 Glória Jaime
Glória Jaime Alexandre Hobeika
Alexandre Hobeika Muriel Figuié
Muriel Figuié- 1CIRAD, UMR MoISA, Montpellier, France
- 2MoISA, Univ Montpellier, CIRAD, CIHEAM-IAMM, INRAE, Institut Agro, IRD, Montpellier, France
- 3Eduardo Mondlane University, Maputo, Mozambique
Background: Access to veterinary drugs for livestock has become a major issue over the last decade. Analysis has tended to focus on the demand for these products, while studies looking at the drivers behind their use generally focus on farmer behavior and interactions between veterinarians and farmers. However, the use of drugs also depends on structural factors that determine the functioning of the drug supply chain and farmers' access to the drugs. This article presents an overview of the factors that limit access to veterinary drugs in sub-Saharan Africa (SSA) as well as the international policy tools and arrangements that claim to improve it.
Methods: We have conducted a scoping review of the scientific and grey literature as well as the publicly-available data from both the animal health industry and international organizations. We aimed to gather information on the veterinary drugs market in SSA as well as on the international norms, recommendations, guidelines, and initiatives that impact SSA farmers' access to these drugs.
Findings: We highlight numerous barriers to veterinary drug access in SSA. The SSA market is highly dependent on imports, yet the region attracts little attention from the international companies capable of exporting to it. It suffers from a high level of fragmentation and weak distribution infrastructures and services, and is driven by the multiplication of private non-professional actors playing a growing role in the veterinary drug supply chain. The distribution system is increasingly dualized, with on the one hand the public sector (supported by development organizations) supplying small scale farmers in rural areas, but with limited and irregular means; and on the other side a private sector largely unregulated which supplies commercial and industrial farming systems. Different innovations have been developed at the international and regional levels to try to reduce barriers, such as homogenizing national legislations, donations, and vaccine banks. Alongside decades-old inter-state cooperation, many new forms of public-private partnerships and other hybrid forums continue to emerge, signaling the private sector's increasing influence in global governance.
Conclusions: Policies on animal health would be bolstered by a better understanding of the drivers behind and the components of access to veterinary drugs in different regional and national contexts. Inequalities in drug access need to be addressed and a market-driven approach adopted in order to strengthen our understanding of what determines veterinary drug use at the farm level. Policies should balance the interests of the various stakeholders, being careful not to reinforce bias toward certain diseases deemed “interesting” and neglect others that could prove to be highly important for veterinary public health.
Introduction
Over the last 30 years, integrative approaches have been adopted in health policies, placing interdependencies on a global scale and between species at the forefront with the Global Health and One Health paradigms. Global, cross-species interdependency has been pushed to the forefront of discussions through Global Health and One Health paradigms. This approach has been justified by the increasing prominence of emerging infectious disease risks, such as HIV/AIDS, Ebola virus disease, antimicrobial resistance (AMR), and Covid-19. Most of these risks emerged in developing countries due to increasing contact with reservoirs of pathogens in animals as well as flawed health systems.
Access to drugs is a core component of any health system or policy. In the last few years, multilateral organizations have pushed for the reinforcement of regulation of the trade and use of drugs within the context of the struggle against AMR. These efforts have highlighted the importance of tailoring policies to national contexts if they are to be effective (1). However, although access to drugs has been the subject of many academic works dedicated to human health, in particular within the context of developing countries (2–6), the animal health sector has received much less attention. Recent attention given to AMR in international and national policy has led to an increase in animal health studies (7–9).
The aim of this paper is to provide an initial general picture of the issues related to drug access in the context of livestock farming in SSA. We focus on SSA because it is the poorest region in the world and thus demonstrates the most salient issues regarding access to drugs, and most SSA countries bear a heavy burden when it comes to the economic and health impacts of animal diseases (10). Secondly, SSA is large enough to provide examples of a wide range of national situations.
When it comes to understanding the drivers of consumption of veterinary medicines, previous studies have tended to emphasize the role of demand—that is the “final” consumers, whether farmers or veterinarians. These studies are mainly published in veterinary journals not directly concerned with publishing social science research. The conditions under which drugs can be accessed and the importance of supply have been overlooked. Pioneering work on these issues in the social sciences has focused on Western countries (11–14). In SSA, a few studies have adopted a market-driven approach to veterinary drugs: this is partly the case for Bardosh et al. (15) in Uganda, Bessell et al. (16) in Tanzania, Kingsley (17) in Nigeria, and (18, 19) in Kenya. Available data on the veterinary drug supply chain have described the world market of veterinary drugs (20, 21), the regulation of this market (22–24), and the processes of harmonization of technical specifications at an international level (22, 25, 26), but they are to a certain extent outdated and only include brief references to SSA.
In studies on SSA specifically, more attention has been given to veterinary infrastructures, and their role in delivering services to low-income farmers in view of agricultural development (27–33). Some elements on access to drugs can be found indirectly in works focusing on specific animal health issues (e.g., bovine trypanosomiasis, tick-borne diseases, Newcastle disease, etc.) or products (vaccines, trypanocidal drugs). These studies describe the uses and misuses of drugs by farmers and animal health workers as a consequence of their knowledge and perceptions of diseases and drugs. They provide information on farmers' perceptions and self-assessment of veterinary drug-dispensing services [see for example Somda et al. (34) for Gambia; Enahoro et al. (33) for Ghana and Tanzania; Machila et al. (35, 37) and Higham et al. (36) for Kenya; Moffo et al. (8) for Cameroon; Soudre et al. (38) for Burkina Faso]. Many of these studies highlight farmers' lack of knowledge, awareness, or compliance (39, 40). Less common are studies that attest to the farmer's essential and positive role in animal disease management (41).
This paper is a scoping review based on the academic literature and publicly available grey literature. We aim to underline the main challenges sub-Saharan countries face in providing equitable access to veterinary drugs. We adopt here the definition of veterinary drugs proposed by the FAO (42), which includes: “drugs, insecticides, vaccines and biological products, used or presented as suitable for use, to prevent, treat, control or eradicate animal pests or diseases, or to be given to animals to establish a veterinary diagnosis, or to restore, correct or modify organic functions.” In this paper, we focus on drugs used for livestock (excluding pets), and on modern drugs (excluding traditional or ethnoveterinary medicines). According to the WHO (43), drug access is defined by the availability of drugs, including issues of quantity, regularity, quality and diversity, and affordability (or economic accessibility).
We present the information we gathered according to a socio-economic framework of supply chains. We consider access to drugs as the result of activities carried out by various entities (public and private) from the conception of a product to its final use, including the issue of residues. These activities include research and development, production, distribution, prescription, and use of drugs. The stakeholders and activities involved can be referred to as the veterinary drugs supply chain, using a broad understanding of the notion of a supply chain, which also includes all of the actors that contribute indirectly to the organization and functioning of the circulation of drugs, from molecules to residues, through the drafting of norms, rules, and recommendations.
This approach makes it possible for us to highlight the variations and inequalities between and inside countries, and the structural factors that limit the choices available to low-income farmers while minimizing the role of individual attitudes and perceptions as social determinants of consumption patterns. It looks at supply as a driver of consumption, and at policies on access to drugs, and regulation of their use.
After describing how the material used for this study was selected (Section Materials and Methods), we present the main socio-economic barriers to drug access in SSA (section The Many Factors That Limit Access to Veterinary Drugs in SSA) before presenting an overview of the contemporary political arrangements that have emerged at the international and regional level (Section International and Regional Arrangements for Improving Access to Veterinary Drugs) as part of efforts to improve access to veterinary drugs in SSA.
Materials and Methods
Data were collected through a scoping review (44) of academic work and grey literature containing empirical material. The main objective was to map existing knowledge and to identify gaps in knowledge on veterinary drug access in SSA.
For the academic work, a scoping review was conducted using the scientific database Web of Science. The search terms used to identify publications were: [(drug* OR medicin* OR pharma* OR access) AND (veterinary* OR animal OR zoo* OR husbandry OR livestock OR poultry OR sheep OR goat OR pork OR cattle) AND (trade OR use OR delivery OR service*) AND Africa AND (health OR disease OR epidemic OR epizoo*) NOT ethno]. These terms were searched in the topic (= title, abstract key word) and for the publication period 1975 to 2021, in all types of documents. From the 1,076 documents pre-selected, a first screening based on title and abstract and a second one based on the full texts, and 46 relevant documents were finally selected.
For the grey literature, we looked at the websites of different organizations involved in animal health in SSA and in some cases contacted them directly. This included the World Organization for Animal Health (OIE), Food and Agriculture Organization of the United Nations (FAO), AU-IBAR (the African Union – Interafrican Bureau for Animal Resources), ILRI (International Livestock Research Institute), World Trade Organization (WTO) as well as the Veterinary International Committee for Harmonization (VICH), GALVmed (The Global Alliance for Livestock Veterinary Medicines), HealthforAnimals (a non-profit, non-governmental organization representing companies and trade associations from developed and developing countries), pharmaceutical companies (Elanco Animal Health, Virbac, Zoetis, and MSD), and market research companies (Vetnosis, Mordor intelligence, Transparency market, Future Market insights). We collected data and technical reports describing the international veterinary drug market, veterinarian services, and drug distribution and use in SSA. Our material also includes recommendations, guidelines, norms, directives, and agreements related to veterinary drugs.
Results and Discussion
We present and summarize here results concerning factors that limit access to veterinary drugs (understood in terms of quantity, diversity, adequacy, physical or geographic accessibility, affordability) by using a general framework of supply chains: overall market size, production, trade, and consumption. Subsequently, we present the contemporary repertoire of policy tools used to overcome these barriers.
The Many Factors That Limit Access to Veterinary Drugs in SSA
What little information there is on the veterinary drugs market in SSA is difficult to access. Market information is not freely or wholly shared by the economic actors involved; information transmitted by national bodies to international organizations such as the OIE is not always publicly accessible, e.g., the OIE reports assessing the performance of the national veterinary services (PVS) or the veterinary legislation (VLSP). Moreover, any statistics that are publicly available are likely to only partly document the circulation of veterinary drugs, due to the market share held by informal products. “Illegal drugs” represent 20–30% of the market, according to HealthforAnimals (45). Additionally, the categories used to describe this market vary according to the source. These variations relate to the types of drug (insecticides, vaccines, biologicals, pharmaceuticals, feed additives), types of animals (pets, farmed animals), and geographic groups.
Nevertheless, these sources give an overall picture of the veterinary drug market in SSA: a small share of the world market, indicators of low use in some production systems, a limited local production of drugs (exemplified by the vaccines sector), weak distribution infrastructures and services, a lack of professionalization in the supply chains, and serious quality issues.
Production and Imports
The production of veterinary drugs is limited in SSA. Only a few countries have private drug manufacturers (mainly tertiary manufacturers), such as Bupo Animal Health (formerly Bedson) in South Africa and Cooper-K in Kenya, or the capacity to even partly supply neighboring countries. The production of veterinary drugs is often underpinned by public veterinary structures that focus on easy-to-produce generic medicines to support veterinary public health activities for small-scale farmers through vaccination campaigns or parasite control.
Regarding the specific case of vaccines (see Figure 1), the information provided by the OIE Wahis database1 for 19 countries in SSA suggests 500 million doses a year were produced in the region during the 2014–2018 period, covering around 20 different types of vaccines. Ethiopia represents a third of this production, the vast majority of which was vaccines for poultry. The most widely produced vaccines were for Newcastle disease and anthrax (produced in 14 of the 19 countries where data is available), followed by the vaccine against Peste des Petits Ruminants (PPR) produced in 9 of the considered countries. Production mainly responds to national needs. Few countries have the capacity to export: the most salient exception is Botswana, a country that exports around 80% of its production and represents 43% of all recorded exports in SSA. Regional cooperation exists, such as the Pan-African Veterinary Center of the African Union (AU-PANVAC) in Ethiopia, which produces biological reagents for animal disease diagnosis and also provides independent quality control of veterinary vaccines.
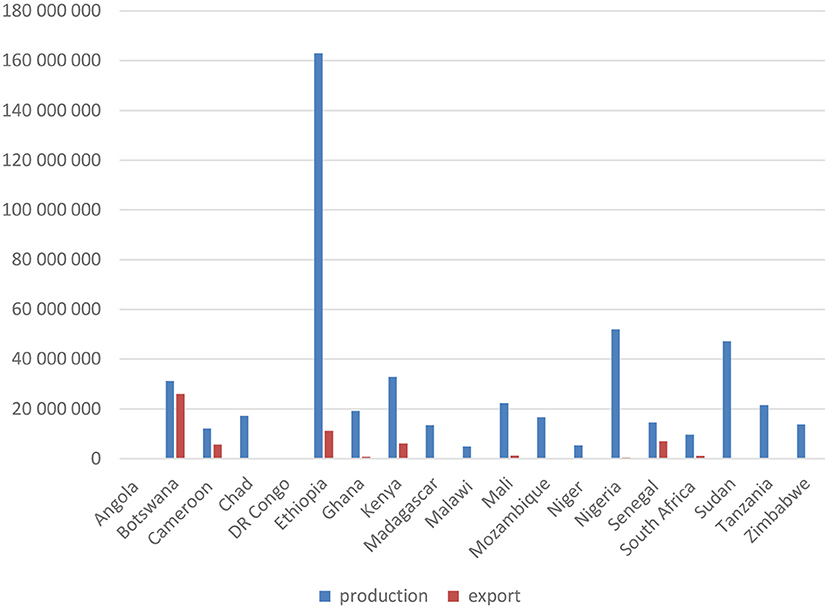
Figure 1. Production and export of vaccines for animals in sub-Saharan African countries (based on OIE Wahis database, average number of doses for 2014–2018).
The veterinary drugs market in SSA is dependent on imports from Europe, the US, Brazil, and, increasingly, China and India, with a complex organization between primary, secondary, and tertiary manufacturers and export and re-export processes that still need to be clarified by further research. Most of these products are imported by national distributors. Among the larger pharmaceutical companies, only a few have established branch offices in SSA, according to their annual reports and websites. Elanco Animal Health, Virbac, Zoetis, and MSD Animal Health have all established branch offices (subsidiaries) in South Africa. The Elanco Animal Health group, which acquired Boehringer Ingelheim's veterinary branch in 2016 and Bayer's in 2019, has the most extensive presence on the continent, with subsidiaries also in Angola, Kenya, Mozambique, Zambia, and Zimbabwe. The lack of harmonization in SSA national regulation, in particular when it comes to drug registration processes, contributes to a market fragmentation that discourages importation (46).
Weak Distribution Infrastructures and Services in the Public Sector
Infrastructure and services are necessary for the adequate distribution of drugs to their final users. Various papers underline how limited access to veterinary services is a major problem for livestock producers in sub-Saharan countries: see the issues of the OIE review dedicated to Veterinary institutions in the developing world: current status and future needs with a special focus on SSA countries in 2004 and the issue Good governance and financing of efficient veterinary services in 2012; as well as the recent review of Abakar et al. (32) on the status of veterinary services in the Sahel over the last 20 years. Other studies focus on a specific country or group of countries such as Kenya and Uganda (47–50), Tanzania (51), Central Africa (52), South Africa (53, 54), or Tanzania, Uganda, and Ethiopia (55).
In most countries in SSA, access to veterinary drugs was provided in the past by a centralized public sector inherited from the colonial period (31), managed by the veterinary profession and based on a populational approach to animal health (56). However, in the 1980s, under pressure from the World Bank, most developing countries adopted structural adjustment programs (SAPs) taking a market approach as the preferred means of providing services whilst at the same time reducing state expenditure. Impacts of the SAPs have been extensively analyzed and discussed in several international forums and publications in the decades following the reform, analyzing the consequences of the subsequent drastic shift of responsibility from the public to the private sector, including in the veterinary drug deliveries and veterinary services (30, 48, 52).
For example, Smith (52) indicates that the SAPs “imposed drastic reforms aimed at restructuring the public veterinary service and at privatization”; this process has been top-down and at times chaotic with no attempts made to find appropriate solutions for the diversity of production systems. Smith concludes that only a handful of countries and a small proportion of producers have benefited from this privatization. A successful example is that of cattle breeders in the Central African Republic, whose access to trypanocides (for the control of trypanosomiasis) was greatly improved. This success is attributed to the powerful cattle breeders' association determinant in driving the reform (52).
Veterinarians and para veterinarians2 are few and far between in SSA, see for example (57) in Ethiopia. Based on data from the OIE WAHIS database, we estimate that there are ~7.4 animal health professionals for every 100,000 inhabitants in SSA (made up of two veterinarians and 5.4 para-veterinarians). By comparison, there are on average 49 and 53 animal health professionals for every 100,000 inhabitants in the UK and US, respectively. Moreover, public services suffer from inadequate and unpredictable budgetary allocations and drug supply and have limited capacity to visit farmers. Their role as drug suppliers is restricted to the delivery of parasiticides and to vaccination, particularly during outbreaks. Rates of absenteeism are high and opportunities for career progress are limited. Some of these veterinarians work in parallel for private clinics, selling drugs and delivering therapeutic individual care for pets and farmed animals. This partly makes up for the absence of the private sector but also contributes to the blurring of lines between public and private services (27).
The performance of the veterinary authorities in regulating the circulation and use of veterinary drugs is also described as limited in many SSA countries, according to the PVS evaluation tool developed by the OIE. This tool includes a section on the technical authority and capability in relation to veterinary medicines and biologicals. Grading ranges from one (“The veterinary services cannot regulate veterinary medicines and biologicals”) to five (“The control systems for veterinary medicines and biologicals are regularly audited, tested and updated when necessary, including via an effective pharmacovigilance program”). In SSA, based on the currently available reports on the OIE website for 20 countries, two countries are graded level one (Guinea Bissau and Congo), 15 countries level two (Guinea, Ivory Coast, Benin, Mali, Mauritania, Namibia, Niger, RCA, Kenya, Seychelles, Rep of Sudan, South Africa, Togo, Chad, and Nigeria), two countries level three (Senegal and Swaziland), one country level four (Botswana), and none are graded level five.
This public sector weakness has a greater impact on low-income farmers, particularly in remote areas. It also limits the potential to face public health challenges requiring the intervention of public authorities, and regional or international coordination.
Challenges in the Development of Private Distribution of Veterinary Drugs
The number of public veterinary services has not been fully offset by the private sector, particularly with regards to the distribution of veterinary drugs in rural areas. These reductions have led to many failures in the supply of veterinary drugs and services (48, 49). Gehring et al. (58) indicate that in some villages in South Africa, the nearest accessible outlet for veterinary drugs was between 10 and 30 km. There is little incentive for private veterinarians and pharmacists to provide services in areas where the use of veterinary drugs per cattle head is low, purchasing power is limited, animals are widely dispersed, and transaction costs are high. Private veterinarians are more likely to commit to sectors where revenue is higher, such as the emerging market for pet health in cities or the burgeoning sector of intensive livestock farming in peri-urban areas (31, 52, 59, 60).
The privatization of veterinary services has contributed to the transformation of veterinary drugs and services from public goods to simple commodities. This privatization has an impact on drug availability: it favors the offer of drugs with high economic returns or those that respond to farmers' habits regardless of efficiency and adequacy. For example, Bardosh et al. (15) show that product availability in Uganda is dependent on what interests the animal health industry, which has led to higher sales in non-tsetse effective drugs.
Most studies on the provision of veterinary services conclude that there is a need for collaboration between the different stakeholders of veterinary services (public/private, donors) (32, 61), including farmers (41), as well as between human and animal health services (62, 63). More recently, to support veterinary drug delivery and services, new business models and institutional arrangements have emerged, such as cost recovery for public veterinary services, public/private partnerships, or contract farming. Experiences of contracted farming have been documented, for example, in the poultry and aquaculture sector in Burundi, Kenya, Rwanda, and Uganda (64).
The Multiplication of Non-professional Actors in Veterinary Drug Supply Chains
Gaps in delivery of veterinary services following the implementation of the SAPs have been partly filled by a variety of actors with basic knowledge or by other unqualified actors (65–69). Some studies, for example, that of Turkson (70) in Ghana, describe how shortages of practicing veterinarians see farmers taking the medication of their animals into their own hands.
Community animal health workers (CAHWs), sometimes referred to as the third sector (as opposed to the public or private sectors), have been trained to fill this gap, usually through the support of donors (49). They provide basic veterinary services to farmers in rural areas. Their formal knowledge consists of brief training from public veterinary services and NGOs (71). They are encouraged to develop a private veterinary drug supply system to finance their activities long term. Successful examples have been reported, for example in Kenya (18, 72). However, as public services, this CAHW-provided service also suffers from many constraints such as irregular supply, the low purchasing power of farmers, and transport difficulties (73, 74).
In various countries, the liberalization of veterinary drug distribution has also encouraged the emergence of alternative supply chains made up of a large number of middlemen (66, 69), mostly in peri-urban areas. In these areas, livestock farming is developing in conjunction with the increasing urban consumer demand for meat and a process of intensification supported by urban investors or by producer organizations (e.g., commercial poultry farmers' associations). The private markets for veterinary drugs have become concentrated in these areas. Private as well as public veterinarians (as part of a secondary activity) are involved in these private supply chains. Some of the individuals involved only have practical knowledge of drug use (e.g., commercial poultry farmers), while others do not have any knowledge at all but have capital they wish to invest in growing markets. Frequent failures observed in veterinary administration and regulation have left the private supply chains unregulated from imports to retail, and many drugs are sold without prescription. As a consequence, veterinary medicines can be found anywhere, anyhow (27). Gehring (75) describes a significant record of adverse reactions reported to the Veterinary pharmacovigilance center in South Africa due to inappropriate, extra-label uses of products by non-veterinarians.
Issues With Convenience and Quality of Available Drugs
The issue of veterinary drug accessibility also includes questions around convenience, suitability for local needs, and quality. As in the human health sector, (76), diseases endemic to Africa have received little attention from the pharmaceutical industry or research into disease epidemiology, which raises the issue of neglected animal diseases (77). The low level of training provided to CAHWs also limits both the convenience and diversity of available veterinary drugs. The role of CAHWs in delivering medicines is generally officially limited to drugs that represent the least potential for abuse, those with a broad-spectrum, and those that can be sold over the counter.
This lack of diversity, along with differences in price, may encourage the extra-label use of medicines, including use for other indications, methods of administration, species, age groups, and so on. This practice also includes the use of human medicines for animals, particularly when human medicines are more easily available and affordable, which can be the case when different countries adopt economic policies including low import taxes and grants aimed at improving access to human drugs. These uses give rise to inappropriate use of drugs, particularly in the absence of technical supervision and an effective regulatory framework. For example, veterinary services in Madagascar have reported injectable contraceptives intended for women (progestogens Confiance™, Pfizer), easily available at a low price, being used as an alternative for surgical castration of adult sows before culling (78). Misuse is also fostered by unsuitable packaging, for example, labels in foreign languages, or when small-scale farmers only have access to 1,000-dose packs Newcastle-disease vaccines, despite only having a relatively small number of animals.
Sub-standard and non-registered drugs are also an issue. The market for illegal drugs is estimated to be worth 400 million US dollars a year in SSA and North Africa and 1–2 billion US dollars worldwide (45, 79). Institutions for drug quality control are sorely lacking and only a few countries with significant production capacities (Botswana and Ethiopia) have properly equipped control laboratory facilities staffed by technically competent personnel, according to the aforementioned PVS tool. The lack of quality control and reliable certification of quality hinders farmers in their distinction between high- and low-quality drugs. Consequently, this deters sales of high-quality products, leading to an economic mechanism of adverse selection whereby bad products drive good products off the market (80).
Various issues with quality have been raised, from lower concentrations of active ingredients than that stated on labels to toxicity. According to a survey conducted in West Africa by the Interstate School of Veterinary Science and Medicine in Dakar and quoted by Le Minor (26), 67 and 69% of the veterinary drugs sampled in the formal and informal sectors, respectively, were of sub-standard quality. Of these sub-standard drugs, most were trypanocides and antibiotics (oxytetracycline). The sub-quality of trypanocides sold in SSA has been demonstrated by numerous studies. Bengaly et al. (81) provide an assessment of the quality of trypanocidal drugs sold in French-speaking countries in West Africa (Benin, Burkina Faso, Côte d'Ivoire, Mali, Niger, and Togo) in which “51.90% of the samples were non-compliant compared to the standards and were containing lower quantity [sic] of the active ingredient compared to the indications on the packaging.” Another study conducted by Tchamdja et al. (82) revealed a high proportion of trypanocides of sub-standard quality on the Togolese market (40%) and an even higher proportion (53.57%) for the sample collected from unofficial markets. The same problem is described by Tekle et al. (83) in Ethiopia, with 28% of trypanocidal drugs tested failing to comply with quality requirements. Vougat Ngom et al. (40) analyzed the quality of veterinary drugs sold in the Far North Region of Cameroon and concluded more positively that general quality was good, with concentrations often different but similar to that which is labeled and with no differences between vendors. Furthermore, they concluded that some differences in concentrations were likely the result of poor storage rather than intentional dilution and said the main problem in the region was poor compliance with recommended treatments among farmers.
At Farm Level: Low Availability and Affordability
Overall, the use of veterinary drugs in SSA is low. The global veterinary drug market has been described by Crosia (21) as globalized and dominated by less than ten American and European pharmaceutical firms. Recent analyses by market research firms have described the dynamic nature of the global veterinary pharmaceutical market thanks to a growing pet sector in Western countries and an increasing number of farmed animals in emerging Asian countries (84). SSA's contribution to this dynamic is difficult to calculate since data are scarce, but the omission of SSA in such market reports is also telling. Annual reports of the major companies and most market studies on veterinary pharmaceuticals do not refer to Africa or SSA or do so only indirectly through the category “rest of the word” (21, 85) or jointly within the category Middle East (84, 86). South Africa is the only country in SSA sometimes highlighted in market analysis (87). This indicates a lack of corporate interest in the SSA market. Other rare studies give an overview of the situation in specific countries in SSA: Messomo Ndjana (88) in his veterinary thesis on the distribution and quality of veterinary drugs in Cameroon; and Grasswitz et al. (20) in a report for UA-IBAR on the veterinary pharmaceutical industry in three sub-Saharan countries (Kenya, Uganda, and South Africa).
Depending on the source, the SSA market, along with other countries in North Africa and the Middle East, represents 1.7–7% of the global market (20, 21, 84). While there is a lack of recent data, past calculations have indicated that more than half of this market is concentrated in South Africa (20). These figures can be compared with the livestock population in SSA: according to FAO (10), SSA accounts for 14% of livestock worldwide (and North Africa and the Middle East represent 3.3%). Therefore, the average level of consumption of veterinary drugs per livestock unit in SSA can be estimated as between 12% (1.7/14) and 50% (7/14) of the world average use level.
Although the overall availability and diversity of veterinary drugs are low, significant differences exist between countries, farming systems, and animal species. A study conducted by GALVmed (unpublished, personal communication) based on a survey administered to local veterinarians in seven countries in SSA (Burkina Faso, Ghana, Kenya, Uganda, Nigeria, Senegal, Tanzania), documents the variations in farmer's access to drugs. Backyard poultry is the least “medicated” species in all countries studied. More than half of the backyard poultry farmers in Senegal, Uganda, Tanzania, and Kenya do not have any access to veterinary drugs. In the low-input small ruminant sector, veterinarians declared that half of the farmers did not have any access to drugs in Nigeria, and only had access to one type of drug (dewormers or antibiotics) in Burkina, Uganda, Tanzania, and Kenya. Access was assessed by veterinarians as very limited in Uganda and Tanzania, compared to Senegal, Burkina Faso, and Ghana. In Nigeria, the situation differs between species, with better access to treatments for small ruminants compared to those for poultry and cattle. The most accessible drugs were vaccines against Newcastle disease, antibiotics and anticoccidials for poultry, and antibiotics and vaccines against PPR for small ruminants (goats and sheep). In Tanzania, access is described as limited for the majority of farmers, however, a few cattle owners have access to a relatively large diversity of drugs (21 different drugs, which was the highest level of diversity reported by this survey for any species). Interestingly, in Uganda, antibiotics for backyard poultry are said to be more accessible than vaccines; and in the commercial sector, more than half of farmers only have access to antibiotics. Similarly, for small ruminants in Kenya, Uganda, and Tanzania, antibiotics were reported as being more accessible than vaccines.
Similarly, high variations in access and use between and within countries in SSA are shown in data focusing on antibiotics. The Fifth annual report on antimicrobial agents intended for use in animals edited by the OIE (89) indicates for 2017 an average consumption of 117.48 mg/kg of adjusted animal biomass for the 102 reporting countries, compared with an average of 30.35 mg/kg for the 24 reporting African countries (sub-Saharan and north-African countries). The specific case of Cameroon described by Mouiche et al. (90) shows large differences between species, from 213.32 mg/kg for poultry to 0.47 mg/kg for goats.
Finally, accessibility also depends on affordability. Most farmers in SSA have low purchasing power. According to the International Livestock Research Institute (91), poverty is widespread among livestock owners in SSA. Modern drugs are therefore less affordable for these farmers and the market opportunities are limited for supply chain stakeholders. Moreover, compared to emerging Asian countries engaged in what is commonly described as the “livestock revolution” (92), low-input farming systems remain predominant in SSA. For example, in 2011, SSA represented 2.1% of the world-intensive poultry production compared to 38% for China (and 46.8% for the whole East Asia and Pacific Region) (93). Low-input livestock production (including inputs such as veterinary drugs) is the main approach for farmers in pastoral areas who have limited and uncertain access to markets and cash and are exposed to external threats such as climate-related risks (94).
International and Regional Arrangements for Improving Access to Veterinary Drugs
Different international- and regional-level institutional arrangements have emerged over time to help SSA countries improve drug access and coordinate and harmonize actions. This can directly improve access to veterinary drugs, promote the regulatory policies of international organizations, and mobilize pharmaceutical firms. Veterinary drug supply chains are framed by arrangements that have been promoted and institutionalized by international organizations such as the World Organization for Animal Health (OIE), the Food and Agriculture Organization (FAO) of the United Nations (UN), the Codex Alimentarius and the Veterinary International Conference on Harmonization (VICH), and the World Trade Organization (WTO) Sanitary and Phytosanitary Measures (SPS) Agreement (22–24). Standards set by the VICH and Codex Alimentarius also provide countries with a set of norms with which to regulate production, marketing authorizations, trade, and use of veterinary drugs (22, 24). Bilateral and regional agreements also contribute in the form of donations and vaccine banks. Aside from inter-state cooperation, we note a rapid increase in initiatives where the private sector plays a central role, in particular pharmaceutical companies. However, these arrangements rarely include Research and Development and are mainly focused on trade and veterinary advice rather than on the production side.
We focus here on the arrangements implemented at the international level, within a framework of international cooperation in which animal health is considered a global public good. Important efforts are also carried out at the national level, including, for instance, price subsidies, taxes, flexibilities in the Agreement on Trade-Related Aspects of Intellectual Property (TRIPS). However, they go beyond the scope of this paper.
Slow Harmonization of Regional and National Regulations
As mentioned above, many countries in SSA have very weak regulatory systems. For example, in Mozambique, there is no legislation addressing veterinary drugs, whilst in Angola, it appears that veterinary drugs are only superficially mentioned in legislation that mainly focuses on human medicines (95, 96). Moreover, regulations that are in place are not always effective, and the heterogeneity between countries restricts the opportunity for a regional market. To combat weaknesses in many national regulations—their lack of effectiveness and their heterogeneity inside the SSA—diverse initiatives have been implemented at the international or regional level. We present here the main international organizations participating in the regulation of drug access in SSA, as well as recently developed regional initiatives.
The Main International Institutions Regulating Veterinary Drugs
The OIE, established in 1924, is a major actor in this domain. It institutionalizes the sanitary norms for the international trade of animals and animal products, which member countries can use to prevent the introduction of diseases and pathogens without creating unjustified sanitary barriers (24, 97). For example, the Sanitary Code for Terrestrial Animals formalizes guidelines for the prudent and responsible use of antimicrobials. It also promotes the development of professional veterinary capacities and the involvement of veterinary services in the creation of regulations.
As with other commodities, the international trade of veterinary drugs is subject to norms set by the WTO. Through the SPS agreement, which came into force in 1995, the WTO seeks to reduce state use of non-tariff barriers that could be deemed unjustified and protectionist (98). The Codex Alimentarius, a joint program of the FAO and WHO established in 1963, focuses on food safety. It develops norms concerning the maximum residue limits of veterinary drugs in food, and by this means regulates the use of drugs in farming worldwide, throughout the supply chain (99, 100).
The VICH, the International Cooperation on Harmonization of Technical Requirements for Registration of Veterinary Medicinal Products, brings together regulatory authorities and the pharmaceutical industry in setting internationally recognized norms for veterinary drug registration and marketing authorizations (22–24). Established in the mid-1990s by industrialized countries (the EU, US, Japan), and inspired by the ICH (the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use), it is currently expanding its scope to become more global by including Nigeria, Uganda, Tanzania, and Zimbabwe. It aims to achieve greater international harmonization of registration requirements for veterinary drugs, to ease their circulation, and support their access (101).
The Regional Harmonization Initiatives From WAEMU, SADC and EAC
The African Union, through the AU-IBAR, is leading the harmonization of veterinary laws and regulations across various regional communities in Africa. This process is combined with harmonization in the domain of human health. GALVmed plays an important role in supporting this process. GALVmed is a non-profit NGO, with charity status, set up in the early 2000s by the UK's Department for International Development (DFID) and funded by the Gates Foundation. GALVmed takes inspiration from GAVI, the Vaccine Alliance, which works in the human health sector. It has been working since 2011 to promote drug access for small-scale livestock farmers in SSA (102). In particular, GALVmed is supporting the initiative “Harmonization of Registration Requirements for Veterinary Immunologicals and Development of a Mutual Recognition Procedure in East Africa Community (EAC)” which is funded by the Gates Foundation (46).
Other examples of ongoing initiatives aimed at homogenizing market authorization processes and quality control are given by the centralized system set up by the West African Economic and Monetary Union (WAEMU) in 2007 with the support of ANSES (the French Agency for Food, Environmental and Occupational Health & Safety) (103), and also by the adoption of the “Regional Guidelines for the Regulation of Veterinary Drugs in the Southern Africa” in 2011 (104). Despite these numerous initiatives, the harmonization process is said to be slow due to problems including weak national regulatory systems, financial problems, lack of institutional capacity, and challenges related to human resources (96).
Donations and Vaccine Banks
Donations and vaccine banks also contribute directly to the availability of veterinary drugs in SSA. In the human health area, Various authors (105–109) described the three main situations in which governments, companies, and NGOs donate drugs: emergency aid, development programs, de-stocking of unsold and almost expired drugs. Donations can also contribute to the improvement of drug access through a transfer of technology. For example, from 2018 to early 2021, the FAO and the EU donated equipment needed for the production of thermo-tolerant vaccines against PPR in Ethiopia. This donation has boosted the national production capacity and supported the National PPR Eradication Campaign (110, 111).
Donations can also be used to protect the commercial interests of the country making the donation. A donation of foot-and-mouth disease (FMD) vaccines made by the government of Botswana to Zimbabwe in 2017 is a case in point. The country donated over 473,200 doses of vaccines manufactured by the Botswana Vaccine Institute (BVI) in order to help Zimbabwe control outbreaks of FMD at their shared border (112).
The OIE (113) defines vaccine banks in its Manual of Diagnostic Tests and Vaccines for Terrestrial Animals (chapter 1.1.10) as “antigen or vaccine reserves, which can be of different types”. These banks enable the rapid supply of emergency stocks of vaccines in case of outbreaks, and lower delivery costs for systematic mass vaccination campaigns (114). According to Lombard and Füssel (115) and the OIE (116), banks are supplied by vaccine producers selected through international tenders. The cost of vaccines and their transportation to the recipient countries are generally borne by donors. To date, the OIE has set up two vaccine banks: one for avian influenza, and one for the PPR.
The avian influenza bank created in 2006, and now closed, received financial support from the EU through the PACE program and delivered 62,017 million doses of vaccines to six countries in SSA: Mauritania, Senegal, Egypt, Mauritius, Ghana, and Togo (117). In 2013, the OIE created the PPR vaccine bank under the Vaccine Standards and Pilot Approach to PPR Control in Africa Project (VSPA) with funding from the Gates Foundation and the World Bank through the Regional Sahel Pastoralism Support Project (PRAPS) (118). The Botswana Vaccine Institute (BVI) was chosen, after an international call for tender, to supply the PPR vaccines and the corresponding quantities of vaccine diluent (118). Different access modalities were deployed: direct purchase by a country (Togo), purchased through donors, or as part of regional programs (Burkina Faso, Ghana and Mali, Chad, Mauritania, Niger, and Burundi), or within the context of an emergency (Burundi in 2018). This vaccine bank has not only ensured the timely supply of high-quality vaccines complying with international standards, but it also facilitates the harmonization of PPR control methods in SSA. Regional organizations play a part as well. The Continental Veterinary Vaccine Bank was created in 2018 by the African Union and its Pan-African Veterinary Vaccine Center (PANVAC) with the support of the FAO, the OIE, the EU, the Gates Foundation, USAid, GALVmed, and certain countries (119). It mainly focuses on the prevention of a resurgence of Rinderpest.
Public-Private Partnerships
Over the last decade, public-private partnerships (PPPs) have become an increasingly common method of improving access to veterinary drugs. PPPs are defined as “a collaborative approach in which the public and private sector share resources, responsibilities and risks to achieve common objectives and mutual benefits in a sustainable manner” (120, 121). Recently, the OIE (121) published guidelines for PPPs in the veterinary domain. According to these guidelines, PPPs enable the development of animal health services, policies, and trade to a scale, quality, or degree of geographic coverage that would be unattainable for the public sector alone. PPPs can contribute to the improvement of access to drugs, reinforcement of veterinary services, encouragement of technology transfer agreements, and an increase in R&D into new drugs (121–123).
Over the last few years, different actors (governments, international organizations, NGOs, private companies, philanthropic foundations) have increasingly promoted the value of PPPs. At an international level, many authors in the humane health sector have documented the importance of PPPs and note their implementation as evidence of the increasingly proactive role played by the private sector in global decision-making processes, including in UN activities (108, 124–127). In the veterinary domain, their importance was further emphasized in the OIE Performance of Veterinary Services (PVS) pathway diagram (122), but a limited number of examples of PPPs are available.
The PPP initiated by the Gates Foundation and Zoetis in 2017 within the framework of the African Livestock Productivity and Health Advancement (ALPHA) initiative is one such example. The Gates Foundation pledged an investment of $14.4 million over 3 years (later extended to 5 years until 2022) to bolster the sustainable growth and development of the livestock sector in SSA (primarily in Nigeria, Ethiopia, Uganda, and, more recently, also Tanzania) (128). The partnership aims to improve access to veterinary drugs and services, provide training and education, and implement diagnostic infrastructure (128). Zoetis' role was to: establish basic infrastructure; increase the reliable supply of quality veterinary drugs, diagnostics, and services; develop veterinary laboratory networks and dialogue with government stakeholders to understand local requirements and needs, including regulatory issues (128). The governments of these countries were not directly involved in the partnership, but this example shows how the PPPs can be complementary to public action, which could provide some of the efficiency, management capacities, and culture of evaluation more commonly associated with the private sector.
PPPs can strengthen veterinary services in SSA. The PPP signed in 2011 between the Gates Foundation and Sidai Africa (a private company supplying livestock and crop inputs, and training to farmers and pastoralists across Kenya) pledged to build around 150 branded franchise outlets to facilitate the supply of good quality and affordable veterinary products to 300,000 livestock-keeping households in rural Kenya over a 4-year period (129). While this is not a direct partnership with a government, this PPP demonstrates how the Kenyan government has enabled the private sector to complement its provision of veterinary services and provide veterinary products to rural areas (120).
Conclusion
The different sources mobilized in our paper show that despite differences between and within countries, the Sub-Saharan African drugs market as a whole holds little appeal for international pharmaceutical companies compared to other geographical areas such as emerging Asian countries. It remains peripheral in the global market for modern veterinary drugs, with the exception of South Africa where most of the market is concentrated. The market supply chains are largely unregulated and highly fragmented in terms of registration procedures and market authorization. The distribution chains are weak economically and lack professionals as a consequence of the wave of privatization of veterinary services seen in the 1980s. Therefore, in various countries, we see a dual system for veterinary medicines. On the one hand, the public sector, supported by development organizations, supplies small-scale farmers, mainly in rural areas, but with limited and irregular resources. It focuses on the distribution of vaccines and parasiticides through large-scale campaigns. On the other hand, the largely unregulated private sector supplies the growing market of commercial and industrial livestock farming It relies on private veterinarians, a variety of wholesalers, and retailers (pharmacies, agricultural stores, etc.) including unqualified ones, all tending to cluster in urban and peri-urban areas.
Arrangements have been implemented at the international level to improve drug access in SSA and the efficiency of drug supply chains. They provide “traditional” supports to the different functions of the national veterinary services. Significant efforts have also been made to support national legislation on veterinary drugs (in particular to include the issue of AMR), harmonization of the registration procedures of drugs in SSA, and different arrangements to improve availability (donation, vaccine banks) relying increasingly on PPPs and the involvement of pharmaceutical companies in the drafting and implementation of public policies.
Several conclusions can be drawn for AMR policies and on policies that intend to turn animal health services into a global public good. These policies need to be informed by a better understanding of the drivers behind and the components of access to veterinary drugs in different regional and national contexts. Analysis of what stimulates the use of veterinary drugs in animal farming should not rely too heavily on farmer-veterinarian interactions or on cognitive and psychological factors that shape individual behaviors. These factors are over-emphasized by the studies based on the KAP—Knowledge Attitude and Practices—methodology because the use of drugs by farmers depends greatly on their accessibility. First, there is a need to identify the reasons for low accessibility, which we can divide into low availability (geographic accessibility, potential drug deserts), quality (of drugs, advice, and medical equipment), and economic affordability. In particular, economic studies on affordability are essential if we are to understand the price formation process and how relative prices of drugs influence the decisions of stakeholders. Assessment of drug access should also include the capacity of the whole supply chain to face epidemics and emergencies. Secondly, evolutions in international policy arrangements for veterinary supply chains show the increasing role played by commercial actors in selecting which drugs are made available and under what conditions. This has been made possible by the weak regulation of supply chains and public veterinary services. Policies should balance the interests of the various stakeholders, being careful not to reinforce bias toward certain diseases deemed “interesting” while others, which may still be important for veterinary public health, are neglected.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
Author Contributions
GJ, AH, and MF: conception and design of the work, data collection, data analysis and interpretation, and drafting the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research is part of the ROADMAP project (Rethinking of Antimicrobial Decision-Systems in the Management of Animal Production). It has received funding from the European Union's Horizon 2020 research and innovation program under Grant Agreement No. 817626.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^OIE-WAHIS (OIE World Animal Health Information System) is a database providing worldwide data on the animal health situation and animal health capacities https://wahis.oie.int/.
2. ^According to the OIE terrestrial code, “Para-veterinarians”, or “veterinary paraprofessionals” are professionals authorized by the veterinary status body, working under the direction and responsibility of veterinarians.
References
2. Reynolds Whyte S, Van der Geest S, Hardon A. Social Lives of Medicines. Cambridge: Cambridge University Press (2002).
3. Peterson K. Speculative Markets Drug Circuits and Derivative Life in Nigeria. Durham, NC: Duke University Press Books (2014).
4. Baxerres C, Cassier M, Chabrol F, Haxaire C. Trente-cinq ans d'anthropologie du médicament en Afrique: retour sur l'étude des marchés informels, des hôpitaux et des usages pharmaceutiques. Anthropol Santé. (2017) 14:2462. doi: 10.4000/anthropologiesante.2462
5. Quet M. Impostures pharmaceutiques. Médicaments illicites et luttes pour l'accès à la santé. Paris: La Découverte (2018).
6. Abecassis P, Coutinet N. Marché. Mondial du médicament: une forte dichotomie Nord/Sud. Diplomatie. (2019) 96:74–8. doi: 10.3917/dec.abeca.2018.01. Available online at: https://www.jstor.org/stable/26983306
7. Gemeda BA, Amenu K, Magnusson U, Dohoo I, Hallenberg GS, Alemayehu G, et al. Antimicrobial use in extensive smallholder livestock farming systems in ethiopia: knowledge, attitudes, and practices of livestock keepers. Front Vet Sci. (2020) 7:15. doi: 10.3389/fvets.2020.00055
8. Moffo F, Mouiche MMM, Kochivi FL, Dongmo JB, Djomgang HK, Tombe P, et al. Knowledge, attitudes, practices and risk perception of rural poultry farmers in Cameroon to antimicrobial use and resistance. Prev Vet Med. (2020) 182:105087. doi: 10.1016/j.prevetmed.2020.105087
9. Tebug SF, Mouiche MMM, Abia WA, Teno G, Tiambo CK, Moffo F, et al. Antimicrobial use and practices by animal health professionals in 20 sub-Saharan African countries. Prev Vet Med. (2021) 186:8. doi: 10.1016/j.prevetmed.2020.105212
10. FAO. World Livestock Disease Atlas: A Quantitative Analysis of Global Animal Health Data (2006–2009). Washington: World Bank (2011).
11. Fortané N, Bonnet-Beaugrand F, Hémonic A, Samedi C, Savy A, Belloc C. Learning processes and trajectories for the reduction of antibiotic use in pig farming: a qualitative approach. Antibiotics. (2015) 4:435–54. doi: 10.3390/antibiotics4040435
12. Lhermie G, Raboisson D, Krebs S, Dupraz P. Facteurs déterminants et leviers de réduction de l'usage des antibiotiques en productions animales. Econ Rurale. (2015) 348:3–22. doi: 10.4000/economierurale.4671
13. Dangy L, Fortané N. Les frontières floues de l'expertise scientifique Le cas de la normalisation du medicament vétérinaire. Cahiers Droit Sci Technol. (2016) 6:103–121. doi: 10.4000/cdst.492
14. Fortané N. Antimicrobial resistance: preventive approaches to the rescue? Professional expertise and business model of French “industrial” veterinarians. Rev Agric Food Environ Stud. (2021) 102:213–38. doi: 10.1007/s41130-019-00098-4
15. Bardosh K, Waiswa C, Welburn SC. Conflict of interest: use of pyrethroids and amidines against tsetse and ticks in zoonotic sleeping sickness endemic areas of Uganda. Parasit Vectors. (2013) 6:1–15. doi: 10.1186/1756-3305-6-204
16. Bessell PR, Kushwaha P, Mosha R, Woolley R, Al-Riyami L, Gammon N. Assessing the impact of a novel strategy for delivering animal health interventions to smallholder farmers. Prev Vet Med. (2017) 147:108–16. doi: 10.1016/j.prevetmed.2017.08.022
17. Kingsley P. Inscrutable medicines and marginal markets: tackling substandard veterinary drugs in Nigeria. Pastoral Res Policy Pract. (2015) 5:13. doi: 10.1186/s13570-014-0021-6
18. Rubyogo JC, Murithii PM, Agumbah GJO, Obhai G. Sustainability of a privatized community-based animal health worker system in Mwingi District, Kenya. Trop Anim Health Prod. (2005) 37:253–66. doi: 10.1007/s11250-005-4164-8
19. Muriithi BW, Gathogo NG, Diiro GM, Kidoido MM, Nyanganga MO, Masiga DK. Farmer perceptions and willingness to pay for novel livestock pest control technologies: a case of tsetse repellent collar in Kwale County in Kenya. PLoS Negl Trop Dis. (2021) 15:e0009663. doi: 10.1371/journal.pntd.0009663
20. Grasswitz TR, Leyland TJ, Musiime JT, Sones KR. The Veterinary Pharmaceutical Industry in Africa: A Study of Kenya, Uganda and South Africa. Nairobi, Kenya: African Union, Interafrican Bureau for Animal Resources (AU/IBAR) (2004).
21. Crosia JL. Worldwide market of veterinary drugs: trends analysis for the last ten years and growth forecast. Bull l'Acad Vét France. (2011) 164:21–5. doi: 10.4267/2042/48065
22. Blancou J, Truszczynki M. The role of international and regional organisations in the regulation of veterinary biologicals. Rev Sci Tech Off Int Epiz. (1995) 14:1193–206. doi: 10.20506/rst.14.4.901
23. Thompson S. International harmonization issues. Vet Clin North Am Food Anim Pract. (1999) 15:181–95. doi: 10.1016/S0749-0720(15)30213-9
24. Smith MV. The role of veterinary medicine regulatory agencies. Rev Sci Tecn Office Int Epiz. (2013) 32:393–408. doi: 10.20506/rst.32.2.2229
25. Holmes M, Hill RE. International harmonisation of regulatory requirements. Rev Sci Tech Off int Epiz. (2007) 26:415–20. doi: 10.20506/rst.26.2.1751
26. Le Minor O. L'Asie du Sud-est, un foyer pandémique? Le médicament vétérinaire en question. Bangkok: IRASEC (2016).
27. Cirad and VSF. Document Study on Animal Health Auxiliaries. Paris: MAE, Agricultural Policies and Food Security Bureau (2003).
28. Catley A, Leyland T, Mariner JC, Akabwai DMO, Admassu B, Asfaw W, et al. Para-veterinary professionals and the development of quality, self-sustaining community-based services. Rev Sci Tech Office Int Des Epiz. (2004) 23:225–52. doi: 10.20506/rst.23.1.1476
29. Niang AB. Successful privatisation of para-professional services in traditional livestock farming systems: the case of Senegal. Rev Sci Tech Office Int Epiz. (2004) 23:341–9. doi: 10.20506/rst.23.1.1482
30. Luseba D, Rwambo P. Review of the Policy, Regulatory and Administrative Framework for Delivery of Livestock Health Products and Services in Eastern and Southern Africa. Scotland: GALVMed (2015).
31. Magnani S, Bonnet B, Lancelot R, Metras R. Amélioration de la santé animale en zone sahélienne. Fonctionnement et structure des services vétérinaires Gestion des maladies transfrontalières. Note de cadrage 3è édition des Entretiens techniques du PRAPS (ETP3). Ouagadougou, Burkina Faso: Projet Régional d'Appui au Pastoralisme au Sahel (2018).
32. Abakar MF, Kallo V, Yacoub AH, Souleyman AM, Schelling E. Public and Private Veterinary Services in West and Central Africa: Policy Failures and Opportunities. Cham: Springer International Publishing Ag (2019).
33. Enahoro D, Galie A, Abukari Y, Chiwanga GH, Kelly TR, Kahamba J, et al. Strategies to upgrade animal health delivery in village poultry systems: perspectives of stakeholders from northern Ghana and central zones in Tanzania. Front Vet Sci. (2021) 8:15. doi: 10.3389/fvets.2021.611357
34. Somda J, Kamuanga M, Tollens E. Prospective analysis for community participation in trypanosomosis control in The Gambia. Trop Anim Health Prod. (2006) 38:103–11. doi: 10.1007/s11250-006-4308-5
35. Machila N, Emongor R, Shaw AP, Welburn SC, McDermott J, Maudlin I, Eisler MC. A community education intervention to improve bovine trypanosomiasis knowledge and appropriate use of trypanocidal drugs on smallholder farms in Kenya. Agric Syst. (2007) 94, 261–272. doi: 10.1016/j.agsy.2006.09.004
36. Higham LE, Ongeri W, Asena K, Thrusfield MV. Characterising and comparing drug-dispensing practices at animal health outlets in the Rift Valley, Kenya: an exploratory analysis (part II). Trop Anim Health Prod. (2016) 48:1633–43. doi: 10.1007/s11250-016-1137-z
37. Machila N, Wanyangu SW, McDermott J, Welburn SC, Maudlin I, Eisler MC. Cattle owners' perceptions of African bovine trypanosomiasis and its control in Busia and Kwale Districts of Kenya. Acta Trop. (2003) 86:25–34. doi: 10.1016/S0001-706X(02)00288-7
38. Soudre A, Ouedraogo-Kone S, Wurzinger M, Muller S, Hanotte O, Ouedraogo AG, et al. Trypanosomosis: a priority disease in tsetse-challenged areas of Burkina Faso. Trop Anim Health Prod. (2013) 45:497–503. doi: 10.1007/s11250-012-0248-4
39. Ngumbi AF, Silayo RS. A cross-sectional study on the use and misuse of trypanocides in selected pastoral and agropastoral areas of eastern and northeastern Tanzania. Parasites Vectors. (2017) 10:1–9. doi: 10.1186/s13071-017-2544-3
40. Vougat Ngom RRB, Tomdieu T, Ziébé R, Foyet HS, Moritz M, Vondou L, et al. Quality of veterinary pharmaceuticals and their use by pastoralists in the Far North Region of Cameroon. Pastoralism. (2017) 7:6. doi: 10.1186/s13570-017-0081-5
41. Grace D, Randolph T, Affognon H, Dramane D, Diall O, Clausen PH. Characterisation and validation of farmers' knowledge and practice of cattle trypanosomosis management in the cotton zone of West Africa. Acta Trop. (2009) 111:137–43. doi: 10.1016/j.actatropica.2009.03.009
42. FAO. Legislation for Veterinary Drugs Control. Roma: UN Food and Agriculture Organization (2004).
44. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
45. HealthforAnimals. Illegal Veterinary Medecines. Bruxelles: Impact on effective control. HealthforAnimals (2017).
46. GALVmed. Review of the Policy, Regulatory and Administrative Framework for Delivery of Livestock Health Products and Services in Eastern and Southern Africa. Edinburg: GALVmed (2015).
47. Dione MM, Ouma EA, Roesel K, Kungu J, Lule P, Pezo D. Participatory assessment of animal health and husbandry practices in smallholder pig production systems in three high poverty districts in Uganda. Prev Vet Med. (2014) 117:565–76. doi: 10.1016/j.prevetmed.2014.10.012
48. Ilukor J, Birner R, Nielsen T. Addressing governance challenges in the provision of animal health services: a review of the literature and empirical application transaction cost theory. Prev Vet Med. (2015) 122:1–13. doi: 10.1016/j.prevetmed.2015.10.003
49. Ilukor J. Improving the delivery of veterinary services in Africa: insights from the empirical application of transaction costs theory in Uganda and Kenya. Rev Sci Tech. (2017) 36:279–89. doi: 10.20506/rst.36.1.2628
50. Chema S, Gathuma JM. Kenya: the development of private services and the role of the Kenya Veterinary Association. Rev Sci Tech. (2004) 23:331–40. discussion 391–401. doi: 10.20506/rst.23.1.1483
51. Woodford JD. Synergies between veterinarians and para-professionals in the public and private sectors: organisational and institutional relationships that facilitate the process of privatising animal health services in developing countries. Rev Sci Tech. (2004) 23, 115–135. discussion 391-401. doi: 10.20506/rst.23.1.1472
52. Smith LD. Reform and Decentralization of Agricultural Services: A Policy Framework. Geneva: FAO, Food and Agriculture Organization of the United Nations (2001).
53. Jenjezwa VR, Seethal CEP. The role of the state in stock farming in rural areas: a case study of Hertzog, Eastern Cape, South Africa. J S Afr Vet Assoc. (2014) 85:7. doi: 10.4102/jsava.v85i1.912
54. Bath GF, Penrith ML, Leask R. A questionnaire survey on diseases and problems affecting sheep and goats in communal farming regions of the Eastern Cape province, South Africa. J S Afr Vet Assoc. (2016) 87:10. doi: 10.4102/jsava.v87i1.1348
55. Armson B, Ekiri AB, Alafiatayo R, Cook AJ. Small ruminant production in Tanzania, Uganda, and Ethiopia: a systematic review of constraints and potential solutions. Vet Sci. (2021) 8:13. doi: 10.3390/vetsci8010005
56. Landais E. Sur les doctrines des vétérinaires français coloniaux en Afrique noire. Cahier Sci Hum. (1990) 26:33–71.
57. Mayen F. A status report of veterinary education in Ethiopia: perceived needs, past history, recent changes, and current and future concerns. J Vet Med Educ. (2006) 33:244–7. doi: 10.3138/jvme.33.2.244
58. Gehring R, Swan GE, Sykes RD. Supply of veterinary medicinal products to an emerging farming community in the North West Province of South Africa. J South African Vet Assoc. (2002) 73:185–9. doi: 10.4102/jsava.v73i4.584
59. Cheneau Y, El Idrissi AH, Ward D. An assessment of the strengths and weaknesses of current veterinary systems in the developing world. Rev Sci Tech L Office Int Epiz. (2004) 23:351–9. doi: 10.20506/rst.23.1.1489
60. Tourrand J-F, Waquil P, Maraval M-C, Sraïri MT, Duarte LMG, Kozloski GV. Livestock Policy. Montpellier: CIRAD (2020). doi: 10.19182/agritrop/00143
61. Roger F, Thonnat J, Hendrikx P, Domenech J. Disease monitoring and surveillance systems and the role of public and private animal health agents: the experience of Africa. Rev Sci Techniq Office Int Epiz. (2004) 23:137–45. doi: 10.20506/rst.23.1.1471
62. Marcotty T, Matthys F, Godfroid J, Rigouts L, Ameni G, Gey van Pittius N, et al. Zoonotic tuberculosis and brucellosis in Africa: neglected zoonoses or minor public-health issues? The outcomes of a multi-disciplinary workshop. Ann Trop Med Parasitol. (2009) 103:401–11. doi: 10.1179/136485909X451771
63. Greter H, Jean-Richard V, Crump L, Bechir M, Alfaroukh IO, Schelling E, et al. The benefits of 'One Health' for pastoralists in Africa. Onderstepoort J Vet Res. (2014) 81:3. doi: 10.4102/ojvr.v81i2.726
64. FAO. Contract Farming and Public–Private Partnerships in Aquaculture. Lessons Learned From East African Countries. Geneva: FAO (2018).
65. Umali DL, Feder G, Haan CD. The Balance Between Public and Private Sector Activities in the Delivery of Livestock Services. Washington, DC: World Bank (1992).
66. FAO. Animal Health Service Activities in the Field of Privatization, Restructuring and Decentralization of Veterinary Services in Africa. Rome: FAO (2018).
67. Catley A, Leyland T. Community participation and the delivery of veterinary services in Africa. Prev Vet Med. (2001) 49:95–113. doi: 10.1016/S0167-5877(01)00171-4
68. Silkin T, Kasirye F. Veterinary services in the Horn of Africa: Where Are We Now? A Review of Animal Health Policies and Institutions Focusing in Pastoral Areas. Nairobi: AU/IBAR.
69. Daborn C, Cooper JE, Kithuka MA. History of the Animal Health and Industry Training Institute, Kenya. Vet Rec. (2013) 172:430. doi: 10.1136/vr.f2440
70. Turkson PK. A comparison of the delivery of veterinary services to small-scale and medium to large-scale poultry keepers in peri-urban Ghana. Rev Sci Tech. (2008) 27:719–30. doi: 10.20506/rst.27.3.1834
71. Diop BA, Bessin R. Liens entre agents non professionnels et Services vétérinaires officiels en Afrique au Sud du Sahara. Rev Sci Tech Off Int Epiz. (2004) 23:147–56. doi: 10.20506/rst.23.1.1470
72. Mugunieri GL, Irungu P, Omiti JM. Performance of community-based animal health workers in the delivery of livestock health services. Trop Anim Health Prod. (2004) 36:523–35. doi: 10.1023/B:TROP.0000040930.94967.77
73. Peeling D, Holden S. The effectiveness of community-based animal health workers, for the poor, for communities for public safety. Rev Sci Tech L'Office Int Des Épiz. (2004) 23:253–76. doi: 10.20506/rst.23.1.1475
74. Bleich EG, Rhissa Z, Mack S. The FAO special programme for food security: livestock diversification - a case study in Chad. Worlds Poultry Sci J. (2005) 61:23–9. doi: 10.1079/WPS200438
75. Gehring R. Suspected adverse reactions to veterinary drugs reported in South Africa (January 1998-February 2001). J S Afr Vet Assoc. (2001) 72:120–6. doi: 10.4102/jsava.v72i3.634
76. Coutinet N, Abecassis P. Les freins à la production locale et à l'accès aux traitements en Afrique. In: Le médicament en Afrique: répondre aux enjeux d'accessibilité et de qualité, editor, Proparco. Paris: AFD (2018).
77. Roger F, Bonnet P. Control of endemic tropical diseases Identifying certain animal diseases as neglected. Perspect Policy Brief. (2015) 15:18. doi: 10.19182/agritrop/00018
78. Porphyre V, Rakotoharinome M, Randriamparany T, Pognon D, Prévost S, Le Bizec B. Residues of medroxyprogesterone acetate detected in sows at a slaughterhouse, Madagascar. Food Additiv Contam Part A. (2013) 30:2108–13. doi: 10.1080/19440049.2013.848293
79. Kingsley P. Fake Animal Drugs Threaten African Livestock and Livelihoods. Melbourne: The Conversation (2012).
80. Akerlof GA. The market for lemons. Quality uncertainty and the market mechanism. Q J Econ. (1970) 84:488–500. doi: 10.2307/1879431
81. Bengaly Z, Vitouley SH, Somda MB, Zongo A, Teko-Agbo A, Cecchi G, et al. Drug quality analysis of isometamidium chloride hydrochloride and diminazene diaceturate used for the treatment of African animal trypanosomosis in West Africa. BMC Vet Res. (2018) 14:1–8. doi: 10.1186/s12917-018-1633-7
82. Tchamdja E, Kulo AE, Akoda K, Teko-Agbo A, Assoumy AM, Niang EMM, et al. Drug quality analysis through high performance liquid chromatography of isometamidium chloride hydrochloride and diminazene diaceturate purchased from official and unofficial sources in Northern Togo. Prev Vet Med. (2016) 126:151–8. doi: 10.1016/j.prevetmed.2016.02.001
83. Tekle T, Terefe G, Cherenet T, Ashenafi H, Akoda KG, Teko-Agbo A, et al. Aberrant use and poor quality of trypanocides: a risk for drug resistance in south western Ethiopia. BMC Vet Res. (2018) 14:1–8. doi: 10.1186/s12917-017-1327-6
84. Mordor Intelligence. Global Veterinary Healthcare Market 2018–2023. Report sample. Bengaluru: Mordor (2017).
86. Transparency Market Research. Veterinary Drugs Market: Global Industry Analysis, Size, Share, Growth, Trends, and Forecast, 2016–2024. Albany: Transparency Market Research (2017).
87. Future Market Insights. Animal Healthcare Market: Global Industry Analysis 2012 −2016 and Opportunity Assessment 2017–2027 (Report Sample). London: FMI (2017).
88. Messomo Ndjana F. Etude de la distribution et de la qualité des médicaments vétérinaires au Cameroun. Ecole Inter-Etats des Sciences et Médecine Vétérinaires de Dakar (EISMV). Dakar: UCAD (2006).
90. Mouiche MMM, Moffo F, Betsama JDB, Mapiefou NP, Mbah CK, Mpouam SE, et al. Challenges of antimicrobial consumption surveillance in food-producing animals in sub-Saharan African countries: patterns of antimicrobials imported in Cameroon from 2014 to 2019. J Glob Antimicrob Resist. (2020) 22:771–8. doi: 10.1016/j.jgar.2020.06.021
91. ILRI. Mapping of Poverty and Likely Zoonoses Hotspots. Geneva: ILRI, Report to Department for International Development (DFID), UK (2012).
92. Delgado C, Rosegrant M, Steinfeld H, Ehui S, Courboi C. Livestock to 2020 – The Next Food Revolution. Washington: International Food Policy Research Institute (1999).
93. Robinson TP, Thornton PK, Francesconi GN, Kruska RL, Chiozza F, Notenbaert AMO, et al. Global Livestock Production Systems. Rome: FAO and ILRI (2011).
95. Gongora V, Rogers J. Report of the Veterinary Legislation Identification Mission: Republic of Mozambique. Paris: OIE (2015).
96. GatesFoundation. Options Assessment for Regulatory Harmonisation of Livestock Products in Sub-Saharan Africa Veterinary. Edinburgh: Gates Foundation (2019).
97. Orand J-P. Normes de l'Organisation mondiale de la santé animale et besoins futurs. Rev Sci Tech Off Int Epiz. (2012) 31:325–34. doi: 10.20506/rst.31.1.2121
99. Mitema ES. Improved management of drugs, hormones and pesticides in Africa. Onderstepoort J Vet Res. (2009) 76:155–9. doi: 10.4102/ojvr.v76i1.80
100. FAO and OMS. Commission du codex Alimentarius: Manuel de procédure 24 edition. Rome: FAO (2015).
101. Marion H. Antimicrobial resistance and the guidelines of the International Cooperation on Harmonisation of Technical Requirements for Registration of Veterinary Medicinal Products (VICH). Rev Sci Tech Off Int Epiz. (2012) 1:299–306. doi: 10.20506/rst.31.1.2113
102. GALVmed. A Policy Scoping Study on Harmonization of Registration Requirements for Veterinary Products for Mutual Recognition Among East African Community Partner States. Edinburg: GALVmed (2016).
103. Daré I. Harmonisation of Marketing Authorisations and Quality Control of Veterinary Products Within the WAEMU Region, Presentation to the “Regional Training Seminar for OIE Focal Points for Veterinary Products in Africa. Johannesburg, South Africa (2010).
104. SADC. Regional Guidelines for the Registration of Veterinary Drugs in SADC Member States. Gaborone: SADC (2011).
105. Schouten E. Drug donations must be strictly regulated. BMJ. (1995) 1995:311–s684. doi: 10.1136/bmj.311.7006.684
106. Hogerzeil HV. Guidelines for drug donations. BMJ Br Med J. (1997) 314:737. doi: 10.1136/bmj.314.7082.737
107. Clark M, Embrey M. Pharmaceutical donations. In: MSD-3: Managing Access to Medicines and Health Technologies. Arlington, TX: Management Sciences for Health (2012). p. 275–87.
108. Guilbaud A. Business partners: firmes privées et gouvernance mondiale de la santé. Paris: Presses de Sciences Po (2015).
109. Guilloux A, Moon S. Hidden Price Tags: Disease-Specific Drug Donations: Costs and Alternatives. MSF/DND Working Group:189-2010 (2001).
111. FAO. FAO, EU Donate Peste des Petis Ruminants (PPR) Vaccine Machine to Ethiopia. Rome: FAO (2021).
115. Lombard M, Füssel AE. Antigen and vaccine banks: technical requirements and the role of the european antigen bank in emergency foot and mouth disease vaccination. Rev Sci Tech. (2007) 26:117–34. doi: 10.20506/rst.26.1.1733
119. AfricanUnion. The Chairperson of the African Union Commission inaugurates the Continental Veterinary Vaccine Bank. AfricanUnion (2018).
120. Thevasagayamn SJ, Dieuzy-Labaye I, Tagliaro E. Partenariats public-privé: attentes des partenaires privés concernant la santé animale au niveau international et les programmes de développement de l'élevage. Paris: OIE (2017).
121. OIE. The OIE PPP Handbook: Guidelines for Public-Private Partnerships in the Veterinary Domain. Paris: OIE (2019).
122. Galière M, Peyre M, Muñoz F, Poupaud M, Dehove A, Roger F, et al. Typological analysis of public-private partnerships in the veterinary domain. PLoS ONE. (2019) 14:e0224079. doi: 10.1371/journal.pone.0224079
124. Buse K, Walt G. Global public-private partnerships—Part 1: a new development in health? Bull World Health Organ. (2000) 78:549–61.
125. Ndour M. Partenariats public-privé mondiaux pour la santé: L'émergence d'une gouvernance transnationale des problèmes de santé des pays en développement? Coll. Idées pour le débate Vol. 7. Paris: Iddri (2006). Available online at: https://www.iddri.org/sites/default/files/import/publications/id_0607_ndour_ppp.pdf
126. Barry M, Boidin B, Yaya S. Les partenariats multipartites pour l'aide à la santé: fondements et ambiguïtés. J Gest Econ Méd. (2014) 32:308–26. doi: 10.3917/jgem.144.0308
127. Guilbaud A. Les partenariats public-privé sanitaires internationaux: diffusion et incarnation d'une norme de coopération. Mondes Dév. (2015) 2:91–104. doi: 10.3917/med.170.0091
Keywords: access to medicines (ATM), animal health, international pharmaceutical market, supply chain, Sub-Saharan Africa (SSA), veterinary drugs
Citation: Jaime G, Hobeika A and Figuié M (2022) Access to Veterinary Drugs in Sub-Saharan Africa: Roadblocks and Current Solutions. Front. Vet. Sci. 8:558973. doi: 10.3389/fvets.2021.558973
Received: 04 May 2020; Accepted: 10 December 2021;
Published: 09 March 2022.
Edited by:
Gareth Enticott, Cardiff University, United KingdomReviewed by:
Mohamed Moctar Mouliom Mouiche, University of Ngaoundéré, CameroonLisa A. Murphy, University of Pennsylvania, United States
Copyright © 2022 Jaime, Hobeika and Figuié. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Glória Jaime, Z2xvcmlhLmphaW1lQGNpcmFkLmZy