Abstract
Background: Inflammatory bowel disease (IBD), comprising ulcerative colitis (UC), and Crohn's disease (CD), has been reported to be associated with an increased risk of atrial fibrillation (AF). However, the causal role of the chronic intestinal inflammation (CII) in the development of AF remains controversial. We use Mendelian randomization (MR) analysis to explore the causal inference of CII on AF.
Methods: A two-sample MR analysis was performed to estimate the potential causal effect of CII on AF. Statistical summaries for the associations between single nucleotide polymorphisms (SNPs) and phenotypes of CII were obtained from genome-wide association studies (GWAS) with cohorts of CD (n = 51,874), UC (n = 47,745), and IBD (n = 65,642) of European descent. The GWAS of 1,030,836 people of European ancestry, including 60,620 AF cases and 970,216 controls was collected to identify genetic variants underlying AF. The causal inference was estimated using the multiplicative random effects inverse-variance weighted method (IVW). The methods of MR-Egger, simple median, and weighted median were also employed to avoid the bias of pleiotropy effects.
Results: Using three sets of SNPs (75 SNPs of CD, 60 SNPs of UC, and 95 SNPs of IBD), multiplicative random-effect IVW model estimated a universal null effect of CII on AF (CD: OR = 1.0059, 95% CI: 0.9900, 1.0220, p = 0.47; UC: OR = 1.0087, 95% CI: 0.9896, 1.0281, p = 0.38; IBD: OR = 1.0080, 95% CI: 0.9908, 1.0255, p = 0.37). Similar results were observed using the MR-Egger, simple median, weighted median methods.
Conclusion: As opposing to the traditional observational studies, our two-sample MR analysis did not find enough evidence to support a causal role of either CD or UC in the development of AF.
Introduction
It has long been established that inflammation plays a vital role in the pathological progress of atrial fibrillation (AF). The activated NLRP3 receptor promotes autophagy and mitophagy, which lead to impaired mitochondrial function and reactive oxygen species, contributing to premature atrial beats that may initiate episodes of AF (1). Interleukin-6 and interleukin-8, as pro-inflammatory cytokines, may disrupt the structure of the atrial myocardium, resulting in slow conduction, which in turn maintains the burst of AF (2). Given the implication of inflammation in the development of AF, the assumption of AF susceptibility in inflammatory disease has been made and verified. Compared with age- and sex-matched general patients, systemic lupus erythematosus was associated with a doubled rate of hospitalization for AF (3). A systematic review and meta-analysis have revealed an increased risk ratio of 1.29 (95% CI, 1.05–1.59) in the development of AF in patients with rheumatoid arthritis, as compared to the control group (4).
As a state of chronic intestinal inflammation (CII), inflammatory bowel disease (IBD), comprised of ulcerative colitis (UC) and Crohn's disease (CD), was also reported to be associated with AF incidence in several studies. A retrospective study showed that AF has an overall higher prevalence across all age groups in the IBD population (5). During the follow-up of a population-based cohort study, patients with IBD were identified at a 36% (95% CI, 20–54%) higher risk of AF than controls (6). On the contrary, using the nationwide inpatient database in the United States, patients with IBD were found less likely to be hospitalized for arrhythmias than the non-IBD (9.7 vs. 14.2%, p < 0.001) (7). The potential biases of confounding factors and reverse causation may contribute to such controversy (8), leaving the specific relationship between IBD and AF yet to be determined.
Given that the exposure-associated genetic variants are randomly distributed and not subject to reverse causation, Mendelian randomization (MR) serves as a valuable approach to assess the causal inference of an observed association between a modifiable exposure and a clinically relevant outcome (9). Therefore, we applied MR analysis to explore the potential causal association between CII and AF in this study.
Methods and Materials
Study Design and Data Sources
Valid estimates could be explored from two-sample MR analyses when three key assumptions are met: (1) the instrumental variants (SNPs) are associated with the exposure (CD, UC, and IBD); (2) the instruments may impact the outcome (AF) only via their effects on exposure; and (3) the instruments are independent of any confounders for the association between exposure and outcome.
Candidate genetic instruments for CII were selected from genome-wide association studies (GWAS). In terms of the radiologic, endoscopic, and histopathologic evaluation, cases that fit the clinical criteria for CII phenotypes (CD, UC) and matched controls of European ancestry were recruited. To prevent the pleiotropic bias from trans-ancestry cases (10), all individuals in this study were of European ancestry. Following quality-control, the cohorts of CD (n = 51,874), UC (n = 47,745), and IBD (n = 65,642) of European descent were used to carry out the GWAS (11) (Table 1). The diagnosis of CD and UC was made at the age of 28.39 ± 14.16 and 34.10 ± 15.78 years old. Males accounted for 45.1% of CD and 52.1% of UC patients. Nearly half of CD cases (46.8%) had ileocolonic lesions while 48.9% of UC cases had extensive lesions. Over half of CD patients (52.8%) received abdominal surgery whereas only 18.5% of UC patients took colectomy. To derive the causal effect of CII on AF, three sets of genetic instruments (CD, UC, and IBD) were extracted from combined summary statistics of GWAS.
Table 1
| Contribution | Traits | Sample size | Number of SNPs | Author | Population |
|---|---|---|---|---|---|
| Exposure | Crohn's disease | 51,874 | 124,888 | Rinse KW | European |
| Ulcerative colitis | 47,745 | 156,116 | Rinse KW | European | |
| Inflammatory bowel disease | 65,642 | 157,116 | Rinse KW | European | |
| Outcome | Atrial fibrillation | 1,030,836 | 33,519,037 | Nielsen JB | European |
Description of contributing studies.
Selection of Genetic Instrumental Variants
With 17,897 CD cases, 13,768 UC cases, and 33,977 controls, this European GWAS reported 124,888, 156,116, and 157,116 single nucleotide polymorphisms (SNPs) for phenotypes of CD, UC, and IBD, respectively (11) (Table 1). For the first key assumption of MR analysis, since the selected SNPs were identified through the GWAS, such instruments are likely to be associated with three sets of exposures (CD, UC, and IBD) in the source population. The protocol for the selection of genetic instrumental variants contained three steps. During the preliminary selection, parameters used to identify candidate instrumental variants included a p-value of 5 × 10−8 for genome-wide significance, the minor allele frequency of 0.3 for allowing SNPs in palindromic regions, and r2 < 0.001 over a 10 kb region for linkage disequilibrium clumping (accounts for SNPs correlations). After the preliminary selection, Phenoscanner (12) was used to remove SNPs that potentially violate the second and third key assumptions by having pleiotropic effects on other phenotypes (body mass index, smoking status, hypertension, coronary artery disease, chronic renal failure, and diabetes). Finally, pleiotropic outliers were identified and excluded with MR pleiotropy residual sum and outlier (MR-PRESSO) (13).
Data Sources of Outcomes
To identify genetic variants underlying AF, six discovery cohorts (HUNT, deCODE, MGI, DiscovEHR, UK Biobank, and AFGen Consortium) were gathered to carry out the GWAS of 1,030,836 people of European ancestry, including 60,620 AF cases and 970,216 controls (14) (Table 1). Phenotype-related cases in hospital, out-patient, and emergency room were collected from the electronic health record, using the International Classification of Diseases diagnosis codes (ICD, 427.3 or I48). The electrocardiogram (ECG) was digitally recorded with the Philips Page Writer cardiographs and stored in the Philips TraceMasterVue ECG Management System. Waveforms and parameters of digital ECGs were measured and adjusted for gender and age before extracting them from the database for analysis. For individuals with multiple ECG measurements, the mean standardized value was used.
Statistical Analysis
Multiplicative random-effects inverse-variance weighted (IVW) MR analysis (15) was performed to estimate the possible association between CII and AF, presented as log odds ratios (OR) with 95% confidence intervals (CIs) per unit increase in the log OR of CD, UC, or IBD (16). Also, the methods of MR-Egger, simple median, and weighted median were employed to avoid the bias of pleiotropy effects (17). Heterogeneity was assessed with the I2 index (18) and the funnel plot (19). The power in MR analysis for each association was calculated using a web-based application (http://cnsgenomics.com/shiny/mRnd/) (20). Alpha < 0.05 was set as the two-sided threshold for statistical significance. Statistical software included STATA (StataCorp, 16) and R (R Development Core Team, 3.2.5).
Data Availability Statements
The datasets processed in this study were acquired from GWAS (11, 14), which authorizes secondary analysis through copying and redistributing the material in any medium or format (21); thus no ethical approval was required.
Results
On the basis of the abovementioned protocol, there were 75, 60, and 95 SNPs extracted as instrumental variables, which explained 10.0, 10.0, and 9.0% of the variance in the liability of CD, UC, and IBD, respectively. The I2 index of 30% and the funnel plots did not support substantial heterogeneity across the estimates, suggesting an absence of potential pleiotropic effects among SNPs of CD or UC (Figures 1, 2). A similar presence of low heterogeneity in IBD was displayed in Supplementary Figure 1. The detailed characteristics and associations with the remaining SNPs were presented in Supplementary Tables 1–3. The MR analysis had 75% power at an alpha rate of 5% to detect an OR of 1.08 per log odds of CD, UC, and an OR of 1.07 per log odds of IBD.
Figure 1
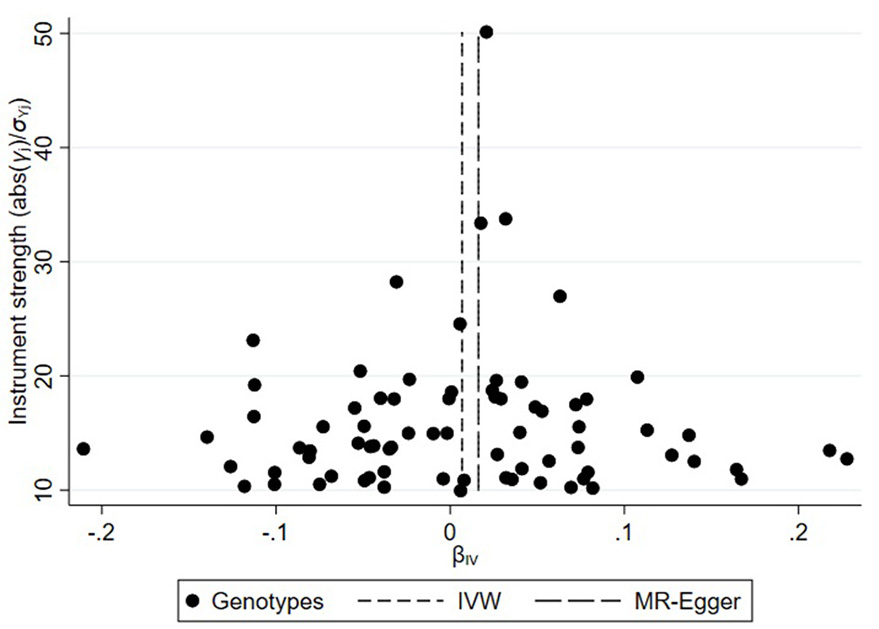
Funnel plot of genetic associations with Crohn's disease against causal estimates based on each genetic variant individually, where the causal effect is expressed in the log odds ratio of atrial fibrillation for each unit increase in Crohn's disease. The overall causal estimates (β coefficients) of Crohn's disease on atrial fibrillation given by weighted inverse-variance (short dashed line) and MR-Egger (long dashed line) methods are shown.
Figure 2
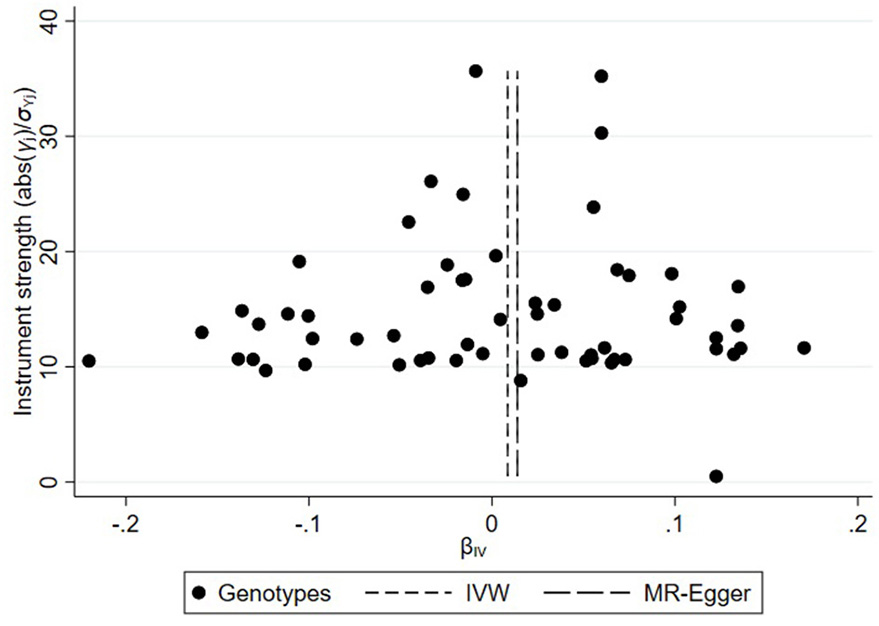
Funnel plot of genetic associations with ulcerative colitis against causal estimates based on each genetic variant individually, where the causal effect is expressed in the log odds ratio of atrial fibrillation for each unit increase in ulcerative colitis. The overall causal estimates (β coefficients) of ulcerative colitis on atrial fibrillation estimated by weighted inverse-variance (short dashed line) and MR-Egger (long dashed line) methods are shown.
A universal null association between CII and AF was captured by each multiplicative random effect IVW model (CD: OR = 1.0059, 95% CI: 0.9900, 1.0220, p = 0.47; UC: OR = 1.0087, 95% CI: 0.9896, 1.0281, p = 0.38; IBD: OR = 1.0080, 95% CI: 0.9908, 1.0255, p = 0.37; Table 2). Methods of MR-Egger, simple median, and the weighted median also found a lack of evidence to support a causal effect of CII on AF (Table 2). The association between each variant with CD/UC and risk of AF was displayed in Figures 3, 4. The scatterplots of IBD variants associated with AF are presented in Supplementary Figure 2. The results of leave-one-out sensitivity analysis (22) indicated that the null association was not remarkably affected by any individual SNP in each MR model (Supplementary Figures 3–5).
Table 2
| Models | CD | UC | IBD | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Inverse variance weighted (multiplicative random effects) | 1.0059 | 0.9900, 1.0220 | 1.0087 | 0.9896, 1.0281 | 1.0080 | 0.9908, 1.0255 |
| MR Egger | 1.0187 | 0.9788, 1.0603 | 1.0140 | 0.9695, 1.0605 | 0.9938 | 0.9558, 1.0333 |
| Simple median | 1.0032 | 0.9818, 1.0251 | 1.0046 | 0.9779, 1.0321 | 1.0089 | 0.9847, 1.0338 |
| Weighted median | 1.0189 | 0.9964, 1.0420 | 1.0004 | 0.9745, 1.0271 | 0.9936 | 0.9671, 1.0209 |
MR estimates of the causal effect of CD, UC, and IBD on AF.
MR, Mendelian randomization; IBD, inflammatory bowel disease; UC, ulcerative colitis; CD, Crohn's disease, AF, atrial fibrillation; OR, odds ratio; CI, confidence interval.
Figure 3
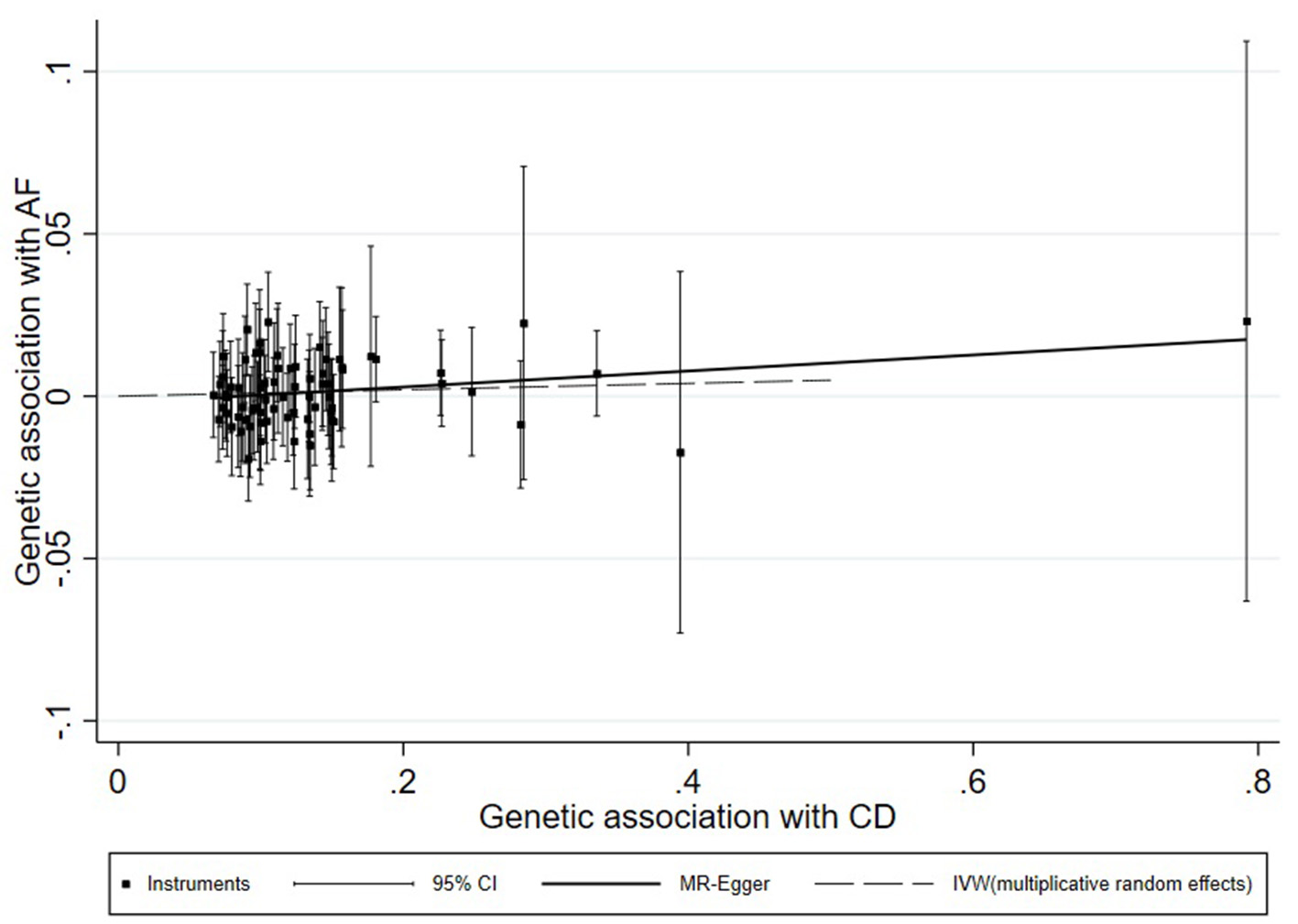
Scatterplot of genetic associations with atrial fibrillation against associations with Crohn's disease, with causal estimates (β coefficients) of Crohn's disease on atrial fibrillation estimated by weighted inverse-variance (dashed line), and MR-Egger (solid line) methods. The straight lines should be the change in the log odds of atrial fibrillation per unit increase of the log odds of Crohn's disease.
Figure 4
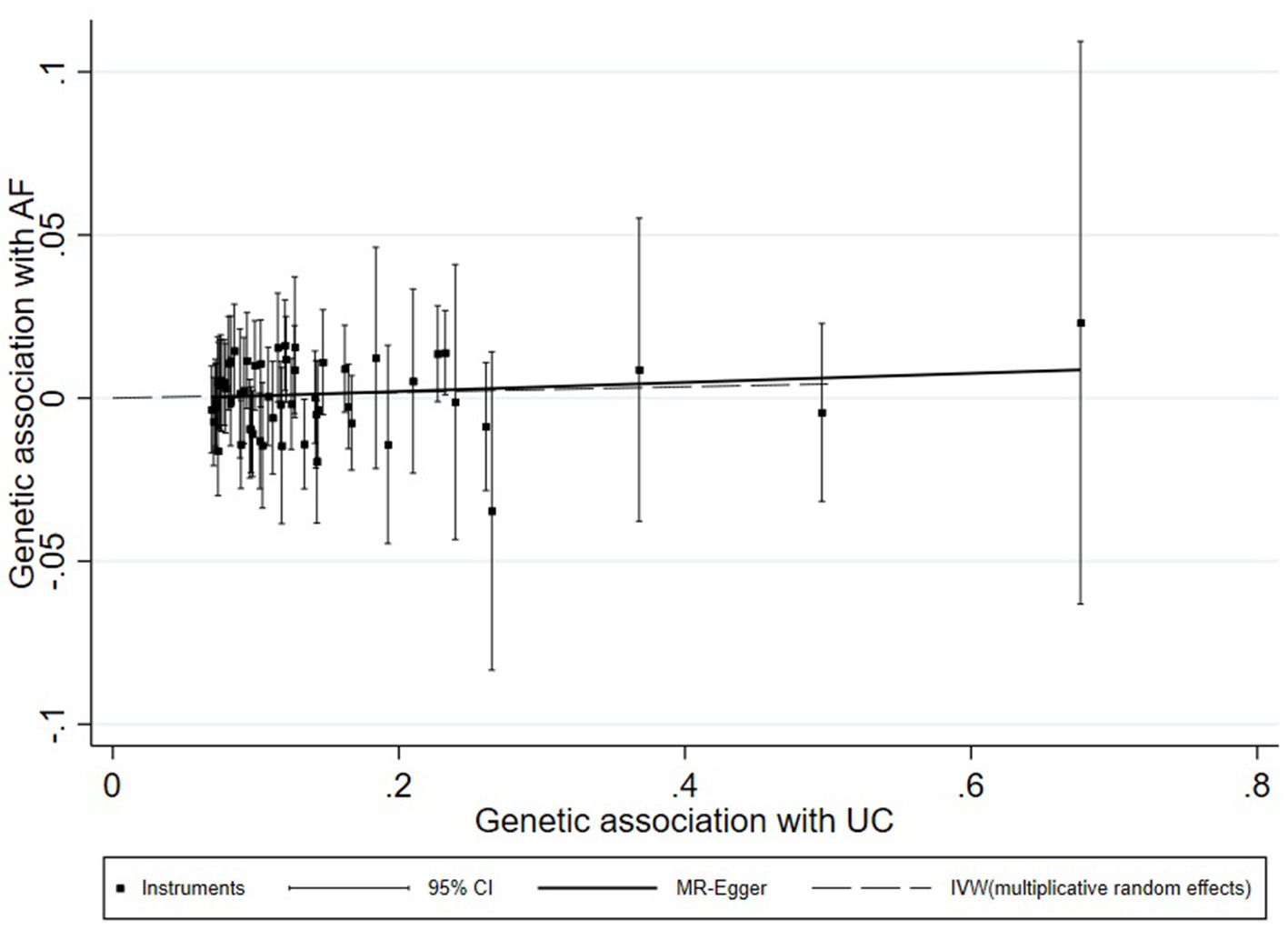
Scatterplot of genetic associations with atrial fibrillation against associations with ulcerative colitis, with causal estimates (β coefficients) of ulcerative colitis on atrial fibrillation estimated by weighted inverse-variance (dashed line), and MR-Egger (solid line) methods. The straight lines should be the change in the log odds of atrial fibrillation per unit increase of the log odds of ulcerative colitis.
Discussion
With large-scale GWAS studies, our two-sample MR analysis demonstrated that neither CD nor UC had a causal effect on AF. With the use of IBD SNPs as the instruments, the estimated effects on AF also become null. Multiple methods including IVW, MR-Egger, the simple median, and weighted median were employed in MR analysis for each set of SNPs, which resulted in a similar conclusion, indicating the robustness of our findings.
The association between cardiac disease and CII has been reported in traditional observational studies. A nationwide investigation of IBD-associated risk of heart failure (HF) in Denmark showed that subjects with IBD had an increased risk of hospitalization for HF (23). Another population-based cohort study reported that during 13 years of follow-up after IBD diagnosis, the risk of ischemic heart disease (IHD) was increased (IRR = 1.22, 95% CI: 1.14, 1.30), as compared with IBD-free individuals (24). While focusing on arrhythmic attack, compared with age- and sex-matched controls, IBD patients corresponded to an increased AF incidence (IRR = 1.26, 95% CI: 1.16, 1.36) (25).
Despite prior reports of a potentially increased risk of cardiac disease among patients with IBD, our MR analysis did not provide sufficient evidence to support a causal role of either IBD or subcategories (CD or UC) on the risk of AF. Given the random allocation of genetic variants, MR analysis may provide a more robust result, as compared with the traditional observational study, which is more likely prone to confounders and reverse causation. The association observed in previous studies may be attributable to several common risk factors shared by IBD and AF. Cigarette smoking is a well-established and modifiable risk factor for AF (26), but it is also associated with a greater likelihood of aggressive CD including the need for surgery (27). While diabetes is a risk factor for the development of AF (28), after adjustment for steroid use and baseline glucose levels, incident diabetes also more frequently occurred in IBD patients (29). A retrospective cohort study reported that increased body weight is associated with a higher likelihood of developing CD and UC flare-ups despite ongoing medical therapy (30). A systematic review showed that general adiposity and higher body fat mass increase the risk of atrial fibrillation (31).
The large population of CD, UC, and AF patients was the main strength of this study. Compared with the association concluded by the observational study design, two-sample MR analyses warrant an exploration of causal conclusion. However, there are several limitations to the current study. While the GWAS presented the descriptive statistics of lesion location and the surgical procedures IBD patients received, these clinical characteristics related to genotype-phenotype mapping were not examined, hindering us from drawing more specific conclusions. Also, the patients' laboratory tests (biomarkers of inflammation) and flare duration were not reported in the GWAS, which could have contributed to the definition of IBD status (active vs. remission). Due to the lack of information on the monitoring and the AF identification by ECG (and not by the use of an implanted recording device), AF incidence may be underestimated, because of the nature of silent AF and cryptogenic strokes. Additionally, it is unlikely to completely remove the biased estimation of causal inference due to potential horizontal pleiotropy. However, MR-Egger regression, MR-PRESSO, and a heterogeneity test were performed, which showed no pleiotropic effect.
Conclusions
Using two-sample MR analysis, we found no convincing evidence to support a causal effect of chronic intestinal inflammation on the risk of developing AF in a population of European ancestry.
Statements
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://gwas.mrcieu.ac.uk/datasets/ebi-a-GCST006414/; https://gwas.mrcieu.ac.uk/datasets/ieu-a-292/.
Author contributions
LC and CJ: conceptualization, data curation, and formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, roles/writing – original draft, and writing – review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2021.641291/full#supplementary-material
Supplementary Figure 1Funnel plot of genetic associations between inflammatory bowel disease and causal estimates of atrial fibrillation.
Supplementary Figure 2Scatterplot of genetic associations between atrial fibrillation and inflammatory bowel disease.
Supplementary Figure 3Leave-one-out sensitivity analysis for causal effect of Crohn's disease on atrial fibrillation. The estimate is indicated by the odds ratio (OR).
Supplementary Figure 4Leave-one-out sensitivity analysis for causal effect of ulcerative colitis on atrial fibrillation.
Supplementary Figure 5Leave-one-out sensitivity analysis for causal effect of inflammatory bowel disease on atrial fibrillation.
References
1.
Van Wagoner DR Chung MK . Inflammation, inflammasome activation, and atrial fibrillation. Circulation. (2018) 138:2243–6. 10.1161/CIRCULATIONAHA.118.036143
2.
Levelt E Pavlides M Banerjee R Mahmod M Kelly C Sellwood J et al . Ectopic and visceral fat deposition in lean and obese patients with type 2 diabetes. J Am Coll Cardiol. (2016) 68:53–63. 10.1016/j.jacc.2016.03.597
3.
Chen SK Barbhaiya M Solomon DH Guan H Yoshida K Feldman CH et al . Atrial fibrillation/flutter hospitalizations among us medicaid recipients with and without systemic lupus erythematosus. J Rheumatol. (2020) 47:1359–65. 10.3899/jrheum.190502
4.
Ungprasert P Srivali N Kittanamongkolchai W . Risk of incident atrial fibrillation in patients with rheumatoid arthritis: a systematic review and meta-analysis. Int J Rheum Dis. (2017) 20:434–41. 10.1111/1756-185X.12820
5.
Pattanshetty DJ Anna K Gajulapalli RD Sappati-Biyyani RR . Inflammatory bowel “cardiac” disease: point prevalence of atrial fibrillation in inflammatory bowel disease population. Saudi J Gastroenterol. (2015) 21:325–9. 10.4103/1319-3767.166208
6.
Choi YJ Choi EK Han KD Park J Moon I Lee E et al . Increased risk of atrial fibrillation in patients with inflammatory bowel disease: a nationwide population-based study. World J Gastroenterol. (2019) 25:2788–98. 10.3748/wjg.v25.i22.2788
7.
Mubasher M Syed T Hanafi A Yu Z Yusuf I Abdullah AS et al . An investigation into the association between inflammatory bowel disease and cardiac arrhythmias: an examination of the united states national inpatient sample database. Clin Med Insights Cardiol. (2020) 14:1179546820955179. 10.1177/1179546820955179
8.
Glass TA Goodman SN Hernan MA Samet JM . Causal inference in public health. Annu Rev Public Health. (2013) 34:61–75. 10.1146/annurev-publhealth-031811-124606
9.
Bochud M Rousson V . Usefulness of mendelian randomization in observational epidemiology. Int J Environ Res Public Health. (2010) 7:711–28. 10.3390/ijerph7030711
10.
Burgess S Davey Smith G Davies NM Dudbridge F Gill D Glymour MM et al . Guidelines for performing mendelian randomization investigations. Wellcome Open Res. (2019) 4:186. 10.12688/wellcomeopenres.15555.1
11.
Liu JZ van Sommeren S Huang H Ng SC Alberts R Takahashi A et al . Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat Genet. (2015) 47:979–986.
12.
Staley JR Blackshaw J Kamat MA Ellis S Surendran P Sun BB et al . Phenoscanner: A database of human genotype-phenotype associations. Bioinformatics. (2016) 32:3207–9. 10.1093/bioinformatics/btw373
13.
Verbanck M Chen CY Neale B Do R . Detection of widespread horizontal pleiotropy in causal relationships inferred from mendelian randomization between complex traits and diseases. Nat Genet. (2018) 50:693–8. 10.1038/s41588-018-0099-7
14.
Nielsen JB Thorolfsdottir RB Fritsche LG Zhou W Skov MW Graham SE et al . Biobank-driven genomic discovery yields new insight into atrial fibrillation biology. Nat Genet. (2018) 50:1234–9. 10.1038/s41588-018-0171-3
15.
Yavorska OO Burgess S . Mendelianrandomization: an r package for performing mendelian randomization analyses using summarized data. Int J Epidemiol. (2017) 46:1734–9. 10.1093/ije/dyx034
16.
Burgess S Labrecque JA . Mendelian randomization with a binary exposure variable: Interpretation and presentation of causal estimates. Eur J Epidemiol. (2018) 33:947–52. 10.1007/s10654-018-0424-6
17.
Didelez V Meng S Sheehan N . Assumptions of IV methods for observational epidemiology. Statist. Sci. (2010) 25:22–40. 10.1214/09-STS316
18.
Higgins JP Thompson SG Deeks JJ Altman DG . Measuring inconsistency in meta-analyses. Bmj. (2003) 327:557–60. 10.1136/bmj.327.7414.557
19.
Sterne JA Sutton AJ Ioannidis JP Terrin N Jones DR Lau J et al . Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. (2011) 343:d4002. 10.1136/bmj.d4002
20.
Brion MJ Shakhbazov K Visscher PM . Calculating statistical power in mendelian randomization studies. Int. J. Epidemiol. (2013) 42:1497–501. 10.1093/ije/dyt179
21.
Walker VM Davies NM Hemani G Zheng J Haycock PC Gaunt TR et al . Using the mr-base platform to investigate risk factors and drug targets for thousands of phenotypes. Wellcome Open Res. (2019) 4:113. 10.12688/wellcomeopenres.15334.1
22.
Cheng H Garrick DJ Fernando RL . Efficient strategies for leave-one-out cross validation for genomic best linear unbiased prediction. J Anim Sci Biotechnol. (2017) 8:38. 10.1186/s40104-017-0164-6
23.
Kristensen SL Ahlehoff O Lindhardsen J Erichsen R Lamberts M Khalid U et al . Inflammatory bowel disease is associated with an increased risk of hospitalization for heart failure: a Danish nationwide cohort study. Circ Heart Fail. (2014) 7:717–22. 10.1161/CIRCHEARTFAILURE.114.001152
24.
Rungoe C Basit S Ranthe MF Wohlfahrt J Langholz E Jess T . Risk of ischaemic heart disease in patients with inflammatory bowel disease: a nationwide danish cohort study. Gut. (2013) 62:689–94. 10.1136/gutjnl-2012-303285
25.
Kristensen SL Lindhardsen J Ahlehoff O Erichsen R Lamberts M Khalid U et al . Increased risk of atrial fibrillation and stroke during active stages of inflammatory bowel disease: a nationwide study. Europace. (2014) 16:477–84. 10.1093/europace/eut312
26.
Watanabe I . Smoking and risk of atrial fibrillation. J. Cardiol. (2018) 71:111–2. 10.1016/j.jjcc.2017.08.001
27.
Ananthakrishnan AN . Environmental risk factors for inflammatory bowel diseases: a review. Dig. Dis. Sci. (2015) 60:290–8. 10.1007/s10620-014-3350-9
28.
Wang A Green JB Halperin JL Piccini JP Sr . Atrial fibrillation diabetes mellitus: Jacc review topic of the week. J Am Coll Cardiol. (2019) 74:1107–15. 10.1016/j.jacc.2019.07.020
29.
Kang EA Han K Chun J Soh H Park S Im JP et al . Increased risk of diabetes in inflammatory bowel disease patients: a nationwide population-based study in korea. J Clin Med. (2019) 8:343. 10.3390/jcm8030343
30.
Harper JW Sinanan MN Zisman TL . Increased body mass index is associated with earlier time to loss of response to infliximab in patients with inflammatory bowel disease. Inflamm Bowel Dis. (2013) 19:2118–24. 10.1097/MIB.0b013e31829cf401
31.
Aune D Sen A Schlesinger S Norat T Janszky I Romundstad P et al . Body mass index, abdominal fatness, fat mass and the risk of atrial fibrillation: a systematic review and dose-response meta-analysis of prospective studies. Eur J Epidemiol. (2017) 32:181–92. 10.1007/s10654-017-0232-4
Summary
Keywords
atrial fibrillation, inflammatory bowel disease, Mendelian randomization, single nucleotide polymorphisms, risk factor
Citation
Chen L and Jiang C (2021) Does Chronic Intestinal Inflammation Promote Atrial Fibrillation: A Mendelian Randomization Study With Populations of European Ancestry. Front. Cardiovasc. Med. 8:641291. doi: 10.3389/fcvm.2021.641291
Received
15 December 2020
Accepted
23 March 2021
Published
10 May 2021
Volume
8 - 2021
Edited by
Elsayed Z. Soliman, American University in Cairo, Egypt
Reviewed by
Raj Sewduth, VIB KU Leuven Center for Cancer Biology, Belgium; Henry J. Duff, University of Calgary, Canada
Updates
Copyright
© 2021 Chen and Jiang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: ChenYang Jiang cyjiang@zju.edu.cn
This article was submitted to Cardiovascular Genetics and Systems Medicine, a section of the journal Frontiers in Cardiovascular Medicine
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.