Abstract
A Cardiac College for Women curriculum was developed to address the dearth of women-focused cardiac rehabilitation (CR) education. This study investigated: (1) patient utilization of the education; (2) acceptability and applicability of the education; as well as (3) patient and CR providers’ experiences implementing it. This was a multi-site, mixed-methods study. After baseline assessments at an academic CR program in two Canadian provinces, the 12 weekly 30 min structured in-person group education sessions were led by staff in the relevant discipline, with supporting online videos and written materials. Women reported their engagement with the education in weekly diaries, and completed a survey post-program. Semi-structured virtual interviews were held with willing participants and staff delivering the intervention. Transcripts were analyzed concurrently by two researchers independently via NVIVO using text condensation, followed by consensus reconciliation and multi-source validation. Forty patients participated in the women-focused education program, with 28 completing weekly diaries and 36 post-intervention surveys. Participants attended 80% of sessions (67%–89%). They spent an average of 30 min/week engaging additionally with the online education, with 83% rating the weekly content applicable (73%–100%). Overall acceptability was rated 4.3 ± 1.7/5. Twelve patients and 5 staff participated in interviews. Four themes were identified: contextual considerations, staffing and implementation issues, valued aspects, and suggestions for improvement. In conclusion, Cardiac College for Women was established as highly acceptable and applicable to patients, supporting their self-management. The women-specific CR education materials were also established as readily implementable by CR staff.
1 Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide (1), with 20% of individuals dying after an initial cardiac event (2). Due to advances in care improving survival, CVD is also one of the most prevalent conditions globally (3). Given that 40% of patients experience another cardiovascular event within three years (2, 4), prioritizing secondary prevention is crucial. Cardiac rehabilitation (CR) is an established outpatient model of comprehensive secondary prevention composed of risk factor modification, exercise training, nutrition counselling, psychosocial management, and notably, patient education (5). Patients are empowered through education to recognize and respond to cardiac symptoms, as well as to actively manage their cardiovascular risk factors, to reduce their risk of further sequelae (6). Robust evidence has demonstrated that CR reduces mortality and morbidity (5, 7), as well as improves functional capacity (8) and quality of life (9).
Despite its benefits, few women access CR (10, 11), and where they do, often they do not achieve the same gains as men (12). Reasons are multifactorial, and include transportation barriers, family obligations, as well as finding exercise to be painful or tiring, often due to their different forms of CVD or burden of comorbidities when compared to men (13). Resources to optimize secondary prevention for women are needed. Indeed, an international clinical practice guideline advocating for women-focused CR was recently published, recommending the tailoring of education to target women's needs (14).
Accordingly, our group rigorously developed Cardiac College for Women, which offers a comprehensive CR curriculum available open access in multiple formats (15). Preliminary evaluation confirmed its efficacy in improving cardiac knowledge and clinically-prognostic outcomes, such as functional capacity (16). Alongside the prospective evaluation, its implementation was also investigated. The objectives were to: (1) assess degree of utilization of Cardiac College for Women education materials throughout CR; (2) investigate women participants’ perceptions of the acceptability, applicability and usability of the tailored education and their satisfaction with it; and (3) explore CR provider's experiences adopting, implementing, and sustaining delivery of the education curriculum in their programs.
2 Materials and methods
2.1 Design
This was a multi-site, mixed-methods study (protocol registered at: https://osf.io/b2jz3/). Mixed-methods were applied to achieve contextualization, validation and triangulation of findings, enhance interpretation of findings, and achieve comprehensive understanding of the research questions. An exploratory, sequential design was used for this two-staged study (17): the first stage comprised a prospective, uncontrolled sub-study, and a subsequent qualitative study. Data were collected between September 2023 and March 2024.
Study approval was obtained from the University Health Network (Toronto, Canada: 23-5427) and Centre Intégré de Santé et the Services Sociaux de Claudiére-Appalaches (Lévis, Canada: 2024-1076). All participants provided written informed consent.
2.2 Intervention: women-focused CR education
The women-focused education intervention for this study—Cardiac College for Women—was rigorously developed following a user needs assessment, and considering health literacy as well as principles of adult education, as summarized elsewhere (15). It was delivered within a 12-week in-person women's-only CR class (schedule of topics shown in Table 1), with education and individually-prescribed supervised exercise at each session (16).
Table 1
| Weekly topic | In-person education session | Supportive online written materials | Supportive online videos | Optional website information | Applicability | |
|---|---|---|---|---|---|---|

|
Orientation | 19 (70%) | 18 (67%) 3 (11%) |
20 (74%) 1 (4%) |
21 (81%) | 20 (74%) 6 (22%) |

|
About your heart | 22 (82%) | 17 (63%) 0 (0%) |
19 (70%) 2 (7%) |
19 (73%) | 22 (82%) 3 (11%) |

|
Cardiovascular risk factors | 22 (82%) | 18 (67%) 1 (4%) |
20 (74%) 3 (11%) |
18 (69%) | 23 (85%) 3 (11%) |

|
Cardiac medications | 24 (83%) | 19 (66%) 2 (7%) |
18 (64%) 4 (14%) |
21 (75%) | 25 (89%) 1 (4%) |

|
Exercise (aerobic) | 22 (79%) | 19 (73%) 3 (12%) |
23 (85%) 2 (7%) |
21 (81%) | 26 (100%) 0 (0%) |

|
Exercise (safety) | 22 (88%) | 18 (72%) 3 (12%) |
18 (72%) 1 (4%) |
18 (72%) | 21 (88%) 2 (8%) |

|
Exercise (resistance training) | 21 (81%) | 19 (73%) 1 (4%) |
17 (65%) 2 (8%) |
20 (77%) | 25 (96%) 1 (4%) |

|
Nutrition (Mediterranean pattern) | 23 (89%) | 13 (54%) 2 (8%) |
19 (73%) 2 (8%) |
19 (73%) | 19 (73%) 6 (23%) |

|
Nutrition (Healthy relationship with food) | 18 (67%) | 16 (64%) 2 (8%) |
21 (78%) 1 (4%) |
21 (78%) | 20 (74%) 5 (19%) |

|
Psychosocial health (Depression and anxiety) | 21 (81%) | 15 (58%) 2 (8%) |
18 (69%) 0 (0%) |
18 (69%) | 20 (77%) 1 (4%) |

|
Psychosocial health (Relationships and self-management while juggling multiple roles) | 18 (78%) | 12 (52%) 4 (17%) |
19 (79%) 1 (4%) |
16 (70%) | 19 (79%) 2 (8%) |

|
Maintenance post-program | 19 (83%) | 14 (64%) 1 (4%) |
18 (78%) 1 (4%) |
16 (76%) | 16 (76%) 4 (17%) |
| Mean percentage yes across all sessions | 80% | 73% | 80% | 75% | 83% | |
Engagement with, as well as utilization and applicability of, weekly Cardiac College for Women content by mode (n = 28).
Valid percentages reported. Non-italicized n (%) for yes responses. Italicized n (%) for “somewhat” responses (where queried).
The group education program comprised didactic sessions based on structured learning plans regarding CVD self-management and healthy behavior change (16). The slides guiding each session were similarly developed through a rigorous process as outlined above, and are available upon request (15). Each education session was planned for 30 min. Participants were also referred to specific corresponding supportive information on the Cardiac College for Women website (open access) (15), with over 70 assets available in text or video.
Compared to men on average, women often have different CV diagnoses (e.g., spontaneous coronary artery dissection [SCAD], myocardial infarction with non-obstructive coronary arteries [M/INOCA], cardiomyopathy), different risk factor burden (i.e., tobacco use, diabetes, peri/menopause), and comorbidities (i.e., alcohol or cannabis abuse, cancer, osteoporosis, autoimmune disease, polycystic ovarian syndrome); these may complicate their CVD management. While women require education about these and it is not readily available, they are not universal and hence it is not cost or time efficient or prudent (e.g., applicability, patient preference) for the CR education program to be exhaustive. Thus, as applicable, specific content about each of these clinical matters was offered to individual participants. Where agreed, relevant website links were provided via email; patients were directed to follow-up with their CR supervisors with any further questions.
2.3 Setting
This study was conducted in two Canadian CR programs: Toronto Rehabilitation Institute, University Health Network in Toronto, Ontario and Prévention Secondaire et Réadaptation Cardiovasculaire in Lévis, Quebec. They are both academic institutions.
Staff at both centers were provided the 12 education session slide sets in the applicable language (15). Training by the last author was provided for the relevant disciplines who would be delivering each session: 6 staff at the Ontario center and 4 at the Quebec center.
The CR programs including the education were offered in English at the Ontario site, and in French at the Quebec site (15). The education was delivered in a group setting (no rolling intakes) over a 12-week period, in-person, and led by a case-managing physiotherapist or kinesiologist for care continuity. Both programs were comprehensive and delivered based on clinical practice guidelines (18–20).
2.4 Participants
Patients identifying as women who presented at the CR centers during the period of recruitment were included in the study if they had one of the following conditions or procedures: acute coronary syndrome, revascularization (i.e., percutaneous coronary intervention or coronary artery bypass graft surgery), SCAD, M/INOCA, Takotsubo cardiomyopathy, or heart failure (with preserved or reduced ejection fraction; HFpEF). Women at the Toronto site were given the choice of program model in which to enroll based on their preferred class time, and only those in the women-only model were included in this sub-study. At the French site, all women enrolled in the women-only model during the period of study were invited to participate.
The inclusion criteria were age >18 years, as well as access to the internet and a computer, tablet and/or smartphone. The exclusion criteria were: any comorbid physical, sensory, or serious mental condition which would interfere with the patient's ability to read and participate in in-person education sessions, and lack of English or French-language proficiency. Patients who only had a smartphone (i.e., no access to larger screen) were excluded from being interviewed.
The inclusion criteria for CR staff were being involved in the delivery of the women-focused education materials at the centres under study. There were no exclusion criteria. For both patients and staff, interviews were held until thematic saturation was achieved (21).
2.5 Procedures
Baseline clinical data were extracted from medical charts. Assessment of participant sociodemographic characteristics was undertaken before CR started via online or paper versions (based on patient preference) of identical surveys.
Participants were similarly provided with a diary, and they were reminded to complete it each week of the education program. At 3 months (in accordance with the end of the CR programs and corresponding education), a survey was administered again either online or on paper.
After the intervention, patients in the intervention group at both sites were contacted by the research team via email and were invited to participate in one virtual interview. Similarly, staff who administered the education materials were emailed an interview invitation.
Semi-structured one-on-one interviews were conducted with willing participants via Zoom, with live transcription enabled and cameras on. The interviews were conducted by the first author (RC), who was trained by the last and second author (GG, SG); a second team member observed to record nonverbal communication. The first author is a master's student who underwent qualitative methods training and was not involved in the development or delivery of the education. She only knew the participants through study recruitment and data collection (which was often virtual). The interview guide was displayed on screen throughout.
2.6 Measures
To characterize the sample, patient clinical characteristics extracted included cardiovascular diagnoses/procedures, risk factors and comorbidities. Patients self-reported their sociodemographic characteristics, including gender-related factors (22).
The weekly diaries were used to track participant utilization of, engagement with, and their perceptions of the applicability of, the Cardiac College for Women intervention. Items were investigator generated, with forced-choice response options, such as whether they attended the session (yes or no; for utilization), whether they went to the website for more information (engagement), and whether the content was deemed relevant to their lives (yes, somewhat, or no; applicability). Each week's diary concluded with an open-ended item where participants were directed to add any questions or comments.
The utilization and acceptability surveys administered post-intervention pertained to the full 12 weeks of education. Utilization items were also investigator generated. Attendance at sessions, completion of weekly assigned readings and watching of assigned videos were assessed, using 5-point Likert type scales from 1 (never) to 5 (always), a question about amount of time spent (minutes), and proportion of assigned materials covered (%). Using similar response options, participants were also asked about their use of the website for additional learning. Participants were also asked about whether they agreed to receive additional individualized education for topics not covered in the curriculum; if so, they were asked about their degree of independent engagement with those online materials, and whether they contacted their CR provider(s) with queries about the content. Acceptability items –shown to be valid in previous work (23, 24)—were adapted for this curriculum, with 2 additional items created. The responses for the 14 items ranged from 1 (strongly disagree) to 5 (strongly agree) on a Likert-type scale. One item was reverse-scored to minimize acquiescence bias. An overall mean acceptability score was computed.
Two semi-structured interview guides were developed by SG and GG, one for patients and one for staff. They were informed by our previous literature review (16), and input from the investigative team. Questions and corresponding probes for patients explored overall satisfaction with content and delivery, how the progression of weekly topics flowed from session to session and degree to which it was perceived integrated, specific applicability and implementability into their lives, as well as suggestions for improvement. Questions and corresponding probes for patients explored implementability into the program, applicability, sustainability, and similarly suggestions for improvement. They were pilot-tested before formal interview initiation, and refined accordingly. The auto-generated transcripts were cleaned verbatim, except to preserve anonymity.
2.7 Data analyses
Participant characteristics were analyzed using descriptive statistics (e.g., frequency and percentage for categorical data; mean and standard deviation for continuous data). Utilization and acceptability ratings were similarly analyzed. Open-ended diary responses were content analyzed manifestly (25).
The qualitative data were analyzed using an inductive and text-driven approach to ensure rigor (26). Given that two different stakeholder groups were involved, transcripts were analyzed using systematic text condensation (27). Comments related to CR in general (i.e., non-education components such as exercise, general non-women-focused education) were not the focus of analysis. NVivo software (version 14) was used for data organization and coding, concurrently with interviews (28).
After training and calibration, two researchers (RC, AB) initially read through the the patient and staff transcripts independently, to get an overall sense of the content and identify preliminary themes from the raw data. They then broke the data down into smaller units of meaning, which they sorted into code groups based on thematic similarities. The researchers then met to review the coding and condense it to distill the essence of the data, transforming the codes into more concise and meaningful summaries. This condensed data was brought forward to a third author (GG) to discuss and reconcile where needed. The coding was then synthesized into descriptions and concepts to provide a coherent narrative and deeper understanding of the themes identified. For member checking, themes and their corresponding subthemes were shared with the education staff from both programs. Subsequently, themes were shared with the second author (SG) for validation. Data saturation was considered, confirming that no new themes were identified. Finally, themes were shared with all authors, such that consensus was reached, ultimately ensuring credibility and trustworthiness of the findings (29).
The quantitative and qualitative methods were integrated by means of merging, such that results of both stages were then brought together for analysis contiguously. By comparing and cross-verifying the results from both methods, consistencies and discrepancies were identified, to increase the validity and reliability of conclusions. This methodological triangulation enabled a comprehensive understanding of Cardiac College for Women utilization, acceptability, applicability, usability and implementability from multiple perspectives. Interpretation of the integrated results was performed narratively, including consideration of fit of the results from the two stages (17), as well as with available literature.
3 Results
3.1 Participant characteristics
Of women approached during the period of study, 54.4% consented and met the inclusion criteria; 40 (19; 47.5% French-speaking) of these patients enrolled in the women-only program. Of these, 36 (90.0%) completed the post-intervention utilization and acceptability surveys and form the cohort for this study. Sociodemographic and clinical characteristics are shown in Table 2. Of these participants, 28 (77.7%) completed any of the 12 weekly diaries.
Table 2
| Characteristic | Retained quantitative sample (N = 36) |
Qualitative interviewees (n = 12) |
|---|---|---|
| Sociodemographic & gender-related characteristics | ||
| Site (Toronto) | 19 (52.8%) | 5 (41.6%) |
| Age (years) | 66.3 ± 9.7 | 67.8 ± 9.8 |
| Ethnocultural background | ||
| White/Western European | 32 (91.4%) | 12 (100.0%) |
| South Asian | 1 (2.9%) | 0 (0.0%) |
| Asian | 1 (2.9%) | 0 (0.0%) |
| Multi-racial or other | 1 (2.9%) | 0 (0.0%) |
| Highest education | ||
| Some secondary school | 8 (22.9%) | 1 (8.3%) |
| Some college | 13 (37.1%) | 6 (50.0%) |
| Some university or greater | 14 (40.0%) | 5 (41.7%) |
| Health literacya | 17.8 ± 2.9 | 19.0 ± 1.4 |
| Limited | 1 (2.8%) | 0 (0.0%) |
| Marginal | 7 (19.4%) | 0 (0.0%) |
| Adequate | 28 (77.8%) | 12 (100.0%) |
| Work status | ||
| Paid employment (full or part-time) | 13 (36.1%) | 5 (41.7%) |
| Other (disability, retired, household management) | 23 (63.9%) | 7 (58.3%) |
| Financial worryb | 3.2 ± 1.1 | 3.2 ± 0.9 |
| Neighborhood environment walkable (e.g., treed, safe, low pollution) | 32 (88.9%) | 12 (100.0%) |
| Marital status | ||
| Married or equivalent | 21 (60.0%) | 6 (50.0%) |
| Widowed or single | 10 (28.6%) | 3 (27.3%) |
| Divorced or separated | 4 (11.4%) | 2 (18.2%) |
| Number of children | 1.7 ± 1.2 | 1.8 ± 1.0 |
| Children reside with patient (% yes) | 8 (22.9%) | 2 (16.7%) |
| Living situation | ||
| With partner and/or family | 26 (72.2%) | 8 (66.7%) |
| Alone | 10 (27.8%) | 4 (33.3%) |
| Emotional supportb | 4.3 ± 0.9 | 4.5 ± 0.8 |
| Health supportb | 4.6 ± 0.7 | 4.6 ± 0.7 |
| Informal caregiving responsibilities | ||
| Yes | 5 (13.9%) | 0 (0.0%) |
| Sometimes | 2 (5.6%) | 1 (8.3%) |
| Hours/week | 14.8 ± 8.4 | 10.0 ± 0.0 |
| Most responsible for domestic management in home | 26 (74.3%) | 7 (58.3%) |
| Number of hours spent per week on housework | 9.1 ± 7.5 | 8.7 ± 7.4 |
| Clinical characteristics | ||
| CR indicationc | ||
| Myocardial infarction | 11 (30.6%) | 5 (41.7%) |
| Coronary artery disease | 11 (30.6%) | 6 (50.0%) |
| PCI | 9 (25.0%) | 3 (25.0%) |
| Valve disease | 2 (5.6%) | 1 (8.3%) |
| CABG surgery | 3 (8.3%) | 0 (0.0%) |
| Stroke/TIA | 4 (11.1%) | 1 (8.3%) |
| SCAD | 2 (5.6%) | 0 (0.0%) |
| MINOCA/INOCA | 2 (5.6%) | 1 (8.3%) |
| HFrEF | 2 (5.6%) | 0 (0.0%) |
| Stable angina | 1 (2.8%) | 0 (0.0%) |
| Cardiomyopathy | 2 (5.6%) | 0 (0.0%) |
| Other (e.g., arrhythmia, atrial fibrillation, pacemaker, primary prevention) | 23 (63.9%) | 7 (58.3%) |
| CV risk factorsc | ||
| Dyslipidemia | 26 (72.2%) | 10 (83.3%) |
| Hypertension | 19 (52.8%) | 6 (50.0%) |
| Diabetes | 6 (16.7%) | 2 (16.7%) |
| Overweight (BMI > 25 kg/m2) | 7 (19.4%) | 1 (8.3%) |
| Depression and/or anxiety | 8 (22.2%) | 3 (25.0%) |
| Alcohol use (≥once/month) | 8 (22.2%) | 4 (33.3%) |
| Comorbiditiesc | ||
| Chronic pain/joint repair or replacement | 8 (22.9%) | 5 (41.7%) |
| Autoimmune disease | 5 (14.3%) | 1 (8.3%) |
| Osteoporosis | 5 (14.3%) | 2 (16.7%) |
| Sleep apnea | 6 (16.7%) | 1 (8.3%) |
| Cancer history | 6 (17.1%) | 2 (16.7%) |
| Tobacco use (current) | 1 (2.8%) | 1 (8.3%) |
| COPD | 1 (2.9%) | 0 (0.0%) |
| Musculoskeletal issues | 2 (5.6%) | 2 (16.7%) |
| Osteoarthritis | 1 (2.8%) | 0 (0.0%) |
| Frailty | 1 (2.8%) | 1 (8.3%) |
Sociodemographic and clinical characteristics of patient participants.
BMI, body mass index; CABG, coronary artery bypass graft; COPD, chronic obstructive pulmonary disease; CR, cardiac rehabilitation; CV, cardiovascular; HFrEF, heart failure with reduced ejection fraction; INOCA, ischemic and non-obstructive coronary arteries; MINOCA, myocardial infarction with non-obstructive coronary arteries; PCI, percutaneous coronary intervention; SCAD, spontaneous coronary artery dissection; TIA, transient ischemic attack.
n (valid%) or mean ± standard deviation shown.
Scores range from 4 to 20, with classifications of limited health literacy (4–12 points), marginal health literacy (13–16 points), and adequate health literacy (17–20 points).
Rated on a 5-point Likert-type scale, such that higher scores denote greater endorsement of the given construct.
As many as applicable reported.
3.2 Patient education use, engagement, acceptability and applicability
Weekly engagement with Cardiac College for Women elements as reported in the diaries is shown in Table 1; it was quite consistently high across all topics. Attendance at synchronous education sessions ranged from 67%–89% across all topics. Participants generally watched assigned weekly videos more often than read materials, with the notable exception of the resistance training content. Generally, at least 75% of the time participants visited the website for more information about a given topic, with the notable exception of the psychosocial content, and that about risk factors. Finally, with the exception as expected of the introduction and concluding sessions, relevance/applicability of the content to women's lives was rated very highly, other than the sessions regarding nutrition, and to a lesser degree psychosocial health.
Overall utilization of Cardiac College for Women materials across the program as shown in Table 3 echoes the weekly data. Participants almost always completed the weekly education. Participants read supporting weekly assigned readings or watched assigned videos at least “sometimes” or more, engaging with over two-thirds of this material for 30 min per week an average, be it reading or watching videos. Participants rarely perceived a need to contact CR staff with questions outside of the education sessions. Nine participants accepted the additional education based on reporting a non-universal CR indication, CV risk factor or comorbidity not covered in the curriculum, all of whom reported accessing the material provided. Correspondingly, Table 4 displays perceived curriculum acceptability, revealing high ratings by all participants (all means ≥4/5).
Table 3
| Item | Mean ± SD |
|---|---|
| How often completed recommended weekly heart education (/5a) | 4.0 ± 0.9 |
| How often read the assigned materials (/5a) | 3.9 ± 1.0 |
| Mean minutes per week reading the materials | 30.3 ± 18.0 |
| Proportion of weekly assigned reading completed (%) | 71.7 ± 32.9 |
| How often watched the assigned videos (/5a) | 3.6 ± 1.3 |
| Mean minutes per week watching the videos | 30.1 ± 24.5 |
| Proportion of weekly assigned videos watched (%) | 63.9 ± 37.1 |
| Accepted any additional educational material based on indication, risk factor or comorbidity not addressed in group education programb (n,% yes) | 9 (47.6%) |
| Additional education completed | 9 (100.0%) |
| How often visited the Cardiac College website to learn more about any educational topic (/5a) | 3.3 ± 1.1 |
| Mean minutes per week learning over and above assigned content | 28.6 ± 25.0 |
| Contacted the healthcare team to ask questions about the educational content outside of the synchronous group education sessions (/5a) | 1.7 ± 1.0 |
Overall utilization of Cardiac College for Women educational resources (N = 36).
Scored from 1 “never” to 5 “always”.
e.g., diabetes, alcohol use, obesity, spontaneous coronary artery dissection, myocardial infarction with non-obstructive coronary arteries.
SD, standard deviation.
Valid percentages reported.
Table 4
| Item | Mean ± SD |
|---|---|
| 1. The education met my approval | 4.4 ± 0.9 |
| 2. The education was appealing to me | 4.5 ± 0.8 |
| 3. I liked the education | 4.5 ± 0.8 |
| 4. The education helped me improve my heart health | 4.3 ± 0.9 |
| 5. I will use the information in my daily life | 4.5 ± 0.8 |
| 6. I understood all the information | 4.2 ± 0.8 |
| 7. The content was clear | 4.4 ± 0.9 |
| 8. The information was relevant to my life | 4.5 ± 0.9 |
| 9. The information was difficult to understandb | 4.0 ± 0.1 |
| 10. I got all the information I was needing | 4.2 ± 0.9 |
| 11. I will refer to this information again | 4.4 ± 0.8 |
| 12. I would recommend the education to my friends and family | 4.5 ± 0.8 |
| 13. The information was easy to read and hear | 4.3 ± 0.9 |
| 14. The education was too longb | 4.1 ± 1.3 |
| Overall Acceptability Rating | 4.3 ± 1.7 |
Assessment of acceptability of Cardiac College for Women education materialsa (N = 36).
Acceptability scores ranged from 1 to 5, with 1 = strongly disagree to 5 = strongly agree.
Reverse-scoring shown, and included when computing the overall mean acceptability rating.
3.3 Qualitative perspectives of patients and programs
Of the 36 intervention-completing participants, 12 (33.3%) agreed to be, and subsequently were, interviewed. Sociodemographic and clinical characteristics of interview participants are shown in Table 2. While generalizability is not a goal of qualitative research, data in the Table suggests interview participants were generally representative of the program participants, although they may have been somewhat more educated and health literate, had fewer informal caregiving and domestic obligations (leaving them more time to be interviewed) and they may have suffered more comorbidities.
Five of the 10 involved staff consented to participate, and were interviewed; four were from the Toronto site. All were female. The following disciplines were represented: kinesiology (n = 2, 40.0%), dietetics (n = 2, 40.0%), medicine (n = 1, 20.0%).
The 17 interviews conducted were of a median duration of 25 minutes (interquartile range: 17–34 min). Upon analysis of the interviews, it was agreed thematic saturation was attained (21). After excluding general comments about CR education (e.g., technological literacy of participants, hearing quality, desire for post-CR maintenance programming), four overarching themes were identified, with corresponding subthemes (Figure 1), each described below. Illustrative quotes supporting each are shown in Table 5.
Figure 1
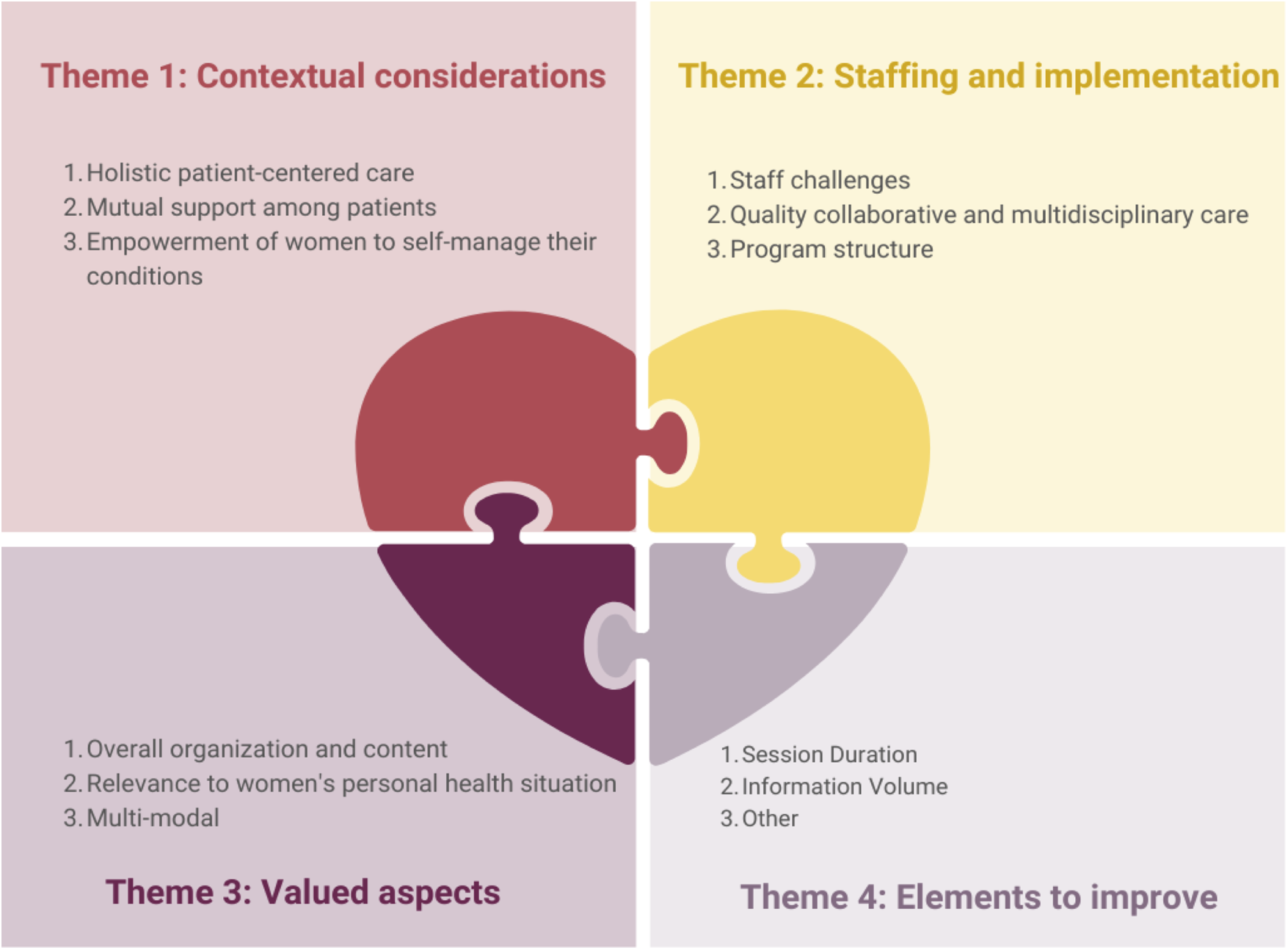
Themes and subthemes related to women-focused cardiac rehabilitation education and its’ implementation. CR, cardiac rehabilitation.
Table 5
| Theme | Sub-theme | Illustrative quotes (participant #) |
|---|---|---|
| Contextual considerations for women-focused CR education | Holistic patient-centered care |
|
| Mutual support among patients |
|
|
| Empowerment of women to self-manage their conditions |
|
|
| Staffing and implementation of women-focused CR education | Staff challenges |
|
| Quality collaborative and multidisciplinary care |
|
|
| Program structure |
|
|
| Valued aspects of women-focused CR education | Overall organization and content |
|
| Relevance to women's personal health situation |
|
|
| Multi-modal |
|
|
| Elements to improve | Session duration |
|
| Information volume |
|
|
| Other |
|
Illustrative quotes supporting themes and subthemes from patient and staff interviews regarding Cardiac College for Women.
CR, cardiac rehabilitation; P, patient; S, staff.
The first theme pertained contextual considerations for optimal women-focused CR education delivery, with 3 elucidatory subthemes. Firstly, a holistic, patient-centered context was raised as foundational for the education, entailing personalized care respective of participant's individual preferences and values. Secondly, mutual support among peers was considered as a foundational springboard, enabling participants to learn from others’ experiences, within an environment of respect and laughter. Finally, women discussed how the education empowered them to self-manage their health, through facilitation of action planning to achieve behavior change. The women-focused context and education enhanced their motivation and adherence to the program.
The second theme pertained to staffing and implementation, again with 3 subthemes. The first concerned staff challenges, such a lack of formal training in women-focused curricula content and limited time in their workday for session preparation for first-time delivery. The second subtheme concerned the provision of quality collaborative and multidisciplinary care. Participants duly recognized the efforts of diverse healthcare professionals in creating a comprehensive program. Despite a multitude of expert presenters, participants perceived the education as cohesive, based on the adeptness of a main CR lead. Lastly was structural considerations of the program, such as optimal class size. Relatedly, optimal delivery of some content was considered more suited to group vs. individual delivery; while the group dynamic was considered foundational as above, for some content individualized delivery was preferred (e.g., nutrition, psychosocial).
The third theme raised valued aspects of the women-focused CR education, which should be maintained and replicated where possible for optimal implementation. Firstly, participants appreciated the overall organization and content of the session topics, reporting the information provided as high-quality, comprehensive, and concise. They valued the cohesive integration and flow of educational material, prefaced by a helpful orientation. Women considered it convenient to access all materials through the Cardiac College for Women online platform, and the information was trusted. Secondly, that the content was relevant to women's unique personal health situations was highly valued. They previously did not have such in-depth yet tailored information about their diverse health conditions, risk factors, and backgrounds. Lastly, participants valued the multi-modal learning formats for their flexibility and convenience, given the CR barriers they experienced in their lives.
The last theme captured some ways to potentially improve the women-focused education. Participants expressed satisfaction with the volume of information provided in synchronous education sessions, yet desired more time for raising questions and sharing among participants. Some staff and patients suggested extending session duration from 30–45 min to avoid feeling rushed, with the additional time dedicated to such interactions to enhance the learning experience. In addition, they suggested considering additional weeks or sessions to extend the program duration, allowing for more comprehensive coverage of topics, and again to avert any rushing through content.
3.4 Merging of mixed-methods
While overall satisfaction, usability, acceptability, and applicability were quantitatively rated highly, some anomalies and discrepancies were elucidated in the qualitative findings. For instance, in the interviews, feedback regarding the nutrition education was that this information was highly desirable, but was preferred in an individual rather than group format. Indeed, for some topics, patients did not want generic education, but tailored information to their needs one-on-one. Other participants desired that the kinesiologist lead most group education sessions for continuity. Overall, through merged analysis, vagaries in individual preferences were elucidated (e.g., some patients had high health literacy or prior knowledge on a specific topic so the content a specific week was considered too simple, some patients preferred not to learn from the website but in-person, and vice versa), to inform future program implementation.
4 Discussion
The population of women with CVD is increasing globally, with a corresponding recognition of their unique risk and hence needs; sadly, these often go unaddressed. Recent CR guidelines call attention to this gap (14), stressing the need for women-focused education such as Cardiac College for Women. In this first implementation evaluation in programs and with patients, usability has been tested through a mixed-method study. Engagement was high, with 80% of the 12 sessions attended on average, and women doing a further 30 min per week in independent learning online. The education was liked, and deemed informative and relevant to women's lives. CVD patients reported implementing heart-health behavior changes based on the education provided. In light of evidence also supporting clinical efficacy of Cardiac College for Women (18), CR staff recommend the education curricula for other programs, where delivery staff and infrastructure are available.
Rigorous reviews have established that patient education may reduce morbidity, and significantly improves quality of life (30) and self-management in heart patients (31). However, there have been few studies regarding acceptability and implementation of patient education interventions in CR, or in other chronic diseases more broadly (32). Results herein are consistent with the many studies where the generic (i.e., non-women-focused) Cardiac College has been successfully adapted and implemented in diverse cultural contexts (33, 34). Barriers reported by staff related to lack of time and training in this study are common to those reported by patient educators for other chronic diseases (35).
4.1 Implications
Based on the results of this study, some revisions have been made to the education curricula. The generic (i.e., non-women-focused) education content on the Cardiac College website—such as regarding cardiovascular medications, among other clinical information—has been updated for currency. Navigation design could be improved so women can more readily find the specific information they seek. The team hopes to create a dedicated section on the Cardiac College website for professionals, to support programs and clinician providers implement the curriculum.
From a program perspective, some implementation matters merit consideration (36). First, program leadership should allocate sufficient time for staff to learn the needed content and prepare for optimal delivery, so they are adequately equipped to deliver the curriculum effectively. The Canadian Women's Heart Health Alliance offers clinician education for women and CVD which could fill staff education gaps (https://www.cwhha.ca/healthcare-professional-e-course-toolkit).
With regard to delivery format, while women desired and valued the group sessions, women-focused CR programs may better meet the needs of participants with individualized education regarding patient-specific clinical and psychosocial matters. To individually tailor education for less common CR indications and risk factors, women were directed to specific online educational resources to review independently in this study; this could ideally be done one-on-one with staff where resources permit. Local needs assessment regarding feasibility, staff expertise and patient preference for learning in each content area would facilitate optimal translation to other settings.
In addition, there were suggestions to extend the duration of each session and/or relatedly to increase the total number of sessions. Considering CR in Canada is among the longest globally, and the “dose” in terms of education time per program comparatively high (37), this likely cannot be heeded in most settings. Cardiac College for Women is multi-modal, such that where in-person synchronous congregation of women is infeasible, the online and asynchronous assets available freely online could be exploited to balance the preferences and needs of women with their lived realities and available program resources. Again, local needs assessment with patients and providers should be undertaken to optimally tailor the women-focused education.
In conjunction with supportive evaluation results (18), the curriculum should be tried in more diverse settings, with evaluation (36). Indeed, the open-access materials in English and French have been broadly disseminated through the International Council of Cardiovascular Prevention and Rehabilitation (ICCPR) community.
4.2 Limitations
Caution is warranted when interpreting these results. Foremost, generalizability is limited given that the study was only undertaken at two centres in a high-income country (although in one province CR is reimbursed by government health insurance and the other it is not). It is also limited given the small sample size, and the exclusion of participants with comorbidities. However, generalizability is not an aim of mixed-methods research. Second, results may be biased because the characteristics of patients who were eligible but not referred or were referred and did not enroll in CR are not available to compare to the characteristics of patients consenting to participate in this study. Thus, selection bias may be a concern, however retention bias is not.
With regard to design, the control participants from the larger quantitative study (18) were not asked to complete weekly diaries or complete post-program utilization and acceptability surveys. Thus, it is possible acceptability and engagement were as high with usual care, or that socially-desirable responding was at play. Indeed, the usability items in particular were investigator-generated hence with unknown reliability and validity. Future randomized, controlled research with objective measures of usability (e.g., website traffic) is warranted so causal conclusions may be drawn (36).
In conclusion, Cardiac College for Women has been demonstrated to be highly usable and used, as well as acceptable and applicable to the lives of CVD patients identifying as women. The education supported women's implementation of recommended disease management behaviors in their lives. Moreover, program staff perceived that the curricula and associated materials was highly feasible to implement, and reported that delivery can be sustained within their programs for the benefit of future women participants. Along with preliminary data supporting the efficacy of this education (18), overall results support dissemination to scale.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University Health Network (Toronto, Canada: 23-5427) and Centre Intégré de Santé et the Services Sociaux de Claudiére-Appalaches (Lévis, Canada: 2024-1076). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RC: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft. SG: Conceptualization, Funding acquisition, Methodology, Resources, Software, Supervision, Validation, Writing – original draft. AB: Writing – review & editing, Validation, Formal Analysis, Data curation. AH: Investigation, Writing – review & editing. MR: Conceptualization, Project administration, Resources, Software, Supervision, Writing – review & editing. PO: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing. GG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Canadian Institutes of Health Research (CIHR #487149).
Acknowledgments
We are grateful to the leaders at our program who inaugurated our women's only cardiac rehabilitation, including Drs. Tracey Colella and Rajni Nijhawan. We are grateful to Crystal Aultman for managing all the content organization to the website and updates. Finally, we recognize our patient partner Gayl McKinley for sharing her perspectives to inform and refine this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor LB declared a past collaboration with the authors SG, GM.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403(10440):2100–32. 10.1016/S0140-6736(24)00367-2
2.
Redfern J Hyun K Brieger D Chew D French J Hammett C et al SNAPSHOT ACS cohort follow-up—what happens to Australian patients in the 3 years after hospital discharge: a national data linkage study. Heart Lung Circ. (2020) 28:S373. 10.1016/j.hlc.2019.06.558
3.
Roth GA Mensah GA Johnson CO Addolorato G Ammirati E Baddour LM et al Global burden of cardiovascular diseases and risk factors, 1990–2019. J Am Coll Cardiol. (2020) 76(25):2982–3021. 10.1016/j.jacc.2020.11.010
4.
Li S Peng Y Wang X Qian Y Xiang P Wade SW et al Cardiovascular events and death after myocardial infarction or ischemic stroke in an older medicare population. Clin Cardiol. (2019) 42(3):391–9. 10.1002/clc.23160
5.
Kabboul NN Tomlinson G Francis TA Grace SL Chaves G Rac V et al Comparative effectiveness of the core components of cardiac rehabilitation on mortality and morbidity: a systematic review and network meta-analysis. J Clin Med. (2018) 7(12):514. 10.3390/jcm7120514
6.
Labrunée M Pathak A Loscos M Coudeyre E Casillas JM Gremeaux V . Therapeutic education in cardiovascular diseases: state of the art and perspectives. Ann Phys Rehabil Med. (2012) 55(5):322–41. 10.1016/j.rehab.2012.04.003
7.
Dibben G Faulkner J Oldridge N Rees K Thompson DR Zwisler AD et al Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. (2021) 11(11):CD001800. 10.1002/14651858.cd001800.pub4
8.
Prabhu N Maiya AG Prabhu NS . Impact of cardiac rehabilitation on functional capacity and physical activity after coronary revascularization: a scientific review. Cardiol Res Pract. (2020) 2020:1236968. 10.1155/2020/1236968
9.
Francis TA Kabboul NN Rac V Mitsakakis N Pechlivanoglou P Bielecki J et al The effect of cardiac rehabilitation on health-related quality of life in patients with coronary artery disease: a meta-analysis. Can J Cardiol. (2019) 35(3):352–64. 10.1016/j.cjca.2018.11.013
10.
Samayoa L Grace SL Gravely S Scott LB Marzolini S Colella TJ . Sex differences in cardiac rehabilitation enrollment: a meta-analysis. Can J Cardiol. (2014) 30(7):793–800. 10.1016/j.cjca.2013.11.007
11.
Oosenbrug E Marinho RP Zhang J Marzolini S Colella TJ Pakosh M et al Sex differences in cardiac rehabilitation adherence: a meta-analysis. Can J Cardiol. (2016) 32(11):1316–24. 10.1016/j.cjca.2016.01.036
12.
Bouakkar J Pereira TJ Pakosh M Drake JDM . Sex differences in the physiological responses to cardiac rehabilitation: a systematic review. BMC Sports Sci Med Rehabil. (2024) 16(1):74. 10.1186/s13102-024-00867-9
13.
Lima de Melo Ghisi G Kim WS Cha S Zhang L Tourkmani N Grace SL . Women’s cardiac rehabilitation barriers: results of the international council of cardiovascular prevention and rehabilitation’s first global assessment. Can J Cardiol. (2023) 39(11):S375–83. 10.1016/j.cjca.2023.07.016
14.
Lima de Melo Ghisi G Marzolini S Price J Beckie T Mamataz T Naheed A et al Women-focused cardiovascular rehabilitation: an international council of cardiovascular prevention and rehabilitation clinical practice guideline. Can J Cardiol. (2022) 38(12):1786–98. 10.1016/j.cjca.2022.06.021
15.
Lima de Melo Ghisi G Hebert AA Oh P Colella T Aultman C Carvalho C et al Evidence-informed development of women-focused cardiac rehabilitation education. Heart Lung. (2024) 64:14–23. 10.1016/j.hrtlng.2023.11.004
16.
Mamataz T Lima de Melo Ghisi G Pakosh M Grace SL . Nature, availability, and utilization of women-focused cardiac rehabilitation: a systematic review. BMC Cardiovasc Disord. (2021) 21:459. 10.1186/s12872-021-02267-0
17.
Fetters MD Curry LA Creswell J . Achieving integration in mixed methods designs-principles and practices. Health Serv Res. (2013) 48(6 pt 2):2134–56. 10.1111/1475-6773.12117
18.
Ghisi GLM Carson RP Hebert AA Ross MK Colella T Oh P et al A multi-site prospective controlled pilot evaluation of cardiac college for women in the cardiac rehabilitation setting. Patient Educ Couns. Under revision.
19.
Mehra VM Gaalema D Pakosh M Grace SL . Systematic review of cardiac rehabilitation guidelines: quality and scope. Eur J Prev Cardiol. (2020) 27(9):912–28. 10.1177/2047487319878958
20.
Grace SL Turk-Adawi K Contractor A Atrey A Campbell NR Derman W et al Cardiac rehabilitation delivery model for low-resource settings: an international council of cardiovascular prevention and rehabilitation consensus statement. Prog Cardiovasc Dis. (2016) 59(3):303–22. 10.1016/j.pcad.2016.08.004
21.
Saunders B Sim J Kingstone T Baker S Waterfield J Bartlam B et al Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. (2018) 52(4):1893–907. 10.1007/s11135-017-0574-8
22.
Pelletier R Ditto B Pilote L . A composite measure of gender and its association with risk factors in patients with premature acute coronary syndrome. Psychosom Med. (2015) 77(5):517–26. 10.1097/PSY.0000000000000186
23.
Weiner BJ Lewis CC Stanick C Powell BJ Dorsey CN Clary AS et al Psychometric assessment of three newly developed implementation outcome measures. Implement Sci. (2017) 12:108. 10.1186/s13012-017-0635-3
24.
Liu X Grace SL Ghisi GLM Wendan S Shen C Oh P et al Controlled pilot test of a translated cardiac rehabilitation education curriculum in percutaneous coronary intervention patients in a middle-income country delivered using WeChat: acceptability, engagement, satisfaction and preliminary outcomes. Health Educ Res. (2022) 37(5):314–32. 10.1093/her/cyac022
25.
Kleinheksel AJ Rockich-Winston N Tawfik H Wyatt TR . Demystifying content analysis. Am J Pharm Educ. (2020) 84(1):7113. 10.5688/ajpe7113
26.
Crabtree BF Miller WL . A template approach to text analysis: developing and using codebooks. Doing Qual Res. (1992):93–109.
27.
Malterud K . Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. (2012) 40(8):795–805. 10.1177/1403494812465030
28.
Jackson K Bazeley P . Qualitative Data Analysis with NVivo. 3rd ed. London, UK: Sage Publications (2019).
29.
Tong A Sainsbury P Craig J . Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19(6):349–57. 10.1093/intqhc/mzm042
30.
Anderson L Brown JP Clark AM Dalal H Rossau HKK Bridges C et al Patient education in the management of coronary heart disease. Cochrane Database Syst Rev. (2017) 6:CD008895. 10.1002/14651858.cd008895.pub3
31.
Shi W Ghisi GLM Zhang L Hyun K Pakosh M Gallagher R . Systematic review, meta-analysis and meta-regression to determine the effects of patient education on health behaviour change in adults diagnosed with coronary heart disease. J Clin Nurs. (2023) 32(15–16):5300–27. 10.1111/jocn.16519
32.
Siddharthan T Rabin T Canavan ME Nassali F Kirchhoff P Kalyesubula R et al Implementation of patient-centered education for chronic-disease management in Uganda: an effectiveness study. PLoS One. (2016) 11(11):e0166411. 10.1371/journal.pone.0166411
33.
Trani MR Bilocura I Bersabal S Panilagao RK Toledo BR Garrido E et al Effects of a comprehensive structured patient education intervention on disease-related knowledge and behaviour change among people living with type 2 diabetes in the Philippines. Front Rehabil Sci. (2024) 5:1374850. 10.3389/fresc.2024.1374850
34.
Ghisi GLM Aultman C Konidis R Sandison N Oh P . Developing a group-based virtual education curriculum for cardiac rehabilitation and the associated toolkit to support implementation in Canada and across the globe. Heart Lung. (2023) 57:80–94. 10.1016/j.hrtlng.2022.08.011
35.
Bennett SE Zangi HA Larsson I Beauvais C Boström C Domján A et al Assessing acceptability and identifying barriers and facilitators to implementation of the EULAR recommendations for patient education in inflammatory arthritis: a mixed-methods study with rheumatology professionals in 23 European and Asian countries. Ann Rheum Dis. (2022) 81(10):1348. 10.1136/annrheumdis-2022-222253
36.
Klaic M Kapp S Hudson P Chapman W Denehy L Story D et al Implementability of healthcare interventions: an overview of reviews and development of a conceptual framework. Implement Sci. (2022) 17(1):10. 10.1186/s13012-021-01171-7
37.
Chaves G Turk-Adawi K Supervia M Santiago de Araújo Pio C Abu-Jeish Ah Mamataz T et al Cardiac rehabilitation dose around the world. Circ Cardiovasc Qual Outcomes. (2020) 13(1). 10.1161/CIRCOUTCOMES.119.005453
Summary
Keywords
cardiac rehabilitation, women's health, patient education as topic, patient compliance, patient satisfaction, health personnel
Citation
Carson RP, Grace SL, Bomtempo APD, Hebert A-A, Ross M-K, Oh P and Ghisi G (2024) A multi-site mixed-method evaluation of ‘Cardiac College for Women’ implementation: perspectives of cardiac rehabilitation patients and providers. Front. Cardiovasc. Med. 11:1430268. doi: 10.3389/fcvm.2024.1430268
Received
09 May 2024
Accepted
19 September 2024
Published
08 October 2024
Volume
11 - 2024
Edited by
Ladislav Batalik, Masaryk University, Czechia
Reviewed by
Mei Sin Chong, National University of Singapore, Singapore
Faye Forsyth, University of Cambridge, United Kingdom
Updates
Copyright
© 2024 Carson, Grace, Bomtempo, Hebert, Ross, Oh and Ghisi.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Sherry L. Grace sgrace@yorku.ca
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.