Abstract
Background:
Hypertension (HTN) currently affects over 120 million Americans, in the United States (US). Thus, the implementation of evidence-based interventions (EBI) for blood pressure (BP) reduction is pivotal in minimizing this burden. We sought to evaluate evidence from published literature on the effectiveness of musical interventions for BP reduction within the US.
Methods:
A systematic review of studies that utilize music interventions to manage BP was conducted in October of 2022. An extensive search of several databases utilizing MeSH terms and relevant keywords was conducted for articles published through October 2022. An updated search was conducted in October 2023 to identify additional studies.
Results:
2,381 studies were screened for title/abstract relevancy. 1,885 studies were deemed irrelevant, and 495 studies were examined for full-text review; of which 384 were excluded due to being non-US-based. Overall, 25 studies were found where BP was the primary outcome and discussed musical interventions within the US. Of the 25 studies, 72% reported a significant decrease in BP after the administration of a musical intervention and only 28% reported the race and ethnicity of participants.
Conclusion:
There are limited studies that examine the effect of music interventions on BP reduction in the US, as a primary outcome. However, based on the evidence, musical interventions are effective for BP reduction. Moreover, the studies that were conducted in the US include a low percentage of high-risk racial and ethnic minority populations. Future EBI should target this underserved/high-burden group to improve disparity gaps within BP reduction via non-pharmacological means.
Systematic Review Registration:
Open Science Framework, doi: 10.17605/OSF.IO/4G3EB.
Introduction
Hypertension (HTN), characterized by consistently high blood pressure (BP) is a persistent condition that burdens global populations, including racial and ethnic groups in the United States. Individuals with HTN have an increased susceptibility to cardiovascular diseases such as heart disease and stroke (1). If left untreated, HTN can lead to further complications, which requires the use of innovative tailored interventions (i.e., musical interventions) (2) as a preventative measure to curtail the impact. HTN (defined as systolic and diastolic BP ≥ 130/80) (3) was the primary or contributing cause of death for about 500,000 individuals in the United States in 2018 (1), with certain racial and ethnic minority groups being disproportionately impacted (4–6). According to current estimates, the prevalence of HTN among Black adults is highest in the United States (54%), compared to Asian adults (39%), Hispanic/Latinx adults (36%), and non-Hispanic/Latinx White individuals (46%) (1). Moreover, racial and ethnic minorities also have lower HTN control rates [Black individuals (48.5%), Hispanic/Latinx (47.4%), and Asian individuals (43.5%)] compared to non-Hispanic/Latinx White individuals (55.7%)] (7). In urban areas, the disparity in HTN prevalence and control is even greater for racial and ethnic minority groups, which may be attributed to limited access to healthcare, inadequate/poor diet, exposure to harmful pollutants/carcinogens, and other structural barriers (3, 4). Existing research has shown that Black individuals develop HTN at an earlier age than White individuals (8) due to variations in the levels of risk factors for HTN. These factors include high sodium intake, physical inactivity, unhealthy diet, (9) obesity, and stress due to racial discrimination (10, 11).
The racial disparities in HTN rates and control are growing. The disproportionate rates of HTN among various racial and ethnic groups in the United States suggest the need to implement innovative evidence-based tailored interventions for BP control among these groups. Existing evidence has confirmed that music is an effective intervention for BP control, anxiety, depression, and other physiological conditions (12–14). Therefore, a non-pharmacological intervention such as music could be beneficial for patients with high BPs. There has also been documented success of BP being controlled using music in different countries around the world (13, 15, 16).
Although music is extensively used in other parts of the world, its implementation in the United States is severely limited despite the documented advantages to lower systolic BP (SBP), diastolic BP (DBP), and heart rate (HR) (14, 17). Clinical studies have underscored the remarkable efficacy of music listening in significantly reducing SBP, DBP, HR when compared to individuals or patients who did not receive any musical intervention (13). Moreover, incorporating variable tempo and strategic pauses during music sessions has been shown to elicit favorable effects on BP, further lowering SBP, DBP, and HR (13–15). However, it is noteworthy that these studies were not conducted within the United States and had a notably limited representation of participants from diverse racial backgrounds, who could particularly benefit from such evidence-based interventions. Furthermore, these studies lacked comprehensive reporting on the specific styles of music employed, leaving a critical gap in understanding the influence of personal musical preferences and cultural relevance on health outcomes, particularly within culturally diverse communities.
Recognizing this significant gap in the existing literature, the primary objective of this review is to synthesize available evidence regarding the impact of music interventions on BP reduction within United States populations. By garnering a comprehensive understanding of this therapeutic modality, this review aims to inform evidence-based practices aimed at reducing BP and enhancing HTN control within diverse communities.
Methods
The review protocol is registered in Open Science Framework (DOI 10.17605/OSF.IO/4G3EB).
Search strategy
We searched PubMed/Medline, Global Health, Embase, Web of Science, Music Index, CINAHL, and Wiley Cochrane Library. We searched the grey literature in OpenGrey, WorldCat, the New York Academy of Medicine (NYAM) Grey Literature database, and references of recently published systematic reviews from inception to date. We searched PubMed Central and Google Scholar using an abbreviated strategy to ensure comprehensiveness in searching. The original search was conducted from database inception to October 2022, and updated in October 2023.
The search strategy included terms related to music, musical interventions, BP, and United States. We conducted an in-depth search using the following parameters: (music interventions OR music therapy OR community music OR musical education OR music intervention OR music medicine OR music OR musical OR singing OR songs) AND (hypertension OR high blood pressure OR blood pressure OR blood pressure determination OR diastolic OR systolic OR pulse pressure OR arterial OR pulmonary wedge OR venous OR central venous OR portal) AND (adult OR adults OR elder*OR aged) AND (Appalachian Region OR Alabama OR Georgia OR Kentucky OR Maryland OR New York OR North Carolina OR Ohio OR Pennsylvania OR South Carolina OR Tennessee OR Virginia OR West Virginia OR Great Lakes Region OR Illinois OR Indiana OR Michigan OR Minnesota OR Wisconsin OR Mid-Atlantic Region OR Delaware OR District of Columbia OR Maryland OR New Jersey OR Midwestern United States OR Iowa OR Kansas OR Kentucky OR Missouri OR Nebraska OR North Dakota OR Oklahoma OR South Dakota OR Wisconsin OR New England OR Connecticut OR Maine OR Massachusetts OR New Hampshire OR Rhode Island OR Vermont OR Idaho OR Montana OR Washington OR Wyoming OR Pacific States OR Alaska OR California OR Hawaii OR Oregon OR Alabama OR Arkansas OR Florida OR Louisiana OR Mississippi OR Arizona OR Colorado OR Nevada OR New Mexico OR Texas OR Utah OR United States OR United States OR America* OR “U.S.” OR US).
Eligibility criteria for inclusion of studies
All citations found through the searches were downloaded to Covidence, a systematic review management tool, for title and abstract screening (18). Titles and abstracts of all articles were independently screened and rated by at least two reviewers to determine if the article meets the inclusion criteria. Following the double-screening protocol, articles were excluded if they did not contain information relevant to the systematic review objective. Articles were assessed for full-text eligibility. Eligible full-text articles were reviewed, and relevant information was extracted. The eligibility criteria included: (1) A musical intervention was used; (2) The study was conducted in the United States; (3) The study sample consisted of an Adult (18+) population; and (4) The study quantitatively measured the effect of the musical intervention on systolic and/or diastolic BP; (5) BP is a primary and or secondary outcome. Non-English studies were also included if translation was available. We excluded articles that did not meet any of the above criteria.
Data extraction
Full search strategies of all the databases were completed, yielding 3,799 articles in total. After duplicates were removed, 2,381 articles made it to title and abstract screening. 495 articles were included in the full-text review and examined against the review criteria. Of these, 438 articles were then excluded for various reasons including Retracted (n = 1), Abstract only (n = 4), Wrong outcome measured (n = 8), Wrong intervention implemented (n = 8), Wrong study design (n = 24), Non-US Based Studies (n = 384), Pediatric population (n = 12), Experiment consisted of patients playing rather than listening to music (n = 1), Non-numerical collection of BP (n = 4). 57 articles met the inclusion criteria and were examined for full-text data extraction (Figure 1).
Figure 1
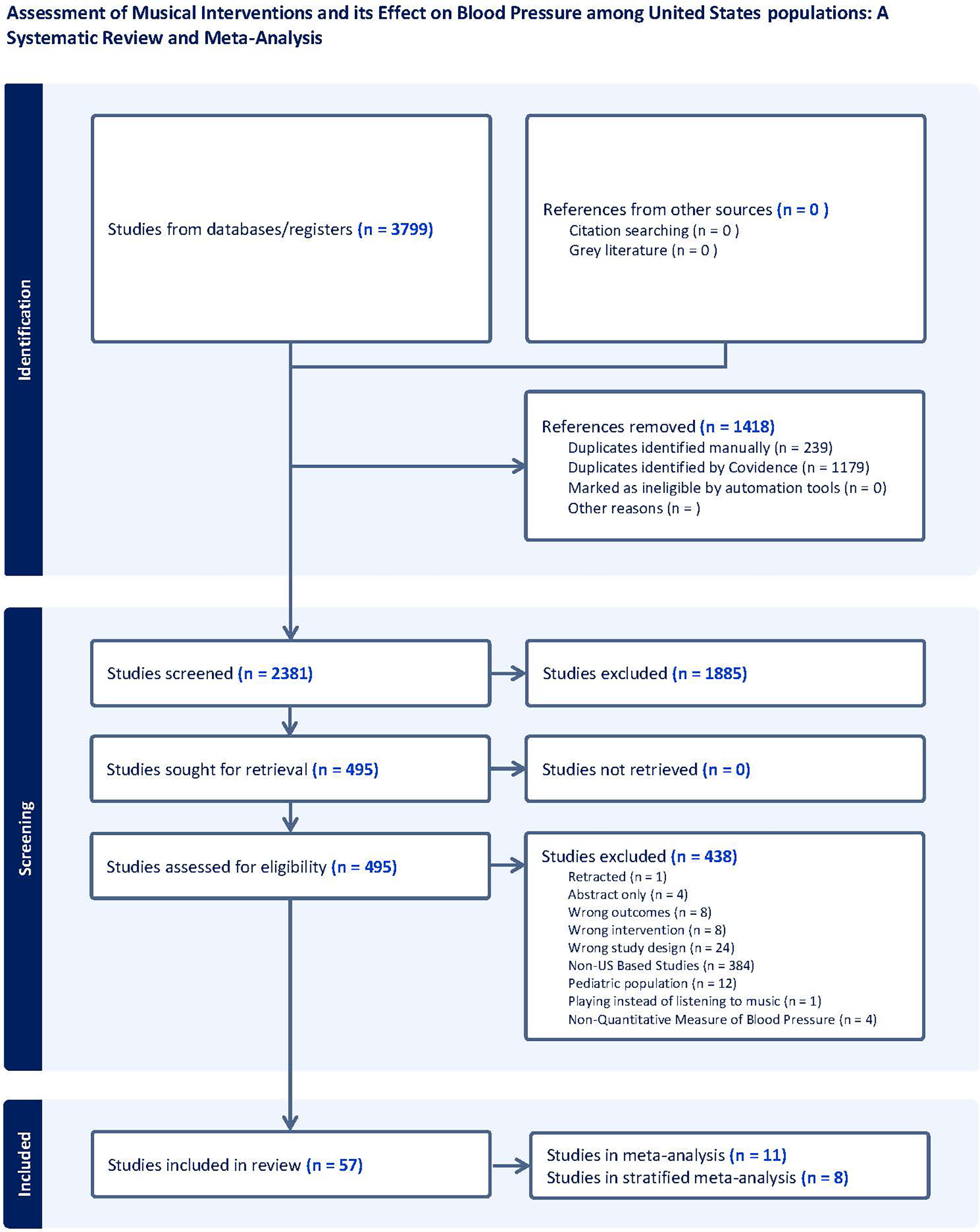
Prisma flowchart.
Quality of assessment
The risk of bias assessment was conducted using an independently designed Google Form based on the Ma et al. article that provides an assessment tool for each study design (19). Data from Covidence was extrapolated into the Google Form that incorporated the assessment for each study design. Studies that did not report study design were not included in the Risk of Bias Assessment.
Synthesis methods and effect measure
We conducted a meta-analysis of the effect of music on BP. All meta-analyses were conducted using RevManWeb (Cochrane collaboration). A random effects model was used due to the heterogeneous nature of the studies in terms of varying study populations and non-stratification of the study outcome. Subsequently, sub-group analysis was done for the two types of studies (RCTs and non-randomized studies). Heterogeneity was assessed using Cochrane's Q and degree of inconsistency (I2). The findings of the remaining studies were presented in a narrative format.
Results
Characteristics of studies
Of the 57 articles, 25 articles assessed BP as a primary outcome, and the remaining 32 articles evaluated BP as a secondary outcome. Below we provide findings from the studies that examined BP as a primary outcome. Additional information for the studies that provided BP as a secondary outcome can be found in Supplementary Tables S1, S2.
A total of 25 studies reported BP as the primary outcome (20–44) (Tables 1A–2B). An additional 32 studies were included in the review that reported BP as the secondary outcome (44–74). The studies that reported BP as the primary outcome utilized RCT designs (n = 15), Non-RCT designs (n = 5), Case-Control design (n = 1), Mixed Methods design (n = 1), Qualitative design (n = 1), and Not Reported Study Design (n = 2) (Table 1A). The average sample size varied across study designs. Sample size ranged from 16 to 855 participants for RCT designs, 40–203 participants for non-RCT designs, 10–101 participants for quasi-experimental designs, 14–234 participants for other designs, and 75–254 participants for studies where the design was not reported (Table 1A). The most represented age range across all studies was middle-aged (45–64) with 19 studies including this population. Of the 25 studies, 13 studies investigated physiological responses during a music intervention. In one study, the primary purpose was to examine the autonomic response during a musical intervention, and in 10 studies, the primary purpose was to examine the response or reaction to stress/coping/anxiety/trauma during a musical intervention. The primary objective of one study was to assess the BP effects of music therapy during exercise.
Table 1A
| Author (year) | Experimental condition vs. control | Study design | Sample size | Female # (%) | Male #/(%) |
|---|---|---|---|---|---|
| Allen (20) | Tasks performed during music-free vs. self-selected vs. investigator-selection music conditions | Within subjects laboratory experiment | 50 | 0 (0) | 50 (100) |
| Allen (21) | Cassette with 22 types of music vs. no music during intervention | Cohort studies/non-RCT prospective & retrospective | 40 | 30 (75) | 10 (25) |
| Bell (22) | MP3 player preloaded with preferred instrumental classical, jazz, or rock and roll music vs. no music | Double blind | 217 | 156 (72) | 61 (28) |
| Bittman (23) | Gospel music program (weekly 45-min vocal and instrumental sessions) vs. no music program | RCT | 71 | 58 (82) | 13 (18) |
| Blanchard (24) | Rock and roll music vs. classical music vs. no music | RCT | 254 | 130 (51) | 124 (49) |
| Cadigan (25) | Music through a headset from a hand-held compact disc player vs. no music | Randomized, two-group, pretest/post-test design | 140 | 40 (29) | 100 (71) |
| Camara (26) | A classically trained pianist by study surgeon played the piano while patients were being transported into the OR from the preoperative holding area vs. no music being played | Cohort studies/non-RCT prospective & retrospective | 203 | 137 (67) | 66 (33) |
| Chafin (27) | Was able to chose classical, jazz, or pop music vs. no music during mental arthmetic task | Did not report | 75 | 52 (69) | 23 (31) |
| Cheng (28) | Classical music vs. no music | RCT | 222 | 100 (45) | 122 (55) |
| Geden (29) | Experiment 1 easy-listening music vs. rock music vs. self-selected music vs. dissertation (placebo-attention) Experiment 2 musical selection while using self-generated imagery vs. self-generated imagery without music vs. musical selection while using guided imagery vs. guided imagery without music vs. no music and no imagery |
RCT | 102 | 102 (100) | 0 (0) |
| Ghetti (30) | Music therapy emotional-approach coping group vs. talk-based emotional-approach coping group vs. standard emotional-approach coping group | RCT | 37 | 13 (35) | 24 (65) |
| Hamel (31) | 20 min of music vs. no music | Quasi experimental design | 101 | 38 (38) | 63 (62) |
| Maldonado-Resto (32) | Post- music therapy vs. pre-music therapy | Quasi experimental design | 11 | 7 (63.6) | 4 (36.4) |
| Mandel (33) | DSME/T plus MARI CD VS DSME/T plus music therapy vs. DSME/T only | Mixed methods | 14 | 6 (43) | 8 (57) |
| Salamon (34) | “ZZ Top” rock music vs. classical music | RCT | 16 | Not reported | Not reported |
| Schuster (35) | Dialysis plus music vs. dialysis only | Case-control | 63 | 39 (62) | 24 (38) |
| Sendelbach (36) | Brief session of relaxation and music via headphone for 20 min twice per day vs. 20 min of rest only | RCT | 86 | 26 (30.2) | 60 (69.8) |
| Smolen (37) | Subj self-selected music through headphones vs. no music | RCT | 32 | 15 (47) | 17 (53) |
| Steelman (38) | Choice of music vs. no music | RCT | 43 | Not reported | Not reported |
| Tang (39) | Revitalizer II program (audio guided relaxation) vs. mozart group | RCT | 41 | 35 (85) | 6 (15) |
| Tyndall (40) | Live preferential music (LPM) vs. no LPM | RCT | 855 | 479 (56) | 376 (44) |
| Vanderark (41) | Listening to music from Holst's “The Planets” for 10 min vs. sitting in silence for 10 min | Did not report | 101 | 48 (48) | 53 (52) |
| Volkov (42) | Music in check in area vs. no music | Qualitative study | 234 | 145 (62) | 89 (38) |
| Walters (43) | Music when in surgical holding area vs. no music | RCT | 39 | 39 (100) | 0 (0) |
| Whipple (44) | Soothing music vs. stimulating music vs. no music | Quasi experimental design | 10 | 10 (100) | 0 (0) |
Characteristics of studies assessing change in blood pressure as the primary outcome.
Table 1B
| Author (Year) | Race/Ethnicity | Age Range | Study Setting/Location |
|---|---|---|---|
| Allen (20) | Not Reported | Adult 25–44; Middle Aged 45–64 | Hospital |
| Allen (21) | Not Reported | Middle Aged 45–64; Aged 65–79 | Ambulatory surgery Center |
| Bell (22) | Black | Young Adult 18–24 | Research Laboratory |
| Bittman (23) | Black | Adult 25–44; Middle Aged 45–64; Aged 65–79; Elderly 80+ | Religious/Church/Temple/Mosque |
| Blanchard (24) | Not Reported | Young Adult 18–24; Adult 25–44 | School |
| Cadigan (25) | Not Reported | Middle Aged 45–64; Aged 65–79 | Hospital |
| Camara (26) | Not Reported | Middle Aged 45–64; Aged 65–79; Elderly 80+ | Hospital |
| Chafin (27) | Not Reported | Young Adult 18–24 | University |
| Cheng (28) | Not Reported | Middle Aged 45–64; Aged 65–79 | Medical Center |
| Geden (29) | Not Reported | Young Adult 18–24; Adult 25–44 | Laboratory |
| Ghetti (30) | Not Reported | Middle Aged 45–64; Aged 65–79; Elderly 80+ | Hospital |
| Hamel (31) | Not Reported | Adult 25–44; Middle Aged 45–64; Aged 65–79 | Hospital |
| Maldonado-Resto (32) | White; Hispanic; Mixed Race | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79 | Clinic |
| Mandel (33) | Not Reported | Middle Aged 45–64; Aged 65–79 | Hospital |
| Salamon (34) | Asian | Young Adult 18–24; Adult 25–44 | School |
| Schuster (35) | Not Reported | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79; Elderly 80+ | Not Reported |
| Sendelbach (36) | Not Reported | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79; Elderly 80+ | Hospital |
| Smolen (37) | Not Reported | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79; Elderly 80+ | Hospital |
| Steelman (38) | Not Reported | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79 | Hospital |
| Tang (39) | White; Asian | Middle Aged 45–64; Aged 65–79; Elderly 80+ | Retirement Living Facility |
| Tyndall (40) | Not Reported | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79 | Emergency department |
| Vanderark (41) | White | Young Adult 18–24; Adult 25–44 | School |
| Volkov (42) | Not Reported | Young Adult: 18–24; Adult: 25–44; Middle Aged: 45–64; Aged: 65–79; Elderly: 80+ | Clinic |
| Walters (43) | Not Reported | Young Adult 18–24; Adult 25–44; Middle Aged 45–64; Aged 65–79 | Hospital |
| Whipple (44) | White; Asian | Young Adult 18–24; Adult 25–44; Middle Aged 45–64 | Laboratory |
Characteristics of studies assessing change in blood pressure as the primary outcome.
Table 2A
| Author (year) | Sample size (T/C) | Mean SBP (mmHg) at Baseline (SD) | Mean DBP (mmHg) at Baseline (SD) | Mean SBP (mmHg) at Endpoint (SD) | Mean DBP (mmHg) at Endpoint (SD) |
|---|---|---|---|---|---|
| Allen (20) | Not reported | Not reported | Not reported | Not reported | Not reported |
| Allen (21) | Music: 20 Non music: 20 |
Music: 158 (4.2) Non music: 160 (3.8) |
Music: 92 (1.4) Non music: 92 (1.4) |
Music: 123 (1.5) Non music: 141 (3.6) |
Music: 68 Non music: 75 |
| Bell (22) | Classical: 56 Jazz: 56 Rock: 56 control: 55 |
Not reported | Not reported | Not reported | Not reported |
| Bittman (23) | Music: 36 No music: 35 |
Music: 140.99 No music: 138.48 |
Music: 82.88 No music: 80.33 |
Music: 131.26 No music: 132 |
Music:79.87 No music: 79.06 |
| Blanchard (24) | No music: 82 Rock: 87 Classical: 85 |
No music: 118 Rock: 122 Classical: 131 |
No music: 58 Rock: 65 Classical: 68 |
No music: 147 Rock: 122 Classical: 131 |
No music: 108 Rock: 68 Classical: 69 |
| Cadigan (25) | Music: 75 No music: 65 |
Music: 114 (18) No music: 118 (14) |
Music: 60 (12) No music: 63 (14) |
Music: 112 (16) No music: 121 (18) |
Music: 57 (11) No music: 61 (11) |
| Camara (26) | Music: 115 No music: 88 |
Not reported | Not reported | Not reported | Not reported |
| Chafin (27) | Music: 75 No music: 75 |
Not reported | Not reported | Not reported | Not reported |
| Cheng (28) | Music: 112 No music: 120 |
Music: 141.94 (20.21) No music: 140.53 (18.80) |
Music: 70.93 (11.46) No music: 64.60 (10.24) |
Music: 135.72 (18.24) No music: 140.57 (20.46) |
Music: 66.23 (10.24) No music: 64.99 (7.70) |
| Geden (29) | Not reported | Not reported | Not reported | Not reported | Not reported |
| Ghetti (30) | Music: 11 No music: 9 |
Music: 121.91 (15.99) No music: 122.00 (19.72) |
Music: 63.82 (14.67) No music: 63.78 (9.35) |
Music: 129.36 (17.01) No music: 128.67 (23.21) |
Music: 68.55 (16.87) No music: 65.56 (16.04) |
| Hamel (31) | Music: 51 No music: 50 |
Music: 135.43 (21.82) No music: 133.44 (17.90) |
Music: 73.67 (12.51) No music: 72.50 (9.44) |
Music: 133.53 (19.79) No music: 139.72 (21.61) |
Music: 72.78 (10.91) No music: 75.52 (11.94) |
| Maldonado-Resto (32) | Paired design 11 | 120.4 (12.4) | 75.6 (7.2) | 116.4 (9.5) | 74.0 (7.0) |
| Mandel (33) | 14 pre and post | 119.86 (10.18) | Not reported | 114.71 (9.66) | 70.64 (12.28) |
| Salamon (34) | Classical: 8 Rock: 8 |
Classical: 119.875 (5.817) Rock: 109.0 (9.411) |
Not reported | Classical: 112.5 (3.854) Rock: 107.875 (9.978) |
Classical: 77.25 (5.418) Rock: 71.5 (6.782) |
| Schuster (35) | Music: 31 No music: 32 |
Music: 155.41 | Music: 97.50 | Music: 124.24 | Music: 68.46 |
| Sendelbach (36) | Music: 50 No music: 36 |
Music: 116 No music: 115 |
Music: 58 No music: 62 |
Music: 110 No music: 118 |
Music: 57 No music: 61 |
| Smolen (37) | Music: 16 No music: 16 |
Music: 135 No music: 122 |
Music: 77 No music: 74 |
Music: 116 No music: 126 |
Music: 69 No music: 74 |
| Steelman (38) | Music: 21 No music: 22 |
Music: 146.381 (22.418) No music: 139.591 (17.495) |
Music: 86.047 (13.048) No music: 80.182 (7.774) |
Music: 139.905 (19.491) No music: 139.864 (14.403 |
Music: 80.810 (11.272) No music: 81.591 (10.051) |
| Tang (39) | Revitalizer: 19 Mozart: 22 |
Revitalizer: 148 (21) Mozart: 145 (19) |
Revitalizer: 78 (11) Mozart: 74 (10) |
Revitalizer: 143 (17) Mozart: 139 (17) |
Revitalizer: 77 (14) Mozart: 71 (10) |
| Tyndall (40) | Music: 432 No music: 423 |
Music: 139.12 (26.87) No music: 135.36 (25.07) |
Music: 78.86 (16.89) No music: 78.50 (16.60) |
Not reported | Not reported |
| Vanderark (41) | Control biology: 38 Control music: 32 Experimental biology: 14 Experimental music: 17 |
Control biology: 115 (10) Control music: 116 (10) Experimental biology: 123 (12) Experimental music: 121 (9) |
Control biology: 77 (10) Control music: 77 (7) Experimental biology: 78 (9) Experimental music: 76 (9) |
Control biology: 114 (13) Control music: 116 (10) Experimental biology: 120 (12) Experimental music: 115 (8) |
Control biology: 75 (10) Control music: 77 (8) Experimental biology: 78 (10) Experimental music: 75 (9) |
| Volkov (42) | Music: 102 No music: 100 |
Not reported | Not reported | Not reported | Not reported |
| Walters (43) | VT: 13 M: 13 Control: 13 |
VT: 117.33 MT: 115.62 Control: 117.55 |
VT: 66.73 MT: 60.44 Control: 65.77 |
VT: 124.03 MT: 133.54 Control: 126.66 |
VT: 74.67 MT: 81.38 Control: 76.38 |
| Whipple (44) | Total: 10 | Not reported | Not reported | Not reported | Not reported |
Systolic and diastolic blood pressure across studies with blood pressure as the primary outcome.
Table 2B
| Author (Year) | Mean SBP (mmHg) Difference (SD) | Mean DBP (mmHg) Difference (SD) | Was Difference Statistically Significant? | Were patients with HTN Included? |
|---|---|---|---|---|
| Allen (20) | Not Reported | Not Reported | Yes | Not Reported |
| Allen (21) | Not Reported | Not Reported | Yes | No |
| Bell (22) | Not Reported | Not Reported | Yes | Not Reported |
| Bittman (23) | Not Reported | Not Reported | Yes SBP (In both groups when looking at baseline BP) | Yes |
| Blanchard (24) | Not Reported | Not Reported | Yes | Not Reported |
| Cadigan (25) | Not Reported | Not Reported | Yes | Not Reported |
| Camara (26) | Not Reported | Not Reported | Yes | Not Reported |
| Chafin (27) | Not Reported | Not Reported | Yes | Not Reported |
| Cheng (28) | Music: 6.21 (9.83) No music: −0.05 (11.24) |
Music: 4.70 (8.88) No music: −0.39 (5.75) |
Yes | Not Reported |
| Geden (29) | Not reported | Not reported | Not Reported | Not Reported |
| Ghetti (30) | Not Reported | Not Reported | Yes | Not Reported |
| Hamel (31) | Not Reported | Not Reported | Yes | Not Reported |
| Maldonado-Resto (32) | −4 | −1.6 | No | Yes |
| Mandel (33) | Not Reported | Not Reported | Yes | Not Reported |
| Salamon (34) | Not Reported | Not Reported | Yes | Not Reported |
| Schuster (35) | Not Reported | Not Reported | No | Not Reported |
| Sendelbach (36) | Not Reported | Not Reported | No | Not Reported |
| Smolen (37) | Not Reported | Not Reported | Yes | Not Reported |
| Steelman (38) | Not Reported | Not Reported | Yes | Not Reported |
| Tang (39) | Not Reported | Not Reported | Yes | Not Reported |
| Tyndall (40) | Music: 9.03 | Music: 5.86 | Yes | Not Reported |
| Vanderark (41) | Not Reported | Not Reported | No | Not Reported |
| Volkov (42) | Music: −29.26 No Music: −11.17 |
Music: −5.99 No Music: −3.98 |
Yes | Yes |
| Walters (43) | Vibrotactile Therapy: 6.7 Music Therapy: 17.92 Control: 9.11 |
VT: 7.94 MT: 20.94 Control: 10.61 |
No | Not Reported |
| Whipple (44) | Not Reported | Not Reported | No | Not Reported |
Mean blood pressure difference across studies with blood pressure as the primary outcome.
Intervention administration for studies reporting BP as a primary outcomes
Intervention durations differed across all 25 studies. Duration of musical interventions ranged from 10 min to 2.5 h; however, the number of times the intervention was administered on an hourly, weekly, or monthly basis varied across the studies. Only five studies reported administering the intervention twice or more. Among these five studies, there are variations in the period of the study duration with the range being 1 day to 1 year. Aside from these five studies, 14 studies reported providing the musical intervention once, and six studies did not report or were unclear on the duration of the musical interventions.
Overall, interventions were conducted in hospitals (n = 10), clinics (n = 2), schools (n = 3), laboratories (n = 3), a religious center (n = 1), a retirement living facility (n = 1), an emergency department (n = 1), an ambulatory surgery center (n = 1), and a medical center (n = 1). Several of the studies reviewed included a sample of patients undergoing medical procedures including Camara et al. (26), Cheng et al. (28), Hamel et al. (31), Schuster et al. (35), Sendelbach et al. (36), Smolen et al. (37), Steelman et al. (38), and Walters et al. (43) The musical interventions were done in the preoperative period (n = 3), during the procedure (n = 3), and in the postoperative period (n = 2), with the intervention in Allen et al. (21) administered during the preoperative, surgical, and postoperative periods. Mandel et al. (33), Tyndall et al. (40), and Volkov et al. (42) administered the musical intervention to a patient population not undergoing procedures. Blanchard et al. (24), Salamon et al. (34), and Vanderark et al. (41) utilized a student population. Whipple et al. (44) used a college graduate sample.
Listening to recorded music was an essential part of the interventions administered in all the studies reviewed. Some studies did have additional components in the intervention. Allen et al. (20) and Chafin et al. (27) asked participants to do a mental arithmetic task during the music listening. Bittman et al. (23) enrolled participants into a gospel music program that had both vocal and instrumental sessions. Blanchard et al. (24) instructed students to take a final examination during the music listening. Ghetti et al. (30) incorporated emotional support coaching into the intervention. Maldonado-Resto et al. (32) asked participants to exercise. Finally, Geden et al. (29) used guided imagery along with the music listening.
Ethnicity of participants in which BP was a primary outcome
Of the 25 studies, only 7 (28%) of studies reported the race and ethnicity of participants. 18 studies (72%) did not report the ethnic or racial background of participants. Of the studies that reported race and ethnicity, Bell et al. (22) and Bittman et al. (23) included only Black participants. Vanderark et al. (41) included only white participants. Salamon et al. (34) included solely Asian participants. Whipple et al. (44) and Tang et al. (39) included White and Asian participants. Maldonado-Resto et al. (32) included White and Hispanic/Latinx Participants. Overall, among the 7 studies that reported the race and ethnicity of participants, 4 Studies had White Participants, 3 Studies had Asian Participants, 2 Studies had Black Participants, and 1 Study had Hispanic/Latinx Participant.
Impact of diverse music genres on BP
Among the 25 studies, a diverse array of musical genres was employed as part of the interventions. These included Classical Music, Rock and Roll Music, Jazz Music, and live piano performances, among others. Notably, 8 studies assessed the effectiveness of classical music on reducing BP. Within these studies, 7 of them reported statistically significant reduction of BP measurements.
Several studies individually evaluated the efficacy of each music genre in reducing BP. For example, a study that included Classical music with a robust sample size was conducted by Bell and colleagues (22). In this study, the experimental group of 162 participants listened to music for 30 min from 1 of the 3 genres offered (Classical, Classic jazz, or Classic rock and roll). The intervention was administered 4 times per week for a total of 12 weeks. The control condition which consisted of 55 participants was instructed to not listen to any music and to sit at the table quietly for 30 min during the entire study duration. Following the intervention, participants measured their BP using an ambulatory BP machine and noted their post-intervention BP. The change in SBP in the experimental condition was statistically significant at 14.26 mmHg lower.
Live vs. recorded music on blood pressure reduction
Within the studies where BP was the primary outcome that was measured, several studies utilized live music as the medium for musical intervention compared to recorded music. Out of the 25 studies, 2 studies reported using live music as part of the musical intervention. Camara (26) measured the effect live piano music had on patients when they were being transported from the preoperative holding area to the operating room. Compared to the control group, it was found that the patients that listened to live piano music during their transport had BP measurements in the Operating Room that was significantly lower than what was measured in the pre-operating room. In Tyndall (40), patients who were in the emergency room were subjected to Live Preferential Music in the form of live guitar or live vocal music. When compared to patients who did not receive Live Preferential Music during their time in the Emergency Room, the patients who did receive the live music had statistically significant BP reductions, which was not seen in the control group.
Quantitative analysis of BP outcomes in music intervention studies
Tables 2A, 2B displays the quantitative SBP/DBP values reported by the studies where BP was the primary outcome. Among the 25 studies that reported BP as the primary outcome, the mean baseline SBP/DBP, endpoint SBP/DBP, and difference in SBP/DBP were not reported in six studies. The mean difference in SBP/DBP was not reported in seventeen studies (68%). Out of the 25 studies, 18 reported statistically significant differences (72%) in SBP and DBP measurements for participants in the intervention arm. When measured, BP was collected by a manual sphygmomanometer or by an automated BP monitor.
BP as a secondary outcome measure in music intervention
An additional 32 studies were included in the review that reported BP as the secondary outcome (45–75). These studies aimed to investigate the use of musical interventions on anxiety, psychological distress, pain, relaxation, and satisfaction. Anxiety was the primary outcome that was measured for most of the studies, and pain was a primary outcome for a few studies. Nevertheless, across the studies, BP was assessed as a secondary variable to gauge the effects on the primary outcome. Interestingly, the analysis revealed a significant reduction in BP in 10 out of the 32 studies (31%). Additional details for these studies can be found in Supplementary Tables S1, S2.
Risk of bias assessment
Overall, based on the results in Figure 2, there is a low risk of bias within the results that were reported by the studies where BP was a primary outcome of measurement. One major source of bias that may have affected the reporting of the outcomes is that most of the studies using the RCT design did not have allocation concealment, blinding of participants, or blinding of personnel. Consequently, this limits the anonymity of the participants to the research staff conducting the final physiological measurements. However, due to the inherent nature of the studies and the impracticality of implementing a placebo, achieving true blinding and allocation concealment may have been challenging if not impossible.
Figure 2
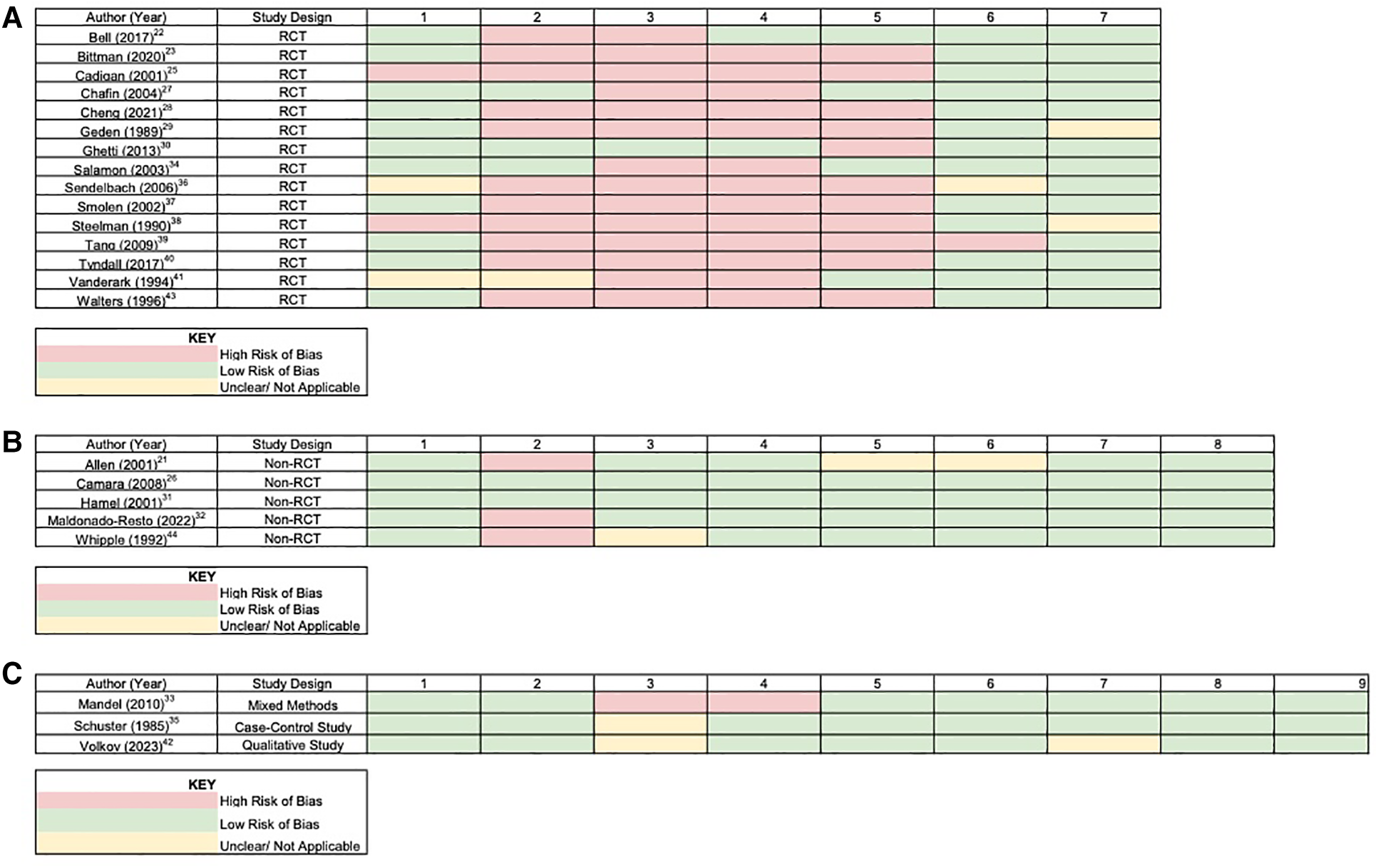
(A) Risk of bias table—RCT studies. Column numbers represent the criteria of the risk of bias assessment for randomized control trials: (1) random sequence generation; (2) allocation concealment; (3) blinding of participants; (4) blinding of personnel; (5) blinding of outcome assessors; (6) incomplete outcome data; (7) selective reporting. (B) Risk of bias table—non-RCT studies. Column numbers represent the criteria of the risk of bias assessment for non-randomized control trials: (1) clarity of cause and effect; (2) participants receiving in similar treatments other than intervention; (3) control group; (4) several measurements pre and post intervention; (5) complete follow-up; (6) outcomes compared similarly; (7) outcomes measured reliably; (8) appropriate statistical analysis. (C) Risk of bias table—other studies. Column numbers represent the criteria of the risk of bias assessment for non-randomized control trials: (1) clarity of cause and effect; (2) participants compared similarly; (3) participants receiving in similar treatments other than intervention; (4) control Group; (5) several measurements pre and post intervention; (6) complete Follow-up; (7) outcomes compared similarly; (8) outcomes measured reliably; (9) appropriate statistical analysis.
Meta-analysis findings
Among the 25 studies examining BP as a primary outcome, those that reported the effect of music intervention on systolic and diastolic BP, and provided sufficient data were included in the meta-analysis. The pooled results from eleven studies, with one study being split into two due to different participant arms, (n = 984; Experimental = 481 and Control = 503) reporting on the effect of music intervention regarding systolic BP were found to favor the music intervention. The results showed the pooled Mean Difference as −5.15 mmHg (95% CI −7.10 to −3.19) with greater evidence of heterogeneity between these studies (I2 = 79%, p-value = 0.00001). In contrast to these findings, the pooled results from these eleven studies reporting on the effect of music intervention for diastolic BP did not favor the music intervention. The results showed minimal reduction in DBP (Pooled Mean Difference −0.18 mmHg; 95% CI −1.49 to −1.14) with little evidence of heterogeneity between the studies (I2 = 41%, p-value = 0.79) (Figures 3A,B).
Figure 3
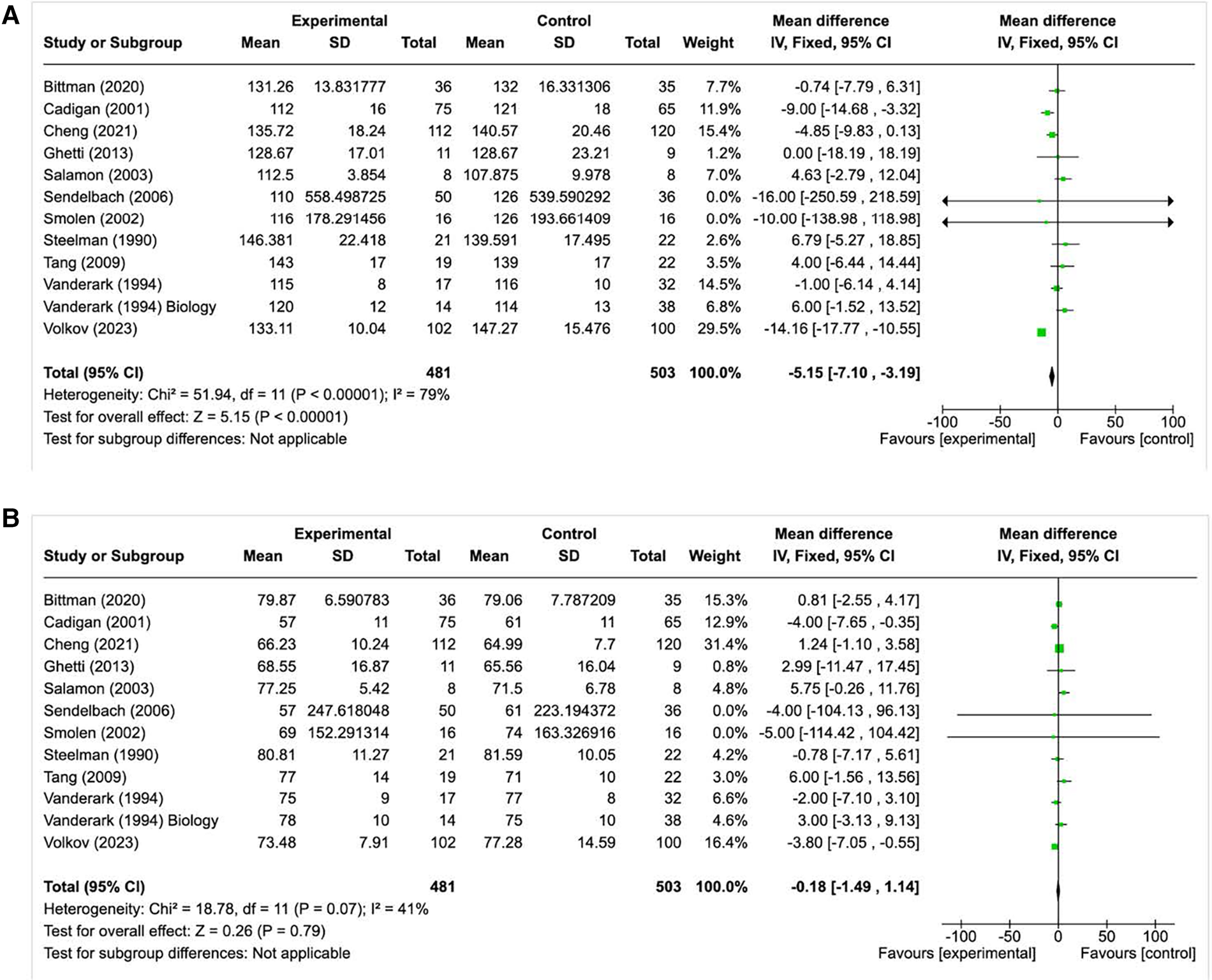
(A) Forest plot for studies highlighting the effect of music on systolic BP (BP as a primary outcome). (B) Forest plot for studies highlighting the effect of music on diastolic BP (BP as a primary outcome).
Discussion
Our investigation delved into the efficacy of musical interventions in lowering BP among adults in the United States. In studies where BP served as the primary outcome measurement, compelling evidence emerged, indicating a statistically significant reduction in BP through musical interventions. Among the 25 studies prioritizing BP as the primary outcome, a unique approach involved employing a single-encounter musical intervention to assess the impact of music on BP levels preceding either a medical procedure or an office visit (Table 1A). There were very few studies that examined the effect that musical interventions had on BP for a longer duration of time. Among the studies, the intervention duration ranged from 10 min to two and half hours. The findings of this systematic review underscore the necessity for additional research focusing on evidence-based musical interventions, specifically targeting BP as a primary outcome. In addition to this, 3 out of the 25 studies (12%) where BP was the primary outcome (Table 2B) reported that patients with HTN diagnosis were included in the sample. There is clear evidence of limited information on how musical interventions can help reduce BP in the United States. Such studies should also be extended over a longer duration, instead of a single encounter, to effectively ascertain their potential as non-pharmacological solutions for BP reduction and HTN control.
Within this systematic review, 18 of the studies neglected to report the racial or ethnic composition of their participants. Among the seven studies that did provide this information, there was a notable disparity: four studies predominantly included White participants, three studies had mostly Asian participants, two studies focused on Black participants, and one study centered on Hispanic/Latinx participants. The existing evidence suggests a serious gap in the reporting of demographic information for study participants. Additionally, fewer studies examined interventions for Black and Hispanic/Latinx communities, two ethnic groups that are disproportionately burdened by HTN in the United States. There is a clear paucity of studies that report racial and ethnic makeup. This stark underrepresentation of racial and ethnic minorities in the primary literature underscores the urgent need for future studies to encompass a more diverse sample to accurately assess the impact of music interventions on BP reduction among various racial and ethnic minority populations.
Furthermore, among the studies that included mixed racial and ethnic minority populations, three studies failed to stratify their results and report them based on population demographics. This oversight has significant implications, as it hinders our ability to discern any population-specific effects within the interventions studied. Given that high BP and related disorders disproportionately affect racial and ethnic minority populations, particularly Black and Hispanic/Latinx communities compared to Caucasian communities, it is imperative that medical interventions and policy decisions adequately account for and address these disparities.
To further examine how music can help reduce BP, specifically in Black and Hispanic/Latinx communities, tailored cost-effective, and feasible interventional studies are needed. This will allow for high BP to be addressed among this group, leading to long-term systematic changes to BP treatment protocol within the healthcare system. This will eventually allow healthcare systems to avoid multi-system downstream effects of uncontrolled high BP/HTN (e.g., stroke, kidney disease, etc.).
Based on the studies conducted where BP was the primary outcome, only two studies looked at the effect of live music on reducing BP. Within these studies, it was found that BP was reduced significantly in the intervention group compared to the control group which comprised of participants who did not receive the live music intervention. However, due to the limited number of studies that only looked at live music, we cannot draw conclusions about the overall effectiveness of live music vs. recorded music on reducing BP. In addition to this, the studies that used live music for their musical intervention had very short intervention durations, lasting at most 2 h. Based on this, it is evident that there is a need for studies to be conducted that encompass a longer intervention duration to evaluate the true potential of live music for BP reduction.
Music was also shown to be an effective non-pharmacological therapy when implemented over an extended duration. For the Bell et al. study (22), participants completed the musical intervention for 30 min each week over 12 weeks. In the Bittman et al. (23) study, the participants completed the musical intervention for 45 min every other week for a total duration of a year. The researchers found that the positive healthcare outcomes were due to participants being exposed to the repetitiveness and abundance of musical interventions. Therefore, by increasing the time to which music is listened to, a greater reduction in BP may be achieved. This finding is in alignment with evidence from a recent systematic review showing that multi-component interventions over a longer duration of time yield statistically significant decreases in BP (76). Intervention duration or music exposure dosage, and music type should be considered along with other proven therapies when designing evidence-based interventions to reduce BP among racial and ethnic minorities at the population level.
Among studies conducted within the United States, it has been shown that classical music reduced BP greater than other types of music. Bell et al. (22) was able to compare the different types of music on overall BP reduction. The authors concluded that music interventions were indeed effective in reducing BP. Moreover, the findings indicate that classical music notably outperformed other genres such as jazz and rock and roll in significantly reducing participants’ BP levels. This suggests a distinct advantage of classical music over jazz and rock and roll in its impact on BP reduction. Additionally, a study conducted by Chafin et al. (27) measured how various types of music can affect BP during a stressful arithmetic session. In comparison to pop music, jazz music, and no music; classical music was able to significantly reduce BP by 2.1 mmHg after the stressful task when compared to the baseline. This study shows that even within stressful situations, classical music still has the potential to significantly reduce BP compared to other types of music. In addition to this, it has been found that relaxing musical stimuli causes an increase in cardiac vagal modulation and cardiac vagal tone, which is not affected by other types of music (77). The findings from Bell et al. (22) and Chafin et al. (27) emphasize the therapeutic potential of a non-pharmacological intervention including classical music to help reduce BP due to the effect classical and relaxing music has on physiological parameters.
It is crucial to underscore the familiarity and effectiveness of utilizing music interventions for HTN control, as evidenced by successful implementation internationally. For example, researchers in Turkey (17) investigated the effects of Turkish classical music on HTN patients revealing significant positive effects. Notably, the study demonstrated a mean reduction of SBP of 13.00 mmHg in the experimental group, and 6.50 mmHg in the control group (17).
Similarly, a study in Brazil investigated the efficacy of a musical intervention in alleviating anxiety and improving vital parameters among individuals with head and neck cancer. The experimental group, exposed to a classical piece called “Spring” from The Four Seasons by Vivaldi (15) demonstrated remarkable reductions in BP, with a 95% decrease in systolic BP and a 55% decrease in diastolic BP, compared to the control group's reductions of 55% and 30%, respectively. Furthermore, a study conducted with hemodialysis patients in Italy found that live saxophone music therapy significantly reduced BP and enhanced quality of life, with statistical significance (p < .05) (78). These studies combined with the US-based studies that looked at classical music collectively accentuate the effectiveness of classical and culturally relevant musical interventions in reducing BP. Moreover, these studies shed light into possible musical interventions beneficial for racial and ethnic minority populations, offering promising avenues for long-term HTN management.
Based on our findings, studies conducted in the United States on music interventions and BP reduction specifically with racial and ethnic minority populations remains scarce. However, given the success of music interventions in other countries, there is an opportunity to replicate such interventions tailored specifically for high-risk racial and ethnic minority populations in the United States. For instance, a notable US-based study targeted stroke prevention, an outcome often associated with uncontrolled HTN, through a culturally tailored musical intervention, has had great success. William and colleagues introduced “Hip-Hop Stroke,” a program in central Harlem, New York City, designed to enhance stroke knowledge using culturally and age-appropriate music and dance alongside an interactive didactic stroke curriculum incorporating the FAST mnemonic (Facial droop, Arm weakness, Speech disturbance, Time to call 911). (79) The findings highlighted the effectiveness of this approach, as students retained stroke knowledge due to the cultural relevance of the music, particularly in a community with high stroke risk. Although this study did not investigate how music, as itself, helps to reduce BP, it highlights how music exposure is very feasible for a large population, allowing for future EBIs to follow a similar protocol.
Moving forward, it is imperative for future studies to focus on culturally appropriate musical interventions to control HTN for racial and ethnic minority populations in the United States and abroad, akin to the Hip-Hop stroke project. Exploring the role of cultural appropriateness of music in facilitating acceptance, uptake, and adherence to music interventions for BP management in culturally diverse communities holds promise for advancing HTN control efforts.
Conclusion
The findings derived from this systematic review strongly indicate the effectiveness of musical interventions in reducing BP among at-risk populations in the United States, particularly through the utilization of classical music either independently or in conjunction with other musical genres. However, a significant deficiency exists in the reporting of racial and ethnic data, a critical aspect necessary for informing culturally tailored interventions aimed at enhancing the acceptability, uptake, sustainability, and scalability of interventions. Addressing this gap is crucial for advancing health equity in HTN management.
Moreover, there is an urgent need for improvements in data reporting and transparency within research studies. Additionally, further research is warranted to thoroughly investigate the benefits of culturally appropriate musical interventions for BP reduction among racial and ethnic minority populations. Such endeavors are essential for optimizing HTN management strategies and fostering health equity across diverse communities.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
SM: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Writing – original draft, Writing – review & editing. JG: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. KP: Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. FI: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. DV: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. SN: Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. CR: Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. KB: Writing – review & editing. HC: Writing – review & editing. ST: Writing – review & editing. DA: Writing – review & editing. EA: Writing – review & editing. AC: Writing – review & editing. JO: Writing – review & editing. TO: Writing – review & editing. CC: Writing – review & editing. OW: Writing – review & editing. OO: Writing – review & editing. EP: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1405455/full#supplementary-material
Abbreviations
HTN, hypertension; BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; EBI, evidence-based interventions.
References
1.
CDC. Facts About Hypertension. Atlanta, Georgia: Centers for Disease Control and Prevention. Available online at:https://www.cdc.gov/bloodpressure/facts.htm(Accessed February 4 2024).
2.
American Music Therapy Association. What is Music Therapy?Silver Spring, MD: The American Music Therapy Association (2005). (Accessed February 5 2024).
3.
Whelton PK Carey RM Aronow WS Casey DE Jr Collins KJ Dennison Himmelfarb C et al 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. (2018) 71(19):e127–248. 10.1016/j.jacc.2017.11.006
4.
Hertz RP Unger AN Cornell JA Saunders E . Racial disparities in hypertension prevalence, awareness, and management. Arch Intern Med. (2005) 165(18):2098–104. 10.1001/archinte.165.18.2098
5.
Gyamfi J Butler M Williams SK Agyemang C Gyamfi L Seixas A et al Blood pressure control and mortality in US- and foreign-born blacks in New York city. J Clin Hypertens (Greenwich). (2017) 19(10):956–64. 10.1111/jch.13045
6.
Fei K Rodriguez-Lopez JS Ramos M Islam N Trinh-Shevrin C Yi SS et al Racial and ethnic subgroup disparities in hypertension prevalence, New York city health and nutrition examination survey, 2013–2014. Prev Chronic Dis. (2017) 14:160478. 10.5888/pcd14.160478
7.
Yoon SS Fryar CD Carroll MD . Hypertension Prevalence and Control among Adults: United States, 2011–2014. Hyattsville, MD: US Department of Health and Human Services, Centers for Disease Control and… (2015).
8.
Lackland DT . Racial differences in hypertension: implications for high blood pressure management. Am J Med Sci. (2014) 348(2):135–8. 10.1097/MAJ.0000000000000308
9.
Mills KT Stefanescu A He J . The global epidemiology of hypertension. Nat Rev Nephrol. (2020) 16(4):223–37. 10.1038/s41581-019-0244-2
10.
Paradies Y Ben J Denson N Elias A Priest N Pieterse A et al Racism as a determinant of health: a systematic review and meta-analysis. PLoS One. (2015) 10(9):e0138511. 10.1371/journal.pone.0138511
11.
Pascoe EA Smart Richman L . Perceived discrimination and health: a meta-analytic review. Psychol Bull. (2009) 135(4):531. 10.1037/a0016059
12.
Kamioka H Tsutani K Yamada M Park H Okuizumi H Koki Tsuruoka K et al Effectiveness of music therapy: a summary of systematic reviews based on randomized controlled trials of music interventions. Patient Prefer Adherence. (2014) 8:727–54. 10.2147/PPA.S61340
13.
do Amaral MA Neto MG de Queiroz JG Martins-Filho PR Saquetto MB Oliveira Carvalho V . Effect of music therapy on blood pressure of individuals with hypertension: a systematic review and meta-analysis. Int J Cardiol. (2016) 214:461–4. 10.1016/j.ijcard.2016.03.197
14.
Knight WE Rickard Ph DN . Relaxing music prevents stress-induced increases in subjective anxiety, systolic blood pressure, and heart rate in healthy males and females. J Music Ther. (2001) 38(4):254–72. 10.1093/jmt/38.4.254
15.
Firmeza MA Rodrigues AB Alencar Melo GA Freire de Aguiar MI da Cunha GH de Oliveira PP et al Control of anxiety through music in a head and neck outpatient clinic: a randomized clinical trial. Revista Da Escola De Enfermagem Da Usp. (2017) 51. 10.1590/S1980-220X2016030503201
16.
Bernardi L Porta C Sleight P . Cardiovascular, cerebrovascular, and respiratory changes induced by different types of music in musicians and non-musicians: the importance of silence. Heart. (2006) 92(4):445–52. 10.1136/hrt.2005.064600
17.
Bekiroğlu T Ovayolu N Ergün Y Ekerbiçer H . Effect of Turkish classical music on blood pressure: a randomized controlled trial in hypertensive elderly patients. Complement Ther Med. (2013) 21(3):147–54. 10.1016/j.ctim.2013.03.005
18.
Covidence Systematic Review Software. Melbourne, Australia: Veritas Health Innovation. Available online at:www.covidence.org
19.
Ma L-L Wang Y-Y Yang Z-H Huang D Weng H Zeng X-T . Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better?Mil Med Res. (2020) 7:7. 10.1186/s40779-020-00238-8
20.
Allen K Blascovich J . Effects of music on cardiovascular reactivity among surgeons. JAMA. (1994) 272(11):882–84. 10.1001/jama.1994.03520110062030
21.
Allen K Golden LH Izzo JL Jr Ching MI Forrest A Niles CR et al Normalization of hypertensive responses during ambulatory surgical stress by perioperative music. Psychosom Med. (2001) 63(3):487–92. 10.1097/00006842-200105000-00019
22.
Bell TP Akombo DO . Long-term music-listening's effects on blood pressure, heart rate, anxiety, and depression. J Altern Med Res. (2017) 9(1):57–64.
23.
Bittman B Poornima I Smith MA Heidel RE . Gospel music: a catalyst for retention, engagement, and positive health outcomes for African Americans in a cardiovascular prevention and treatment program. Adv Mind Body Med. (2020) 34(1):8–16.
24.
Blanchard BE . The effect of music on pulse-rate, blood-pressure and final exam scores of university students. J Sports Med Phys Fitness. (1979) 19(3):305–8.
25.
Cadigan ME Caruso NA Haldeman SM McNamara ME Noyes DA Spadafora MA et al The effects of music on cardiac patients on bed rest. Prog Cardiovasc Nurs. (2001) 16(1):5–13. 10.1111/j.0889-7204.2001.00797.x
26.
Camara JG Ruszkowski JM Worak SR . The effect of live classical piano music on the vital signs of patients undergoing ophthalmic surgery. Medscape J Med. (2008) 10(6):149.
27.
Chafin S Roy M Gerin W Christenfeld N . Music can facilitate blood pressure recovery from stress. Br J Health Psychol. (2004) 9(Pt 3):393–403. 10.1348/1359107041557020
28.
Cheng H Breitbart G Giordano L Richmand D Wong G . Music in the wound care center: effects on anxiety levels and blood pressure measurements in patients receiving standard care. Wound Manag Prev. (2021) 67(4):16–22. 10.25270/wmp.2021.4.1622
29.
Geden EA Lower M Beattie S Beck N . Effects of music and imagery on physiologic and self-report of analogued labor pain. Nurs Res. (1989) 38(1):37–41. 10.1097/00006199-198901000-00008
30.
Ghetti CM . Effect of music therapy with emotional-approach coping on preprocedural anxiety in cardiac catheterization: a randomized controlled trial. J Music Ther. (2013) 50(2):93–122. 10.1093/jmt/50.2.93
31.
Hamel WJ . The effects of music intervention on anxiety in the patient waiting for cardiac catheterization. Intensive Crit Care Nurs. (2001) 17(5):279–85. 10.1054/iccn.2001.1594
32.
Maldonado-Resto JK . Utilizing Music Therapy During an Exercise Program to Reduce Blood Pressure and Depressive Symptoms in Adult Patients with Cardiovascular Diseases. Ann Arbor, MI: ProQuest Information & Learning (2021).
33.
Mandel SE Hanser SB Ryan LJ . Effects of a music-assisted relaxation and imagery compact disc recording on health-related outcomes in cardiac rehabilitation. Music Ther Perspect. (2010) 28(1):11–21. 10.1093/mtp/28.1.11
34.
Salamon E Bernstein SR Kim S-A Kim M Stefano GB . The effects of auditory perception and musical preference on anxiety in naive human subjects. Med Sci Monit. (2003) 9(9):CR396-9.
35.
Schuster BL . The effect of music listening on blood-pressure fluctuations in adult hemodialysis-patients. J Music Ther. (1985) 22(3):146–53. 10.1093/jmt/22.3.146
36.
Sendelbach SE Halm MA Doran KA Miller EH Gaillard P . Effects of music therapy on physiological and psychological outcomes for patients undergoing cardiac surgery. J Cardiovasc Nurs. (2006) 21(3):194–200. 10.1097/00005082-200605000-00007
37.
Smolen D Topp R Singer L . The effect of self-selected music during colonoscopy on anxiety, heart rate, and blood pressure. Appl Nurs Res. (2002) 15(3):126–36. 10.1053/apnr.2002.34140
38.
Steelman VM . Intraoperative music therapy. Effects on anxiety, blood pressure. Aorn j. (1990) 52(5):1026–34. 10.1016/s0001-2092(07)69164-9
39.
Tang H-Y Harms V Speck SM Vezeau T Jesurum JT . Effects of audio relaxation programs for blood pressure reduction in older adults. Eur J Cardiovasc Nurs. (2009) 8(5):329–36. 10.1016/j.ejcnurse.2009.06.001
40.
Tyndall J Kerrigan M Baker Chowdhury MA Elie M-C Gul S Balakrishnan MP et al Music in emergent settings: a randomized controlled trial. Ann Emerg Med. (2017) 70(4):S167. 10.1016/j.annemergmed.2017.07.306
41.
Vanderark SD Ely D . University biology and music majors’ emotional ratings of musical stimuli and their physiological correlates of heart, rate, finger temperature, and blood pressure. Percept Mot Skills. (1994) 79(3 Pt 1):1391–7. 10.2466/pms.1994.79.3.1391
42.
Volkov R Volkova N . Effects of listening to music during blood pressure check in primary care clinic settings. Am J Lifestyle Med. (2023). 10.1177/15598276231181073
43.
Walters CL . The psychological and physiological effects of vibrotactile stimulation, via a somatron, on patients awaiting scheduled gynecological surgery. J Music Ther. (1996) 33(4):261–87. 10.1093/jmt/33.4.261
44.
Whipple B Glynn NJ . Quantification of the effects of listening to music as a noninvasive method of pain control. Sch Inq Nurs Pract. (1992) 6(1):43–58.
45.
Alam M Roongpisuthipong W Kim NA Goyal A Swary JH Brindise RT et al Utility of recorded guided imagery and relaxing music in reducing patient pain and anxiety, and surgeon anxiety, during cutaneous surgical procedures: a single-blinded randomized controlled trial. J Am Acad Dermatol. (2016) 75(3):585–89. 10.1016/j.jaad.2016.02.1143
46.
Allen MT Bocek CM Burch AE . Gender differences and the relationships of perceived background stress and psychological distress with cardiovascular responses to laboratory stressors. Int J Psychophysiol. (2011) 81(3):209–17. 10.1016/j.ijpsycho.2011.06.013
47.
Aragon D Farris C Byers JF . The effects of harp music in vascular and thoracic surgical patients. Altern Ther Health Med. (2002) 8(5):52–4.
48.
Augustin P Hains AA . Effect of music on ambulatory surgery patients’ preoperative anxiety. Aorn J. (1996) 63(4):750. 10.1016/s0001-2092(06)63126-8
49.
Barnason S Zimmerman L Nieveen J . The effects of music interventions on anxiety in the patient after coronary artery bypass grafting. Heart Lung. (1995) 24(2):124–32. 10.1016/s0147-9563(05)80007-x
50.
Chen Y Hawkins J . Effects of music listening to reduce preprocedural dental anxiety in special needs patients. Complement Ther Clin Pract. (2021) 42:101279. 10.1016/j.ctcp.2020.101279
51.
Chiasson AM Linda Baldwin A McLaughlin C Cook P Sethi G . The effect of live spontaneous harp music on patients in the intensive care unit. Evid Based Complement Alternat Med. (2013) 2013:428731. 10.1155/2013/428731
52.
Conrad C Niess H Jauch K-W Bruns CJ Hartl W Welker L . Overture for growth hormone: requiem for interleukin-6?Crit Care Med. (2007) 35(12):2709–13. 10.1097/01.CCM.0000291648.99043.B9
53.
Dubois JM Bartter T Pratter MR. Music improves patient comfort level during outpatient bronchoscopy. Chest. (1995) 108(1):130. 10.1378/chest.108.1.129
54.
Eckhouse DR Hurd M Cotter-Schaufele S Sulo S Sokolowski M Barbour L . A randomized controlled trial to determine the effects of music and relaxation interventions on perceived anxiety in hospitalized patients receiving orthopaedic or cancer treatment. Orthop Nurs. (2014) 33(6):342–51. 10.1097/NOR.0000000000000098
55.
Ferrer AJ . The effect of live music on decreasing anxiety in patients undergoing chemotherapy treatment. J Music Ther. (2007) 44(3):242–55. 10.1093/jmt/44.3.242
56.
Gendolla GH Abele AE Krüsken J . The informational impact of mood on effort mobilization: a study of cardiovascular and electrodermal responses. Emotion. (2001) 1(1):12–24. 10.1037/1528-3542.1.1.12
57.
Gosselin KP Holland B Mulcahy A Williamson S Widacki A . Music for anxiety reduction and performance enhancement in nursing simulation. Clin Simul Nurs. (2016) 12(1):16–23. 10.1016/j.ecns.2015.12.002
58.
Halbert JD van Tuyll DR Purdy C Hao G Cauthron S Crookall C et al Low frequency music slows heart rate and decreases sympathetic activity. Music Med. (2018) 10(4):180–85. 10.47513/mmd.v10i4.614
59.
Hanser SB Bauer-Wu S Kubicek L Healey M Manola J Hernandez M et al Effects of a music therapy intervention on quality of life and distress in women with metastatic breast cancer. J Soc Integr Oncol. (2006) 4(3):124. 10.2310/7200.2006.014
60.
Haun M Mainous RO Looney SW . Effect of music on anxiety of women awaiting breast biopsy. Behav Med. (2001) 27(3):127–32. 10.1080/08964280109595779
61.
Hayes A Buffum M Lanier E Rodahl E Sasso C . A music intervention to reduce anxiety prior to gastrointestinal procedures. Gastroenterol Nurs. (2003) 26(4):145–9. 10.1097/00001610-200307000-00002
62.
Krumhansl CL . An exploratory study of musical emotions and psychophysiology. Can J Exp Psychol. (1997) 51(4):336–53. 10.1037/1196-1961.51.4.336
63.
Kshettry VR Carole LF Henly SJ Sendelbach S Kummer B . Complementary alternative medical therapies for heart surgery patients: feasibility, safety, and impact. Ann Thorac Surg. (2006) 81(1):201–5. 10.1016/j.athoracsur.2005.06.016
64.
Liang Z Ren D Choi J Happ MB Hravnak M Hoffman LA . Music intervention during daily weaning trials-a 6 day prospective randomized crossover trial. Complement Ther Med. (2016) 29:72–7. 10.1016/j.ctim.2016.09.003
65.
Mandel SE Davis BA Secic M . Effects of music therapy and music-assisted relaxation and imagery on health-related outcomes in diabetes education: a feasibility study. Diabetes Educ. (2013) 39(4):568–81. 10.1177/0145721713492216
66.
Rafer L Austin F Frey J Mulvey C Vaida S Prozesky J . Effects of jazz on postoperative pain and stress in patients undergoing elective hysterectomy. Adv Mind Body Med. (2015) 29(1):6–11.
67.
Rao SSC Hatfield RA Suls JM Chamberlain MJ . Psychological and physical stress induce differential effects on human colonic motility. Am J Gastroenterol. (1998) 93(6):985–90. 10.1016/S0002-9270(98)00174-9
68.
Ripley L Christopoulos G Michael TT Alomar M Rangan BV Roesle M . Randomized controlled trial on the impact of music therapy during cardiac catheterization on reactive hyperemia index and patient satisfaction: the functional change in endothelium after cardiac catheterization, with and without music therapy (FEAT) study. J Invasive Cardiol. (2014) 26(9):437–42.
69.
Schandert LC Affronti ML Prince MS Schneider SM . Music intervention: nonpharmacologic method to reduce pain and anxiety in adult patients undergoing bone marrow procedures. Clin J Oncol Nurs. (2021) 25(3):314–20. 10.1188/21.Cjon.314-320
70.
Shultis CL . Effects of Music Therapy vs. Music Medicine on Physiological and Psychological Parameters of Intensive Care Patients: A Randomized Controlled Trial. Ann Arbor, MI: ProQuest Information & Learning (2013). 10.34944/dspace/2367
71.
Strauser JM . The effects of music versus silence on measures of state anxiety, perceived relaxation, and physiological responses of patients receiving chiropractic interventions. J Music Ther. (1997) 34(2):88–105. 10.1093/jmt/34.2.88
72.
Tsivian M Qi P Kimura M Chen VH Chen SH Gan TJ et al The effect of noise-cancelling headphones or music on pain perception and anxiety in men undergoing transrectal prostate biopsy. Urology. (2012) 79(1):32–6. 10.1016/j.urology.2011.09.037
73.
Vanderboom TL Arcari PM Duffy ME Somarouthu B Rabinov JD Yoo AJ et al Effects of a music intervention on patients undergoing cerebral angiography: a pilot study. J Neurointerv Surg. (2012) 4(3):229–33. 10.1136/neurintsurg-2011-010052
74.
Wang SM Kulkarni L Dolev J Kain ZN . Music and preoperative anxiety: a randomized, controlled study. Anesth Analg. (2002) 94(6):1489–94. 10.1097/00000539-200206000-00021
75.
White JM . Effects of relaxing music on cardiac autonomic balance and anxiety after acute myocardial infarction. Am J Crit Care. (1999) 8(4):220–30. 10.4037/ajcc1999.8.4.220
76.
Gyamfi J Vieira D Iwelunmor J Watkins BX Williams O Peprah E et al Assessing descriptions of scalability for hypertension control interventions implemented in low-and middle-income countries: a systematic review. PLoS One. (2022) 17(7):e0272071. 10.1371/journal.pone.0272071
77.
Raglio A Maestri R Robbi E Pierobon A La Rovere MT Pinna GD . Effect of algorithmic music listening on cardiac autonomic nervous system activity: an exploratory, randomized crossover study. J Clin Med. (2022) 11(19):5738. 10.3390/jcm11195738
78.
Burrai F Lupi R Luppi M Micheluzzi V Donati G Lamanna G et al Effects of listening to live singing in patients undergoing hemodialysis: a randomized controlled crossover study. Biol Res Nurs. (2019) 21(1):30–8. 10.1177/1099800418802638
79.
Williams O Noble JM . “Hip-hop” stroke—a stroke educational program for elementary school children living in a high-risk community. Stroke. (2008) 39(10):2809–16. 10.1161/STROKEAHA.107.513143
Summary
Keywords
hypertension, music, USA, BP reduction, musical interventions, racial/ethnic minorities
Citation
Meda S, Gyamfi J, Patel K, Islam F, Vieira D, Nyame S, Ruan C, Boradia K, Chhetri H, Thunga S, Adenikinju D, Amesimeku E, Cohen A, Opeyemi J, Ojo T, Chirinos C, Williams O, Ogedegbe O and Peprah E (2024) Assessment of musical interventions and its effect on blood pressure among United States populations: a systematic review and meta-analysis. Front. Cardiovasc. Med. 11:1405455. doi: 10.3389/fcvm.2024.1405455
Received
27 March 2024
Accepted
20 June 2024
Published
15 October 2024
Volume
11 - 2024
Edited by
Nizamettin Aydin, Istanbul Technical University, Türkiye
Reviewed by
Sadik Kara, Durham Technical Community College, United States
Ahmet Elbir, Yıldız Technical University, Türkiye
Updates
Copyright
© 2024 Meda, Gyamfi, Patel, Islam, Vieira, Nyame, Ruan, Boradia, Chhetri, Thunga, Adenikinju, Amesimeku, Cohen, Opeyemi, Ojo, Chirinos, Williams, Ogedegbe and Peprah.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Shreya Meda sm9223@nyu.edu
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.