 Heber Isac Arbildo-Vega1,2
Heber Isac Arbildo-Vega1,2 Fredy Hugo Cruzado-Oliva3
Fredy Hugo Cruzado-Oliva3 Franz Tito Coronel-Zubiate4*Rubén Aguirre-Ipenza5Joan Manuel Meza-Málaga6,7Sara Antonieta Luján-Valencia6,8Eduardo Luján-Urviola9Adriana Echevarria-Goche10
Franz Tito Coronel-Zubiate4*Rubén Aguirre-Ipenza5Joan Manuel Meza-Málaga6,7Sara Antonieta Luján-Valencia6,8Eduardo Luján-Urviola9Adriana Echevarria-Goche10 Carlos Alberto Farje-Gallardo4Tania Belú Castillo-Cornock1,11Katherine Serquen-Olano1,11
Carlos Alberto Farje-Gallardo4Tania Belú Castillo-Cornock1,11Katherine Serquen-Olano1,11 Tania Padilla-Cáceres12,13
Tania Padilla-Cáceres12,13 Luz Caballero-Apaza14
Luz Caballero-Apaza14
- 1Faculty of Dentistry, Dentistry School, Universidad San Martin de Porres, Chiclayo, Peru
- 2Faculty of Human Medicine, Human Medicine School, Universidad San Martín de Porres, Chiclayo, Peru
- 3Faculty of Stomatology, Stomatology School, Universidad Nacional de Trujillo, Trujillo, Peru
- 4Faculty of Health Sciences, Stomatology School, Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas, Chachapoyas, Peru
- 5Faculty of Health Sciences, Universidad Continental, Lima, Peru
- 6Faculty of Dentistry, Dentistry School, Universidad Católica de Santa María, Arequipa, Peru
- 7Faculty of Medicine, Medicine School, Universidad Católica de Santa María, Arequipa, Peru
- 8Postgraduate School, Universidad Católica de Santa María, Arequipa, Peru
- 9Faculty of Dentistry, Universidad Andina Néstor Cáceres Velásquez, Juliaca, Peru
- 10Department of Dentistry, Dentistry School, Universidad Norbert Wiener, Lima, Peru
- 11Faculty of Health Sciences, Stomatology School, Universidad Señor de Sipán, Chiclayo, Peru
- 12Department of General Dentistry, Dentistry School, Universidad del Altiplano, Puno, Peru
- 13Research Institute in Environmental Sciences, Health and Biodiversity - IICASB, Universidad del Altiplano, Puno, Peru
- 14Department of Nursing, School of Nursing, Universidad del Altiplano, Puno, Peru
Background: Alzheimer's disease (AD) and periodontal disease (PD) are both chronic conditions with rising global prevalence. Emerging research suggests a possible link between PD-induced systemic inflammation and neurodegeneration observed in AD.
Objective: Employ an umbrella review to look into the association between periodontal disease and Alzheimer's disease.
Materials and methods: A comprehensive search was conducted until March 2025 across various electronic databases, including: PubMed, Cochrane Library, Scopus, SciELO, Web of Science, Google Scholar, ProQuest, and OpenGrey, and Dissertations and Theses. There were no time or language restrictions on the inclusion of systematic reviews (SR), with or without meta-analysis, as long as they looked at primary research that connected PD and AD. The following were excluded: preclinical and fundamental research, summaries, comments, case reports, protocols, personal opinions, letters, posters, literary or narrative reviews, fast reviews, intervention studies, and observational studies. The quality and general confidence of the included studies were evaluated using the AMSTAR-2 technique.
Results: A total of 358 items were found following the first search. 16 articles were left for additional review after the selection criteria were applied. With odds ratios (OR) and risk ratios (RR) ranging from 1.67 to 2.17 and 1.11 to 2.26, respectively, 14 studies showed a correlation between PD and AD.
Conclusions: Drawing from the findings and conclusions of the SR demonstrating a high overall confidence, it's established that PD and tooth loss exhibit an association with AD.
Systematic Review Registration: Registered in the Open Science Framework (OSF): DOI 10.17605/OSF.IO/GS367.
1 Introduction
Chronic diseases are responsible for approximately 60% of annual deaths worldwide, according to the WHO (1). Risk factors include age, genetics, obesity, poor diet, smoking, and physical inactivity (2). Although temporary inflammation is expected in the face of injury or infection, when local immune balance is not restored, chronic inflammation develops (3).
The progression of chronic diseases follows a common pattern: identification of the irritant, activation of inflammatory pathways, cytokine release, and cell recruitment (3, 4). The proinflammatory cytokines IL-1β, IL-6, and TNF-α, activate immune cells and perpetuate inflammation (5–7).
The human oral microbiota is composed of approximately 770 microorganisms that form a biofilm on the teeth (8). Under optimal hygiene conditions, a healthy balance of gram-positive bacteria predominates. However, factors such as high sugar intake, acid exposure, or poor brushing habits can alter composition (9). Diseases like periodontal disease (PD) can result from this imbalance, known as oral dysbiosis, which promotes the growth of anaerobic gram-negative bacteria (8). Between 20% and 50% of people worldwide suffer from PD, which includes periodontitis and gingivitis, making it one of the most prevalent chronic illnesses (10, 11). The advanced stage of periodontitis is typified by tooth loss, loss of bone support, and ongoing inflammation (12, 13). It is caused by polymicrobial infections and poor oral hygiene habits, such as lack of flossing (8, 14).
When the immune system cannot completely eliminate oral bacteria, gum inflammation becomes chronic (13). This leads to a continuous release of destructive inflammatory cells. In this context, Porphyromonas gingivalis, Treponema denticola, Fusubacterium nucleatum, and Aggregatibacter actinomycetemcomitans are commonly associated with PD (8, 12, 15). Since they are also present in healthy mouths, it's clear that the host´s inflammatory response-rather than just the presence of bacteria- determines how a disease develops (5, 13, 16).
Alzheimer's disease (AD) affects 47 million people. AD is a long-term neuroinflammatory condition that causes brain degeneration, with the hippocampus being one of the most affected regions (17), cognitive decline, and eventually death (1, 8). Approximately 7 out of ten cases of dementia are related to this disease, moreover, its prevalence increases with age (1). By 2040, dementia is expected to affect more than 81 million people worldwide (18).
AD progresses through the preclinical stage, then becomes mild cognitive impairment and finally triggers severe dementia (1). In the first stage, there are no visible symptoms, but neuropathological changes and inflammatory markers are already present (19). These changes can begin decades before the onset of clinical symptoms. Currently, definitive diagnosis is made postmortem through a brain autopsy, which limits the possibilities for early intervention (1).
AD is marked by the accumulation of amyloid plaques alongside tau protein neurofibrillary tangles (20, 21). Although the amyloid hypothesis postulates that amyloid initiates brain damage, some studies show its presence in people without AD (22) and its absence in patients with clinical symptoms (21). In contrast, the tau hypothesis argues that this protein is present even in early stages without amyloid, and may be the primary contributor to neurodegeneration (23).
Moreover, to amyloid plaques and tau tangles, brain inflammation is also observed in AD. The inflammatory hypothesis argues that AD develops due to a host immune response caused by plaques and tangles, which activate immune cells such as microglia (24). This triggers the release of proinflammatory cytokines such as IL-1, IL-6, and TNF-α (25, 26), which in turn can generate more amyloid and tau (27). As in PD, the interaction between bacteria and host immunity determines the severity of brain damage (1).
According to the focal infection idea, localized infections are the root cause of many chronic illnesses (27). From this perspective, a local alteration can trigger systemic effects, as microorganisms and inflammatory mediators can circulate throughout the body (1). Recently, a relationship has been identified between periodontitis and diseases such as atherosclerosis and diabetes mellitus, where oral bacteria can enter the bloodstream and promote systemic inflammation (10, 28–30).
Several studies show that periodontitis is associated with an increased risk of cardiovascular events, bacteremia, and systemic inflammation (10, 30–32). The relationship between diabetes mellitus (DM) and periodontitis has also been shown to be bidirectional: DM increases the risk of PD, and PD, in turn, impairs glycemic control (33).
Recent studies have investigated the potential influence of gut microbiota on neurodegenerative diseases, including Alzheimer's disease (14, 34). Stress-related disruptions of the gur-brain axis can elevate intestinal permeability, permitting endotoxins to breach the bloodstream. In turn, this elicits an immune reaction that may reach the central nervous system and foster disorders such as anxiety and depression (35), however, a direct causal link to Alzheimer's disease has yet to be established (14).
The Spanish Society of Neurology described a possible connection between periodontal disease and Alzheimer's disease. AD involves progressive brain degeneration, with loss of memory and cognitive skills, making independent living difficult. Furthermore, the relationship may be bidirectional: cognitive decline in AD reduces oral hygiene, increasing periodontal inflammation, while chronic periodontal infection may contribute to neuroinflammation and accelerate cognitive deterioration (14, 36, 37). This interplay highlights the importance of oral health maintenance in elderly patients with cognitive decline, especially considering the increasing susceptibility to infection and reduced ability to perform adequate self-care.
According to one study, Alzheimer's disease patients tend to have more missing teeth and edentulism than people without the disease (38). This suggests that tooth loss, potentially related to PD, may be implicated in the development of AD. A recent finding highlights the involvement of Porphyromonas gingivalis, a pathogenic bacterium linked to PD, in cognitive decline due to the release of inflammatory toxins (8, 39–43).
Increasing evidence has shown that Porphyromonas gingivalis, a keystone pathogen in periodontitis, can invade the brain, promoting neuroinflammation and tau protein phosphorylation through its virulence factor gingipains (44, 45). In murine models, oral infection with Porphyromonas gingivalis resulted in brain colonization and increased amyloid-β production, supporting a causal role (44). Moreover, Porphyromonas gingivalis DNA and gingipains have been detected in the hippocampus of AD patients (45), suggesting a potential mechanistic pathway between oral infection and neurodegeneration.
Research suggests a bidirectional relationship between PD and AD: PD may increase the risk of Alzheimer's disease and vice versa (46, 47). In accordance to research by Qi et al., the risk of dementia rose by 1.1% and the chance of cognitive impairment by 1.4% for every tooth lost (37). Although PD is the leading cause of tooth loss (1), how this loss is linked to cognitive decline is not yet fully understood. Two pathways have been proposed: oral bacterial migration to other organs and secondary systemic inflammation (4).
In recent years, scientific research has focused more attention on the relationship between oral health and neurodegenerative diseases. AD, one of the most prevalent conditions, continues to be studied to understand its complex etiology. In this context, PD, a chronic inflammatory oral disease, has gained prominence as a possible factor in the development or progression of AD (44). This growing interest promotes an interdisciplinary approach that integrates oral health as a fundamental component of neurological well-being.
Figure 1 illustrates the hypothesized biological pathways linking periodontal disease with Alzheimeŕs disease. This schematic representation integrates current evidence on microbial translocation, systemic inflammation, neuroimmune responses, and behavioral changes, and highlights the bidirectional interplay between both conditions.
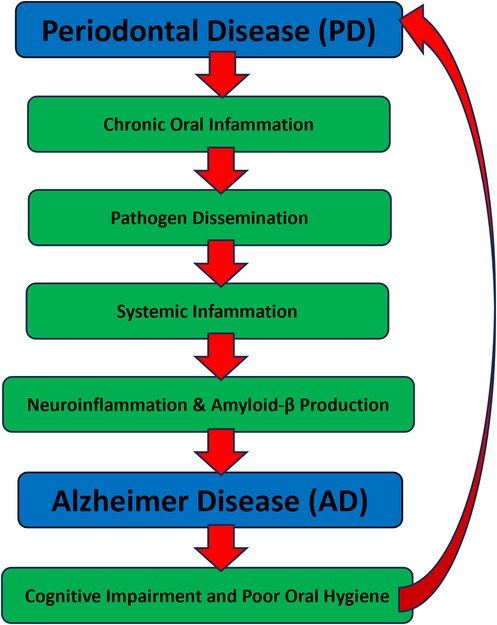
Figure 1. Hypothesized pathways linking periodontal disease and Alzheimeŕs disease. The diagram illustrates the proposed bidirectional relationship between periodontal disease (PD) and Alzheimeŕs disease (AD). Chronic inflammation originating in PD promotes pathogen dissemination and systemic immune activation, which can lead to neuroinflammation, amyloid-β accumulation, and Alzheimeŕs pathology. As AD progresses, cognitive decline and reduced self-care capacity impair oral hygiene, exacerbating periodontal inflammation. This creates a self-perpetuating cycle involving bacterial virulence factors (e.g., gingipains), proinflammatory cytokines (e.g., IL-1β, IL-6, TNF-α), and disruption of the blood-brain barrier.
Therefore, the objective of this overview was to consolidate the existing evidence and address the following question: “What is the current understanding regarding the relationship between PD and AD?” Additionally, how overall confidence are systematic reviews in evaluating this topic?
2 Materials and methods
2.1 Protocol and registration
We drafted a protocol aligned with the PRISMA-P guidelines (48) and officially registered it on the Open Science Framework (DOI 10.17605/OSF.IO/GS367). The review follows the PRIO-harms (49), and no ethical clearance was required for this umbrella review.
The research question was formulated using the PECO framework (population, exposure, comparison, and outcomes), aimed to evaluate the association between periodontal disease and Alzheimer's disease. The PECO elements were defined as follows:
– Population: individuals of all ages evaluated for cognition function.
– Exposure: individuals with periodontal disease or tooth loss.
– Comparison: individuals without periodontal disease.
– Outcomes: diagnosis or risk of Alzheimeŕs disease, cognitive impairment, or dementia.
This framework guided the elegibility criteria, for the included systematic reviews. Only reviews reporting a measurable association betweern PD and AD (or related cognitive outcomes) were considered.
2.2 Eligibility criteria and results of interest
The eligible studies comprised SR with or without meta-analysis, without limitations on publication date or language, that investigated primary studies exploring the association between PD and AD. Excluded were literature or narrative reviews, rapid reviews, intervention studies, observational studies, preclinical and basic research, abstracts, commentaries, case reports, protocols, personal opinions, letters, and posters.
2.3 Sources of information, search strategy, and additional search for primary studies
On March 25th, 2025, an electronic search was conducted across five databases, including PubMed, Cochrane database, Scielo, Web of Science, and Scopus. Grey literature was explored using the top 100 reports from Google Scholar, Proquest Dissertations and Theses, and OpenGrey. Furthermore, reference lists of the included studies were screened. Retrieved articles were managed using reference management software (Zotero® 6.0, Center for History and New Media, Fairfax, Virginia, USA), and duplicate entries were eliminated. The search strategies implemented for each database are detailed in Table 1.
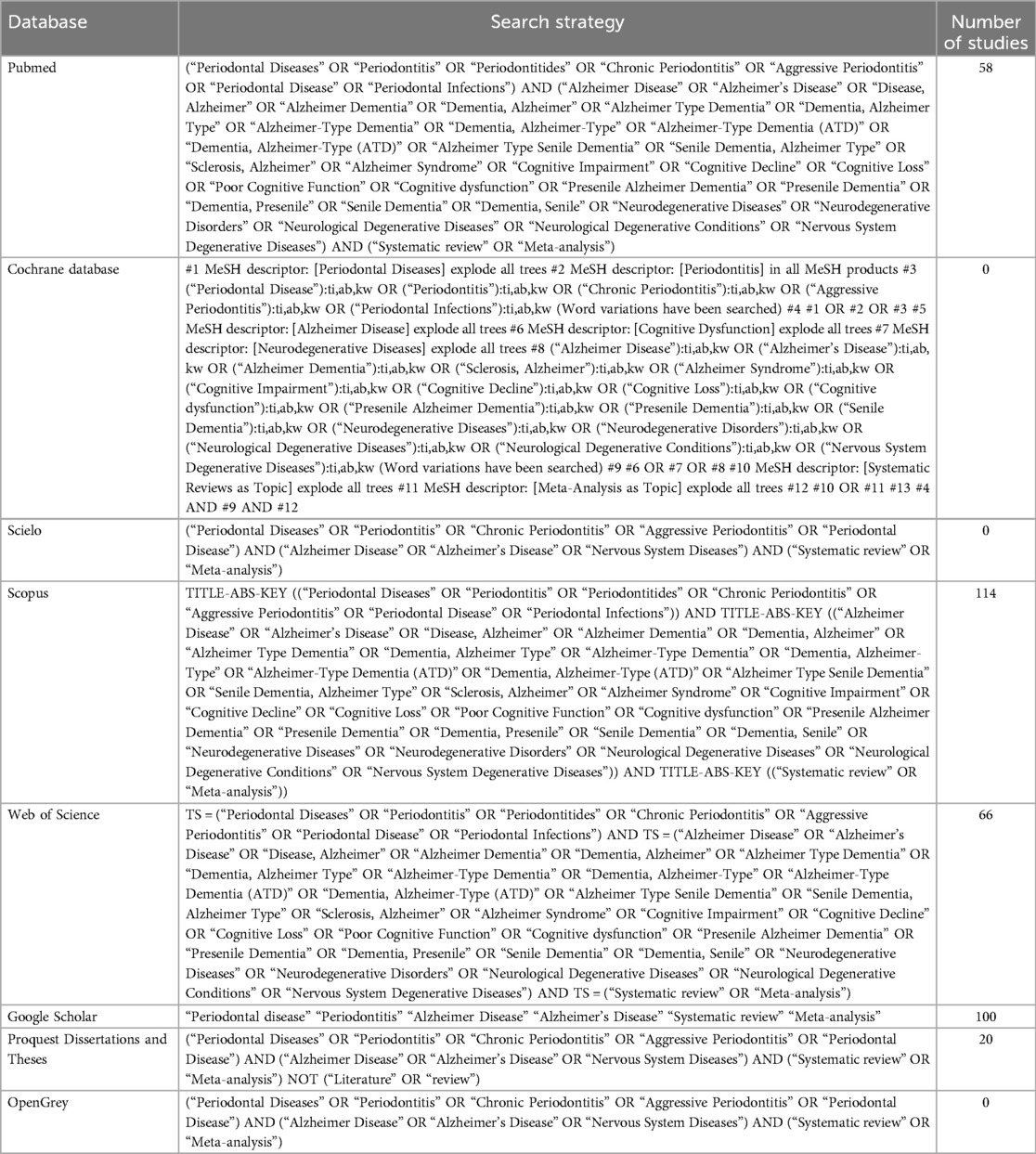
Table 1. Search strategy for each search engine.
2.4 Data management and selection process
All identified articles were imported into Rayyan®, an online systematic review platform maintained by the Qatar Computing Research Institute in Doha, Qatar. The study Selection process was conducted in two sequential phases. In the first phase, two reviewers (F.C.O and F.C.Z) independently evaluated the titles and abstracts of the identified articles.
Subsequently, in the second phase, the same two reviewers independently reviewed the full text of each article. Any discrepancies between the two reviewers were resolved through consultation with a third reviewer (H.A.).
2.5 Data collection process
Data were independently and in duplicate extracted from each study using a standardized table prepared by two reviewers (F.C.O and R.A.). These entries were then cross-checked, and any disagreements were settled by consulting the third author (H.A.). The information gathered from the chosen articles comprised author names, publication year, study and primary designs, count of studies included in qualitative vs. quantitative synthesis, findings, key conclusions, and any mention of employed frameworks or methods- such as PRISMA, PROSPERO, GRADE, and meta-analysis.
2.6 Assessment of methodological quality, quality of evidence, and meta-bias
Two reviewers (J.M. and S.L.) independently conducted a duplicate evaluation of the methodological quality of the included SRs, with a calibration of Kappa 0.85, using the AMSTAR-2 checklist (A Measurement Tool to Assess Systemic Reviews) (50). AMSTAR-2 assesses the methodological quality of SRs through 16 questions, each with three possible responses: “yes,” “no,” or “partially yes.” The overall confidence rating of the studies, categorized as high, moderate, low, or critically low, was determined following the guidelines proposed by Shea et al. (50).
2.7 Summary of measures
For SR without meta-analysis, we considered the summarized results from the primary studies included. However, if the SR included a meta-analysis, we focused on the results presented with odds ratio (OR) or risk/rate ratio (RR) to assess the association between PD and AD.
2.8 Summary of results
The primary outcomes of the included SR were summarized, with their findings classified into multiple AD-related categories.
3 Results
3.1 Review and selection of primary studies
From the electronic database search, 358 articles, and 121 remained after duplicate removal. During phase one, titles and abstracts narrowing the list to 20 articles full-text review. Ultimately, 16 systematic reviews met inclusion criteria for qualitative synthesis. Article exclusion criteria appear in Table 2, and the complete study selection workflow is depicted in Figure 2.
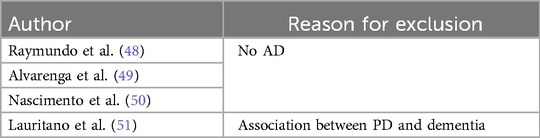
Table 2. Reason for exclusion of studies.
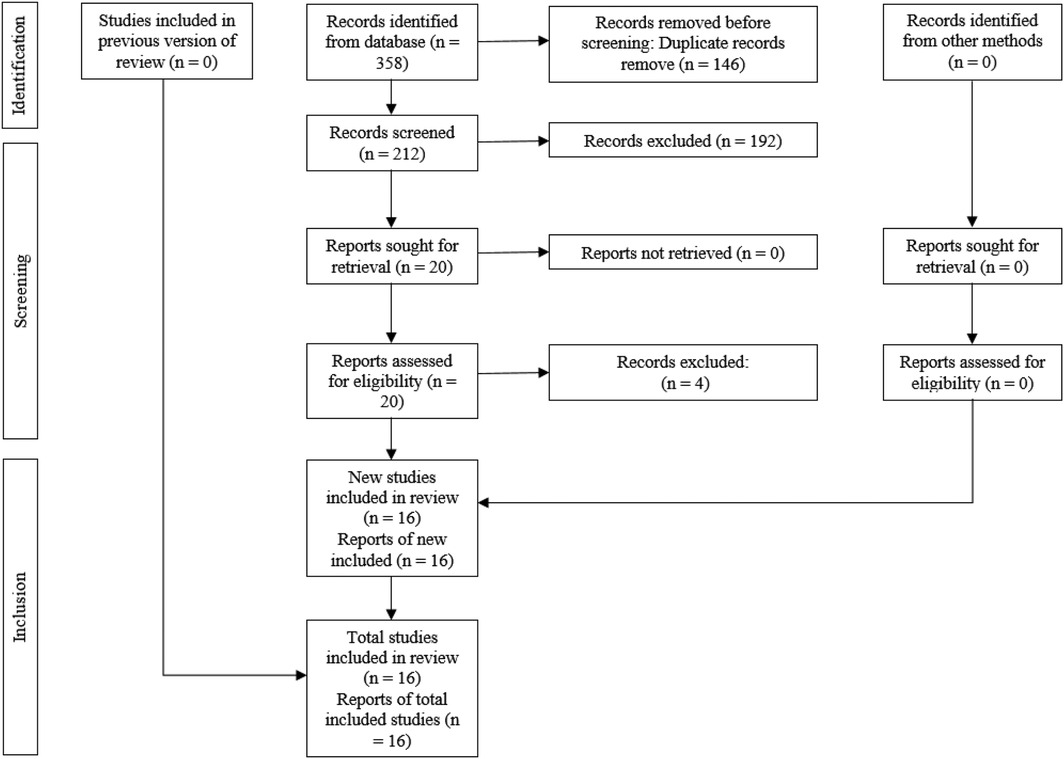
Figure 2. PRISMA flow diagram of the study selection process.
3.2 Review and characteristics of included studies
The SR included in the analysis were published between 2017 and 2025 and originated from various countries, including China (41, 52–54), France (8), India (55), Italy (38), Morocco (56), Poland (57), Republic of Korea (58), Singapore (59), Spain (60, 61), United Arab Emirates (62) and United Kingdom (63, 64). Thirteen (8, 41, 54–64) and three (38, 52, 53) SR evaluated the association of PD and tooth loss, respectively. Additional details pertaining to the characteristics of these systematic reviews can be found in Table 3.
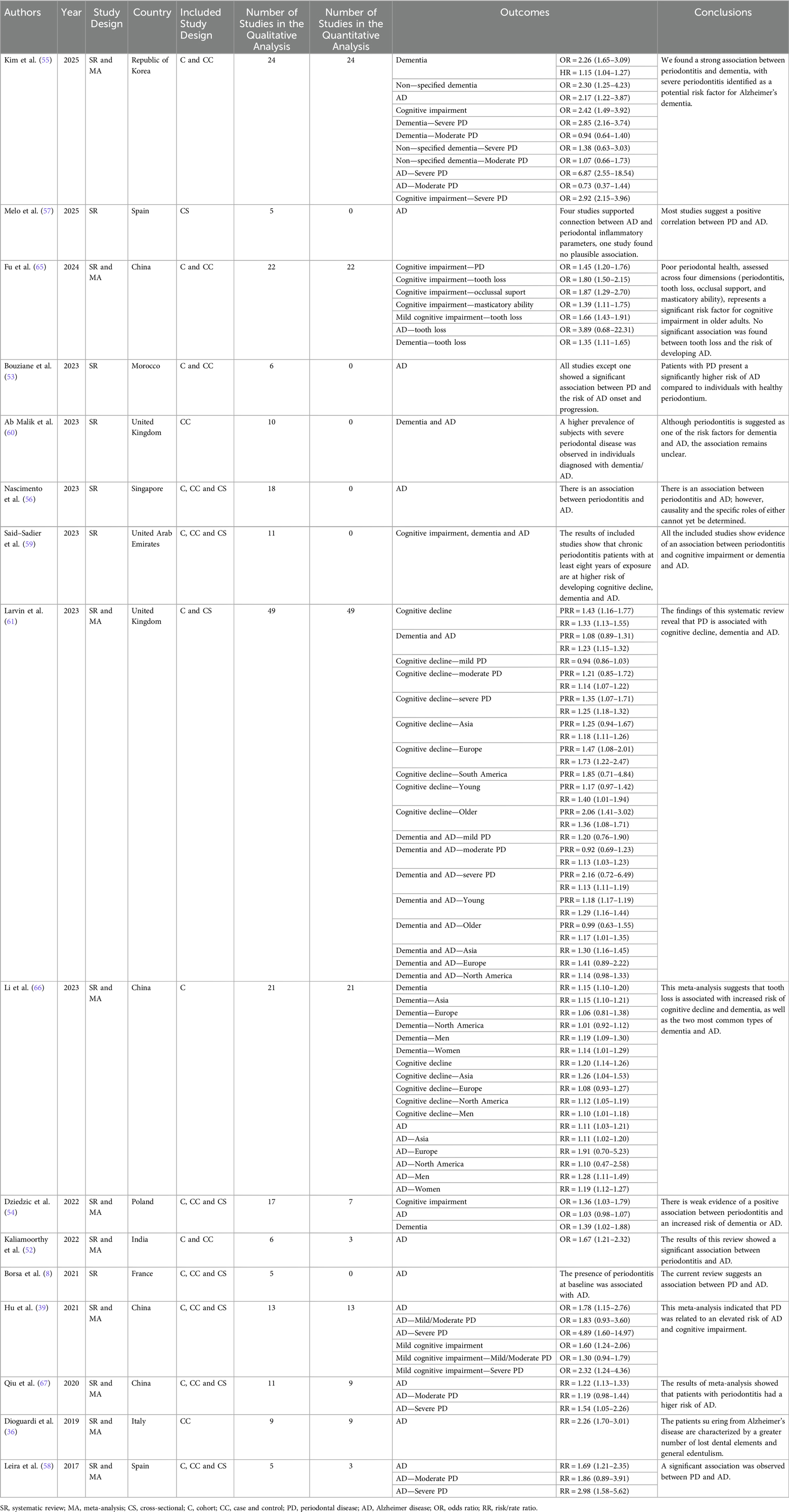
Table 3. Characteristics of included studies.
3.3 Assessment of methodological quality and quality of evidence
Ten SR (8, 54–56, 58–62, 64) were considered to have high confidence, and six SR (39, 41, 52, 53, 57, 63) had low confidence (Table 4).
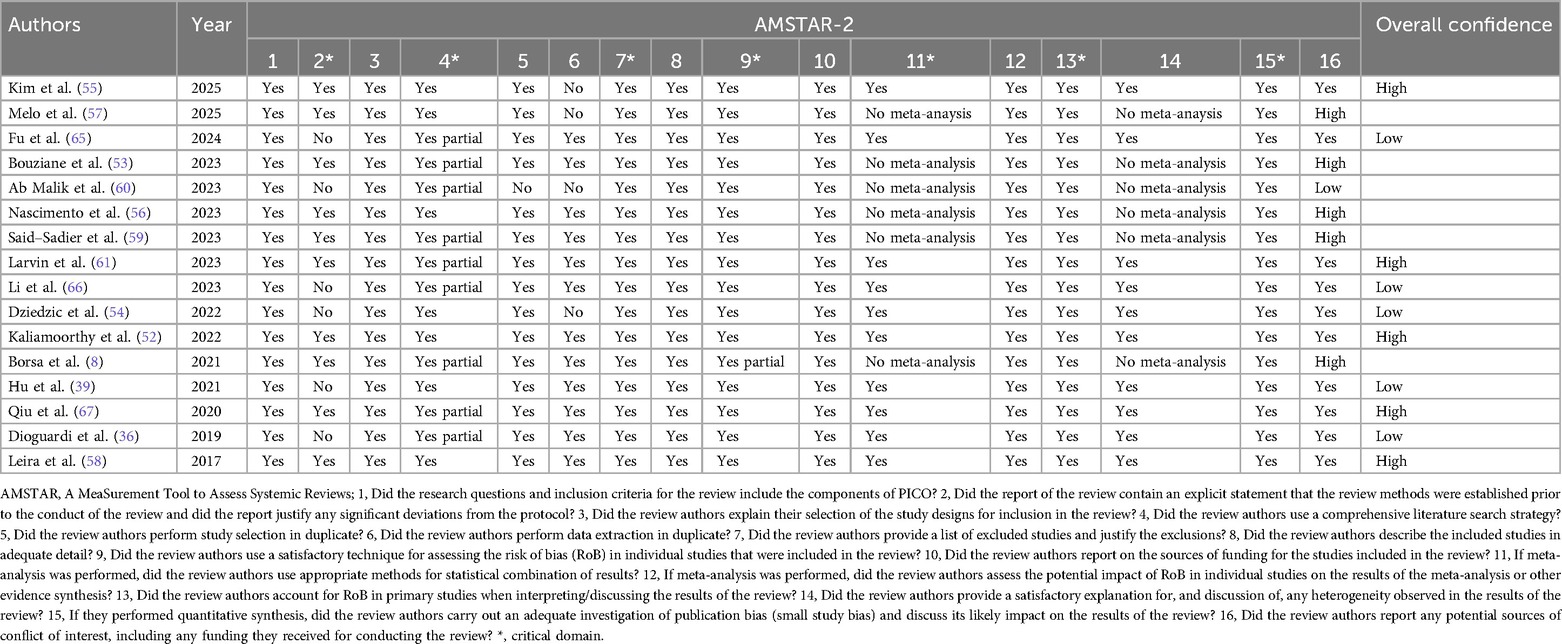
Table 4. Assessment of the methodological quality and the quality of the evidence of the included systematic reviews.
3.4 Overlapping
A total of 232 primary studies were identified across the included SR. Of these, approximately 75.86% exhibited overlap, having been included in more than one SR. Specifically, 28 studies were duplicated in two reviews, 11 appeared in three, and 6 were present in four. Additionally, 5 studies were included in five reviews, 1 in six, 2 in seven, 1 in eight, and 1 in ten reviews. Detailed information regarding the extent of overlap and the characteristics of the primary studies is provided in Supplementary Appendix A.
3.5 Synthesis of results
The summaries of the findings are displayed in Table 5.
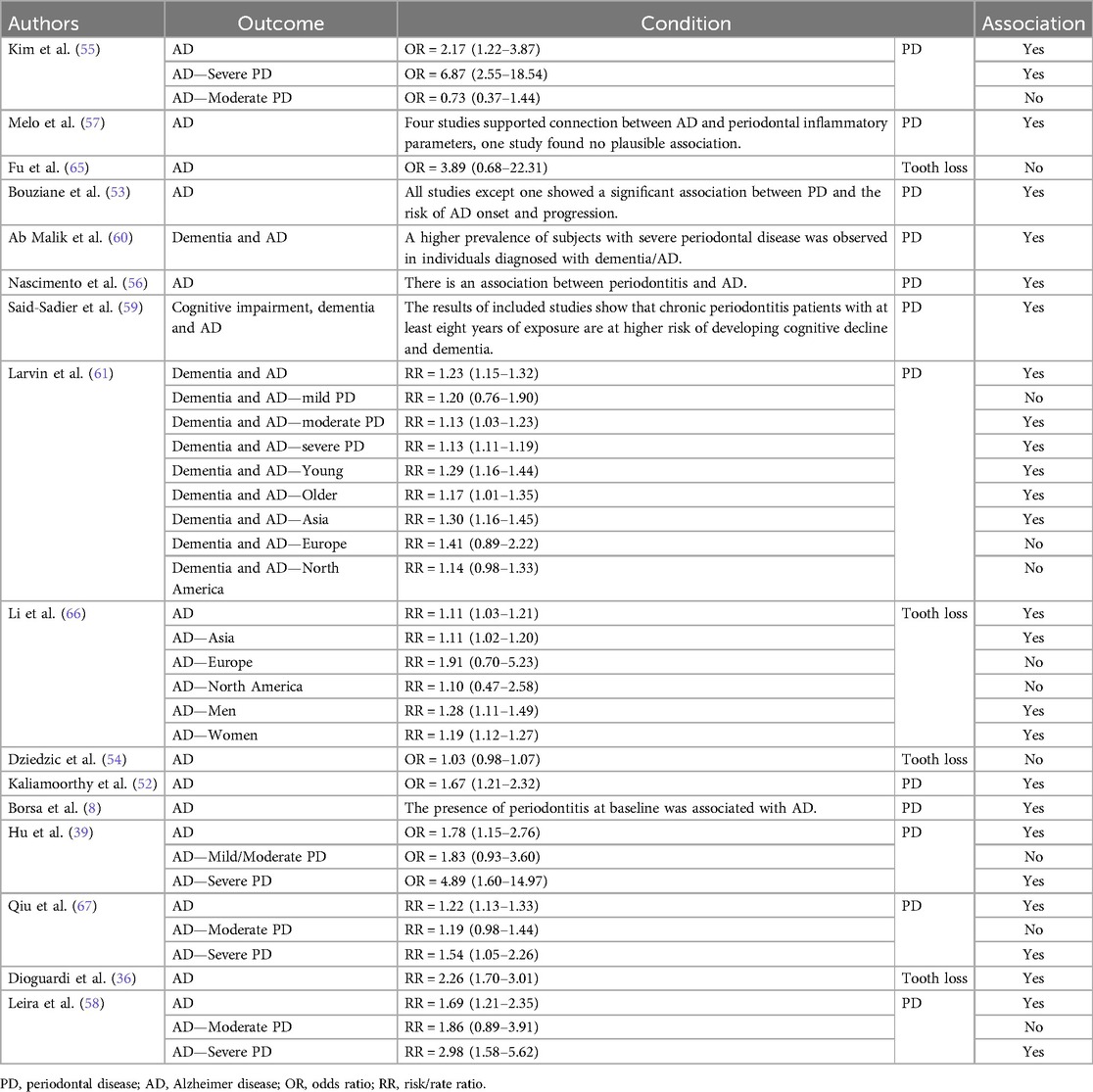
Table 5. Synthesis of the results of the included studies.
3.6 Alzheimer disease (AD)
Nine SR (8, 41, 54–56, 58–61) included reported that there was an association between PD and AD, but in 1 SR (54) this association was not found. Six SR (41, 54, 55, 57, 58, 61) meta-analyzed the results and found that the OR ranged from 1.03 [CI: 0.98–1.07] (57) to 2.17 [CI: 1.22–3.87] (58) and the RR ranged from 1.22 [CI: 1.13–1.33] (54) to 1.69 [CI: 1.21–2.35] (61). Melo et al. (60), Bouziane et al. (56), Nascimento et al. (59) and Borsa et al. (8) reported that there is an association between AD and PD.
One SR (63) included reported that there was an association between PD and AD for Asia, but not Europe and North America. This study meta-analyzed its results and found that the RR for Asia was 1.11 [CI: 1.02–1.20], for Europe was 1.91 [CI: 0.70–5.23], and for North America was 1.10 [CI: 0.47–2.58].
One SR (53) included reported that there was an association between PD and AD for sex. This studies meta-analyzed its results and found that the RR for men was 1.28 [CI: 1.11–1.49] and for women was 1.19 [CI: 1.12–1.27].
Four SR (41, 54, 58, 61) included reported that there was an association between PD and AD for severe PD, but not mild or moderate PD. This studies meta-analyzed its results and found that the OR for mild—moderate PD ranged from 0.73 [CI: 0.37–1.44] (58) to 1.83 [CI: 0.93–3.60] (41) and the RR ranged from 1.19 [CI: 0.98–1.44] (54) to 1.86 [CI: 0.89–3.91] (61), and for severe PD the OR ranged from 4.89 [CI: 1.60–14.97] (41) to 6.87 [CI: 2.55–18.54] (58) and the RR ranged from 1.54 [CI: 1.05–2.26] (54) to 2.98 [CI: 1.58–5.62] (61).
Two SR (38, 53) included reported that there was an association between tooth loss and AD, but in 1 SR (52) this association was not found. These studies meta-analyzed their results and found that the OR was 3.89 [CI: 0.68–22.31] (52) and the RR ranged from 1.11 [CI: 1.03–1.21] (53) to 2.26 [CI: 1.70–3.01] (38).
3.7 Dementia and Ad
Three SR (62–64) included reported that there was an association between PD and cognitive impairment, dementia and AD. One SR (64) meta-analyzed its results and found that the RR was 1.23 [CI: 1.15–1.32]. Ab Malik et al. (63) reported that there is an association between PD and dementia and AD, and Said-Sadier et al. (62) reported that there is an association between PD and cognitive impairment, dementia and AD.
One SR (64) included reported that there was an association between PD and dementia and AD for Asia, but not Europe and North America. This study meta-analyzed its results and found that the RR for Asia was 1.30 [CI: 1.16–1.45], for Europe was 1.41 [CI: 0.89–2.22], and for North America was 1.14 [CI: 0.98–1.33].
One SR (64) included reported that there was an association between PD and dementia and AD for age. These studies meta-analyzed its results and found that the RR for young was 1.29 [CI: 1.16–1.44] and for older was 1.17 [CI: 1.01–1.35].
One SR (64) included reported that there was an association between PD and dementia and AD for moderate or severe PD, but not mild PD. This study meta-analyzed its results and found that the RR for mild PD was 1.20 [CI: 0.76–1.90], for moderate PD was 1.13 [CI: 1.03–1.23], and for severe PD was 1.13 [CI: 1.11–1.19].
4 Discussion
This umbrella review aimed to elucidate the link between PD and AD by gathering and examining pertinent systematic reviews and meta-analysis. From this investigation, we distilled these principal findings: the systematic reviews included here corroborate an association between PD and AD, aligning with the evidence presented by Hernández-Nieto et al. (14).
The investigation involved an exhaustive literature search aimed at gathering and critically evaluating all existing systematic reviews on the relationship between PD and AD. Sixteen SRs were identified that met the established selection criteria. Although SRs constitute a reliable source of scientific evidence, it is important to exercise caution when interpreting their results due to the possibility of bias (68). The SRs considered in this research were subject to certain limitations stemming from the chosen primary studies-for instance, the inclusion of various types of studies, the fact that some of them did not present AD as a primary outcome but addressed it in conjunction with dementia and cognitive impairment, and the high overlap of primary studies. These limitations within the primary studies impeded the feasibility of performing a meta-analysis. Although several of the reviews analysed demonstrated high confidence ratings-potentially bolstering the study's findings and conclusions-the fact that numerous systematic reviews exhibited low confidence underscores the imperative for more stringent research methods in this field. We evaluated the methodological rigor of the included SRs with the updated and well-established AMSTRAR-2 instrument (69). Weaknesses were identified in critical domain 2, which included the lack of an explicit statement on the establishment of review methods prior to the review. In addition, deficiencies were found in non-critical domains 5 and 6, which included the lack of selection and data extraction from duplicate studies. These results emphasize the necessity of resolving these methodological challenges in upcoming systematic reviews (SRs).
An umbrella review conducted in 2024 (14), which included 13 systematic reviews on the association between PD and AD, highlighted that, although there is a relationship between AD and PD according to the studies analyzed, more support is needed in the literature and the inclusion of randomized clinical trials on this topic.
Interest in exploring the link between PD and AD. Has surged in recent years, with extensive research confirming this connection. AD now stands as the leading cause of dementia and ranks among the top causes of death in older adults globally, impacting individuals across all racial and ethnic groups (1, 8). While prevention remains elusive and prevalence rises with age, evidence indicates that modifiable risk factors can be addressed and cognitive health supported (70, 71).
Dental health researchers have long investigated the link between AD and PD, identifying two main mechanistic pathways: one hand, the gradual loss of cognitive function in patients may lead to poorer oral hygiene practices and thus elevate periodontal risk; on the other hand, chronic immune-driven inflammation originating in periodontitis can trigger neuroinflammatory responses that promote Alzheimer's pathology (14).
Care must be taken when interpreting the results of SRs, as approximately 76% of the primary studies are recurrently included in multiple reviews. This redundancy may lead to repeated analyses of the same data, which could bias the perceived scope and depth of research activity in this field. Nevertheless, the development of new SRs remains warranted, particularly those designed to address the methodological limitations noted by Moher (72), given the considerable degree of overlap identified among existing reviews.
As individuals age, the link between PD and AD becomes more pronounced. The likely cause is that aging gradually impairs the immune system and the body's protective barriers. This facilitates the persistence of chronic infections such as PD and, simultaneously, the accumulation of neuroinflammatory damage. Furthermore, with age, the cognitive and physical abilities to maintain adequate oral hygiene decline, which aggravates PD and, consequently, enhances systemic inflammation that can affect the brain (73–75).
Furthermore, this association was found to be common in both men and women. This could be explained by the universality of shared risk factors, such as advanced age, chronic systemic inflammation, and altered immune response. Furthermore, periodontal bacteria and their neuroinflammatory effects do not discriminate by gender, with both men and women having similar exposures to oral pathogens and systemic risk factors related to AD (57, 76).
Additionally, this association was observed to be common in people suffering from severe PD. This could be explained by the fact that in severe cases of PD, damage to periodontal tissues allows for greater release of bacteria and toxins into the bloodstream, which intensifies systemic inflammation. This persistent inflammation can reach the central nervous system and trigger or aggravate neurodegenerative processes related to AD. Studies have shown that the presence of bacteria such as P. gingivalis in the brain is related to more severe cases of cognitive decline (39, 40, 77).
Finally, the association was observed to be present in Asia. This could be attributed to cultural, dietary, and genetic factors that influence both oral health and the predisposition to AD. High rates of population aging in several Asian countries, along with reduced access to preventive dental care in some regions, may also play a role, favoring severe forms of PD and, consequently, a higher likelihood of AD-associated neuroinflammation (78, 79).
4.1 Implications for clinical practice
Patients with Alzheimeŕs disease present unique challenges to oral care providers. These includes cognitive decline leading to poor cooperation during procedures, difficulties in understanding and following hygiene instructions, increase risk of aspiration during treatments, and the need for caregiver involvement in daily oral care routines. Behavioral management techniques, shorter appointment times, and frequent preventive visits are often required.
Oral health practitioners are tasked with informing and empowering patients about the link between PD and AD. Encouraging consistent oral hygiene-brushing, flossing, and using mouthwash- helps control plaque formation and may lower Alzheimer's risk. In personalized care, it's advisable to include periodontal evaluations in routine risk screening alongside patient education on Alzheimer's. implementing preventive actions to modify risk factors is essential to reduce the chances of both conditions. Additionally, creating a follow-up protocol for Alzheimer's patients—including regular dental exams and timely periodontal assessments-is key. Working in tandem with psychiatrists, nutritionists, and other health professionals ensures a comprehensive, coordinated approach to the dental and medical management of Alzheimer's patients.
4.2 Implications for research
This review highlights the critical need to enhance the quality of SR reporting. To address this need, the authors advocate the adoption of robust quality assessment tools to guide the development of future SRs. They stress that primary studies should be conducted with rigorous methodological standards to ensure reliable results.
For future research in this field, the authors recommend conducting high-quality prospective studies with large sizes and standardized measurements. They also call for more comprehensive investigations to clarify the precise mechanisms and the scope of the relationship between PD and AD.
4.3 Limitations
This umbrella review has some limitations. First, many of the included systematic reviews were based on observational studies, which, despite revealing associations, do not confirm causality. Second, there was high overlap among primary studies (over 75%), potentially inflating the evidence base and reducing independence across reviews. Third, meta-analyses were not available for all included systematic reviews, and where present, they often varied in effect measures and population characteristics. Fourth, diagnostic criteria for both PD and AD differed across studies, contributing to clinical heterogeneity and limiting comparability. Finally, some reviews lacked protocol registration or risk of bias assessment, which reduces confidence in their findings. Future systematic reviews should follow standardized protocols (e.g., PRISMA, AMSTAR 2) to improve methodological rigor.
Despite these limitations, this umbrella review provides a structures synthesis of the best available evidence, guiding future research and informing clinical awareness.
5 Conclusion
Drawing from the findings and conclusions of the including systematic reviews-many of which demonstrated high methodological confidence- there is consistent observational evidence supporting an association between periodontal disease and Alzheimer's disease. This relationship appears to be bidirectional, as cognitive impairment affects oral hygiene practices, while chronic periodontal inflammation may contribute to neurodegeneration. Given the aging global population and the growing burden of Alzheimeŕs disease, early periodontal evaluation and management should be considered part of comprehensive geriatric care. Additionally, interdisciplinary strategies involving dental professionals, neurologists, caregivers, and primary healthcare providers are essential for improving the quality of life and clinical outcomes of these patients. Future research should aim to clarify causal mechanisms and evaluate the effectiveness of preventive periodontal interventions in reducing Alzheimeŕs disease progression.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
HA-V: Conceptualization, Formal analysis, Supervision, Methodology, Writing – original draft, Writing – review & editing. FC-O: Investigation, Methodology, Writing – original draft. FC-Z: Writing – review & editing, Writing – original draft, Software. RA-I: Data curation, Writing – review & editing, Software. JM-M: Writing – original draft, Validation. SL-V: Writing – original draft, Validation. EL-U: Software, Writing – original draft. AE-G: Investigation, Writing – original draft. CF-G: Writing – review & editing, Resources. TC-C: Writing – original draft, Resources. KS-O: Data curation, Writing – original draft. TP-C: Visualization, Writing – original draft. LC-A: Funding acquisition, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdmed.2025.1635200/full#supplementary-material
Abbreviations
PD, periodontal disease; AD, Alzheimer's disease; SR, systematic review; OR, odds ratio; RR, risk ratio; WHO, World Health Organization; IL-1, interleukin-1; IL-6, interleukin-6; PRISMA-P, preferred reporting items for systematic reviews and meta-analysis protocols; PRIO-harms, preferred reporting items for overview of systematic reviews checklist; PECO, population, exposure, comparison, outcomes; GRADE, grading of recommendations assessment, development and evaluation; MA, meta-analysis; C, CC, CS, cohort (C), case-control (CC), cross-sectional (CS); RoB, risk of bias; AMSTAR-2, A measurement tool to assess systematic reviews—2nd version; OSF, open science framework.
References
1. Lamphere AK, Nieto VK, Kiser JR, Haddlesey CB. Potential mechanisms between periodontitis and Alzheimer's Disease: a scoping review. Can J Dent Hyg. (2023) 57:52–60.36968797
2. Kotas ME, Medzhitov R. Homeostasis, inflammation, and disease susceptibility. Cell. (2015) 160(5):816–27. doi: 10.1016/j.cell.2015.02.010
3. Chen L, Deng H, Cui H, Fang J, Zuo Z, Deng J, et al. Inflammatory responses and inflammation-associated diseases in organs. Oncotarget. (2017) 9:7204–18. doi: 10.18632/oncotarget.23208
4. Hasturk H, Kantarci A. Activation and resolution of periodontal inflammation and its systemic impact. Periodontol 2000. (2015) 69:255–73. doi: 10.1111/prd.12105
5. Pan W, Wang Q, Chen Q. The cytokine network involved in the host immune response to periodontitis. Int J Oral Sci. (2019) 11:30. doi: 10.1038/s41368-019-0064-z
6. Gleerup HS, Hasselbalch SG, Simonsen AH. Biomarkers for Alzheimer’s disease in Saliva: a systematic review. Dis Markers. (2019) 2019:4761054. doi: 10.1155/2019/4761054
7. Cardoso EM, Reis C, Manzanares-Céspedes MC. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad Med. (2018) 130:98–104. doi: 10.1080/00325481.2018.1396876
8. Borsa L, Dubois M, Sacco G, Lupi L. Analysis the link between periodontal diseases and Alzheimer’s disease: a systematic review. Int J Environ Res Public Health. (2021) 18:9312. doi: 10.3390/ijerph18179312
9. Ezzo PJ, Cutler CW. Microorganisms as risk indicators for periodontal disease. Periodontol 2000. (2003) 32:24–35. doi: 10.1046/j.0906-6713.2003.03203.x
10. Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci. (2017) 11:72–80.
11. Jin LJ, Lamster IB, Greenspan JS, Pitts NB, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis. (2016) 22:609–19. doi: 10.1111/odi.12428
12. Kurgan S, Kantarci A. Molecular basis for immunohistochemical and inflammatory changes during progression of gingivitis to periodontitis. Periodontol. (2000 2018) 76:51–67. doi: 10.1111/prd.12146
13. Cekici A, Kantarci A, Hasturk H, Van Dyke TE. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000. (2014) 64:57–80. doi: 10.1111/prd.12002
14. Hernández-Nieto L, Barrios-Ayola F, Diaz-Caballero A. Existe relación entre el alzheimer y la enfermedad periodontal? Una Revisión Tipo Paraguas. Actabioclinica. (2024) 14(28):381–409. doi: 10.53766/acbio/2024.14.28.20
15. Paster BJ, Olsen I, Aas JA, Dewhirst FE. The breadth of bacterial diversity in the human periodontal pocket and other oral sites. Periodontol 2000. (2006) 42:80–7. doi: 10.1111/j.1600-0757.2006.00174.x
16. Yu N, Van Dyke TE. Periodontitis: a host mediated disruption of microbial homeostasis. Curr Oral Health Rep. (2020) 7:3–11. doi: 10.1007/s40496-020-00256-4
17. Wilckens KA, Stillman CM, Waiwood AM, Kang C, Leckie RL, Peven JC, et al. Exercise interventions preserve hippocampal volume: a meta-analysis. Hippocampus. (2021) 31:335–47. doi: 10.1002/hipo.23292
18. Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguli M, et al. Global prevalence of dementia: a delphi consensus study. Lancet Lond Engl. (2005) 366:2112–7. doi: 10.1016/S0140-6736(05)67889-0
19. Villemagne VL, Burnham S, Bourgeat P, Brown B, Ellis KA, Salvado O, et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. (2013) 12:357–67. doi: 10.1016/S1474-4422(13)70044-9
20. Kent SA, Spires-Jones TL, Durrant CS. The physiological roles of tau and aβ: implications for Alzheimer’s disease pathology and therapeutics. Acta Neuropathol (Berl). (2020) 140:417–47. doi: 10.1007/s00401-020-02196-w
21. Kametani F, Hasegawa M. Reconsideration of amyloid hypothesis and tau hypothesis in Alzheimer’s disease. Front Neurosci. (2018) 12:25. doi: 10.3389/fnins.2018.00025
22. Edison P, Archer HA, Hinz R, Hammers A, Pavese N, Tai YF, et al. Amyloid, hypometabolism, and cognition in Alzheimer disease: an [11C]PIB and [18F]FDG PET study. Neurology. (2007) 68:501–8. doi: 10.1212/01.wnl.0000244749.20056.d4
23. de Paula VDJR, Guimarães FM, Diniz BS, Forlenza OV. Neurobiological pathways to Alzheimer’s disease: amyloid-beta, TAU protein or both? Dement Neuropsychol. (2009) 3:188–94. doi: 10.1590/S1980-57642009DN30300003
24. Kinney JW, Bemiller SM, Murtishaw AS, Leisgang AM, Salazar AM, Lamb BT. Inflammation as a central mechanism in Alzheimer’s disease. Alzheimers Dement N Y N. (2018) 4:575–90. doi: 10.1016/j.trci.2018.06.014
25. McGeer PL, McGeer EG. The amyloid cascade-inflammatory hypothesis of Alzheimer disease: implications for therapy. Acta Neuropathol (Berl). (2013) 126:479–97. doi: 10.1007/s00401-013-1177-7
26. Kamer AR, Craig RG, Dasanayake AP, Brys M, Glodzik-Sobanska L, de Leon MJ. Inflammation and Alzheimer’s disease: possible role of periodontal diseases. Alzheimers Dement J Alzheimers Assoc. (2008) 4:242–50. doi: 10.1016/j.jalz.2007.08.004
27. Rocca J-P, Fornaini C, Wang Z, Tan L, Merigo E. Focal infection and periodontitis: a narrative report and new possible approaches. Int J Microbiol. (2020) 2020:8875612. doi: 10.1155/2020/8875612
28. Naruishi K. Carotenoids and periodontal infection. Nutrients. (2020) 12:269. doi: 10.3390/nu12010269
29. Han YW, Houcken W, Loos BG, Schenkein HA, Tezal M. Periodontal disease, atherosclerosis, adverse pregnancy outcomes, and head-and-neck cancer. Adv Dent Res. (2014) 26:47–55. doi: 10.1177/0022034514528334
30. Mattila KJ, Pussinen PJ, Paju S. Dental infections and cardiovascular diseases: a review. J Periodontol. (2005) 76:2085–8. doi: 10.1902/jop.2005.76.11-S.2085
31. López NJ, Chamorro A, Llancaqueo M. Association between atherosclerosis and periodontitis. Rev Médica Chile. (2011) 139:717–24. doi: 10.4067/S0034-98872011000600004
32. Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. (2006) 33:401–7. doi: 10.1111/j.1600-051X.2006.00924.x
33. Fajardo Puig ME, Rodríguez Reyes O, Hernández Cunill M, Mora Pacheco N. Diabetes mellitus and periodontal disease: current pathophysiological aspects of their relationship. MEDISAN. (2016) 20:845–50.
34. Harach T, Marungruang N, Duthilleul N, Cheatham V, Mc Coy KD, Frisoni G, et al. Reduction of abeta amyloid pathology in APPPS1 transgenic mice in the absence of gut microbiota. Sci Rep. (2017) 7:41802. doi: 10.1038/srep41802
35. Peirce JM, Alviña K. The role of inflammation and the gut microbiome in depression and anxiety. J Neurosci Res. (2019) 97:1223–41. doi: 10.1002/jnr.24476
36. Kamer AR, Pirraglia E, Tsui W, Rusinek H, Vallabhajosula S, Mosconi L, et al. Periodontal disease associates with higher brain amyloid load in normal elderly. Neurobiol Aging. (2015) 36(2):627–33. doi: 10.1016/j.neurobiolaging.2014.10.038
37. Qi X, Zhu Z, Plassman BL, Wu B. Dose-Response meta-analysis on tooth loss with the risk of cognitive impairment and dementia. J Am Med Dir Assoc. (2021) 22:2039–45. doi: 10.1016/j.jamda.2021.05.009
38. Dioguardi M, Gioia GD, Caloro GA, Capocasale G, Zhurakivska K, Troiano G, et al. The association between tooth loss and Alzheimer’s disease: a systematic review with meta-analysis of case control studies. Dent J. (2019) 7:49. doi: 10.3390/dj7020049
39. Costa MJF, de Araújo IDT, da Rocha Alves L, da Silva RL, dos Santos Calderon P, Borges BCD, et al. Relationship of Porphyromonas gingivalis and Alzheimer’s disease: a systematic review of pre-clinical studies. Clin Oral Investig. (2021) 25:797–806. doi: 10.1007/s00784-020-03764-w
40. Elwishahy A, Antia K, Bhusari S, Ilechukwu NC, Horstick O, Winkler V. Porphyromonas Gingivalis as a risk factor to Alzheimer’s disease: a systematic review. J Alzheimers Dis Rep. (2021) 5:721–32. doi: 10.3233/ADR-200237
41. Hu X, Zhang J, Qiu Y, Liu Z. Periodontal disease and the risk of Alzheimer’s disease and mild cognitive impairment: a systematic review and meta-analysis. Psychogeriatrics. (2021) 21:813–25. doi: 10.1111/psyg.12743
42. Dioguardi M, Crincoli V, Laino L, Alovisi M, Sovereto D, Mastrangelo F, et al. The role of periodontitis and periodontal Bacteria in the onset and progression of Alzheimer’s disease: a systematic review. J Clin Med. (2020) 9:495. doi: 10.3390/jcm9020495
43. Nadim R, Tang J, Dilmohamed A, Yuan S, Wu C, Bakre AT, et al. Influence of periodontal disease on risk of dementia: a systematic literature review and a meta-analysis. Eur J Epidemiol. (2020) 35:821–33. doi: 10.1007/s10654-020-00648-x
44. Dominy SS, Lynch C, Ermini F, Benedyk M, Marczyk A, Konradi A, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. (2019) 5(1):eaau3333. doi: 10.1126/sciadv.aau3333
45. Olsen I, Singhrao SK. Can oral infection be a risk factor for Alzheimer’s disease? J Oral Microbiol. (2015) 7:29143. doi: 10.3402/jom.v7.29143
46. Ju X, Kapellas K, Jamieson LM, Mueller N, Wang X. The association between periodontal disease and dementia: a systematic review and meta-analysis. Dent Oral Biol Craniofacial Res. (2019) 2019:1–11. doi: 10.31487/j.DOBCR.2019.01.005
47. Villar A, Paladini S, Cossatis J. Periodontal disease and Alzheimer’s: insights from a systematic literature network analysis. J Prev Alzheimers Dis. (2024) 11:1148–65. doi: 10.14283/jpad.2024.79
48. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Br Med J. (2015) 350:g7647. doi: 10.1136/bmj.g7647
49. Bougioukas KI, Liakos A, Tsapas A, Ntzani E, Haidich A-B. Preferred reporting items for overviews of systematic reviews including harms checklist: a pilot tool to be used for balanced reporting of benefits and harms. J Clin Epidemiol. (2018) 93:9–24. doi: 10.1016/j.jclinepi.2017.10.002
50. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Br Med J. (2017) 358:j4008. doi: 10.1136/bmj.j4008
51. Raymundo MLB, da Silva RO, de Araújo ECF, de Lucena EHG, Cavalcanti YW. Is the history of periodontal disease a risk factor for cognitive decline? systematic review and meta-analysis. Res Soc Dev. (2022) 11:e15811527931. doi: 10.33448/rsd-v11i5.27931
52. Fu Y-D, Li C-L, Hu C-L, Pei M-D, Cai W-Y, Li Y-Q, et al. Meta analysis of the correlation between periodontal health and cognitive impairment in the older population. J Prev Alzheimers Dis. (2024) 11:1307–15. doi: 10.14283/jpad.2024.87
53. Li L, Zhang Q, Yang D, Yang S, Zhao Y, Jiang M, et al. Tooth loss and the risk of cognitive decline and dementia: a meta-analysis of cohort studies. Front Neurol. (2023) 14:1103052. doi: 10.3389/fneur.2023.1103052
54. Qiu C, Zhou W, Shi W-T, Song Z-C. Association between periodontitis and Alzheimer disease: a meta analysis. Shanghai Kou Qiang Yi Xue Shanghai J Stomatol. (2020) 29:661–8. doi: 10.19439/j.sjos.2020.06.020
55. Kaliamoorthy S, Nagarajan M, Sethuraman V, Jayavel K, Lakshmanan V, Palla S. Association of Alzheimer’s disease and periodontitis—a systematic review and meta-analysis of evidence from observational studies. Med Pharm Rep. (2022) 95:144–51. doi: 10.15386/mpr-2278
56. Bouziane A, Lattaf S, Abdallaoui Maan L. Effect of periodontal disease on Alzheimer’s disease: a systematic review. Cureus. (2023) 15:e46311. doi: 10.7759/cureus.46311
57. Dziedzic A. Is periodontitis associated with age-related cognitive impairment? The systematic review, confounders assessment and meta-analysis of clinical studies. Int J Mol Sci. (2022) 23:15320. doi: 10.3390/ijms232315320
58. Kim D-H, Han GS. Periodontitis as a risk factor for dementia: a systematic review and meta-analysis. J Evid-Based Dent Pract. (2025) 25:102094. doi: 10.1016/j.jebdp.2025.102094
59. Nascimento GG, Leite FRM, Mesquita CM, Vidigal MTC, Borges GH, Paranhos LR. Confounding in observational studies evaluating the association between Alzheimer’s disease and periodontal disease: a systematic review. Heliyon. (2023) 9:e15402. doi: 10.1016/j.heliyon.2023.e15402
60. Melo A, Flores-Fraile J, Lo Giudice R, Marchetti E, Nart J, Greethurst AR, et al. Association between Alzheimer’s disease and periodontal inflammatory parameters: a systematic review. J Clin Exp Dent. (2025) 17(3):e310–23. doi: 10.4317/jced.62519
61. Leira Y, Domínguez C, Seoane J, Seoane-Romero J, Pías-Peleteiro JM, Takkouche B, et al. Is periodontal disease associated with Alzheimer’s disease? A systematic review with meta-analysis. Neuroepidemiology. (2017) 48:21–31. doi: 10.1159/000458411
62. Said-Sadier N, Sayegh B, Farah R, Abbas LA, Dweik R, Tang N, et al. Association between periodontal disease and cognitive impairment in adults. Int J Environ Res Public Health. (2023) 20:4707. doi: 10.3390/ijerph20064707
63. Ab Malik N, Walls AWG. Periodontal health status of people with dementia—a systematic review of case-control studies. Saudi Dent J. (2023) 35:625–40. doi: 10.1016/j.sdentj.2023.06.004
64. Larvin H, Gao C, Kang J, Aggarwal VR, Pavitt S, Wu J. The impact of study factors in the association of periodontal disease and cognitive disorders: systematic review and meta-analysis. Age Ageing. (2023) 52:afad015. doi: 10.1093/ageing/afad015
65. Alvarenga MOP, Frazão DR, de Matos IG, Bittencourt LO, Fagundes NCF, Rösing CK, et al. Is there any association between neurodegenerative diseases and periodontitis? A systematic review. Front Aging Neurosci. (2021) 13:651437. doi: 10.3389/fnagi.2021.651437
66. Nascimento PC, Castro MML, Magno MB, Almeida APCPSC, Fagundes NCF, Maia LC, et al. Association between periodontitis and cognitive impairment in adults: a systematic review. Front Neurol. (2019) 10:323. doi: 10.3389/fneur.2019.00323
67. Lauritano D, Moreo G, Della Vella F, Di Stasio D, Carinci F, Lucchese A, et al. Oral health Status and need for oral care in an aging population: a systematic review. Int J Environ Res Public Health. (2019) 16:4558. doi: 10.3390/ijerph16224558
68. Esene I, Tantengco OAG, Robertson FC, Still ME, Ukachukwu AE, Baticulon RE, et al. A guide to interpreting systematic reviews and meta-analyses in neurosurgery and surgery. Acta Neurochir. (2024) 166:250. doi: 10.1007/s00701-024-06133-8
69. Lu C, Lu T, Ge L, Yang N, Yan P, Yang K. Use of AMSTAR-2 in the methodological assessment of systematic reviews: protocol for a methodological study. Ann Transl Med. (2020) 8:652. doi: 10.21037/atm-20-392a
70. Frisoni GB, Altomare D, Ribaldi F, Villain N, Brayne C, Mukadam N, et al. Dementia prevention in memory clinics: recommendations from the European task force for brain health services. Lancet Reg Health Eur. (2023) 26:100576. doi: 10.1016/j.lanepe.2022.100576
71. Crous-Bou M, Minguillón C, Gramunt N, Molinuevo JL. Alzheimer’s disease prevention: from risk factors to early intervention. Alzheimers Res Ther. (2017) 9:71. doi: 10.1186/s13195-017-0297-z
72. Moher D. The problem of duplicate systematic reviews. Br Med J. (2013) 347:f5040. doi: 10.1136/bmj.f5040
73. Zhang M, Mi N, Ying Z, Lin X, Jin Y. Advances in the prevention and treatment of Alzheimer’s disease based on oral bacteria. Front Psychiatry. (2023) 14:1291455. doi: 10.3389/fpsyt.2023.1291455
74. Desta NT. Pathophysiological association between periodontal disease and Alzheimer’s disease: importance of periodontal health in the elderly. J Oral Biosci. (2021) 63:351–9. doi: 10.1016/j.job.2021.08.007
75. Plachokova AS, Gjaltema J, Hagens ER, Hashemi Z, Knüppe TB, Kootstra TJ, et al. Periodontitis: a plausible modifiable risk factor for neurodegenerative diseases? A comprehensive review. Int J Mol Sci. (2024) 25:4504. doi: 10.3390/ijms25084504
76. Maitre Y, Mahalli R, Micheneau P, Delpierre A, Amador G, Denis F. Evidence and therapeutic perspectives in the relationship between the oral microbiome and Alzheimer’s disease: a systematic review. Int J Environ Res Public Health. (2021) 18:11157. doi: 10.3390/ijerph182111157
77. Jungbauer G, Stähli A, Zhu X, Auber Alberi L, Sculean A, Eick S. Periodontal microorganisms and Alzheimer disease–A causative relationship? Periodontol 2000. (2022) 89:59–82. doi: 10.1111/prd.12429
78. Manap AS A, Almadodi R, Sultana S, Sebastian MG, Kavani KS, Lyenouq VE, et al. Alzheimer’s disease: a review on the current trends of the effective diagnosis and therapeutics. Front Aging Neurosci. (2024) 16:1429211. doi: 10.3389/fnagi.2024.1429211
Keywords: Alzheimer's disease, periodontal disease, tooth loss, periodontitis, review
Citation: Arbildo-Vega HI, Cruzado-Oliva FH, Coronel-Zubiate FT, Aguirre-Ipenza R, Meza-Málaga JM, Luján-Valencia SA, Luján-Urviola E, Echevarria-Goche A, Farje-Gallardo CA, Castillo-Cornock TB, Serquen-Olano K, Padilla-Cáceres T and Caballero-Apaza L (2025) Association between periodontal disease and Alzheimer's disease: umbrella review. Front. Dent. Med. 6:1635200. doi: 10.3389/fdmed.2025.1635200
Received: 26 May 2025; Accepted: 23 June 2025;
Published: 9 July 2025.
Edited by:
Deepa Ponnaiyan, SRM Dental College, IndiaReviewed by:
Sruthy Prathap, Yenepoya University, IndiaDivya Shree Pandian, Karpaga Vinayaga Institute of Dental Sciences, India
Copyright: © 2025 Arbildo-Vega, Cruzado-Oliva, Coronel-Zubiate, Aguirre-Ipenza, Meza-Málaga, Luján-Valencia, Luján-Urviola, Echevarria-Goche, Farje-Gallardo, Castillo-Cornock, Serquen-Olano, Padilla-Cáceres and Caballero-Apaza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Franz Tito Coronel-Zubiate, ZnJhbnouY29yb25lbEB1bnRybS5lZHUucGU=