Abstract
Parachute tricuspid valve is an exceedingly rare congenital anomaly, often described in association with acyanotic heart defects. Its occurrence alongside cyanotic congenital heart disease is even less common. We report the case of a 1-year-old boy presenting with complex cyanotic heart disease along with parachute tricuspid valve. Detailed evaluation revealed a constellation of anomalies, including parachute tricuspid valve, double outlet right ventricle with D-malposed great arteries, severe pulmonary stenosis, and a non-routable ventricular septal defect. Echocardiography played a vital role in defining the complex anatomy and guided the decision toward single-ventricle palliation. This case underscores the importance of meticulous anatomical assessment in patients with congenital heart disease and contributes to the sparse literature on this rare condition.
Introduction
Double outlet right ventricle (DORV) is a congenital cardiac malformation in which both great arteries arise predominantly from the right ventricle. Systemic output in DORV depends on the size and routability of the ventricular septal defect. Juxtaposed atrial appendages refer to an abnormal spatial arrangement in which both atrial appendages lie on the same side of the great arteries. Parachute valve anomalies are characterized by insertion of all chordae tendineae into a single papillary muscle (1). While the parachute mitral valve is a well-recognized component of Shone's complex and other left-sided obstructive lesions, the tricuspid variant is rarely reported.
We report a rare case of parachute tricuspid valve associated with complex cyanotic congenital heart disease in a 1-year-old child. The associated anomalies included double outlet right ventricle with D-malposed great arteries; a large, non-routable inlet ventricular septal defect; severe infundibular and valvar pulmonary stenosis; fossa ovalis atrial septal defect; juxtaposed atrial appendages; and a right-sided aortic arch. The rarity of parachute tricuspid valve in association with such complex cyanotic heart disease makes this case noteworthy.
Case report
A 1-year-old male child was referred for evaluation of persistent cyanosis and failure to gain weight since early infancy. There was no antenatal diagnosis, and fetal echocardiography had not been performed. There was no family history of congenital heart disease or consanguinity. Cyanosis was noted within the first few weeks of life and progressively worsened. The child had poor weight gain but no prior cardiac interventions.
At presentation, the child weighed 7.9 kg and measured 75 cm in height. Oxygen saturation on room air ranged from 72% to 76%. There was a grade 3/6 ejection systolic murmur best heard at the left upper sternal border.
Chest radiography revealed mild cardiomegaly with a narrow mediastinum and oligemic lung fields. Cardiac situs was normal, and the aortic arch was right-sided. Electrocardiography demonstrated sinus rhythm with a normal QRS axis, right atrial enlargement, and right ventricular hypertrophy (Figure 1).
Figure 1
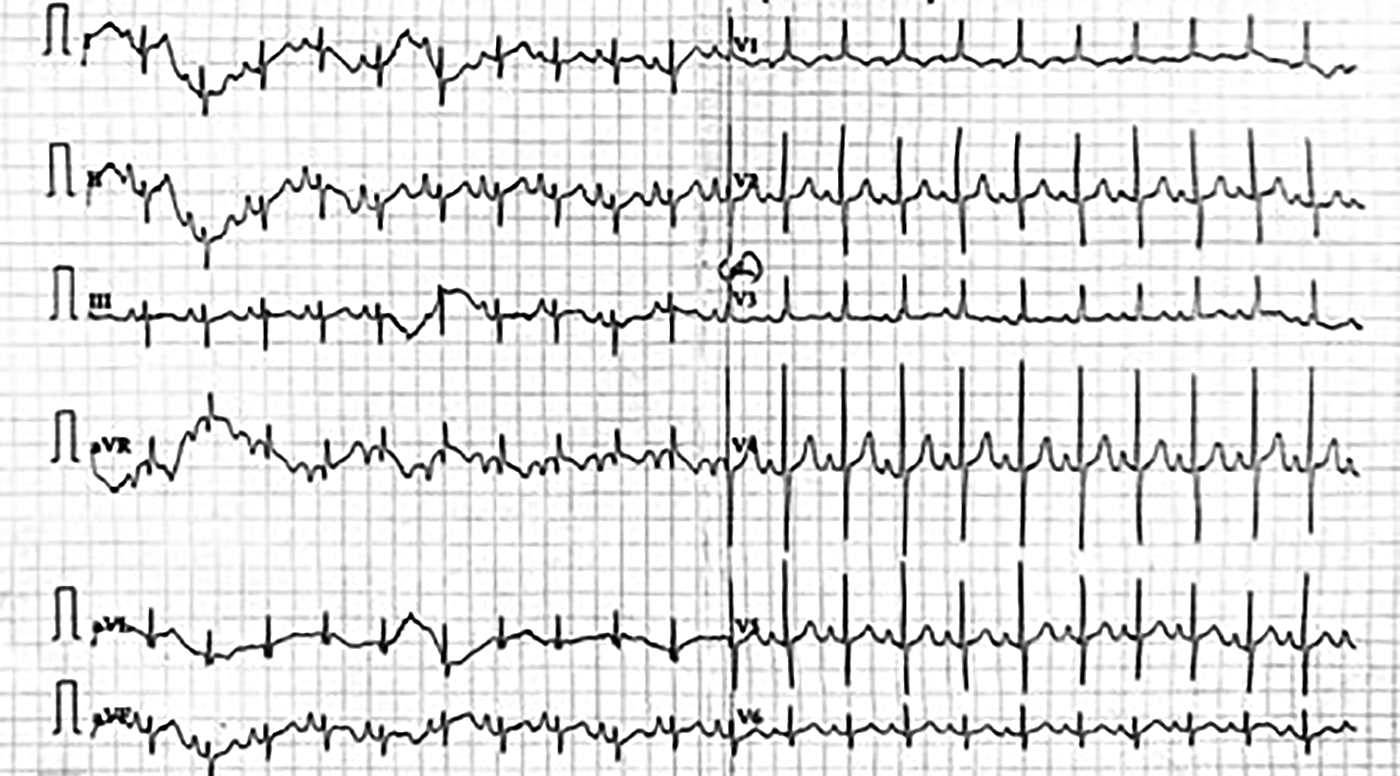
Full standardised ECG shows HR = 125/min, sinus rhythm with a normal QRS axis. There is evidence of right atrial enlargement.
Cross-sectional echocardiography and Doppler interrogation revealed situs solitus, levocardia, and concordant atrioventricular connections. Both systemic and pulmonary venous drainage were normal. A 6-mm fossa ovalis atrial septal defect with right-to-left shunt was present. The atrial appendages were juxtaposed to the left.
The tricuspid valve annulus measured 11 mm (Z score −2.3). Color and continuous-wave Doppler interrogation revealed flow acceleration across the tricuspid valve with a mean gradient of 6 mmHg (Figure 2). Further evaluation showed that all chordae of the tricuspid valve were inserted into a single papillary muscle attached near the septal surface of the right ventricle, consistent with parachute tricuspid valve (Figure 3). No tricuspid regurgitation was noted.
Figure 2
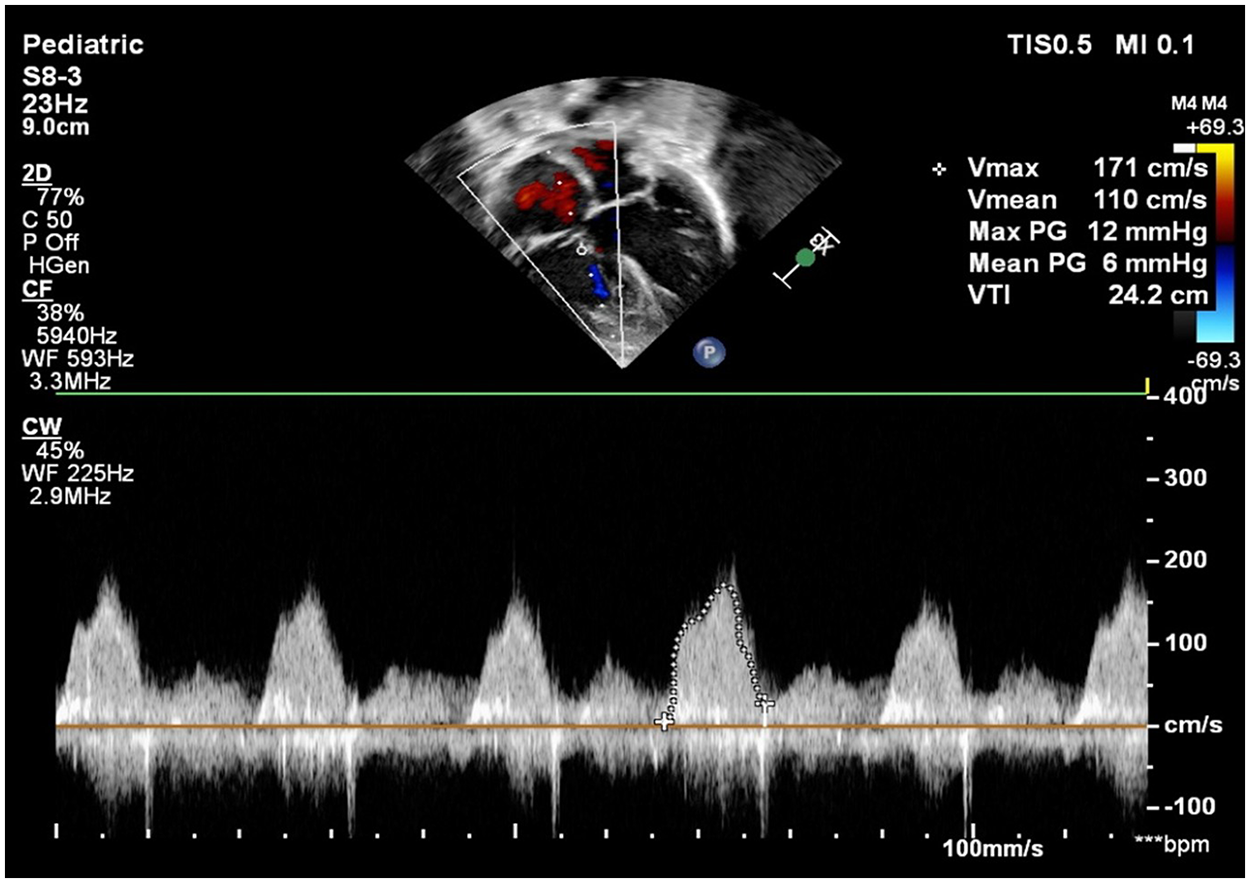
Continuous wave doppler at tricuspid inflow flow showing tricuspid valve stenosis mean gradient of 6 mmHg across tricuspid valve.
Figure 3
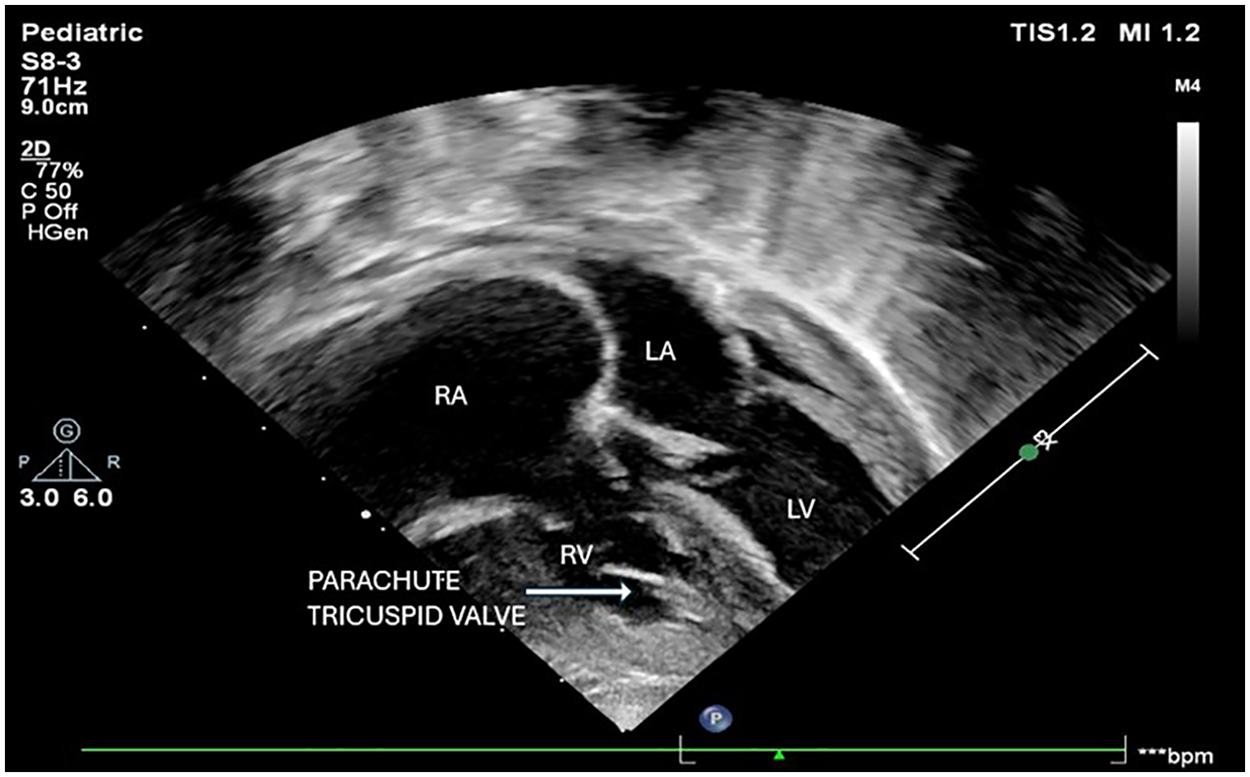
Apical four chamber view showing single papillary muscle on septal surface with chordal attachment from septal and anterior leaflets of tricuspid valve. Right atrium (RA), Right ventricle (RV), Left atrium (LA), Left ventricle (LV).
The morphological right ventricle was hypoplastic. Both great arteries originated from the right ventricle, with D-malposition of the great vessels. There was severe pulmonary stenosis with a peak gradient of 78 mmHg. The left ventricle was of normal size and communicated with the right ventricle through a non-restrictive, non-routable inlet ventricular septal defect. Branch pulmonary arteries were of acceptable size for age, and biventricular systolic function was preserved.
The combination of a non-routable ventricular septal defect, severe pulmonary stenosis, hypoplastic right ventricle, and tricuspid inflow obstruction precluded biventricular repair. The child underwent atrial septectomy along with a bidirectional Glenn shunt. No intervention was done on the tricuspid valve. Intraoperative findings confirmed the echocardiographic anatomy. The postoperative course was uneventful, and the patient was discharged on postoperative day 7. Postoperative echo on day 7 revealed good ventricular function, good interatrial communication, no gradient across the tricuspid valve, and a patent and well-functioning bidirectional Glenn shunt.
Discussion
Parachute tricuspid valve is a rare abnormality, far less commonly reported than its mitral counterpart. The defining feature of this anomaly is the insertion of all tricuspid chordae into a single papillary muscle, resulting in varying degrees of tricuspid inflow obstruction. Most reported cases have been associated with acyanotic cardiac defects such as atrial or ventricular septal defects (2, 3). In the published literature, only two cases have been reported in association with complex cardiac defects—one with Tetralogy of Fallot (4) and another with congenitally corrected transposition of great arteries (5).
Recognition of tricuspid inflow obstruction is particularly important when biventricular repair is contemplated. In the presence of a right-to-left atrial shunt, it is often difficult to assess tricuspid valve stenosis, and one may underestimate or completely miss the stenosis on Doppler alone. However, a properly performed cross-sectional study can clearly document chordal attachments and detect the abnormality. In the presence of tricuspid stenosis, complete closure of the atrial communication can cause a rise in atrial pressure and lead to deleterious effects upon hepatic and splanchnic circulation. Leaving a small atrial communication or adding a superior cavopulmonary anastomosis may be needed in such patients.
In our patient, the presence of a large inlet ventricular defect, double outlet right ventricle, and D-malposed aorta precluded a biventricular option. The patient underwent a bidirectional Glenn shunt with enlargement of atrial communication. The patient remains under regular follow-up and is scheduled for Fontan completion after 2 years.
Echocardiography played a vital role in delineating the anatomical details and surgical planning.
Case reports of parachute tricuspid valve with other associated heart disease mentioned in Table 1 have been described previously by Yuan et al. (6).
Table 1
| Year | Author | Age | Sex | Papillary muscle | Associated anomalies | TV dysfunction | Diagnostic modality | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1979 | Milo et al. | Neonate (op at 6 years 8 months) | M | Single | DORV, straddling MV, RVOT obstruction, inlet VSD | TS | Autopsy | MV repair + VSD closure | Died |
| 1979 | Ariza et al. (4) | Neonate | NR | Single | TOF with pulmonary atresia | TS | Echo | NR | NR |
| 1980 | Maitre Azcarate | NR | NR | Single (apical) | Cor triatriatum | Leaflet fusion | Autopsy | None | Died |
| 1997 | Godart et al. | Neonate (followed to 2 years) | F | Single anterior | CCTGA, VSDs, hypoplastic arch, CoA, PDA, PAH | Severe TS (annular ring) | Echocardiography | Annular ring resection + TVR | Died (septic shock) |
| 2006 | Marwah et al. (2) | 21 years | F | Single | ASD, VSD | Mild TS/near-normal | TTE | Follow-up | Unchanged |
| 2010 | Uçar et al. | 25 years | M | Single | VSD | TR | TTE | Follow-up | NR |
| 2012 | Demirkol et al. | 21 years | M | Single | Isolated PTV | Trivial TR | TTE, 3D-TTE, 3D-TEE, CTA | Follow-up | Stable |
| 2012 | Demirkol et al. | 24 years | M | Single (bifid) | ASD | Trivial TR | TTE, 3D-TEE, CTA | Surgical ASD closure | Recovered |
| 2012 | Mohan et al. (3) | 30 years | NR | Single (short) | ASD, PAH | TR | TTE, Cardiac CT | Follow-up | NR |
| 2013 | Kurtul et al. | 33 years | M | Single | PMV, VSD, PAH, anomalous LCx | Normal TV function | TTE | Transcatheter VSD closure | Recovered |
| 2015 | Mohan et al. (5) | 23 years | F | Single | PMV, CCTGA, PS, BAV | Mild TR | TTE | Follow-up | Unchanged |
| 2016 | Gupta et al. | 7.5 months | M | Single | ASD, VSD | Severe TS | TTE | VSD closure + chordal transfer + ASD closure | Recovered |
| 2017 | Alimi and Fazlinezhad | 52 years | F | Single (calcified) | ASD | Moderate–severe TR | TTE, 3D-TEE | ASD device closure | Improved |
| 2017 | Alimi and Fazlinezhad | 30 years | F | Single (calcified) | None | Mild–moderate TR | TTE, 3D-TTE | Follow-up | No change |
Published case reports of parachute tricuspid valve.
[Data summarized from Yuan et al. (6)]. ASD, atrial septal defect; BAV, bicuspid aortic valve; CCTGA, congenitally corrected transposition of great arteries; CoA, coarctation of aorta; CTA, computed tomographic angiography; DORV, double outlet right ventricle; MV, mitral valve; PAH, pulmonary artery hypertension; PMV – parachute mitral valve; PS – pulmonary stenosis; PTV, parachute tricuspid valve; TR, tricuspid regurgitation; TS, tricuspid stenosis; TVR, tricuspid valve replacement; VSD, ventricular septal defect.
However, to the best of our knowledge, the occurrence of parachute tricuspid valve in association with double outlet right ventricle, D-malposed great arteries, severe pulmonary stenosis, non-routable ventricular septal defect, and juxtaposed atrial appendages has not been previously reported.
Conclusion
This report describes an exceptionally rare constellation of congenital cardiac anomalies, including parachute tricuspid valve, double outlet right ventricle with D-malposed great arteries, severe pulmonary stenosis, non-routable ventricular septal defect, and juxtaposed atrial appendages. These findings resulted in severe cyanosis and necessitated a single-ventricle palliation strategy. The case highlights the importance of detailed echocardiographic assessment in complex congenital heart disease, using both two-dimensional and color Doppler to achieve a complete diagnosis. Furthermore, the report also demonstrates how a rare atrioventricular valve abnormality can affect surgical decision-making.
Statements
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s), and minor(s)' legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributions
DS: Writing – review & editing, Writing – original draft. AM: Writing – original draft, Investigation, Supervision, Validation, Writing – review & editing. VJ: Writing – original draft, Writing – review & editing.
Funding
The author(s) declared that financial support was not received for this work and/or its publication.
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
PTV, parachute tricuspid valve; CCHD, cyanotic congenital heart disease; RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle; DORV, double outlet right ventricle; VSD, ventricular septal defect; PS, pulmonary stenosis.
References
1.
Swan H Trapnell JM Dens TJ . Congenital mitral stenosis and systemic right ventricle with associated pulmonary vascular changes frustrating surgical repair of patent ductus arteriosus and coarctation of the aorta. Am Heart J. (1949) 38(6):914–23. 10.1016/0002-8703(49)90892-3
2.
Marwah A Suresh PV Shah S Misra A Maheshwari S . Parachute tricuspid valve. Eur J Echocardiogr. (2006) 7:226–7. 10.1016/j.euje.2005.10.002
3.
Mohan JC Shekhar C Mohan V Kaur B Singh SK . Parachute tricuspid valve in an asymptomatic adult. Indian Heart J. (2012) 64(1):93–4. 10.1016/S0019-4832(12)60020-0
4.
Ariza S Cintado C Castillo JA Descalzo A Cañadas M Santos J et al Parachute tricuspid valve associated with fallot’s tetralogy. Arch Mal Coeur Vaiss. (1979) 72(3):317–20.
5.
Mohan JC Shukla M Sethia A . Parachute deformity of both atrioventricular valves with congenitally corrected transposition in an adult. Indian Heart J. (2015) 67(6):565–9. 10.1016/j.ihj.2015.06.012
6.
Yuan SM . Parachute tricuspid valve: a systematic review. Orphanet J Rare Dis. (2020) 15(1):305. 10.1186/s13023-020-01561-y
Summary
Keywords
cyanotic congenital heart disease, double outlet right ventricle, parachute tricuspid valve, pulmonary stenosis, ventricular septal defect
Citation
Sangwan D, Marwah A and Jain V (2026) Case Report: Parachute tricuspid valve in association with cyanotic congenital heart disease and juxtaposed atrial appendages in a 1-year-old boy—a rare anatomical association. Front. Cardiovasc. Med. 13:1683429. doi: 10.3389/fcvm.2026.1683429
Received
11 August 2025
Revised
06 January 2026
Accepted
16 January 2026
Published
19 February 2026
Volume
13 - 2026
Edited by
Xiaofeng Yang, Temple University, United States
Reviewed by
Maruti Haranal, U N Mehta Institute of Cardiology and Research, India
Ayham Qatza, University of Hama, Syria
Updates
Copyright
© 2026 Sangwan, Marwah and Jain.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Devender Sangwan devsangwan9@gmail.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.