 Lavinia Bianca Balea
Lavinia Bianca Balea Ragnhild J. A. Gulestø
Ragnhild J. A. Gulestø Hongxuan Xu
Hongxuan Xu Stinne Glasdam
Stinne Glasdam- 1Private, Bucharest, Romania
- 2Department of Health Sciences, Institute of Nursing, VID Specialized University, Oslo, Norway
- 3Department of Care Sciences, Faculty of Health and Society, Malmö University, Malmö, Sweden
- 4Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden
Background: Patients’ adherence to antibiotic treatment and related prevention of AMR is significant. Understanding healthcare professionals’ strategies for advising and educating patients in primary care settings is crucial.
Aim: From the perspectives of professionals and patients, to explore how physicians, pharmacists, and nurses educate patients about antibiotic use and antimicrobial resistance in primary care settings.
Methods: A qualitative systematic literature review was conducted in MEDLINE, EMBASE, CINAHL Complete, Eric, SocINDEX, PsycInfo, Web of Science and Scopus. The study included 102 publications, followed PRISMA recommendations and was registered in PROSPERO (reg.no. CRD4202455761). The studies were screened and selected based on specific inclusion and exclusion criteria using Covidence. Quality appraisal followed the Critical Appraisal Skills Program (CASP) qualitative study checklist. Data were extracted, and the analysis consisted of a descriptive numerical summary analysis and a qualitative thematic analysis.
Results: The analyzed studies spanned multiple countries and settings and included perspectives of primary care physicians, pharmacists, nurses and patients. Two main themes emerged: (1) Relationships between professionals and patients influenced educational strategies, showing that trust and rapport between healthcare professionals and patients played a crucial role in shaping educational strategies around antibiotic use; (2) The organizational structures challenged professionals in guiding and educating patients, highlighting how limited resources, time constraints, and system-level pressures hindered healthcare professionals’ ability to provide consistent and effective education. Often, structural challenges led to not educating the patients on the risks of antibiotic misuse and antimicrobial resistance. The use of delayed prescriptions emerged as a strategy for improved AMR stewardship and to meet patients’ expectations for antibiotic treatment, though it raised concerns about undermining professional responsibility and authority in ensuring appropriate antibiotic use.
Conclusion: Healthcare professionals’ role in educating patients about antibiotic use and AMR in primary care settings was complex, with different challenges faced by nurses, pharmacists and primary care physicians. These challenges extended beyond the clinical level, including relational, social and structural factors. Power dynamics, trust issues, and time pressures often hindered effective education on antibiotic use. Addressing gaps in education on antibiotic use and AMR requires acknowledging these multifaceted challenges, with future efforts focusing on better supporting healthcare professionals in this context.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD4202455761.
Introduction
According to the World Health Organization (WHO, 2017), antimicrobial resistance (AMR) occurs when bacterial, viral, parasitic, and fungal microorganisms develop resistance to antimicrobial medicines. AMR is a significant contemporary social issue and a global priority for policymakers (Andersson et al., 2019; Center for Disease Dynamics, Economics & Policy, 2015; World Health Organization, 2015). In 2019, AMR was associated with 4.95 million deaths and directly attributable to 1.27 million deaths (Antimicrobial Resistance Collaborators, 2022). If unaddressed, the burden of the AMR-related disease is projected to reach 10 million deaths annually by 2050. A major driver of AMR is the misuse and overuse of antibiotics, particularly in primary care, which accounts for over 80% of antibiotic use worldwide (Wang et al., 2021). Thus, decreasing the inappropriate use of antibiotics in primary care is crucial to tackling AMR (Heyman et al., 2014).
Primary care physicians, pharmacists, and nurses are on the front lines of managing antibiotic use and advising patients on the prevention of AMR in primary care settings (Alves et al., 2021; Burnett, 2018; Sumner et al., 2018; Wong et al., 2021). Proper education regarding antibiotic use may ensure that patients understand the importance of rational antibiotic therapy, which is essential for reducing the risk of resistance (Korkmaz et al., 2024; Lambert et al., 2024; Rao et al., 2020). However, a survey-based study reveals that although 67% of patients received advice about their infection, only 8% recalled being informed about antibiotic resistance (McNulty et al., 2016). This significant gap highlights the need for improved education and communication strategies provided by healthcare professionals regarding both the proper use of antibiotics and the implications of AMR. A key prerequisite for addressing the gap is ensuring that healthcare professionals possess adequate knowledge regarding the appropriate use of antibiotics (Lalithabai et al., 2022; Lim et al., 2022; Ness et al., 2014). Research indicates that effective patient education and guidance from healthcare professionals play a crucial role in supporting antimicrobial stewardship. This involves strategies aimed at optimizing antibiotic use to prevent resistance (Ha et al., 2017; Miller et al., 2020). For instance, informing patients about the potential side effects of antibiotics and how to manage them can improve treatment compliance and health outcomes (Nieuwlaat et al., 2014). A recent review highlights that public health campaigns utilizing mass media for information dissemination, along with targeted messaging about specific infections and interactions between healthcare professionals and patients, can effectively improve public awareness of AMR and influence patients’ behavior regarding antibiotic use (Gilham et al., 2024).
Non-adherence to antibiotic treatment remains a critical challenge. Several factors influence patients’ adherence, including their knowledge of antibiotics and AMR, past experiences with infections and treatments, attitudes towards antibiotics use, as well as considerations like time and financial resources. Additionally, trust in prescribed treatment regimens and the level of social support they receive also play crucial roles in their adherence to treatment (Gualano et al., 2015; Lee et al., 2023; McCubbin et al., 2021; Pristianty et al., 2019). Responsible antibiotic use is determined not only by patient-related factors but also by a complex interplay of external influences at different levels, such as healthcare professionals’ practices, societal norms, healthcare guidelines or policies, and public health initiatives (Schmiege et al., 2020; Sievert et al., 2024). In primary care settings, physicians play a pivotal role in antibiotic prescriptions. However, they often face challenges stemming from limited knowledge or misconceptions about antibiotic use. Additionally, patient expectations and external influences, such as pharmaceutical marketing, can contribute to the overprescription of antibiotics, ultimately leading to antibiotic misuse and AMR (Md Rezal et al., 2015; Sievert et al., 2024; Sulis et al., 2020). While pharmacists and nurses are crucial in promoting antibiotic stewardship, their ability to influence prescriptions is limited once antibiotics are prescribed. This highlights the need for improved collaboration and continuous education across all healthcare professionals in primary care settings (Lim et al., 2022; Ness et al., 2014). Given that primary care’s nature and mission are to provide accessible, comprehensive, and preventive care, primary healthcare professionals are often the first point of contact for patients seeking medical care, providing them a critical position as gatekeepers to influence the appropriate use of antibiotics and reduce the occurrence of AMR (Sijbom et al., 2023; World Health Organization, 2018).
Despite these critical issues within primary care settings, existing literature primarily focuses on hospital settings or patients behaviors (Camerini et al., 2024; Giamarellou et al., 2023; Rachina et al., 2024), leaving the practices and educational strategies in primary care largely unexplored. Given the significant impact of patients’ non-adherence to antibiotic treatment and prevention of AMR, understanding the specific educational roles and strategies of healthcare professionals in primary care settings is crucial. Therefore, from the perspectives of both professionals and patients, the study aimed to explore how physicians, pharmacists, and nurses educate patients about antibiotic use and AMR in primary care settings.
Method
This study carried out a qualitative systematic review to synthesize findings from various qualitative research studies. The method was inspired by Bettany-Saltikov and McSherry (2016). The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, ensuring transparency, rigor, and consistency in the systematic review process (Page et al., 2021). The review protocol is registered with PROSPERO (registration number CRD4202455761).
Inclusion and exclusion criteria
Inclusion and exclusion criteria were established based on the PEO model (Table 1). The PEO model was chosen as it provided a structured approach to framing research questions and organizing data that aligns well with qualitative methodologies (Bettany-Saltikov and McSherry, 2016; Khan et al., 2004). The inclusion criteria were: 1) Primary care physicians (e.g., GPs, surgeons, and pediatricians), pharmacists, and nurses, working in primary healthcare settings or community care advising, 2) Perspectives of patients/citizens and primary care physicians, pharmacists, and nurses, 3) Qualitative studies or qualitative sub-studies in mixed method studies, 4) Published between 2014 to 2024, to reflect the most current evidence related to antibiotic stewardship, and 5) Published in English, Scandinavian or Romanian. The review excluded: 1) Systematic literature reviews, 2) Intervention studies, 3) Studies about vaccination, 4) Editorials/comments, 5) Dental care, 6) Guidelines/recommendations, and 7) Simulation studies.

Table 1. Populations, Exposures, and Outcomes (PEO).
Searching, selection, appraising, and extraction relevant data
A qualitative systematic literature review was conducted in MEDLINE, EMBASE, CINAHL Complete, Eric, SocINDEX, PsycInfo, and Web of Science (Last search 8 July 2024), supported by an experienced librarian. The initial search retrieved 9948 publications, which were transferred to Covidence software for screening. The search strategies are presented in Table 2. To identify additional relevant studies, a citation pearl search was conducted in the Scopus database (Last search 1 August 2024).
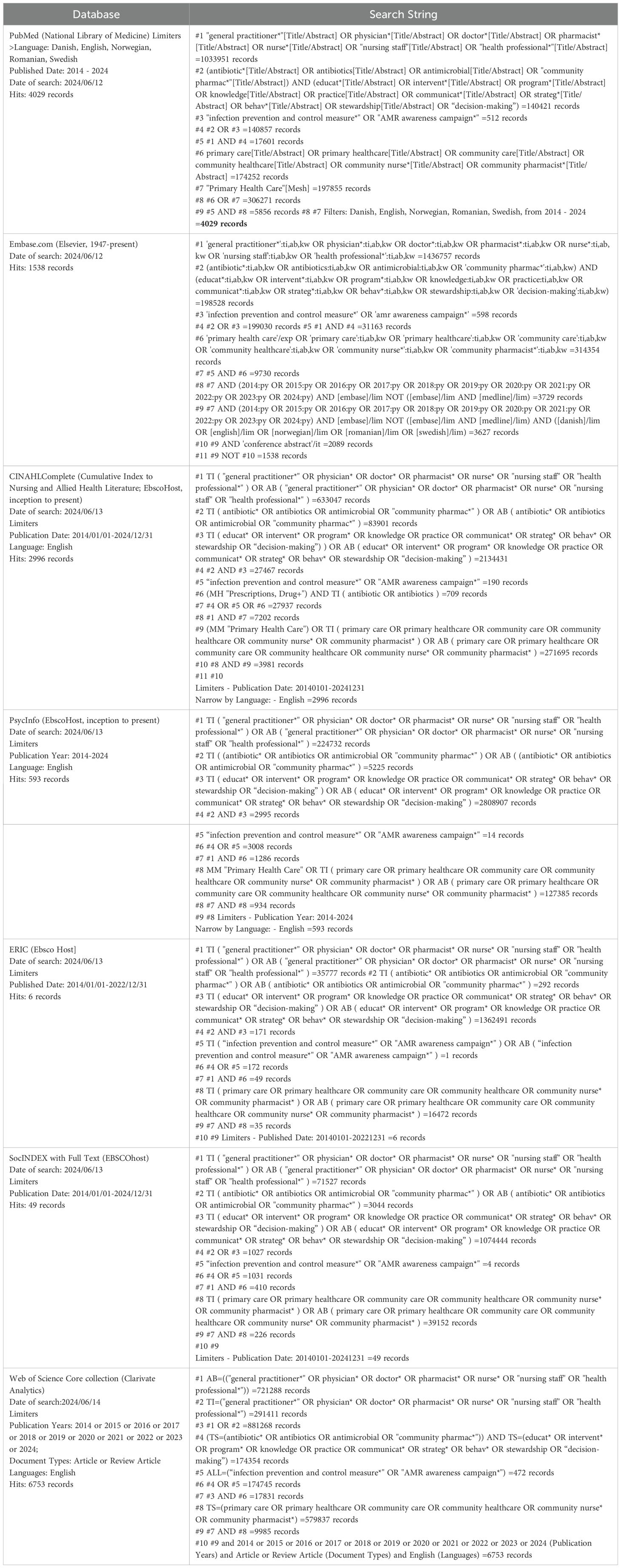
Table 2. The full electronic search strategy for all three databases.
Two of the authors (LBB and SG) collaborated on the study selection process. In cases of disagreement during the screening, full-text review, or citation search processes, discussions were held with the other authors (RJAG and HX) until a consensus was reached. A PRISMA flow diagram illustrates the study selection process (Figure 1). As a second opinion, RJAG reviewed all the included articles in relation to the inclusion and exclusion criteria, which supported the selection. The 102 included publications are marked with an asterisk (*) in the reference list.
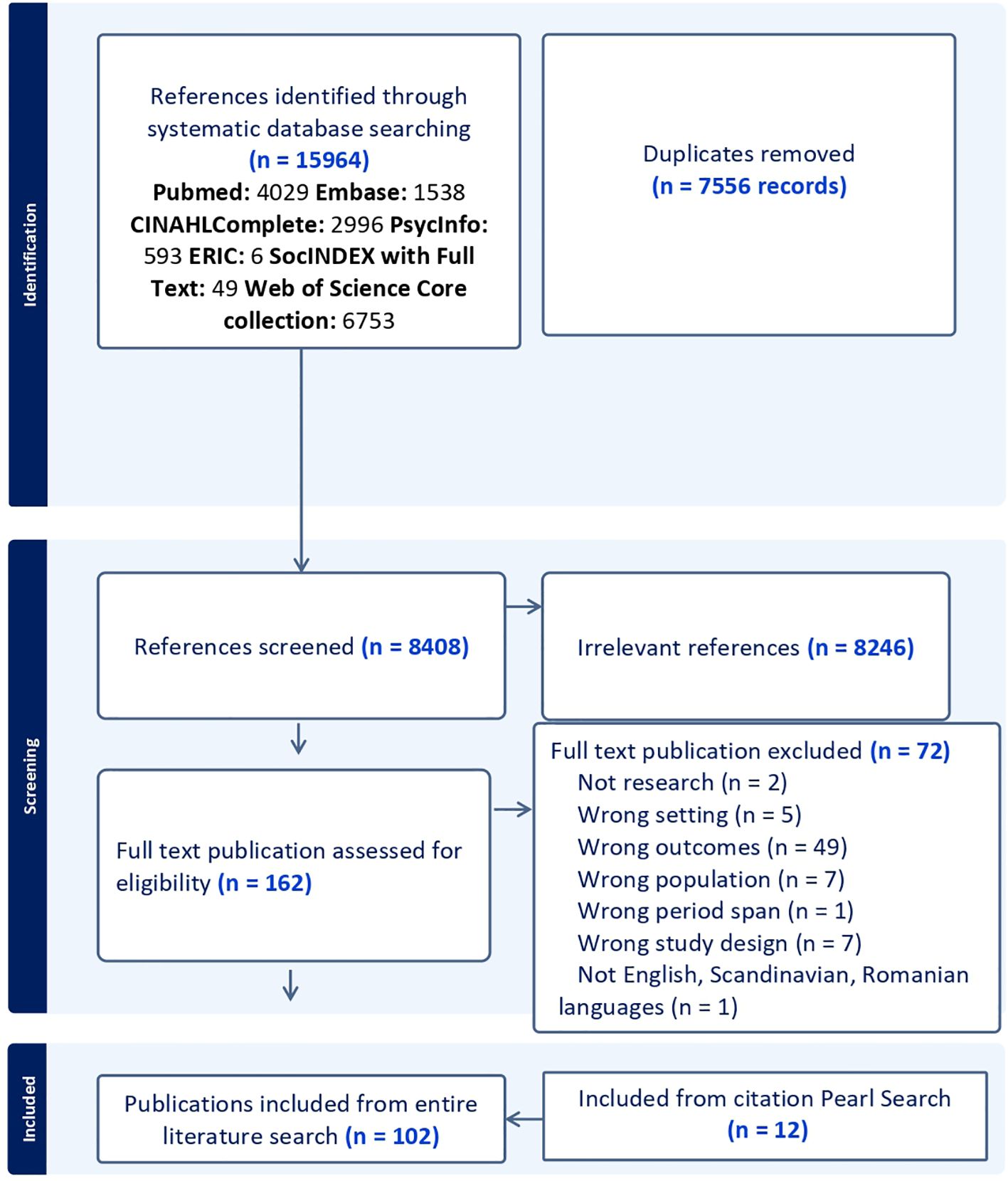
Figure 1. PRISMA 2020 flow diagram of study selection here.
The quality of the included publications was assessed using the Critical Appraisal Skills Program (CASP) qualitative study checklist (Critical Appraisal Skills Program, 2018). The use of the CASP qualitative study checklist provided a systematic method for assessing the quality of included publications, demonstrating a commitment to methodological rigor and ensuring the review’s findings were grounded in credible, high-quality evidence. The use of the checklist was endorsed by the Cochrane Qualitative and Implementation Methods Group (Long et al., 2020). This checklist consists of ten questions evaluating various aspects of the studies, including their aim, methodology and design, recruitment strategy, data collection, data analysis, findings, and overall research value (see Table 3). The purpose of the quality appraisal was to ensure the strength of the evidence in addressing our research question.
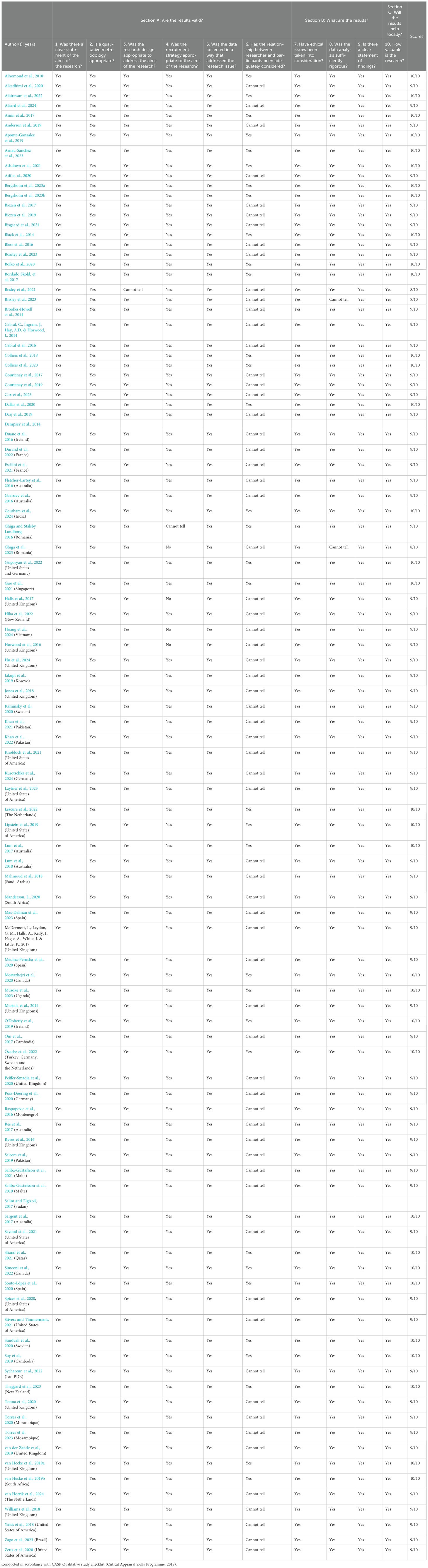
Table 3. Qualitative study appraisal*.
Strategy for data analysis
The data analysis strategy included a descriptive numerical summary analysis, presented as ‘Characteristics of the Studies’, and an inductive thematic analysis inspired by Braun and Clarke (2006).
First, the publications were read multiple times, facilitating familiarization with the material (Braun and Clarke, 2006). The following data were extracted: 1) Authors, 2) Location, 3) Journal, 4) Study period, 5) Study design, 6) Sample size, 7) Target group and context, 8) Theory/concepts, 9) Results, and 10) Limitations. Data extraction focused on the qualitative findings relevant to the review aim (Bettany-Saltikov and McSherry, 2016). The included studies represent diverse contexts and countries, each with unique cultural and healthcare system characteristics. To manage this heterogeneity, we focused on extracting data that was applicable across various settings while noting contextual differences. All authors checked the extracted data for accuracy. A selection of this data extraction is presented in Table 4.

Table 4. Study characteristics.
The results sections of the publications were coded, and these codes were reorganized to align with the review’s aim (Braun and Clarke, 2006). Initial themes were constructed from the coded material based on similarities and differences. Similar codes were grouped into themes. The themes were reviewed and further developed through a consensual process among the authors, iterating between the constructed themes, the empirical data, and the research question to ensure the themes accurately reflected the empirical material (Braun and Clarke, 2006). Finally, each main theme and sub-theme were defined, refined, named, and reviewed to ensure they were concise and adequately descriptive (Braun and Clarke, 2006). The (sub)themes were narratively described to achieve the study’s aim. For practical reasons, we refer to all non-professional actors as patients. However, we recognize that many participants are not current patients but citizens representing former or potential patients, clients, parents, or others.
Results
Characteristics of the studies
In total, 102 publications were included, all published in English (see Table 4 for details). Of these, 14 publications primarily focused on primary care physicians’, pharmacists’, and nurses’ education of patients about antibiotic use and antimicrobial resistance in primary care settings (Alzard et al., 2024; Atif et al., 2020; Bergsholm et al., 2023a, 2023b; Cabral et al., 2014, 2016; Durand et al., 2022; Essilini et al., 2021; Ghiga and Stålsby Lundborg, 2016; Hu et al., 2024; Knobloch et al., 2021; Manderson, 2020; Musoke et al., 2023; Peiffer-Smadja et al., 2020). The remaining 88 publications addressed primary care physicians’, pharmacists’, and nurses’ education of patients about antibiotic use and antimicrobial resistance in primary care settings as a secondary focus.
The studies were conducted in 38 different countries across all populated continents: the United Kingdom (n=21), Australia (n=11), the USA (n=10), Spain (n=6), the Netherlands (n=5), Pakistan (n=4), Germany (n=4), Sweden (n=3), and Norway (n=3). Additionally, 13 other countries each contributed two publications, and 17 countries were represented by one publication each. Three studies were conducted across multiple countries (Brookes-Howell et al., 2014; Grigoryan et al., 2022; Özcebe et al., 2022).
A majority of the publications (n = 66) used individual semi-structured interviews as a data collection method, conducted either face-to-face or through video/telephone. Eleven publications used focus groups as the only data collection method, one study collected reports/documents as empirical material, and one publication used observations. Fourteen publications combined qualitative methods such as observations, video recordings, documents, and individual and/or focus group interviews. Mixed methods using different quantitative and qualitative data collection methods were used in nine publications.
The studies were all published between 2014 and 2024 and conducted between 2010 and 2022. One study, Stivers and Timmermans (2021) also included a study period from 2003 to 2004. Seventeen of the other publications did not specify their study periods. The publications’ total population included 962 primary care physicians, such as GPs, psychiatrists, surgeons, pediatricians and unspecified physicians, 591 pharmacists, 147 nurses, 1100 (+) patients and 236 others, including stakeholders and other health care professionals.
All selected publications demonstrated appropriate methodological rigor based on the outcomes of the CASP checklist (Critical Appraisal Skills Program, 2018) (Table 3).
Relationships between patients and professionals influenced educational strategies
The significance of a robust patient-professional relationship
From the perspectives of primary care physicians, pharmacists, nurses, and patients, a trusting relationship was perceived to create an environment where patients could feel acknowledged and heard (Alzard et al., 2024; Bergsholm et al., 2023a; Brookes-Howell et al., 2014; Dallas et al., 2020; Durand et al., 2022; Ghiga and Stålsby Lundborg, 2016; Hika et al., 2022; Khan et al., 2022; Mustafa et al., 2014; Sargent et al., 2017; Sköld et al., 2017; Souto-López et al., 2020; Spicer et al., 2020; Suy et al., 2019; Thaggard et al., 2023; Zetts et al., 2020). Trust and robustness was crucial when facilitating effective education and guidance regarding antibiotic use, and it reduced patient expectations for antibiotics (Alhomoud et al., 2018; Aponte-González et al., 2019; Bergsholm et al., 2023b; Ghiga and Stålsby Lundborg, 2016; Saleem et al., 2019; Sargent et al., 2017; Simeoni et al., 2022; Zetts et al., 2020). This allowed the professionals to manage patient expectations more effectively, including explaining the reasons for not prescribing antibiotics (Simeoni et al., 2022; Zetts et al., 2020). For instance, both primary care physicians and nurses highlighted the importance of discussing treatment options with the patients’, facilitating a collaborative environment where patients felt their input was valued (Boiko et al., 2020; Guo et al., 2021; Halls et al., 2017). Discussing antibiotic use with patients gave some primary care physicians a sense of control over the situation (Dallas et al., 2020; Guo et al., 2021; Kurotschka et al., 2024). This included discussing different treatments’ potential benefits and AMR risks (Ashdown et al., 2016; Kurotschka et al., 2024). Several primary care physicians perceived these approaches as critical components of the educational role (Ashdown et al., 2016; Guo et al., 2021; Kurotschka et al., 2024).
According to primary care physicians’, pharmacists’ and patients’ view, a solid relationship promoted adherence to prescribed treatments and overall receptiveness to medical advice (Alzard et al., 2024; Guo et al., 2021; Hika et al., 2022; Kurotschka et al., 2024; Lum et al., 2017; Mustafa et al., 2014). Pharmacists also engaged patients in decision-making by asking pertinent questions about physicians’ advice, such as dosing intervals or indications of a specific antibiotic (Bergsholm et al., 2023a). Furthermore, taking into account patients’ previous experiences with medications was reported to foster trust, which emerged as a critical factor in building confidence in prescribing/dispensing decisions (Bergsholm et al., 2023b; Brookes-Howell et al., 2014; Courtenay et al., 2019; Dallas et al., 2020; Guo et al., 2021; Knobloch et al., 2021; van der Zande et al., 2019; Zetts et al., 2020). Some pharmacists highlighted that informal interactions fostered rapport, increased awareness of antibiotic use and resistance (Durand et al., 2022), and enhanced their accessibility and role in community healthcare through valuable information and free counselling during medication dispensing (Alhomoud et al., 2018). Primary care physicians and pharmacists also noted that a solid relationship could help manage patient dissatisfaction, even when treatments did not meet patients’ expectations (Kurotschka et al., 2024; Ghiga et al., 2023; Simeoni et al., 2022). Explaining why antibiotics were not prescribed while acknowledging patients’ experiences helped build stronger relationships.
Various strategies for facilitating effective communication
Several primary care physicians and nurses emphasized the significance of practical communication skills in explaining treatment decisions, particularly the decision not to prescribe antibiotics (Bergsholm et al., 2023a; Courtenay et al., 2017; Sköld et al., 2017). Effective communication involved using precise language, providing clear information, and addressing potential misunderstandings, regardless of the healthcare professional’s background (Alkirawan et al., 2022; Bergsholm et al., 2023b; Fletcher-Lartey et al., 2016; Lum et al., 2017). Various strategies were reported, such as creating a more inclusive and supportive environment, bridging gaps in patient understanding, and using informal language (Bergsholm et al., 2023b; Guo et al., 2021). Addressing language barriers and providing both verbal and written information were also perceived as effective strategies for improving communication (Fletcher-Lartey et al., 2016; Laytner et al., 2023).
Primary care physicians frequently used clinical tools, such as C-reactive protein tests, to explain why antibiotics were unnecessary (Lescure et al., 2022; Özcebe et al., 2022). Pharmacists supported reduction of antibiotic misuse by providing clear instructions on dosages, explaining the risks of misuse, and offering non-antibiotic alternatives (Jones et al., 2018; Manderson, 2020; Om et al., 2017; Özcebe et al., 2022; Saleem et al., 2019; Sayood et al., 2021). Some pharmacists also asked follow-up questions to assess symptom severity and to guide or advise patients to see a physician (Mahmoud et al., 2018; Sayood et al., 2021). Some experienced primary care physicians also developed strategies such as ‘preparing the ground’, which involved taking a comprehensive history, conducting thorough examinations, and communicating decisions empathetically (Lum et al., 2018). Medical histories and clinical examinations also played a crucial role in explaining why antibiotics were not prescribed, demonstrating that decisions were made with patients’ best interests in mind while fostering trust and managing expectations (Lum et al., 2018; Manderson, 2020).
Primary care physicians, pharmacists and nurses emphasized the risks associated with overusing antibiotics, storing leftover medications, self-medicating, and stopping treatment prematurely. They also reassured patients about viral illnesses and normalized infections and encouraged self-management to reduce unnecessary antibiotic use (Anderson et al., 2019; Biezen et al., 2017; Boaitey et al., 2023; Boiko et al., 2020; Saliba-Gustafsson et al., 2021; Yates et al., 2018). Many primary care physicians and nurses viewed running commentary and acknowledging patients’ illnesses during consultations as crucial to reduce unnecessary antibiotic use (Mustafa et al., 2014; Williams et al., 2018). This was perceived as an important help to adjust patients’ preconceived notions about the necessity of antibiotics (Mustafa et al., 2014). Both primary care physicians and pharmacists emphasized the absence of bacterial symptoms (Bergsholm et al., 2023b; Colliers et al., 2020; Knobloch et al., 2021; Cabral et al., 2016; Mustafa et al., 2014; Sköld et al., 2017; Özcebe et al., 2022), which several patients recognized as a valuable effort to educate them and reinforce trust in the decision-making process (Brookes-Howell et al., 2014; Cabral et al., 2014).
Some primary care physicians used therapeutic guidelines on antibiotic use. However, more of them had had negative experiences using guidelines during the consultation, fearing that patients might judge them and believe they were unsure how to treat the condition (Boaitey et al., 2023). In contrast, patients reported a lack of sufficient ‘safety-netting advice,’ indicating that healthcare professionals did not provide enough information (Alhomoud et al., 2018; Alkadhimi et al., 2020; Alzard et al., 2024; Boiko et al., 2020; Colliers et al., 2020; Horwood et al., 2016; Kurotschka et al., 2024). Specifically, patients often felt the information was inadequate regarding the details of their infection, the rationale for not prescribing antibiotics, and the manner in which the information was conveyed (Bergsholm et al., 2023b; Cabral et al., 2014; Souto-López et al., 2020).
Different priorities and wishes for treatment
From primary care physicians’ perspectives, while empowered patients were more motivated to engage with and follow the information provided at the pharmacy (Alzard et al., 2024; Bergsholm et al., 2023a), some of them perceived that this level of involvement occasionally undermined trust in their professionality (Mustafa et al., 2014). However, in episodic care settings, where primary care physicians often lacked an established rapport with patients, time constraints and limited access to patient history further challenged their ability to confidently avoid unnecessary antibiotic prescriptions (Ryves et al., 2016; Simeoni et al., 2022). The unfamiliarity with the patients hindered effective patient education about the risks of antibiotics, often leading to a greater likelihood of issuing an antibiotic prescription (Colliers et al., 2020; Duane et al., 2016; Ryves et al., 2016; Simeoni et al., 2022). Moreover, the interpretation of patient histories, symptoms, and test results varied among primary care physicians, reflecting individualized strategies. Some primary care physicians also found it difficult to explain their antibiotic treatment choices, as these decisions were often based on instinct (Bisgaard et al., 2021).
Several primary care physicians, pharmacists and nurses reported that patients often expected antibiotics as a quick fix (Biezen et al., 2019; Bisgaard et al., 2021; Fletcher-Lartey et al., 2016; Horwood et al., 2016; Manderson, 2020; Res et al., 2017; Sharaf et al., 2021; van der Zande et al., 2019). Managing these multifaceted pressures required a range of strategies, with both primary care physicians and pharmacists relying on patient education to address misconceptions about antibiotic use. However, several primary care physicians, pharmacists and nurses also yielded to patient demands, especially when faced with persistent pressure or difficult consultations to avoid conflict (Biezen et al., 2017; Black et al., 2014; Courtenay et al., 2019; Fletcher-Lartey et al., 2016; Kaminsky et al., 2020; Kurotschka et al., 2024; Lum et al., 2018; Manderson, 2020; Mahmoud et al., 2018; Musoke et al., 2023; Res et al., 2017; Ryves et al., 2016; Saliba-Gustafsson et al., 2021). Primary care physicians, pharmacists and nurses often assumed that patients expected antibiotic prescriptions during consultations (Biezen et al., 2017; Boiko et al., 2020; Dallas et al., 2020; Kaminsky et al., 2020; Ryves et al., 2016; Saliba-Gustafsson et al., 2021; Sargent et al., 2017). While some professionals stated to be unaffected by this pressure (Saliba-Gustafsson et al., 2021), primary care physicians and nurses expressed feeling pressured to prescribe antibiotics for infections they did not consider requiring treatment (Arnau-Sánchez et al., 2023; Boaitey et al., 2023; Courtenay et al., 2019; Duane et al., 2016; Hu et al., 2024; Kurotschka et al., 2024; Lum et al., 2018; Mustafa et al., 2014; O'Doherty et al., 2019; van der Zande et al., 2019). Pharmacists reported similar challenges (Mahmoud et al., 2018; Jones et al., 2018), noting that patients frequently pressured pharmacists to dispense antibiotics, sometimes without a prescription. However, as Manderson (2020) highlighted, patients did not always seek antibiotics, indicating that healthcare professionals sometimes misjudged patients’ needs or failed to recognize the importance of patient education.
Social position made a difference
Power asymmetries in healthcare interactions were reported as an essential factor that affected both trust and robustness of the patient-professional relationship. Factors such as patient age, cultural background, comorbidities, and symptom severity were stated by professionals to contribute to increased antibiotic prescribing in, for example, episodic care settings (Simeoni et al., 2022). Language and cultural barriers complicated the efforts to educate patients about proper antibiotic use, especially in multicultural settings where communication challenges were common (Colliers et al., 2018; Hu et al., 2024; Lescure et al., 2022; Peiffer-Smadja et al., 2020). Primary care physicians often found it challenging to explain the importance of appropriate antibiotic use, mainly when they encountered patients who had poor language skills, low literacy or cultural differences (Duane et al., 2016; Fletcher-Lartey et al., 2016; Lescure et al., 2022). Primary care physicians, pharmacists and nurses acknowledged that specific training in handling difficult situations and patient conversations could enhance communication and reduce misunderstandings (Ashdown et al., 2016; Biezen et al., 2017; Guo et al., 2021; Lum et al., 2018; Mustafa et al., 2014; Poss-Doering et al., 2020; Raspopovic et al., 2016; Res et al., 2017).
From the patients’ perspectives, a lack of commitment or attentiveness from primary care physicians often undermined trust (Cabral et al., 2014; Grigoryan et al., 2022; Zago et al., 2023). Patients expressed a sense of distrust stemming from the perceived lack of personal commitment from some primary care physicians, who appeared uncaring and inattentive during consultations, marked by minimal eye contact and engagement (Cabral et al., 2014; Zago et al., 2023). Additionally, some pharmacists felt that asking too many diagnostic questions was undesirable, as it could make patients perceive them as uncertain or unqualified (Hoang et al., 2024). In some cases, from patients’ perspective, primary care physicians responded to patients’ questions with dismissive remarks, such as questioning patients’ desire for more information (Gautham et al., 2024). Moreover, an absence of explicit discussion around repeated antibiotic prescriptions by primary care physicians could lead to patients’ distrust (Halls et al., 2017; Hika et al., 2022; Lum et al., 2017). This distrust could sometimes hinder patients’ receptiveness to the information provided (Bergsholm et al., 2023a). Some patients trusted pharmacists more than primary care physicians, viewing pharmacists as impartial, affordable healthcare professionals and the most knowledgeable in medication-related matters (Alhomoud et al., 2018; Mortazhejri et al., 2020). However, other patients perceived pharmacists more as ‘shopkeepers’ than qualified healthcare professionals, which could undermine their role in antibiotic stewardship (Darj et al., 2019).
Organizational structures challenged professionals in guiding and educating patients
Time is money, and vice versa
Primary care physicians, pharmacists, nurses, and patients recognized the urgent need for systemic changes to enhance antibiotic stewardship (Black et al., 2014; Courtenay et al., 2019; Horwood et al., 2016; Manderson, 2020). The practical challenges faced by healthcare professionals in primary care settings significantly affected their ability to effectively educate patients about antibiotic use and AMR (Bosley et al., 2021; Courtenay et al., 2019; Guo et al., 2021; Manderson, 2020; Mas-Dalmau et al., 2023; Peiffer-Smadja et al., 2020; Sharaf et al., 2021; Williams et al., 2018; Yates et al., 2018). These challenges primarily stem from a lack of resource allocation within the healthcare system and time constraints, which hindered the implementation of practices aimed at improving the management of antibiotic prescribing and dispensing (Biezen et al., 2019; Courtenay et al., 2019; Mas-Dalmau et al., 2023; Peiffer-Smadja et al., 2020).
In time-pressured environments, many primary care physicians perceived shared decision-making as too time-consuming, particularly when a more significant number of treatment options needed to be discussed (Alkadhimi et al., 2020; Alzard et al., 2024; Bergsholm et al., 2023a; van Horrik et al., 2024). Time pressures were particularly intense during peak consultation periods or at the end of the week, restricting educational opportunities for physicians and patients (Guo et al., 2021; Kurotschka et al., 2024). Moreover, in some countries such as South Africa, long journeys to clinics and crowded conditions impeded patients’ access to follow-up care and proper education, leading to increased antibiotic use (van Hecke et al., 2019b). Often primary care physicians and nurses managed a high volume of patients each day, which forced them to rely on providing written information to save time during consultations. Nevertheless, some healthcare professionals expressed concern that offering only written information may limit the effectiveness of the educational message reaching patients (Boiko et al., 2020). Furthermore, from nurses’ perspective, time constraints during consultations often led to a focus on advising patients to take prescribed antibiotics without adequately addressing essential topics such as antibiotic resistance or self-care (Manderson, 2020). Patients often perceived rushed consultations as unhelpful, leading them to struggle with understanding essential treatment details such as dosage, duration, and appropriate antibiotic use (Cox et al., 2023; Gautham et al., 2024; Zago et al., 2023).
Less experienced professionals and those working in high-pressure environments were particularly prone to over-prescribing antibiotics (Ryves et al., 2016; Sundvall et al., 2020). Some primary care physicians and nurses opted to prescribe antibiotics as a quicker solution than not doing it, especially when they were running behind schedule or facing a high volume of patients (Biezen et al., 2017, 2019; Brisley et al., 2023; Guo et al., 2021; Kurotschka et al., 2024; Lescure et al., 2022; van der Zande et al., 2019). Discussions about risks and benefits of antibiotics were often limited, and some patients reported that primary care physicians did not always provide essential information regarding the administration of antibiotics or potential adverse reactions (Lum et al., 2017; Manderson, 2020; Mas-Dalmau et al., 2023; Mortazhejri et al., 2020). This lack of education left patients dissatisfied with the consultation and uncertain about when antibiotics were appropriate, contributing to confusion and frustration (Brookes-Howell et al., 2014; Gaarslev et al., 2016; Halls et al., 2017; Laytner et al., 2023; Lipstein et al., 2019; Sychareun et al., 2022; van Hecke et al., 2019a). Pharmacists often faced pressure to provide quick solutions after doctor consultations, leaving little time to assess antibiotic treatments or educate patients on proper use (Alzard et al., 2024). This challenge was especially acute in low-resource settings, where limited healthcare access led patients to rely on pharmacists or informal sources, prioritizing rapid dispensing over patient education (Suy et al., 2019).
The structure of the healthcare system, particularly in private sector settings, introduced another layer of complexity to antibiotic stewardship. A notable conflict existed between financial incentives and the goal of appropriate antibiotic use. Pharmacists often balanced patient numbers and sales targets, which sometimes led to inappropriate dispensing and prescribing of antibiotics, hence prioritizing profitability over patient education (Alkadhimi et al., 2020; Alhomoud et al., 2018; Musoke et al., 2023; Saleem et al., 2019; Salim and Elgizoli, 2017). The commercial pressure to increase sales, therefore, undermined their ability to focus on patient education and AMR prevention (Alkadhimi et al., 2020; Amin et al., 2017; Salim and Elgizoli, 2017; Torres et al., 2020). In some primary care practices with more resources, such as extended consultation times and triage systems, physicians could reduce unnecessary antibiotic prescriptions by educating patients about alternative treatments. However, in some private clinics, the pressure of paid consultations made it challenging for primary care physicians to refuse requests for antibiotics. They felt obligated to provide ‘value’ to private patients who paid a premium, further complicating efforts to educate patients about appropriate antibiotic use (O'Doherty et al., 2019).
Technical and educational tools at stake
Several primary care physicians, pharmacists, and nurses believed that handouts and posters could effectively educate patients about unnecessary antibiotics for acute bronchitis. However, some remain skeptical about their effectiveness (Dempsey et al., 2014; Tonna et al., 2020). Pharmacists pointed out that well-intentioned awareness campaigns, such as European Antibiotic Awareness Day, often fail due to information overload, which hinders prescribers and pharmacists from delivering clear and impactful educational messages (Tonna et al., 2020). Patients expressed a desire for more comprehensive information, highlighting that gaps in communication from healthcare professionals lead to changes in how antibiotics are prescribed (BrookesHowell et al., 2014). Additionally, patients wanted primary care physicians to take a more proactive role in antibiotic stewardship (Lum et al., 2017). In contrast, some primary care physicians viewed their involvement in antibiotic stewardship as non-essential, feeling compelled to prescribe (Ghiga et al., 2023) and influenced by the limited use of guidelines (Arnau-Sánchez et al., 2023).
Several primary care physicians refrained from using decision aids to educate patients, citing concerns that these tools might prolong consultations and disrupt their schedules (Boaitey et al., 2023). They also acknowledged the limited education patients receive regarding antibiotics and antimicrobial resistance. To address this gap, they advocated for broader public education efforts, such as school programs, media campaigns, and other community initiatives, to enhance patient awareness on these critical topics (Arnau-Sánchez et al., 2023; O'Doherty et al., 2019; Özcebe et al., 2022). Digital tools were often limited by patients’ lack of digital literacy (Lescure et al., 2022). Existing educational materials were reported not to meet patients’ specific needs. Furthermore, insufficient educational materials tailored to specific patient groups further restricted effective communication and patient education among primary care physicians, pharmacists, and nurses (Fletcher-Lartey et al., 2016; Kaminsky et al., 2020; Manderson, 2020; Sharaf et al., 2021). The absence of adequate IT infrastructure, such as electronic links between physicians and other healthcare professionals, also contributed to defensive prescribing practices (Saliba-Gustafsson et al., 2021). To address this issue, some primary care physicians utilized resources like ‘Choosing Wisely’ pamphlets, which support non-antibiotic alternatives and help reassure patients that their symptoms are being taken seriously (Simeoni et al., 2022). However, some pharmacists pointed out that outdated guidelines complicated their ability to stay informed about antimicrobial treatments, leading them to rely on various online platforms, like Google and Medscape, or to consult drug leaflets (Jakupi et al., 2019; Musoke et al., 2023).
Lack of collaboration - a professional hierarchy
Pharmacists emphasized the importance of correct antibiotic use and education in combating antimicrobial resistance (Alhomoud et al., 2018; Alzard et al., 2024; Bergsholm et al., 2023b; Peiffer-Smadja et al., 2020; Res et al., 2017; Sayood et al., 2021). However, pharmacists often encountered patients seeking clarification on issues not fully explained during consultations with primary care physicians. These issues included the reasons for delayed prescriptions and the appropriate dosage and timing of antibiotics (Bergsholm et al., 2023b; Jakupi et al., 2019; Sayood et al., 2021). Consequently, many pharmacists viewed themselves as crucial in educating patients about antibiotic use. They frequently served as the first point of contact for advice on proper usage, potential side effects, and treatment adherence.
Additionally, socioeconomic factors greatly influenced how pharmacists educated patients about antibiotics. Financial constraints often led low-income patients to request fewer antibiotics or seek them without a prescription. Some pharmacists noted that these patients frequently turn to them for advice instead of consulting a physician (Saleem et al., 2019; Salim and Elgizoli, 2017). However, pharmacists’ ability to educate patients was often hindered by limited access to patients’ medical histories, which prevented them from making well-informed decisions about the appropriateness of prescribed antibiotics (Atif et al., 2020; Jones et al., 2018; Khan et al., 2021; Peiffer-Smadja et al., 2020; Sayood et al., 2021). Additionally, many pharmacists encountered communication barriers with primary care physicians, which further limited their ability to support antibiotic stewardship initiatives (Atif et al., 2020; Khan et al., 2021). In contrast, nurses had limited influence on prescribing decisions, as physicians held the final authority in cases such as managing respiratory tract infections. However, nurses frequently encouraged patients to ask their primary care physician about the rationale behind antibiotic prescriptions and offered guidance on managing symptoms without the use of antibiotics (Biezen et al., 2017). From the perspective of primary care physicians, on the other hand, pharmacists’ educational advice regarding antibiotics could conflict with their own guidance, potentially confusing patients (Bergsholm et al., 2023a). Several primary care physicians expressed concerns that pharmacists might exceed their role by providing information beyond what was discussed during consultations. They preferred that pharmacists focus on dispensing medications rather than engaging in clinical discussions with patients (Bergsholm et al., 2023b).
Delayed prescription as a tool to balance all demands
When time constraints, follow-up appointments, and collaborative relations were challenging, primary care physicians often felt pressured to prescribe antibiotics as a precaution (Manderson, 2020; Ryves et al., 2016). The practice of issuing delayed prescriptions, in which healthcare professionals such as primary care physicians or nurses provide a prescription for antibiotics but advise patients to wait a specified period before filling it, has become a common yet complex approach (Biezen et al., 2017; Lum et al., 2017, 2018; McDermott et al., 2017; O'Doherty et al., 2019; Poss-Doering et al., 2020; Ryves et al., 2016; Saliba-Gustafsson et al., 2019; Sargent et al., 2017; van der Zande et al., 2019). Both primary care physicians and nurses reported that delayed prescriptions aimed to encourage patients to follow medical advice, thereby granting them greater control over their treatment plans (Boiko et al., 2020; Dallas et al., 2020; Duane et al., 2016; Fletcher-Lartey et al., 2016; Horwood et al., 2016; Lum et al., 2018; Ryves et al., 2016; Saliba-Gustafsson et al., 2019; Sargent et al., 2017).
Variations in prescribing practices among primary care physicians often resulted in patients receiving conflicting advice, making it harder to understand when antibiotics are necessary (Lum et al., 2018; McDermott et al., 2017). Some primary care physicians noted that inconsistent messaging confuses patients and limited opportunities to educate them about respiratory infections (Ryves et al., 2016). Delayed prescriptions or granting patients complete decision-making autonomy were often suggested for specific individuals, based on their ability to understand the strategy (Mas-Dalmau et al., 2023; Ryves et al., 2016; Saliba-Gustafsson et al., 2019). However, many patients expressed discomfort with deciding whether to use antibiotics, preferring to have the physician make that decision instead (Lum et al., 2017), indicating that these strategies were not always effective or productive.
Some primary care physicians acknowledged that they prescribed delayed antibiotics despite weak evidence and concerns regarding misuse or the potential for missing severe infections (Lum et al., 2018; Ryves et al., 2016; Sargent et al., 2017). Additionally, some pharmacists dispense antibiotics without a prescription when patients requested them by name, assuming these patients were knowledgeable about their appropriate use (Mahmoud et al., 2018). Moreover, several primary care physicians pointed out that delayed prescriptions could lead to inappropriate antibiotic use, with patients either storing antibiotics for future use or taking them immediately (Sargent et al., 2017). Nevertheless, diagnostic uncertainty and lack of time led many primary care physicians to prescribe antibiotics ‘just in case’ rather than educating patients on appropriate usage (Biezen et al., 2019; Saliba-Gustafsson et al., 2021; Sayood et al., 2021). Consequently, delayed prescriptions were viewed as a strategy to alleviate professional insecurity and avoid the risk of neglecting to prescribe antibiotics for severe infections (Dallas et al., 2020; Lum et al., 2018; O'Doherty et al., 2019; Ryves et al., 2016; Saliba-Gustafsson et al., 2021; Sargent et al., 2017).
Discussion
The discussion will focus on three main findings: the importance of relationships between healthcare professionals and patients in facilitating successful patient education about antibiotic use and AMR, the structural challenges that often hindered healthcare professionals from providing detailed education to patients, and the use of delayed prescriptions to balance the improvement of AMR stewardship and met patients’ expectations for antibiotic treatment.
The results showed that strong relationships between healthcare professionals and patients are vital for effective patient education on antibiotic use and AMR. Trust and effective communication were consistently identified as key in ensuring patients feel understood and informed. Primary care physicians, pharmacists, and nurses each play distinct roles in fostering trust, which could encourage patients to follow advice regarding antibiotics. When patients trusted healthcare professionals, they were more likely to accept not receiving unnecessary antibiotics. These findings contribute to the existing literature (Gulliford et al., 2021; Jorgoni et al., 2022) by emphasizing the importance of relationship-building as a central component of antibiotic stewardship rather than focusing solely on medical interventions. This trust-building process is essential in overcoming patient expectations for antibiotics and can significantly influence patient engagement in antibiotic stewardship efforts. Moreover, actively involving patients in conversations about antibiotic use and respecting their preferences can foster a sense of shared decision-making, which is associated with increased patient engagement and better health outcomes (Elwyn et al., 2012; Santana et al., 2018). Such a perception aligns with the idea about person-centered care, which emphasizes the importance of acknowledging patients’ concerns and experiences to build trust (Ekman and Swedberg, 2022; Ridd et al., 2009; Santana et al., 2018). However, the findings also revealed significant challenges in building trust, especially in the context of power dynamics within healthcare settings. The findings indicated that the hierarchical nature of healthcare interactions, where physicians and pharmacists hold positions of authority, could hinder open communication with patients. This power imbalance was found to affect both the trust patients have in healthcare professionals and the effectiveness of educational efforts. In line with Bourdieu’s concept of cultural and symbolic capital (Bourdieu, 1984), the study’s findings suggest that healthcare professionals’ authority can create an asymmetry in patient interactions, reducing opportunities for shared decision-making and undermining the patient’s active role in their treatment. This contrasts with the person-centered approach that the study highlights as being essential for better patient engagement in AMR stewardship. The current study not only confirmed the importance of trust but also revealed how structural and power dynamics within healthcare settings, rooted in the biomedical perspective, may limit the achievement of successful patient education and antibiotic stewardship. These findings resonate with Foucault’s concept of the ‘medical gaze,’ which suggests that the dominance of healthcare professionals’ authority often reframes patient narratives to fit within a biomedical framework, overlooking non-biomedical dimensions of their experiences (Foucault, 2003). Such power dynamics can reduce patients’ agency, thereby affecting the trust required for successful patient education on antibiotics and AMR. In healthcare contexts, patient encounters tend to be more ‘medical/professional-oriented’ than ‘patient/person-oriented’ as they prioritize diagnosing and prescribing over a holistic approach, leading to an asymmetric power structure in primary healthcare (Misselbrook, 2013; Glasdam et al., 2020).
The results showed that pharmacists who adopted informal communication styles were more successful in building relationships with patients, where inconsistent communication between primary care physicians and pharmacists complicated these dynamics. This inconsistency in information exchange regarding antibiotic treatments could undermine patients’ confidence, creating confusion about treatment plans and antibiotic use. Previous literature suggests that this could stem from differing professional positions, roles and responsibilities, and a lack of collaboration between healthcare professionals, highlighting the need for a unified approach to antibiotic stewardship (Balea and Glasdam, 2024; Reeves et al., 2017). Moreover, in line with previous literature, collaboration is embedded in hierarchical structures (Essex et al., 2023). The issue of perceived power asymmetry raises questions about whether healthcare professionals always recognize the impact of their authority on patient interactions. Previous literature shows that failing to address patients’ concerns may diminish trust (Epstein and Street, 2011). This could explain why some patients were less receptive to educational messages about antibiotic use and AMR stewardship, as highlighted in our findings. This study is, however, limited by its lack of focus on patients’ attitudes, knowledge levels, and cultural values. Stewart et al. (2022) argue that patient adherence is influenced by both motivation and ability. Some studies highlight that many young people are inadequately informed about antibiotic treatment and antimicrobial resistance (AMR), often perceiving antibiotics as a universal remedy and demonstrating limited understanding of the differences between viral and bacterial infections (Crago et al., 2022; Hawking et al., 2017). Conversely, other studies suggest that attitudes towards antibiotic treatments and AMR prevention are not necessarily age-dependent (e.g., Zaykova et al., 2022) but are instead shaped by cultural and social factors (Dionisio et al., 2023; Minnssen et al., 2020). This underscores the need for future research to adopt relational perspectives on antibiotic treatment and AMR stewardship, focusing on interactions between healthcare professionals and patients from both perspectives.
The results mainly focused on primary care physicians working as primary care physicians’ and pharmacists’ patient education about antibiotics and AMR. The literature searches did not identify any publications that addressed nurses’ patient education about antibiotic treatment or AMR stewardship in home care and nursing home settings, which are significant areas within primary care. In primary care, including nursing homes, nurses meet patients with infections, treated with antibiotics or not (Alberg et al., 2017; Tark et al., 2020). The current review only found studies about nurses’ patient education concerning prescription. However, follow-up education during treatment and AMR preventive initiatives may also be important tasks for nurses in primary care, which calls for future studies. Nurses, among other healthcare professionals, play a major role when it comes to the spreading of infections and the development/stewardship of AMR (Glasdam et al., 2021; Singh et al., 2022), as they act as carriers and thereby transmit resistant bacteria to patients (Fracarolli et al., 2017; de Oliveira et al., 2012).
Furthermore, the results suggested that structural challenges, such as time pressures, heavy workloads, and the commercial nature of pharmacies and general practices, often hinder healthcare professionals from providing detailed patient education, leading to gaps in understanding of both treatment and prevention of AMR. Time constraints are among the most significant barriers healthcare professionals face today (Kasse et al., 2024; Lansink et al., 2024), directly impacting professionals’ ability to provide comprehensive patient education about antibiotic use (Bosley et al., 2018). As the current results showed, primary care physicians often managed large numbers of patients daily, leaving insufficient time for thorough conversations about whether antibiotics were necessary for a given condition. Consequently, patients may not fully understand why antibiotics are being withheld, leading to frustration or demands for unnecessary prescriptions. The desire to increase patient turnover, in line with commercial goals, was evident in the current results, limiting the duration and quality of consultations. Pharmacists in commercially driven settings faced the dual challenge of high patient demand and the pressure to maintain profitability. While pharmacists were tasked with counselling patients on safe medication use, including antibiotics, their ability to provide detailed guidance was compromised by the need to meet sales targets. The prioritization of profitability over patient care may lead to less time spent educating patients about the risks of antibiotic misuse (Balea and Glasdam, 2024). In such profit-oriented environments, the commercial pressures conflict with the professional responsibility as healthcare professionals may feel driven to maximize income at the expense of providing adequate patient education (Balea and Glasdam, 2024; Saleh et al., 2021). The pursuit of financial success, therefore, further complicates efforts to combat AMR, as pharmacists and primary care physicians may be incentivized to prioritize sales/number of consultations over detailed patient education.
Moreover, the global shortage of primary care physicians exacerbates this problem. In many parts of the world, the demand for healthcare professionals far exceeds supply, resulting in overwhelmed primary care physicians who must see more patients in less time (Shen et al., 2020; Velgan et al., 2023). This shortage amplifies the pressures to balance patient care with business success, particularly in private practices where primary care physicians must manage the financial sustainability of their operations. The drive to earn more money can increase patient throughput, limiting the time available for important discussions about antibiotic use and AMR prevention.
These findings underscore the persistent tension between the demands of efficient healthcare delivery and the ethical responsibility to provide thorough patient care, which can lead to unnecessary prescriptions and contribute to the AMR crisis (Cutrell and Sanders, 2024; Pokharel et al., 2024). The findings highlight a central challenge in modern healthcare: balancing the commercial aspects of healthcare provision with the moral obligation to uphold the principles of the Hippocratic Oath as interpreted in the Geneva Declaration (World Medical Association, 2017) and the medical ethical principle, especially the duty to ‘do no harm’ (Varkey, 2021). This tension is particularly evident in the context of AMR and the roles of primary care physicians and pharmacists in ensuring proper antibiotic stewardship. At the heart of this dilemma is also the desire of healthcare professionals to achieve financial success in their business (Noor et al., 2022). The conflict between profitability and patient care invites reflection on how healthcare systems might address the balance so as not to harm the patient in the first instance, and society at large by contributing to the development of AMR. However, the current findings also revealed that some primary care physicians and pharmacists were able to educate patients under the existing structural framework.
The results revealed the use of delayed prescriptions to balance the improvement of AMR stewardship and meeting patients’ expectations for antibiotic treatment. Traditionally, physicians are the primary decision-makers and prescribers in antibiotic therapy (Carlsson et al., 2023). However, findings revealed a role inversion, shifting the basis of antibiotic stewardship from the expert, alias the physician, to the patient, thereby diminishing the professional autonomy, pointing to a form of de-professionalization of medicine (Engelhardt, 2002). This suggests that, in their efforts to maintain professional authority, physicians often rely on personal judgement, allowing external factors, such as patient preferences and concerns about risks of bacterial infection, to influence their decisions regarding antibiotic stewardship (Kasse et al., 2024; Lansink et al., 2024). This trend reflects broader challenges within healthcare, such as diagnostic uncertainties and time constraints, which can complicate the decision-making processes. While delayed prescriptions aim to reduce unnecessary antibiotic use, they also raise concerns about whether this approach may undermine professional responsibility and the authority of healthcare professionals in ensuring optimal antibiotic stewardship (Mcleod et al., 2024).
Davari et al. (2018) state that, in practice, physicians’ prescribing decisions are influenced by numerous factors, including clinical uncertainties, comorbidities, and patient expectations. When faced with unclear diagnoses or fear of complications, physicians may shift from clinical guidelines to a more individualized approach, as Md Rezal et al. (2015) demonstrate, despite acknowledging guidelines, many physicians deviate due to pressures like patient demands or diagnostic uncertainty. Similarly, McCullough et al. (2017) found a gap between guideline recommendations and actual prescribing rates, particularly for respiratory infections. Not all healthcare settings universally provide or follow detailed guidelines, as their availability often depends on the healthcare system’s resources (Balea and Glasdam, 2024; Gu et al., 2022). Even when available, guidelines may not always be the most appropriate solution in every clinical scenario (Pouwels et al., 2019). To address these challenges, it is essential to maintain an up-to-date knowledge base and develop robust patient-provider relationships along with person-centered communication strategies. These measures may support both healthcare professionals and patients in making qualified and informed decisions about when antibiotics are truly necessary. Ultimately, such approaches could enhance efforts to prevent AMR at both individual and societal levels. Moreover, Spurling et al. (2017) warn that inconsistencies in antibiotic stewardship, reducing the effectiveness of evidence-based practices in managing AMR, risks weakening the overall efforts to maintain a clear and effective strategy against AMR, locally, nationally, and internationally. Hence, the current study calls for re-evaluation and development of healthcare policies prioritizing commercial interests and financial success over patient care, ensuring that ethical standards remain central to healthcare provision generally and specifically in relation to antibiotic treatment and AMR stewardship in primary care settings.
Finally, the current study’s method has strengths and limitations. The study’s multifaceted approach enhances the analysis and fosters a more robust, effective, and sustainable understanding of how professionals educate patients about antibiotic treatment and the prevention of AMR. The review was conducted following the PRISMA 2020 guidelines, ensuring a transparent, thorough, and accurate presentation of the methods, which supports the assessment of its quality (Garcia-Doval et al., 2017; Page et al., 2021). Additionally, the review was pre-registered on PROSPERO, providing access to the protocol and enabling a comparison between the registered elements and the final manuscript, thereby enhancing transparency (Schiavo, 2019). The construction of the search strings yielded a high volume of hits. The Boolean operator ‘NOT’ was deliberately avoided to prevent the exclusion of potentially relevant studies. As a result, filters for terms such as hospital*, quantitative stud* and dental care were not applied. Consequently, an extensive manual screening was required to identify the relevant articles. The systematic search was conducted with the support of an experienced university librarian to retrieve the most relevant and comprehensive literature aligned with the study’s aim, ensuring a systematic and transparent process. The screening process, data extraction and analysis were carried out alongside regular evaluations and discussions among all authors, further enhancing the study’s credibility. The included studies were assessed as being of moderate to high quality using the CASP qualitative study checklist, ensuring the findings’ credibility and relevance to the review’s aim. However, the chosen checklist can be criticized for not including a question regarding the studies’ underlying theoretical, ontological, and epistemological framework, which is also essential for assessing the quality of the studies (Long et al., 2020). Another limitation of the current study is that the review only included studies published in English, Scandinavian or Romanian, potentially excluding valuable perspectives presented in other languages. While the representation of 38 different countries in this study is a strength, the selected language may limit the transferability of the findings to other contexts. Furthermore, the limitations identified in the included studies, such as small sample sizes and unspecified healthcare professionals, are also considered limitations in the current literature review. A limitation is also the variation in national regulations on antibiotic use across the included studies. Different prescribing practices and antibiotic stewardship policies can affect the results, making it harder to compare findings and apply them to regions with different regulations.
Conclusion
Focusing on primary care settings, the findings of this systematic review highlighted the complexity healthcare professionals face in educating patients about antibiotic use and AMR, with each profession—physicians, pharmacists, and nurses encountering unique challenges. These challenges went beyond the clinical levels, involving relational, social and personal levels. While many physicians focused on building trust and shared decision-making, although struggling with time constraints and patient expectations, pharmacists often played a key role in providing accessible advice. However, they were limited by commercial pressures and a lack of patient medical history, which impacted their ability to offer thorough education. Nurses, though less involved in prescribing, were essential in reinforcing antibiotic treatments. Relationally, the interactions between healthcare professionals and patients/other healthcare professionals were influenced by power dynamics, trust issues, and inconsistent communication. These factors often hindered the effectiveness of educational efforts regarding antibiotic use and AMR stewardship. Moreover, many patients felt dissatisfied when the provided consultations were rushed, or their questions remained unanswered, which could lead to confusion and possible misuse of antibiotics. In primary care, physicians, pharmacists and nurses operated within structural frameworks influenced by time pressures, heavy workloads, and commercial demands, limiting their capacity to provide detailed patient education. These demands made it difficult for them to meet their ethical responsibilities. On a personal level, they faced the challenge of acting on behalf of patients’ health while also managing the fear of losing patients or being perceived negatively if they did not prescribe antibiotics, even when they were aware it was not medically necessary.
Although often articulated as the most important act against the AMR crisis, this study demonstrated that providing adequate education on antibiotic use and AMR was not a straightforward path with simple solutions. Instead, it required acknowledging the multifaceted challenges that physicians, pharmacists and nurses faced on a daily basis. The complexity of these relational, social, and personal factors meant that there was no ‘quick fix’ through the implementation of evidence-based interventions alone. Future research and policymaking should focus on understanding these dynamics and creating environments that better support healthcare professionals in educating patients and tackling AMR. Given the limited research on nurses identified in this study, future studies should focus on the role of this professional group in antibiotic stewardship.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
LB: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. RG: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. HX: Writing – original draft, Writing – review & editing, Conceptualization, Methodology. SG: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Formal analysis, Project administration, Supervision.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank Krister Aronsson (Librarian at support for research and learning, Library & ICT, Faculty of Medicine, Lund University) for his dedicated assistance and work in designing and performing the literature searches.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alberg T., Holen Ø., Blix H. S., Lindbæk M., Bentele H., Eriksen H. M. (2017). Antibiotic use and infections in nursing homes. Antibiotikabruk og infeksjoner i sykehjem. Tidsskrift den Norske laegeforening: Tidsskrift Praktisk Medicin 137, 357–361. doi: 10.4045/tidsskr.16.0621
Alhomoud F., Almahasnah R., Alhomoud F. K. (2018). You could lose when you misuse" - factors affecting over-the-counter sale of antibiotics in community pharmacies in Saudi Arabia: A qualitative study. BMC Health Serv. Res. 18, 915. doi: 10.1186/s12913-018-3753-y
Alkadhimi A., Dawood O. T., Hassali M. A. (2020). Dispensing of antibiotics in community pharmacy in Iraq: A qualitative study. Pharm. Pract. (Granada) 18, 2095. doi: 10.18549/PharmPract.2020.4.2095
Alkirawan R., Kawous R., Bloemen E., van den Muijsenbergh M., Goosen S., Suurmond J., et al. (2022). Perspectives of Syrian refugees on antibiotic use and prescribing in Dutch primary care: a qualitative study. Int. J. Migration Health Soc. Care 18, pp.153163. doi: 10.1108/IJMHSC-12-2021-0112
Alves P. G., Hayward G., Leydon G., Barnes R., Woods C., Webb J., et al. (2021). Antibiotic prescribing in UK out-of hours primary care services: A realist-informed scoping review of training and guidelines for healthcare professionals. BJGP Open 5, BJGPO.2020.0167. doi: 10.3399/BJGPO.2020.0167
Alzard S., Wen J., Huynh N. P. Q., Shirkhanzadeh S., Tso J. Y., Rabino M., et al. (2024). Opportunities and barriers to pediatric antimicrobial stewardship by community pharmacists. J. Pediatr. Infect. Dis. Soc. 13, pp.313–pp.316. doi: 10.1093/jpids/piae039
Amin M. E. K., Amine A., Newegy M. S. (2017). Perspectives of pharmacy staff on dispensing subtherapeutic doses of antibiotics: A theory-informed qualitative study. Int. J. Clin. Pharm. 39, 1110–1118. doi: 10.1007/s11096-017-0510-y
Anderson E. C., Kesten J. M., Lane I., Hay A. D., Moss T., Cabral C. (2019). Primary care clinicians' views of pediatric respiratory infection surveillance information to inform clinical decision making: A qualitative study. BMJ Pediatr. Open 3, e000418. doi: 10.1136/bmjpo-2018000418
Andersson M., Schulze K., Cassini A., Plachouras D., Mossialos E. (2019). A governance framework for development and assessment of national action plans on antimicrobial resistance. Lancet Infect. Dis. 19, e371–e384. doi: 10.1016/S1473-3099(19)30415-3
Antimicrobial Resistance Collaborators (2022). Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 399, 629–655. doi: 10.1016/S01406736(21)02724-0
Aponte-González J., González-Acuña A., Lopez J., Brown P., Eslava-Schmalbach J. (2019). Perceptions in the community about the use of antibiotics without a prescription: Exploring ideas behind this practice. Pharm. Pract. 17, 1394. doi: 10.18549/PharmPract.2019.1.1394
Arnau-Sánchez J., Jiménez-Guillén C., Alcaraz-Quiñonero M., Vigueras-Abellán J. J., GarnicaMartínez B., Soriano-Ibarra J. F., et al. (2023). Factors influencing inappropriate use of antibiotics in infants under 3 years of age in primary care: A qualitative study of the pediatricians' perceptions. Antibiotics 12, 727. doi: 10.3390/antibiotics12040727
Ashdown H. F., Räisänen U., Wang K., Ziebland S., Harnden A. (2021). Prescribing antibiotics to 'at-risk' children with influenza-like illness in primary care: qualitative study. BMJ Open 6, e011497. doi: 10.1136/bmjopen-2016-011497
Atif M., Asghar S., Mushtaq I., Malik I. (2020). Community pharmacists as antibiotic stewards: A qualitative study exploring the current status of Antibiotic Stewardship Program in Bahawalpur, Pakistan. J. Infection Public Health 13, 118–124. doi: 10.1016/j.jiph.2019.07.003
Balea L. B., Glasdam S. (2024). Practices, strategies, and challenges in antibiotic treatment and prevention of antimicrobial resistance from the perspectives of Romanian community pharmacists and general practitioners. Front. Antibiotics 3. doi: 10.3389/frabi.2024.1439688
Bergsholm Y. K. R., Feiring M., Charnock C., Holm L. B., Krogstad T. (2023a). Exploring patients' adherence to antibiotics by understanding their health knowledge and relational communication in encounters with pharmacists and physicians. Exploratory Res. Clin. Soc. Pharm. 12, 100372. doi: 10.1016/j.rcsop.2023.100372
Bergsholm Y. K. R., Feiring M., Charnock C., Krogstad T., Holm L. B. (2023b). Positioning of community pharmacists in interactions with general practitioners and patients regarding prescribing and using antibiotics. J. Interprofessional Care 37, 886–895. doi: 10.1080/13561820.2023.2203698
Bettany-Saltikov J., McSherry R. (2016). How to do a systematic literature review in nursing: A step by-step guide. 2nd (London: Open University Press).
Biezen R., Brijnath B., Grando D., Mazza D. (2017). Management of respiratory tract infections in young children-A qualitative study of primary care providers' perspectives. NPJ Primary Care Respir. Med. 27, 15. doi: 10.1038/s41533-017-0018-x
Biezen R., Grando D., Mazza D., Brijnath B. (2019). Dissonant views - GPs' and parents' perspectives on antibiotic prescribing for young children with respiratory tract infections. BMC Family Pract. 20, 46. doi: 10.1186/s12875-019-0936-5
Bisgaard L., Andersen C. A., Jensen M. S. A., Bjerrum L., Hansen M. P. (2021). Danish GPs' experiences when managing patients presenting to general practice with symptoms of acute lower respiratory tract infections: A qualitative study. Antibiotics (Basel) 10, 661. doi: 10.3390/antibiotics10060661
Black E., Cartwright A., Bakharaiba S., Al-Mekaty E., Alsahan D. (2014). A qualitative study of pharmacists' perceptions of, and recommendations for improvement of antibiotic use in Qatar. Int. J. Clin. Pharm. 36, 787–794. doi: 10.1007/s11096-014-9960-7
Bless P. J., Muela Ribera J., Schmutz C., Zeller A., Mäusezahl D. (2016). Acute gastroenteritis and campylobacteriosis in Swiss primary care: The viewpoint of general practitioners. PloS One 11, e0161650. doi: 10.1371/journal.pone.0161650
Boaitey K. P., Hoffmann T., Baillie E., Bakhit M. (2023). Exploring general practitioners' perception of the value of natural history information and their awareness and use of guidelines' resources to support antibiotic prescribing for self-limiting infections: A qualitative study in Australian general practice. Aust. J. Primary Health 29, 558–565. doi: 10.1071/PY22258
Boiko O., Burgess C., Fox R., Ashworth M., Gulliford M. C. (2020). Risks of use and non-use of antibiotics in primary care: Qualitative study of prescribers' views. BMJ Open 10, e038851. doi: 10.1136/bmjopen-2020-038851
Bordado Sköld M., Aabenhus R., Guassora A. D., Mäkelä M. (2017). Antibiotic treatment failure when consulting patients with respiratory tract infections in general practice. A qualitative study to explore Danish general practitioners’ perspectives. Euro. J. General Practice 23, 121–128. doi: 10.1136/bmjopen-2020-038851
Bosley H., Henshall C., Appleton J. V., Jackson D. (2018). A systematic review to explore influences on parental attitudes towards antibiotic prescribing in children. J. Clin. Nurs. 27, e861–e885. doi: 10.1111/jocn.14266
Bosley H., Henshall C., Appleton J. V., Jackson D. (2021). Mixed methods case study exploring primary care antibiotic prescribing practices and maternal expectations of using antibiotics in children. Contemp. Nurse 57, 245–257. doi: 10.1080/10376178.2021.1994865
Bourdieu P. (1984). Distinction: A social critique of the judgement of taste (Cambridge, MA: Harvard University Press).
Braun V., Clarke V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Brisley A., Lambert H., Rodrigues C. (2023). Antibiotics in Catalan primary care: Prescription, use and remedies for a crisis of care. Med. Anthropology 42, 682–696. doi: 10.1080/01459740.2023.2256451
Brookes-Howell L., Wood F., Verheij T., Prout H., Cooper L., Hood K., et al. (2014). Trust, openness and continuity of care influence acceptance of antibiotics for children with respiratory tract infections: A four country qualitative study. Family Pract. 31, 102–110. doi: 10.1093/fampra/cmt052
Burnett E. (2018). Effective infection prevention and control: The nurse's role. Nurs. Standard 33, 68–72. doi: 10.7748/ns.2018.e11171
Cabral C., Ingram J., Hay A. D., Horwood J., TARGET team (2014). They just say everything's a virus"—Parents' judgment of the credibility of clinician communication in primary care consultations for respiratory tract infections in children: A qualitative study. Patient Educ. Couns. 95, 248–253. doi: 10.1016/j.pec.2014.01.010
Cabral C., Ingram J., Lucas P. J., Redmond N. M., Kai J., Hay A. D., et al. (2016). Influence of clinical communication on parents' antibiotic expectations for children with respiratory tract infections. Ann. Family Med. 14, 141–147. doi: 10.1370/afm.1892
Camerini F. G., Cunha T. L., Fassarella C. S., de Mendonça Henrique D., Fortunato J. G. S. (2024). Nursing strategies in antimicrobial stewardship in the hospital environment: A qualitative systematic review. BMC Nurs. 23, 147. doi: 10.1186/s12912-024-01753-y
Carlsson F., Jacobsson G., Lampi E. (2023). Antibiotic prescription: Knowledge among physicians and nurses in western Sweden. Health Policy 130, 104733. doi: 10.1016/j.healthpol.2023.104733
Center for Disease Dynamics, Economics and Policy (2015). State of the world’s antibiotic (Washington, D.C.: CDDEP).
Colliers A., Coenen S., Bombeke K., Remmen R., Philips H., Anthierens S. (2020). Understanding general practitioners' antibiotic prescribing decisions in out-of-hours primary care: A video elicitation interview study. Antibiotics (Basel) 9, 115. doi: 10.3390/antibiotics9030115
Colliers A., Coenen S., Remmen R., Philips H., Anthierens S. (2018). How do general practitioners and pharmacists experience antibiotic use in out-of-hours primary care? An exploratory qualitative interview study to inform a participatory action research project. BMJ Open 8, e023154. doi: 10.1136/bmjopen-2018-023154
Courtenay M., Rowbotham S., Lim R., Deslandes R., Hodson K., MacLure K., et al. (2017). Antibiotics for acute respiratory tract infections: A mixed-methods study of patient experiences of non-medical prescriber management. BMJ Open 7, e013515. doi: 10.1136/bmjopen-2016-013515
Courtenay M., Rowbotham S., Lim R., Peters S., Yates K., Chater A. (2019). Examining influences on antibiotic prescribing by nurse and pharmacist prescribers: A qualitative study using the Theoretical Domains Framework and COM-B. BMJ Open 9, e029177. doi: 10.1136/bmjopen-2019029177corr1
Cox S., Vleeming M., Giorgi W., Dinant G. J., Cals J., de Bont E. (2023). Patients' experiences, expectations, motivations, and perspectives around urinary tract infection care in general practice: A qualitative interview study. Antibiotics (Basel) 12, 241. doi: 10.3390/antibiotics12020241
Crago A.-L., Alexandre S., Abdesselam K., Tropper D. G., Hartmann M., Smith G., et al. (2022). Understanding Canadians’ knowledge, attitudes and practices related to antimicrobial resistance and antibiotic use: Results from public opinion research. Canada Communicable Dis. Rep. 48, 550–558. doi: 10.14745/ccdr.v48i1112a08
Critical Appraisal Skills Program (2018). CASP qualitative checklist. (Oxford). Available at: https://caspuk.net/casp-tools-checklists/ (Accessed August 20, 2024).
Cutrell J. B., Sanders J. M. (2024). How should clinicians navigate interprofessional tension in their roles as antimicrobial stewards? AMA J. Ethics 26, E441–E447. doi: 10.1001/amajethics.2024.441
Dallas A., Davey A., Mulquiney K., Davis J., Glasziou P., Van Driel M., et al. (2020). Delayed prescribing of antibiotics for acute respiratory infections by GP registrars: A qualitative study. Family Pract. 37, 406–411. doi: 10.1093/fampra/cmz079
Darj E., Newaz M. S., Zaman M. H. (2019). Pharmacists’ perception of their challenges at work, focusing on antimicrobial resistance: A qualitative study from Bangladesh. Global Health Action 12, p. doi: 10.1080/16549716.2020.1735126
Davari M., Khorasani E., Tigabu B. M. (2018). Factors influencing prescribing decisions of physicians: A review. Ethiopian J. Health Sci. 28, 795–804. doi: 10.4314/ejhs.v28i6.15
Dempsey P. P., Businger A. C., Whaley L. E., Gagne J. J., Linder J. A. (2014). Primary care clinicians' perceptions about antibiotic prescribing for acute bronchitis: A qualitative study. BMC Family Pract. 15, 194. doi: 10.1186/s12875-014-0194-5
de Oliveira A. C., Medeiros Silva M. D., Garbaccio J. L. (2012). Clothing of health care professional as potential reservoirs of micro-organisms: An integrative review. Texto Contexto Enfermagem 21, 684–691. doi: 10.1590/S0104-07072012000300025
Dionisio F., Baquero F., Fuertes M. (2023). Psychological and cultural factors influencing antibiotic prescription. Trends Microbiol. 31, 559–570. doi: 10.1016/j.tim.2022.12.010
Duane S., Domegan C., Callan A., Galvin S., Cormican M., Bennett K., et al. (2016). Using qualitative insights to change practice: Exploring the culture of antibiotic prescribing and consumption for urinary tract infections. BMJ Open 6, e008894. doi: 10.1136/bmjopen2015-008894
Durand C., Chappuis A., Douriez E., Poulain F., Ahmad R., Lescure F. X., et al. (2022). Perceptions, current practices, and interventions of community pharmacists regarding antimicrobial stewardship: A qualitative study. J. Am. Pharmacists Assoc. 62, 1239–1248.e1. doi: 10.1016/j.japh.2022.02.003
Ekman I., Swedberg K. (2022). “Person-centered care, theory, operationalization and effects,” in Intelligent systems for sustainable person-centered healthcare, vol. 205 . Eds. Kriksciuniene D., Sakalauskas V. (Springer, Cham). doi: 10.1007/978-3-030-79353-1_2
Elwyn G., Frosch D., Thomson R., Joseph-Williams N., Lloyd A., Kinnersley P., et al. (2012). Shared decision making: A model for clinical practice. J. Gen. Internal Med. 27, 1361–1367. doi: 10.1007/s11606-012-2077-6
Engelhardt H. T. (2002). “Managed care and the deprofessionalization of medicine,” in The ethics of managed care: Professional integrity and patient rights. Philosophy and Medicine, vol. 76 . Eds. Bondeson W. B., Jones J. W. (Springer). doi: 10.1007/978-94-017-0413-7_7
Epstein R. M., Street R. L. Jr. (2011). The values and value of patient-centered care. Ann. Family Med. 9, 100–103. doi: 10.1370/afm.1239
Essex R., Kennedy J., Miller D., Jameson J. (2023). A scoping review exploring the impact and negotiation of hierarchy in healthcare organizations. Nurs. Inq. 30, 1–10. doi: 10.1111/nin.1257
Essilini A., Pierre A., Bocquier A., Pulcini C., Wilcke C., Gravoulet J., et al. (2021). Community pharmacists' views on their current role and future opportunities for antibiotic stewardship: A French qualitative study. JAC Antimicrobial Resistance 3, dlab129. doi: 10.1093/jacamr/dlab129
Fletcher-Lartey S., Yee M., Gaarslev C., Khan R. (2016). Why do general practitioners prescribe antibiotics for upper respiratory tract infections to meet patient expectations: A mixed methods study. BMJ Open 6, e012244. doi: 10.1136/bmjopen-2016-012244
Foucault M. (2003). The birth of the clinic. An archaeology of medical perception (London: Routledge).
Fracarolli I. F. L., de Oliveira S. A., Marziale M. H. P. (2017). Bacterial colonization and antimicrobial resistance in healthcare workers: An integrative review. Acta Paulista Enfermagem 30, 651–657. doi: 10.1590/1982-0194201700086
Gaarslev C., Yee M., Chan G., Fletcher-lartey S., Khan R. (2016). A mixed methods study to understand patient expectations for antibiotics for an upper respiratory tract infection. Antimicrobial Resistance Infection Control 5, 39. doi: 10.1186/s13756-016-0134-3
Garcia-Doval I., van Zuuren E. J., Bath-Hextall F., Ingram J. R. (2017). Systematic reviews: Let's keep them trustworthy. Br. J. Dermatol. 177, 888–889. doi: 10.1111/bjd.15826
Gautham M., Bhattacharyya S., Maity S., Roy M. B., Balasubramaniam P., Ebata A., et al. (2024). Just as curry is needed to eat rice, antibiotics are needed to cure fever" -A qualitative study of individual, community and health system-level influences on community antibiotic practices in rural West Bengal, India. BMJ Open 14, e076616. doi: 10.1136/bmjopen-2023076616
Ghiga I., Pitchforth E., Stålsby Lundborg C., Machowska A. (2023). Family doctors' roles and perceptions on antibiotic consumption and antibiotic resistance in Romania: A qualitative study. BMC Primary Care 24, p.93. doi: 10.1186/s12875-023-02047-z
Ghiga I., Stålsby Lundborg C. (2016). 'Struggling to be a defender of health' -A qualitative study on the pharmacists' perceptions of their role in antibiotic consumption and antibiotic resistance in Romania. J. Pharm. Policy Pract. 9, 10. doi: 10.1186/s40545-016-0061-y
Giamarellou H., Galani L., Karavasilis T., Ioannidis K., Karaiskos I. (2023). Antimicrobial stewardship in the hospital setting: A narrative review. Antibiotics 12, 1557. doi: 10.3390/antibiotics12101557
Gilham E. L., Pearce-Smith N., Carter V., Ashiru-Oredope D. (2024). Assessment of global antimicrobial resistance campaigns conducted to improve public awareness and antimicrobial use behaviors: A rapid systematic review. BMC Public Health 24, 396. doi: 10.1186/s12889024-17766-w
Glasdam S., Ekstrand F., Rosberg M., van der Schaaf A. M. (2020). A gap between the philosophy and the practice of palliative healthcare: sociological perspectives on the practice of nurses in specialized palliative homecare. Medicine Health care philosophy 23, 141–152. doi: 10.1007/s11019-019-09918-2
Glasdam S., Loodin H., Wrigstad J. (2021). Articulations of antimicrobial resistance in trade union financed journals for nurses in Scandinavia -A Foucauldian perspective. Nurs. Inq. 28, e12396. doi: 10.1111/nin.12396
Grigoryan L., Mulgirigama A., Powell M., Schmiemann G. (2022). The emotional impact of urinary tract infections in women: A qualitative analysis. BMC Women's Health 22, 182. doi: 10.1186/s12905-022-01757-3
Gu T., Li W., Yang L.-L., Yang S.-M., He Q., He H.-Y., et al. (2022). Systematic review of guidelines for the diagnosis and treatment of Clostridioides difficile infection. Front. Cell. Infection Microbiol. 12. doi: 10.3389/fcimb.2022.926482
Gualano M. R., Gili R., Scaioli G., Bert F., Siliquini R. (2015). General population's knowledge and attitudes about antibiotics: A systematic review and meta-analysis. Pharmacoepidemiology Drug Saf. 24, 2–10. doi: 10.1002/pds.3716
Gulliford M. C., Charlton J., Boiko O., Winter J. R., Rezel-Potts E., Sun X., et al. (2021). Safety of reducing antibiotic prescribing in primary care: a mixed-methods study. NIHR Journals Library 9 (9). doi: 10.3310/hsdr09090
Guo H., Hildon Z. J., Loh V. W. K., Sundram M., Ibrahim M. A. B., Tang W. E., et al. (2021). Exploring antibiotic prescribing in public and private primary care settings in Singapore: A qualitative analysis informing theory and evidence-based planning for value-driven intervention design. BMC Family Pract. 22, 205. doi: 10.1186/s12875-021-01556-z
Ha D. R., Haste N. M., Gluckstein D. P. (2017). The role of antibiotic stewardship in promoting appropriate antibiotic use. Am. J. Lifestyle Med. 13, 376–383. doi: 10.1177/1559827617700824
Halls A., Van't Hoff C., Little P., Verheij T., Leydon G. M. (2017). Qualitative interview study of parents' perspectives, concerns and experiences of the management of lower respiratory tract infections in children in primary care. BMJ Open 7, e015701. doi: 10.1136/bmjopen-2016015701
Hawking M. K., Lecky D. M., Touboul Lundgren P., Aldigs E., Abdulmajed H., Ioannidou E., et al. (2017). Attitudes and behaviors of adolescents towards antibiotics and self-care for respiratory tract infections: A qualitative study. BMJ Open 7, e015308. doi: 10.1136/bmjopen-2016-015308
Heyman G., Cars O., Bejarano M. T., Peterson S. (2014). Access, excess, and ethics–towards a sustainable distribution model for antibiotics. Upsala J. Med. Sci. 119, 134–141. doi: 10.3109/03009734.2014.904958
Hika K., Harwood M., Ritchie S., Chan A. H. Y. (2022). Māori experiences and beliefs about antibiotics and antimicrobial resistance for acute upper respiratory tract symptoms: A qualitative study. Antibiotics 11, p.714. doi: 10.3390/antibiotics11060714
Hoang D. T., McKinn S., Drabarek D., Thu Trieu T., Thuy Pham V., Ngoc Pham Y., et al. (2024). [amp]]lsquo;When I tried to explain, they shouted back at me!’: Exploring how community pharmacists navigate tensions implementing antimicrobial stewardship in Vietnam. Crit. Public Health 34, 1–14. doi: 10.1080/09581596.2024.2303421
Horwood J., Cabral C., Hay A. D., Ingram J. (2016). Primary care clinician antibiotic prescribing decisions in consultations for children with RTIs: A qualitative interview study. Br. J. Gen. Pract. 66, e207–e213. doi: 10.3399/bjgp16X683821
Hu X. Y., Logue M., Maund E., Santer M., Willcox M. L., Islam S., et al. (2024). Pharmacists' perspectives on recommending herbal medicines for acute infections: A qualitative study. BJGP Open 8, BJGPO.2023.0138. doi: 10.3399/BJGPO.2023.0138
Jakupi A., Raka D., Kaae S., Sporrong S. K. (2019). Culture of antibiotic use in Kosovo - an interview study with patients and health professionals. Pharm. Pract. 17, 1540. doi: 10.18549/PharmPract.2019.3.1540
Jones L. F., Owens R., Sallis A., Ashiru-Oredope D., Thornley T., Francis N. A., et al. (2018). Qualitative study using interviews and focus groups to explore the current and potential for antimicrobial stewardship in community pharmacy informed by the Theoretical Domains Framework. BMJ Open 8, e025101. doi: 10.1136/bmjopen-2018-025101
Jorgoni L., Camardo E., Jeffs L., Nakamachi Y., Somanader D., Bell C. M., et al. (2022). Knowledge, perspectives and health outcome expectations of antibiotic therapy in hospitalized patients. Infection Prev. Pract. 4, 100245. doi: 10.1016/j.infpip.2022.100245
Kaminsky E., Aurin I. E., Hedin K., Andersson L., André M. (2020). Registered nurses' views on telephone nursing for patients with respiratory tract infections in primary healthcare - A qualitative interview study. BMC Nurs. 19, 65. doi: 10.1186/s12912-020-00459-1
Kasse G. E., Humphries J., Cosh S. M. (2024). Factors contributing to the variation in antibiotic prescribing among primary health care physicians: A systematic review. BMC Primary Care 25, 8. doi: 10.1186/s12875-023-02223-1
Khan F. U., Khan F. U., Hayat K., Ahmad T., Khan A., Chang J., et al. (2021). Knowledge, attitude, and practice on antibiotics and its resistance: A two-phase mixed-methods online study among Pakistani community pharmacists to promote rational antibiotic use. Int. J. Environ. Res. Public Health 18, 1320. doi: 10.3390/ijerph18031320
Khan K. S., Kunz R., Kleijnen J., Antes G. (2004). Systematic reviews to support evidence-based medicine: how to review and apply findings of healthcare research. 2nd (London: The Royal Society of Medicine Press Limited).
Khan F. U., Mallhi T. H., Khan F. U., Hayat K., Rehman A. U., Shah S., et al. (2022). Evaluation of consumers' perspective on the consumption of antibiotics, antibiotic resistance, and recommendations to improve the rational use of antibiotics: An exploratory qualitative study from post-conflicted region of Pakistan. Front. Pharmacol. 13. doi: 10.3389/fphar.2022.881243
Knobloch M. J., Musuuza J., Baubie K., Saban K. L., Suda K. J., Safdar N. (2021). Nurse practitioners as antibiotic stewards: Examining prescribing patterns and perceptions. Am. J. Infection Control 49, 1052–1057. doi: 10.1016/j.ajic.2021.01.018
Korkmaz P., Mıstanoğlu-Özatağ D., Paşalı-Kilit T., Toka O., Onbaşı K. (2024). Knowledge and attitudes of patients about the rational use of antibiotics. Infect. Dis. Clin. Microbiol. 6, 11–21. doi: 10.36519/idcm.2024.305
Kurotschka P. K., Hemkeppler J., Gierszewski D., Ghirotto L., Gágyor I. (2024). General practitioners' decision making managing uncomplicated urinary tract infections in women: A qualitative study. BJGP Open p, BJGPO.2023.0224. doi: 10.3399/BJGPO.2023.0224
Lalithabai D. S., Hababeh M. O., Wani T. A., Aboshaiqah A. E. (2022). Knowledge, attitude and beliefs of nurses regarding antibiotic use and prevention of antibiotic resistance. SAGE Open Nurs. 8, 1–9. doi: 10.1177/23779608221076821
Lambert M., Wonink A., Benko R., Plejdrup Hansen M., van Dijk L., Taxis K. (2024). Pharmacists combating antimicrobial resistance: A Delphi study on antibiotic dispensing. Res. Soc. Administrative Pharm. 20 (8), S1551–7411(24)00120-7. doi: 10.1016/j.sapharm.2024.04.006
Lansink C., Sinha B., Meessen N., Dekkers T., Beerlage-de Jong N. (2024). Why do physicians prescribe antibiotics? A systematic review of the psycho-socio-organizational factors related to potentially inappropriate prescribing of antimicrobials in Europe. Infect. Dis. Rep. 16, 664–683. doi: 10.3390/idr16040051
Laytner L., Chen P., Nash S., Paasche-Orlow M. K., Street R., Zoorob R., et al. (2023). Perspectives on non-prescription antibiotic use among Hispanic patients in the Houston Metroplex. J. Am. Board Family Med. 36, 390–404. doi: 10.3122/jabfm.2022.220416R1
Lee S. Y., Shanshan Y., Lwin M. O. (2023). Are threat perceptions associated with patient adherence to antibiotics? Insights from a survey regarding antibiotics and antimicrobial resistance among the Singapore public. BMC Public Health 23, 1–8. doi: 10.1186/s12889-023-15184y
Lescure D. L. A., van Oorschot W., Brouwer R., van der Velden J., Tjon-A-Tsien A. M. L., Bonnema I. V., et al. (2022). Providing antibiotics to immigrants: A qualitative study of general practitioners' and pharmacists' experiences. BMC Primary Care 23, 100. doi: 10.1186/s12875-022-01706-x
Lim K., Broom A., Olsen A., Seale H. (2022). Community pharmacists as antimicrobial guardians and gatekeepers - A qualitative study of the perspectives of pharmacy sector stakeholders. Exploratory Res. Clin. Soc. Pharm. 9, 100212. doi: 10.1016/j.rcsop.2022.100212
Lipstein E. A., Block J. P., Dodds C., Forrest C. B., Heerman W. J., Law J. K., et al. (2019). Early antibiotics and childhood obesity: Do future risks matter to parents and physicians? Clin. Pediatr. 58, 191–198. doi: 10.1177/0009922818809534
Long H. A., French D. P., Brooks J. M. (2020). Optimizing the value of the critical appraisal skills program (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 1, 31–42. doi: 10.1177/2632084320947559
Lum E. P. M., Page K., Nissen L., Doust J., Graves N. (2017). Australian consumer perspectives, attitudes and behaviors on antibiotic use and antibiotic resistance: A qualitative study with implications for public health policy and practice. BMC Public Health 17, 799. doi: 10.1186/s12889-017-4813
Lum E. P. M., Page K., Whitty J. A., Doust J., Graves N. (2018). Antibiotic prescribing in primary healthcare: Dominant factors and trade-offs in decision-making. Infect. Dis. Health 23, 74–86. doi: 10.1016/j.idh.2017.12.002.-7
Mahmoud M. A., Aldhaeefi M., Sheikh A., Aljadhey H. (2018). Community pharmacists' perspectives about reasons behind antibiotics dispensing without prescription: A qualitative study. Biomed. Res. 29, 3792–3796. doi: 10.4066/biomedicalresearch.29-18-1112
Manderson L. (2020). Prescribing, care and resistance: Antibiotic use in urban South Africa. Humanities Soc. Sci. Commun. 7, 77. doi: 10.1057/s41599-020-00564-1
Mas-Dalmau G., Pequeño-Saco S., de la Poza-Abad M., Borrell-Thió E., Besa-Castellà M., AlsinaCasalduero M., et al. (2023). Perceptions and attitudes regarding delayed antibiotic prescription for respiratory tract infections: A qualitative study. BMC Primary Care 24, 204. doi: 10.1186/s12875-023-02123-4
McCubbin K. D., Anholt R. M., de Jong E., Ida J. A., Nóbrega D. B., Kastelic J. P., et al. (2021). Knowledge gaps in the understanding of antimicrobial resistance in Canada. Front. Public Health 9. doi: 10.3389/fpubh.2021.726484
McCullough A. R., Pollack A. J., Plejdrup Hansen M., Glasziou P. P., Looke D. F., Britt H. C., et al. (2017). Antibiotics for acute respiratory infections in general practice: Comparison of prescribing rates with guideline recommendations. Med. J. Aust. 207, 65–69. doi: 10.5694/mja16.01042
McDermott L., Leydon G. M., Halls A., Kelly J., Nagle A., White J., et al. (2017). Qualitative interview study of antibiotics and self-management strategies for respiratory infections in primary care. BMJ Open 7, e016903. doi: 10.1136/bmjopen-2017-016903
Mcleod M., Campbell A., Hayhoe B., Borek A. J., Tonkin-Crine S., Moore M. V., et al. (2024). How, why and when are delayed (back-up) antibiotic prescriptions used in primary care? A realist review integrating concepts of uncertainty in healthcare. BMC Public Health 24, 2820. doi: 10.1186/s12889-024-20248-8
McNulty C. A., Lecky D. M., Hawking M. K., Roberts C., Quigley A., Butler C. C. (2016). How much information about antibiotics do people recall after consulting in primary care? Family Pract. 33, 395–400. doi: 10.1093/fampra/cmw022
Md Rezal R. S., Hassali M. A., Alrasheedy A. A., Saleem F., Md Yusof F. A., Godman B. (2015). Physicians' knowledge, perceptions and behavior towards antibiotic prescribing: A systematic review of the literature. Expert Rev. Anti-infective Ther. 13, 665–680. doi: 10.1586/14787210.2015.1025057
Medina-Perucha L., García-Sangenís A., Moragas A., Gálvez-Hernández P., Cots J. M., Lanau-Roig A., et al. (2020). Autonomy, power dynamics and antibiotic use in primary healthcare: A qualitative study. PloS One 15, e0244432. doi: 10.1371/journal.pone.0244432
Miller B. J., Carson K. A., Keller S. (2020). Educating patients on unnecessary antibiotics: Personalizing potential harm aids patient understanding. J. Am. Board Family Medicine: JABFM 33, 969–977. doi: 10.3122/jabfm.2020.06.200210
Minssen T., Outterson K., Rogers Van Katwyk S., Batista P. H. D., Chandler C. I. R., Ciabuschi F., et al. (2020). Social, cultural and economic aspects of antimicrobial resistance. Bull. World Health Organ. 98, 823–823A. doi: 10.2471/BLT.20.275875
Mortazhejri S., Patey A. M., Stacey D., Bhatia R. S., Abdulla A., Grimshaw J. M. (2020). Understanding determinants of patients' decisions to attend their family physician and to take antibiotics for upper respiratory tract infections: A qualitative descriptive study. BMC Family Pract. 21, 119. doi: 10.1186/s12875-020-01196-9
Musoke D., Lubega G. B., Gbadesire M. S., Boateng S., Twesigye B., Gheer J., et al. (2023). Antimicrobial stewardship in private pharmacies in Wakiso district, Uganda: A qualitative study. J. Pharm. Policy Pract. 16, 147. doi: 10.1186/s40545-023-00659-5
Mustafa M., Wood F., Butler C. C., Elwyn G. (2014). Managing expectations of antibiotics for upper respiratory tract infections: A qualitative study. Ann. Family Med. 12, 29–36. doi: 10.1370/afm.1583
Ness V., Price L., Currie K., Reilly J. (2014). Antimicrobial resistance and prescribing behavior. Nurse Prescribing 12, 248–253. doi: 10.12968/npre.2014.12.5.248
Nieuwlaat R., Wilczynski N., Navarro T., Hobson N., Jeffery R., Keepanasseril A., et al. (2014). Interventions for enhancing medication adherence. Cochrane Database Systematic Rev. 2014, CD000011. doi: 10.1002/14651858.CD000011.pub4
Noor M. N., Liverani M., Bryant J., Rahman-Shepherd A., Sharif S., Aftab W., et al. (2022). The healthcare field as a marketplace: General practitioners, pharmaceutical companies, and profit-led prescribing in Pakistan. Health Sociology Rev. 32, 198–212. doi: 10.1080/14461242.2022.2139628
O'Doherty J., Leader L. F. W., O'Regan A., Dunne C., Puthoopparambil S. J., O'Connor R. (2019). Over prescribing of antibiotics for acute respiratory tract infections: A qualitative study to explore Irish general practitioners' perspectives. BMC Family Pract. 20, 27. doi: 10.1186/s12875019-0917-8
Om C., Daily F., Vlieghe E., McLaughlin J. C., McLaws M. L. (2017). Pervasive antibiotic misuse in the Cambodian community: Antibiotic-seeking behavior with unrestricted access. Antimicrobial Resistance Infection Control 6, 30. doi: 10.1186/s13756-017-0187-y
Özcebe H., Üner S., Karadag O., Daryani A., Gershuni O., Czabanowska K., et al. (2022). Perspectives of physicians and pharmacists on rational use of antibiotics in Turkey and among Turkish migrants in Germany, Sweden and the Netherlands: A qualitative study. BMC Primary Care 23, 29. doi: 10.1186/s12875-022-01636-8
Page M. J., McKenzie J. E., Bossuyt P. M., Boutron I., Hoffmann T. C., Mulrow C. D., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Systematic Rev. 10, 89. doi: 10.1186/s13643-021-01626-4
Peiffer-Smadja N., Allison R., Jones L. F., Holmes A., Patel P., Lecky D. M., et al. (2020). Preventing and managing urinary tract infections: Enhancing the role of community pharmacists - a mixed methods study. Antibiotics 9, 583. doi: 10.3390/antibiotics9090583
Pokharel S., Adhikari B., Johnson T., Cheah P. Y. (2024). Interventions to address antimicrobial resistance: An ethical analysis of key tensions and how they apply in low-income and middle-income countries. BMJ Global Health 9, e012874. doi: 10.1136/bmjgh-2023-012874
Poss-Doering R., Kamradt M., Stuermlinger A., Glassen K., Kaufmann-Kolle P., Andres E., et al. (2020). The complex phenomenon of dysrational antibiotics prescribing decisions in German primary healthcare: A qualitative interview study using dual process theory. Antimicrobial Resistance Infection Control 9, 6. doi: 10.1186/s13756-019-0664-6
Pouwels K. B., Hopkins S., Llewelyn M. J., Walker A. S., McNulty C. A., Robotham J. V. (2019). Duration of antibiotic treatment for common infections in English primary care: cross sectional analysis and comparison with guidelines. BMJ 364, l440. doi: 10.1136/bmj.l440
Pristianty L., Kurniati V. L., Hidayati I. R. (2019). Knowledge and attitude: Two fundamental factors that determine patient compliance in antibiotic therapy. J. Basic Clin. Physiol. Pharmacol. 30, N.PAG. doi: 10.1515/jbcpp-2019-0321
RaChina S., Zakharenkova P., Kozlov R., Palagin I., Shishkina K., Strelkova D., et al. (2024). The antibiotic knowledge, attitudes and behaviors of patients purchasing antibiotics with prescription in Russia: A qualitative, comparative analysis. JAC-Antimicrobial Resistance 6, dlae041. doi: 10.1093/jacamr/dlae041
Rao I., Shaham A., Yavneh A., Kahana D., Ashlagi I., Brandeau M. L., et al. (2020). Predicting and improving patient-level antibiotic adherence. Health Care Manage. Sci. 23, 507–519. doi: 10.1007/s10729-020-09523-3
Raspopovic K., Jankovic S., Opancina V. (2016). Factors affecting inappropriate prescription of antibiotics and the emergence of antibiotic resistance in patients in primary health care. Medicinski Casopis 50, 85–90. doi: 10.5937/mckg50-12699
Reeves S., Pelone F., Harrison R., Goldman J., Zwarenstein M. (2017). Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Systematic Rev. 6, CD000072. doi: 10.1002/14651858.CD000072.pub3
Res R., Hoti K., Charrois T. L. (2017). Pharmacists' perceptions regarding optimization of antibiotic prescribing in the community. J. Pharm. Pract. 30, 146–153. doi: 10.1177/0897190015623883
Ridd M., Shaw A., Lewis G., Salisbury C. (2009). The patient-doctor relationship: A synthesis of the qualitative literature on patients' perspectives. Br. J. Gen. Pract. 59, e116–e133. doi: 10.3399/bjgp09X420248
Ryves R., Eyles C., Moore M., McDermott L., Little P., Leydon G. M. (2016). Understanding the delayed prescribing of antibiotics for respiratory tract infection in primary care: A qualitative analysis. BMJ Open 6, p.e011882. doi: 10.1136/bmjopen-2016-011882
Saleem Z., Hassali M. A., Hashmi F. K., Godman B., Saleem F. (2019). Antimicrobial dispensing practices and determinants of antimicrobial resistance: A qualitative study among community pharmacists in Pakistan. Family Med. Community Health 7, e000138. doi: 10.1136/fmch-2019-000138
Saleh D., Abu-Farha R., Mukattash T. L., Barakat M., Alefishat E. (2021). Views of community pharmacists on antimicrobial resistance and antimicrobial stewardship in Jordan: A qualitative study. Antibiotics 10, p.384. doi: 10.3390/antibiotics10040384
Saliba-Gustafsson E. A., Nyberg A., Borg M. A., Rosales-Klintz S., Stålsby Lundborg C. (2021). Barriers and facilitators to prudent antibiotic prescribing for acute respiratory tract infections: A qualitative study with general practitioners in Malta. PloS One 16, p.e0246782. doi: 10.1371/journal.pone.0246782
Saliba-Gustafsson E. A., Röing M., Borg M. A., Rosales-Klintz S., Lundborg C. S. (2019). General practitioners' perceptions of delayed antibiotic prescription for respiratory tract infections: A phenomenographic study. PloS One 14, e0225506. doi: 10.1371/journal.pone.0225506
Salim A. M., Elgizoli B. (2017). Exploring the reasons why pharmacists dispense antibiotics without prescriptions in Khartoum state, Sudan. Int. J. Pharm. Pract. 25, 59–65. doi: 10.1111/ijpp.12317
Santana M. J., Manalili K., Jolley R. J., Zelinsky S., Quan H., Lu M. (2018). How to practice person centered care: A conceptual framework. Health Expectations 21, 429–440. doi: 10.1111/hex.12640
Sargent L., McCullough A., Del Mar C., Lowe J. (2017). Using theory to explore facilitators and barriers to delayed prescribing in Australia: A qualitative study using the Theoretical Domains Framework and the Behavior Change Wheel. BMC Family Pract. 18, 20. doi: 10.1186/s12875-017-0589-1
Sayood S. J., Botros M., Suda K. J., Foraker R., Durkin M. J. (2021). Attitudes toward using clinical decision support in community pharmacies to promote antibiotic stewardship. J. Am. Pharmacists Assoc. 61, 565–571. doi: 10.1016/j.japh.2021.04.008
Schiavo J. H. (2019). PROSPERO: An international register of systematic review protocols. Med. Reference Serv. Q. 38, 171–180. doi: 10.1080/02763869.2019.1588072
Schmiege D., Evers M., Kistemann T., Falkenberg T. (2020). What drives antibiotic use in the community? A systematic review of determinants in the human outpatient sector. Int. J. Hygiene Environ. Health 226, 113497. doi: 10.1016/j.ijheh.2020.113497
Sharaf N., Al-Jayyousi G. F., Radwan E., Shams Eldin S. M. E., Hamdani D., Al-Katheeri H., et al. (2021). Barriers of appropriate antibiotic prescription at PHCC in Qatar: Perspective of physicians and pharmacists. Antibiotics 10, 317. doi: 10.3390/antibiotics10030317
Shen X., Jiang H., Xu H., et al. (2020). The global prevalence of turnover intention among general practitioners: A systematic review and meta-analysis. BMC Family Pract. 21, 246. doi: 10.1186/s12875-020-01309-4
Sievert E. D. C., Korn L., Gross M., Santana A. P., Böhm R., Betsch C. (2024). Communicating diagnostic uncertainty reduces expectations of receiving antibiotics: Two online experiments with hypothetical patients. Appl. Psychol. Health Well-Being 16, 1459–1478. doi: 10.1111/aphw.12536
Sijbom M., Büchner F. L., Saadah N. H., Numans M. E., de Boer M. G. J. (2023). Determinants of inappropriate antibiotic prescription in primary care in developed countries with general practitioners as gatekeepers: A systematic review and construction of a framework. BMJ Open 13, e065006. doi: 10.1136/bmjopen-2022-065006
Simeoni M., Saragosa M., Laur C., Desveaux L., Schwartz K., Ivers N. (2022). Coping with 'the grey area' of antibiotic prescribing: A theory-informed qualitative study exploring family physician perspectives on antibiotic prescribing. BMC Primary Care 23, 188. doi: 10.1186/s12875-02201806-8
Singh S., Degeling C., Fernandez D., Montgomery A., Caputi P., Deane F. P. (2022). How do aged care staff feel about antimicrobial stewardship? A systematic review of staff attitudes in long-term residential aged-care. Antimicrobial Resistance Infection Control 11 92. doi: 10.1186/s13756-022-01128-5
Sköld M., Aabenhus R., Guassora A. D., Mäkelä M. (2017). Antibiotic treatment failure when consulting patients with respiratory tract infections in general practice: A qualitative study to explore Danish general practitioners' perspectives. Eur. J. Gen. Pract. 23, 120–127. doi: 10.1080/13814788.2017.1305105
Souto-López L., Vazquez-Cancela O., Vazquez-Lago J. M., López-Durán A., Figueiras A. (2020). Parent-related factors influencing antibiotic use in a pediatric population: A qualitative study in Spain. Acta Paediatrica 109, 2719–2726. doi: 10.1111/apa.15277
Spicer J. O., Roberts R. M., Hicks L. A. (2020). Perceptions of the benefits and risks of antibiotics among adult patients and parents with high antibiotic utilization. Open Forum Infect. Dis. 7, p. doi: 10.1093/ofid/ofaa544
Spurling G. K., Del Mar C. B., Dooley L., Foxlee R., Farley R. (2017). Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Systematic Rev. 2017, .CD004417. doi: 10.1002/14651858.CD004417
Stewart S. J. F., Moon Z., Horne R. (2022). Medication nonadherence: Health impact, prevalence, correlates and interventions. Psychol. Health 38, 726–765. doi: 10.1080/08870446.2022.2144923
Stivers T., Timmermans S. (2021). Arriving at no: Patient pressure to prescribe antibiotics and physicians' responses. Soc. Sci. Med. 290, 114007. doi: 10.1016/j.socscimed.2021.114007
Sulis G., Adam P., Nafade V., Gore G., Daniels B., Daftary A., et al. (2020). Antibiotic prescription practices in primary care in low- and middle-income countries: A systematic review and meta-analysis. PloS Med. 17, e1003139. doi: 10.1371/journal.pmed.1003139
Sumner S., Forsyth S., Collette-Merrill K., Taylor C., Vento T., Veillette J., et al. (2018). Antibiotic stewardship: The role of clinical nurses and nurse educators. Nurse Educ. Today 60, 157–160. doi: 10.1016/j.nedt.2017.10.011
Sundvall P. D., Skoglund I., Hess-Wargbaner M., Åhrén C. (2020). Rational antibiotic prescribing in primary care: Qualitative study of opportunities and obstacles. BJGP Open 4, bjgpopen20X101079. doi: 10.3399/bjgpopen20X101079
Suy S., Rego S., Bory S., Chhorn S., Phou S., Prien C., et al. (2019). Invisible medicine sellers and their use of antibiotics: A qualitative study in Cambodia. BMJ Global Health 4, e001787. doi: 10.1136/bmjgh-2019-001787
Sychareun V., Phounsavath P., Sihavong A., Kounnavong S., Chaleunvong K., Machowska A., et al. (2022). Perceptions and reported practices of pregnant women and mothers of children under two years of age regarding antibiotic use and resistance in Vientiane province, Lao PDR: A qualitative study. BMC Pregnancy Childbirth 22, 569. doi: 10.1186/s12884022-04894-7
Tark A., Estrada L. V., Tresgallo M. E., Quigley D. D., Stone P. W., Agarwal M. (2020). Palliative care and infection management at end of life in nursing homes: A descriptive survey. Palliative Med. 34, 580–588. doi: 10.1177/0269216320902672
Thaggard S., Reid S., Chan A., White C., Fraser L., Arroll B. A., et al. (2023). Whānau Māori and Pacific peoples' knowledge, perceptions, expectations and solutions regarding antibiotic treatment of upper respiratory tract infections: A qualitative study. BMC Infect. Dis. 23, 458. doi: 10.1186/s12879-023-08431-5
Tonna A. P., Weidmann A. E., Sneddon J., Stewart D. (2020). Views and experiences of community pharmacy team members on antimicrobial stewardship activities in Scotland: A qualitative study. Int. J. Clin. Pharm. 42, 1261–1269. doi: 10.1007/s11096-020-01042z
Torres N. F., Solomon V. P., Middleton L. E. (2020). Pharmacists' practices for non-prescribed antibiotic dispensing in Mozambique. Pharm. Pract. (Granada) 18, 1965. doi: 10.18549/PharmPract.2020.3.1965
Torres N. F., Solomon V. P., Middleton L. E. (2023). “Antibiotics heal all diseases”; the factors influencing the pratices of self-medication with antibiotics in Maputo City, Mozambique. J. Public Health (Berl.) 31, 73–84. doi: 10.1007/s10389-020-01416-7
van der Zande M. M., Dembinsky M., Aresi G., van Staa T. P. (2019). General practitioners' accounts of negotiating antibiotic prescribing decisions with patients: A qualitative study on what influences antibiotic prescribing in low, medium and high prescribing practices. BMC Family Pract. 20, 172. doi: 10.1186/s12875-019-1065-x
van Hecke O., Butler C., Mendelson M., Tonkin-Crine S. (2019b). Introducing new point-of-care tests for common infections in publicly funded clinics in South Africa: A qualitative study with primary care clinicians. BMJ Open 9, e029260. doi: 10.1136/bmjopen-2019-029260
van Hecke O., Butler C. C., Wang K., Tonkin-Crine S. (2019a). Parents' perceptions of antibiotic use and antibiotic resistance (PAUSE): A qualitative interview study. J. Antimicrobial Chemotherapy 74, 1741–1747. doi: 10.1093/jac/dkz091
van Horrik T. M., Colliers A., Blanker M. H., de Bont E. G., van Driel A. A., Laan B. J., et al. (2024). Qualitative study on shared decision making in cystitis management in general practice. BJGP Open 8 (3), BJGPO.2023.0179. doi: 10.3399/BJGPO.2023.0179
Varkey B. (2021). Principles of clinical ethics and their application to practice. Med. principles Pract. 30, 17–28. doi: 10.1159/000509119
Velgan M., Vanderheyde T., Kalda R., Michels N. (2023). Driving forces of GPs' migration in Europe: An exploratory qualitative study. BJGP Open 7, p. doi: 10.3399/BJGPO.2022.0132
Wang D., Liu C., Zhang X., Liu (2021). Does diagnostic uncertainty increase antibiotic prescribing in primary care? NPJ Primary Care Respir. Med. 31, 17. doi: 10.1038/s41533-02100229-9
Williams S. J., Halls A. V., Tonkin-Crine S., Moore M. V., Latter S. E., Little P., et al. (2018). General practitioner and nurse prescriber experiences of prescribing antibiotics for respiratory tract infections in UK primary care out-of-hours services (the UNITE study). J. Antimicrobial Chemotherapy 73, 795–803. doi: 10.1093/jac/dkx429
Wong L. H., Tay E., Heng S. T., Guo H., Kwa A. L. H., Ng T. M., et al. (2021). Hospital pharmacists and antimicrobial stewardship: A qualitative analysis. Antibiotics 10, 1441. doi: 10.3390/antibiotics10121441
World Health Organization (2015). Global action plan on antimicrobial resistance. (Geneva: World Health Organization).
World Health Organization (2017). Antimicrobial Resistance. Fact sheets on sustainable development goals: Health targets (Geneva: World Health Organization).
World Health Organization (2018). Antimicrobial resistance and primary health care. (Geneva: World Health Organization).
Yates T. D., Davis M. E., Taylor Y. J., Davidson L., Connor C. D., Buehler K., et al. (2018). Not a magic pill: A qualitative exploration of provider perspectives on antibiotic prescribing in the outpatient setting. BMC Family Pract. 19, 96. doi: 10.1186/s12875-018-0788-4
Zago L. F., Correa J. S., da Silva B. R. R., Fracolli L. A., Padoveze M. C., de Oliveira S. M., et al. (2023). Experiences of antibiotic use among Brazilian healthcare users: An exploratory study. Health Expectations 26, 343–354. doi: 10.1111/hex.13664
Zaykova K., Nikolova S., Pancheva R., Serbezova A. (2022). A survey of knowledge, attitudes and use of antibiotics among Bulgarian population. Biotechnol. Biotechnol. Equip. 36, 933–941. doi: 10.1080/13102818.2022.2145237
Zetts R. M., Stoesz A., Garcia A. M., Doctor J. N., Gerber J. S., Linder J. A., et al. (2020). Primary care physicians' attitudes and perceptions towards antibiotic resistance and outpatient antibiotic stewardship in the USA: A qualitative study. BMJ Open 10, e034983. doi: 10.1136/bmjopen2019-034983
Keywords: antimicrobial resistance, patient education, primary care, professionals, qualitative systematic literature review
Citation: Balea LB, Gulestø RJA, Xu H and Glasdam S (2025) Physicians’, pharmacists’, and nurses’ education of patients about antibiotic use and antimicrobial resistance in primary care settings: a qualitative systematic literature review. Front. Antibiot. 3:1507868. doi: 10.3389/frabi.2024.1507868
Received: 08 October 2024; Accepted: 17 December 2024;
Published: 09 January 2025.
Edited by:
Mohd Nasir Mohd Desa, Putra Malaysia University, MalaysiaReviewed by:
Jennifer Hanrahan, Eastern Virginia Medical School, United StatesMazen M. Jamil Alobaidi, College of Applied Sciences, Rustaq, Oman
Copyright © 2025 Balea, Gulestø, Xu and Glasdam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stinne Glasdam, c3Rpbm5lLmdsYXNkYW1AbWVkLmx1LnNl