In the original article, there was a numerical error in the legend for Figure 2 as published. The correct legend appears below.
3D dataset image quality score stratified by ethnicity in the overall SABRE population [N = 1,001, (A)] and among men [N = 768, (B)] and women [N = 233, (C)] participants. Numbers are percentages.
In the original article, there was a numerical error for some measures in Table 4 as published. The corrected Table 4 appears below.
Table 4
| 2D | |
|---|---|
| LVIDd | 1,354 (94%) |
| LVIDs | 1,352 (94%) |
| IVSd | 1,354 (94%) |
| IVSs | 1,352 (94%) |
| PWd | 1,354 (94%) |
| PWs | 1,353 (94%) |
| LA diameter | 1,344 (93%) |
| LVOT diameter | 1,363 (95%) |
| Spectral-Doppler | |
| AV VTI | 1,355 (94%) |
| AV max velocity | 1,358 (94%) |
| E wave | 1,366 (95%) |
| A wave | 1,326 (92%) |
| Deceleration time | 1,360 (95%) |
| Tissue-Doppler | |
| e' septal | 1,359 (95%) |
| a' septal | 1,320 (92%) |
| s' septal | 1,362 (95%) |
| e' lateral | 1,360 (95%) |
| a' lateral | 1,321 (92%) |
| s' lateral | 1,361 (95%) |
| E/e' | 1,337 (93%) |
| 3DE | |
| QLAB EF, EDV, ESV | 924 (92%) |
| QLAB LV mass | 897 (89.6%) |
| 3D-STE* | |
| GLS, GCS | 529 (53%) |
| Twist and rotations | 529 (53%) |
| Vascular* | |
| cIMT | 1,331 (92.5%) |
| Central SBP and DBP | 1,316 (91.5%) |
| AIx, | 1,316 (91.5%) |
| Total CACS | 1,203 (83.7%) |
| PWV | 1,054 (91%) |
Feasibility of the cardiovascular measures in 1,438 SABRE participants.
See text in the manuscript for details.
AV, aortic valve; AIx, augmentation index; CACS, coronary artery calcification score; cIMT, common carotid intimal medial thickness, DBP, diastolic blood pressure; EDV, end-diastolic volume; ESV, end-systolic volume; EF, ejection fraction; GCS, global circumferential strain; GLS, global longitudinal strain; IVSd, diastolic interventricular septal thickness; IVSs, systolic interventricular septal thickness; LA, left atrial; LV, left ventricle; LVIDd, diastolic left ventricular internal diameter; LVIDs, systolic left ventricular internal diameter; LVOT, left ventricular outflow tract; PWTd, diastolic posterior wall thickness; PWTs, systolic posterior wall thickness; PWV, pulse wave velocity; SBP, systolic blood pressure; VTI, velocity time integral.
In the original article, there was a numerical error in Figure 1A as published. The corrected Figure 1A appears below.
Figure 1
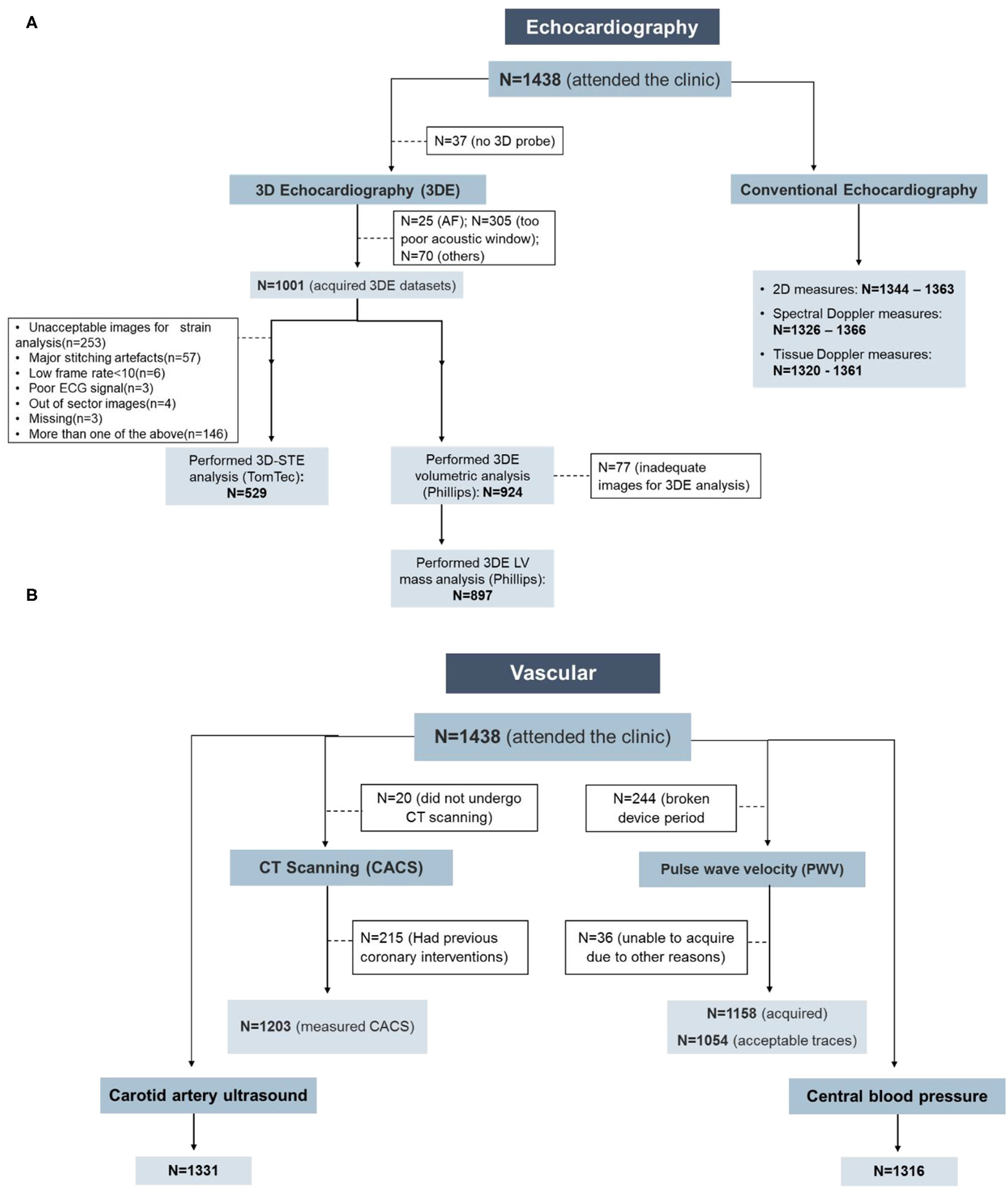
In the original article, there was an error. A correction has been made to Abstract, Results:
Conventional echocardiography and all vascular measurements showed high feasibility (>90% analyzable of clinic attendees), but 3D-echocardiography (3DE) and 3D-STE were less feasible (71% 3DE acquisition feasibility and 38% 3D-STE feasibility of clinic attendees).
In the original article, there was an error. A correction has been made to Results, Echocardiography, Paragraph Number 1:
3DE was acquired in 71% of all clinic attendees and, using QLAB, 924 (92%) had successful volumetric analysis and 897 (89.6%) had LV mass calculated. The difference in these numbers reflects difficulties in tracking the epicardium compared to the endocardium. Fifty three percent of those who had 3DE datasets had 3D deformation measurements by TomTec.
In the original article, there was an error. A correction has been made to Results, Echocardiography, Paragraph Number 2:
Broadly similar trends were observed in men (P < 0.0001, n=768) and women (P =0.005, n=233); however, in South Asians, there were more women with unreadable 3D images compared to men (67 vs. 58%, Figure 2).
In the original article, there was an error. A correction has been made to Discussion, Paragraph Number 1:
By contrast, 3DE had ~ 71% acquisition feasibility, while 3D-STE feasibility was highly influenced by image quality and only half of the datasets could be analyzed.
The authors apologize for this error and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Summary
Keywords
population-based, cardiovascular, imaging, echocardiography, vascular, feasibility, reproducibility
Citation
Al Saikhan L, Alobaida M, Bhuva A, Chaturvedi N, Heasman J, Hughes AD, Jones S, Eastwood S, Manisty C, March K, Ghosh AK, Mayet J, Oguntade A, Tillin T, Williams S, Wright A and Park C (2021) Corrigendum: Imaging Protocol, Feasibility, and Reproducibility of Cardiovascular Phenotyping in a Large Tri-Ethnic Population-Based Study of Older People: The Southall and Brent Revisited (SABRE) Study. Front. Cardiovasc. Med. 8:769050. doi: 10.3389/fcvm.2021.769050
Received
01 September 2021
Accepted
11 October 2021
Published
04 November 2021
Volume
8 - 2021
Edited by
Sebastian Kelle, Deutsches Herzzentrum Berlin, Germany
Reviewed by
Matthias Schneider, Charité – Universitätsmedizin Berlin, Germany; Allison G. Hays, Johns Hopkins University, United States
Updates
Copyright
© 2021 Al Saikhan, Alobaida, Bhuva, Chaturvedi, Heasman, Hughes, Jones, Eastwood, Manisty, March, Ghosh, Mayet, Oguntade, Tillin, Williams, Wright and Park.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lamia Al Saikhan lkalsaikhan@iau.edu.sa
This article was submitted to Cardiovascular Imaging, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.