Abstract
Background:
In patients with atrial fibrillation (AF) undergoing coronary artery bypass grafting (CABG) or aortic valve replacement (AVR), many surgeons are reluctant to open the left atrium for surgical ablation. However, especially in those with persistent AF, a box lesion isolating the entire posterior left atrial wall may be beneficial. Here, we describe our initial experience with a novel closed atrium bipolar radio-frequency left atrial box ablation technique.
Methods:
Between January 2023 and June 2024, 22 patients underwent the closed atrium radio-frequency box lesion set. Left left atrial appendage (LAA) closure was performed using an LAA clip in all patients. We evaluated the technical feasibility, safety, and efficacy of this new concomitant surgical AF ablation approach.
Results:
The mean patient age was 67.9 ± 5.3 years, and 68.2% were male. 12 patients (54.5%) had persistent AF, while 10 (45.5%) had paroxysmal AF. Creation of a complete box lesion from the right side was feasible in 14 patients; in 8 patients, the lesion had to be completed from the left side. No major ablation-related complications occurred. Successful intraoperative LAA closure was confirmed by TEE in all patients. There were no periprocedural strokes, and in-hospital mortality was 0%. Freedom from AF was 86.4% at discharge and 77.2% at a mean follow-up of 12.6 ± 3.9 months.
Conclusion:
The closed atrium left atrial box lesion technique for surgical treatment of AF concomitant with CABG or AVR is safe and technically feasible. This approach enables complete isolation of the posterior left atrial wall without the need to open the left atrium.
Introduction
Atrial fibrillation (AF) stands as the most prevalent arrhythmia and is linked to thromboembolic incidents, such as strokes, and is even correlated with an increase in mortality (1, 2). Additionally, it contributes to an increased frequency of hospitalizations and can lead to heart failure (1, 2). Concomitant Surgical AF ablation has demonstrated restoration of sinus rhythm in both, retrospective and prospective randomized trials (3–7). Retrospective studies and prospective registries have also indicated a survival advantage for patients with atrial fibrillation undergoing concurrent AF surgery (5, 8, 9). Consequently, guidelines and consensus statements recommend concurrent surgical ablation for atrial fibrillation (10, 11). In recent ESC/EACTS guidelines, surgical ablation in non-mitral valve surgery has a class IIa indication.
The original Cox Maze procedure, incorporating the cut-and-sew technique, has evolved into the Cox Maze III procedure, serving as the gold standard for surgical ablation for many years. However, due to the complexity of this technique, it has been employed by only a limited number of surgeons. The replacement of the cut-and-sew technique with the creation of thermal lesions has simplified the procedure, leading to widespread application as the Cox MAZE IV procedure. Throughout the years, numerous modifications of the original Cox Maze IV lesion set have been utilized with varying success rates. In procedures where the atria are not routinely opened for the surgical process, such as in CABG or AVR cases, many surgeons are hesitant to perform an atriotomy to conduct a complete left-atrial or even a biatrial ablation. However, electrical isolation of the posterior left atrial wall has been shown to increase success rate of AF ablation in prior studies. We here describe and evaluate a new technique of closed atrium left-atrial box lesion for surgical ablation in patients undergoing AVR or CABG procedures.
Materials and methods
Between January 2023 and December 2024, 22 patients underwent concomitant surgical ablation with the new closed atrium left-atrial box lesion set in our institution. IRB approval was obtained (Ethikkommission der Ärztekammer Hamburg 2020-10183). A retrospective single center data analysis was performed.
Surgical technique
All patients in this study were treated with an Atricure Isolator Synergy Access Clamp EML2, EMR2 or EMT1, (Atricure Inc. West Chester, Ohio). The curved bipolar radio-frequency clamp was introduced from the right-sided pulmonary veins through the transverse sinus to the end of the left-sided pulmonary veins (Figure 1). In case of enlarged atria, the box lesion was completed from the left side (Figure 2). To have the right angle to complete the box lesion from the left side, the radio-frequency clamp was introduced through the left-sided drainage tube hole (Figure 2). Alternatively, after opening of the oblique and transverse sinus, the curved bipolar radio-frequency clamp was introduced from the right side and subsequently from the left side to complete the left atrial box. The lesion set results in a bilateral epicardial isolation of the pulmonary veins and the left atrial posterior wall. Additionally, the Atriclip provided electrical isolation of the LAA: (Figure 3). The electrical isolation of the box was confirmed using the Atricure Isolator MAX Pen 5 (Atricure Inc. West Chester, Ohio). All patients received LAA closure, using the Atriclip or Atriclip PRO1 40 or 45 mm (Atricure Inc. West Chester, Ohio). Intraoperative TEE was used to confirm successful occlusion of the left left atrial appendage.
Figure 1
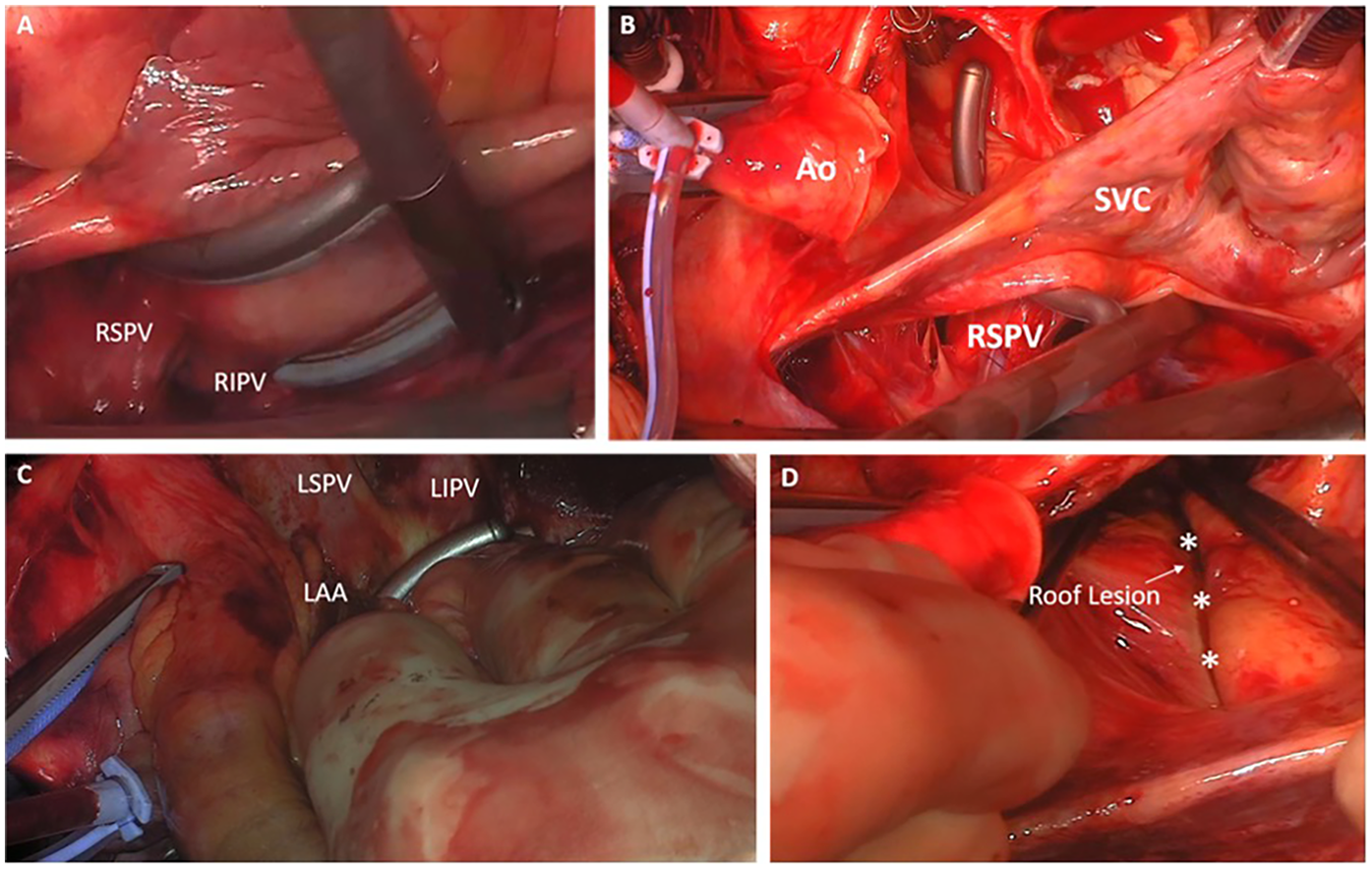
Creation of the left-atrial box lesion with the bipolar radio-frequency clamp. (A) Introduction of the curved bipolar radio-frequency clamp from the right-sided pulmonary veins (B,C) passing of the clamp to the side of the left pulmonary veins and ablation of the box lesion (D) LA roof lesion after the ablation procedure (*Roof line).
Figure 2
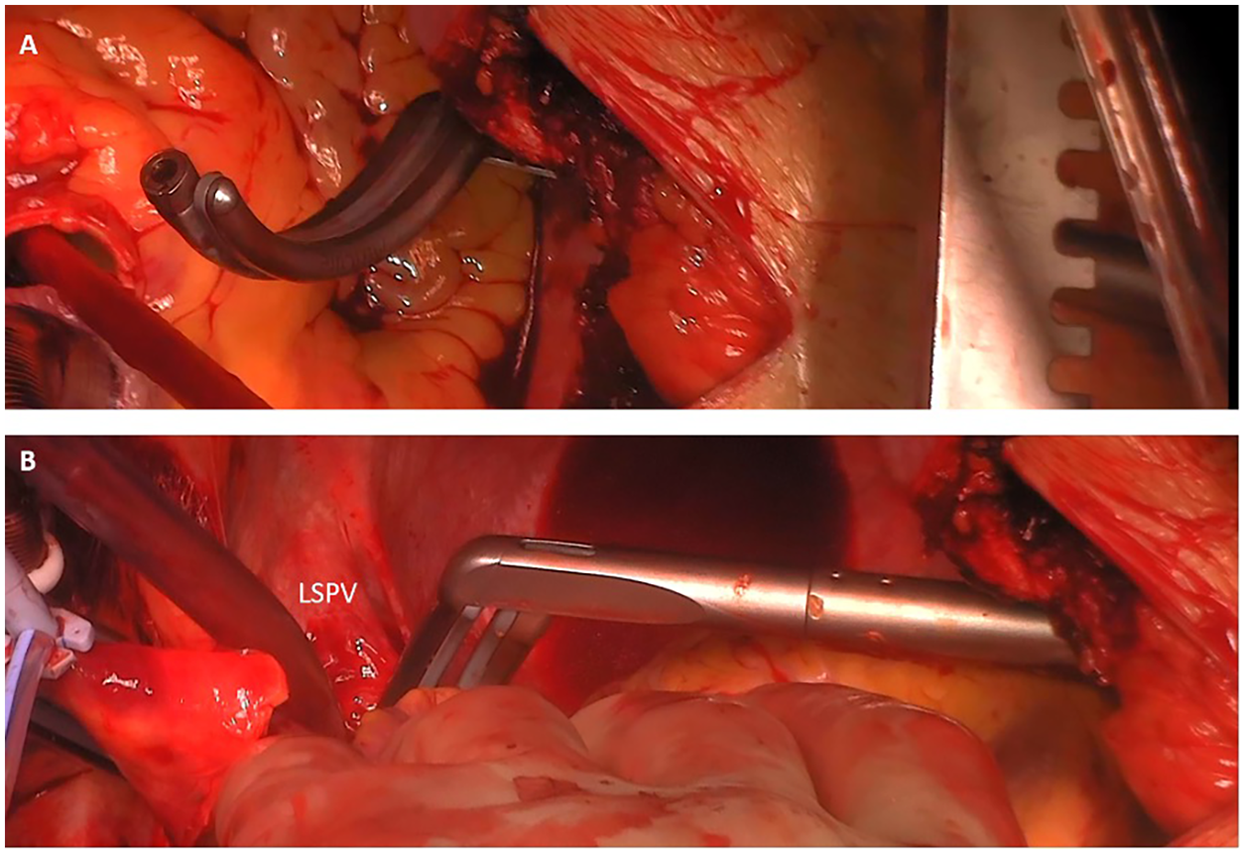
Completion of the box lesion from the left side. (A) Introduction of the bipolar radio-frequency clamp through the drainage tube hole. (B) Completion of the LA box from the left side. Introduction of the clamp from the left side. Overlapping with the previously performed ablation lines from the right side to complete the box.
Figure 3
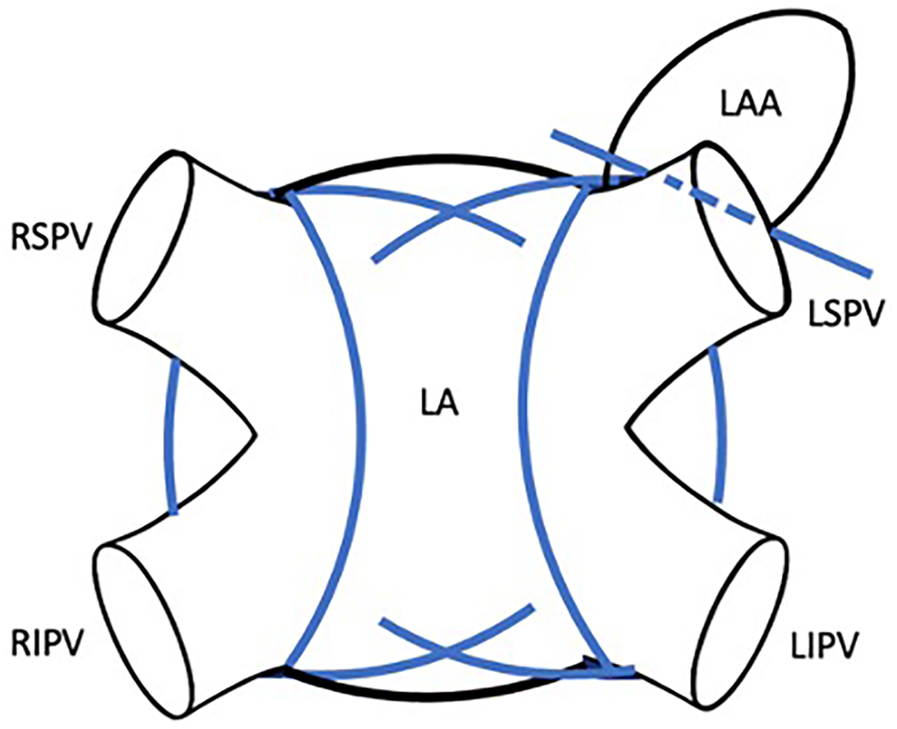
Closed-atrium box lesion set including bilateral pulmonary vein isolation, isolation of the left-atrial posterior wall and electrical isolation and occlusion of the LAA using atriclip.
Follow-up
24-h Holter ECG was conducted at latest follow-up. AF recurrence was defined by AF episode >30 s in 24 h- Holter-ECG. The discharge rhythm results were obtained by 12 lead ECG. Anticoagulation regimen was maintained for 3 months postoperative in all patients and then adapted according to CHA2DS2-VASc Score. Patients undergoing biological AVR received either coumadin, or NOAC according to their preoperative medication. In CABG patients, thrombocyte aggregation with Clopidogrel was added to the pre-operative anticoagulation (NOAC or Coumadin) for 6 months.
In patients without contraindications, amiodarone was used as first-line antiarrhythmic drug therapy, otherwise other class I or III antiarrhythmic drugs were used for at least 3 months postoperative.
Statistical analysis
All statistical analyses were performed with SPSS statistical software version 21.0 (SPSS Inc., Chicago, Illinois) Continuous values are expressed as mean ± standard deviation Categorical variables are displayed as frequency and percentages.
Results
Patient characteristics
The study population consisted of 22 patients with a mean age of 67.9 ± 5.2 years. Of these, 15 patients (68.2%) were male. Median CHA₂DS₂-VASc Score was 3.0 (IQR 2;4). Paroxysmal atrial fibrillation (AF) was observed in 10 patients (45.5%), while 12 patients (54.5%) had persistent or long-standing persistent AF. The mean left atrial (LA) volume index was 41.8 ± 7.7 ml/m2 and the average AF duration was 3.1 ± 2.7 years. The mean left ventricular ejection fraction (LVEF) was 54.7 ± 6.2%.
Comorbidities were prevalent, with arterial hypertension present in 13 patients (59.1%), coronary artery disease in 11 (50.0%), hyperlipidemia in 6 (27.3%), and diabetes mellitus in 5 (22.7%). Chronic kidney disease was documented in 5 patients (22.7%), and 2 patients (9.1%) had a history of stroke. One patient (4.6%) had a preoperative pacemaker (Table 1).
Table 1
| Patients | n = 22 |
|---|---|
| Age (years) | 67.9 ± 5.2 |
| Sex [male n, (%)] | 15 (68.2) |
| Type of Atrial fibrillation - Paroxysmal n (%)
|
10 (45.5) 12 (54.5) |
| La volume index (ml/m2) | 41.8 ± 7.7 |
| AF duration (years) | 3.1. ± 2.7 |
| LVEF (%) | 54.7 ± 6.2 |
| Diabetes mellitus n (%) | 5 (22.7) |
| Hyperlipidemia | 6 (27.3) |
| Arterial hypertension n (%) | 13 (59.1) |
| Chronic kidney disease n (%) | 5 (22.7) |
| Coronary artery disease n (%) | 11 (50.0) |
| Previous stroke n (%) | 2 (9.1) |
| Preoperative pacemaker (%) | 1 (4.6) |
Patient baseline characteristics.
Procedural data
Performed surgical procedures were isolated coronary artery bypass grafting (CABG) in 5 (22.7%) patients. Aortic valve replacement was performed in 14 (63.6%) patients. A combined CABG and AVR operation was conducted in 3 (13.6%) patients.
Mean cross-clamp time was 58.4 ± 6.3 min, mean cardiopulmonary bypass time was 93.3 ± 14.3 min.
No major ablation related complication occurred in any of the patients. There was no intraoperative death and no in-hospital mortality. One patient received re-thoracotomy for bleeding, unrelated to the performed ablation. There was no intra- or perioperative stroke in any of the patients. Permanent Pacemaker implantation was necessary in one patient (4.6%) during follow-up (Table 2).
Table 2
| Patients | n = 22 |
|---|---|
| CABG n (%) | 5 (22.7) |
| AVR n (%) | 14 (63.6) |
| CABG + AVR n (%) | 3 (13.6) |
| Mean cross clamp time (min) | 58.4 min ± 6.3 |
| Mean cardiopulmonary bypass time (min) | 93.3 ± 14.3 |
| Successful LAA closure (TEE) n (%) | 22 (100) |
| Re-thoracotomy for bleeding n (%) | 1 (4.6) |
| In-hospital mortality n (%) | 0 (0) |
| Perioperative stroke n (%) | 0 (0) |
| Postoperative pacemaker implantation n (%) | 1 (4.6) |
Perioperative data.
Rhythm results
Acute epicardial entrance- and exit block was confirmed intraoperatively in 21/22 patients, One patient that was still in SR after cross clamp release and intraoperative electrical cardioversion only had entrance block documented. Freedom from AF at discharge was obtained by 12-lead ECG and was 86.4%. All patients received 24 h Holter-ECG at latest follow-up (mean follow-up duration 12.6 ± 3.9 months). The rate of freedom from AF at latest follow-up was 77.2%, while freedom from AF off antiarrhythmic drugs was 68.2%, respectively.
Intraoperative transesophageal echo confirmed successful LAA closure in all patients, without any leakage or stump >10 mm.
Discussion
In this study, we demonstrated the safety and efficacy of a novel technique for performing a closed atrium bipolar radio-frequency box lesion, which isolates the posterior left atrial wall. No ablation-related complications were observed, and freedom from atrial fibrillation (AF) was achieved in 77.2% of patients at a mean follow-up of 12.6 ± 3.9 months. The box ablation can be achieved without need for additional tools.
In a landmark electrophysiological study by Haissaguerre et al., it was shown that in cases of stand-alone paroxysmal AF, the triggers initiating AF predominantly originate from the pulmonary veins (1). Since then, catheter-based ablation strategies have primarily targeted the pulmonary veins (2, 3). In surgical AF ablation, the Cox-Maze procedure—first performed by James Cox in 1987—has remained the gold standard, with excellent outcomes. However, it requires opening both atria for ablation (4). Over the years, several modifications to the biatrial lesion set have been proposed (5). In patients with paroxysmal AF, a left atrial lesion set or isolated pulmonary vein isolation (PVI) are commonly employed alternatives (6–9).
In cases involving concomitant coronary artery bypass grafting (CABG) or aortic valve replacement (AVR), many surgeons are reluctant to open the left atrium for surgical ablation due to the increased cross-clamp and cardiopulmonary bypass times, as well as added procedural complexity. Whether the addition of a complete left atrial lesion set improves rhythm outcomes remains a subject of debate. In recent years, only a limited number of studies have compared complete left atrial lesion sets with PVI alone, with conflicting results. A recently published randomized controlled trial investigating surgical AF ablation during mitral valve surgery found that isolated PVI achieved similar results to a biatrial lesion set (10). In contrast, Soni et al. (11) demonstrated that a complete left atrial lesion set significantly improved freedom from AF compared to PVI alone—reporting rates of 57% in the PVI group vs. 76% in the extended left atrial group (p < 0.001).
Furthermore, Henn et al. showed that isolating the posterior left atrial wall resulted in significantly better long-term outcomes. At 1-year follow-up, sinus rhythm was observed in 93% of patients with box isolation and 85% without. However, at 5-year follow-up, sinus rhythm was maintained in 78% of the box isolation group compared to only 45% of the group without posterior wall isolation (12).
Our new technique for a closed atrium bipolar radio-frequency box lesion provides a safe and straightforward method to isolate both the pulmonary veins and the posterior left atrial wall. Importantly, the procedure does not require atriotomy, thereby simplifying the operation and reducing cross-clamp time, as the ablation can be performed on the beating heart. After opening the oblique and transverse sinuses, the bipolar radio-frequency clamp can be inserted from the right-sided to the left-sided pulmonary veins. In cases of significantly enlarged left atria, the box lesion can be completed from the left side by introducing the clamp through the left-sided drainage tube incision to achieve an optimal angle. This approach is technically simple and was not associated with any procedural complications in our series.
The ablation was performed on cardiopulmonary bypass without aortic cross-clamping in 82% of patients. In four cases, cross-clamping and cardiac arrest were required due to markedly enlarged left atria, which made it difficult to access the left pulmonary veins via the transverse and oblique sinuses from the right side. The use of a bipolar clamp for all lesions is a more reliable method for ensuring complete transmurality compared to surgical ablation with unipolar devices (13).
We observed a low rate of postoperative permanent pacemaker implantation (4.6%), which is comparable to previously published findings (11).
Our freedom from AF rate of 77.2% at a mean follow-up of 12.9 months is consistent with previous studies. For example, Soni et al. (11) reported a sinus rhythm rate of 76% at 1 year, which is comparable to our data.
In patients with long-standing persistent AF, a more extensive lesion set—such as a complete left atrial or even biatrial ablation—may be necessary to effectively eliminate non-pulmonary vein triggers and rotors. Additionally, in patients with structural mitral valve disease, AF may originate from the left atrial wall itself due to increased atrial volume and pressure caused by mitral regurgitation. In such cases, a more comprehensive lesion set, including a mitral isthmus line and possibly right atrial lesions, may be required.
Alternatively, hybrid approaches combining epicardial surgical and endocardial catheter-based ablation have gained increasing popularity, particularly in patients with symptomatic persistent or longstanding persistent atrial fibrillation (AF). Hybrid ablation has received a Class IIa recommendation in the most recent ESC/EACTS/EHRA guidelines (14). Recent studies have demonstrated promising outcomes in this patient population, reporting 12-month freedom from AF rates between 67% and 71.9% (15–17). Various surgical access routes—including thoracoscopic and robot-assisted techniques—have been employed in combination with endocardial catheter ablation (15–17).
In contrast to our patient cohort, these hybrid ablation studies included only patients with lone AF and without significant structural heart disease, thereby limiting direct comparability. Nonetheless, catheter-based endocardial ablation remains a valuable therapeutic option in our population, particularly in the event of symptom recurrence or AF recurrence following the blanking period. In such cases, a second-step endocardial procedure to identify conduction gaps or additional triggers for AF may be warranted and should be considered as part of a stepwise rhythm control strategy.
Future studies with longer follow-up periods and larger patient cohorts are needed to validate our preliminary findings with this novel closed atrium bipolar radio-frequency box lesion technique.
Limitations
This study is a retrospective study with the potential risk of bias by unknown confounders. Furthermore, our series is a single-center study and is limited by the small number of patients and rather short follow-up period.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethikkommission der Ärztekammer Hamburg 2020-10183. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SP: Conceptualization, Investigation, Methodology, Writing – original draft. JP: Data curation, Investigation, Writing – original draft. YY: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. IB: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. HR: Supervision, Writing – review & editing. YA: Formal analysis, Investigation, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. We acknowledge financial support from the Open Access Publication Fund of UKE-Universitätsklinikum Hamburg-Eppendorf.
Conflict of interest
SP has received speaker honoraria and consultation fees from Atricure.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1655695/full#supplementary-material
References
1.
Haissaguerre M Jais P Shah DC Takahashi A Hocini M Quiniou G et al Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. (1998) 339:659–66. 10.1056/NEJM199809033391003
2.
Cosedis Nielsen J Johannessen A Raatikainen P Hindricks G Walfridsson H Kongstad O et al Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med. (2012) 367:1587–95. 10.1056/NEJMoa1113566
3.
Vogler J Willems S Sultan A Schreiber D Luker J Servatius H et al Pulmonary vein isolation versus defragmentation: the CHASE-AF clinical trial. J Am Coll Cardiol. (2015) 66:2743–52. 10.1016/j.jacc.2015.09.088
4.
Cox JL . The surgical treatment of atrial fibrillation. IV. Surgical technique. J Thorac Cardiovasc Surg. (1991) 101:584–92. 10.1016/S0022-5223(19)36685-1
5.
Gillinov AM Bhavani S Blackstone EH Rajeswaran J Svensson LG Navia JL et al Surgery for permanent atrial fibrillation: impact of patient factors and lesion set. Ann Thorac Surg. (2006) 82:502–13; discussion 13–4. 10.1016/j.athoracsur.2006.02.030
6.
Barnett SD Ad N . Surgical ablation as treatment for the elimination of atrial fibrillation: a meta-analysis. J Thorac Cardiovasc Surg. (2006) 131:1029–35. 10.1016/j.jtcvs.2005.10.020
7.
Abreu Filho CA Lisboa LA Dallan LA Spina GS Grinberg M Scanavacca M et al Effectiveness of the maze procedure using cooled-tip radio-frequency ablation in patients with permanent atrial fibrillation and rheumatic mitral valve disease. Circulation. (2005) 112:I20–5. 10.1161/CIRCULATIONAHA.104.526301
8.
Gelsomino S La Meir M Van Breugel HN Renzulli A Rostagno C Lorusso R et al Surgical ablation in patients undergoing mitral valve surgery: impact of lesion set and surgical techniques on long-term success. Europace. (2016) 18(10):1528–37. 10.1093/europace/euv402
9.
McCarthy PM Manjunath A Kruse J Andrei AC Li Z McGee EC Jr et al Should paroxysmal atrial fibrillation be treated during cardiac surgery? J Thorac Cardiovasc Surg. (2013) 146:810–23. 10.1016/j.jtcvs.2013.05.015
10.
Gillinov AM Gelijns AC Parides MK DeRose JJ Jr Moskowitz AJ Voisine P et al Surgical ablation of atrial fibrillation during mitral-valve surgery. N Engl J Med. (2015) 372:1399–409. 10.1056/NEJMoa1500528
11.
Soni LK Cedola SR Cogan J Jiang J Yang J Takayama H et al Right atrial lesions do not improve the efficacy of a complete left atrial lesion set in the surgical treatment of atrial fibrillation, but they do increase procedural morbidity. J Thorac Cardiovasc Surg. (2013) 145:356–61; discussion 61–3. 10.1016/j.jtcvs.2012.09.091
12.
Henn MC Lancaster TS Miller JR Sinn LA Schuessler RB Moon MR et al Late outcomes after the cox maze IV procedure for atrial fibrillation. J Thorac Cardiovasc Surg. (2015) 150(5):1168–76, 1178.e1–2. 10.1016/j.jtcvs.2015.07.102
13.
Harlaar N Verberkmoes NJ van der Voort PH Trines SA Verstraeten SE Mertens BJA et al Clamping versus nonclamping thoracoscopic box ablation in long-standing persistent atrial fibrillation. J Thorac Cardiovasc Surg. (2020) 160(2):399–405. 10.1016/j.jtcvs.2019.07.104
14.
Van Gelder IC Rienstra M Bunting KV Casado-Arroyo R Caso V Crijns H et al 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-thoracic Surgery (EACTS). Eur Heart J. (2024) 45:3314–414. 10.1093/eurheartj/ehae176
15.
DeLurgio DB Crossen KJ Gill J Blauth C Oza SR Magnano AR et al Hybrid convergent procedure for the treatment of persistent and long-standing persistent atrial fibrillation: results of CONVERGE clinical trial. Circ Arrhythm Electrophysiol. (2020) 13(12):e009288. 10.1161/CIRCEP.120.009288
16.
Doll N Weimar T Kosior DA Bulava A Mokracek A Mönnig G et al Efficacy and safety of hybrid epicardial and endocardial ablation versus endocardial ablation in patients with persistent and longstanding persistent atrial fibrillation: a randomised, controlled trial. EClinicalMedicine. (2023) 61:102052. 10.1016/j.eclinm.2023.102052
17.
Schena S Lindemann J Carlson A Wilcox T Oujiri J Berger M et al Robotic-enhanced hybrid ablation for persistent and long-standing atrial fibrillation: early assessment of feasibility, safety, and efficacy. JTCVS Tech. (2024) 25:81–93. 10.1016/j.xjtc.2024.02.013
Summary
Keywords
atrial fibrillation, surgical ablation, arrhythmia surgery, left-atrial box lesion, AF surgery
Citation
Pecha S, Petersen J, Yildirim Y, Bazhanov I, Reichenspurner H and Alassar Y (2025) Closed atrium bipolar radiofrequency box lesion for concomitant surgical atrial fibrillation ablation. Front. Cardiovasc. Med. 12:1655695. doi: 10.3389/fcvm.2025.1655695
Received
28 June 2025
Accepted
05 August 2025
Published
20 August 2025
Volume
12 - 2025
Edited by
Federico Migliore, University of Padua, Italy
Reviewed by
Ernesto Cristiano, Humanitas Gavazzeni, Italy
Manuel De Lazzari, University Hospital of Padua, Italy
Raimondo Pittorru, University of Padua, Italy
Updates
Copyright
© 2025 Pecha, Petersen, Yildirim, Bazhanov, Reichenspurner and Alassar.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Simon Pecha s.pecha@uke.de
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.