 Cornelia Schneider
Cornelia Schneider Philipp Rameder1
Philipp Rameder1- 1Institute of Computer Science, University of Applied Sciences Wiener Neustadt, Wiener Neustadt, Austria
- 2Institute of Medical Informatics, UMIT TIROL – Private University for Health Sciences and Health Technology, Hall in Tirol, Austria
- 3Research Institute for Economics of Aging, WU Vienna University of Economics and Business, Vienna, Austria
The rising demand for home care services in Europe, driven by an aging population, presents challenges such as staffing shortages and resource limitations. One way to address these challenges is to increase the use of innovative digital solutions. For this reason, the ‘Care about Care’ project developed the digital Remote Care Assist (RCA) system to enable remote on-site support for professional home care, with a Care Expert Center web application for providing and a mixed-reality Remote Support application for Microsoft HoloLens 2 for receiving support. The solution was tested in two test centers located in Austria and Luxembourg. This paper aims to explore both the general perception and the actual interaction with the RCA system by nursing and care staff and experts in the two test centers. It also aims to identify barriers and potential use cases for successful implementation. We applied a mixed-methods approach by combining usage data measurement and focus group interviews. The results highlight the potential of RCA to improve remote consultations, with key benefits in wound care/medical issues, hands-free interaction and smooth service handovers to colleagues. Barriers were related to the device weight, handling and issues when using the device in areas with poor internet connectivity. The lack of availability of experienced staff to work in the Expert Center has affected usage. Improved device design, centralized expertise and enhanced connectivity are essential for successful integration of RCA into home care.
1 Introduction
The population in Europe is ageing and will develop an increasing need for care services (European Commission, Directorate-General for Employment, and Social Affairs and Inclusion, 2021). The situation will be exacerbated in the coming years by the ageing of the baby boomers (Directorate-General for Economic and Financial Affairs, 2021). In addition to increased demand for institutional care (Famira-Mühlberger, 2024), home care in particular is expected to increase for two reasons, namely the preference of older people to stay at home as long as possible (Wagnild, 2001; Wiles et al., 2012) and the political priority in many European countries, which favors home care over inpatient care (Spasova et al., 2018). However, home care is already reaching its limits as it is struggling with increasingly complex and resource-intensive health and care needs and a drastic shortage of (experienced) long-term care staff, making it difficult to adequately meet the needs of their service users (Organisation for Economic Co-operation and Development, 2020). In addition, unlike residential care, where nursing and care staff can more easily receive support from their teammates, nursing/care staff in home care settings are generally on their own and have little opportunity to discuss with their colleagues (Bauer et al., 2018; Briar et al., 2014). Especially when it comes to caring for people with multiple illnesses, this can be challenging and stressful. Moreover, specialists (e.g., wound managers, therapists) cannot always be on site when nursing and care staff need their expertise. The demand for such advice is increasing, and it is difficult to provide this support in remote areas. Staff shortages in home care affect quality and job satisfaction and reduce the length of time spent in the profession, further reducing human resources (Krajic et al., 2005). Each time an experienced care worker leaves, valuable know-how is lost.
Professional home care is a relatively “low-tech” (Bandini et al., 2023) field of long-term care. On-site support from colleagues and communication with relatives is generally only possible by telephone. The disadvantages of information exchange by telephone are manifold – different people will explain situations on-site in different ways. Some situations are explained worse than they actually are, others are played down in significance. Particularly in a healthcare context, the use of images and sound through video telephony or video conferencing enables more accurate assessments of situations that require visual evaluation (Rush et al., 2018). Video telephony can offer benefits, but only if information is exchanged confidentially. However, some widely used messaging apps, such as WhatsApp, do not comply with European GDPR regulations (Masoni and Guelfi, 2020) and are not tailored to long-term care settings, e.g., they do not offer the possibility to save consultations into care documentation. Additionally, smartphone apps have limitations in scenarios where nursing/care staff need both hands free (Klinker et al., 2019) for tasks like wound care. Marking specific elements, such as a rash on the skin, with arrows, circles, or rectangles during a video call can improve clarity and communication (Schneider et al., 2023). In conclusion, an improved video conferencing solution that enables expert consultation while allowing hands-free operation, marking and saving consultations directly into care documentation would be a significant advancement for professional home care.
Augmented reality (AR) and mixed reality (MR) applications could offer valuable support for communication in long-term care settings. Often, an AR app on the company smartphone can be sufficient, but when nursing and care staff need both hands free to follow instructions, AR/MR glasses, such as Vuzix Blade 2 or Microsoft HoloLens 2 provide a clear advantage (FFG Projektdatenbank, 2020; Klinker et al., 2019). Unlike their use in medical settings (Eckert et al., 2019) and inpatient acute care (Romare and Skär, 2020), these technologies have seen limited adoption in home care. However, the COVID-19 pandemic has accelerated the shift toward virtual care (Babaei et al., 2023). Research into usability, AR workflows, wound management, and outpatient intensive care (Janßen and Prilla, 2019a, 2019b; Klinker et al., 2019; Prilla et al., 2019) emphasizes the continuing need for applied research, particularly in home care.
One of the main objectives of the European project Care about Care (C^C) (AAL Programme, 2021; Care about Care, 2021) was to develop and test a Remote Care Assist (RCA) solution for the home care sector. For the final test, dedicated Remote Care Assist (RCA) HoloLens test centers were established with each of the care organizations in Austria and Luxembourg to evaluate the RCA components (i) Care Expert Center web application and (ii) HoloLens Remote Support app.
This paper seeks to explore both the general perception and actual interaction with the RCA system by nursing/care staff and experts in two HoloLens test centers in Austria and Luxembourg. It also aims to identify barriers and potential use cases for successful implementation, with the aim of informing future developments and implementations and proactively addressing challenges.
The remainder of the paper is organized as follows: Section 2 introduces the RCA system used in the test, Section 3 outlines the test design and details the various aspects examined, including recruitment and data collection methods. Section 4 presents the results, followed by a discussion of these findings in Section 5.
2 Remote Care Assist system using AR/MR technologies
The Remote Care Assist (RCA) service consisted of the RCA backend, handling administrative functions, and two components for the RCA frontend. (i) The Care Expert Center (CXC), a web application for remote care guidance (Figure 1). In addition to video telephony, the CXC provided features, such as file and screen sharing, taking and sending screenshots, marking specific areas or points on-site, and – a feature most specific for professional care – saving consultations directly into care documentation. (ii) The Remote Support HoloLens (RS-HL), an app for the Microsoft (MS) HoloLens 2 that enables nursing and care staff to receive remote visual and audio on-site support (Figure 2). The RS-HL also included a ‘Learning Experience’ module (Figure 3). On the RS-HL app, developed specifically for professional home care, users could also access virtual rulers, take and send photos and receive virtual markers. Interaction helpers included toggling hand rays on/off and support for working with virtual windows. Since interacting with the HoloLens was unfamiliar to all test participants, a Learning Experience module was developed to introduce them to MR and the concept of virtual interfaces, such as near- and far-interaction, hand menus, and hand rays. The Learning Experience was mandatory for all users during their first login and could be revisited later to refresh their knowledge. For an overview of the RCA feature set, refer to Schneider et al. (2023).
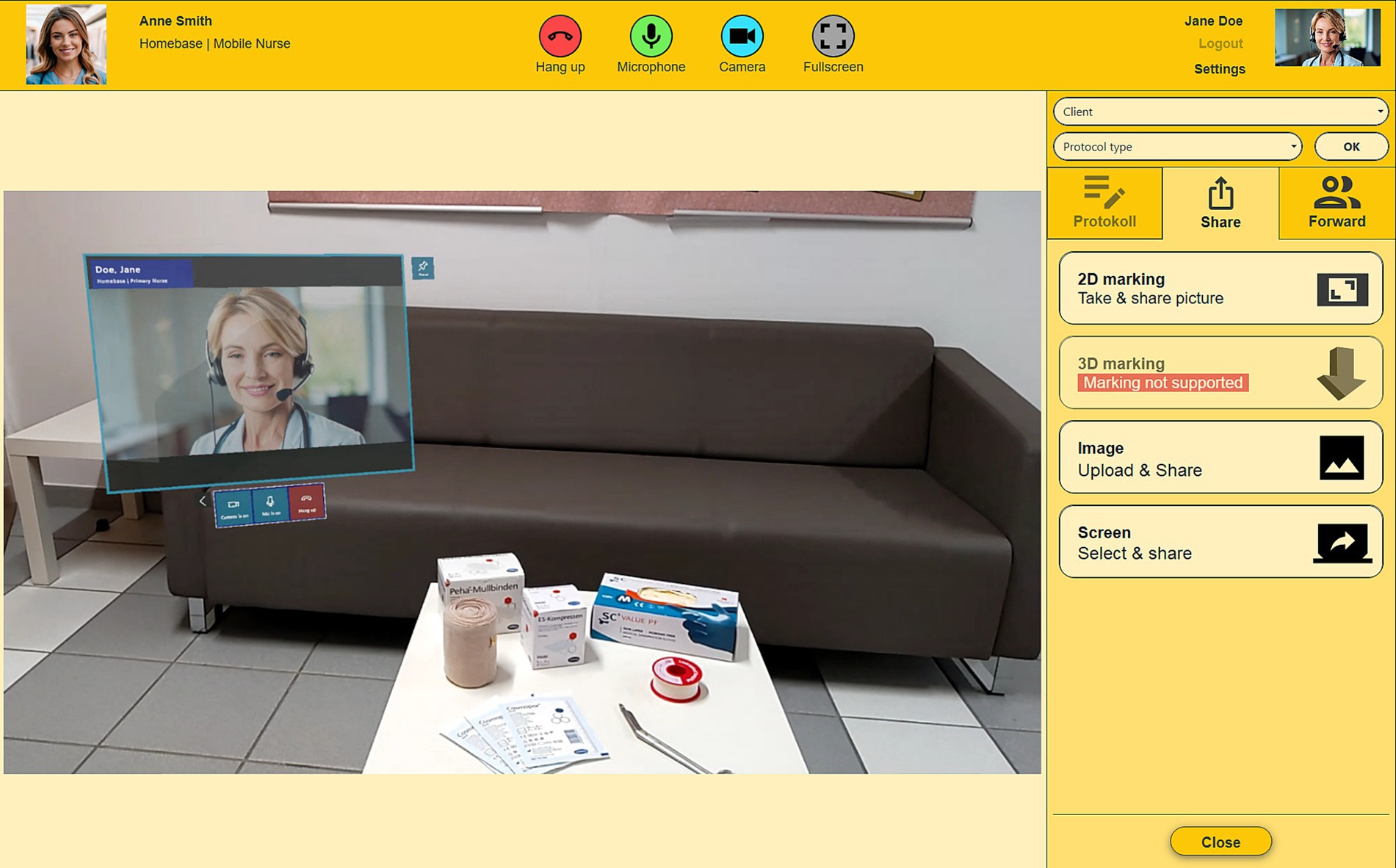
Figure 1. Care Expert Center (CXC) web application with tools for sharing (person(s) generated with Adobe Firefly). Source: FHWN (University of Applied Sciences Wiener Neustadt).

Figure 2. Remote Support HoloLens (RS-HL) including additional image displayed (person(s) generated with Adobe Firefly). Source: FHWN.
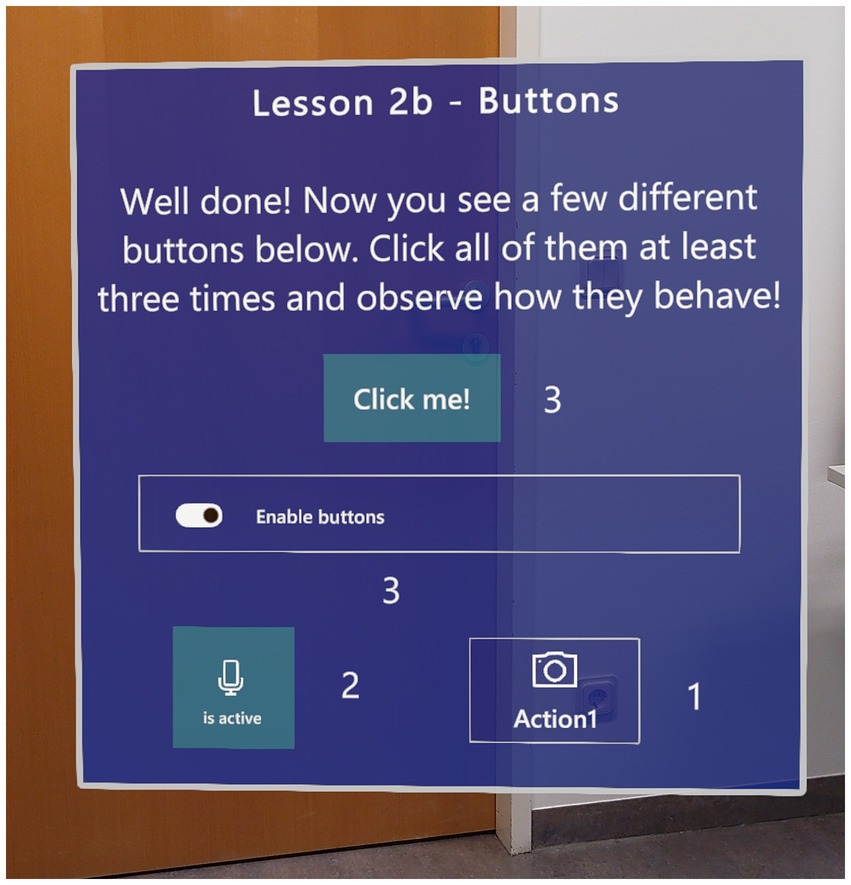
Figure 3. Lesson 2b of the “Learning Experience” as part of RS-HL. Source: FHWN.
The MS HoloLens 2 was configured in ‘kiosk mode’, meaning the RS-HL app launched automatically upon starting, with no access to other apps. To ensure internet connectivity, a mobile wireless router with a SIM card (TP-Link M7200 and Alcatel MW40V-2AALDE1) was provided, along with a power bank (HUAWEI 55030727, 12,000 mAh) to extend the device’s runtime.
3 Methods
3.1 RCA HoloLens test centers
Since high-quality MR headsets were still relatively expensive (the MS HoloLens 2 costed around 3,850 Euros at the time of testing), it was expected to be unlikely that a care organization will be able to provide every member of staff with their own headset for everyday use in the near future. Therefore, one service unit responsible for a specific region in Austria and one in Luxembourg were selected to test the MR headsets. The criteria for selecting the test centers in both countries were: (i) commitment to testing the RCA system, (ii) person power to carry out the test, (iii) not having been involved in previous user testing of the project, (iii) good internet connection in the region (Trukeschitz et al., 2022a), and in Austria (iv) driving distance for the technical support team within 100 km. The care organization’s service unit for the test center in Austria was chosen in collaboration with the technical, end-user and the evaluation partner, while in Luxembourg, the selection was solely made by the end-user partner. A test was initially also planned in Belgium, but it could not be conducted as intended.
The headsets were shared among the nursing and care staff (four devices in Austria and three devices in Luxembourg), while nursing experts of each test center used their computers in the service units to access the CXC web application. The end-user partner’s utilization concept included having care experts available at the RCA HoloLens test center to answer questions from nursing and care staff. These experts included senior or deputy care managers from each region; in addition, wound care managers could be consulted at specific times if available at the centers. Any changes in availability were to be communicated to the team via the chat function of the care management system.
3.2 The support process using the Remote Care Assist system
The remote support process was divided into four steps: (i) the home care service user is visited by nursing and care staff, (ii a) if no issues arise, the visit proceeds as planned, (ii b) if an issue arises during the visit that needs clarification or guidance from an experienced care expert, then (iii) the nursing/care staff contacts the CXC, and (iv) the nursing/care staff exchanges information with the expert to collaboratively find a solution.
3.3 Software roll-out, training and test start
The RS-HL app software was provided by the technical project partner and was installed by the IT departments of the care organizations (henceforth also end-user partners) on the MS HoloLenses. No installation was required for the CXC web application. However, it was argued to be crucial that the web application should run on the main computer in the care service unit that was used by the care expert/wound manager and not on a separate laptop that could not be monitored for incoming calls.
The technical project partner conducted training sessions in Austria, tested the materials with the care organization’s test participants, and trained a trainer from the end-user partner’s care quality department in Luxembourg (Trukeschitz et al., 2022a). This approach followed a train-the-trainer concept (Berggren et al., 2023) to ensure local readiness and continuity.
The initial HoloLens training for the test centers was conducted in three steps. In the first step, participants completed the learning experience with a trainer’s guidance. Next, they ran through test scenarios included in the training materials. Finally, they received training on device charging, handling the mobile wireless router and power bank, and proper disinfection procedures.
In Austria and Luxembourg, the first visits to home care service users per nursing/care staff member were planned to be accompanied by trainers (Austria: project members of the technical partner; Luxembourg: a member of the care organization trained on the HoloLens) to give nursing and care staff a sense of security. Ethical approval for the test was obtained in both Austria and Luxembourg (Section 7). Nursing/care staff and home care users visited were informed and signed an informed consent form.
3.4 Usage data measurement
The use of logging to find bugs in software systems is a common practice. Recently, it has been recognized that logging can also aid in understanding user behavior and extracting domain knowledge (Korzeniowski and Goczyla, 2022), as well as providing valuable information for effectiveness analysis (Trukeschitz et al., 2022b). Analyzing logging data can reveal usage patterns and behaviors, with analyses that may be descriptive, predictive, or prescriptive (Jain et al., 2013; Meyer et al., 2017; Rubin et al., 2014; Shneiderman et al., 2017; Turkington et al., 2018; Zhao et al., 2016). Additionally, the automatic recording of objective usage data is less intrusive than collecting subjective data via surveys (Schneider et al., 2020).
In the “Care about Care” project, we employed usage data measurement to gain insights into the actual use of individual features and their sub-features by logging user interactions, such as clicks and gestures. This allows for a precise assessment of feature usage, which is essential in research projects to determine which functions are adopted. It also enables the identification of usability issues, as problems in task execution can be inferred when users are unable to complete a task. These issues can then be addressed either through targeted focus group discussions or direct feature refinement when user input is not necessary.
The use of the Remote Care Assist system was measured following the usage data evaluation framework outlined in Schneider et al. (2020). User interactions with the CXC and the RS-HL application were tracked using the open-source software Matomo (InnoCraft Limited, 2024). This enabled the logging of every interaction with user interface components, such as buttons, input fields, or checkboxes. Care about Care usage measurement was designed to provide data on the frequency of use of the CXC and RS-HL applications and their respective features per user. As proposed by Schneider et al. (2020), logging included: “(i) a unique user identification number (UUID) (who); (ii) type of interaction, such as click, touch, or scroll (what); (iii) UI component that was interacted with (where); and (iv) date and time of the interaction (when)”.
For interactions not captured by Matomo, data was accessed indirectly through the system’s database MariaDB (MariaDB Foundation LLC, 2024), where supplementary information was stored – for example, data resulting from user interactions, the number of user accounts created, or successfully initiated or completed calls via the underlying framework. Grafana (Raintank Inc., 2024), an open-source analytics solution, facilitated data analysis and visualization.
3.5 Focus group interviews
Focus group interviews conducted during testing are an effective way to address specific questions, uncover surprising usage patterns and reveal hidden issues that can be quickly discussed and validated with participants (Shneiderman et al., 2017). For this reason, three focus group interviews were planned per country with: (i) nursing and care staff who had used the RS-HL app on the MS HoloLens, (ii) care experts (senior and deputy care managers and wound care managers) who had used the CXC web application and (iii) nursing/care staff and care experts together to explore issues common to both groups. All nursing staff involved in the trial were informed about the background of the testing, the procedures, and the focus group format. All participants provided informed consent for participation and data collection during the trial phase. The focus groups were conducted at the regional offices of the care providers.
Interview schedules were created for each staff and expert focus group, accompanied by photos of the Remote Care Assist system to support participants in reflecting on their experiences. These focus group schedules comprised questions and prompts to help respondents to recall and talk about their experiences using the RCA system. The topics prepared covered (i) the handling of the devices (power management and coordinating the use of the MS HoloLens for home care visits), (ii) any obstacles experienced when using the devices, (iii) perceived value of using such a system for home care, (iv) nursing staff experiences with home care service users’ responses to the MS HoloLens, and (v) their need for further development of the devices and software. The third focus group (staff and experts) was used to reflect together on the findings of each group.
Since the Remote Care Assist system was developed in Austria, we initiated the focus group series there. This decision allowed us to invite the technical partners to the discussions, enabling them to acquire firsthand insights into the use and perception of the technology by the nurses testing the system. The Austrian evaluation team led the discussions in Austria, ensuring that everyone had the opportunity to express their views while guiding the conversation through the relevant topics. It was important to allow space not only for the pre-planned subjects but also for any issues raised by the participants. The methodological learnings of the Austrian focus group sessions (e.g., order of questions, dynamics during the sessions) where then shared with the team in Luxembourg.
The focus groups were recorded and transcribed. The transcripts were analyzed using topic analysis (Döring and Bortz, 2016; Froschauer and Lueger, 2020; Mason, 2018). NVivo (release 1.6.1) – a qualitative data analysis software – was used for coding the transcripts.
4 Results
4.1 Sample description
In the Austrian RCA HoloLens test center (March 14 – July 4, 2023) 3 experts and 6 members of nursing staff participated (8 women, 1 man), while in Luxembourg (May 23 – October 15, 2023), 4 experts and 7 members of nursing and care staff participated (6 women, 5 men). In both countries, one expert was a wound care manager (see Table 1), and most participants were employees with nursing backgrounds (nurses and nursing assistants); additionally, a family and social care worker participated in Luxembourg.
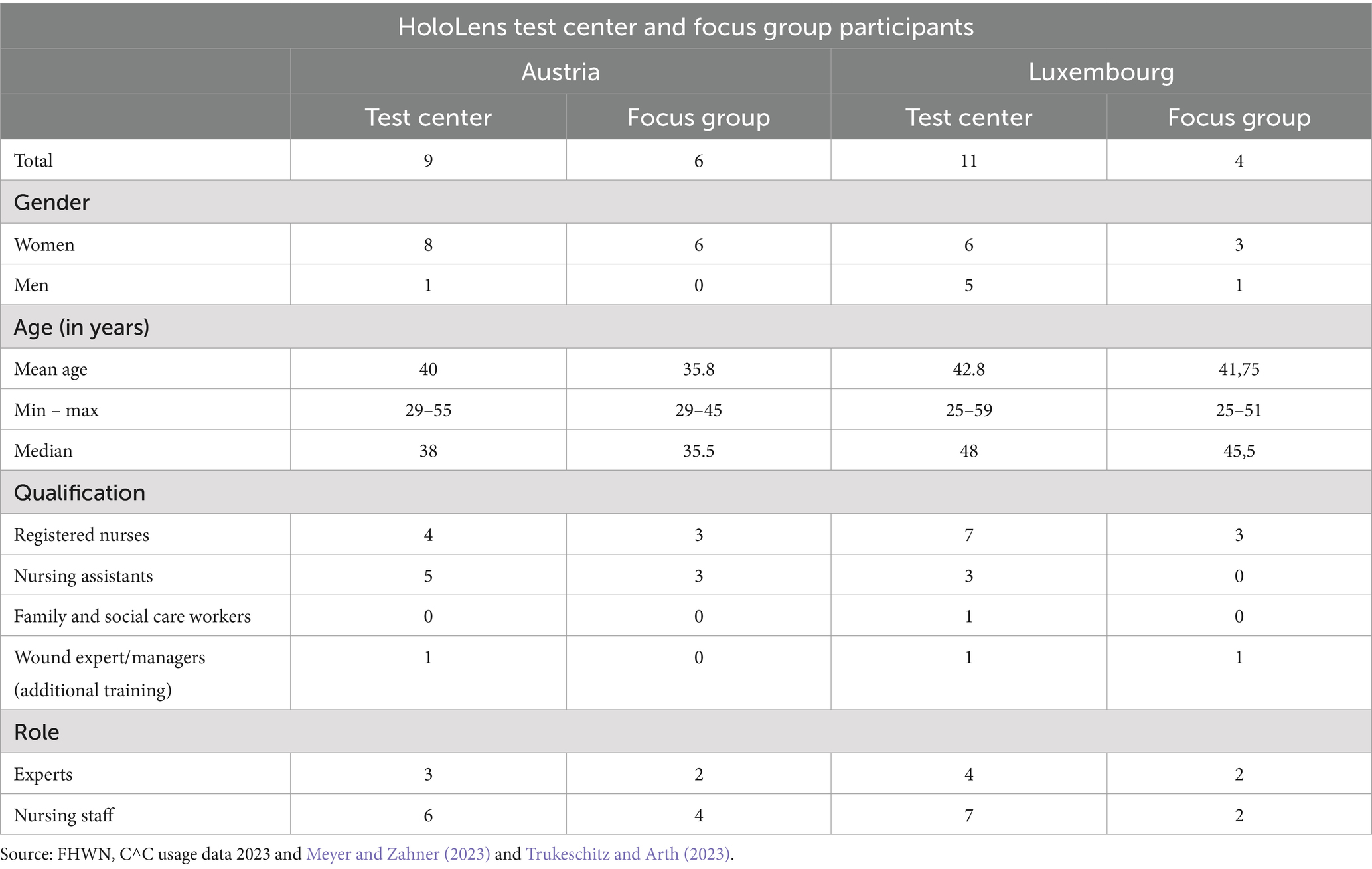
Table 1. HoloLens test center and focus group participants in Austria (n = 9; n = 6) & Luxembourg (n = 11; n = 4).
The focus groups were conducted face-to-face in Austria (Trukeschitz and Arth, 2023) and online in Luxembourg (Meyer and Zahner, 2023), all focus groups per country were held on the same day. In Austria, two experts and four members of nursing staff participated, while in Luxembourg, two experts (including a wound care manager) and two members of nursing and care staff attended (see Table 1).
The nursing and care sector is predominantly female (Kalavrezou et al., 2025), which was reflected in the high number of participating women. Furthermore, the workforce in home care is generally slightly older than average workforce (Kalavrezou et al., 2025), which was particularly evident in the Luxembourg sample (see Table 1). In comparison to Luxembourg, focus group participants in Austria were younger.
4.2 Call statistics overview
Not taking the training into account, during the test period in Austria, the experts used the Care Expert Center (CXC) web application to initiate 24 calls to nursing staff who were equipped with the MS HoloLens at home care service users’ homes. Nursing staff started 95 calls using the Remote Support HoloLens (RS-HL) app (Table 2). In Luxembourg, the experts made only 6 calls from CXC, and nursing and care staff initiated 37 RS-HL calls. In Luxembourg, the planned scenario – nursing and care staff using RS-HL to call the CXC – occurred relatively more frequently than in Austria. In Austria, calls were also frequently initiated from the Care Expert Center (CXC). As Table 3 shows, the number of calls varied over the test period and had its peak in Austria in test month three and in Luxembourg in test month two. The sharp decline in Austria after the third month is explained by the departure of a wound management expert and staff shortages. One very long call of more than one hour explains the high average call time in Luxembourg.
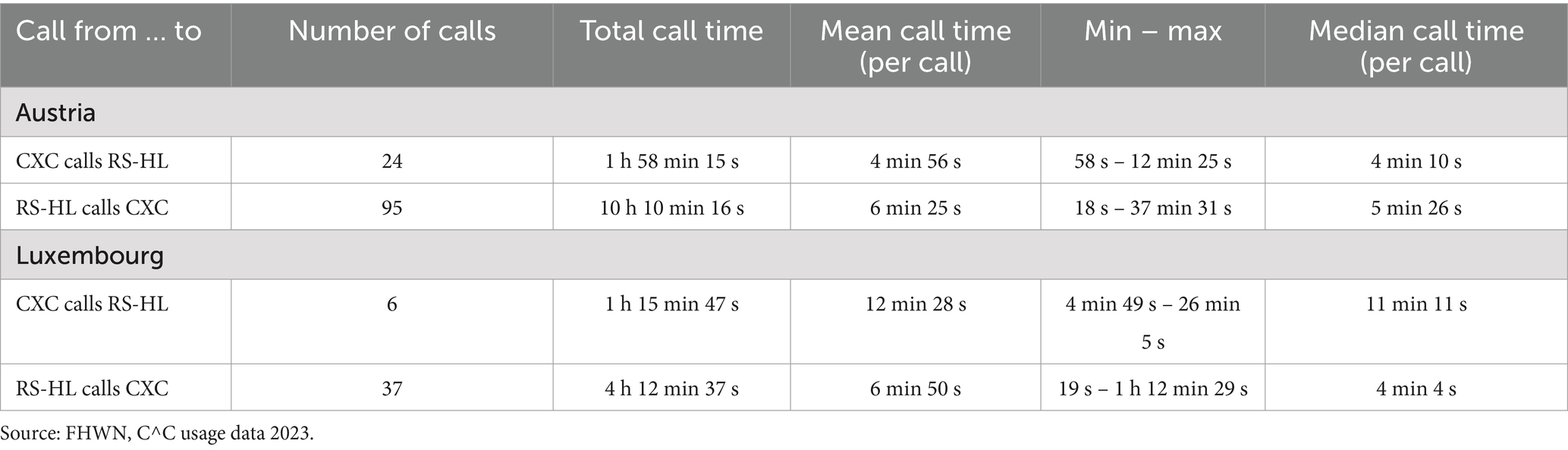
Table 2. RCA calls in Austria and Luxembourg (n = 162).

Table 3. RCA calls per month in Austria and Luxembourg (n = 162).
4.3 Training and learning how to use the RCA
The RCA training in Austria and Luxembourg followed the planned three-step-process and trainers accompanied the first visits of home care service users (Section 3.3). As the HoloLens was in ‘kiosk mode’ only the Remote Support HoloLens (RS-HL) application was available for the testers. At test start, before using the software, both care experts and nursing/care staff had to complete the Learning Experience for the RS-HL. As shown in Table 4, several users engaged with the learning experience more than once to practise using the HoloLens.
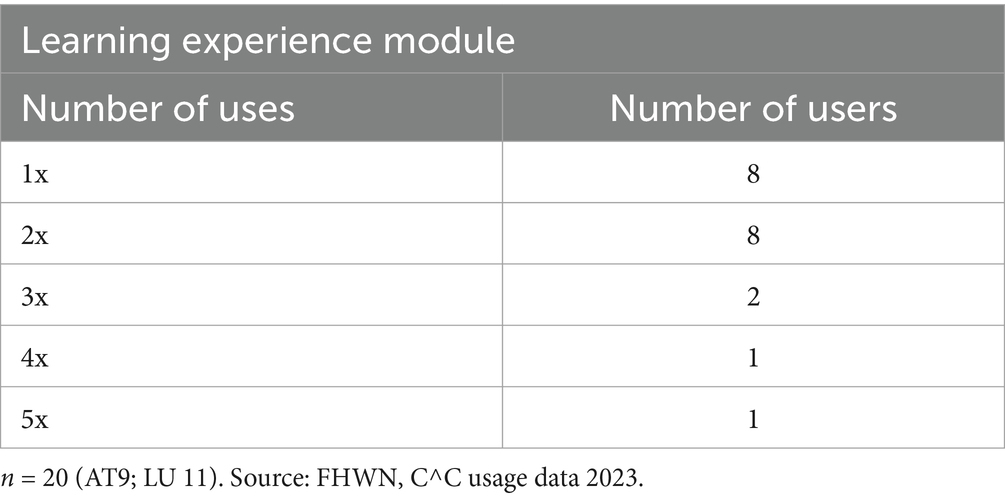
Table 4. Frequency of use of the learning experience by individual user.
In Austria, participants reported that the RCA system and the use of the RS-HL were not that demanding (Trukeschitz and Arth, 2023): “I think the handling, we were quickly there […]. I think the system, would have been […] super. You already know what you have to press. That was super anyway. That was easy, in my opinion.” (B3, L229-232).
Participants in Luxembourg reported that the training was sufficient (Meyer and Zahner, 2023) Care experts in Luxembourg further acknowledged that it was difficult to get used to the CXC as it was “unchartered nursing territory.” The care experts noted that with practice, using the CXC became easier, and they felt more comfortable with it. There were several issues with call stability and quality during the training sessions, which were resolved but disrupted the training. Nursing and care staff concluded that if the system had worked better during the training sessions, they would have felt more confident sooner, but nevertheless it became easier to use over time.
4.4 Care Expert Center – feature use, impression and handling
The following functions were used in the Care Expert Center (CXC): place 2D and 3D markers, send screenshot, share image or screen and keep care records (Figure 1). Any 2D marker required an image to be placed on, which could be either a screenshot from the video stream, a photo selected via the CXC or received from the RS-HL. However, it was also possible to send screenshots without 2D markers. With 2D and 3D markers, it was also possible to move the markers several times to achieve the final position (increasing use). Table 5 shows that in Austria 2D markers were placed/repositioned 42 times and 70 screenshots with and without markers were sent. In Luxembourg, more 2D markers were positioned/repositioned (54) than screenshots were sent (30), suggesting that marked screenshots were commonly used there. In both countries, 3D markers and image/screen sharing were rarely utilized. The ‘keep care records’ feature, though important, could only be tested in Austria and was used 82 times in the Austrian test center, with documentation imported into the primary administration system as images and text. In Luxembourg, the approval of the quality assurance department was missing for the test and was only given at the end of the test.
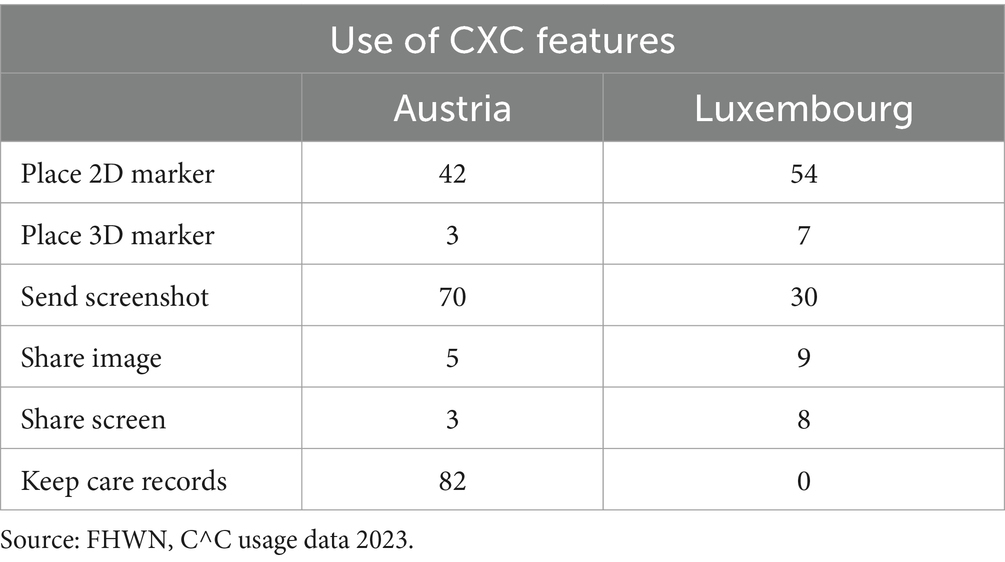
Table 5. Use of CXC features in Austria and Luxembourg.
Nursing and care staff often rely on phone calls for support when visiting home care service users. The RCA system enabled care experts to view and assess care situations remotely, aiding in a better understanding of requests and sometimes replacing the need for in-person visits. Care experts in the focus groups in Austria (Trukeschitz and Arth, 2023) reported that the combination of visual and audio information facilitated a deeper insight, allowing quicker issue recognition and informed decision-making. This visual access proved crucial for accurately assessing critical care needs and determining whether on-site assistance was essential. “But it was […] two home care service users where I can remember well now where we really need to have seen that so we can have assessed it. And if it will be really necessary deployments and calls, it really makes sense.” (X2, L276-278) In Luxembourg, too, the importance of seeing things in the same way as the care worker was rated very highly by care experts (Meyer and Zahner, 2023). In both countries, care experts emphasized the importance of the CXC’s ability to take screenshots out of the video call and to mark specific positions to facilitate communication and reduce the risk of misunderstandings.
4.5 Remote Support HoloLens – feature use, impression and handling
The RS-HL app offered the following functions: show image/screenshot (Figure 2), toggle hand rays, take/send a photo, and different rulers (Figure 4). As with the CXC (Section 4.4), the RS-HL displayed all images and screenshots in the same way, and all types of images could be enhanced with 2D markers – screenshots from the CXC, images sent from the RS-HL, or images selected via CXC. The number displayed by the ‘Show image/screenshot’ function therefore represents all these types together. In Austria, a received image was displayed 68 times, and in Luxembourg 49 times (Table 6). The hand rays were turned off 41 times in Austria and 19 times in Luxembourg and reactivated 26 times in Austria and 14 times in Luxembourg. Through the ‘Send photo’ feature, 77 photos were captured in Austria and 51 in Luxembourg and then transmitted to the CXC for further processing. Four rulers were available: one-hand, two-hand, ray-pointer, and way-pointer. The one-hand and two-hand rulers were the most frequently used in Austria and Luxembourg, while the ray-pointer and way-pointer rulers saw limited use in both countries (Table 6).

Figure 4. Remote Support HoloLens (RS-HL) hand menu with options for hand rays, taking/sending a photo and rulers (person(s) generated with Adobe Firefly). Source: FHWN.
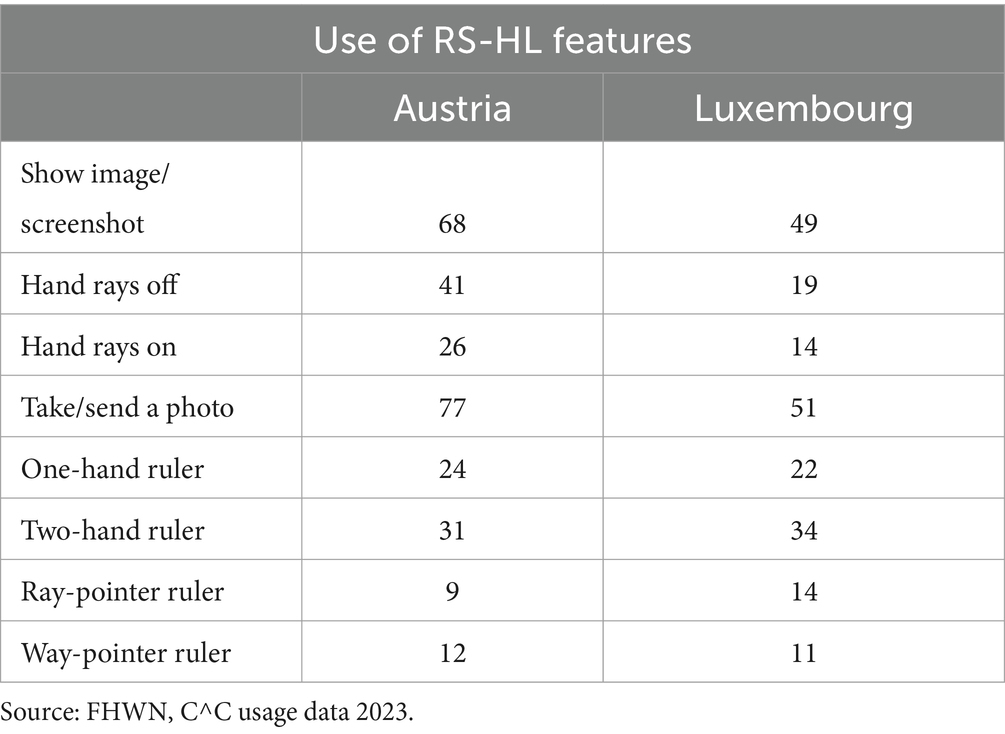
Table 6. Use of RS-HL app features in Austria and Luxembourg.
Nursing staff in the focus groups in Austria (Trukeschitz and Arth, 2023) reported that they could easily identify the markers set by care experts (2D markers). The ability to take photos was also well received. 3D markers were tested in Austria but not utilized, as its practical benefit remained unclear to the users (B3; B2, L683-687). In Austria the rulers were deemed insufficiently accurate, with dimensions often perceived as unreliable, rendering it unhelpful for their tasks. As a result, they preferred to continue using conventional paper rulers. “It just wasn’t always accurate. You were not allowed to move a little bit, because otherwise it was completely inaccurate right away when measuring wounds. Whereas the two-handed works better than the one-handed.” (B4, L570-572) For nursing and care staff in Luxembourg (Meyer and Zahner, 2023), the most valuable feature was the fact that the care expert could see what their staff at the home care service users’ households see; additional features, such as taking photos or measuring wounds, were considered ‘nice-to-have’ but non-essential. Some nursing and care staff noted these features could detract from home care service user-centered attention.
In Austria, the focus group participants mentioned that in warmer months, nursing staff found the temperature under the MS HoloLens uncomfortably high, causing excessive sweating due to the device’s heat output. Additionally, employees wearing optical glasses reported discomfort and the necessity to make adjustments to fit both sets of glasses comfortably on their head. Nursing staff also reported that effective use of the RS-HL in home care settings depends on adequate lighting and stable internet connection. Bright lighting in home care service users’ homes sometimes hindered visibility for remote care experts. Video quality varied, often impacted by poor internet reception in certain regions and within the care facility itself. These connection issues led to blurry images, interrupted support calls, and delays in sending images, requiring frequent troubleshooting like restarting the device. Keeping the mobile wireless router charged was also important. The nursing staff noted that poor connectivity was partly due to regional limitations and inadequate facility internet infrastructure (Trukeschitz and Arth, 2023). Besides internet connection problems, nursing/care staff in Luxembourg agreed that a simpler, more discreet device with fewer features would enhance user-friendliness and be better accepted by home care services users (Meyer and Zahner, 2023).
4.6 Nursing and care staff experiences on the interaction with home care service users
The nursing and care staff in Austria and Luxembourg (Meyer and Zahner, 2023; Trukeschitz and Arth, 2023) reported mixed reactions of home care service users to the RCA system and RS-HL in particular: some home care service users rejected the HoloLens without explanation, while others showed interest. Misunderstandings arose, with home care service users concerned that the HoloLens might record them or be worn by nursing and care staff during personal care tasks. To clarify, nursing/care staff let some home care service users try the HoloLens, which fostered understanding and even enthusiasm in some. While home care service users observed technical issues, they understood these as early-stage challenges, often finding humor in the appearance of nursing/care staff in the HoloLens, which they described as ‘extraterrestrial’. Nursing and care staff sometimes served as intermediaries between care experts and home care service users (the care expert could hear the home care service users via the HoloLens, but the home care service users could not hear the expert due to technical limitations of the HoloLens). On one occasion, this allowed a care expert to personally wish a home care service user a happy birthday with the help of the care worker.
Nursing/care staff in Luxembourg described their experience with the HoloLens as positive and appreciated the opportunity to test it. They valued the ability to contact a care expert directly for a second opinion without lengthy explanations. Other nursing and care staff not using the HoloLens showed interest in their colleagues’ experiences.
Until 30 April 2023, face masks were mandatory in Austria in some areas, including home care, as part of the COVID-19 regulations. As a result, nursing staff had to wear a mask in addition to the HoloLens glasses. This was a challenge for both nursing staff, who had to deal with potential fogging, and home care service users, as the mask obscured the carer’s lower face and the HoloLens covered part of the upper face, limiting the view of facial expressions.
4.7 Suitable and unsuitable use cases
Suitable and unsuitable use cases identified for RCA use in Austria and Luxembourg (Meyer and Zahner, 2023; Trukeschitz and Arth, 2023) during focus groups are described below.
4.7.1 Suitable use cases
Nursing and care staff found the HoloLens most beneficial for remote wound evaluations, reducing unnecessary visits by allowing immediate consultations with wound experts. Key advantages included real-time feedback on wounds or skin conditions and direct photo capture through the RS-HL app, which improved resource allocation and responsiveness. “For wounds, it [the RS-HL] was really golden.” (B3, L898) The RS-HL app was especially valuable in hands-free scenarios. In addition, the RCA system facilitated smoother service handovers to new colleagues or colleagues who had been away for a period of time by providing live video, which improved clarity over static photos. For medication issues, nursing and care staff consulted experts via RS-HL, though they reported that in such cases, phone consultations offered similar benefits – but without image.
4.7.2 Unsuitable use cases
The virtual rules of the RS-HL offered no added value over a conventional tape measure, which was faster and more accurate. Nursing and care staff also found the RS-HL inappropriate for use with home care service users with dementia, who are confused by technology and require clear facial expressions for effective communication – so it was not used there. Additionally, nursing and care staff considered it unnecessary to use RS-HL to display completed documentation forms to care experts, as it added no significant benefit (in the Austrian test region, care documentation was still done on paper). However, there were differences with the experts who saw benefits in seeing parts of the documentation.
4.8 Barriers and how to make it work in this setting
This section summarizes the main barriers identified in the focus groups (Meyer and Zahner, 2023; Trukeschitz and Arth, 2023) and highlights the key factors that are essential for effective implementation of this solution in the given setting.
4.8.1 Main barriers
The focus groups in Austria and Luxembourg identified three main barriers: technical, organizational and practical/psychological.
From a technical point, focus group participants reported three key issues: (i) lighting conditions: Bright lighting in home care service users’ homes sometimes caused visibility issues for remote care experts. (ii) internet connectivity: Connectivity issues, including weak regional and facility-based reception, impacted video quality and led to interruptions and delays. (iii) device reliability: Occasional technical glitches, such as non-responsive HoloLens controls and failures in establishing calls, disrupted workflows.
On the organizational side, there were four main points that were mentioned: (i) limited staffing and expertise: Staff shortages, frequent sick leave, and limited trained personnel constrained effective RCA system use. (ii) coordination of care experts: Difficulty in spontaneous RS-HL use due to pre-scheduling needs and limited availability of care experts for support. (iii) informed consent (IC) requirements: IC requirements limited which home care service users could participate, necessitating additional coordination. (iv) device management: Shared HoloLens devices required organized distribution, increasing planning burdens.
From a practical and psychological perspective, they identified two issues: (i) unfamiliarity and training time: Some staff felt the system required more time to learn and adapt. (ii) stress from testing: The added pressure to integrate RS-HL into daily tasks led to reluctance and occasional resentment towards the technology.
4.8.2 Factors for successful implementation
The focus groups identified three points for successful implementation in home care: (i) device adaptation, (ii) organizational improvements and (iii) user guidance.
Nursing and care staff mentioned that they would like to see the following adaptation to the device – more compact design (smaller and lighter) and to the RS-HL app, e.g., improved measurement tools.
With regard to organizational improvements, they mentioned three points: (i) centralized care expert centers: Deploying experts centrally or combining several regions would ensure consistent access across care units. (ii) advanced scheduling practices: Pre-planning the use of RS-HL applications would streamline usage for two reasons – first, useful cases would be identified and second, the availability of support could be better planned. (iii) targeted qualifications: Expanding care experts’ qualifications, especially in wound and palliative care, was recommended for optimized support.
Concerning user guidance, nursing and care staff indicated that they would like guidance on a realistic scope of application, i.e., specific situations in which the system should be used, to reduce pressure and increase acceptance. For example, it was reported that some members of the nursing and care staff wore their HoloLens glasses throughout a service user’s home visit, while others only took it out to make calls – the latter was preferred by nursing and care staff and should be encouraged for future use.
5 Discussion
This test of the RCA system in Austria and Luxembourg, consisting of a web-based Care Expert Center and the Remote Support app on the MS HoloLens, including a Learning Experience module, shows feature use, suitable and unsuitable use cases, barriers and factors for successful implementation of such a solution in home care settings.
After several months of testing and collecting usage data, the focus groups interviews allowed us to discuss the use of each feature, as well as the test set-up and training with the nursing/care staff and experts. Although the feedback from nursing and care staff and experts in the focus groups indicated a shared enthusiasm for the concept, technical and organizational barriers hampered its acceptance and functionality.
5.1 Remote care assist: system use
Usage data showed that the RCA system was used to interact with each other and to share screenshots with markings. In Austria, the usage data shows that marking was often not used, but ‘only’ images were shared. Focus group interviews did not provide more insights. From the authors‘point of view, there are two possible explanations: (i) the markers were not needed or (ii) people did not take the time or did not have the time to set the markers. The ‘keep care records’ feature could only be tested in Austria but was used there frequently (Table 5). ‘Keep care records’ could not be tested in Luxembourg as a result of organizational planning. The mandatory feature to practice/train with the Learning Experience was used multiple times by most test participants (Table 4). This certainly made learning to use the RS-HL software easier. The one- and two-hand rulers were mainly used for measuring (Table 6) – due to the fluctuating accuracy, this feature could only be used for approximate measurements. The ability to exchange image files or share the screen was used only to a limited extent (Table 5). During the focus groups it was felt that these functions were also less perceived and that the ‘need’ was clearly for ‘participation’ in the situation on-site via video or by marking things on a screenshot/photo for better exchange.
5.2 Technical: device dimensions
Both nursing/care staff and experts in the test recognized the general usefulness of the RCA system, particularly the ability for experts to directly view care scenarios remotely without relying on potentially ambiguous verbal descriptions. However, they noted that the HoloLens device would benefit from being smaller and lighter, aligning with consumer expectations for compact AR/MR devices. Currently, this is generally a problem with AR/MR devices, as a recent study shows (Ericsson, 2024). They report that consumers have strong market interest in lightweight portable AR/MR devices for everyday use.
5.3 Technical: connection issues
A reliable internet connection proved to be a critical factor, with both Luxembourg and Austria reporting difficulties due to regional differences in connection quality. The Austrian test, in particular, was hampered by poor mobile internet reception, which reduced the frequency and quality of video connections and led nursing staff to revert to traditional telephone calls. This aligns with suggestions that AR/MR ecosystem improvements, including enhanced connectivity, are vital for widespread adoption (Ericsson, 2024).
5.4 Organizational: care expert center and staff shortages
Staff shortages compounded the technology’s challenges, particularly in Austria, where the limited availability of care experts, scheduling constraints and exchanging the devices with each other prevented optimal use of the RCA system over time (Table 3). The staffing for the Care Expert Center in the respective region was challenging to maintain under these conditions. A need for centralized centers of expertise with reliable availability of experts was identified in both regions, only the integration of the care quality department in Luxembourg was able to fulfil this role temporarily. The test highlighted that robust organizational support, including a consistent staffing model and structured scheduling, is crucial for integrating such technology into daily workflows.
5.5 Organizational: feasibility and scalability
Both nursing/care staff and experts recognized the potential of the RCA system to reduce travel time and streamline communication, enabling remote consultation, particularly for specialists such as wound care managers. However, they also raised concerns about the cost of scaling up, particularly given the cost of the MS HoloLens devices. They suggested exploring alternative devices that could also allow hands-free interaction, as this seemed to be an important requirement.
5.6 Acceptance and future directions
A significant finding from the focus groups was the importance of gradual familiarization for societal acceptance of AR/MR devices in healthcare, as also noted in Ericsson (2024). Staff suggested that initial use cases should focus on high-impact, low-effort scenarios – such as wound assessment – where the benefits of the technology are immediately clear. Feedback from the test emphasized the need for continuous improvement and iterative testing with user feedback to refine both the technology and organizational processes.
Our findings can be beneficial for other work areas involving inexperienced workers who need guidance or employees working outside the company who require support in their tasks. Our results indicate that overly large MR headsets can lead to discomfort (e.g., heat, pressure sensations). On the other hand, the handling and use of MR headsets can also be learned by a non-tech-savvy group if they are well-prepared. Considering the limited use of MR headsets across all industries, additional testing and development of this technology is necessary to expand its applications and experience.
From a methods perspective, the use of usage data offers insights into the actual utilization of data glasses. The interdisciplinary approach to evaluation, involving computer science and social sciences, provides a more comprehensive understanding of the integration of technology into professional routines. Future research is thus encouraged to involve different disciplines when evaluating complex technological interventions.
5.7 Limitations
Nursing and care staff agreed to test this new system despite staff shortages and significant challenges in organizing the test, for example collection of informed consents or scheduling visits (Meyer and Zahner, 2023; Trukeschitz and Arth, 2023). As a result, the stress of juggling daily tasks and testing, along with other unknown factors, may have influenced their feedback. In addition, the test was limited to one service unit each in Austria and Luxembourg, with the unit in Austria also experiencing problems with internet reception.
As this was the first time the Remote Care Assist system was tested without project staff in the field of home care, we selected nursing and care staff who were interested in the technology and willing to test. Results may be different with less tech-savvy nursing staff. However, it was found that in many cases the technical skills of the nursing/care staff were not as important to success as their job experience, which facilitated a quicker identification of care situations where this new tool could be a useful addition. Some usage was induced by prompting the care organization to keep testing and by announcing a visit to discuss the devices. Further research would be needed to gain insights into completely independent usage in future field trials.
In addition, part of the testing was conducted during the COVID-19 pandemic in Austria, where nursing staff were required to wear face masks in the home of the home care service user. Wearing a HoloLens is not a natural human experience, nor is wearing a mask, and certainly not wearing both at the same time. Therefore, the results – particularly in terms of acceptance of the HoloLens – may have been influenced by this increased physical restriction and intrusion into the nursing staff’s personal space.
Originally, the project was to establish centralized care expert centers, but this was not realized, so we lack data on how the RCA system with HoloLenses would be received by care experts who are available when needed and by nursing/care staff who can always reach out to an expert whenever they want to. Further research is needed to test centralized expert centers and service units.
6 Conclusion
While the RCA system using MS HoloLens 2 has proven beneficial in some targeted scenarios, wider adoption will require improvements in device design, connectivity and integration into professional care routines. In addition, the model of centralizing expertise across regions to provide virtual support offers a scalable solution. This solution could also allow highly skilled staff with poor health, such as back problems, to remain in the workforce. For younger staff, the RCA system could increase efficiency and job attractiveness, making it a valuable tool for modernizing home care and meeting increasing demand. Further research is needed to investigate the effectiveness of Remote Care Assist systems in long-term care settings.
Data availability statement
The datasets presented in this article are not readily available because the test participants have not given their consent. Requests to access the datasets should be directed to Y29ybmVsaWEuc2NobmVpZGVyQGZod24uYWMuYXQ=.
Ethics statement
The studies involving humans were approved by the Ethics Board of the University of Applied Sciences Wiener Neustadt (09/09/2021; chairperson: Nimmerichter Alfred), Comité national d’éthique de recherche Luxembourg (no. 202209/07 Version 4.0, 23/05/2023) and Ministère de la Santé (reference 840xe52b7, 14/12/2022). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CS: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing, Investigation. PR: Formal analysis, Software, Visualization, Writing – review & editing, Investigation. PK: Data curation, Formal analysis, Software, Writing – review & editing, Investigation. BT: Conceptualization, Project administration, Funding acquisition, Methodology, Writing – review & editing, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Active Assisted Living Programme grant number aal-2020-7-144-CP. It received funding from the Active Assisted Living Programme, cofounded by the European Commission, National Funding Authorities of Austria, Belgium, Luxembourg and Switzerland and the individual project partners. Collaborating partners in the “Care about Care” project were University of Applied Sciences Wiener Neustadt (lead partner), WU Vienna University of Economics and Business (co-lead partner), MOCCA Software GmbH, Hilfswerk Niederösterreich, Korian Belgium, Stëftung Hëllef Doheem, Distrac Group and Eichenberger-Szenografie. The WU Research Institute for Economics of Aging received financial support from the Vienna Social Funds (Fonds Soziales Wien-FSW).
Acknowledgments
The authors would like to thank Thomas Grem (University of Applied Sciences Wiener Neustadt, Institute of Computer Science) for his support in the development of the RCA service. We would also like to thank Lara Arth and David Schermann (WU University of Economics and Business, Research Institute of Economics of Aging) for contributing to focus group interview data collection and analysis. We are also grateful to Stephanie Meyer and Nadine Zahner (Stëftung Hëllef Doheem) for conducting and documenting the focus groups in Luxembourg.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. This article is the result of human creativity and the joint efforts of the authors. The authors would like to acknowledge the assistance of OpenAI’s ChatGPT 4o and DeepL to improve readability.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
AAL Programme. (2021). Care about care (C^C). Available online at: https://www.aal-europe.eu/projects/care-about-care-cc/
Babaei, N., Zamanzadeh, V., Valizadeh, L., Lotfi, M., Samad-Soltani, T., Kousha, A., et al. (2023). A scoping review of virtual care in the health system: infrastructures, barriers, and facilitators. Home Health Care Serv. Q. 42, 69–97. doi: 10.1080/01621424.2023.2166888
Bandini, J. I., Siconolfi, D., Feistel, K., and Etchegaray, J. (2023). Low tech, high potential: using technology to improve communication across home care workers. J. Appl. Gerontol. 42, 776–781. doi: 10.1177/07334648221144027
Bauer, G., Rodrigues, R., and Leichsenring, K. (2018). Arbeitsbedingungen in der Langzeitpflege aus Sicht der Beschäftigten in Österreich.
Berggren, P., Ryrberg, T., Lindhagen, A., and Johansson, B. (2023). Building capacity – conceptualizing training of trainers. Proceedings of the International ISCRAM Conference, 701–710.
Briar, C., Liddell, E., and Tolich, M. (2014). Still working for love? Recognising skills and responsibilities of home-based care workers. Qual. Ageing Older Adults 15, 123–135. doi: 10.1108/QAOA-04-2014-0006
Care about Care. (2021). Project website. Available online at: https://www.careaboutcare.eu/
Directorate-General for Economic and Financial Affairs. (2021). The 2021 ageing report. Economic and budgetary projections for the EU member states (2019–2070). Available at: https://economy-finance.ec.europa.eu/publications/2021-ageing-report-economic-and-budgetary-projections-eu-member-states-2019-2070_en
Döring, N., and Bortz, J. (2016). Forschungsmethoden und Evaluation in den Sozial- und Humanwissenschaften. Berlin Heidelberg: Springer.
Eckert, M., Volmerg, J. S., and Friedrich, C. M. (2019). Augmented reality in medicine: systematic and bibliographic review. JMIR Mhealth Uhealth 7:e10967. doi: 10.2196/10967
Ericsson. (2024). Augmented tomorrow: AR experiences beyond smartphones and AR filters: Exploring consumer expectations and needs in an evolving XR landscape. Available online at: https://www.ericsson.com/en/reports-and-papers/consumerlab/reports/augmented-tomorrow-ar-experiences-beyond-smartphones-and-ar-filters
European Commission, Directorate-General for Employment, and Social Affairs and Inclusion. (2021). Long-term care report – Trends, challenges and opportunities in an ageing society (Vol. 1).
Famira-Mühlberger, U. (2024). Eine Projektion der öffentlichen Pflegekosten und des benötigten Pflegepersonals bis 2050. Available online at: https://www.wifo.ac.at/wwa/pubid/71450
FFG Projektdatenbank. (2020). Augmented reality Brillen für Virtuell-Kooperative active assisted living Szenarien—AuReAAL. Available online at: https://projekte.ffg.at/projekt/3311829
InnoCraft Limited. (2024). Matomo. Available online at: https://matomo.org/
Jain, M., Kumar, M., and Aggarwal, N. (2013). Web usage mining: an analysis. J. Emerg. Technol. Web Intell. 5, 240–246. doi: 10.4304/jetwi.5.3.240-246
Janßen, M., and Prilla, M. (2019a). Adjusting AR-workflows of care tasks: experiences from an initial study. Mensch Comput., 214–220. doi: 10.18420/muc2019-ws-623
Janßen, M., and Prilla, M. (2019b). Usability and utility of head mounted displays in care according to caregivers. 7th International Conference on Infrastructures in Healthcare, 1–9. Available at: https://dl.gi.de/items/b009b615-b3be-4aba-9dcd-fa51e6deeb66
Kalavrezou, N., Pot, M., Kadi, S., Simmons, C., and Leichsenring, K. (2025). Facts and figures on healthy ageing and long-term care. Available online at: https://www.euro.centre.org/publications/detail/5202
Klinker, K., Wiesche, M., and Krcmar, H. (2019). Digital transformation in health care: augmented reality for hands-free service innovation. Inf. Syst. Front. 22, 1419–1431. doi: 10.1007/s10796-019-09937-7
Korzeniowski, L., and Goczyla, K. (2022). Landscape of automated log analysis: a systematic literature review and mapping study. IEEE Access 10, 21892–21913. doi: 10.1109/ACCESS.2022.3152549
Krajic, K., Nowak, P., and Rappold, E. (2005). Pflegenotstand in der mobilen Pflege? Wissenschaftliches Gutachten gefördert durch die Fachgruppenvereinigung Gesundheitsberufe im ÖGB. Available at: https://scholar.google.at/citations?view_op=view_citation&hl=de&user=yCxQ-uQAAAAJ&citation_for_view=yCxQ-uQAAAAJ:ldfaerwXgEUC
MariaDB Foundation LLC. (2024). MariaDB Foundation. Available online at: https://mariadb.org/
Masoni, M., and Guelfi, M. R. (2020). WhatsApp and other messaging apps in medicine: opportunities and risks. Intern. Emerg. Med. 15, 171–173. doi: 10.1007/s11739-020-02292-5
Meyer, J., Wasmann, M., Heuten, W., El Ali, A., and Boll, S. C. J. (2017). Identification and classification of usage patterns in long-term activity tracking. Proceedings of the 2017 CHI conference on human factors in computing systems, 667–678. Project consortium of the C^C project.
Meyer, S., and Zahner, N. (2023). The C^C remote care assist HoloLens test center in Luxembourg: Evaluation results, part of deliverable 19 of the “care about care” project—unpublished manuscript. Stëftung Hëllef Doheem.
Organisation for Economic Co-operation and Development (2020). Who cares? Attracting and Retaining Elderly Care Workers. Paris: OECD Publishing.
Prilla, M., Recken, H., and Janßen, M. (2019). “Die Pflegebrille – Möglichkeiten und Barrieren der Nutzung von Augmented-Reality-Technologie in der ambulanten Intensivpflege” in Digitale Transformation von Dienstleistungen im Gesundheitswesen VI. (Gabler, Wiesbaden: Springer), 281–309.
Raintank Inc. (2024). Grafana OSS. Available online at: https://grafana.com/oss/grafana/
Romare, C., and Skär, L. (2020). Smart glasses for caring situations in complex care environments: scoping review. JMIR Mhealth Uhealth 8:e16055. doi: 10.2196/16055
Rubin, V. A., Mitsyuk, A. A., Lomazova, I. A., and van der Aalst, W. M. P. (2014). Process mining can be applied to software too! Proceedings of the 8th ACM/IEEE international symposium on empirical software engineering and measurement, 1–8.
Rush, K. L., Howlett, L., Munro, A., and Burton, L. (2018). Videoconference compared to telephone in healthcare delivery: a systematic review. Int. J. Med. Inform. 118, 44–53. doi: 10.1016/j.ijmedinf.2018.07.007
Schneider, C., Rameder, P., Kolmann, P., and Trukeschitz, B. (2023). “Remote assistance for home care workers: concept and technical implementation at a glance” in dHealth 2023. eds. B. Pfeifer, G. Schreier, M. Baumgartner, and D. Hayn (Amsterdam: IOS Press), 39–47.
Schneider, C., Trukeschitz, B., and Rieser, H. (2020). Measuring the use of the active and assisted living prototype CARIMO for home care service users: evaluation framework and results. Appl. Sci. 10:38. doi: 10.3390/app10010038
Shneiderman, B., Cohen, M., Jacobs, S., Plaisant, C., Diakopoulos, N., and Elmqvist, N. (2017). Designing the user Interface: Strategies for effective human-computer interaction (6th ed.) Pearson Education, Inc. Available online at: https://elibrary.pearson.de/book/99.150005/9781292153926
Spasova, S., Baeten, R., Coster, S., Ghailani, D., Peña-Casas, R., and Vanhercke, B. (2018). Challenges in long-term care in Europe: A study of national policies. doi: 10.2767/84573
Trukeschitz, B., and Arth, L. (2023). The C^C remote care assist HoloLens test center in Austria: Evaluation results, part of deliverable 19 of the “care about care” project—unpublished manuscript. WU Vienna.
Trukeschitz, B., Arth, L., and Schneider, C. (2022a). “Field trials of the C^C remote care assist system in Austria, Belgium and Luxembourg” in Study design & guidelines for recruitment & trial execution, deliverable D17 & D18 of the “care about care” project—unpublished manuscript. WU Vienna.
Trukeschitz, B., Eisenberg, S., Schneider, C., and Schneider, U. (2022b). Exploring the effectiveness of a fitness-app prototype for home care service users in Austria and Italy. Health Soc. Care Community. Wiley. 30, 1–12. doi: 10.1111/hsc.13733
Turkington, R., Mulvenna, M., Bond, R., O Neill, S., and Armour, C. (2018). The application of user event log data for mental health and wellbeing analysis. Proceedings of the 32nd international BCS human computer interaction conference, HCI 2018.
Wagnild, G. (2001). Chapter 4 growing old at home. J. Hous. Elder. 14, 71–84. doi: 10.1300/J081v14n01_04
Wiles, J. L., Leibing, A., Guberman, N., Reeve, J., and Allen, R. E. S. (2012). The meaning of “aging in place” to older people. The Gerontologist 52, 357–366. doi: 10.1093/geront/gnr098
Keywords: mixed-reality, remote support, home care, ambient assisted living, usage data
Citation: Schneider C, Rameder P, Kolmann P and Trukeschitz B (2025) Mixed-reality-supported communication for professional home care: system, use, barriers and use cases. Front. Comput. Sci. 7:1527038. doi: 10.3389/fcomp.2025.1527038
Edited by:
Deepak Dhungana, IMC University of Applied Sciences Krems, AustriaReviewed by:
Saulius Gudas, Vilnius University, LithuaniaMarkus Widhalm, IMC University of Applied Sciences Krems, Austria
Copyright © 2025 Schneider, Rameder, Kolmann and Trukeschitz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cornelia Schneider, Y29ybmVsaWEuc2NobmVpZGVyQGZod24uYWMuYXQ=