 Michaël R. Laurent1,2*
Michaël R. Laurent1,2* Stefan Goemaere3
Stefan Goemaere3 Charlotte Verroken3,4Pierre Bergmann5Jean-Jacques Body6Olivier Bruyère7
Charlotte Verroken3,4Pierre Bergmann5Jean-Jacques Body6Olivier Bruyère7 Etienne Cavalier8Serge Rozenberg9Bruno Lapauw3,4
Etienne Cavalier8Serge Rozenberg9Bruno Lapauw3,4 Evelien Gielen1,10
Evelien Gielen1,10- 1Centre for Metabolic Bone Diseases, Department of Geriatrics, University Hospitals Leuven, Leuven, Belgium
- 2Department of Geriatrics, Imelda Hospital, Bonheiden, Belgium
- 3Unit for Osteoporosis and Metabolic Bone Diseases, Ghent University Hospital, Ghent, Belgium
- 4Department of Endocrinology and Metabolism, Ghent University Hospital, Ghent, Belgium
- 5Department of Nuclear Medicine, CHU Brugmann, Université Libre de Bruxelles, Brussels, Belgium
- 6Department of Medicine, CHU Brugmann, Université Libre de Bruxelles, Brussels, Belgium
- 7WHO Collaborating Center for Public Health Aspects of Musculoskeletal Health and Ageing, Division of Public Health, Epidemiology and Health Economics, University of Liège, Liège, Belgium
- 8Department of Clinical Chemistry, University of Liège, CHU de Liège, Liège, Belgium
- 9Department of Gynaecology and Obstetrics, Université Libre de Bruxelles, Brussels, Belgium
- 10Gerontology and Geriatrics section, Department of Public Health and Primary Care, University Hospitals Leuven and KU Leuven, Leuven, Belgium
Glucocorticoids are effective immunomodulatory drugs used for many inflammatory disorders as well as in transplant recipients. However, both iatrogenic and endogenous glucocorticoid excess are also associated with several side effects including an increased risk of osteoporosis and fractures. Glucocorticoid-induced osteoporosis (GIOP) is a common secondary cause of osteoporosis in adults. Despite availability of clear evidence and international guidelines for the prevention of GIOP, a large treatment gap remains. In this narrative review, the Belgian Bone Club (BBC) updates its 2006 consensus recommendations for the prevention and treatment of GIOP in adults. The pathophysiology of GIOP is multifactorial. The BBC strongly advises non-pharmacological measures including physical exercise, smoking cessation and avoidance of alcohol abuse in all adults at risk for osteoporosis. Glucocorticoids are associated with impaired intestinal calcium absorption; the BBC therefore strongly recommend sufficient calcium intake and avoidance of vitamin D deficiency. We recommend assessment of fracture risk, taking age, sex, menopausal status, prior fractures, glucocorticoid dose, other clinical risk factors and bone mineral density into account. Placebo-controlled randomized controlled trials have demonstrated the efficacy of alendronate, risedronate, zoledronate, denosumab and teriparatide in GIOP. We suggest monitoring by dual-energy X-ray absorptiometry (DXA) and vertebral fracture identification one year after glucocorticoid initiation. The trabecular bone score might be considered during DXA monitoring. Extended femur scans might be considered at the time of DXA imaging in glucocorticoid users on long-term (≥ 3 years) antiresorptive therapy. Bone turnover markers may be considered for monitoring treatment with anti-resorptive or osteoanabolic drugs in GIOP. Although the pathophysiology of solid organ and hematopoietic stem cell transplantation-induced osteoporosis extends beyond GIOP alone, the BBC recommends similar evaluation, prevention, treatment and follow-up principles in these patients. Efforts to close the treatment gap in GIOP and implement available effective fracture prevention strategies into clinical practice in primary, secondary and tertiary care are urgently needed.
1 Introduction
Glucocorticoids are a group of endogenous hormones and/or drugs, which act mostly through the glucocorticoid receptor to exert anti-inflammatory, immunosuppressive, anti-proliferative and vasoconstrictive effects. Glucocorticoids are widely used for the treatment of acute and chronic inflammatory conditions, for the treatment of lymphoproliferative diseases, to alleviate side effects of chemotherapy or radiotherapy and to prevent rejection of organ transplants. Glucocorticoids are also used chronically as replacement therapy in patients with adrenal insufficiency.
About 1% of the adult population uses glucocorticoids chronically, particularly older adults (1). In large observational studies, ~3 % of post-menopausal women and older men were currently taking oral glucocorticoids (2, 3).
Chronic glucocorticoid excess increases the risk of adverse effects including both early and progressive bone loss, resulting in osteoporosis and increased risk of fractures. This also applies to endogenous or iatrogenic hypercortisolism in patients with Cushing’s syndrome, in whom side effects may be reverted upon curative treatment or dose reduction, respectively (4).
Glucocorticoid-induced osteoporosis (GIOP) is the most common drug-induced cause of secondary osteoporosis. In patients starting glucocorticoids, there is a rapid phase of bone loss (6-12% decline in lumbar spine bone mineral density [BMD] in the first year), followed by a slower but continuous decline thereafter (5, 6). This bone loss is most pronounced in regions of the skeleton with abundant trabecular bone, such as the lumbar spine (5, 7). Although vertebral fractures are particularly characteristic of GIOP (five-fold higher risk in high-dose glucocorticoid users), the risk of non-vertebral and hip fractures is also increased by ~65% and ~130%, respectively (8, 9). Glucocorticoid initiators have an annual incidence of ~5% for vertebral fractures and ~2.5% for non-vertebral fractures, while the risk of both types of fractures is about ~3% annually in chronic users (6). These findings suggest that glucocorticoid initiators are at imminent vertebral fracture risk (6). The economic burden of GIOP remains poorly characterized though it is likely substantial (10, 11).
Fracture risk increases early after initiation of glucocorticoid therapy (within the first three to six months), usually even before a substantial loss of BMD has become apparent (12). When glucocorticoids are discontinued, BMD may return towards baseline levels, while fracture risk decreases after ~1 year (5, 9, 12). Following glucocorticoid discontinuation BMD may only recover partially, depending on e.g. the underlying disease or the menopausal status in women. Fractures in GIOP occur at higher BMD than in postmenopausal osteoporosis (13). While some studies suggest that (current) daily glucocorticoid dose is the main determinant of fracture risk (14) others suggest that high cumulative doses (>1 g prednisolone equivalent) are an independent risk factor (9, 15). In long-term glucocorticoid users, the prevalence of fractures amounts to 30-50% (13). Also in endogenous Cushing syndrome, duration and severity of hypercortisolism has been associated with osteoporosis severity and fracture risk (16, 17).
The pathophysiology of GIOP is complex and consists of both direct effects on bone cells (osteoblasts, osteoclasts and osteocytes) and indirect effects through suppression of the somatotropic and gonadotropic axes, reduced intestinal calcium absorption and glucocorticoid-induced myopathy and cataracts, which increase the risk of falls (13). Glucocorticoids promote osteoclastogenesis and the survival of osteoclasts, stimulate adipogenesis, inhibit osteoblastogenesis and induce apoptosis of osteoblasts and osteocytes (13) in part via suppression of Wnt agonists (18) and upregulation of Wnt signaling inhibitors such as sclerostin and Dkk1 (19). Not only does this lead to reduced bone mass, they may also affect the unmineralized bone matrix, which may partly explain their BMD-independent effects (20, 21). Recent preclinical studies additionally show that glucocorticoid excess also disrupts the intestinal microbiota (18) endogenous biological rhythm of glucocorticoids, which may contribute to the detrimental effects on bone (22).
Glucocorticoids are prescribed for inflammatory or other conditions which themselves predispose to osteoporosis (23, 24). Therefore, fracture risk in glucocorticoid users may be drug-induced, related to the underlying disease, or both. In rheumatoid arthritis (RA) for example, patients requiring glucocorticoids have slightly lower spine and hip BMD than non-glucocorticoid users. About one-third of glucocorticoid-treated RA patients have osteoporotic BMD T-scores, and their prevalence of vertebral fractures is 6-20% (7). Still, in patients with early and active RA, meta-analyses of randomized controlled trials (RCTs) show no significant difference in BMD between glucocorticoid and placebo users through 24 months, suggesting that the positive effects on inflammation may counterbalance the direct adverse skeletal effects of glucocorticoids (25, 26). Cumulative glucocorticoid exposure also contributes to osteoporosis in systemic lupus erythematosus (27, 28), and psoriatic arthritis (29). Inflammatory bowel disease (IBD) itself is associated with lower BMD (30) but glucocorticoid use in IBD patients has been associated with an increased risk of vertebral fractures (31) as well as hip fracture in older IBD patients (32). Meta-analyses show that bisphosphonates prevent bone loss and vertebral fractures in patients with rheumatic diseases (33) (34) and IBD (35) but evidence in other chronic inflammatory conditions remains more limited.
Dosage of systemic exposure and duration of glucocorticoid treatment, but also age, low body mass index (BMI), underlying disease and low BMD are risk factors for glucocorticoid-induced fractures. Traditional clinical risk factors, such as previous fractures, family history of fractures, smoking, alcohol consumption and frequent falls independently contribute to fracture risk in persons taking glucocorticoids (36). The longer and the higher the glucocorticoid dose, the higher the risk of fractures. However, even long-term glucocorticoid doses < 5 mg prednisolone equivalent/day are associated with bone loss and fractures (8, 9). Repeated glucocorticoid courses also result in considerable cumulative exposure in older adults with asthma and chronic obstructive pulmonary disease (COPD), which contributes to the increased risk of osteoporosis and vertebral fractures in these conditions (9) (37–40).
Glucocorticoid exposure in children might impair peak bone mass and increase the risk of fractures later in life (41) although pediatric GIOP is outside the scope of this review. Osteoporosis in children and younger adults has been reviewed elsewhere (42).
The aim of this work is to provide up-to-date evidence-based recommendations for the prevention and treatment of GIOP in adults, building on our previous guidelines (43, 44). Since our previous recommendation from 2006, many relevant studies have been published and new treatments have become available (zoledronate, teriparatide, denosumab), while other recommendations covered drugs that are no longer recommended or available in Belgium (e.g. calcitonin, etidronate). The target audience are health professionals caring for adults at risk of GIOP, particularly in Belgium (although our work may be of interest for practitioners in other countries too). Of note, whereas some regulators distinguish between prevention of GIOP and treatment of (established) GIOP, we will not maintain this distinction and use both terms interchangeably, because we believe this distinction may be somewhat arbitrary and is not useful in clinical practice.
2 Materials and Methods
In order to obtain the best available evidence, the authors searched PubMed from 2005 (when our previous consensus recommendations were written (43) to March 31st, 2022 for existing systematic reviews and meta-analyses of RCTs or observational human studies to inform all different aspects of GIOP prevention and treatment. In case multiple meta-analyses were available, we gave priority to network meta-analyses and meta-analyses that included the most recent studies. However, a preliminary search showed that a recent meta-analysis was lacking for several subtopics. When a recent meta-analysis was unavailable, evidence prior to 2005 was also considered, and we searched for published RCTs or relevant observational human studies, depending upon the research question.
The inclusion criteria were defined in terms of PICOS (44): population, intervention, comparator, outcome and study type. The population was defined as glucocorticoid-treated adults. Each guideline subtopic (e.g. calcium and/or vitamin D, monitoring, exercise etc.) was considered as an intervention. Interventions (e.g. drugs) not available in Belgium, studies in children, or meta-analyses focusing exclusively on different populations (e.g. Asian countries) were excluded. Placebo, open-label or active-controlled comparators were allowed. Priority was given to fracture outcomes and falls, but in their absence, BMD and biochemical parameters were also included.
Keywords in our search included “glucocorticoids”, “steroid-induced” or “corticosteroids”, “osteoporosis”, “fracture” or (“bone” AND “density”), and keywords related to each of the subtopics of this consensus document. We also searched for guidelines from other scientific societies, and extracted relevant systematic review, meta-analyses, RCTs or observational studies from the reference lists. Finally, each of the authors was allowed to provide additional references.
We used the simplified GRADE system to indicate the strength of recommendations and the quality of the supporting evidence (Table 1) (45).
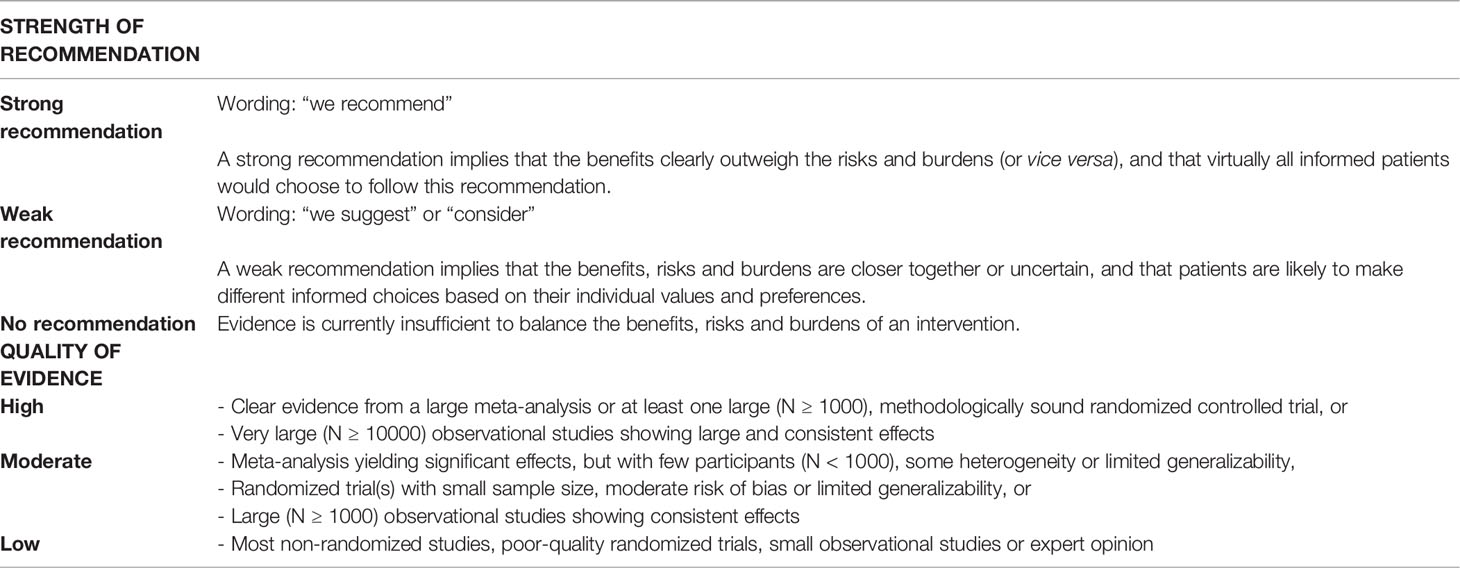
Table 1 Simplified GRADE approach.
The Belgian Bone Club (BBC) is a multidisciplinary national scientific society established in 1987, devoted to promoting understanding of bone disorders in general and osteoporosis in particular. All co-authors were asked to review and shape recommendations pertaining to one particular subtopic, but all co-authors revised the different subtopics in consecutive revisions. Furthermore, all authors discussed and unanimously agreed upon the grading of the recommendations and the assessment of the quality of the supporting evidence. Following keynote lectures on clinical trials and guidelines by two international experts, these recommendations were presented to membership at the 2021 BBC Clinical Update Symposium and refined further after plenary discussions.
3 Results
More than 150 systematic reviews and meta-analyses were identified and included in this work. Ten strong and ten weak recommendations were formulated, based on high quality (2 recommendations), moderate quality (7 recommendations) or low quality evidence (11 recommendations). The different subtopics of this review and their corresponding recommendations (with the strength of the recommendation and quality assessment of the underlying evidence), are summarized in Table 2 and discussed below in more detail.
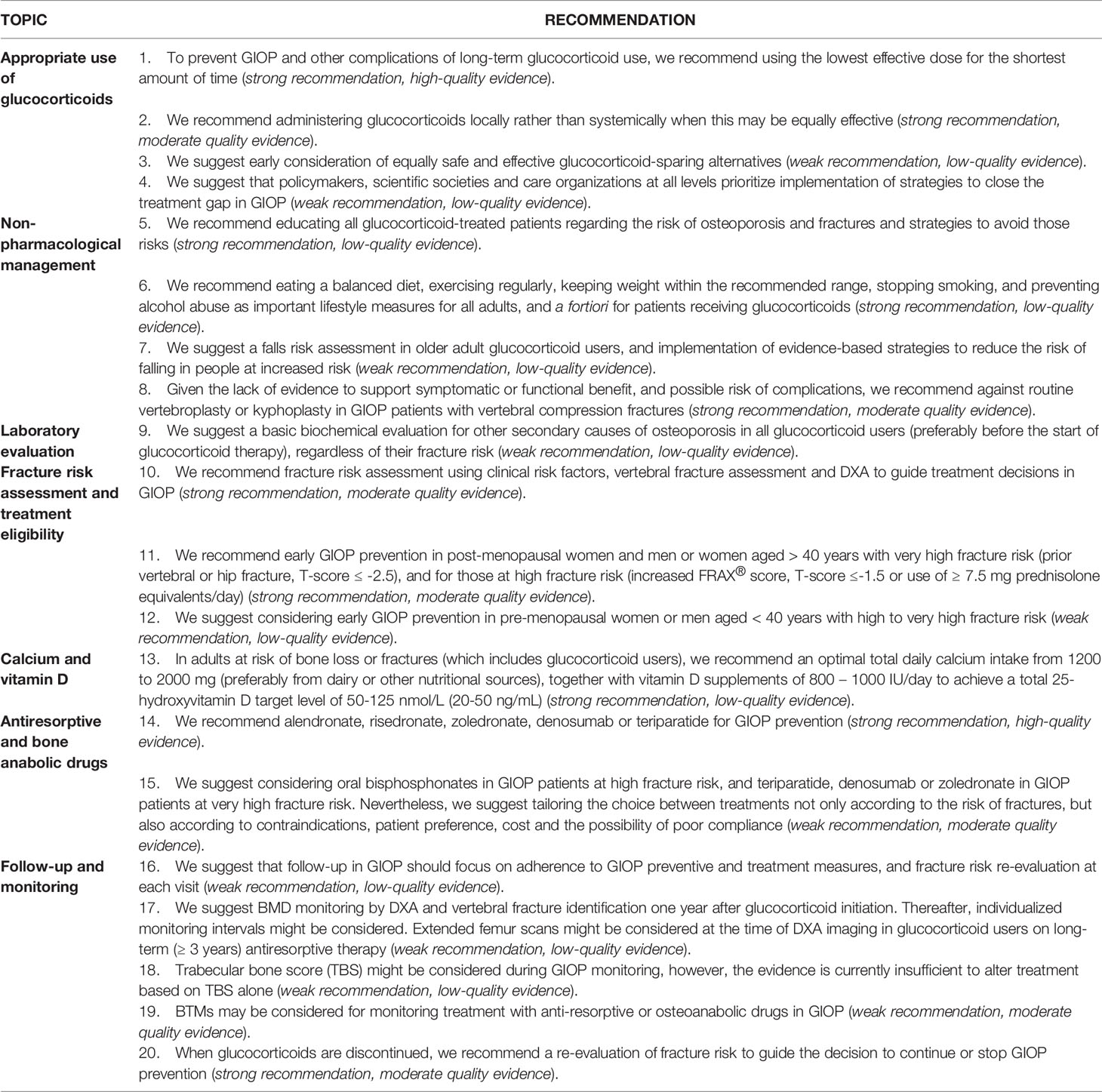
Table 2 Summary of the BBC recommendations for GIOP in adults.
3.1 Appropriate Use of Glucocorticoids
● Recommendation 1: To prevent GIOP and other complications of long-term glucocorticoid use, we recommend using the lowest effective dose for the shortest amount of time (strong recommendation, high-quality evidence).
Meta-analyses of RCTs and very large observational studies consistently show that the association of glucocorticoid excess with fractures, BMD decline and increased bone turnover is dose- and duration-dependent, while tapering or stopping glucocorticoids reduces these risks (5, 9, 12, 15, 46, 47). Moreover, high-dose glucocorticoids may result in less fracture risk when given in short course rather than chronically (15, 48). In COPD for example, shorter glucocorticoid pulses are nowadays preferred over longer courses, due to similar effectiveness and the possibility of less cumulative toxicity (49). Glucocorticoid stewardship in general involves prescribing the lowest effective dose for the shortest possible time (50).
Prolonged courses of high glucocorticoid doses remain a cornerstone of therapy in many conditions e.g. RA, polymyalgia rheumatica/giant cell arteritis, or immune-mediated hemolytic anemia/thrombocytopenia. Some of these patients are considered glucocorticoid-dependent but can still be tapered after prolonged follow-up. Others may suffer tertiary adrenal insufficiency, which may also be amenable to slow glucocorticoid weaning. In some progressive conditions such as Duchenne muscular dystrophy, glucocorticoids are the standard of care, although they contribute to the high fracture burden in these younger patients (51). Despite the necessity for prolonged glucocorticoid usage in these conditions, attention to GIOP prevention remains poor, particularly in hematological conditions such as immune thrombocytopenia, autoimmune hemolytic anemias or lymphomas (52–54).
There is reassuring evidence that long-term low-dose hydrocortisone replacement therapy in Addison’s disease is safe (55). However, glucocorticoid doses are often above the physiological range in patients with adrenal insufficiency (46) and fractures rates appear to be increased in this context (56). The use of prednisone, prednisolone or dexamethasone rather than hydrocortisone, or higher hydrocortisone doses, have been associated with lower BMD, although the available evidence is scant and heterogeneous (55) (57–59). There is also low-quality evidence that primary hyperaldosteronism might increase the risk of GIOP (60, 61).
● Recommendation 2: We recommend administering glucocorticoids locally rather than systemically when this may be equally effective (strong recommendation, moderate quality evidence).
Local glucocorticoid therapy remains an underused yet feasible strategy in dermatological conditions, respiratory diseases (intranasal or inhaled corticosteroids), acute non-infectious mono-arthritis (intra-articular injection) or IBD (delayed-release oral formulations). Nevertheless, some systemic glucocorticoid exposure remains with all of these routes, which are associated with a non-negligible risk of GIOP in chronic users, mainly at high doses (47) (62–64).
Systemic glucocorticoids increase the risk of GIOP and fractures in asthma, while the effect of high doses of inhaled corticosteroids remains equivocal (24) (65, 66). In COPD, a meta-analysis of RCTs and observational studies showed that inhalation corticosteroids are associated with a significant but modest dose-dependent increase in fracture risk (67) although RCTs alone show no clear effect on BMD (68). High-dose cumulative corticosteroid exposure from epidural injections is associated with lower BMD and increased vertebral fracture risk, particularly in post-menopausal women not receiving concomitant anti-osteoporosis medication (69). In early active RA, one RCT showed that intra-articular glucocorticoids were associated with bone loss, which could be prevented by alendronate (70). Glucocorticoid-naïve Crohn’s disease patients showed less bone loss with oral budesonide (which is available as a delayed release formulation and has extensive first-pass hepatic metabolism) than with prednisolone in one RCT (71). However, this may be associated with lower efficacy (72) and budesonide showed some evidence of bone loss in primary biliary cirrhosis (73). A recent nationwide retrospective cohort study showed that potent topical corticosteroids also slightly increase the risk of osteoporotic fractures (64) but whether this risk is lower than for oral glucocorticoids remains unknown. For other routes of administration however, the risk of GIOP remains poorly defined (74). Local administration may carry a risk of local side-effects e.g. joint infection in case of breached injection sterility. Therefore, the benefits and risks of local vs. systemic glucocorticoids need to be carefully balanced according to the needs and the preferences of each specific patient.
● Recommendation 3: We suggest early consideration of equally safe and effective glucocorticoid-sparing alternatives (weak recommendation, low-quality evidence).
Glucocorticoid-sparing regimens are increasingly popular in organ transplantation (75) psoriasis, IBD and rheumatological conditions. In general, however, high-quality evidence that glucocorticoid-sparing therapies reduce fracture risk in these patients remains lacking (76). In a meta-analysis in RA patients, tumor necrosis factor inhibitors showed no significant effect on hip and spine BMD compared to placebo, whereas glucocorticoids impaired spine BMD compared to placebo (26). Direct comparisons remain however missing.
Alternative immunosuppressants also have side effects, and it is often easier, more evidence-based and cheaper to apply GIOP prevention or treatment rather than switching to biologicals solely because of osteoporosis risk. Cyclosporine and tacrolimus are also associated with bone loss, while azathioprine and mycophenolic acid are not (20). Methotrexate is only very rarely associated with osteopathy, mainly at excessive doses or due to drug interactions (77). While the mammalian target of rapamycin (mTOR) pathway plays an important role in bone metabolism, the clinical effects of mTOR inhibitors on osteoporosis or fracture risk remain poorly understood (20).
● Recommendation 4: We suggest that policymakers, scientific societies and care organizations at all levels prioritize implementation of strategies to close the treatment gap in GIOP (weak recommendation, low-quality evidence).
Despite the frequency and the severe complications of GIOP, and the existence of clear guidelines and evidence-based fracture reduction strategies, considerable underdiagnosis and undertreatment of GIOP remains (78). A systematic review of observational studies showed that < 40% of chronic glucocorticoid users received BMD testing or osteoporosis medications (79). Although the use of bisphosphonates in GIOP has increased since their introduction, there is little evidence of improvement in GIOP prevention over time (80). Although there is strong evidence of a treatment gap in GIOP, the strength of the recommendation was judged “weak” because of a lack of strategies with demonstrated efficacy to close the gap.
One RCT showed that pharmacist feedback did not increase the uptake of bisphosphonates for GIOP prevention. Although a beneficial effect was observed in the subgroups of men and patients ≥ 70 years, the prescription rate in these populations still only increased from 5% in the control group to 13% in the intervention group (81). Similar RCTs of pharmacist-led interventions confirm positive trends but with a very large remaining treatment gap (82, 83). Nevertheless, system-based and electronic medical record-based interventions (84) may be more successful than patient or provider education alone (85). Some studies have reported improved compliance with GIOP guidelines following a multidisciplinary quality improvement initiative (86, 87). However, another trial of a web-based quality improvement program found no significant effect (88). One systematic review found that no GIOP care quality improvement interventions produced robust changes, with overall adherence remaining low (85).
Notably, implementation of multifaceted interventions to improve GIOP prevention might be cost-effective if they succeed in promoting uptake of generic bisphosphonates in a large proportion of high-risk patients (89). Barriers in fracture prevention include cost of therapy, time and cost required for diagnosis, concerns about medication side-effects, and lack of clarity regarding the responsibility to undertake GIOP prevention (90). We believe GIOP prevention is the responsibility of every physician prescribing glucocorticoids. In case of doubt however, asking advice from, or referring to a specialist in osteoporosis is encouraged.
3.2 Non-Pharmacological Management
● Recommendation 5: We recommend educating all glucocorticoid-treated patients regarding the risk of osteoporosis and fractures and strategies to avoid those risks (strong recommendation, low-quality evidence).
In line with the BBC guidelines on post-menopausal osteoporosis (44), we highly recommend patient education as likely being beneficial from a patient perspective, although there is no direct supporting evidence. A discussion on GIOP is particularly advised with long-term (≥ 3 months) glucocorticoid users, while reassurance may be offered to short-term (< 3 months), low-dose (< 5 mg/day) users at low fracture risk. Patients can be reassured that osteoporosis is generally not a contraindication for glucocorticoid therapy if they have an evidence-based indication for such a therapy, provided that the risk of GIOP is systematically assessed and appropriately treated.
● Recommendation 6: We recommend eating a healthy diet, exercising regularly, keeping weight within the recommended range, stopping smoking, and preventing alcohol abuse as important lifestyle measures for all adults, and a fortiori for patients receiving glucocorticoids (strong recommendation, low-quality evidence).
● Recommendation 7: We suggest a falls risk assessment in older adult glucocorticoid users, and implementation of evidence-based strategies to reduce the risk of falling in people at increased risk (weak recommendation, low-quality evidence).
Our previous GIOP guidelines recommended that non-pharmacological treatment (primarily nutrition and exercise) should be considered (43). More than fifteen years later, most international GIOP guidelines still recommend lifestyle as an important general management strategy, despite lack of evidence (91).
Glucocorticoid excess causes detrimental effects not only on bone but also on muscle, cartilage and fat mass, all of which might be mitigated by a healthy diet and regular physical exercise. It should be emphasized, however, that only indirect evidence is available, based on data in postmenopausal osteoporosis or from preclinical or clinical studies of limited quality and quantity in GIOP. Still, a healthy lifestyle has numerous other beneficial effects on health and quality of life. When it comes to physical exercise, the focus should be on body balance, impact training, and strength and resistance training tailored to the needs and abilities of each patient, as recommended by the BBC guidelines on post-menopausal osteoporosis (44).
Glucocorticoids might also increase the risk of falls. In a population with median age 60 years, Van Staa et al. reported that falls incidence increased from 1.6 to 2.8 per 100 person-years in the first 3 months of glucocorticoid use, and decreased to baseline fairly rapidly after discontinuation (8). Clinical trials on fall prevention in glucocorticoid users remain however lacking. We suggest falls risk screening in adults aged 65 years and older, although this is based on expert opinion. Even in adults in midlife, very high glucocorticoid doses may lead to significant muscle atrophy and risk of falls.
Simple assessments are available and recommended to screen for muscle weakness and/or falls risk in GIOP patients. These include identification of clinical risk factors for falls, such as history of falls in the previous year, mobility limitations, visual impairments, neuromuscular diseases, advanced age, polypharmacy and sarcopenia. Clinical assessment of falls risk involves observing gait and mobility, or more formal practical tests such as the sit-to-stand test, four-stage balance test, timed up and go test, gait speed, Tinetti assessment of balance and gait, etc. Multifactorial and exercise interventions have shown greatest promise in reducing falls risk in older adults in general (92).
● Recommendation 8: Given the lack of evidence to support symptomatic or functional benefit, and possible risk of complications, we recommend against routine vertebroplasty or kyphoplasty in GIOP patients with vertebral compression fractures (strong recommendation, moderate quality evidence).
Given the frequency of vertebral compression fractures in GIOP, it is relevant to note that a Cochrane systematic review found high to moderate quality evidence that vertebroplasty has no important benefit in terms of pain, disability or quality of life in routine practice when compared with a sham procedure (93, 94). Furthermore, a systematic review found an increased risk of vertebral fractures following vertebroplasty in patients with low bone mineral density as well as in glucocorticoid users (odds ratio 2.632; 95% CI 1.399 to 4.950) (95). Still, patients with vertebral fractures, particularly with posterior displacement, should be educated regarding and monitored for symptoms of spinal cord compression, and be considered for surgical referral. In individual patients with exceptional pain refractory to optimal analgesia however, referral to a bone specialist might be considered to discuss the potential benefit in terms of pain relief vs. the risk of complications (including additional vertebral fractures).
3.3 Laboratory Evaluation
● Recommendation 9: We suggest a basic biochemical evaluation for other secondary causes of osteoporosis in all glucocorticoid users (preferably before the start of glucocorticoid therapy), regardless of their fracture risk (weak recommendation, low-quality evidence).
We suggest a basic biochemical evaluation, even before the start of glucocorticoids, to inform osteoporosis treatment and to identify possible additional secondary causes of osteoporosis. Suggested basic and optional additional laboratory tests are listed in Table 3 (96). The suggested laboratory investigation is similar as in post-menopausal osteoporosis (44). There are only observational studies reporting on biochemical testing to identify secondary causes of osteoporosis (44). In GIOP specifically, even those studies appeared lacking in our literature search. Additional tests to identify or guide management of other side effects of glucocorticoids (e.g. fasting glucose, hemoglobin A1c, lipid panel, etc.) may simultaneously be considered.
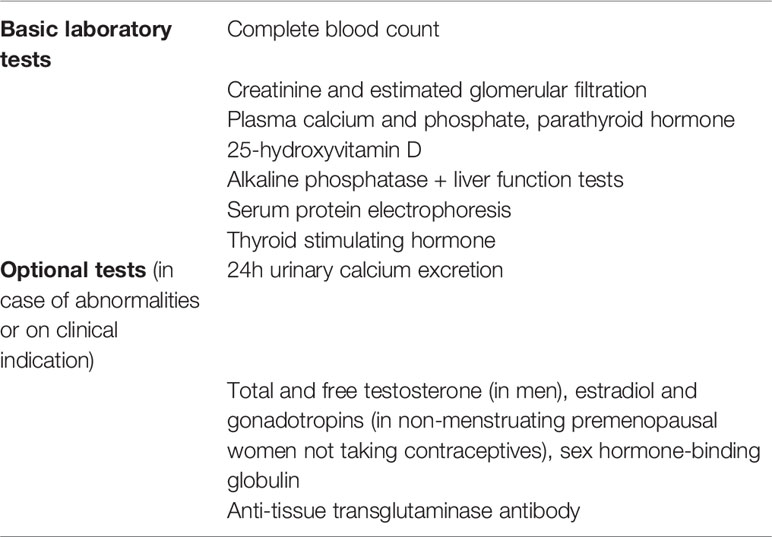
Table 3 Recommended laboratory tests in the evaluation of glucocorticoid-induced osteoporosis.
Currently available circulating biomarkers are not useful to distinguish primary from secondary osteoporosis in general, or to diagnose GIOP in particular. Serum biomarkers may however be useful for osteoporosis treatment monitoring (44). Two bone turnover markers (BTMs), namely procollagen type I N-propeptide (PINP), a bone formation marker, and C-terminal cross-linking telopeptide of collagen (β-CTX), a bone resorption marker, are currently preferred for osteoporosis treatment monitoring (97, 98). One bone formation marker (e.g. P1NP or bone-specific alkaline phosphatase) and one bone resorption marker (e.g. β-CTX or TRAP-5b) can be prescribed per request and are refunded in Belgium, in case of (suspected) metabolic bone disease. Yet, their interpretation is rather difficult due to preanalytical (circadian rhythm, influence of food intake) and analytical factors (lack of standardization). Blood samples should preferably be obtained in the morning in the fasted stated (especially for β-CTX). In patients with renal insufficiency, bone-specific alkaline phosphatase, intact P1NP or TRAP-5b should be preferred over total P1NP or β-CTX. Due to the lack of standardization of β-CTX assays we recommend that patients should be followed by the same laboratory and that laboratories performing bone turnover measurement mention the method used on their results protocols (99, 100). Of note, BTM concentrations increase and may remain elevated up to one year after a fracture. Furthermore, BTMs may be affected not only by initiation of glucocorticoids, but also by the underlying disease (101).
Biomarkers are useful in research to help understand the mechanisms of bone loss in GIOP, and they have been used frequently in clinical trials. The most studied BTM in GIOP is osteocalcin. After initiation of glucocorticoids in healthy volunteers, the bone formation markers osteocalcin and PINP both rapidly decrease (102, 103) and the larger the dose given, the larger the decline (104). Bone resorption markers (such as urinary N-terminal cross-linked telopeptide of type 1 collagen) on the other hand slightly increase in young healthy volunteers (101, 104), suggesting a dissociation between bone formation (decreased) and resorption (increased). In post-menopausal women, bone resorption markers may decrease early after experimental low-dose glucocorticoid administration, likely due to a dominant effect on reduced bone formation (105). Interestingly, osteocalcin concentrations return to baseline levels after glucocorticoid withdrawal. This also seems to be the case in long-term users who discontinue glucocorticoids.
3.4 Fracture Risk Assessment and Treatment Eligibility
● Recommendation 10: We recommend fracture risk assessment using clinical risk factors, vertebral fracture assessment and DXA to guide treatment decisions in GIOP (strong recommendation, moderate quality evidence).
Fracture risk in GIOP is associated with clinical risk factors including advanced age, sex, prior fractures, low BMI, dose and duration of glucocorticoid therapy, falls history as well as other traditional risk factors (3, 9, 12, 36). The absolute fracture incidence in GIOP is higher at older ages, whereas the relative increase due to glucocorticoids may become smaller with advancing age (3). For the same BMD, there is no significant difference in glucocorticoid-induced relative fracture risk between men and women (3). Cost-effectiveness of GIOP treatment improves with higher fracture risk in individual glucocorticoid users (106, 107). RCTs of drugs to prevent or treat GIOP have generally selected participants based on DXA T-scores, prior fracture history, or both. Because GIOP is associated with greater fracture risk than post-menopausal osteoporosis for the same age and BMD, there is a rationale for higher T-score cut-offs for treatment in GIOP (3).
The BBC guidelines on post-menopausal osteoporosis recommend fracture risk assessment using calculators like FRAX® or Garvan (44). FRAX® is the most commonly used tool in Belgium, since calculation of the FRAX® score at the time of bone densitometry is mandated for DXA reimbursement. Previous or current (/anticipated) exposure to ≥ 5 mg prednisolone/day (or equivalent) for 3 months or longer is a BMD-independent fracture risk factor in FRAX® (3), whereas glucocorticoids are not accommodated in the Garvan nomogram.
FRAX® and a number of other algorithms lack the ability to provide estimates for patients < 40 years, while many glucocorticoid users are this young. However, fracture incidence in glucocorticoid users below 40 years is very low (9), and treatment below this age is unlikely to be cost-effective using a short time horizon (106). Another limitation of FRAX® is that use of systemic glucocorticoids is entered as a dichotomous risk factor (yes/no), assuming an average risk. Current and cumulative dose (e.g. from intermittent courses) are not taken into account. Under certain assumptions, formulas to adjust conventional FRAX® estimates of hip and major osteoporotic fracture probabilities according to the glucocorticoid dose have been published (Table 4) (108). Still, clinical judgement should assume even higher risk for very high glucocorticoid doses, even when given for < 3 months duration (109). Of note, national FRAX® models may require recalibration, as recently shown by a large Belgian population-based study (110, 111).
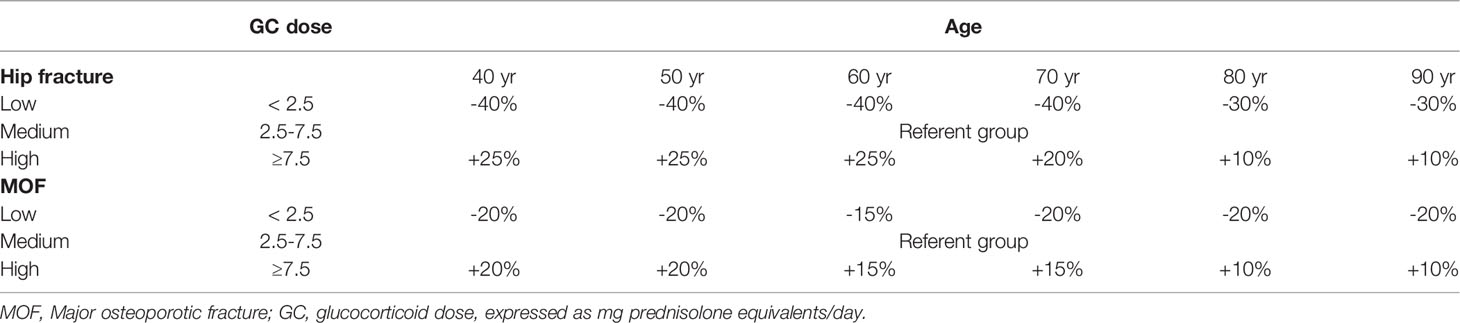
Table 4 Simplified algorithm with percentage adjustment of 10-year probabilities of a hip fracture or a major osteoporotic fracture by age according to dose of glucocorticoids (108).
Both the American College of Rheumatology (ACR) guidelines as well as the International Osteoporosis Foundation (IOF)/European Calcified Tissue Society (ECTS) guidelines on GIOP advise a baseline DXA at the onset of glucocorticoid therapy to better discriminate high-risk from lower-risk patients (91, 96). Vertebral fracture assessment (VFA) at the time of DXA (or spine X-rays) may identify prevalent vertebral fractures, which strongly influences fracture risk and treatment recommendations. The BBC suggests that trabecular bone score (TBS), which can be used to adjust FRAX® scores, may be used to fine-tune baseline and especially follow-up fracture risk assessment (see Section 3.7. below) (112).
In Belgium, parenteral osteoporosis drugs are generally reimbursed only in people with prior radiographic vertebral fractures, hip fractures or DXA T-scores < -2.5 at the lumbar spine or hip. Thus, DXA and spinal X-rays may be used not only for fracture risk assessment, but also for reimbursement purposes, to reduce out-of-pocket expenses for patients. However, initiation of pharmacotherapy e.g. oral bisphosphonates, should not be delayed to obtain a bone densitometry (113). Moreover, in patients with prior vertebral or hip fractures, there may be no need to obtain a DXA, since they often qualify for treatment and reimbursement anyway.
Given that fracture risk increases in GIOP well before any changes are observed on DXA, there is a clear need for additional ways to improve fracture risk assessment in GIOP. High-resolution quantitative computed tomography (114–118) or reference point indentation (119) may be more sensitive that DXA to detect declines in certain bone qualities, although only proof of principle studies are available (120).
● Recommendation 11: We recommend early GIOP prevention in post-menopausal women and men or women aged > 40 years with very high fracture risk (prior vertebral or hip fracture, T-score ≤ -2.5), and for those at high fracture risk (increased FRAX® score, T-score ≤-1.5 or use of ≥ 7.5 mg prednisolone equivalents/day) (strong recommendation, moderate quality evidence).
● Recommendation 12: We suggest considering early GIOP prevention in pre-menopausal women or men aged < 40 years with high to very high fracture risk (weak recommendation, low-quality evidence).
Since fracture risk increases shortly after initiating glucocorticoid therapy, most guidelines emphasize initiation of bone-sparing drugs in eligible patients as early as possible. In general, since prednisolone doses in the range of 2.5-7.5 mg prednisolone are associated with increased fracture risk within 3 months (8, 9) GIOP prevention might be considered in all patients committed or exposed to such glucocorticoid doses. However, as in the general and other clinical populations, patients with the highest risk for fracture are the ones most likely to benefit from non-pharmacological and pharmacological fracture prevention (lowest number needed to treat). Likewise, the cost-effectiveness of GIOP prevention is sensitive to intervention cost, willingness to pay, and fracture risk factors such as older age, lower BMD, higher doses of glucocorticoids and the number of prior fractures (106, 107) (121–124). Thus, despite limitations in our accuracy to predict fracture risk, most guidelines recommend different treatment strategies for patients estimated to be at low, high or very high fracture risk (91). Fracture risk is usually classified in different GIOP guidelines according to DXA T-scores, FRAX® scores, or both (125).
The IOF–ECTS working group on GIOP suggests considering an estimated 10-year fracture risk of 20% as an intervention threshold (96). From a practical point of view, this would imply that virtually all glucocorticoid-treated patients ≥ 70 years and/or with a previous or incident fragility fracture, and all postmenopausal women and men ≥ 50 years on a high dose of glucocorticoids (≥ 7.5 mg prednisolone/day) or with a T-score ≤ -1.5 would be considered eligible for treatment (Table 5) (96). This coincides more or less with cost-effectiveness thresholds, assuming that drugs are similarly effective in GIOP as they are in post-menopausal osteoporosis (123). This framework proposes tailoring recommendations based on country-specific models. Unfortunately, no official willingness to pay threshold exists in Belgium. Our recent national guidelines on post-menopausal osteoporosis suggest a treatment threshold of ≥ 20% for 10-year osteoporotic fracture risk, ≥ 3% for hip fracture risk in individuals aged < 70 years, and ≥ 5% in those aged ≥ 70 years (44). For consistency, we suggest to extend these cut-offs to GIOP in Belgium. We emphasize that the BMD thresholds for the high and very high risk categories in these recommendations pertaining to GIOP, are higher than in our guidelines for postmenopausal osteoporosis (44).
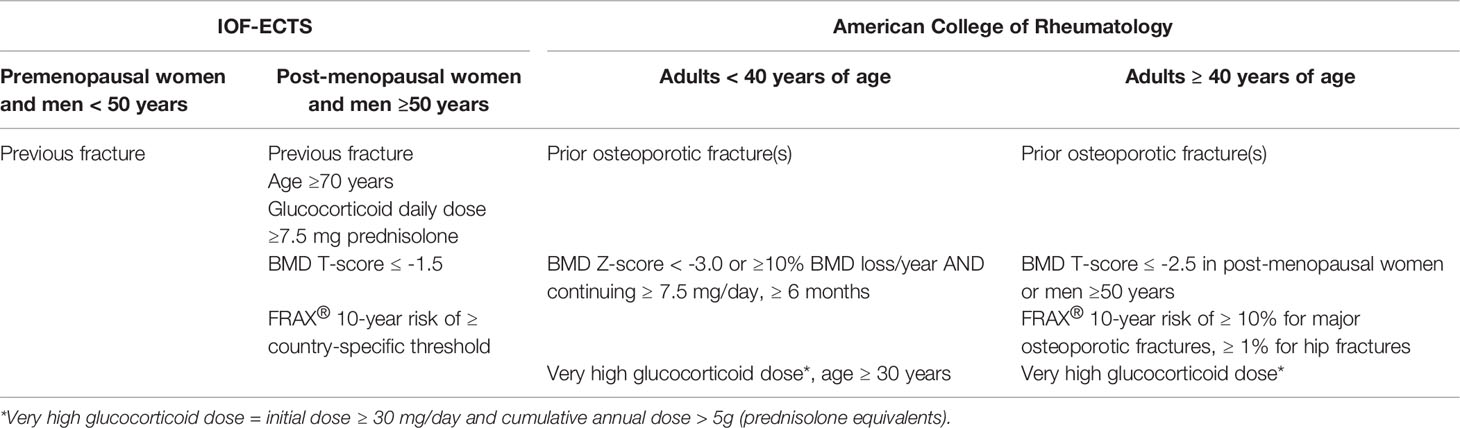
Table 5 Fracture risk groups eligible for bone-sparing drugs in IOF-ECTS (96) and ACR guidelines (91) on GIOP.
More recently, the ACR guidelines (91) suggest three operational fracture risk categories for glucocorticoid-treated patients: low, moderate and high fracture risk (see Table 5). Categorization is determined by patient’s age (< or ≥ 40 years), prior osteoporotic fractures, T-score at the lumbar spine or hip (Z-score if < 40 years), FRAX® score (if ≥ 40 years), and glucocorticoid dose. In the end, there are many similarities between the American and international/European guidelines.
Another important disease and risk modifier to consider is gonadal status, even more as high-dose glucocorticoid therapy will compromise hypothalamic-pituitary-gonadal function in both men and women. Thus, in premenopausal women who become hypogonadal some form of hormone replacement therapy may be considered. In younger men who develop hypogonadism and are symptomatic, testosterone replacement therapy may be considered. However, either hormone therapy should be considered independent of bone health, since there is insufficient evidence to support sex hormone replacement therapy for GIOP prevention alone (126).
In most patients receiving glucocorticoid replacement therapy for adrenal insufficiency, daily glucocorticoid doses are less than the equivalent of 7.5 mg prednisolone but still often supraphysiologic. Moreover, glucocorticoid treatment in patients with primary adrenal insufficiency is lifelong, and in patients with secondary or tertiary adrenal insufficiency, there might have been detrimental musculoskeletal effects of the primary disease or higher initial iatrogenic glucocorticoid doses. As such, despite good evidence, we suggest to apply the same risk categorization and treatment considerations as in other glucocorticoid-treated patients.
Solid organ and bone marrow transplantation are associated with even higher bone loss than GIOP, and high glucocorticoid doses are still often used (127). The pathophysiology of osteoporosis in organ transplantation extends beyond GIOP alone (75). Bisphosphonates have been shown to improve BMD (128–130) and possibly reduce fracture risk in transplant recipients (131), yet the certainty of the evidence is low. Nevertheless, we suggest extending our recommendations for GIOP to glucocorticoid users who are candidates for or recipients of organ transplants (75).
3.5 Calcium and Vitamin D
● Recommendation 13: In adults at risk of bone loss or fractures (which includes glucocorticoid users), we recommend an optimal total daily calcium intake from 1200 to 2000 mg (preferably from dairy or other nutritional sources), together with vitamin D supplements of 800 – 1000 IU/day to achieve a total 25-hydroxyvitamin D target level of 50-125 nmol/L (20-50 ng/mL) (strong recommendation, low-quality evidence).
The pathophysiology of GIOP involves decreased intestinal calcium absorption and increased urinary calcium loss (13). Guidelines in osteoporosis in general and GIOP in particular recommend adequate nutritional calcium intake (preferably from dairy sources) and adequate vitamin D status (44). Supplements of calcium and/or vitamin D should be used if these goals are not met.
Meta-analyses show that bone loss at the lumbar spine, hip and forearm is prevented by calcium and vitamin D supplements in glucocorticoid-treated patients (132). A Cochrane meta-analyses concluded that calcium and vitamin D should therefore be initiated prophylactically in all glucocorticoid users (133). However, evidence on fracture outcomes as well as falls remains lacking, the number of participants in these meta-analyses was very low, different types of vitamin D supplements or analogues were used, and evidence concerning optimal doses or target levels in GIOP remains lacking. Therefore, we judged the quality of evidence to be low.
In analogy to recommendations on post-menopausal osteoporosis, many GIOP guidelines recommend doses of calcium and vitamin D between 1,000 to 1,200 mg/day and 600 to 800 IU/day to achieve 25-hydroxyvitamin D target serum levels, respectively (91). Higher doses are not more effective (except in patients with severe deficiency) and several RCTs suggest that intermittent high-dose vitamin D boluses may even increase the risk of falls, bone loss and fractures (134–136). An upper target level of 125 nmol/L (50 ng/ml) is suggested by the BBC guidelines on post-menopausal osteoporosis (44).
There is moderate quality evidence that active vitamin D analogues maintain BMD and reduce vertebral fracture risk in GIOP, and more so than conventional calcium- and vitamin D supplements (132, 137, 138). However, the use of active vitamin D analogues is not recommended, because bisphosphonates or other bone drugs are more effective (138), and the therapeutic window is narrower than with conventional calcium- and vitamin D-supplements.
Likewise, several small randomized trials with calcifediol have reported increased BMD (139) and lower vertebral fracture risk in GIOP or solid organ transplant recipients (140, 141). Nevertheless, the evidence is insufficient to recommend the routine use of calcifediol, which is more expensive and not necessarily better than cholecalciferol or ergocalciferol in combination with bone drugs such as bisphosphonates.
Calcium- and vitamin D-supplements at excessive doses may be associated with an increased risk of hypercalciuria (142, 143), which is of particular concern in GIOP. Some meta-analyses suggest that calcium supplements are associated with cardiovascular adverse events, although these findings remain quite controversial and unconfirmed by other studies (44). Calcium- and vitamin D supplements are unfortunately not reimbursed in Belgium, even though they may be cost-effective in GIOP (144).
Importantly, calcium- and vitamin D-supplements alone are insufficient in many patients, who require combined therapy with bone-sparing drugs. In randomized trials, GIOP patients receiving calcium with or without vitamin D supplements still lost 1-4% lumbar spine BMD over one year (145, 146). Patients at high to very high fracture risk still more often receive calcium and vitamin D, rather than the combination of bisphosphonates with calcium and vitamin D (147). In other words, calcium- and vitamin D-supplements are useful but should not be an excuse not to prescribe bisphosphonates or other bone-targeted medications (148).
3.6 Antiresorptive and Bone Anabolic Drugs
● Recommendation 14: We recommend alendronate, risedronate, zoledronate, denosumab or teriparatide for GIOP prevention (strong recommendation, high-quality evidence).
● Recommendation 15: We suggest considering oral bisphosphonates in GIOP patients at high fracture risk, and teriparatide, denosumab or zoledronate in GIOP patients at very high fracture risk. Nevertheless, we suggest tailoring the choice between treatments not only according to the risk of fractures, but also according to contraindications, patient preference, cost and the possibility of poor compliance (weak recommendation, moderate quality evidence).
Regulatory approval of drugs to reduce fracture risk in individuals taking glucocorticoids has been based on RCTs showing improvements in BMD. Fractures have been a secondary outcome, and quality of life endpoints remain lacking (149). The duration of most RCTs has been relatively short (mostly 1-3 years) and this, combined with smaller trial populations, reduces the power of the efficacy and safety data. Nevertheless, a Cochrane meta-analysis found high-quality evidence that bisphosphonates (as a class) reduce vertebral fracture risk in GIOP (149). Furthermore, network meta-analyses of RCTs have found moderate quality evidence that alendronate, risedronate, zoledronate, teriparatide and denosumab reduce fracture risk in GIOP (137, 150). For raloxifene and ibandronate, RCTs have reported increased spine and hip BMD (151) but evidence on fracture risk is insufficient (particularly for the key outcome of vertebral fractures) (152). One recent RCT found a significant but small increase in lumbar spine BMD with bazedoxifene compared to placebo in RA patients taking low glucocorticoid doses (153) but this drug is no longer available in Belgium. Still, raloxifene might be considered in post-menopausal women with contraindications to all other drugs, but no contraindication to a selective estrogen receptor modulator (such as increased risk of cardiovascular disease or venous thromboembolism) (91).
There is high-quality evidence that bone-protective agents prevent GIOP (154, 155). Therefore, we strongly recommend initiation of bone-targeted drugs in patients at risk of GIOP as early as possible, preferably at the start of glucocorticoid treatment. Still, it is never too late to initiate GIOP prevention in the large group of untreated long-term glucocorticoid users, since RCTs have demonstrated efficacy in both new and chronic glucocorticoid users (152). In population-based studies, delayed initiation of anti-osteoporosis medications has been associated with increased vertebral and hip fracture risk (156).
Glucocorticoids themselves, as well as the underlying disease, co-morbidities and co-medications, may explain why patients treated for GIOP might be susceptible to side effects. Glucocorticoid therapy is a documented risk factor for osteonecrosis of the jaw (157) and probably also for atypical femoral fractures (158). Meta-analyses have found no significant increase in upper gastrointestinal side effects with oral bisphosphonates in GIOP trials; however, these trials may collectively have been underpowered (154). A recent very large population-based cohort study found significantly increased fracture risk in RA patients co-prescribed glucocorticoids and proton pump inhibitors, compared to non-use or either drug alone (159).
Most guidelines give preference to oral bisphosphonates as first-line GIOP drugs, because they are easy to use, safe, cheap and cost-effective (91, 106, 107) (121–124). In terms of comparative effectiveness however, network meta-analyses of RCTs in GIOP suggest that teriparatide and denosumab reduce the risk of vertebral fractures more than oral bisphosphonates (152, 160, 161). Individual RCTs in GIOP have shown that teriparatide, denosumab and zoledronate produce greater BMD gains than risedronate (162–164). Furthermore, there is evidence in GIOP that teriparatide reduces vertebral fracture risk more than alendronate (162, 165). Moreover, compliance with osteoporosis drugs is often suboptimal, but may be poorest with oral bisphosphonates. Therefore, we suggest considering teriparatide, denosumab or zoledronate in patients at very high fracture risk (i.e. those with prior vertebral or hip fracture and/or a T-score ≤ -2.5). However, these parenteral treatment options are more expensive. Still, even teriparatide may be cost-effective, at least in patients with very high vertebral fracture risk (122). We suggest considering patient preference in treatment choice (166) which may also be influenced by cost and reimbursement. Specifically, teriparatide is the most expensive and most strictly reimbursed GIOP drug in Belgium, which may prevent its use as first-line therapy in most patients.
In summary, we recommend alendronate, risedronate, zoledronate, denosumab and teriparatide as evidence-based treatment options to prevent fractures in GIOP. Raloxifene might be considered if no alternatives are available (e.g. due to contraindications). Other treatments mentioned in our previous recommendations from 2006 (ibandronate, calcitonin, strontium ranelate etc.) are no longer recommended.
Given the pathophysiological contribution of impaired osteoblast activity in GIOP, the potential for combination therapy (e.g. denosumab plus teriparatide (167)) or sequential therapy (168) as well as sclerostin inhibitors to prevent or reverse GIOP merits further investigation. One recent observational study reported similar effect of one year denosumab or romosozumab for treatment of GIOP in RA patients (169).
Of note, women of childbearing potential should be asked about their desire for future pregnancies, counselled regarding the benefits and risks of osteoporosis medications related to pregnancy, and advised to take adequate birth control if appropriate while taking osteoporosis drugs.
3.6.1 Bisphosphonates
Bisphosphonates are the most commonly used drugs in the management of GIOP. Oral alendronate (10 mg daily or 70 mg once weekly) and risedronate (5 mg daily or 35 mg once weekly), and intravenous zoledronate (5 mg once yearly by intravenous infusion) are all approved for this indication (although marketing authorization has not been approved in Europe for all available dosage forms, the BBC does not consider this to be clinically relevant). All improve lumbar spine and hip BMD in patients treated with glucocorticoids (145, 163, 170, 171). Oral bisphosphonates are nowadays generic and cheap. Still, in a comparative effectiveness trial, zoledronate was superior to risedronate to increase lumbar spine BMD (163). For alendronate and risedronate, there is evidence from network meta-analyses that they reduce the rate of vertebral fractures (137, 161). There is moderate quality evidence from meta-analyses (137) as well as real-world observational evidence suggesting that oral bisphosphonates also reduce non-vertebral fractures (172–176). In the pivotal non-inferiority study comparing zoledronate with risedronate, the fracture rate was too low to ascertain anti-fracture effectiveness (163). Given the high fracture risk in GIOP and the proven efficacy of oral bisphosphonates however, placebo-controlled RCTs in GIOP would not have been ethical for newer drugs.
In post-menopausal osteoporosis, a drug holiday may be considered after 5 years of alendronate or 3 annual zoledronate infusions (44). Given their long biological half-life, these drugs continue to reduce fracture risk following their discontinuation, while the risk of adverse effects such as atypical femoral fractures diminishes within months (177). Given the high risk of vertebral fractures however, the concept of drug holiday has not been studied nor recommended in GIOP. Risedronate has a lower affinity for hydroxyapatite and a quicker offset than alendronate or zoledronate, therefore drug holidays have not been studied extensively with risedronate (178). However, there is insufficient data to make recommendations for or against treatment beyond 10 years of oral bisphosphonates or 6 annual zoledronate infusions.
3.6.2 Teripartide
The predominant role of reduced bone formation in GIOP provides a rationale for the use of anabolic agents in its treatment. In an active-comparator RCT the effects of 18 months of treatment with subcutaneous teriparatide, 20 µg/day vs. oral alendronate 10 mg/day, were compared in 428 men and women with GIOP. Teriparatide resulted in significantly greater increases in spine and hip BMD than alendronate (162). Although fracture was not a primary end-point of the study, significantly fewer new vertebral fractures occurred in patients treated with teriparatide compared to alendronate (0.6% vs. 6.1%; p = 0.004) (162). The incidence of non-vertebral fractures was similar in the two treatment groups. Results after 36 months of treatment demonstrated a continued increase in spine and hip BMD in the teriparatide treated group, with superiority over alendronate at the 24-month and 36-month time points (165). A lower incidence of new vertebral fractures was also seen in the teriparatide group at 36 months (1.7% vs 7.7%, p = 0.007), with a similar incidence of non-vertebral fractures in the two groups. With regard to safety, increased pre-dose serum calcium levels were significantly more common in the teriparatide than alendronate treated group (21% vs. 7%), but no other concerns were identified. Although teriparatide does not increase the risk of osteosarcoma in adults (179) it is not recommended for osteoporosis in adult cancer patients (180, 181) due to lack of evidence and concerns that increased remodeling and parathyroid hormone signaling may create a “fertile soil” for the development of bone metastases.
3.6.3 Denosumab
In a phase 3 active-controlled RCT of adults taking ≥ 7.5 mg prednisone or equivalent daily, treatment with denosumab, 60 mg once every 6 months by subcutaneous injection, was associated with a significantly greater increase in lumbar spine and hip BMD compared to risedronate 5 mg daily over a 12 months treatment period (164). This effect was confirmed after 24 months (182) and seen both in patients initiating glucocorticoids and in those on long-term therapy, regardless of age, race, baseline BMD T-score, glucocorticoid dose or menopausal status. HR-pQCT outcomes at the distal radius and tibia were also superior with denosumab in this trial (183). Another head-to-head open-label trial showed superiority of denosumab compared to alendronate in increasing lumbar spine BMD and decreasing BTMs in long-term glucocorticoid users (184).
While denosumab is effective in improving bone mass in glucocorticoid-treated subjects, its discontinuation can be associated with rapid bone loss, high bone turnover and potentially increased risk of so-called rebound-associated multiple vertebral fractures (185). Therefore, it is critical that patients either continue denosumab, or receive follow-up therapy with another anti-resorptive drug such as a bisphosphonate to prevent this complication (185). There are no specific studies on the risk of rebound-associated vertebral fractures in GIOP, but we can hypothesize that the risk may exist (186).
3.7 Follow-Up and Monitoring
● Recommendation 16: We suggest that follow-up in GIOP should focus on adherence to GIOP preventive and treatment measures, and fracture risk re-evaluation at each visit (weak recommendation, low-quality evidence).
We suggest that history taking and clinical examination focus on recent falls and incident fractures, smoking and alcohol use, muscle strength and balance, BMI, monitoring of height, back pain and kyphosis, and treatment-related adverse events (96). Symptoms of hip or knee pain might precede atypical femoral fractures.
● Recommendation 17: We suggest BMD monitoring by DXA and vertebral fracture identification one year after glucocorticoid initiation. Thereafter, individualized monitoring intervals might be considered. Extended femur scans might be considered at the time of DXA imaging in glucocorticoid users on long-term (≥ 3 years) antiresorptive therapy (weak recommendation, low-quality evidence).
Three tools can be used to monitor GIOP in routine clinical practice: BMD measurements by DXA (and fracture risk estimation using updated clinical risk factors), diagnosis of vertebral fractures (by VFA or lateral spine X-ray) and BTMs (see recommendation 19).
High glucocorticoid doses cause rapid bone loss, particularly at the lumbar spine and during the first 12 months of treatment (5). In contrast, pharmacotherapy may improve BMD after one year. Thus, both in patients receiving and not receiving bone-active drugs, re-evaluation of BMD may be considered one year after the initiation of glucocorticoids, and every 1 to 5 years thereafter with the shorter interval for those who are taking higher glucocorticoid doses and/or having lower BMD values (91, 187, 188). However, considering the lack of evidence on the clinical value of BMD monitoring in GIOP, we suggest individualized clinical decision making to determine DXA intervals.
VFA (or lateral spine X-rays) to exclude vertebral fractures should be considered at the time of BMD measurement, in case of back pain, or height loss greater than 2 cm since baseline or 4 cm since young adulthood. Improved or stable BMD may be a reason to continue therapy, whereas worsening or stable osteoporosis or identification of (incident or previously unrecognized) vertebral fractures may be an indication to switch drug therapy (see recommendation 15).
Some centers have started using extended DXA scanning (including the subtrochanteric region of both femurs) to screen for cortical thickening (“beaking”) or other radiographic features of (subclinical) atypical femoral fractures (189, 190). The International Society for Clinical Densitometry suggests to consider the use of bilateral full-length femur imaging in patients who are currently or have been in the past year on potent antiresorptive therapy (i.e., oral or intravenous bisphosphonate or subcutaneous denosumab therapy) for a cumulative period of 3 or more years, especially those on long-term glucocorticoid therapy (191). However, the evidence is currently insufficient to make definite recommendations or assess the cost-effectivity of such a screening strategy during antiresorptive treatment in general, and in GIOP in particular.
● Recommendation 18: Trabecular bone score (TBS) might be considered during GIOP monitoring, however, the evidence is currently insufficient to alter treatment based on TBS alone (weak recommendation, low-quality evidence).
TBS has recently emerged as possibly adding value to the assessment of bone microarchitectural decay during glucocorticoid treatment (192–196). In one RCT in GIOP, TBS showed greater improvement with teriparatide than with alendronate therapy (197). TBS can be considered an ancillary test that can be integrated in the FRAX® algorithm. However, the exact clinical role of TBS in guiding treatment decisions remains unclear.
Although TBS can be considered a promising tool that may even be more sensitive to change than DXA BMD under certain conditions, we suggest considering TBS results together with BMD and clinical risk factors and not in isolation.
● Recommendation 19: BTMs may be considered for monitoring treatment with anti-resorptive or osteoanabolic drugs in GIOP (weak recommendation, moderate quality evidence).
Randomized trials in GIOP have shown that teriparatide increases, whereas antiresorptive drugs further reduce bone turnover (165) (198). However, very few studies have evaluated the clinical impact of measuring biomarkers in routine clinical practice. Moreover, specific real-world studies in GIOP are lacking. Thus, whether it improves adherence to osteoporosis drugs or skeletal outcomes in GIOP remains unknown. Monitoring treatment-related changes in BTMs is further limited by pre-analytical and analytical challenges. Therefore, a weak recommendation was made to consider the clinical use of BTMs in monitoring antiresorptive or osteoanabolic pharmacotherapy in GIOP.
● Recommendation 20: When glucocorticoids are discontinued, we recommend a re-evaluation of fracture risk to guide the decision to continue or stop GIOP prevention (strong recommendation, moderate quality evidence).
BMD and fracture risk generally recover towards baseline levels when glucocorticoids are discontinued (9, 12, 43) although some detrimental effects may linger, particularly in post-menopausal women or patients with vertebral fractures. Some patients may qualify for continued treatment or bisphosphonate drug holidays under guidelines for post-menopausal osteoporosis (44) male osteoporosis or osteoporosis in younger persons (42) respectively. Because of their reversible effects, discontinuation of treatment with denosumab (if any) or teriparatide should always be followed by antiresorptive therapy.
4 Discussion
The BBC recommendations for GIOP outlined in this manuscript both update and extend our previous consensus from more than fifteen years ago (43). For example, they include Cushing syndrome and transplantation-associated osteoporosis, which are often neglected in GIOP recommendations. They are also based on an extensive literature review and a standardized grading of the strength of the recommendations and quality of the supporting evidence. We plan to update these recommendation in ten years time, or earlier if major clinically relevant changes are required.
However, we recognize several limitations of this work. In contrast to our previous guideline on post-menopausal osteoporosis (44) this work was not based on a formal umbrella systematic review (as originally planned), due to lack of time and available resources. Only PubMed was searched, therefore some other systematic reviews and meta-analyses could have been missed. Since it was based on a narrative review only, these recommendations should not be considered “guidelines”. However, we believe international guidelines already fulfill this purpose (96). Most recommendations were based on low to moderate quality evidence, highlighting the need for further research into clinical aspects of GIOP. Key areas of GIOP management with remaining uncertainty in terms of clinical evidence identified in this review are summarized in Table 6. We also did not include patients or stakeholders from relevant national societies (e.g. pulmonologists, gastroenterologists, hematologists or primary care physicians), although we plan to divulge our recommendations following publication.
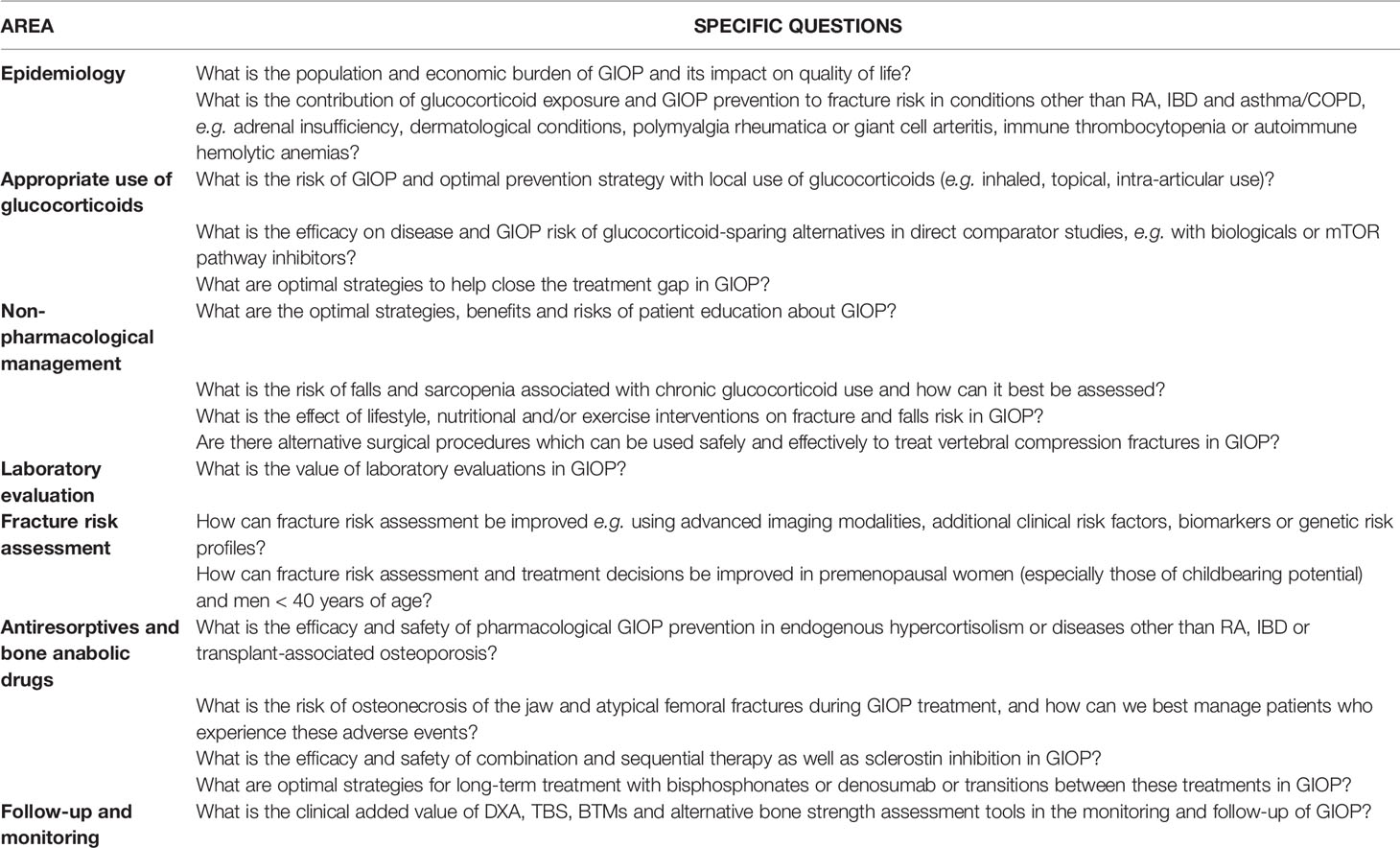
Table 6 The research agenda: key areas in the clinical management of GIOP requiring further research.
In summary, GIOP is a common secondary cause of osteoporosis in adults, resulting in considerable fracture risk, impaired quality of life and health-economic burden. A large treatment gap remains, and many glucocorticoid prescribers do not consider GIOP prevention their responsibility. Nevertheless, effective, safe and cost-effective treatment options for GIOP patients at high and very high fracture risk are available. Efforts to close the treatment gap in GIOP and implement available effective fracture prevention strategies into clinical practice in primary, secondary and tertiary care are urgently needed, and we hope these recommendations contribute to this end. In any case, these recommendations are intended to assist clinicians but not to replace individual clinical judgement.
Author Contributions
All authors contributed to the conceptualization, methodology, data collection, writing of the original draft, editing and reviewing, and approval of the final version for publication.
Conflict of Interest
ML has received consultancy and lecture fees from Alexion, Amgen, Daiichi Sankyo, Kyowa Kirin, Menarini, Orifarm, Sandoz, Takeda, UCB, and Will Pharma. SG has received consultancy, lecture and travel fees from Alexion, Amgen, MSD, Novartis, Takeda, UCB, and Will Pharma. CV has received travel fees from Boehringer Ingelheim. JB has received consultancy, lecture fees and travel support from Alexion, Amgen, Bayer, Sandoz, Takeda, UCB and Will-Pharma. OB has received consultancy fees from Amgen, Biophytis, IBSA, MEDA, Servier, SMB, Teva, TRB Chemedica, and UCB. EC has received consultancy fees from bioMérieux, DiaSorin, Fujirebio, IDS, Menarini, and Nittobo. SR has received travel and consultancy fees from Abbott, Bayer, Eurogenerics, Gedeon Richter, Mylan, Takeda, Theramex, UCB and Will-Pharma. EG has received travel and consultancy fees from Amgen, Alexion, Daiichi Sankyo, Sandoz, Takeda, UCB, and Will Pharma.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fardet L, Petersen I, Nazareth I. Monitoring of Patients on Long-Term Glucocorticoid Therapy: A Population-Based Cohort Study. Med (Baltimore) (2015) 94:e647. doi: 10.1097/MD.0000000000000647
2. Diez-Perez A, Hooven FH, Adachi JD, Adami S, Anderson FA, Boonen S, et al. Regional Differences in Treatment for Osteoporosis. The Global Longitudinal Study of Osteoporosis in Women (GLOW). Bone (2011) 49:493–8. doi: 10.1016/j.bone.2011.05.007
3. Kanis JA, Johansson H, Oden A, Johnell O, de Laet C, Melton IL, et al. A Meta-Analysis of Prior Corticosteroid Use and Fracture Risk. J Bone Miner Res (2004) 19:893–9. doi: 10.1359/JBMR.040134
4. Braun LT, Fazel J, Zopp S, Benedix S, Osswald-Kopp A, Riester A, et al. The Effect of Biochemical Remission on Bone Metabolism in Cushing's Syndrome: A 2-Year Follow-Up Study. J Bone Miner Res (2020) 35:1711–7. doi: 10.1002/jbmr.4033
5. Laan RF, van Riel PL, van de Putte LB, van Erning LJ, van't Hof MA, Lemmens JA. Low-Dose Prednisone Induces Rapid Reversible Axial Bone Loss in Patients With Rheumatoid Arthritis. A Randomized, Controlled Study. Ann Intern Med (1993) 119:963–8. doi: 10.7326/0003-4819-119-10-199311150-00001
6. Amiche MA, Albaum JM, Tadrous M, Pechlivanoglou P, Levesque LE, Adachi JD, et al. Fracture Risk in Oral Glucocorticoid Users: A Bayesian Meta-Regression Leveraging Control Arms of Osteoporosis Clinical Trials. Osteoporos Int (2016) 27:1709–18. doi: 10.1007/s00198-015-3455-9
7. Wang Y, Zhao R, Gu Z, Dong C, Guo G, Li L. Effects of Glucocorticoids on Osteoporosis in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Osteoporos Int (2020) 31:1401–9. doi: 10.1007/s00198-020-05360-w
8. Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Use of Oral Corticosteroids and Risk of Fractures. J Bone Miner Res (2000) 15:993–1000. doi: 10.1359/jbmr.2000.15.6.993
9. Balasubramanian A, Wade SW, Adler RA, Saag K, Pannacciulli N, Curtis JR. Glucocorticoid Exposure and Fracture Risk in a Cohort of US Patients With Selected Conditions. J Bone Miner Res (2018) 33:1881–8. doi: 10.1002/jbmr.3523
10. Rice JB, White AG, Scarpati LM, Wan G, Nelson WW. Long-Term Systemic Corticosteroid Exposure: A Systematic Literature Review. Clin Ther (2017) 39:2216–29. doi: 10.1016/j.clinthera.2017.09.011
11. Sarnes E, Crofford L, Watson M, Dennis G, Kan H, Bass D. Incidence and US Costs of Corticosteroid-Associated Adverse Events: A Systematic Literature Review. Clin Ther (2011) 33:1413–32. doi: 10.1016/j.clinthera.2011.09.009
12. van Staa TP, Leufkens HG, Cooper C. The Epidemiology of Corticosteroid-Induced Osteoporosis: A Meta-Analysis. Osteoporos Int (2002) 13:777–87. doi: 10.1007/s001980200108
13. Weinstein RS. Clinical Practice. Glucocorticoid-Induced Bone Disease. N Engl J Med (2011) 365:62–70. doi: 10.1056/NEJMcp1012926
14. van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Oral Corticosteroids and Fracture Risk: Relationship to Daily and Cumulative Doses. Rheumatol (Oxford) (2000) 39:1383–9. doi: 10.1093/rheumatology/39.12.1383
15. Amiche MA, Abtahi S, Driessen JHM, Vestergaard P, de Vries F, Cadarette SM, et al. Impact of Cumulative Exposure to High-Dose Oral Glucocorticoids on Fracture Risk in Denmark: A Population-Based Case-Control Study. Arch Osteoporos (2018) 13:30. doi: 10.1007/s11657-018-0424-x
16. Trementino L, Appolloni G, Ceccoli L, Marcelli G, Concettoni C, Boscaro M, et al. Bone Complications in Patients With Cushing's Syndrome: Looking for Clinical, Biochemical, and Genetic Determinants. Osteoporos Int (2014) 25:913–21. doi: 10.1007/s00198-013-2520-5
17. Belaya ZE, Hans D, Rozhinskaya LY, Dragunova NV, Sasonova NI, Solodovnikov AG, et al. The Risk Factors for Fractures and Trabecular Bone-Score Value in Patients With Endogenous Cushing's Syndrome. Arch Osteoporos (2015) 10:44. doi: 10.1007/s11657-015-0244-1
18. Schepper JD, Collins F, Rios-Arce ND, Kang HJ, Schaefer L, Gardinier JD, et al. Involvement of the Gut Microbiota and Barrier Function in Glucocorticoid-Induced Osteoporosis. J Bone Miner Res (2020) 35:801–20. doi: 10.1002/jbmr.3947
19. Guanabens N, Gifre L, Peris P. The Role of Wnt Signaling and Sclerostin in the Pathogenesis of Glucocorticoid-Induced Osteoporosis. Curr Osteoporos Rep (2014) 12:90–7. doi: 10.1007/s11914-014-0197-0
20. Vestergaard P. Drugs Causing Bone Loss. Handb Exp Pharmacol (2020) 262:475–97. doi: 10.1007/164_2019_340
21. Takahata M, Shimizu T, Yamada S, Yamamoto T, Hasegawa T, Fujita R, et al. Bone Biopsy Findings in Patients Receiving Long-Term Bisphosphonate Therapy for Glucocorticoid-Induced Osteoporosis. J Bone Miner Metab (2022). doi: 10.1007/s00774-022-01323-9
22. Schilperoort M, Kroon J, Kooijman S, Smit AE, Gentenaar M, Mletzko K, et al. Loss of Glucocorticoid Rhythm Induces an Osteoporotic Phenotype in Female Mice. Aging Cell (2021) 20:e13474. doi: 10.1111/acel.13474
23. Gupta A, Pipe SG, Towheed T, Anastassiades T. Is Rheumatoid Arthritis a Risk Factor for Fractures: A Systematic Review of Observational Studies. Curr Rheumatol Rev (2020) 16:29–37. doi: 10.2174/1573397115666190723160312
24. van Staa TP, Leufkens HG, Cooper C. Use of Inhaled Corticosteroids and Risk of Fractures. J Bone Miner Res (2001) 16:581–8. doi: 10.1359/jbmr.2001.16.3.581
25. Blavnsfeldt AG, de Thurah A, Thomsen MD, Tarp S, Langdahl B, Hauge EM. The Effect of Glucocorticoids on Bone Mineral Density in Patients With Rheumatoid Arthritis: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. Bone (2018) 114:172–80. doi: 10.1016/j.bone.2018.06.008
26. Siu S, Haraoui B, Bissonnette R, Bessette L, Roubille C, Richer V, et al. Meta-Analysis of Tumor Necrosis Factor Inhibitors and Glucocorticoids on Bone Density in Rheumatoid Arthritis and Ankylosing Spondylitis Trials. Arthritis Care Res (Hoboken) (2015) 67:754–64. doi: 10.1002/acr.22519
27. Gu C, Zhao R, Zhang X, Gu Z, Zhou W, Wang Y, et al. A Meta-Analysis of Secondary Osteoporosis in Systemic Lupus Erythematosus: Prevalence and Risk Factors. Arch Osteoporos (2019) 15:1. doi: 10.1007/s11657-019-0667-1
28. Ugarte-Gil MF, Mak A, Leong J, Dharmadhikari B, Kow NY, Reategui-Sokolova C, et al. Impact of Glucocorticoids on the Incidence of Lupus-Related Major Organ Damage: A Systematic Literature Review and Meta-Regression Analysis of Longitudinal Observational Studies. Lupus Sci Med (2021) 8:e000590. doi: 10.1136/lupus-2021-000590
29. Chandran S, Aldei A, Johnson SR, Cheung AM, Salonen D, Gladman DD. Prevalence and Risk Factors of Low Bone Mineral Density in Psoriatic Arthritis: A Systematic Review. Semin Arthritis Rheum (2016) 46:174–82. doi: 10.1016/j.semarthrit.2016.05.005
30. Zhou T, Pan J, Lai B, Cen L, Jiang W, Yu C, et al. Bone Mineral Density is Negatively Correlated With Ulcerative Colitis: A Systematic Review and Meta-Analysis. Clin Transl Med (2020) 9:18. doi: 10.1186/s40169-020-00270-0
31. Komaki Y, Komaki F, Micic D, Ido A, Sakuraba A. Risk of Fractures in Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. J Clin Gastroenterol (2019) 53:441–8. doi: 10.1097/MCG.0000000000001031
32. Ludvigsson JF, Mahl M, Sachs MC, Bjork J, Michaelsson K, Ekbom A, et al. Fracture Risk in Patients With Inflammatory Bowel Disease: A Nationwide Population-Based Cohort Study From 1964 to 2014. Am J Gastroenterol (2019) 114:291–304. doi: 10.14309/ajg.0000000000000062
33. Feng Z, Zeng S, Wang Y, Zheng Z, Chen Z. Bisphosphonates for the Prevention and Treatment of Osteoporosis in Patients With Rheumatic Diseases: A Systematic Review and Meta-Analysis. PloS One (2013) 8:e80890. doi: 10.1371/journal.pone.0080890
34. Fujieda Y, Horita T, Nishimoto N, Tanimura K, Amasaki Y, Kasahara H, et al. Efficacy and Safety of Sodium RISedronate for Glucocorticoid-Induced OsTeoporosis With Rheumatoid Arthritis (RISOTTO Study): A Multicentre, Double-Blind, Randomized, Placebo-Controlled Trial. Mod Rheumatol (2021) 31:593–9. doi: 10.1080/14397595.2020.1812835
35. Yao L, Wang H, Dong W, Liu Z, Mao H. Efficacy and Safety of Bisphosphonates in Management of Low Bone Density in Inflammatory Bowel Disease: A Meta-Analysis. Med (Baltimore) (2017) 96:e5861. doi: 10.1097/MD.0000000000005861
36. van Staa TP, Geusens P, Pols HA, de Laet C, Leufkens HG, Cooper C. A Simple Score for Estimating the Long-Term Risk of Fracture in Patients Using Oral Glucocorticoids. QJM (2005) 98:191–8. doi: 10.1093/qjmed/hci029
37. Hew M, McDonald VM, Bardin PG, Chung LP, Farah CS, Barnard A, et al. Cumulative Dispensing of High Oral Corticosteroid Doses for Treating Asthma in Australia. Med J Aust (2020) 213:316–20. doi: 10.5694/mja2.50758
38. Sweeney J, Patterson CC, Menzies-Gow A, Niven RM, Mansur AH, Bucknall C, et al. Comorbidity in Severe Asthma Requiring Systemic Corticosteroid Therapy: Cross-Sectional Data From the Optimum Patient Care Research Database and the British Thoracic Difficult Asthma Registry. Thorax (2016) 71:339–46. doi: 10.1136/thoraxjnl-2015-207630
39. Chang YP, Lai CH, Lin CY, Chang YC, Lin MC, Chong IW, et al. Mortality and Vertebral Fracture Risk Associated With Long-Term Oral Steroid Use in Patients With Chronic Obstructive Pulmonary Disease: A Systemic Review and Meta-Analysis. Chron Respir Dis (2019) 16:1479973119838280. doi: 10.1177/1479973119838280
40. Volmer T, Effenberger T, Trautner C, Buhl R. Consequences of Long-Term Oral Corticosteroid Therapy and its Side-Effects in Severe Asthma in Adults: A Focused Review of the Impact Data in the Literature. Eur Respir J (2018) 52:1800703. doi: 10.1183/13993003.00703-2018
41. Hansen KE, Kleker B, Safdar N, Bartels CM. A Systematic Review and Meta-Analysis of Glucocorticoid-Induced Osteoporosis in Children. Semin Arthritis Rheum (2014) 44:47–54. doi: 10.1016/j.semarthrit.2014.02.002
42. Rozenberg S, Bruyere O, Bergmann P, Cavalier E, Gielen E, Goemaere S, et al. How to Manage Osteoporosis Before the Age of 50. Maturitas (2020) 138:14–25. doi: 10.1016/j.maturitas.2020.05.004
43. Devogelaer JP, Goemaere S, Boonen S, Body JJ, Kaufman JM, Reginster JY, et al. Evidence-Based Guidelines for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis: A Consensus Document of the Belgian Bone Club. Osteoporos Int (2006) 17:8–19. doi: 10.1007/s00198-005-2032-z
44. Sanchez-Rodriguez D, Bergmann P, Body JJ, Cavalier E, Gielen E, Goemaere S, et al. The Belgian Bone Club 2020 Guidelines for the Management of Osteoporosis in Postmenopausal Women. Maturitas (2020) 139:69–89. doi: 10.1016/j.maturitas.2020.05.006
45. Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, et al. A Guide for Health Professionals to Interpret and Use Recommendations in Guidelines Developed With the GRADE Approach. J Clin Epidemiol (2016) 72:45–55. doi: 10.1016/j.jclinepi.2015.11.017
46. Schulz J, Frey KR, Cooper MS, Zopf K, Ventz M, Diederich S, et al. Reduction in Daily Hydrocortisone Dose Improves Bone Health in Primary Adrenal Insufficiency. Eur J Endocrinol (2016) 174:531–8. doi: 10.1530/EJE-15-1096
47. Lipworth BJ. Systemic Adverse Effects of Inhaled Corticosteroid Therapy: A Systematic Review and Meta-Analysis. Arch Intern Med (1999) 159:941–55. doi: 10.1001/archinte.159.9.941
48. De Vries F, Bracke M, Leufkens HG, Lammers JW, Cooper C, Van Staa TP. Fracture Risk With Intermittent High-Dose Oral Glucocorticoid Therapy. Arthritis Rheum (2007) 56:208–14. doi: 10.1002/art.22294
49. Walters JA, Tan DJ, White CJ, Wood-Baker R. Different Durations of Corticosteroid Therapy for Exacerbations of Chronic Obstructive Pulmonary Disease. Cochrane Database Syst Rev (2018) 3:CD006897. doi: 10.1002/14651858.CD006897.pub4
50. Messina OD, Vidal LF, Wilman MV, Bultink IEM, Raterman HG, Lems W. Management of Glucocorticoid-Induced Osteoporosis. Aging Clin Exp Res (2021) 33:793–804. doi: 10.1007/s40520-021-01823-0
51. Pouwels S, de Boer A, Leufkens HG, Weber WE, Cooper C, van Onzenoort HA, et al. Risk of Fracture in Patients With Muscular Dystrophies. Osteoporos Int (2014) 25:509–18. doi: 10.1007/s00198-013-2442-2
52. Hill QA, Grainger JD, Thachil J, Provan D, Evans G, Garg M, et al. The Prevention of Glucocorticoid-Induced Osteoporosis in Patients With Immune Thrombocytopenia Receiving Steroids: A British Society for Haematology Good Practice Paper. Br J Haematol (2019) 185:410–7. doi: 10.1111/bjh.15735
53. Nomura S, Kurata Y, Tomiyama Y, Takubo T, Hasegawa M, Saigo K, et al. Effects of Bisphosphonate Administration on the Bone Mass in Immune Thrombocytopenic Purpura Patients Under Treatment With Steroids. Clin Appl Thromb Hemost (2010) 16:622–7. doi: 10.1177/1076029609350889
54. Eyre TA, Jensen P, Booth S, El-Galaly TC. Bone Health and Glucocorticoid-Containing Lymphoma Therapy - a Review of Risk Factors and Preventative Measures. Br J Haematol (2022). doi: 10.1111/bjh.18104
55. Jodar E, Valdepenas MP, Martinez G, Jara A, Hawkins F. Long-Term Follow-Up of Bone Mineral Density in Addison's Disease. Clin Endocrinol (Oxf) (2003) 58:617–20. doi: 10.1046/j.1365-2265.2003.01761.x
56. Li L, Bensing S, Falhammar H. Rate of Fracture in Patients With Glucocorticoid Replacement Therapy: A Systematic Review and Meta-Analysis. Endocrine (2021) 74:29–37. doi: 10.1007/s12020-021-02723-z
57. Al Nofal A, Bancos I, Benkhadra K, Ospina NM, Javed A, Kapoor E, et al. Glucocorticoid Replacement Regimens in Chronic Adrenal Insufficiency: A Systematic Review and Meta-Analysis. Endocr Pract (2017) 23:17–31. doi: 10.4158/EP161428.OR
58. Frey KR, Kienitz T, Schulz J, Ventz M, Zopf K, Quinkler M. Prednisolone is Associated With a Worse Bone Mineral Density in Primary Adrenal Insufficiency. Endocr Connect (2018) 7:811–8. doi: 10.1530/EC-18-0160
59. Rangaswamaiah S, Gangathimmaiah V, Nordenstrom A, Falhammar H. Bone Mineral Density in Adults With Congenital Adrenal Hyperplasia: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne) (2020) 11:493. doi: 10.3389/fendo.2020.00493
60. Loh HH, Yee A, Loh HS. Bone Health Among Patients With Primary Aldosteronism: A Systematic Review and Meta-Analysis. Minerva Endocrinol (2019) 44:387–96. doi: 10.23736/S0391-1977.18.02867-5
61. Arlt W, Lang K, Sitch AJ, Dietz AS, Rhayem Y, Bancos I, et al. Steroid Metabolome Analysis Reveals Prevalent Glucocorticoid Excess in Primary Aldosteronism. JCI Insight (2017) 2:e93136. doi: 10.1172/jci.insight.93136
62. Richy F, Bousquet J, Ehrlich GE, Meunier PJ, Israel E, Morii H, et al. Inhaled Corticosteroids Effects on Bone in Asthmatic and COPD Patients: A Quantitative Systematic Review. Osteoporos Int (2003) 14:179–90. doi: 10.1007/s00198-003-1398-z
63. Etminan M, Sadatsafavi M, Ganjizadeh Zavareh S, Takkouche B, FitzGerald JM. Inhaled Corticosteroids and the Risk of Fractures in Older Adults: A Systematic Review and Meta-Analysis. Drug Saf (2008) 31:409–14. doi: 10.2165/00002018-200831050-00005
64. Egeberg A, Schwarz P, Harslof T, Andersen YMF, Pottegard A, Hallas J, et al. Association of Potent and Very Potent Topical Corticosteroids and the Risk of Osteoporosis and Major Osteoporotic Fractures. JAMA Dermatol (2021) 157:275–82. doi: 10.1001/jamadermatol.2020.4968
65. Chalitsios CV, Shaw DE, McKeever TM. Corticosteroids and Bone Health in People With Asthma: A Systematic Review and Meta-Analysis. Respir Med (2021) 181:106374. doi: 10.1016/j.rmed.2021.106374
66. Loke YK, Gilbert D, Thavarajah M, Blanco P, Wilson AM. Bone Mineral Density and Fracture Risk With Long-Term Use of Inhaled Corticosteroids in Patients With Asthma: Systematic Review and Meta-Analysis. BMJ Open (2015) 5:e008554. doi: 10.1136/bmjopen-2015-008554
67. Loke YK, Cavallazzi R, Singh S. Risk of Fractures With Inhaled Corticosteroids in COPD: Systematic Review and Meta-Analysis of Randomised Controlled Trials and Observational Studies. Thorax (2011) 66:699–708. doi: 10.1136/thx.2011.160028
68. Yang IA, Clarke MS, Sim EH, Fong KM. Inhaled Corticosteroids for Stable Chronic Obstructive Pulmonary Disease. Cochrane Database Syst Rev (2012) 7:CD002991. doi: 10.1002/14651858.CD002991.pub3
69. Kerezoudis P, Rinaldo L, Alvi MA, Hunt CL, Qu W, Maus TP, et al. The Effect of Epidural Steroid Injections on Bone Mineral Density and Vertebral Fracture Risk: A Systematic Review and Critical Appraisal of Current Literature. Pain Med (2018) 19:569–79. doi: 10.1093/pm/pnx324
70. Jensen TW, Hansen MS, Horslev-Petersen K, Hyldstrup L, Abrahamsen B, Langdahl B, et al. Periarticular and Generalised Bone Loss in Patients With Early Rheumatoid Arthritis: Influence of Alendronate and Intra-Articular Glucocorticoid Treatment. Post Hoc Analyses From the CIMESTRA Trial. Ann Rheum Dis (2014) 73:1123–9. doi: 10.1136/annrheumdis-2012-203171
71. Schoon EJ, Bollani S, Mills PR, Israeli E, Felsenberg D, Ljunghall S, et al. Bone Mineral Density in Relation to Efficacy and Side Effects of Budesonide and Prednisolone in Crohn's Disease. Clin Gastroenterol Hepatol (2005) 3:113–21. doi: 10.1016/S1542-3565(04)00662-7
72. Kuenzig ME, Rezaie A, Kaplan GG, Otley AR, Steinhart AH, Griffiths AM, et al. Budesonide for the Induction and Maintenance of Remission in Crohn's Disease: Systematic Review and Meta-Analysis for the Cochrane Collaboration. J Can Assoc Gastroenterol (2018) 1:159–73. doi: 10.1093/jcag/gwy018
73. Rautiainen H, Farkkila M, Neuvonen M, Sane T, Karvonen AL, Nurmi H, et al. Pharmacokinetics and Bone Effects of Budesonide in Primary Biliary Cirrhosis. Aliment Pharmacol Ther (2006) 24:1545–52. doi: 10.1111/j.1365-2036.2006.03155.x
74. Chong LY, Head K, Hopkins C, Philpott C, Schilder AG, Burton MJ. Intranasal Steroids Versus Placebo or No Intervention for Chronic Rhinosinusitis. Cochrane Database Syst Rev (2016) 4:CD011996. doi: 10.1002/14651858.CD011996.pub2
75. Anastasilakis AD, Tsourdi E, Makras P, Polyzos SA, Meier C, McCloskey EV, et al. Bone Disease Following Solid Organ Transplantation: A Narrative Review and Recommendations for Management From The European Calcified Tissue Society. Bone (2019) 127:401–18. doi: 10.1016/j.bone.2019.07.006
76. Duru N, van der Goes MC, Jacobs JW, Andrews T, Boers M, Buttgereit F, et al. EULAR Evidence-Based and Consensus-Based Recommendations on the Management of Medium to High-Dose Glucocorticoid Therapy in Rheumatic Diseases. Ann Rheum Dis (2013) 72:1905–13. doi: 10.1136/annrheumdis-2013-203249
77. Robin F, Cadiou S, Albert JD, Bart G, Coiffier G, Guggenbuhl P. Methotrexate Osteopathy: Five Cases and Systematic Literature Review. Osteoporos Int (2021) 32:225–32. doi: 10.1007/s00198-020-05664-x
78. Naranjo A, Lopez R, Garcia-Magallon B, Caceres L, Francisco F, Jimenez-Palop M, et al. Longitudinal Practice Patterns of Prophylaxis of Glucocorticoid-Induced Osteoporosis in Patients With Polymyalgia Rheumatica. Rheumatol Int (2014) 34:1459–63. doi: 10.1007/s00296-014-3014-2
79. Albaum JM, Youn S, Levesque LE, Gershon AS, Cadarette SM. Osteoporosis Management Among Chronic Glucocorticoid Users: A Systematic Review. J Popul Ther Clin Pharmacol (2014) 21:e486–504.
80. Chalitsios CV, Shaw DE, McKeever TM. A Retrospective Database Study of Oral Corticosteroid and Bisphosphonate Prescribing Patterns in England. NPJ Prim Care Respir Med (2020) 30:5. doi: 10.1038/s41533-020-0162-6
81. Klop C, de Vries F, Vinks T, Kooij MJ, van Staa TP, Bijlsma JW, et al. Increase in Prophylaxis of Glucocorticoid-Induced Osteoporosis by Pharmacist Feedback: A Randomised Controlled Trial. Osteoporos Int (2014) 25:385–92. doi: 10.1007/s00198-013-2562-8
82. Yuksel N, Majumdar SR, Biggs C, Tsuyuki RT. Community Pharmacist-Initiated Screening Program for Osteoporosis: Randomized Controlled Trial. Osteoporos Int (2010) 21:391–8. doi: 10.1007/s00198-009-0977-z
83. McDonough RP, Doucette WR, Kumbera P, Klepser DG. An Evaluation of Managing and Educating Patients on the Risk of Glucocorticoid-Induced Osteoporosis. Value Health (2005) 8:24–31. doi: 10.1111/j.1524-4733.2005.04007.x
84. Guzman-Clark JR, Fang MA, Sehl ME, Traylor L, Hahn TJ. Barriers in the Management of Glucocorticoid-Induced Osteoporosis. Arthritis Rheum (2007) 57:140–6. doi: 10.1002/art.22462
85. Tory HO, Solomon DH, Desai SP. Analysis of Quality Improvement Efforts in Preventing Glucocorticoid-Induced Osteoporosis. Semin Arthritis Rheum (2015) 44:483–8. doi: 10.1016/j.semarthrit.2014.09.011
86. Carter M. Prevention of Glucocorticoid-Induced Osteoporosis: Clinical Audit to Evaluate the Implementation of National Osteoporosis Guideline Group 2017 Guidelines in a Primary Care Setting. J Clin Densitom (2019) 22:25–30. doi: 10.1016/j.jocd.2018.03.009
87. Suda M, Suyama Y, Ohde S, Tsuda T, Sawada H, Kishimoto M, et al. Effects of Quality Indicator Monitoring for Glucocorticoid-Induced Osteoporosis and Trends of Drug Treatment in a Japanese Hospital. Int J Rheum Dis (2018) 21:975–81. doi: 10.1111/1756-185X.13310
88. Curtis JR, Westfall AO, Allison J, Becker A, Melton ME, Freeman A, et al. Challenges in Improving the Quality of Osteoporosis Care for Long-Term Glucocorticoid Users: A Prospective Randomized Trial. Arch Intern Med (2007) 167:591–6. doi: 10.1001/archinte.167.6.591
89. Beukelman T, Saag KG, Curtis JR, Kilgore ML, Pisu M. Cost-Effectiveness of Multifaceted Evidence Implementation Programs for the Prevention of Glucocorticoid-Induced Osteoporosis. Osteoporos Int (2010) 21:1573–84. doi: 10.1007/s00198-009-1114-8
90. Elliot-Gibson V, Bogoch ER, Jamal SA, Beaton DE. Practice Patterns in the Diagnosis and Treatment of Osteoporosis After a Fragility Fracture: A Systematic Review. Osteoporos Int (2004) 15:767–78. doi: 10.1007/s00198-004-1675-5
91. Buckley L, Guyatt G, Fink HA, Cannon M, Grossman J, Hansen KE, et al. American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Arthritis Care Res (Hoboken) (2017) 69:1095–110. doi: 10.1002/acr.23279
92. Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL. Interventions to Prevent Falls in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA (2018) 319:1705–16. doi: 10.1001/jama.2017.21962
93. Buchbinder R, Johnston RV, Rischin KJ, Homik J, Jones CA, Golmohammadi K, et al. Percutaneous Vertebroplasty for Osteoporotic Vertebral Compression Fracture. Cochrane Database Syst Rev (2018) 11:CD006349. doi: 10.1002/14651858.CD006349.pub4
94. Ebeling PR, Akesson K, Bauer DC, Buchbinder R, Eastell R, Fink HA, et al. The Efficacy and Safety of Vertebral Augmentation: A Second ASBMR Task Force Report. J Bone Miner Res (2019) 34:3–21. doi: 10.1002/jbmr.3653
95. Cao J, Kong L, Meng F, Zhang Y, Shen Y. Risk Factors for New Vertebral Compression Fractures After Vertebroplasty: A Meta-Analysis. ANZ J Surg (2016) 86:549–54. doi: 10.1111/ans.13428
96. Lekamwasam S, Adachi JD, Agnusdei D, Bilezikian J, Boonen S, Borgstrom F, et al. A Framework for the Development of Guidelines for the Management of Glucocorticoid-Induced Osteoporosis. Osteoporos Int (2012) 23:2257–76. doi: 10.1007/s00198-012-1958-1
97. Eastell R, Black DM, Lui LY, Chines A, Marin F, Khosla S, et al. Treatment-Related Changes in Bone Turnover and Fracture Risk Reduction in Clinical Trials of Antiresorptive Drugs: Proportion of Treatment Effect Explained. J Bone Miner Res (2021) 36:236–43. doi: 10.1002/jbmr.4178
98. Morris HA, Eastell R, Jorgensen NR, Cavalier E, Vasikaran S, Chubb SAP, et al. Clinical Usefulness of Bone Turnover Marker Concentrations in Osteoporosis. Clin Chim Acta (2017) 467:34–41. doi: 10.1016/j.cca.2016.06.036
99. Bhattoa HP, Cavalier E, Eastell R, Heijboer AC, Jorgensen NR, Makris K, et al. Metabolism, Analytical Considerations and Plans to Standardize or Harmonize Assays for the Reference Bone Turnover Markers PINP and Beta-CTX in Blood. Clin Chim Acta (2021) 515:16–20. doi: 10.1016/j.cca.2020.12.023
100. Cavalier E, Eastell R, Jorgensen NR, Makris K, Tournis S, Vasikaran S, et al. A Multicenter Study to Evaluate Harmonization of Assays for C-Terminal Telopeptides of Type I Collagen (Ss-CTX): A Report From the IFCC-IOF Committee for Bone Metabolism (C-Bm). Calcif Tissue Int (2021) 108:785–97. doi: 10.1007/s00223-021-00816-5
101. Devogelaer J-P, Durnez A, Gruson D, Manicourt DH. Bone Turnover Markers and Glucocorticoid Treatments. In: Patel VB, Preedy VR, editors. Biomarkers in Bone Disease. Dordrecht: Springer Netherlands (2017). p. 905–32. p. pp.
102. van Bommel EJM, de Jongh RT, Brands M, Heijboer AC, den Heijer M, Serlie MJ, et al. The Osteoblast: Linking Glucocorticoid-Induced Osteoporosis and Hyperglycaemia? A post-hoc Analysis of a Randomised Clinical Trial. Bone (2018) 112:173–6. doi: 10.1016/j.bone.2018.04.025
103. Kauh E, Mixson L, Malice MP, Mesens S, Ramael S, Burke J, et al. Prednisone Affects Inflammation, Glucose Tolerance, and Bone Turnover Within Hours of Treatment in Healthy Individuals. Eur J Endocrinol (2012) 166:459–67. doi: 10.1530/EJE-11-0751
104. Fleishaker DL, Mukherjee A, Whaley FS, Daniel S, Zeiher BG. Safety and Pharmacodynamic Dose Response of Short-Term Prednisone in Healthy Adult Subjects: A Dose Ranging, Randomized, Placebo-Controlled, Crossover Study. BMC Musculoskelet Disord (2016) 17:293. doi: 10.1186/s12891-016-1135-3
105. Ton FN, Gunawardene SC, Lee H, Neer RM. Effects of Low-Dose Prednisone on Bone Metabolism. J Bone Miner Res (2005) 20:464–70. doi: 10.1359/JBMR.041125
106. van Staa TP, Geusens P, Zhang B, Leufkens HG, Boonen A, Cooper C. Individual Fracture Risk and the Cost-Effectiveness of Bisphosphonates in Patients Using Oral Glucocorticoids. Rheumatol (Oxford) (2007) 46:460–6. doi: 10.1093/rheumatology/kel249
107. Kanis JA, Borgstrom F, Johnell O, Jonsson B. Cost-Effectiveness of Risedronate for the Treatment of Osteoporosis and Prevention of Fractures in Postmenopausal Women. Osteoporos Int (2004) 15:862–71. doi: 10.1007/s00198-004-1643-0
108. Kanis JA, Johansson H, Oden A, McCloskey EV. Guidance for the Adjustment of FRAX According to the Dose of Glucocorticoids. Osteoporos Int (2011) 22:809–16. doi: 10.1007/s00198-010-1524-7
109. Natsui K, Tanaka K, Suda M, Yasoda A, Sakuma Y, Ozasa A, et al. High-Dose Glucocorticoid Treatment Induces Rapid Loss of Trabecular Bone Mineral Density and Lean Body Mass. Osteoporos Int (2006) 17:105–8. doi: 10.1007/s00198-005-1923-3
110. Mugisha A, Bergmann P, Kinnard V, Iconaru L, Baleanu F, Charles A, et al. MOF/Hip Fracture Ratio in a Belgian Cohort of Post-Menopausal Women (FRISBEE): Potential Impact on the FRAX(R) Score. Calcif Tissue Int (2021) 109:600–4. doi: 10.1007/s00223-021-00875-8
111. Baleanu F, Iconaru L, Charles A, Kinnard V, Fils JF, Moreau M, et al. Independent External Validation of FRAX and Garvan Fracture Risk Calculators: A Sub-Study of the FRISBEE Cohort. JBMR Plus (2021) 5:e10532. doi: 10.1002/jbm4.10532
112. McCloskey EV, Oden A, Harvey NC, Leslie WD, Hans D, Johansson H, et al. A Meta-Analysis of Trabecular Bone Score in Fracture Risk Prediction and Its Relationship to FRAX. J Bone Miner Res (2016) 31:940–8. doi: 10.1002/jbmr.2734
113. Conley RB, Adib G, Adler RA, Akesson KE, Alexander IM, Amenta KC, et al. Secondary Fracture Prevention: Consensus Clinical Recommendations From a Multistakeholder Coalition. J Bone Miner Res (2020) 35:36–52. doi: 10.1002/jbmr.3877
114. Shen J, Griffith JF, Zhu TY, Tang P, Kun EW, Lee VK, et al. Microstructure, and Strength Can Discriminate Vertebral Fracture in Patients on Long-Term Steroid Treatment. J Clin Endocrinol Metab (2018) 103:3340–9. doi: 10.1210/jc.2018-00490
115. Liu Y, Dimango E, Bucovsky M, Agarwal S, Nishiyama K, Guo XE, et al. Abnormal Microarchitecture and Stiffness in Postmenopausal Women Using Chronic Inhaled Glucocorticoids. Osteoporos Int (2018) 29:2121–7. doi: 10.1007/s00198-018-4591-9
116. Zhu TY, Griffith JF, Qin L, Hung VW, Fong TN, Au SK, et al. Cortical Thinning and Progressive Cortical Porosity in Female Patients With Systemic Lupus Erythematosus on Long-Term Glucocorticoids: A 2-Year Case-Control Study. Osteoporos Int (2015) 26:1759–71. doi: 10.1007/s00198-015-3077-2
117. Sutter S, Nishiyama KK, Kepley A, Zhou B, Wang J, McMahon DJ, et al. Abnormalities in Cortical Bone, Trabecular Plates, and Stiffness in Postmenopausal Women Treated With Glucocorticoids. J Clin Endocrinol Metab (2014) 99:4231–40. doi: 10.1210/jc.2014-2177
118. Graeff C, Marin F, Petto H, Kayser O, Reisinger A, Pena J, et al. High Resolution Quantitative Computed Tomography-Based Assessment of Trabecular Microstructure and Strength Estimates by Finite-Element Analysis of the Spine, But Not DXA, Reflects Vertebral Fracture Status in Men With Glucocorticoid-Induced Osteoporosis. Bone (2013) 52:568–77. doi: 10.1016/j.bone.2012.10.036
119. Mellibovsky L, Prieto-Alhambra D, Mellibovsky F, Guerri-Fernandez R, Nogues X, Randall C, et al. Bone Tissue Properties Measurement by Reference Point Indentation in Glucocorticoid-Induced Osteoporosis. J Bone Miner Res (2015) 30:1651–6. doi: 10.1002/jbmr.2497
120. Kalpakcioglu BB, Engelke K, Genant HK. Advanced Imaging Assessment of Bone Fragility in Glucocorticoid-Induced Osteoporosis. Bone (2011) 48:1221–31. doi: 10.1016/j.bone.2011.02.005
121. Moriwaki K, Fukuda H. Cost-Effectiveness of Implementing Guidelines for the Treatment of Glucocorticoid-Induced Osteoporosis in Japan. Osteoporos Int (2019) 30:299–310. doi: 10.1007/s00198-018-4798-9
122. Murphy DR, Smolen LJ, Klein TM, Klein RW. The Cost Effectiveness of Teriparatide as a First-Line Treatment for Glucocorticoid-Induced and Postmenopausal Osteoporosis Patients in Sweden. BMC Musculoskelet Disord (2012) 13:213. doi: 10.1186/1471-2474-13-213
123. Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M. Glucocorticoid-Induced Osteoporosis: A Systematic Review and Cost-Utility Analysis. Health Technol Assess (2007) 11:iii–iv, ix-xi, 1-231. doi: 10.3310/hta11070
124. Brecht JG, Kruse HP, Felsenberg D, Mohrke W, Oestreich A, Huppertz E. Pharmacoeconomic Analysis of Osteoporosis Treatment With Risedronate. Int J Clin Pharmacol Res (2003) 23:93–105.
125. Lee TH, Song YJ, Kim H, Sung YK, Cho SK. Intervention Thresholds for Treatment in Patients With Glucocorticoid-Induced Osteoporosis: Systematic Review of Guidelines. J Bone Metab (2020) 27:247–59. doi: 10.11005/jbm.2020.27.4.247
126. Campbell IA, Douglas JG, Francis RM, Prescott RJ, Reid DM. Research Committee of the British Thoracic, Hormone Replacement Therapy (HRT) or Etidronate for Osteoporosis in Postmenopausal Asthmatics on Glucocorticoids: A Randomised Factorial Trial. Scott Med J (2009) 54:21–5. doi: 10.1258/rsmsmj.54.1.21
127. Lems WF, Baak MM, van Tuyl LH, Lodder MC, Dijkmans BA, Boers M. One-Year Effects of Glucocorticoids on Bone Density: A Meta-Analysis in Cohorts on High and Low-Dose Therapy. RMD Open (2016) 2:e000313. doi: 10.1136/rmdopen-2016-000313
128. Palmer SC, Chung EY, McGregor DO, Bachmann F, Strippoli GF. Interventions for Preventing Bone Disease in Kidney Transplant Recipients. Cochrane Database Syst Rev (2019) 10:CD005015. doi: 10.1002/14651858.CD005015.pub4
129. Zhao J, Wang C, Hu Z. Efficacy and Safety of Bisphosphonates for Osteoporosis or Osteopenia in Cardiac Transplant Patients: A Meta-Analysis. Transplant Proc (2015) 47:2957–64. doi: 10.1016/j.transproceed.2015.10.049
130. Kasturi KS, Chennareddygari S, Mummadi RR. Effect of Bisphosphonates on Bone Mineral Density in Liver Transplant Patients: A Meta-Analysis and Systematic Review of Randomized Controlled Trials. Transpl Int (2010) 23:200–7. doi: 10.1111/j.1432-2277.2009.00976.x
131. Stein EM, Ortiz D, Jin Z, McMahon DJ, Shane E. Prevention of Fractures After Solid Organ Transplantation: A Meta-Analysis. J Clin Endocrinol Metab (2011) 96:3457–65. doi: 10.1210/jc.2011-1448
132. Deng J, Silver Z, Huang E, Zheng E, Kavanagh K, Panicker J. The Effect of Calcium and Vitamin D Compounds on Bone Mineral Density in Patients Undergoing Glucocorticoid Therapies: A Network Meta-Analysis. Clin Rheumatol (2021) 40:725–34. doi: 10.1007/s10067-020-05294-y
133. Homik J, Suarez-Almazor ME, Shea B, Cranney A, Wells G, Tugwell P. Calcium and Vitamin D for Corticosteroid-Induced Osteoporosis. Cochrane Database Syst Rev (2000) 2:CD000952. doi: 10.1002/14651858.CD000952
134. Bischoff-Ferrari HA, Dawson-Hughes B, Orav EJ, Staehelin HB, Meyer OW, Theiler R, et al. Monthly High-Dose Vitamin D Treatment for the Prevention of Functional Decline: A Randomized Clinical Trial. JAMA Intern Med (2016) 176:175–83. doi: 10.1001/jamainternmed.2015.7148
135. Burt LA, Billington EO, Rose MS, Raymond DA, Hanley DA, Boyd SK. Effect of High-Dose Vitamin D Supplementation on Volumetric Bone Density and Bone Strength: A Randomized Clinical Trial. JAMA (2019) 322:736–45. doi: 10.1001/jama.2019.11889
136. Waterhouse M, Sanguineti E, Baxter C, Duarte Romero B, McLeod DSA, English DR, et al. Vitamin D Supplementation and Risk of Falling: Outcomes From the Randomized, Placebo-Controlled D-Health Trial. J Cachexia Sarcopenia Muscle (2021) 12:1428–39. doi: 10.1002/jcsm.12759
137. Deng J, Silver Z, Huang E, Zheng E, Kavanagh K, Wen A, et al. Pharmacological Prevention of Fractures in Patients Undergoing Glucocorticoid Therapies: A Systematic Review and Network Meta-Analysis. Rheumatol (Oxford) (2021) 60:649–57. doi: 10.1093/rheumatology/keaa228
138. de Nijs RN, Jacobs JW, Algra A, Lems WF, Bijlsma JW. Prevention and Treatment of Glucocorticoid-Induced Osteoporosis With Active Vitamin D3 Analogues: A Review With Meta-Analysis of Randomized Controlled Trials Including Organ Transplantation Studies. Osteoporos Int (2004) 15:589–602. doi: 10.1007/s00198-004-1614-5
139. Di Munno O, Beghe F, Favini P, Di Giuseppe P, Pontrandolfo A, Occhipinti G, et al. Prevention of Glucocorticoid-Induced Osteopenia: Effect of Oral 25-Hydroxyvitamin D and Calcium. Clin Rheumatol (1989) 8:202–7. doi: 10.1007/BF02030075
140. Garcia-Delgado I, Prieto S, Gil-Fraguas L, Robles E, Rufilanchas JJ, Hawkins F. Calcitonin, Etidronate, and Calcidiol Treatment in Bone Loss After Cardiac Transplantation. Calcif Tissue Int (1997) 60:155–9. doi: 10.1007/s002239900206
141. Talalaj M, Gradowska L, Marcinowska-Suchowierska E, Durlik M, Gaciong Z, Lao M. Efficiency of Preventive Treatment of Glucocorticoid-Induced Osteoporosis With 25-Hydroxyvitamin D3 and Calcium in Kidney Transplant Patients. Transplant Proc (1996) 28:3485–7.
142. Jackson RD, LaCroix AZ, Gass M, Wallace RB, Robbins J, Lewis CE, et al. Calcium Plus Vitamin D Supplementation and the Risk of Fractures. N Engl J Med (2006) 354:669–83. doi: 10.1056/NEJMoa055218
143. Billington EO, Burt LA, Rose MS, Davison EM, Gaudet S, Kan M, et al. Safety of High-Dose Vitamin D Supplementation: Secondary Analysis of a Randomized Controlled Trial. J Clin Endocrinol Metab (2020) 105:1261–73. doi: 10.1210/clinem/dgz212
144. Buckley LM, Hillner BE. A Cost Effectiveness Analysis of Calcium and Vitamin D Supplementation, Etidronate, and Alendronate in the Prevention of Vertebral Fractures in Women Treated With Glucocorticoids. J Rheumatol (2003) 30:132–8.
145. Adachi JD, Saag KG, Delmas PD, Liberman UA, Emkey RD, Seeman E, et al. Two-Year Effects of Alendronate on Bone Mineral Density and Vertebral Fracture in Patients Receiving Glucocorticoids: A Randomized, Double-Blind, Placebo-Controlled Extension Trial. Arthritis Rheum (2001) 44:202–11. doi: 10.1002/1529-0131(200101)44:1<202::AID-ANR27>3.0.CO;2-W
146. Cohen S, Levy RM, Keller M, Boling E, Emkey RD, Greenwald M, et al. Risedronate Therapy Prevents Corticosteroid-Induced Bone Loss: A Twelve-Month, Multicenter, Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study. Arthritis Rheum (1999) 42:2309–18. doi: 10.1002/1529-0131(199911)42:11<2309::AID-ANR8>3.0.CO;2-K
147. McKeown E, Bykerk VP, De Leon F, Bonner A, Thorne C, Hitchon CA, et al. Quality Assurance Study of the Use of Preventative Therapies in Glucocorticoid-Induced Osteoporosis in Early Inflammatory Arthritis: Results From the CATCH Cohort. Rheumatol (Oxford) (2012) 51:1662–9. doi: 10.1093/rheumatology/kes079
148. Sambrook PN, Kotowicz M, Nash P, Styles CB, Naganathan V, Henderson-Briffa KN, et al. Prevention and Treatment of Glucocorticoid-Induced Osteoporosis: A Comparison of Calcitriol, Vitamin D Plus Calcium, and Alendronate Plus Calcium. J Bone Miner Res (2003) 18:919–24. doi: 10.1359/jbmr.2003.18.5.919
149. Allen CS, Yeung JH, Vandermeer B, Homik J. Bisphosphonates for Steroid-Induced Osteoporosis. Cochrane Database Syst Rev (2016) 10:CD001347. doi: 10.1002/14651858.CD001347.pub2
150. Liu Z, Zhang M, Shen Z, Ke J, Zhang D, Yin F. Efficacy and Safety of 18 Anti-Osteoporotic Drugs in the Treatment of Patients With Osteoporosis Caused by Glucocorticoid: A Network Meta-Analysis of Randomized Controlled Trials. PloS One (2020) 15:e0243851. doi: 10.1371/journal.pone.0243851
151. Mok CC, Ying KY, To CH, Ho LY, Yu KL, Lee HK, et al. Raloxifene for Prevention of Glucocorticoid-Induced Bone Loss: A 12-Month Randomised Double-Blinded Placebo-Controlled Trial. Ann Rheum Dis (2011) 70:778–84. doi: 10.1136/ard.2010.143453
152. Amiche MA, Albaum JM, Tadrous M, Pechlivanoglou P, Levesque LE, Adachi JD, et al. Efficacy of Osteoporosis Pharmacotherapies in Preventing Fracture Among Oral Glucocorticoid Users: A Network Meta-Analysis. Osteoporos Int (2016) 27:1989–98. doi: 10.1007/s00198-015-3476-4
153. Cho SK, Kim H, Lee J, Nam E, Lee S, Choi YY, et al. Effectiveness of Bazedoxifene in Preventing Glucocorticoid-Induced Bone Loss in Rheumatoid Arthritis Patients. Arthritis Res Ther (2021) 23:176. doi: 10.1186/s13075-021-02564-1
154. Wang YK, Zhang YM, Qin SQ, Wang X, Ma T, Guo JB, et al. Effects of Alendronate for Treatment of Glucocorticoid-Induced Osteoporosis: A Meta-Analysis of Randomized Controlled Trials. Med (Baltimore) (2018) 97:e12691. doi: 10.1097/MD.0000000000012691
155. Yamaguchi Y, Morita T, Kumanogoh A. The Therapeutic Efficacy of Denosumab for the Loss of Bone Mineral Density in Glucocorticoid-Induced Osteoporosis: A Meta-Analysis. Rheumatol Adv Pract (2020) 4:rkaa008. doi: 10.1093/rap/rkaa008
156. Iki M, Fujimori K, Nakatoh S, Tamaki J, Ishii S, Okimoto N, et al. Delayed Initiation of Anti-Osteoporosis Medications Increases Subsequent Hip and Vertebral Fractures in Patients on Long-Term Glucocorticoid Therapy: A Nationwide Health Insurance Claims Database Study in Japan. Bone (2022) 160:116396. doi: 10.1016/j.bone.2022.116396
157. Khan AA, Morrison A, Hanley DA, Felsenberg D, McCauley LK, O'Ryan F, et al. International Task Force on Osteonecrosis of the, Diagnosis and Management of Osteonecrosis of the Jaw: A Systematic Review and International Consensus. J Bone Miner Res (2015) 30:3–23. doi: 10.1002/jbmr.2405
158. Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, et al. Atypical Subtrochanteric and Diaphyseal Femoral Fractures: Second Report of a Task Force of the American Society for Bone and Mineral Research. J Bone Miner Res (2014) 29:1–23. doi: 10.1002/jbmr.1998
159. Abtahi S, Driessen JHM, Burden AM, Souverein PC, van den Bergh JP, van Staa TP, et al. Concomitant Use of Oral Glucocorticoids and Proton Pump Inhibitors and Risk of Osteoporotic Fractures Among Patients With Rheumatoid Arthritis: A Population-Based Cohort Study. Ann Rheum Dis (2021) 80:423–31. doi: 10.1136/annrheumdis-2020-218758
160. Liu CL, Lee HC, Chen CC, Cho DY. Head-To-Head Comparisons of Bisphosphonates and Teriparatide in Osteoporosis: A Meta-Analysis. Clin Invest Med (2017) 40:E146–57. doi: 10.25011/cim.v40i3.28394
161. Ding L, Hu J, Wang D, Liu Q, Mo Y, Tan X, et al. Efficacy and Safety of First- and Second-Line Drugs to Prevent Glucocorticoid-Induced Fractures. J Clin Endocrinol Metab (2020) 105:600–13. doi: 10.1210/clinem/dgz023
162. Saag KG, Shane E, Boonen S, Marin F, Donley DW, Taylor KA, et al. Teriparatide or Alendronate in Glucocorticoid-Induced Osteoporosis. N Engl J Med (2007) 357:2028–39. doi: 10.1056/NEJMoa071408
163. Reid DM, Devogelaer JP, Saag K, Roux C, Lau CS, Reginster JY, et al. Zoledronic Acid and Risedronate in the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis (HORIZON): A Multicentre, Double-Blind, Double-Dummy, Randomised Controlled Trial. Lancet (2009) 373:1253–63. doi: 10.1016/S0140-6736(09)60250-6
164. Saag KG, Wagman RB, Geusens P, Adachi JD, Messina OD, Emkey R, et al. Denosumab Versus Risedronate in Glucocorticoid-Induced Osteoporosis: A Multicentre, Randomised, Double-Blind, Active-Controlled, Double-Dummy, non-Inferiority Study. Lancet Diabetes Endocrinol (2018) 6:445–54. doi: 10.1016/S2213-8587(18)30075-5
165. Saag KG, Zanchetta JR, Devogelaer JP, Adler RA, Eastell R, See K, et al. Effects of Teriparatide Versus Alendronate for Treating Glucocorticoid-Induced Osteoporosis: Thirty-Six-Month Results of a Randomized, Double-Blind, Controlled Trial. Arthritis Rheum (2009) 60:3346–55. doi: 10.1002/art.24879
166. Fobelo Lozano MJ, Sanchez-Fidalgo S. Adherence and Preference of Intravenous Zoledronic Acid for Osteoporosis Versus Other Bisphosphonates. Eur J Hosp Pharm (2019) 26:4–9. doi: 10.1136/ejhpharm-2017-001258
167. Tsai JN, Uihlein AV, Lee H, Kumbhani R, Siwila-Sackman E, McKay EA, et al. Teriparatide and Denosumab, Alone or Combined, in Women With Postmenopausal Osteoporosis: The DATA Study Randomised Trial. Lancet (2013) 382:50–6. doi: 10.1016/S0140-6736(13)60856-9
168. Karras D, Stoykov I, Lems WF, Langdahl BL, Ljunggren O, Barrett A, et al. Effectiveness of Teriparatide in Postmenopausal Women With Osteoporosis and Glucocorticoid Use: 3-Year Results From the EFOS Study. J Rheumatol (2012) 39:600–9. doi: 10.3899/jrheum.110947
169. Kobayakawa T, Miyazaki A, Kanayama Y, Hirano Y, Takahashi J, Suzuki T, et al. Comparable Efficacy of Denosumab and Romosozumab in Patients With Rheumatoid Arthritis Receiving Glucocorticoid Administration. Mod Rheumatol (2022). doi: 10.1093/mr/roac014
170. Saag KG, Emkey R, Schnitzer TJ, Brown JP, Hawkins F, Goemaere S, et al. Alendronate for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Glucocorticoid-Induced Osteoporosis Intervention Study Group. N Engl J Med (1998) 339:292–9. doi: 10.1056/NEJM199807303390502
171. Wallach S, Cohen S, Reid DM, Hughes RA, Hosking DJ, Laan RF, et al. Effects of Risedronate Treatment on Bone Density and Vertebral Fracture in Patients on Corticosteroid Therapy. Calcif Tissue Int (2000) 67:277–85. doi: 10.1007/s002230001146
172. Axelsson KF, Nilsson AG, Wedel H, Lundh D, Lorentzon M. Association Between Alendronate Use and Hip Fracture Risk in Older Patients Using Oral Prednisolone. JAMA (2017) 318:146–55. doi: 10.1001/jama.2017.8040
173. Bergman J, Nordstrom A, Nordstrom P. Alendronate Use and the Risk of Nonvertebral Fracture During Glucocorticoid Therapy: A Retrospective Cohort Study. J Clin Endocrinol Metab (2018) 103:306–13. doi: 10.1210/jc.2017-01912
174. Amiche MA, Levesque LE, Gomes T, Adachi JD, Cadarette SM. Effectiveness of Oral Bisphosphonates in Reducing Fracture Risk Among Oral Glucocorticoid Users: Three Matched Cohort Analyses. J Bone Miner Res (2018) 33:419–29. doi: 10.1002/jbmr.3318
175. Overman RA, Gourlay ML, Deal CL, Farley JF, Brookhart MA, Layton JB. Fracture Rate Associated With Quality Metric-Based Anti-Osteoporosis Treatment in Glucocorticoid-Induced Osteoporosis. Osteoporos Int (2015) 26:1515–24. doi: 10.1007/s00198-014-3022-9
176. Thomas T, Horlait S, Ringe JD, Abelson A, Gold DT, Atlan P, et al. Oral Bisphosphonates Reduce the Risk of Clinical Fractures in Glucocorticoid-Induced Osteoporosis in Clinical Practice. Osteoporos Int (2013) 24:263–9. doi: 10.1007/s00198-012-2060-4
177. Black DM, Geiger EJ, Eastell R, Vittinghoff E, Li BH, Ryan DS, et al. Atypical Femur Fracture Risk Versus Fragility Fracture Prevention With Bisphosphonates. N Engl J Med (2020) 383:743–53. doi: 10.1056/NEJMoa1916525
178. Hayes KN, Brown KA, Cheung AM, Kim SA, Juurlink DN, Cadarette SM. Comparative Fracture Risk During Osteoporosis Drug Holidays After Long-Term Risedronate Versus Alendronate Therapy : A Propensity Score-Matched Cohort Study. Ann Intern Med (2022) 175:335–43. doi: 10.7326/M21-2512
179. Gilsenan A, Midkiff K, Harris D, Kellier-Steele N, McSorley D, Andrews EB. Teriparatide Did Not Increase Adult Osteosarcoma Incidence in a 15-Year US Postmarketing Surveillance Study. J Bone Miner Res (2021) 36:244–51. doi: 10.1002/jbmr.4188
180. Coleman R, Hadji P, Body JJ, Santini D, Chow E, Terpos E, et al. Bone Health in Cancer: ESMO Clinical Practice Guidelines. Ann Oncol (2020) 31:1650–63. doi: 10.1016/j.annonc.2020.07.019
181. Shapiro CL, Van Poznak C, Lacchetti C, Kirshner J, Eastell R, Gagel R, et al. Management of Osteoporosis in Survivors of Adult Cancers With Nonmetastatic Disease: ASCO Clinical Practice Guideline. J Clin Oncol (2019) 37:2916–46. doi: 10.1200/JCO.19.01696
182. Saag KG, Pannacciulli N, Geusens P, Adachi JD, Messina OD, Morales-Torres J, et al. Denosumab Versus Risedronate in Glucocorticoid-Induced Osteoporosis: Final Results of a Twenty-Four-Month Randomized, Double-Blind, Double-Dummy Trial. Arthritis Rheumatol (2019) 71:1174–84. doi: 10.1002/art.40874
183. Geusens P, Bevers MS, van Rietbergen B, Messina OD, Lespessailles E, Oliveri B, et al. Effect of Denosumab Compared With Risedronate on Bone Strength in Patients Initiating or Continuing Glucocorticoid Treatment. J Bone Miner Res (2022). doi: 10.1002/jbmr.4551
184. Mok CC, Ho LY, Leung SMT, Cheung HN, Chen SPL, Ma KM. Denosumab Versus Alendronate in Long-Term Glucocorticoid Users: A 12-Month Randomized Controlled Trial. Bone (2021) 146:115902. doi: 10.1016/j.bone.2021.115902
185. Tsourdi E, Zillikens MC, Meier C, Body JJ, Gonzalez Rodriguez E, Anastasilakis AD, et al. Fracture Risk and Management of Discontinuation of Denosumab Therapy: A Systematic Review and Position Statement by ECTS. J Clin Endocrinol Metab (2020) 106:264–81. doi: 10.1210/clinem/dgaa756
186. Oelzner P, Eidner T, Pfeil A. [Glucocorticoid-Induced Osteoporosis-Focus Treatment (Part 2)]. Z Rheumatol (2022) 81:125–33. doi: 10.1007/s00393-021-01128-7
187. Briot K, Cortet B, Roux C, Fardet L, Abitbol V, Bacchetta J, et al. 2014 Update of Recommendations on the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Joint Bone Spine (2014) 81:493–501. doi: 10.1016/j.jbspin.2014.10.001
188. Gourlay ML, Fine JP, Preisser JS, May RC, Li C, Lui LY, et al. Bone-Density Testing Interval and Transition to Osteoporosis in Older Women. N Engl J Med (2012) 366:225–33. doi: 10.1056/NEJMoa1107142
189. van de Laarschot DM, Smits AA, Buitendijk SK, Stegenga MT, Zillikens MC. Screening for Atypical Femur Fractures Using Extended Femur Scans by DXA. J Bone Miner Res (2017) 32:1632–9. doi: 10.1002/jbmr.3164
190. Sato H, Takai C, Kondo N, Kurosawa Y, Hasegawa E, Wakamatsu A, et al. Cumulative Incidence of Femoral Localized Periosteal Thickening (Beaking) Preceding Atypical Femoral Fractures in Patients With Rheumatoid Arthritis. Osteoporos Int (2021) 32:363–75. doi: 10.1007/s00198-020-05601-y
191. Cheung AM, McKenna MJ, van de Laarschot DM, Zillikens MC, Peck V, Srighanthan J, et al. Detection of Atypical Femur Fractures. J Clin Densitom (2019) 22:506–16. doi: 10.1016/j.jocd.2019.07.003
192. Harvey NC, Gluer CC, Binkley N, McCloskey EV, Brandi ML, Cooper C, et al. Trabecular Bone Score (TBS) as a New Complementary Approach for Osteoporosis Evaluation in Clinical Practice. Bone (2015) 78:216–24. doi: 10.1016/j.bone.2015.05.016
193. Leib ES, Winzenrieth R. Bone Status in Glucocorticoid-Treated Men and Women. Osteoporos Int (2016) 27:39–48. doi: 10.1007/s00198-015-3211-1
194. Florez H, Hernandez-Rodriguez J, Muxi A, Carrasco JL, Prieto-Gonzalez S, Cid MC, et al. Trabecular Bone Score Improves Fracture Risk Assessment in Glucocorticoid-Induced Osteoporosis. Rheumatol (Oxford) (2020) 59:1574–80. doi: 10.1093/rheumatology/kez464
195. Nowakowska-Plaza A, Wronski J, Sudol-Szopinska I, Gluszko P. Clinical Utility of Trabecular Bone Score (TBS) in Fracture Risk Assessment of Patients With Rheumatic Diseases Treated With Glucocorticoids. Horm Metab Res (2021) 53:499–503. doi: 10.1055/a-1528-7261
196. Lee KA, Kim J, Kim HJ, Kim HS. Discriminative Ability of Trabecular Bone Score Over Bone Mineral Density for Vertebral and Fragility Fracture in Patients Treated With Long-Term and Low-Dose Glucocorticoid. Int J Rheum Dis (2021) 24:1053–60. doi: 10.1111/1756-185X.14164
197. Saag KG, Agnusdei D, Hans D, Kohlmeier LA, Krohn KD, Leib ES, et al. Trabecular Bone Score in Patients With Chronic Glucocorticoid Therapy-Induced Osteoporosis Treated With Alendronate or Teriparatide. Arthritis Rheumatol (2016) 68:2122–8. doi: 10.1002/art.39726
Keywords: adults, Cushing syndrome, glucocorticoid-induced osteoporosis, glucocorticoids, osteoporosis, prevention
Citation: Laurent MR, Goemaere S, Verroken C, Bergmann P, Body J-J, Bruyère O, Cavalier E, Rozenberg S, Lapauw B and Gielen E (2022) Prevention and Treatment of Glucocorticoid-Induced Osteoporosis in Adults: Consensus Recommendations From the Belgian Bone Club. Front. Endocrinol. 13:908727. doi: 10.3389/fendo.2022.908727
Received: 30 March 2022; Accepted: 02 May 2022;
Published: 09 June 2022.
Edited by:
Melanie Haffner-Luntzer, University of Ulm, GermanyReviewed by:
Elena Tsourdi, Technical University Dresden, GermanyJan Josef Stepan, Charles University, Czechia
Copyright © 2022 Laurent, Goemaere, Verroken, Bergmann, Body, Bruyère, Cavalier, Rozenberg, Lapauw and Gielen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michaël R. Laurent, bWljaGFlbC5sYXVyZW50QGltZWxkYS5iZQ==