 Oana Popa
Oana Popa Robert Alexandru Barna
Robert Alexandru Barna Andreea Borlea
Andreea Borlea Marioara Cornianu
Marioara Cornianu Alis Dema2
Alis Dema2 Dana Stoian
Dana Stoian- 1Endocrinology Department, Centre of Molecular Research in Nephrology and Vascular Disease, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania
- 2Discipline of Morphopathology, Department of Microscopic Morphology, ANAPATMOL Research Centre, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania
Introduction: The COVID-19 pandemic had a significant impact on the healthcare system, leading to a prioritization of hospital admissions in many countries. Romania was no exception, and it had to restrict patient access to medical services in hospitals with chronic diseases and oncological pathology, including thyroid cancer. This study aimed to compare the clinical and pathological factors of patients with nodular thyroid disease diagnosed and surgically treated during the two years before and after the COVID-19 pandemic, in a single medical institution.
Methods: The retrospective study included 1505 patients who were diagnosed and operated on for nodular thyroid disease between January 2018 and December 2021. The patients were divided into two groups: the “PRECOVID” group (January 2018 to February 2020), and the “POSTCOVID” group (March 2020 to December 2021). The analyzed parameters included patients’ gender, age, preoperative diagnosis, type of surgical intervention, and pathological diagnosis.
Results: A significant decrease was observed in the number of surgeries performed for thyroid nodular disease during the COVID-19 pandemic period (450 versus 1055 cases, p<0.00001). There was a significant decrease in the number of surgical reinterventions (0.9% in the POSTCOVID group versus 2.9% in the PRECOVID group, p=0.01) and a significant increase in the number of total thyroidectomies (84.9% in the POSTCOVID group versus 80.1% in the PRECOVID group, p=0.02). We also observed a higher incidence of malignant/borderline tumors in the POSTCOVID group compared to the PRECOVID group (p=0.04) and a significantly higher frequency of aggressive forms of thyroid cancer in the POSTCOVID group (p=0.0006).
Discussion: The COVID-19 pandemic had a significant impact on the surgical management of nodular thyroid disease, resulting in a decrease in surgeries and a change in the type of surgical interventions performed. The higher incidence of malignant/borderline tumors diagnosed during the pandemic highlights the importance of timely diagnosis and treatment of thyroid nodules to prevent cancer progression.
1 Introduction
The healthcare system in our country, similar to Europe, starting from March 2020 (1), had to adjust and prioritize hospital admissions to cope with the overwhelming wave of COVID-19-positive cases. The state of emergency and lockdown, active between March 15, 2020, and May 15, 2020 (2), restricted the access of patients with chronic pathology to medical services in hospitals, a situation often encountered worldwide and mentioned in numerous studies (3–8). Within a relatively short period, specific protocols and guidelines were developed, recommending the rescheduling of certain surgical interventions, including those in the oncology field (9–11).
Despite these inconveniences, medical teams consisting of endocrinologists, surgeons, radiologists, and pathologists at our institution, the largest hospital in Western Romania, evaluated patients presenting with nodular thyroid disease and selected patients that needed immediate medical attention. Each case and therapeutic decision was carefully analyzed from the perspective of the benefit-risk balance.
Thyroid carcinoma represents the most frequent endocrine malignant tumor worldwide. Recent studies state that the incidence has tripled in the last 20 years (12). The most recent World Health Organization (WHO) report estimates that in 2020, 449,000 new cases were diagnosed in female and 137,000 in male patients (13). Taking into consideration that thyroid cancer has a much more favorable outcome compared to other types of malignant tumors, recent guidelines mention that the diagnosis and surgical intervention could be postponed during the COVID-19 pandemic without detrimental effects on the patient’s survival and prognosis (14–16).
Our study aims to evaluate the clinical and pathological factors of patients with nodular thyroid disease by comparing the cases that were diagnosed and surgically treated during the 2 years before and after the COVID-19 pandemic in a single medical institution.
2 Materials and methods
We have conducted a retrospective study comprising all cases that were diagnosed with nodular thyroid disease and surgically treated in the three surgical departments of Timisoara County Hospital “Pius Brinzeu”, between January 2018 and December 2021. The patients were divided into two groups: the pre-pandemic group from January 2018 to February 2020 called the “PRECOVID” group (1055 cases) and the post-pandemic group from March 2020 to December 2021 called the “POSTCOVID” group (450 cases). The working protocol was approved by the hospital’s ethics committee and the patients signed informed consent.
All types of thyroid surgeries were included in the study, including total thyroidectomies, unilateral lobectomies, and reinterventions for completion of thyroidectomy after the diagnosis of malignancy or recurrence of suspicious nodules following initial lobectomy. All cases included in the study were examined by an experienced pathologist on HE-stained sections. Immunohistochemistry was performed in challenging cases.
The analyzed parameters were the patient’s gender, age, preoperative diagnosis, type of surgical intervention, and pathological diagnosis. For the systematization of the results and statistical analysis, non-tumor lesions were classified as follows: cases of nodular goiter (NG), nodular goiter evaluated through fine needle aspiration cytology (NG with FNAC), compressive nodular goiters (NG-compressive), hyperthyroid goiter (HTG), Graves’ disease (GD), and chronic autoimmune thyroiditis with thyroid nodules (CAT ± nodules). We have included borderline thyroid tumors/lesions, due to their uncertain malignant potential, in the malignant tumor category, alongside papillary thyroid carcinoma (PTC), micropapillary thyroid carcinoma (micro-PTC), follicular thyroid carcinoma (FTC), medullary thyroid carcinoma (MTC), anaplastic thyroid carcinoma (ATC), and other rare types of tumors. The borderline thyroid tumors/lesions included in the study are noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFT-P), well-differentiated thyroid tumors of uncertain malignant potential (WDT-UMP), and follicular tumors of uncertain malignant potential (FT-UMP).
Statistical analyses were conducted using MedCalc version 20.218 (MedCalc Software Ltd, Belgium). Quantitative variables were presented as mean ± standard deviation (SD) and qualitative data were reported in frequency and percentages. To compare the proportions between two independent samples, we used the two-sample proportion test, and for testing differences between two population means, we used the independent samples t-test. To assess the association between categorical variables, the chi-square test was used. All statistical tests were two-tailed unless otherwise specified. To establish statistical significance for the test results, we employed a predetermined threshold of p-value less than 0.05.
3 Results
The retrospective study included 1505 patients diagnosed and operated for nodular thyroid disease between January 2018 and December 2021, of which 36 patients underwent reintervention. Postoperatively, 992 non-tumor lesions (65.9%) and 513 malignant/borderline tumors (34.1%) were diagnosed.
The results of our study showed that there were significantly fewer surgeries performed for thyroid nodular disease during the time frame of 2020-2021, in comparison with the earlier years (450 cases versus 1055 cases, p<0.00001; Table 1). The distribution of the cases in the two groups was similar in terms of the patient’s gender and median age. We noticed a significant decrease in the number of surgical reinterventions in the post-COVID period (4 cases, 0.9%) compared to the PRECOVID group (32 cases, 2,9%: p=0.01) and an increase in the number of total thyroidectomies (382 cases, 84.9%) in comparison to the PRECOVID group (870 cases, 80,1%; p=0.02). We observed that significantly more cases of malignant/borderline tumors were diagnosed during the period of 2020-2021 compared to non-tumor lesions in the PRECOVID group (p=0.04).

Table 1 Clinical and pathological factors in the PRECOVID and POSTCOVID study groups.
Postoperatively, diagnosed non-tumor lesions presented a relatively similar distribution between the two study groups (Table 2). By analyzing the cases of malignant and borderline tumors, we noticed a slight increase in the number of cases diagnosed in the POSTCOVID period for the age groups of 31-50 years (13.7% versus 11.3%) and 51-65 years (14.1% versus 13.6%), but the number of cases increased significantly for patients over 65 years old (9.2% versus 6.5%), both for women (22.4% versus 19.6%), but especially for men (36.4% versus 23.6%), although the statistical analysis did not show a significant correlation.

Table 2 Distribution of tumoral and non-tumoral lesions among the two study groups.
The comparative study of malignant and borderline tumor cases (Figure 1) highlighted a statistically significant decrease in the number of PTC diagnosed and surgically treated during the post-COVID period (28.4% versus 39.7%, p=0.01), with a slight increase in the number of cases of micro-PTC (45.6% versus 41.2%) and a statistically significant increase in the number of patients with other malignant tumors (17.7% versus 7.6%, p=0.0006). During the time frame of 2020-2021, we identified 14 FTC, 9 MTC, and 5 ATC cases, as well as one case of diffuse large B-cell lymphoma and one case of thyroid metastasis from lung adenocarcinoma.
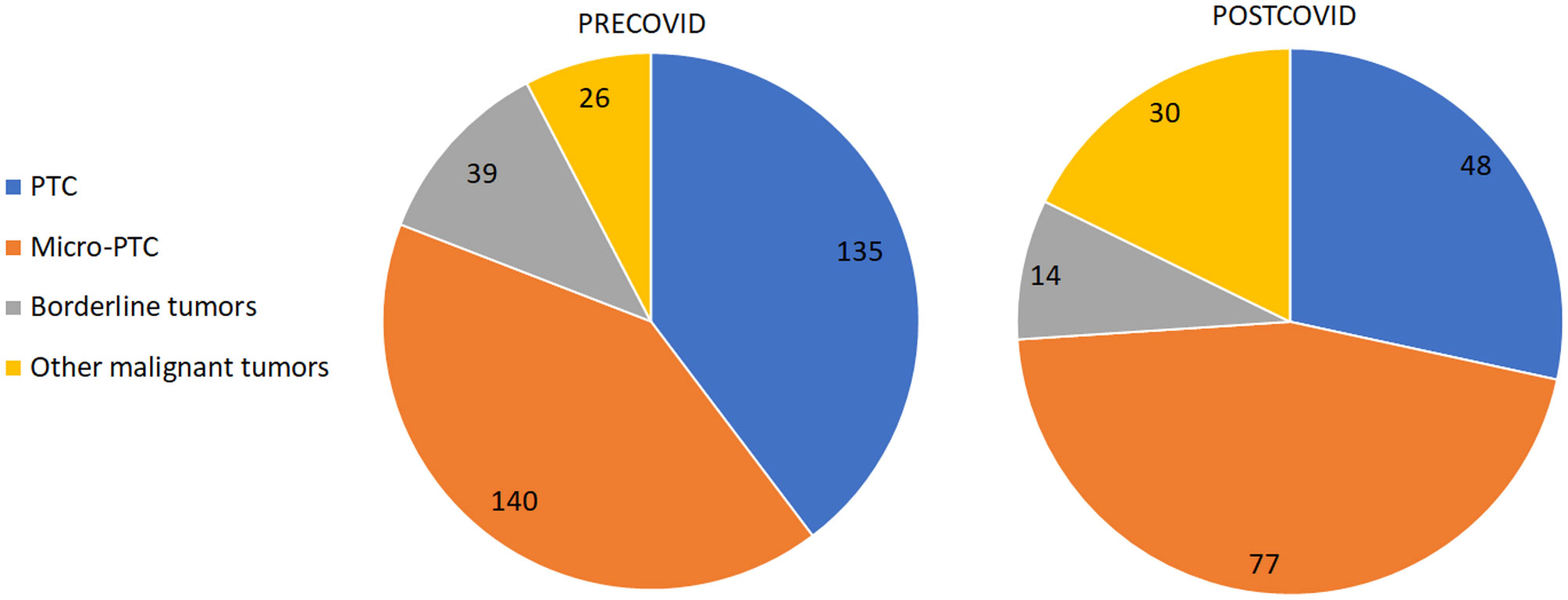
Figure 1 The comparison of tumor types between PRECOVID and POSTCOVID cases.
The comparative analysis of the study groups regarding the concordance between presurgical diagnosis and pathological diagnosis is presented in Table 3. In the POSTCOVID group, we observed more cancers and borderline lesions diagnosed in patients with NG (38.8%) compared to the PRECOVID group (27,5%). Significant increases in malignant lesions in the period of 2020-2021 were observed in patients diagnosed preoperatively with HTG (15.4% versus 9.3%), CAT ± nodules (40% versus 30.9%), and GD (33.3% versus 29,2%).
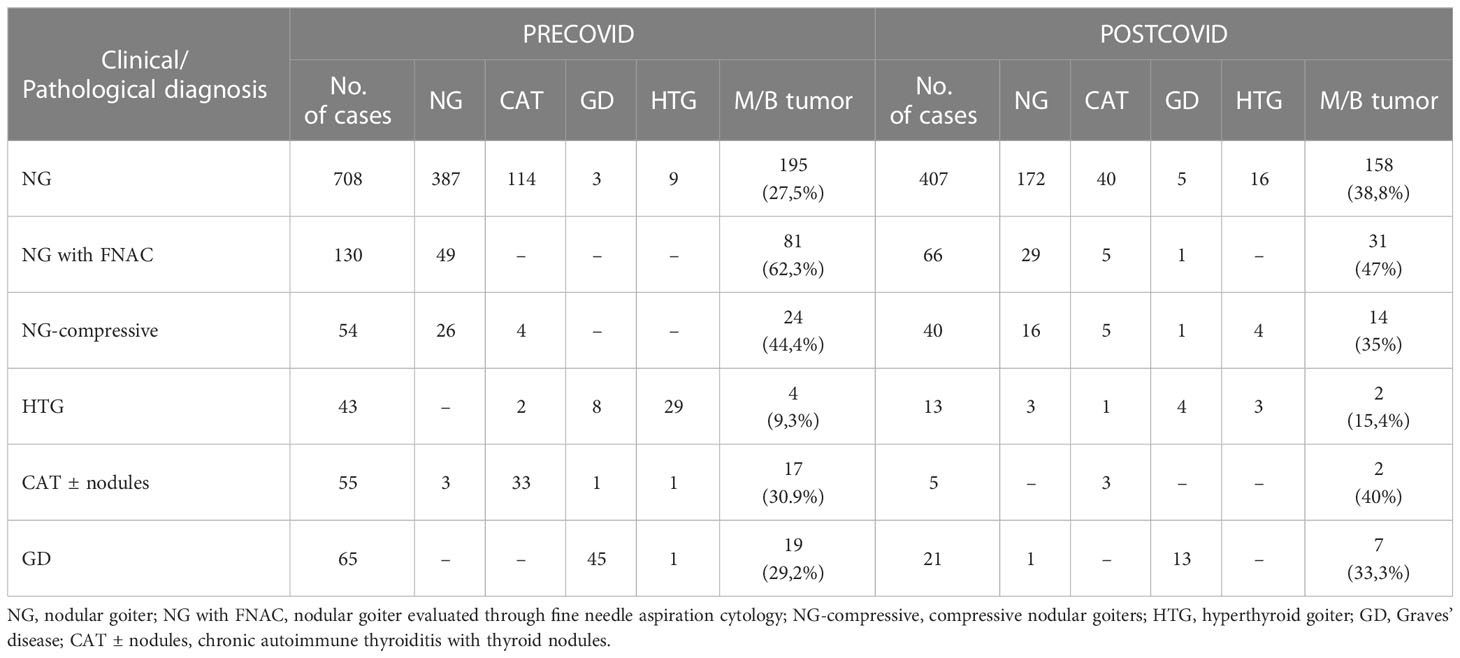
Table 3 The correspondence between presurgical diagnosis and surgical pathology reports.
4 Discussion
The WHO declared COVID-19 a global pandemic on the 11th of March 2020 (1). Social distancing measures and the state of lockdown have profoundly affected the healthcare system in almost all parts of the world (17). As the medical team focused primarily on COVID-positive patients, newly implemented oncology guidelines recommended short-term deferral of certain procedures and surgeries, including cases of aggressive cancers such as gastric, pancreatic, genitourinary, or melanoma (14, 18). Some studies have shown that 38.7% to 59% of cancer patients were advised to delay treatment (12, 19, 20).
Thyroid cancer is the most common endocrine malignancy, with surgical intervention being the first-line therapy. Although the mortality rate is less than 1 per 100,000, delaying treatment can lead to the local extension of neoplastic disease, requiring extensive surgical interventions and sometimes radioactive iodine treatment, with the risk of complications such as hypoparathyroidism, laryngeal recurrent nerve damage, and aesthetic complications due to poor scarring (14, 21). Some studies have shown that extensive surgical interventions and radioactive treatment do not influence the risk of recurrence and survival of patients with micro-PTC (22, 23). The recent guidelines of the American Thyroid Association recommend lobectomy for patients with PTC under 4 cm, without clinical evidence of local extension or lymph node metastasis (22).
The COVID pandemic has affected the diagnosis and surgical treatment of many oncological pathologies, including thyroid nodular disease and, consequently, thyroid cancer (14, 15, 24). Numerous guidelines developed by reputable societies in thyroid pathology recommended delaying surgical interventions for thyroid cancer, except for those cases that endanger patients’ lives (15, 16, 25). Studies by Medas et al. and Bakkar et al. have shown that there are no significant differences in the progression of patients with thyroid cancer before and after the COVID pandemic (26, 27). On the other hand, a study in China reported an increased incidence of severe prognostic factors, such as extrathyroidal extension, multiple tumors, and lymph node metastasis (12). In a study that analyzed the survival of patients with thyroid disease, 87.9% of clinicians expressed concern about delayed treatment during the pandemic (28).
We included in our study all patients that were diagnosed and operated on for thyroid nodular disease in a single medical institution, the largest hospital in western Romania, over 4 years (1505 patients): 2 years before and 2 years after the declaration of the COVID pandemic. We can report that the COVID pandemic has significantly affected the diagnosis and treatment of patients with nodular thyroid disease. Between 2020 and 2021, 450 patients underwent thyroid surgery, significantly fewer patients than in the pre-pandemic period (1055 patients, p<0.00001). The two groups of patients were similar in terms of patient’s gender and age. Our results suggest that in the post-pandemic period, surgeons preferred total thyroidectomy as the first therapeutic option (POSTCOVID 84.9% versus PRECOVID 80.1%, p=0.02) and limited surgical reinterventions (POSTCOVID 0.9% versus PRECOVID 2,9%, p=0.01). Another important result of our study indicated an increase in the number of malignant tumors and borderline thyroid lesions in the post-pandemic years (37.9% versus 32.2%; p=0.04). Non-tumoral lesions showed a relatively similar distribution between the two study groups.
Thyroid cancers and borderline thyroid tumors were diagnosed more frequently in the POSTCOVID group in all age groups, especially in patients over 65 years old (9.2% versus 6.5%) and in men (36.4% versus 23.6%). Our results suggest that elderly patients had reduced access to healthcare due to the greater risk of infection and more severe complications associated with COVID-19.
One of the most important results of our study is the significantly higher frequency of aggressive pathological tumor types in the POSTCOVID group (17.7%) compared to the PRECOVID group (7.6%; p=0.0006). A plausible explanation could be the delay in diagnosis and surgical interventions in the immediate period following the declaration of the COVID pandemic. Certain types of thyroid cancer, such as FTC, MTC, or ATC, are characterized by rapid growth, extrathyroidal extension, and early lymph node metastases (12). In the case of these malignant tumors, delaying surgical intervention, even for a few months, is not desirable or advisable.
Although significantly fewer patients with NG were operated on during the period of 2020-2021, the number of cases diagnosed with malignant tumors and borderline lesions was higher (POSTCOVID - 38.8% versus PRECOVID – 27,5%). Significant increases in malignant lesions in the period of 2020-2021 were also observed in patients diagnosed before surgery with HTG (15.4% versus 9.3%), CAT ± nodules (40% versus 30.9%), and GD (33.3% versus 29,2%)
Presurgical ultrasound (US) evaluation and risk stratification show excellent accuracy for conventional US, especially when combined with elastography assessment. Presurgical evaluation is needed to reduce the unnecessary number of surgical interventions (21, 29, 30). In our study, the high frequency of total thyroidectomies is justified by the increased number of diagnosed thyroid cancers, especially in the POSTCOVID group.
One of the limitations of our study is that the analysis was carried out in a single medical center. Multicenter research is needed to include a larger number of cases to be able to draw an accurate conclusion about the effects of the pandemic on patients with nodular thyroid disease. Additionally, not all patients suspected of thyroid cancer underwent fine-needle aspiration (FNA), which could lead to the underdiagnosis of aggressive forms of cancer.
5 Conclusion
Our results allow us to state that the COVID pandemic has significantly affected the diagnosis and treatment of patients with thyroid nodular disease. After the onset of the COVID pandemic, the number of patients diagnosed and operated on for nodular thyroid disease decreased dramatically. However, the number of thyroid cancer cases did significantly increase, especially for aggressive tumors such as FTC, CMT, and ATC, suggesting better presurgical evaluations of the cases. Between 2020 and 2021, the number of cases of thyroid cancer increased significantly for all age groups, particularly for elderly patients (aged 65 and older).
Under the exceptional conditions imposed by the pandemic, surgeons preferred total thyroidectomies over unilateral lobectomies or reinterventions.
Our study results suggest that delaying diagnosis and treatment during the COVID pandemic, even by a few months, is not the best option for patients with aggressive forms of thyroid cancer. However, multicenter studies are necessary to include a large case series to support our current observations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The working protocol was approved by the hospital’s ethics committee and the patients signed informed consent.
Author contributions
OP was involved in the conceptualization, methodology, validation, supervision, and reviewing and editing of the manuscript; RB performed statistical analysis and visualization. AB was involved in the investigation and writing the original draft; MC and AD were involved in the investigation, resources, and writing the original manuscript; DS was involved in the supervision, validation, reviewing, and editing of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta BioMed (2020) 91:157–60. doi: 10.23750/ABM.V91I1.9397
2. COVID-19 pandemic in Romania - Wikipedia. Available at: https://en.wikipedia.org/w/index.php?title=COVID-19_pandemic_in_Romania&oldid=1142425783 (Accessed May 1, 2023).
3. Duden GS, Gersdorf S, Stengler K. Global impact of the COVID-19 pandemic on mental health services: a systematic review. J Psychiatr Res (2022) 154:354–77. doi: 10.1016/J.JPSYCHIRES.2022.08.013
4. Kostopoulou E, Gkentzi D, Papasotiriou M, Fouzas S, Tagalaki A, Varvarigou A, et al. The impact of COVID-19 on paediatric emergency department visits. a one-year retrospective study. Pediatr Res (2022) 91:1257–62. doi: 10.1038/S41390-021-01815-W
5. McMaster T, Wright T, Mori K, Stelmach W, To H. Current and future use of telemedicine in surgical clinics during and beyond COVID-19: a narrative review. Ann Med Surg (Lond) (2021) 66:102378. doi: 10.1016/J.AMSU.2021.102378
6. Puricelli Perin DM, Christensen T, Burón A, Haas JS, Kamineni A, Pashayan N, et al. Interruption of cancer screening services due to COVID-19 pandemic: lessons from previous disasters. Prev Med Rep (2021) 23:101399. doi: 10.1016/J.PMEDR.2021.101399
7. Kendzerska T, Zhu DT, Gershon AS, Edwards JD, Peixoto C, Robillard R, et al. The effects of the health system response to the COVID-19 pandemic on chronic disease management: a narrative review. Risk Manag Healthc Policy (2021) 14:575–84. doi: 10.2147/RMHP.S293471
8. Kaczmarek K, Kalembkiewicz J, Jankowska M, Kalembkiewicz K, Narożnicki J, Lemiński A, et al. Did the COVID-19 pandemic restrict access to emergency urological services: assessment of reorganisation effectiveness for hospital treatment. Int J Environ Res Public Health (2023) 20(4):3735. doi: 10.3390/IJERPH20043735
9. Al-Jabir A, Kerwan A, Nicola M, Alsafi Z, Khan M, Sohrabi C, et al. Impact of the coronavirus (COVID-19) pandemic on surgical practice - part 1. Int J Surg (2020) 79:168–79. doi: 10.1016/J.IJSU.2020.05.022
10. Diaz A, Sarac BA, Schoenbrunner AR, Janis JE, Pawlik TM. Elective surgery in the time of COVID-19. Am J Surg (2020) 219:900–2. doi: 10.1016/J.AMJSURG.2020.04.014
11. Brindle ME, Gawande A. Managing COVID-19 in surgical systems. Ann Surg (2020) 272(1):e1–e2. doi: 10.1097/SLA.0000000000003923
12. Liu H, Zhan L, Guo L, Yu X, Li L, Feng H, et al. More aggressive cancer behaviour in thyroid cancer patients in the post-COVID-19 pandemic era: a retrospective study. Int J Gen Med (2021) 14:7197–206. doi: 10.2147/IJGM.S339998
13. Pizzato M, Li M, Vignat J, Laversanne M, Singh D, La Vecchia C, et al. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020. Lancet Diabetes Endocrinol (2022) 10:264–72. doi: 10.1016/S2213-8587(22)00035-3
14. Kim SH, Min E, Hwang YM, Choi YS, Yi JW. Impact of COVID-19 pandemic on thyroid surgery in a university hospital in south Korea. Cancers (Basel) (2022) 14:4338. doi: 10.3390/CANCERS14174338
15. Pramono LA. COVID-19 and thyroid diseases: how the pandemic situation affects thyroid disease patients. J ASEAN Fed Endocr Soc (2020) 35:155–7. doi: 10.15605/JAFES.035.02.01
16. Vrachimis A, Iakovou I, Giannoula E, Giovanella L. ENDOCRINOLOGY IN THE TIME OF COVID-19: management of thyroid nodules and cancer. Eur J Endocrinol (2020) 183:G41–8. doi: 10.1530/EJE-20-0269
17. Zhang X, Oluyomi A, Woodard L, Raza SA, Adel Fahmideh M, El-Mubasher O, et al. Individual-level determinants of lifestyle behavioral changes during COVID-19 lockdown in the united states: results of an online survey. Int J Environ Res Public Health (2021) 18:4364. doi: 10.3390/ijerph18084364
18. Garcia D, Siegel JB, Mahvi DA, Zhang B, Mahvi DM, Camp ER, et al. What is elective oncologic surgery in the time of COVID-19? a literature review of the impact of surgical delays on outcomes in patients with cancer. Clin Oncol Res (2020) 3:1–11. doi: 10.31487/j.COR.2020.06.05
19. Frey MK, Fowlkes RK, Badiner NM, Fishman D, Kanis M, Thomas C, et al. Gynecologic oncology care during the COVID-19 pandemic at three affiliated new York city hospitals. Gynecol Oncol (2020) 159:470–5. doi: 10.1016/j.ygyno.2020.09.005
20. Papautsky EL, Hamlish T. Patient-reported treatment delays in breast cancer care during the COVID-19 pandemic. Breast Cancer Res Treat (2020) 184:249–54. doi: 10.1007/s10549-020-05828-7
21. Borlea A, Dobrescu A, Dema A, Cornianu M, Lazãr FO, Brebu D. Presurgical stratification of thyroid nodules - is it really needed? current guidelines versus real life. Chirurgia (Bucur) (2021) 116:66–74. doi: 10.21614/CHIRURGIA.116.1.66
22. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid (2016) 26:1–133. doi: 10.1089/THY.2015.0020
23. Jeon YW, Gwak HG, Lim ST, Schneider J, Suh YJ. Long-term prognosis of unilateral and multifocal papillary thyroid microcarcinoma after unilateral lobectomy versus total thyroidectomy. Ann Surg Oncol (2019) 26:2952–8. doi: 10.1245/S10434-019-07482-W
24. Giannoula E, Iakovou I, Giovanella L, Vrachimis A. Updated clinical management guidance during the COVID-19 pandemic: thyroid nodules and cancer. Eur J Endocrinol (2022) 186:G1–7. doi: 10.1530/EJE-21-0716
25. Tsang VHM, Gild M, Glover A, Clifton-Bligh R, Robinson BG. Thyroid cancer in the age of COVID-19. Endocr Relat Cancer (2020) 27:R407–16. doi: 10.1530/ERC-20-0279
26. Medas F, Ansaldo GL, Avenia N, Basili G, Boniardi M, Bononi M, et al. The THYCOVIT (Thyroid surgery during COVID-19 pandemic in Italy) study: results from a nationwide, multicentric, case-controlled study. Updates Surg (2021) 73:1467–75. doi: 10.1007/S13304-021-01051-1
27. Bakkar S, Al-Omar K, Aljarrah Q, Al-Dabbas M, Al-Dabbas N, Samara S, et al. Impact of COVID-19 on thyroid cancer surgery and adjunct therapy. Updates Surg (2020) 72:867–9. doi: 10.1007/S13304-020-00833-3
28. Nickel B, Miller JA, Cvejic E, Gild ML, Cope D, Dodd R, et al. Thyroid cancer clinicians’ views and experiences of delayed treatment during the COVID-19 pandemic: an international cross-sectional survey. ANZ J Surg (2021) 91:2562–4. doi: 10.1111/ANS.17128
29. Stoian D, Timar B, Craina M, Bernad E, Petre I, Craciunescu M. Qualitative strain elastography - strain ratio evaluation - an important tool in breast cancer diagnostic. Med Ultrason (2016) 18:195–200. doi: 10.11152/MU.2013.2066.182.BCD
30. Cantisani V, D’Andrea V, Biancari F, Medvedyeva O, Di Segni M, Olive M, et al. Prospective evaluation of multiparametric ultrasound and quantitative elastosonography in the differential diagnosis of benign and malignant thyroid nodules: preliminary experience. Eur J Radiol (2012) 81(10):2678–83. doi: 10.1016/j.ejrad.2011.11.056
Keywords: COVID-19, nodular thyroid disease, thyroid cancer, healthcare system, surgery
Citation: Popa O, Barna RA, Borlea A, Cornianu M, Dema A and Stoian D (2023) The impact of the COVID-19 pandemic on thyroid nodular disease: a retrospective study in a single center in the western part of Romania. Front. Endocrinol. 14:1221795. doi: 10.3389/fendo.2023.1221795
Received: 12 May 2023; Accepted: 23 June 2023;
Published: 11 July 2023.
Edited by:
Akira Sugawara, Tohoku University, JapanReviewed by:
Barbara Maria Jarzab, Maria Skłodowska-Curie National Research Institute of Oncology, PolandGoknur Yorulmaz, Eskişehir Osmangazi University, Türkiye
Copyright © 2023 Popa, Barna, Borlea, Cornianu, Dema and Stoian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert Alexandru Barna, cm9iZXJ0LmJhcm5hQHVtZnQucm8=