 Zhuo Li1
Zhuo Li1 Lu Cao
Lu Cao- 1Department of Pharmacy, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi, China
- 2Department of Intensive Care Unit, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi, China
- 3Department of Pharmacy, Nanjing Drum Tower Hospital, Nanjing, Jiangsu, China
- 4Department of Clinical Laboratory, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi, China
Objective: To compare and analyze the efficacy and safety of different antifungal drug treatment regimens for patients with invasive pulmonary aspergillosis (IPA) in the intensive care unit (ICU).
Methods: We retrospectively collected the clinical data of patients with IPA in the ICU in two grade-A tertiary hospitals from January 2019 to January 2024 using the HIS system and compared the clinical efficacy, incidence of adverse drug reactions (ADRs), and all-cause mortality at discharge among different antifungal treatments, such as voriconazole alone, caspofungin alone, and a combination of voriconazole plus caspofungin.
Results: A total of 151 patients were enrolled, including 129 in the monotherapy group (with 92 in the voriconazole subgroup and 37 in the caspofungin subgroup) and 22 in the voriconazole plus caspofungin combination group. Aspergillus fumigatus was the most common pathogenic fungus in patients with IPA, followed by Aspergillus flavus. In terms of clinical efficacy, monotherapy and combination therapy were equally effective (P=0.618), and the efficacy of voriconazole or caspofungin alone and that of voriconazole combined with caspofungin in the treatment of IPA was equivalent (P=0.630). In terms of safety, the total incidence of ADRs in the combination therapy group was greater than that in the monotherapy group, but the difference was not statistically significant (P=0.109). The two groups were also equally safe in terms of causing renal dysfunction, liver dysfunction, visual abnormalities, and hypokalemia. However, compared with the monotherapy group, the combination therapy group exhibited a significantly greater incidence of pancytopenia (P=0.013, P=0.004). The all-cause mortality in the combination therapy group was significantly greater than that in the monotherapy group (P=0.027, P=0.009).
Conclusions: Voriconazole is still the preferred treatment for critically ill patients with IPA, and caspofungin has good clinical efficacy and safety and can effectively replace voriconazole for these patients. However, the combination treatment with voriconazole and caspofungin did not improve the all-cause mortality rate of critically ill patients with IPA, is associated with increased total ADR and pancytopenia incidence and is not recommended as an initial treatment plan.
1 Introduction
Invasive fungal disease (IFD) refers to a severe fungal infection in which fungi invade the human body; proliferate in tissues, organs, or blood; and cause severe inflammation or tissue damage. These are life-threatening fungal infections with a high mortality rate. In recent years, the incidence of IFD has steadily increased due to the widespread use of glucocorticoids, broad-spectrum antibiotics, and immunosuppressive agents in clinical practice. Patients in the ICU are more susceptible to IFD due to the impairment or collapse of their physiological defense mechanisms, which can exacerbate their original diseases. Research shows that the overall case fatality rate of these patients exceeds 80% (Chinese Society of Critical Care Medicine, 2007).
Aspergillus is a fungal genus that is widely distributed in the natural environment, and these fungi have strong adaptability and transmissibility. These microorganisms infiltrate the human body through the respiratory tract, causing aspergillosis (Guo et al., 2023). Among these species, Aspergillus fumigatus is the most common pathogen, accounting for approximately 70~80% of the reported cases (Walsh et al., 2008). Other non-A. fumigatus species include A. flavus, A. niger, A. nidulans, A. terreus, and A. versicolor (Cadena et al., 2016; Yii et al., 2017). Despite significant progress, aspergillosis remains a serious health problem, with its epidemiology constantly evolving and the population of high-risk patients expanding continuously (Herrera et al., 2025). Invasive pulmonary aspergillosis (IPA) is the most severe form of Aspergillus invasion and is also the most common type of invasive fungal infection in ICU patients (Liu et al., 2017; Herrera et al., 2025). IPA carries a significant risk of death and imposes a substantial burden on affected individuals (Quindós, 2014). Improving the clinical prognosis of IPA depends on two key factors: the accuracy of diagnosis and the precision of antifungal treatment. However, unfortunately, owing to the nonspecificity of symptoms, the diagnosis of IPA is extremely challenging (Tunnicliffe et al., 2013). Moreover, for some diagnostic techniques, such as sputum culture, considerable effort is needed to obtain a result (Donnelly et al., 2020). Therefore, clinicians often provide empirical treatment for patients suspected of having IPA, which severely limits the effectiveness of clinical treatment.
The guidelines for the treatment of fungal infections in adult respiratory and ICU Patients published by the American Thoracic Society (ATS) in 2011 recommended prompt and aggressive antifungal therapy upon clinical suspicion or diagnosis of IPA (Limper et al., 2011). The 2016 version of the clinical practice guidelines on Aspergillus infections by the Infectious Diseases Society of America (IDSA) recommended voriconazole as the first-line treatment for IPA, with alternative and salvage therapies including amphotericin B, itraconazole, or caspofungin. Combination therapy with voriconazole and an echinocandin is generally reserved for salvage treatment when the initial therapy is ineffective (Patterson et al., 2016).
The current recommendations for IPA treatment are based primarily on evidence from patients with hematological disorders or malignancies, leaving a gap in recommendations based on evidence from other IPA populations, such as patients in the ICU (Zheng, 2018; Yang et al., 2021). Given that the treatment of IPA is mostly empirical in ICUs, with relatively low cure rates and high mortality rates, clinicians are increasingly inclined to use combination therapy (Yang et al., 2021). Studies have reported that up to 30% of critically ill IPA patients require salvage treatment (Wang and Xu, 2019; Han, 2020; Yang et al., 2021). However, there is limited clinical experience regarding the efficacy and safety of alternative regimens and combination therapy for IPA. Therefore, this study aimed to include patients who were clearly diagnosed with IPA on the basis of the results of fungal culture. First, in this study, we aimed to understand the epidemiological characteristics of Aspergillus in the local area. Second, we compared the efficacy and safety of voriconazole monotherapy, caspofungin monotherapy, and combination therapy with voriconazole plus caspofungin treatment in critically ill IPA patients to provide a reference for clinical practice.
2 Materials and methods
2.1 Study design and eligibility criteria
This retrospective multicenter real-world study included patients diagnosed with IPA based on the European Organization for Research and Treatment of Cancer and Mycoses Study Group Education and Research Consortium (EORTC/MSGERC) consensus definitions of IFD (Donnelly et al., 2020; Alexander et al., 2021); the patients were treated at two Grade-A tertiary hospitals between January 2019 and January 2024. The inclusion criteria for the patients were as follows: (1) aged ≥ 18 years; (2) admitted to ICUs; (3) positive culture of Aspergillus species (Cadena et al., 2016) (e.g., A. fumigatus, A. flavus, A. niger, A. terreus, etc.) from sputum or bronchoalveolar lavage fluid; (3) initial antifungal treatment via monotherapy, including voriconazole alone and caspofungin alone, or combination therapy with voriconazole plus caspofungin, at doses consistent with guidelines and drug labels; and (4) duration of antifungal therapy ≥ 3 days (Cao et al., 2023). The exclusion criteria for patients were as follows (Li et al., 2024; Yuan et al., 2025): (1) patients with documented allergies to voriconazole or caspofungin; (2) patients with Aspergillus genus that had not been identified to the species level; (3) patients who were pregnant or breastfeeding; (4) patients with other severe infectious diseases; (5) patients who were participating in other clinical studies simultaneously; and (6) patients with incomplete medical records or missing clinical laboratory data.
The identification of Aspergillus species was carried out using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) (Zhang et al., 2023), and the specific operation steps are described below. (1) The method for extraction with formic acid and acetonitrile was as follows: Colonies were cultured on potato dextrose agar (PDA) for 3 days were scraped with an inoculation loop. The mycelia at the edge were picked and added to a mixture of 300 μL of pure water and 900 μL of absolute ethanol. The mixture was shaken and then centrifuged at 13,000 r/min for 2 minutes. The supernatant was discarded, and the residue was dried. Then, 50 μL of 70% formic acid was added, and the mixture was shaken for 20 seconds at 4,000 r/min to break the cell wall. This process was repeated twice, after which the mixture was allowed to stand for 5 minutes. Then, 50 μL of acetonitrile was added, and the mixture was left to stand for 5 minutes. The mixture was centrifuged at 13,000 r/min for 2 minutes, and the resulting supernatant was used as the fungal protein template. (2) The modified method of extraction with zirconium bead grinding, formic acid and acetonitrile was as follows: young mycelia cultured on PDA for 2 days were scraped with an inoculation loop, added to 1 mL of potato broth, and shaken horizontally on a shaker at 28°C for 24 hours to enrich the fungi, which formed dense colonies visible to the naked eye. Two zirconium beads were added, and the remaining operations were performed as described for the extraction method with formic acid and acetonitrile. (3) Mass spectrometry was performed as follows: one microliter of fungal protein was used to spot the target plate. After air-drying, the sample was covered with 1 μL of matrix. After air-drying again, mass spectrometry identification was performed. (4) Identification scoring was performed as follows: the target plate was spotted twice for each fungal strain for identification. The names of the fungi and the identification scores were recorded when the results were consistent. The identification criteria were as follows: the score for identification at the species level was ≥ 2.0 points; if the score was lower than 2.0 points but the top 5 results from all identifications were for the same fungal species and the score was between 1.7 and 2.0 points, identification was considered successful at the genus level; if the score was lower than 1.7 points or if the identification results included multiple fungal species, identification was considered unsuccessful.
2.2 Variables and definitions
We collected detailed information from medical records, including information on demographics (e.g., age, sex, and underlying conditions), clinical characteristics (Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, symptoms, imaging results, blood gas parameters, oxygenation indices), biochemical examinations (liver and kidney function (e.g., serum creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), total bilirubin (TB) and conjugated bilirubin (CB) levels), routine blood tests (white blood cell (WBC), neutrophil, hemoglobin (HB) and platelets (PLT) levels), fungal culture results (e.g., fungal detection, sampling and clearance), antifungal treatment regimens and durations, and any recorded adverse drug reactions (ADRs).
Patients were grouped into a voriconazole monotherapy group, a caspofungin monotherapy group, and a combination therapy group treated with voriconazole plus caspofungin. Only the initial therapy regimen was considered for the analysis of clinical efficacy and safety if treatment regimens were subsequently changed during therapy.
2.3 Clinical outcomes and criteria
Clinical outcomes at discharge, including clinical efficacy, all-cause mortality and ADRs, were also assessed.
Safety was evaluated on the basis of ADRs, e.g., liver function, kidney function, routine blood test results, and other ADRs recorded before and after antifungal therapy. Renal toxicity was defined as an increase in serum creatinine level of at least 0.55 mg/dL or a rise of ≥50% from baseline (Cao et al., 2022). Liver damage was diagnosed when AST, ALP, and TB levels were simultaneously elevated, with at least one exceeding twice the upper limit of normal (ULN), or when the ALT or CB level exceeded twice the ULN after ruling out viral hepatitis and other causes of liver injury (Yu et al., 2017). Hematological toxicity was diagnosed as reductions in WBC, HB, and PLT counts to below normal reference ranges after antifungal therapy (Wang et al., 2021). Other ADRs, such as nausea, vomiting, rash, diarrhea, visual disturbances, and hypokalemia, were identified on the basis of drug label descriptions.
According to the published literature (Yang et al., 2021), clinical efficacy was classified into three levels: the patient was considered cured if symptoms, laboratory tests, and imaging findings were normal and all pathogens had been cleared. The treatment was considered markedly effective if significant improvement in symptoms and laboratory tests was observed, with ≥50% improvement on imaging, but with some persisting abnormalities. The treatment was considered ineffective if no significant improvement or worsening of clinical condition or imaging findings, or even death, was observed. The total efficacy of antifungal treatment = (number of cured patients + number of patients with marked effect)/total number of patients × 100%.
2.4 Statistical analysis
Statistical analysis was performed using SPSS 23.0 software. Categorical variables are expressed as frequencies and percentages, with group comparisons via the χ2 test or Fisher’s exact test. Continuous variables conforming to a normal distribution are expressed as x ± s, with group comparisons performed via one-way ANOVA. The ordinal variables were compared using the Mann–Whitney U test. The Logistic regression analysis method was used to evaluate the risk factors associated with all-cause mortality. First, the univariate Logistic regression analysis method was employed. By calculating the P - value, odds ratios (ORs), and 95% confidence intervals (95% CI), the correlation between confounding factors and all-cause mortality was initially explored, especially the impact of antifungal treatment regimens on it. Second, the multivariate Logistic regression analysis method was used. The antifungal treatment regimens and the confounding factors with P < 0.05 in the univariate analysis results were included in the multivariate analysis. A stepwise multiple regression analysis model was adopted for analysis to identify the independent predictors associated with all-cause mortality, especially the impact of antifungal treatment regimens on it. The strength of the correlation between independent risk factors and all - cause mortality was evaluated by calculating the adjusted odds ratios (adjusted ORs) and 95% confidence intervals (95% CI). A p value of <0.05 was considered to indicate statistical significance.
3 Results
3.1 Clinical characteristics
A total of 151 patients were included in this study. The patients were divided into a monotherapy group, which included 129 patients (85.43%), consisting of a voriconazole monotherapy subgroup and a caspofungin monotherapy subgroup, and a combination therapy group, which included 22 patients (14.57%). The voriconazole monotherapy subgroup included 92 patients (64 males, 28 females) with a mean age of 68.48 ± 13.85 years, an average treatment duration of 7.48 ± 5.31 days, and a mean APACHE II score of 15.64 ± 7.24. The most common underlying conditions were type 2 diabetes and chronic obstructive pulmonary disease (COPD). The caspofungin monotherapy subgroup included 37 patients (22 males, 15 females) with a mean age of 67.89 ± 14.14 years, an average treatment duration of 8.92 ± 6.26 days, and a mean APACHE II score of 16.24 ± 5.71. COPD was the most common underlying condition, followed by hypertension and type 2 diabetes. The combination therapy group included 22 patients (13 males, 9 females) with a mean age of 68.23 ± 11.22 years, an average treatment duration of 6.73 ± 3.03 days, and a mean APACHE II score of 18.21 ± 9.46. The common underlying conditions were COPD, renal failure, and type 2 diabetes. Approximately 50% of the patients in each of the three groups had a history of steroid use. There were no statistically significant differences (P>0.05) observed among the three groups in terms of age (P=0.975), sex (P=0.434), BMI (P=0.904), history of steroid use (P=0.722), treatment duration (P=0.244), underlying conditions, APACHE II score (P=0.073), etc. (see Table 1 for details).
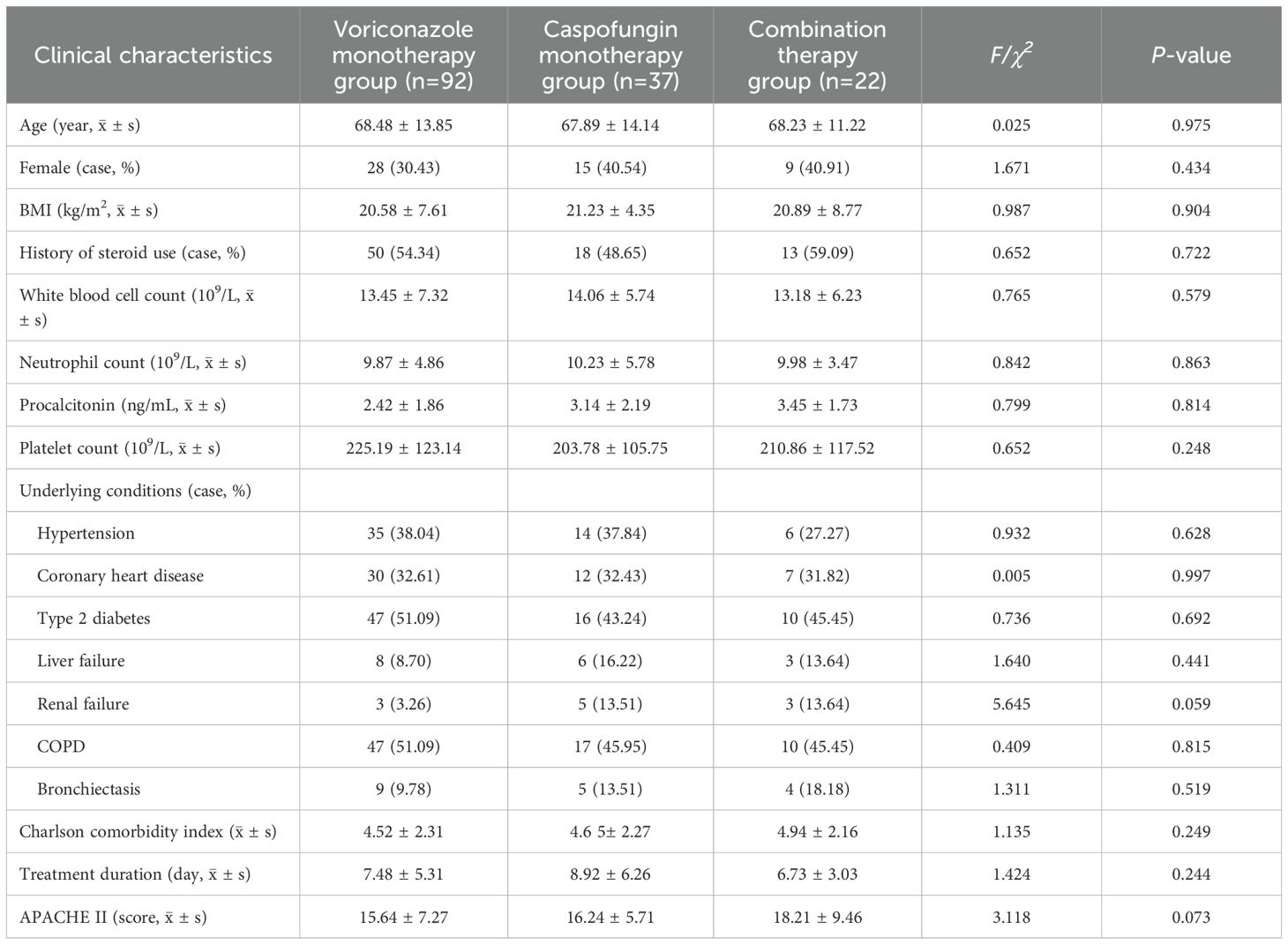
Table 1. Comparison of clinical characteristics among antifungal treatment regimens.
3.2 Fungal culture results
The MALDI-TOF MS identification results of fungal cultures of the included patients were all ≥ 2.0 points. Fungal culture results revealed that A. fumigatus was the most common pathogen in IPA patients, with 106 patients (70.20%) testing positive. A. flavus ranked second, with 27 patients (17.88%), followed by A. niger with 7 patients (6.64%) and A. terreus with 6 patients (3.97%), and A. nidulans was the least common, with 5 patients (3.31%) (see Table 2 for details).
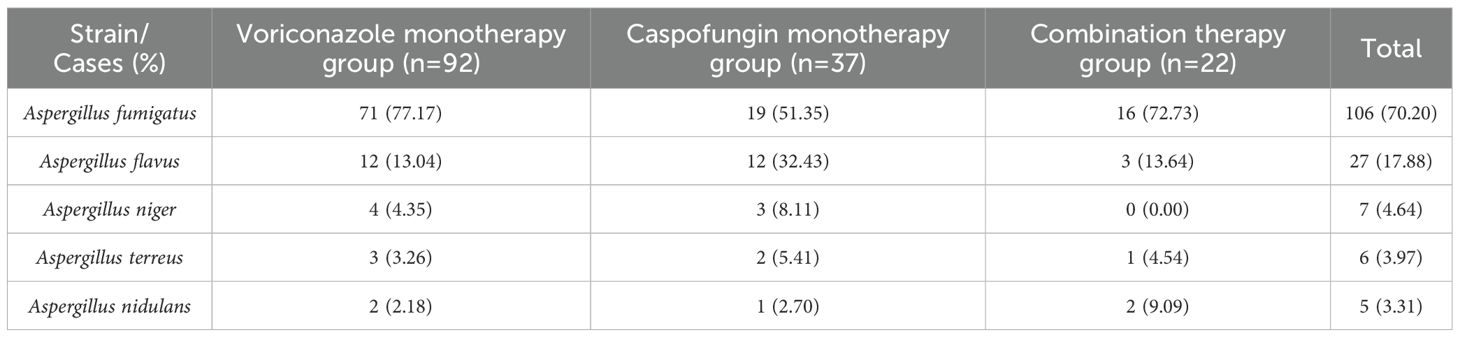
Table 2. Comparison of fungal culture results among antifungal treatment regimens.
3.3 Clinical efficacy
As shown in Table 3, among patients treated with monotherapy, clinical effectiveness was achieved in 50 patients, resulting in an overall effectiveness rate of 38.76%, which was slightly higher than the 36.36% observed in the combination therapy group. However, this difference was not statistically significant (P=0.618). The clinical effectiveness rate for voriconazole monotherapy was 41.30%, which was slightly higher than the 32.43% observed for caspofungin monotherapy and the 36.36% observed for the combination therapy. However, the differences among the three groups were not statistically significant (P=0.630). These results suggested that voriconazole or caspofungin monotherapy was as effective as the combination therapy for IPA treatment.

Table 3. Comparison of clinical efficacy among antifungal treatment regimens.
3.4 Adverse drug reactions
The incidence of ADRs, including liver dysfunction (21 cases, 22.83%), renal dysfunction (18 cases, 19.57%), pancytopenia (8 cases, 8.70%), hypokalemia (4 cases, 4.35%), and visual disturbances (2 cases, 2.17%), was lowest in the voriconazole monotherapy group. The incidence of ADRs in the caspofungin monotherapy group ranked second (67.57%), and the common ADRs were liver dysfunction (11 cases, 29.73%), renal dysfunction (9 cases, 24.32%), pancytopenia (7 cases, 18.92%) and hypokalemia (4 cases, 10.81%). The incidence of ADRs, including pancytopenia (6 patients, 27.27%), renal dysfunction (6 patients, 27.27%), liver dysfunction (4 patients, 18.18%), hypokalemia (3 patients, 13.64%), and visual disturbances (2 patients, 9.09%), was highest in the combination therapy group.
The results revealed no statistically significant differences in total ADR incidence (P=0.109) or the incidence of renal dysfunction (P=0.506), liver dysfunction (P=0.500), visual disturbances (P=0.188), or hypokalemia (P=0.426) between the monotherapy group and the combination therapy group. However, the incidence of pancytopenia was significantly greater in the combination therapy group than in the monotherapy group (P=0.013). Among the three treatment regimens, the differences in the incidence of renal dysfunction (P=0.673), liver dysfunction (P=0.564), visual disturbances (P=0.099), and hypokalemia (P=0.072) were not statistically significant; however, the incidence of total ADRs (P=0.010) and pancytopenia (P=0.004), was highest in the combination group, followed by the caspofungin group and then the voriconazole group, and the differences were statistically significant (Table 4).
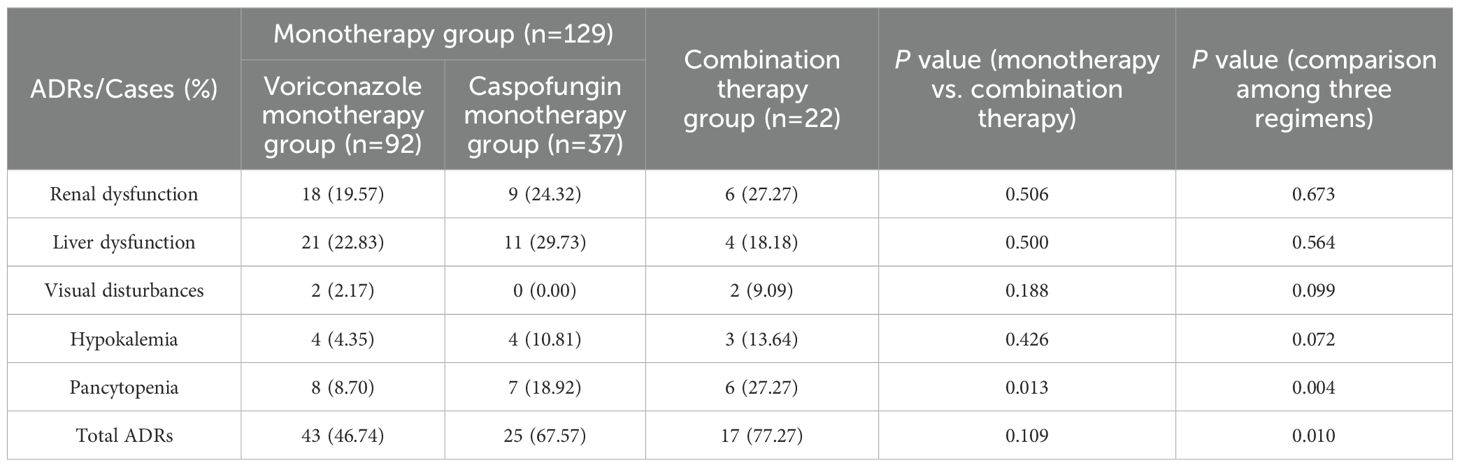
Table 4. Comparison of the incidence of ADRs among antifungal treatment regimens.
3.5 All-cause mortality
The all-cause mortality rate in the monotherapy group was 13.18% (17 cases), which was significantly lower than that in the combination therapy group (7 cases, 37.82%, P=0.027). The voriconazole group had the lowest all-cause mortality rate (8 cases, 8.70%), and the caspofungin group had the second highest all-cause mortality rate (9 cases, 24.32%), all of which were lower than those in the combination group (7 cases, 31.82%). The differences among the three regimens were statistically significant (P=0.009) (Table 5).

Table 5. Comparison of all-cause mortality among antifungal treatment regimens.
The results of both univariate and multivariate regression analyses showed that there was no significant correlation between the three antifungal treatment regimens, namely voriconazole monotherapy, caspofungin monotherapy, and the combination of voriconazole plus caspofungin, and all-cause mortality. That was to say, the initial choice of combination therapy could not reduce the all-cause mortality of IPA. See Table 6.
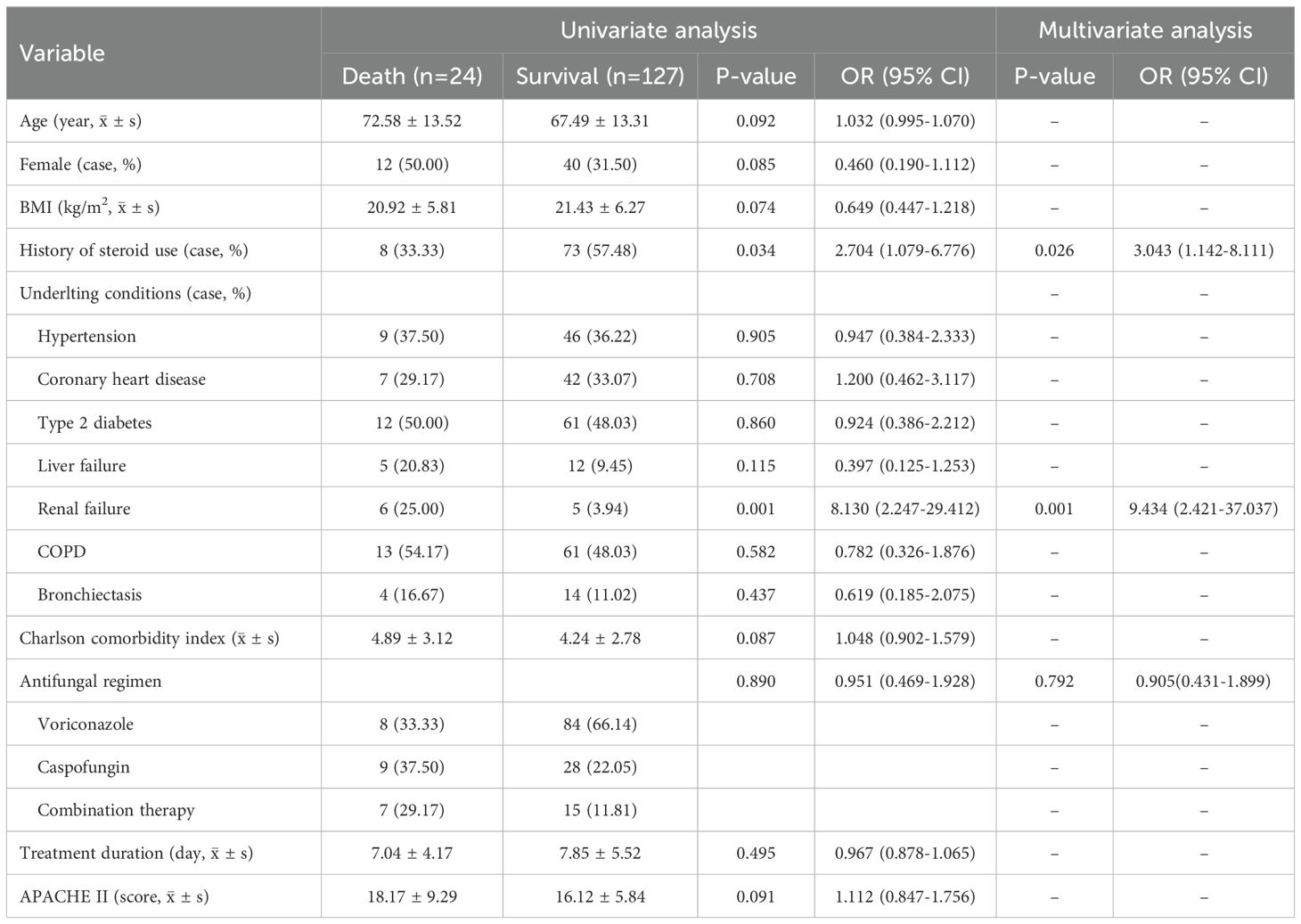
Table 6. Univariate and multivariate analyses of all-cause mortality in patients with IPA.
4 Discussion
IPA is the most common type of IFD in patients in the ICU and is characterized by atypical clinical symptoms, such as cough, sputum production, shortness of breath, chest tightness, and fever, which are often indistinguishable from the symptoms of other pulmonary infections, leading to frequent misdiagnosis or delayed diagnosis (Lei et al., 2020). Although IPA is traditionally associated with immunocompromised patients, recent studies have shown that immunocompetent patients are also at risk, with an increasing incidence in such patients observed in recent years, requiring the attention of clinicians and pharmacists (Wang, 2022).
IPA progresses rapidly and has a high mortality rate. Studies report that, without aggressive treatment, it can lead to patient death within 7–14 days (Lei et al., 2020). Therefore, timely diagnosis and prompt antifungal treatment are crucial for improving outcomes in IPA patients (Tian et al., 2020). Voriconazole is a triazole antifungal agent that works by inhibiting the synthesis of ergosterol, a necessary component of the fungal cell membrane, thus disrupting the integrity of the fungal cell and achieving antifungal effects (Zhang and Ma, 2019; Li et al., 2021). It is the first-line treatment for IPA recommended by the IDSA. Caspofungin is an echinocandin antifungal agent that inhibits the synthesis of β-(1,3)-D-glucan in the cell walls of Aspergillus species, making it an alternative or salvage treatment for IPA, as recommended in the guidelines (Hou and Xu, 2017). In this study, a majority of the 151 IPA patients initially received voriconazole monotherapy, in accordance with the guidelines. Additionally, 25% of patients were treated with caspofungin monotherapy due to good initial empirical treatment response, good liver function at admission, or physician habits and experience. The combination of voriconazole and caspofungin was less frequently used.
When treating IPA, obtaining accurate pathogen information or understanding the epidemiological characteristics of local Aspergillus strains is of utmost importance (Herrera et al., 2025), as different Aspergillus species exhibit varying sensitivities to drugs, and some even have innate resistance. For instance, most Aspergillus species are sensitive to amphotericin B, while A. terreus has innate resistance to amphotericin B, and A. flavus can develop acquired resistance (Su et al., 2019). MALDI-TOF MS is a novel soft ionization mass spectrometry technique for the identification of clinical microbial pathogens. It detects the protein fingerprint of microorganisms and compares the unique mass spectral peaks of different fungal species with the mass spectrometry database to quickly obtain microbial identification results. It demonstrates advantages in fungal homology analysis, pathogen typing, virulence factor identification, and drug resistance detection. The research findings of Zhang et al. showed that the accuracy rate of MALDI-TOF MS in identifying filamentous fungi to the species level was 92.9%, which was significantly higher than that of traditional manual identification methods. In our study, MALDI-TOF MS was used to identify Aspergillus species. The results revealed that in this region, A. fumigatus was the most common pathogenic fungus, accounting for approximately 70% of the fungal community. This was followed by A. flavus, A. niger, A. terreus and A. nidulans. This finding was essentially consistent with the reported epidemiology of Aspergillus species in mainland China (Khan et al., 2024). Previously, epidemiological studies on Aspergillus species have been conducted in China and other countries (Chen et al., 2018; Ma et al., 2019; Romero et al., 2019). In mainland China, A. fumigatus has always been identified as the most common Aspergillus species, accounting for 75.14% (Wang et al., 2019). Among the non-A. fumigatus species, A. flavus (12.25%) has the second highest prevalence rate, followed by A. niger (6.14%), A. terreus (0.82%) and A. nidulans (3.96%). A. flavus, the second most common non-A. fumigatus pathogen, had been reported in many countries (Lestrade et al., 2019; Pfaller et al., 2022). In contrast, in some countries, A. niger and A. terreus were considered the second most common Aspergillus species (He et al., 2012). Aspergillosis is mainly caused by A. fumigatus. However, some reported cases in China had shown that aspergillosis can also be caused by non-A. fumigatus species (Shen et al., 2022). This indicateed that A. fumigatus was not the sole pathogen of aspergillosis.
Voriconazole is the first-line treatment for invasive aspergillosis (IA) and has become the main treatment method in the past 20 years. Studies have reported that it can significantly improve the treatment outcome of patients at 12 weeks (Herbrecht et al., 2002; Ullmann et al., 2018). Caspofungin is an alternative treatment for IA, but it has never been evaluated as a monotherapy for IA in a randomized controlled trial (RCT) (Herrera et al., 2025). It is usually recommended that after the initial treatment regimen fails, other types of drugs should be selected for monotherapy or combination therapy (Patterson et al., 2016; Tissot et al., 2017). In this study, the efficacy of the initial choice of monotherapy or combination therapy was comparable. Further research revealed that the clinical effectiveness rate of voriconazole monotherapy was essentially comparable to that of caspofungin monotherapy and the combination of voriconazole plus caspofungin. That is, in our study, the clinical efficacy of these three regimens for IPA was essentially the same. This finding is consistent with the results of a study published by Yang et al. in 2021, which included 35 critically ill patients with IPA. They reported that, compared with voriconazole monotherapy, the initial choice of the combination of voriconazole plus caspofungin did not improve the clinical treatment effect in patients (Yang et al., 2021). A systematic review involving 1,071 patients revealed that for the treatment of primary IPA, the cumulative evidence regarding the use of combination antifungal therapy is contradictory. Among them, two studies demonstrated that the outcome of combination antifungal therapy was better than that of monotherapy, one study showed a trend toward a better outcome, and the remaining two studies indicated that combination antifungal therapy had no additional advantage over monotherapy or that the response to monotherapy was better (Garbati et al., 2012). Another meta-analysis including 16 studies and 1,833 patients revealed that the combination of echinocandins with triazoles or amphotericin B, compared with nonechinocandin monotherapy, improved the clinical outcomes of salvage treatment (Panackal et al., 2014). The results of a study published by Yang et al. in 2023, which included 60 patients with neutropenia complicated by IFD among patients with malignant hematological diseases, showed that the combination of caspofungin with voriconazole or amphotericin B was acceptable in terms of effectiveness and safety (Yang et al., 2013). The results of a meta-analysis published in 2015 on the safety and effectiveness of caspofungin for the treatment of IFD revealed that, for confirmed IPA, the therapeutic effect of caspofungin monotherapy was comparable to that of voriconazole monotherapy (Li, 2015), which is consistent with the results of this study. In conclusion, multiple studies have reported contradictory findings regarding the choice of treatment regimens between monotherapy and combination therapy. This is considered related to differences among patient populations, the lack of specific clinical characteristics, and differences in underlying diseases. However, for the initial treatment of IPA, a monotherapy regimen of either voriconazole or caspofungin is still recommended. Once the initial treatment fails, a combination therapy regimen of voriconazole combined with caspofungin can be considered.
An analysis of ADRs associated with various antifungal drugs revealed that the ADRs associated with voriconazole mainly manifest as visual abnormalities, rashes, abnormalities in liver and kidney functions, and pancytopenia (Tang and Liu, 2020). In addition, the prolongation of the QT interval (QTc) inherent in the triazole family in general and drug–drug interactions may also be clinical issues that require attention (Maertens et al., 2021). The ADRs associated with caspofungin mainly involve the systemic system, including elevated transaminase levels, chills, nausea, vomiting, fever, rashes, and pancytopenia (Liu et al., 2018). The results of our study revealed that monotherapy, including voriconazole monotherapy or caspofungin monotherapy, was comparable to the combination therapy with voriconazole and caspofungin in terms of the incidence of total ADRs, liver and kidney function impairment, visual abnormalities, and electrolyte metabolism abnormalities. However, the combination therapy significantly increased the incidence of pancytopenia. Therefore, clinicians and pharmacists should strengthen the monitoring of the routine blood test results of critically ill patients with IPA who are receiving the combination therapy.
In terms of all-cause mortality, the combination therapy group had a significantly higher mortality rate than did the monotherapy groups. However, this result should not be interpreted as indicating that combination therapy is a predictor of all-cause mortality. Rather, it is likely related to the severity of the underlying disease and the progression of the condition, as patients who received combination therapy generally presented with more severe symptoms, as indicated by their higher APACHE II scores. This suggests that the initial choice of combination therapy typically reflects more severe disease, thus leading to a higher mortality rate. Nonetheless, this study also confirmed that the initial combination therapy did not improve patient prognosis or reduce all-cause mortality, which was consistent with the results of the RCT conducted by Kieren et al (Marr et al., 2015). They included 454 patients with suspected or confirmed IA infection and compared the efficacy of the combination of echinocandins plus voriconazole with that of voriconazole monotherapy. The results showed that in terms of reducing the 6-week mortality rate of patients, the effectiveness was limited, and no statistically significant results were achieved; thus, a clear conclusion of superiority could not be drawn.
This study has certain limitations. First, as this was a retrospective study, there were differences in data homogeneity, and some data were missing, which could have introduced bias into the results. Second, the study data were collected from two centers, meaning that the results could be influenced by the level of diagnostic and therapeutic expertise at the two institutions, which may have limited the generalizability of the findings. Additionally, alternative therapies recommended in the guidelines, such as amphotericin B and itraconazole, were infrequently used in this study, and given potential data bias, they were not included in the analysis, making it impossible to clarify their efficacy and safety. Finally, the relatively small number of patients included in this study may have impacted the robustness of the results. We will continue to supplement and analyze these data in the future.
In conclusion, in critically ill patients with IPA in the ICU, both voriconazole monotherapy and caspofungin monotherapy were found to be clinically effective and safe. The combination of voriconazole and caspofungin did not offer additional benefits in terms of clinical efficacy or overall survival. Moreover, combination therapy significantly increased the incidence of pancytopenia and did not improve all-cause mortality or prognosis. Therefore, voriconazole monotherapy remains the first-line treatment for IPA in critically ill patients because of its clinical efficacy and safety profile. Caspofungin monotherapy is a viable alternative with comparable efficacy and safety. The combination of voriconazole and caspofungin is not recommended as an initial treatment regimen for IPA in critically ill patients. Further randomized, controlled, multicenter, large-scale clinical trials are needed to confirm the efficacy and safety of various antifungal regimens in critically ill IPA patients.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Shaanxi Provincial People’s Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because This article is a retrospective study, and according to the relevant regulations of the hospital ethics committee, written informed consent was not obtained.
Author contributions
LC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ZL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. YZ: Conceptualization, Data curation, Methodology, Supervision, Writing – review & editing. DC: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. JM: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing. PZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research received five fundings: the Health Commission of Shaanxi Province, the Xi’an Science and Technology Program Project (24KPZT0022); the Scientific Research Project of Shaanxi Provincial People’s Hospital [2021JY-30 and 2021YX-36]; Shaanxi Provincial Natural Science Foundation Project (2019SF-188 and 2022JM-605).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alexander, B. D., Lamoth, F., Heussel, C. P., Prokop, C. S., Desai, S. R., Morrissey, C. O., et al. (2021). Guidance on imaging for invasive pulmonary aspergillosis and mucormycosis: from the imaging working group for the revision and update of the consensus definitions of fungal disease from the EORTC/MSGERC. Clin. Infect. Dis. 72, S79–s88. doi: 10.1093/cid/ciaa1855
Cadena, J., Thompson, G. R., 3rd, and Patterson, T. F. (2016). Invasive aspergillosis: current strategies for diagnosis and management. Infect. Dis. Clin. North. Am. 30, 125–142. doi: 10.1016/j.idc.2015.10.015
Cao, L., Ji, Z., Zhang, P., and Wang, J. (2023)Epidemiology and mortality predictors for severe childhood community-acquired pneumonia in ICUs: A retrospective observational study. Front. Pediatr. 11. doi: 10.3389/fped.2023.1031423
Cao, L., Li, Z., Zhang, P., and Yong, S. (2022). Relationship between vancomycin trough serum concentrations and clinical outcomes in children: a systematic review and meta-analysis. Antimicrob. Agents Chemother. 66, e0013822. doi: 10.1128/aac.00138-22
Chen, M., Xu, Y., and Hong, N. (2018). Epidemiology of fungal infections in China. Front. Med. 12, 58–75. doi: 10.1007/s11684-017-0601-0
Chinese Society of Critical Care Medicine (2007). Guidelines for the diagnosis and treatment of invasive fungal infections in critically ill patients. Chin. J. Intern. Med. 46, 960–9666. doi: 10.3760/j.issn:0578-1426.2007.11.031
Donnelly, J. P., Chen, S. C., Kauffman, C. A., Steinbach, W. J., Baddley, J. W., Verweij, P. E., et al. (2020). Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin. Infect. Dis. 71, 1367–1376. doi: 10.1093/cid/ciz1008
Garbati, M. A., Alasmari, F. A., Al-Tannir, M. A., and Tleyjeh, I. M. (2012). The role of combination antifungal therapy in the treatment of invasive aspergillosis: a systematic review. Int. J. Infect. Dis. 16, e76–e81. doi: 10.1016/j.ijid.2011.10.004
Guo, L., Wu, X., and Wu, X. (2023). Aspergillus infection in chronic obstructive pulmonary diseases. Clin. Respir. J. 17, 129–138. doi: 10.1111/crj.13585
Han, H. H. (2020). Research progress of voriconazole combined with amphotericin B in the treatment of invasive pulmonary aspergillosis. Cent. Sou. Pharm. 18, 1206–1209. doi: 10.7539/j.issn.1672-2981.2020.07.026
He, H. Y., Chang, S., and Ding, L. (2012). Significance of Aspergillus spp. isolation from lower respiratory tract samples for the diagnosis and prognosis of invasive pulmonary aspergillosis in chronic obstructive pulmonary disease. Chin. Med. J. 125, 2973–2978.
Herbrecht, R., Denning, D. W., Patterson, T. F., Bennett, J. E., Greene, R. E., Oestmann, J. W., et al. (2002). Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N. Engl. J. Med. 347, 408–415. doi: 10.1056/NEJMoa020191
Herrera, S., Magyar, U., and Husain, S. (2025). Invasive aspergillosis in the current era. Infect. Dis. Clin. North. Am. e33–e60. doi: 10.1016/j.idc.2025.01.002
Hou, T. and Xu, Y. P. (2017). Clinical efficacy and safety of caspofungin in the treatment of invasive fungal infections in patients with leukemia undergoing chemotherapy. J. Clin. Drug Ther. 15, 71–74. doi: 10.3969/j.issn.1672-3384.2017.02.016
Khan, S., Bilal, H., Shafiq, M., Zhang, D., Awais, M., and Chen, C. (2024). Distribution of Aspergillus species and risk factors for aspergillosis in mainland China: a systematic review. Ther. Adv. Infect. Dis. 11, 20499361241252537. doi: 10.1177/20499361241252537
Lei, Y. Y., Huang, G. Q., and Yan, H. G. (2020). Microbiological examination and clinical diagnosis and treatment of patients with pulmonary aspergillus infection. Mod. Med. Hea. R. 4, 98–99.
Lestrade, P. P. A., Meis, J. F., and Melchers, W. J. G. (2019). Triazole resistance in Aspergillus fumigatus: recent insights and challenges for patient management. Clin. Microbiol. Infect. 25, 799–806. doi: 10.1016/j.cmi.2018.11.027
Li, C. C. (2015). Meta-analysis of the efficacy and safety of caspofungin in the treatment of invasive fungal infections (China: Shandong University).
Li, B. F., Li, G. F., and Lin, H. M. (2021). Clinical efficacy and safety of voriconazole in the treatment of pulmonary invasive fungal infections. J. CRDU. 14, 32–34. doi: 10.15887/j.cnki.13-1389/r.2021.06.011
Li, S., Li, Z., Wang, P., Zhan, Y., Xie, J., and Ye, F. (2024). Efficacy and safety of caspofungin for the treatment of invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. J. Int. Med. Res. 52, 3000605241237878. doi: 10.1177/03000605241237878
Limper, A. H., Knox, K. S., Sarosi, G. A., Ampel, N. M., and Stevens, D. A. (2011). Treatment of fungal infections in adult pulmonary and critical care patients. Rus. Pulmon. 3, 9–52. doi: 10.18093/0869-0189-2011-0-3-9-52
Liu, S. H., Hu, X. M., and Yang, J. (2017). Characteristics and drug resistance analysis of invasive fungal flora in emergency intensive care unit from 2013 to 2017. J. Clin. Emerg 18, 617–621. doi: 10.13201/j.issn.1009-5918.2017.08.015
Liu, X. D., Xiong, M. Y., Zhu, X., Kan, L. Y., and Zhao, L. M. (2018). Analysis of adverse drug reactions of caspofungin. Chin. J. Clin. Pharma. 34, 1574–1576. doi: 10.13699/j.cnki.1001-6821.2018.13.025
Ma, X., Wang, K., and Zhao, X. (2019). Prospective study of the serum Aspergillus-specific IgG, IgA and IgM assays for chronic pulmonary aspergillosis diagnosis. BMC. Infect. Dis. 19, 694. doi: 10.1186/s12879-019-4303-x
Maertens, J. A., Rahav, G., Lee, D. G., Ponce-de-León, A., Ramírez Sánchez, I. C., Klimko, N., et al. (2021). Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: a phase 3, randomised, controlled, non-inferiority trial. Lancet 397, 499–509. doi: 10.1016/s0140-6736(21)00219-1
Marr, K. A., Schlamm, H. T., Herbrecht, R., Rottinghaus, S. T., Bow, E. J., Cornely, O. A., et al. (2015). Combination antifungal therapy for invasive aspergillosis: a randomized trial. Ann. Intern. Med. 162, 81–89. doi: 10.7326/m13-2508
Panackal, A. A., Parisini, E., and Proschan, M. (2014). Salvage combination antifungal therapy for acute invasive aspergillosis may improve outcomes: a systematic review and meta-analysis. Int. J. Infect. Dis. 28, 80–94. doi: 10.1016/j.ijid.2014.07.007
Patterson, T. F., Thompson, G. R., Denning, D. W., Fishman, J. A., Hadley, S., Herbrecht, R., et al. (2016). Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases society of america. Clin. Infect. Dis. 63, e1–e60. doi: 10.1093/cid/ciw326
Pfaller, M. A., Carvalhaes, C. G., and Rhomberg, P. (2022). Correction: Antifungal susceptibilities of opportunistic filamentous fungal pathogens from the Asia and Western Pacific Region: data from the SENTRY Antifungal Surveillance Program (2011–2019). J. Antibiot. 75, 123. doi: 10.1038/s41429-021-00460-z
Quindós, G. (2014). Epidemiology of candidaemia and invasive candidiasis. A changing face. Rev. Iberoam. Micol. 31, 42–48. doi: 10.1016/j.riam.2013.10.001
Romero, M., Messina, F., and Marin, E. (2019). Antifungal resistance in clinical isolates of Aspergillus spp.: when local epidemiology breaks the norm. J. Fungi. 5, 41. doi: 10.3390/jof5020041
Shen, C., Qiao, G., and Wang, C. (2022). Outcomes of surgery for different types of chronic pulmonary aspergillosis: results from a single-center, retrospective cohort study. BMC. Pulm. Med. 22, 40. doi: 10.1186/s12890-022-01836-z
Su, H. L., Chen, Z. Q., and Zhu, J. H. (2019). Retrospective analysis of the data of 1935 clinical isolates of deep Aspergillus. Chin. J. Myco 14, 217–221.
Tang, J. and Liu, Y. (2020). Literature analysis of antifungal adverse drug reactions. For. Med. J. (Antibiot. Sect.). 41, 320–324. doi: 10.13461/j.cnki.wna.005329
Tian, Y. J., Liu, Q. G., and Zhang, Y. (2020). Diagnosis and treatment of a patient with invasive pulmonary aspergillosis. Int. J. Respir. Med. 40, 1648–1653.
Tissot, F., Agrawal, S., Pagano, L., Petrikkos, G., Groll, A. H., Skiada, A., et al. (2017). ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell transplant patients. Haematologica 102, 433–444. doi: 10.3324/haematol.2016.152900
Tunnicliffe, G., Schomberg, L., Walsh, S., Tinwell, B., Harrison, T., and Chua, F. (2013). Airway and parenchymal manifestations of pulmonary aspergillosis. Respir. Med. 107, 1113–1123. doi: 10.1016/j.rmed.2013.03.016
Ullmann, A. J., Aguado, J. M., Arikan-Akdagli, S., Denning, D. W., Groll, A. H., Lagrou, K., et al. (2018). Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 24 Suppl 1, e1–e38. doi: 10.1016/j.cmi.2018.01.002
Walsh, T. J., Anaissie, E. J., Denning, D. W., Herbrecht, R., Kontoyiannis, D. P., Marr, K. A., et al. (2008). Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin. Infect. Dis. 46, 327–360. doi: 10.1086/525258
Wang, C. X. (2022). Risk factors and survival analysis of severe invasive pulmonary aspergillosis (China: Xinjiang Medical University).
Wang, J., Han, Y., and Feng, J. (2019). Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis. BMC. Pulm. Med. 19, 252. doi: 10.1186/s12890-019-1022-4
Wang, J. P. and Xu, M. C. (2019). Case analysis of voriconazole combined with caspofungin in the treatment of invasive pulmonary aspergillosis. Chin. Pres. Drugs 17, 65–66.
Wang, Z. P., Zhu, J. N., and Chen, L. (2021). Pharmaceutical care of a child with pulmonary Nocardia infectious abscess treated clinically. J. CRDU. 14, 42–45. doi: 10.15887/j.cnki.13-1389/r.2021.05.015
Yang, L. J., Gao, L. Y., and Fu, Z. W. (2021). Preliminary clinical experience of antifungal drug combination therapy for invasive pulmonary aspergillosis in critically ill ICU patients. Chin. J. Infect. Cont 20, 532–536. doi: 10.12138/j.issn.1671-9638.20216690
Yang, A. Y., Ma, L., and Chi, X. M. (2013). Exploration of the efficacy and safety of caspofungin combined with other antifungal drugs in the treatment of neutropenia complicated with invasive fungal infection in patients with Malignant hematological diseases. Chin. J. Modern. Drug App. 17, 125–127. doi: 10.14164/j.cnki.cn11-5581/r.2023.09.035
Yii, A. C., Koh, M. S., Lapperre, T. S., Tan, G. L., and Chotirmall, S. H. (2017). The emergence of Aspergillus species in chronic respiratory disease. Front. Biosci (Schol Ed). 9, 127–138. doi: 10.2741/s477
Yu, L. C., Mao, Y. M., and Chen, C. W. (2017). Guidelines for the diagnosis and treatment of drug-induced liver injury. Prac. J. Liver. Dis. 220, 257–274. doi: 10.1007/s12072-017-9793-2
Yuan, C., Zhu, R., Hu, L., and Li, J. (2025). Predictors for invasive pulmonary aspergillosis in acute-on-chronic liver failure patients: A retrospective study. Infect. Drug Resist. 18, 909–918. doi: 10.2147/idr.S497840
Zhang, C. H., Hu, M. D., Jiang, M., and Wu, Q. (2023). A comparative study on the identification results of aspergillus by three methods. Int. J. Lab. Med. 44, 2938–2941. doi: 10.3969/ji.ssn.1673-4130.2023.23.024
Zhang, H. X. and Ma, A. J. (2019). Clinical study of voriconazole in the treatment of 58 cases of chronic obstructive pulmonary disease with invasive pulmonary aspergillus. Shanxi. Med. J. 48, 2008–2010. doi: 10.3969/j.issn.0253-9926.2019.16.025
Keywords: invasive pulmonary aspergillosis, safety, efficacy, voriconazole, caspofungin
Citation: Li Z, Zong Y, Chen D, Ma J, Zhang P and Cao L (2025) Efficacy and safety of voriconazole and caspofungin for the treatment of invasive pulmonary aspergillosis in critically ill patients in China. Front. Cell. Infect. Microbiol. 15:1584950. doi: 10.3389/fcimb.2025.1584950
Received: 28 February 2025; Accepted: 28 April 2025;
Published: 21 May 2025.
Edited by:
María Del Rocío Alicia Reyes-Montes, National Autonomous University of Mexico, MexicoReviewed by:
María Guadalupe Frías De León, Hospital Regional de Alta Especialidad de Ixtapaluca, MexicoEsperanza Duarte-Escalante, National Autonomous University of Mexico, Mexico
Copyright © 2025 Li, Zong, Chen, Ma, Zhang and Cao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lu Cao, Y2FvbHVfY3B1QDE2My5jb20=