniform minimum skill level. Such a competency-based approach is known to reduce inter-participant variability and create a more equitable training platform, particularly beneficial in studies comparing educational interventions such as video feedback (11–13).
Notably, the only critical error observed—tumor incision during dissection—occurred in a single participant. This outcome underscores the value of structured theoretical and simulation training as a reliable foundation for hands-on practice with 3D models.
As shown in Table 2, while the reduction in procedural time was not statistically significant, the observed trends remain clinically relevant. Analysis of operative duration and the amount of renal parenchyma excised demonstrated a significant reduction following video feedback. However, the lack of statistical significance may be due to the limited sample size. Per-participant analysis revealed statistically significant differences (p = 0.043), suggesting that video feedback contributes to improved surgical precision, particularly in enucleation attempts. In the initial procedures, many participants performed a combination of enucleation and resection (enucleoresection). Following video feedback, which emphasized adherence to true enucleation planes, a greater number of participants performed pure enucleation during the second procedures. This shift may account for the observed improvement in surgical precision. Our findings are consistent with Piramide et al., who reported that 3D models enhance enucleation efforts (14).
A comparison of renorrhaphy times indicated a trend toward improvement with video feedback, although the differences did not reach statistical significance. The impact of feedback was more pronounced in dissection times than in suturing times, likely reflecting the nature of surgical learning. Dissection involves learning new techniques and eliminating fundamental errors, whereas renorrhaphy primarily focuses on improving speed in an already familiar skill. This aligns with the principles of proficiency-based progression, a well-established approach in surgical education that has been shown to significantly reduce errors (12).
Our findings support this concept, demonstrating that video feedback is particularly beneficial for refining dissection techniques. Although improvements in surgical times were not always statistically significant, they highlight the potential benefits of integrating 3D models into training programs. This suggests that personalized training strategies may enhance skill acquisition more efficiently and cost-effectively.
Another key finding was that participants receiving video feedback removed significantly less healthy renal parenchyma than those without feedback (p = 0.048). This result correlates with the reduction in dissection time, suggesting that early feedback facilitates a more accurate understanding of the surgical plane. In complex procedures such as partial nephrectomy, unnecessary parenchymal removal often results from an inability to correctly identify dissection planes. Although limited to a single intervention, the observed improvements in dissection precision suggest that video feedback may facilitate a better understanding of the optimal surgical planes. Further studies are needed to confirm the durability and reproducibility of this effect.
Although limited research directly quantifies healthy renal tissue loss, prior studies have reported that using 3D models in partial nephrectomy reduces the frequency of collecting system entry, which aligns with our observations (14). Considering that robotic partial nephrectomy learning curves tend to plateau after approximately 150 cases (15), our findings suggest that case-specific training with 3D models may accelerate this learning curve.
The benefits of preoperative rehearsal using patient-specific models have been demonstrated in previous studies. For example, Ghazi et al. showed that patient-derived 3D models improved intraoperative outcomes in complex cases (16). This highlights the importance of model fidelity when designing patient-specific surgical simulations. When a 3D model is intended for preoperative rehearsal, meticulous attention to anatomical details is crucial to ensure an accurate and meaningful training experience. Additionally, suturable models capable of realistically simulating tissue handling during partial nephrectomy are highly beneficial.
Cost-effectiveness is another critical factor, as large-scale training programs require the production of multiple models. An ideal model should be rapidly producible, anatomically accurate, and affordable while closely mimicking real tissue characteristics.
To the best of our knowledge, this study presents the most cost-effective 3D-printed kidney model for surgical training (17–20), providing an accessible and scalable solution for enhancing surgical education and shortening the learning curve for complex procedures.
Our cost analysis revealed that our model offers a more economical alternative to commercially available options. By deriving models directly from DICOM data, we achieved high anatomical accuracy while maintaining cost efficiency. A notable advantage of our model is its rapid production timeline: within 12 h of a CT scan, the first training model can be fabricated, and within 24–48 h, sufficient models can be produced for an entire training cohort.
This capability enables case-specific surgical rehearsal, particularly for surgeons-in-training, and enhances patient education by allowing visualization of the planned procedure. Personalized training has been shown to improve skill acquisition and reduce surgical errors (21, 22).
Additionally, feedback-based training is a well-established method in surgical education (23, 24), and our findings suggest that its impact may be further amplified when integrated with advanced 3D models. Gallagher et al. demonstrated that proficiency-based progression yields significantly better results than traditional training methods (11, 25, 26). Our study supports this approach, indicating that the combination of 3D models and individualized feedback has the potential to enhance surgical education and optimize learning outcomes.
To the best of our knowledge, this is one of the largest studies evaluating the use of low-cost, anatomically accurate 3D-printed kidney models combined with video feedback in robotic partial nephrectomy training. Despite its promising results, one of the key limitations of the study is the inability to simulate intraoperative bleeding, which remains a challenge in current simulation technologies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Koç University Committee on Human Research, Istanbul, Türkiye (IRB Number: 2024.377.IRB2.161). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS: Visualization, Resources, Writing – original draft, Project administration, Formal analysis, Funding acquisition, Validation, Conceptualization, Writing – review & editing, Supervision, Data curation, Investigation, Software, Methodology. KT: Software, Writing – review & editing, Methodology. EK: Methodology, Writing – review & editing, Software. AÖ: Data curation, Writing – review & editing, Supervision. İA: Data curation, Writing – review & editing. BE: Methodology, Writing – review & editing. UK: Data curation, Writing – review & editing. MM: Data curation, Writing – review & editing. ŞK: Data curation, Writing – review & editing. MK: Writing – review & editing, Methodology, Supervision. YK: Methodology, Supervision, Writing – review & editing. MB: Supervision, Writing – review & editing, Methodology. TE: Writing – review & editing, Supervision, Methodology. SA: Conceptualization, Project administration, Methodology, Supervision, Writing – review & editing. AC: Project administration, Writing – review & editing, Methodology, Supervision, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor NL declared a past collaboration with the author AÖ.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. The author(s) confirm that generative AI tools were used solely for grammar correction and language refinement during manuscript preparation. All scientific content, study design, data analysis, and interpretations were entirely conceived, written, and verified by the authors.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2025.1615817/full#supplementary-material
References
1. Wu Y, Peters RM. International Practice in Cardiothoracic Surgery. Dordrecht: Springer Netherlands (1986).
2. Hutter MM, Kellogg KC, Ferguson CM, Abbott WM, Warshaw AL. The impact of the 80-hour resident workweek on surgical residents and attending surgeons. Ann Surg. (2006) 243(6):864–71. discussion 71–5. doi: 10.1097/01.sla.0000220042.48310.66
3. Ye Z, Dun A, Jiang H, Nie C, Zhao S, Wang T, et al. The role of 3D printed models in the teaching of human anatomy: a systematic review and meta-analysis. BMC Med Educ. (2020) 20(1):335. doi: 10.1186/s12909-020-02242-x
4. Melnyk R, Chen Y, Holler T, Schuler N, Saba P, Quarrier S, et al. Utilizing head-mounted eye trackers to analyze patterns and decision-making strategies of 3D virtual modelling platform (IRIS(™)) during preoperative planning for renal cancer surgeries. World J Urol. (2022) 40(3):651–8. doi: 10.1007/s00345-021-03906-z
5. Giehl-Brown E, Dennler S, Garcia SA, Seppelt D, Oehme F, Schweipert J, et al. 3D liver model-based surgical education improves preoperative decision-making and patient satisfaction-a randomized pilot trial. Surg Endosc. (2023) 37(6):4545–54. doi: 10.1007/s00464-023-09915-w
6. Jiang Y, Jiang H, Yang Z, Li Y. The current application of 3D printing simulator in surgical training. Front Med (Lausanne). (2024) 11:1443024. doi: 10.3389/fmed.2024.1443024
7. Yang J, Luo P, Wang Z, Shen J. Simulation training of laparoscopic pancreaticojejunostomy and stepwise training program on a 3D-printed model. Int J Surg. (2022) 107:106958. doi: 10.1016/j.ijsu.2022.106958
8. Scoll BJ, Uzzo RG, Chen DY, Boorjian SA, Kutikov A, Manley BJ, et al. Robot-assisted partial nephrectomy: a large single-institutional experience. Urology. (2010) 75(6):1328–34. doi: 10.1016/j.urology.2009.10.040
9. Wanderling C, Saxton A, Phan D, Sheppard L, Schuler N, Ghazi A. Recent advances in surgical simulation for resident education. Curr Urol Rep. (2023) 24(11):491–502. doi: 10.1007/s11934-023-01178-1
10. Atroshchenko GV, Navarra E, Valdis M, Sandoval E, Hashemi N, Cerny S, et al. Simulation-based assessment of robotic cardiac surgery skills: an international multicenter, cross-specialty trial. JTCVS Open. (2023) 16:619–27. doi: 10.1016/j.xjon.2023.10.029
11. Gallagher AG, De Groote R, Paciotti M, Mottrie A. Proficiency-based progression training: a scientific approach to learning surgical skills. Eur Urol. (2022) 81(4):394–5. doi: 10.1016/j.eururo.2022.01.004
12. Mazzone E, Puliatti S, Amato M, Bunting B, Rocco B, Montorsi F, et al. A systematic review and meta-analysis on the impact of proficiency-based progression simulation training on performance outcomes. Ann Surg. (2021) 274(2):281–9. doi: 10.1097/SLA.0000000000004650
13. Gallagher AG, Hart M, Cleary D, Hamilton C, McGlinchey K, Kiely P, et al. Proficiency based progression simulation training significantly reduces utility strikes; a prospective, randomized and blinded study. PLoS One. (2020) 15(5):e0231979. doi: 10.1371/journal.pone.0231979
14. Piramide F, Kowalewski KF, Cacciamani G, Rivero Belenchon I, Taratkin M, Carbonara U, et al. Three-dimensional model-assisted minimally invasive partial nephrectomy: a systematic review with meta-analysis of comparative studies. Eur Urol Oncol. (2022) 5(6):640–50. doi: 10.1016/j.euo.2022.09.003
15. Larcher A, Muttin F, Peyronnet B, De Naeyer G, Khene ZE, Dell'Oglio P, et al. The learning curve for robot-assisted partial nephrectomy: impact of surgical experience on perioperative outcomes. Eur Urol. (2019) 75(2):253–6. doi: 10.1016/j.eururo.2018.08.042
16. Ghazi A, Melnyk R, Farooq S, Bell A, Holler T, Saba P, et al. Validity of a patient-specific percutaneous nephrolithotomy (PCNL) simulated surgical rehearsal platform: impact on patient and surgical outcomes. World J Urol. (2022) 40(3):627–37. doi: 10.1007/s00345-021-03766-7
17. Scott ER, Singh A, Quinn AM, Morano S, Karp A, Boyd K, et al. The use of individualized 3D-printed models on trainee and patient education, and surgical planning for robotic partial nephrectomies. J Robot Surg. (2023) 17(2):465–72. doi: 10.1007/s11701-022-01441-6
18. Yamazaki M, Takayama T, Fujisaki A, Kamimura T, Mashiko T, Fujimura T. Robot-assisted partial nephrectomy of initial cases using a 3D square-block type kidney model. Transl Androl Urol. (2020) 9(2):494–500. doi: 10.21037/tau.2019.12.31
19. Dwivedi DK, Chatzinoff Y, Zhang Y, Yuan Q, Fulkerson M, Chopra R, et al. Development of a patient-specific tumor mold using magnetic resonance imaging and 3-dimensional printing technology for targeted tissue procurement and radiomics analysis of renal masses. Urology. (2018) 112:209–14. doi: 10.1016/j.urology.2017.08.056
20. Claflin J, Waits SA. Three dimensionally printed interactive training model for kidney transplantation. J Surg Educ. (2020) 77(5):1013–7. doi: 10.1016/j.jsurg.2020.03.012
21. Hu X, Wang Y, Li J, Qing P, Yang X, Zeng J, et al. Three-dimensional multimodality image reconstruction as teaching tool for case-based learning among medical postgraduates: a focus on primary pelvic bone tumour education. BMC Med Educ. (2023) 23(1):944. doi: 10.1186/s12909-023-04916-8
22. Toale C, O'Byrne A, Morris M, Kavanagh DO. Characterizing individual trainee learning curves in surgical training: challenges and opportunities. Surgeon. (2023) 21(5):285–8. doi: 10.1016/j.surge.2022.11.003
23. El Boghdady M, Alijani A. Feedback in surgical education. Surgeon. (2017) 15(2):98–103. doi: 10.1016/j.surge.2016.06.006
24. Trehan A, Barnett-Vanes A, Carty MJ, McCulloch P, Maruthappu M. The impact of feedback of intraoperative technical performance in surgery: a systematic review. BMJ Open. (2015) 5(6):e006759. doi: 10.1136/bmjopen-2014-006759
25. Mottrie A, Mazzone E, Wiklund P, Graefen M, Collins JW, De Groote R, et al. Objective assessment of intraoperative skills for robot-assisted radical prostatectomy (RARP): results from the ERUS scientific and educational working groups metrics initiative. BJU Int. (2021) 128(1):103–11. doi: 10.1111/bju.15311
Keywords: robotic partial nephrectomy, 3D-printed kidney models, video feedback, surgical simulation training, urology resident education
Citation: Sarıkaya AF, Tarım K, Köseoğlu E, Özkan A, Aykanat İC, Esen B, Karaarslan UC, Müdüroğlu M, Kanlı Ş, Kiremit MC, Kordan Y, Balbay MD, Esen T, Aydın S and Canda AE (2025) The contribution of personalized video feedback to robotic partial nephrectomy training in realistic 3D tumor kidney models: design, production and implementation. Front. Surg. 12:1615817. doi: 10.3389/fsurg.2025.1615817
Received: 21 April 2025; Accepted: 30 June 2025;
Published: 17 July 2025.
Edited by:
Nikolaos Liakos, University of Freiburg Medical Center, GermanyReviewed by:
Mun Su Chung, Davos Hospital, Republic of KoreaMartin W. W. Janssen, University Hospital Münster, Germany
Copyright: © 2025 Sarıkaya, Tarım, Köseoğlu, Özkan, Aykanat, Esen, Karaarslan, Müdüroğlu, Kanlı, Kiremit, Kordan, Balbay, Esen, Aydın and Canda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmet Furkan Sarıkaya, YWhtZXRmc0Bob3RtYWlsLmNvbQ==