 Shiyu Peng
Shiyu Peng Gaoxiang Zhang
Gaoxiang Zhang Decheng Wang
Decheng Wang- Department of Spinal Trauma, Beijing Tongzhou District Hospital of Integrated Traditional Chinese and Western Medicine, Beijing, China
Background: Osteoporosis (OP) is a systemic metabolic skeletal disorder characterized by a decrease in bone mineral density (BMD) and an increase in the risk of fracture. The level of selenium (Se) in serum is associated with BMD. However, the relationship between dietary and total selenium intake and parameters such as osteoporosis and BMD is unclear. By conducting National Health and Nutritional Examination Surveys (NHANES), in this study, we assessed the association of Se intake with BMD and the risk of OP among general middle-aged and elderly people.
Methods: The data were collected from three cycles of NHANES [2009–2010, 2013–2014, and 2017–2020]. Information on the dietary and supplementary Se intake was obtained from 24-h dietary recall interviews. Additionally, dual-energy X-ray absorptiometry (DXA) was performed to measure BMD, which was later transformed into T-scores; OP was diagnosed when the T-score was ≤ -2.5. We constructed a logistic regression model for the association between selenium intake and the risk of OP based on the estimated odds ratios (ORs) and the 95% confidence intervals (CIs). We also constructed a multivariable linear regression model to analyze the relationship between selenium intake and BMD.
Results: In this study, 3,250 individuals (average age: 60.01 ± 10.09 years; 51.88% females) participated. The incidence of OP was 9.35% (3.30% for males and 17.75% for females). In the logistic regression model adjusted for every interested covariate, a higher quartile of dietary Se intake (OR for quartile 4 vs. quartile 1: 0.63; 95% CI: 0.41–0.96; P for trend = 0.027) was related to a lower risk of OP relative to the lowest quartile. The total selenium intake also exhibited a consistent trend (OR for quartile 4 vs. quartile 1: 0.67; 95% CI: 0.44–1.01; P for trend = 0.049). The results of the adjusted multivariate linear regression model showed that the participants with the highest quartile of dietary Se intake (Q4) had higher BMD in the total femur (β = 0.069, P = 0.001; P for trend = 0.001), femoral neck (β = 0.064, P = 0.001; P for trend = 0.001), and total spine (β = 0.030, P = 0.136; P for trend = 0.064) compared to those in quintile 1 (Q1). A similar trend of associations was observed for the total selenium intake with BMD, which was more prominent among females, as determined by the subgroup analysis.
Conclusion: In this study, the dietary intake and total intake of selenium were positively associated with BMD, whereas they were negatively associated with the risk of OP among adults in the US. Further studies are required to verify our results and elucidate the associated biological mechanism.
Introduction
Osteoporosis (OP) is a commonly occurring skeletal disorder and is characterized by a decrease in bone mass, low bone mineral density (BMD), and the deterioration of bone microstructure (1, 2). A study found that in 2010, OP affected 10.2 million adults in the US who were ≥ 50 years old. The number of affected individuals might reach 13.5 million in 2030 (3). OP significantly increases the burden on the social healthcare system because of the high morbidity, mortality, and therapeutic expenses associated with it (4, 5). Various risk factors are associated with the occurrence of OP and a decrease in BMD; these factors include genetic, environmental, and dietary factors (6, 7). Dietary factors are considered to be closely associated with musculoskeletal diseases (8). Some studies have shown that macronutrients (carbohydrates, proteins, and lipids), flavonoid polyphenols, and micronutrients (phosphorus, calcium, magnesium, and vitamins D, C, and K) greatly facilitate the inhibition of osteoporosis (9). Deficiency or excess of zinc, copper, selenium, iron, cadmium, silicon, and fluorine might affect bone mineralization and lead to osteoporosis (10). Some studies have shown that trace elements can help in preventing OP (11, 12).
Selenium (Se) is an essential trace mineral element in the human body. It forms “selenoproteins” after it is incorporated into the protein polypeptide chain. Additionally, Se modulates cell processes by influencing Se-mediated antioxidant enzyme components, which scavenge reactive oxygen species (ROS) in cells. Selenium is closely associated with Keshan disease, thyroid-related diseases, and other functions and diseases (13, 14). Selenium protein P is a critical Se transporter in the bone and is very important for maintaining bone health (15). A deficiency of Se may increase the levels of ROS, and it is the most important cause of OP (16). Some studies have suggested that serum Se level is positively associated with bone outcomes, like BMD and the risk of fracture (17, 18). Only a few studies have shown a non-linear relationship (19) and an inverted U-shaped trend (20) between the dietary intake of Se and osteoporosis. Although recent studies on humans have analyzed the relationship between the dietary Se level and BMD (20), few studies have investigated the relationship of dietary and total Se with BMD and osteoporosis. Hence, the effects of selenium intake on an increase in BMD and a decrease in the risk of osteoporosis need to be investigated to develop more effective preventive measures for reducing the morbidity and mortality of OP globally.
In this study, we investigated the relationship between Se intake and changes in BMD and the risk of OP based on the cross-sectional data collected by conducting National Health and Nutritional Examination Surveys (NHANES).
Materials and methods
Participants
The NHANES was developed in 1959 as a continuous program for conducting cross-sectional examinations of the nutrition and health of people in the United States (US) annually. In this program, information on dietary, demographic, questionnaire, and laboratory data is released every two years. In this study, we included adults who were ≥50 years old, with sufficient selenium intake, and with BMD data recorded in the NHANES that was conducted in 2009–2010, 2013–2014, and 2017–2020 (Figure 1). All participants provided informed consent for this survey, as it was required by the Institutional Review Board of the National Center for Health Statistics.

Figure 1 Flow diagram of inclusion criteria and exclusion criteria.
Selenium intake
The information on the dietary and supplementary selenium intake was collected from two 24-h dietary recall interviews in three NHANES two-year cycles (2009–2010, 2013–2014, and 2017–2020). It was a respondent-driven approach to collect precise and comprehensive data on the food and beverage types and amounts (every water type was included) taken within 24-h immediately before the interview (midnight to midnight). In this survey, two 24-h dietary recalls were conducted; the first one was conducted in person during the mobile examination, whereas the second one was conducted after 3–10 days through a telephone interview. Information on the dietary selenium intake and supplement intake was obtained in each interview; thus, the total selenium intake for each interview was the sum of dietary selenium and supplements. The average selenium intake recorded in two consecutive interviews was considered to be the selenium intake of the participants. A nutrient residual model was used to adjust the selenium intake for total energy intake (21). The approach helped adjust the total energy intake-induced confounding when analyzing the relationship between selenium and OP. Dietary Reference Intakes: Basic Guidelines for Nutritional Requirements (2006) recommended dietary reference intakes (DRIs) of total selenium intakes as follows: an estimated average intake (EAR) of 45µg/day, a recommended dietary allowance (RDA) of 55µg/day, and a tolerable maximum intake (UL) of 400µg/day, without gender differences.
Determination of BMD and the diagnosis of OP
The BMD levels were examined at different regions (total femur, femur neck, and lumbar spine) in the NHANES. Additionally, through dual-energy X-ray absorptiometry (DXA), Hologic QDR-4500A fan-beam densitometers (Hologic, Inc., Bedford, Massachusetts) were used for scanning. Generally, the left hip was examined, only if the subject reported a fracture, a pin, or a replacement of the left hip, the right hip was examined. The BMD of the lumbar spine was determined by the average level of the first to fourth lumbar vertebrae. Pregnant patients, those with a radiographic contrast material history, those with bilateral hip fractures/replacement/pins, and those who were >450 lbs were eliminated from the DXA examination. The diagnostic criteria for osteoporosis were defined using the mean of the peak BMD of the femoral neck, total hip, and lumbar spine from the NHANES III database in the United States and its corresponding standard deviation (SD) in white women aged 20 to 29 years. Then, an established method was used to transform the BMD levels in the femoral neck, total hip, and lumbar spine to T-scores (22, 23), with a T-score≤ -2.5, -2.5 < T-score ≤ -1, and > –1 indicating OP, osteopenia, and normal, respectively. Patients with osteopenia and normal individuals were considered to be non-OP.
Covariate assessment
Based on the statements on the NHANES website, trained personnel collected the data at every study site following standard procedures. In this study, the covariates were age, gender, ethnicity, education level, marital status, history of smoking, hypertension, diabetes, osteoporosis in parents, previous fractures, and body mass index (BMI, which was determined by dividing the body weight (kg) by the body height squared (m2). Participants were weighed in kilograms using a digital weight scale. Standing height was measured using a stadiometer with a fixed vertical backboard and an adjustable head piece.
Statistical analysis
The estimates of the people in the US were generated by data weighting and analyzed by layering and clustering. For descriptive analysis, normally-distributed continuous data were represented by the mean ± standard deviation (SD), whereas non-normally distributed continuous data were expressed as the median and the quartile range. Additionally, categorical data were represented by the frequency and frequency percentage. We conducted the Student’s t-test, non-parametric tests, and the Chi-squared test to analyze the statistical differences between the two groups of continuous variables that followed a normal distribution, continuous variables that did not follow a non-normal distribution, and categorical data, respectively. The dietary and total selenium intake levels were classified according to quartiles (quartiles 1–4 indicated <25th, 25th–50th, 50th–75th, and >75th percentile). Odds ratios (ORs) and 95% confidence intervals (CIs) were determined through logistic regression to analyze the relationship between selenium intake and the risk of OP. We used dietary and total selenium intake for reference. In Model 1, sex, body mass index, marital status, and race were adjusted. In Model 2, a history of hypertension, diabetes, osteoporosis in parents, and previous fractures were also adjusted. In Model 3, every interested covariate was adjusted. Additionally, multivariate linear regression models were constructed to determine the relationship between selenium intake and BMD in the total spine and total femur. The relationships between selenium intake and BMD, as well as the risk of OP were also analyzed through a gender-stratified subgroup analysis. The R (version 3.5.3) and SPSS (version: 24.0; SPSS, Chicago, IL) software programs were used for conducting statistical analyses. All differences among and between groups were considered to be statistically significant at P < 0.05 (two-sided).
Results
Characteristics of the study population
The unqualified patients were excluded (Figure 1), and 3,250 participants were included in this study. The characteristics of the participants with and without OP are presented in Table 1. Compared to the participants without OP, those with OP were thinner and older, mainly women, with lower levels of education, widowed, divorced, or separated, with hypertension, a history of osteoporosis in parents, previous fractures, and less likely to be non-Hispanic Black. In contrast, participants without OP had a greater amount of dietary Se and total Se.
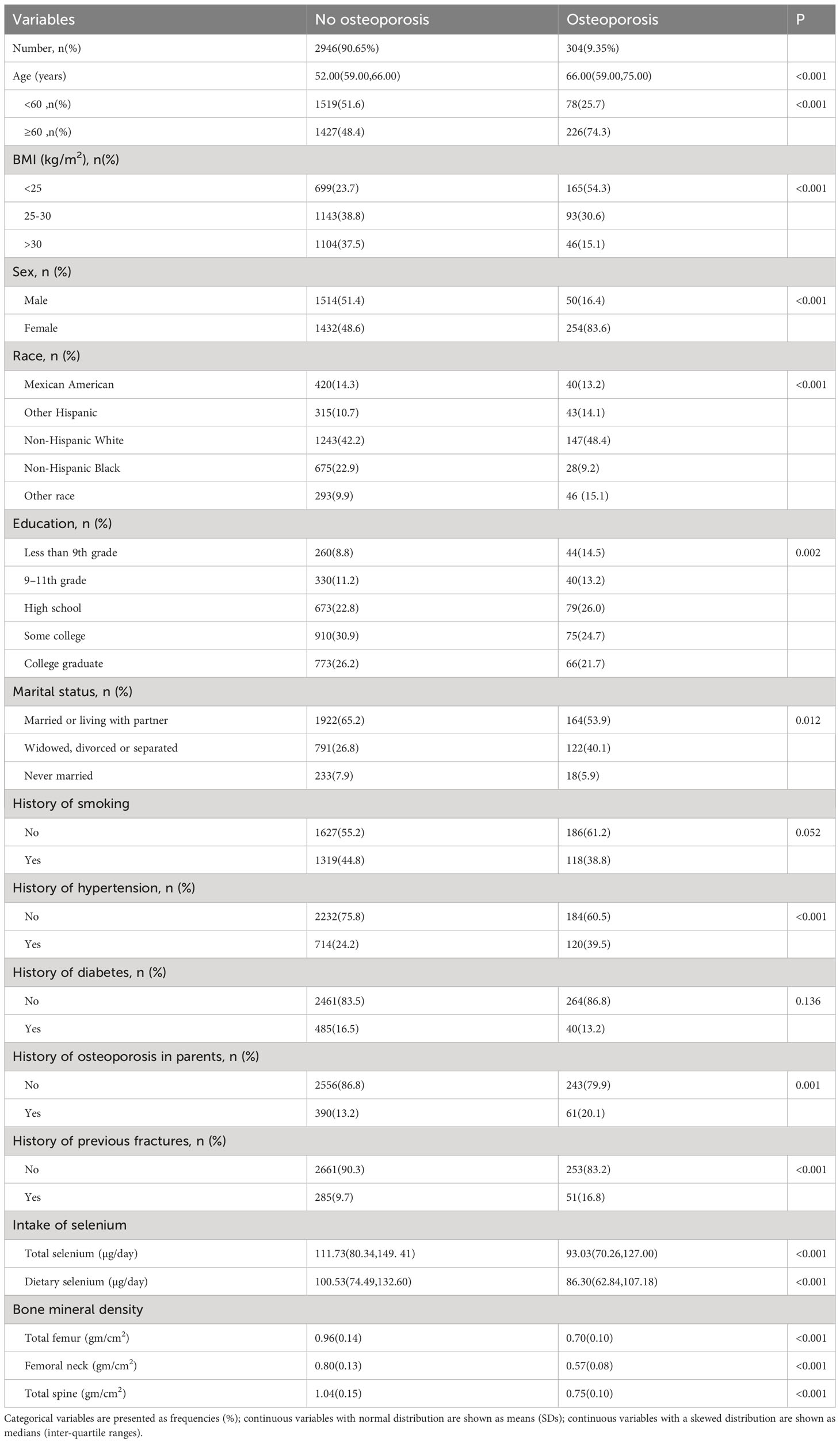
Table 1 Basic characteristics of the OP and non-OP population of NHANES.
Relationship between selenium intake and osteoporosis
The relationship between selenium intake and the risk of OP was analyzed by conducting logistic regression (Table 2). In Model 1, based on the ORs and 95% CIs for the relationship between the dietary intake of Se with the risk of OP, after being adjusted for sex, body mass index, marital status, and race, a higher quartile of dietary selenium intake (0.69 (95% CI: 0.49, 0.98); 0.49 (95% CI: 0.33, 0.74); P for trend = 0.001) indicated a lower risk of OP. Additionally, dietary selenium intake showed consistent results with marginal significance (0.53 (95% CI: 0.35, 0.81); P for trend = 0.002; 0.63 (95% CI: 0.41, 0.96); P for trend = 0.027) after further adjustment for history of hypertension, diabetes, OP in parents, previous fractures (Model 2), and every interested covariate (Model 3). For the relationship between the risk of OP and the total selenium intake, consistent findings were obtained from Models 1, 2, and 3, i.e., 0.58 (95% CI: 0.39, 0.86) (P for trend = 0.005) after being adjusted for sex, BMI, marital status and race (Model 1); 0.60 (95% CI: 0.40, 0.90) (P for trend = 0.012) after further adjustment for history of hypertension, diabetes, OP in parents, and previous fractures (Model 2); 0.67 (95% CI: 0.44, 1.01) after being adjusted for every covariate (Model 3). Relative to the lowest quartile, the dietary and total Se intake did not show a significant inverse relationship in quartile 2.
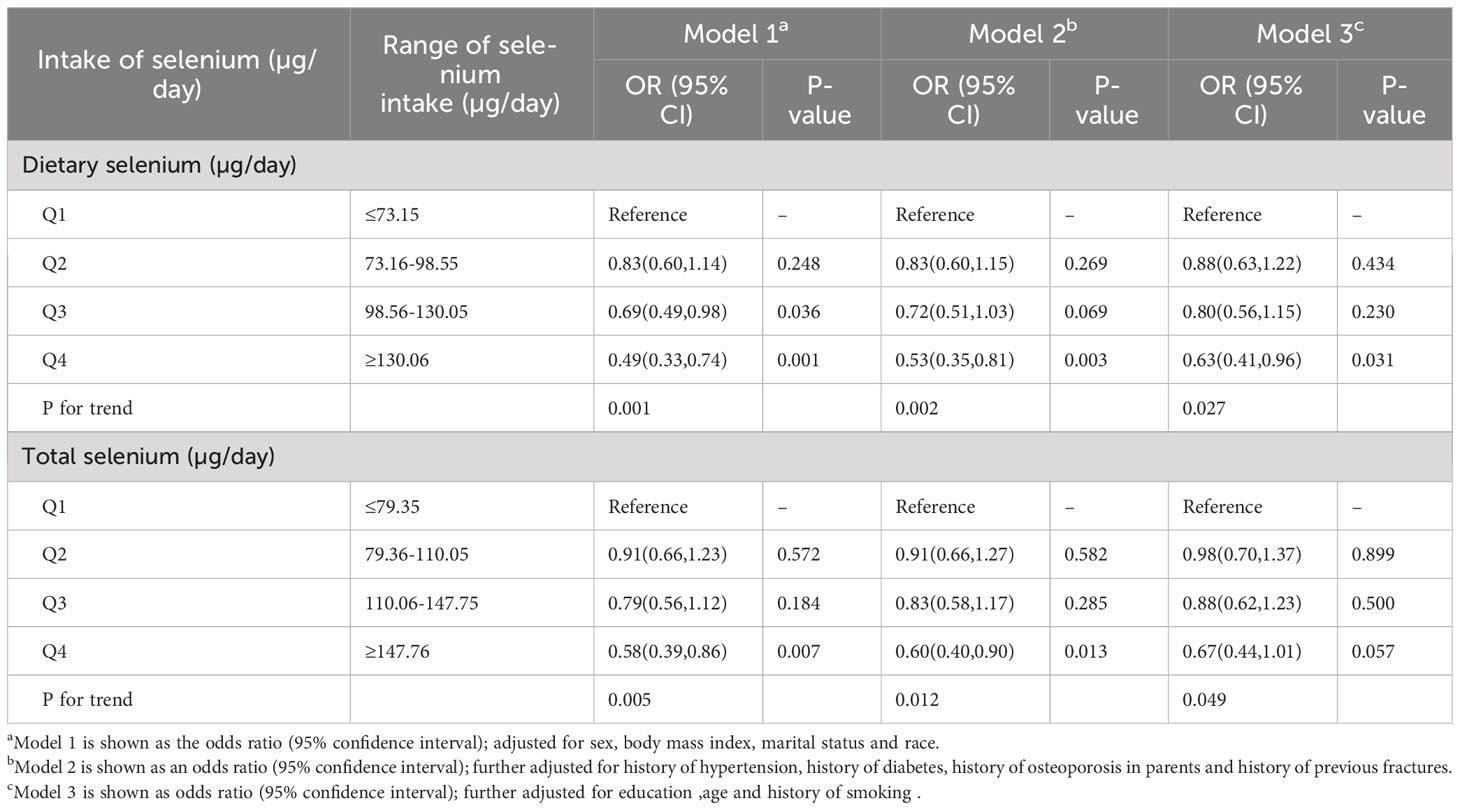
Table 2 Odds Ratio of osteoporosis across quartiles of selenium intakes.
Association of selenium intake with BMD
The results of the multivariate linear regression analysis of selenium intake with BMD are presented in Table 3. The associations between selenium intake and BMD at various bone sites were analyzed (Table 3). In the crude model, relative to the lowest quartile (Q1) of dietary selenium intake, individuals with the highest quartile (Q4) had higher BMD levels in the total femur (β = 0.106, P = 0.001, P for trend = 0.001), femur neck (β = 0.106, P = 0.001, P for trend = 0.001), and total spine (β = 0.053, P = 0.009, P for trend = 0.003). When every interested covariate was adjusted, similar significant positive relationships were also found between the BMD in the total femur and femur neck and selenium intake. A similar association was found between total selenium intake and BMD.
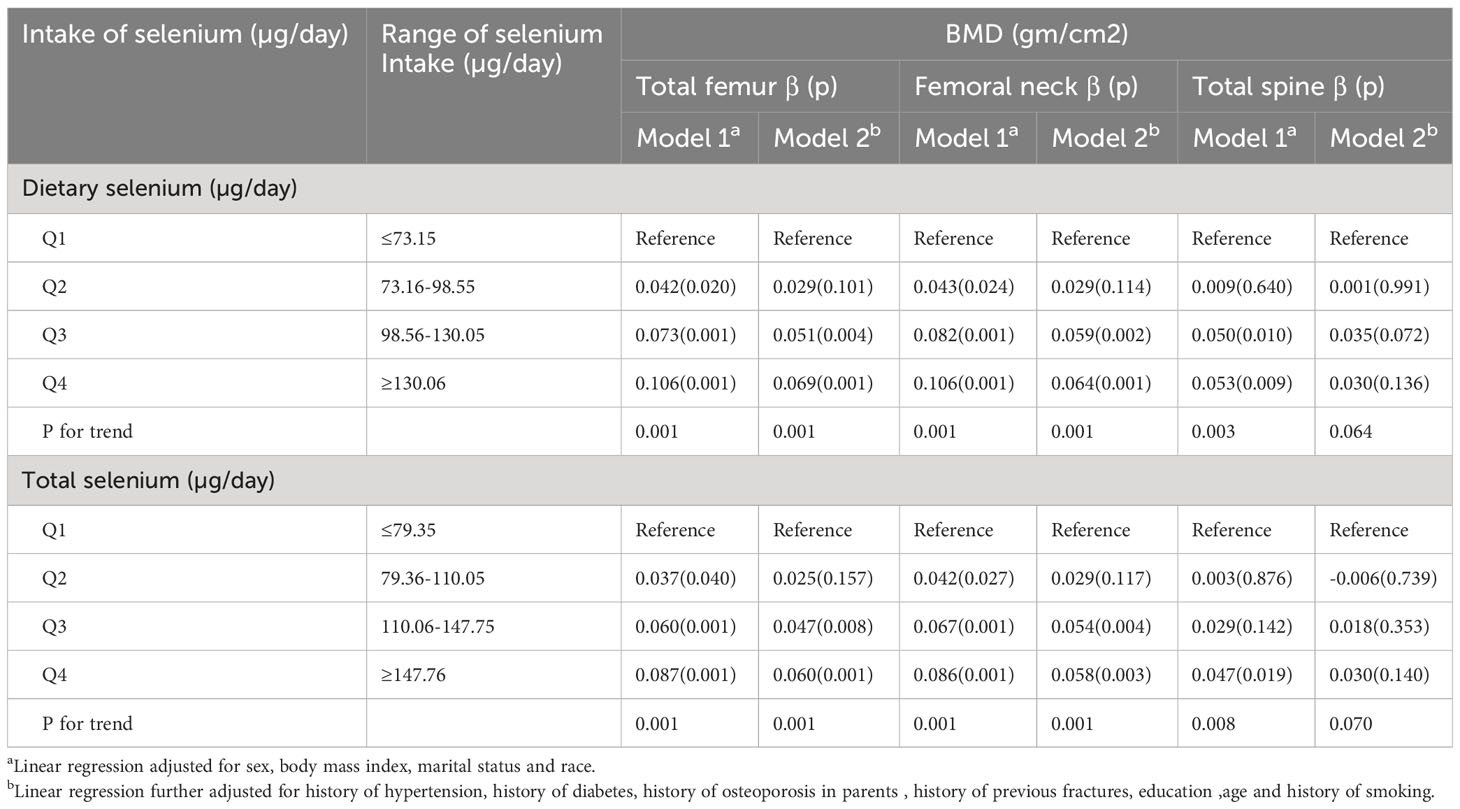
Table 3 Linear regression coefficients for selenium intakes and BMD.
Relation between selenium intake and osteoporosis or BMD in the subgroup analysis by sex
To further demonstrate the relationship between Se intake levels and the risk of OP, we performed a gender-stratified subgroup analysis (Tables 4, 5). The results showed a statistically significant increase in total femur BMD in men and women. However, this relationship was not significantly different between the femoral neck BMD and total spine BMD in men. In women, compared to the lowest quartile (Q1) of Se intake, high Se intake was associated with higher BMD in the femoral neck (all P trend = 0.001). Similar results were obtained when selenium intake was considered to be a continuous variable (per 1-SD increase). Additionally, this positive relationship was significant between the highest and lowest selenium intake quartiles of total spine BMD. According to the logistic regression, the ORs were 0.56 (0.34, 0.91) and 0.62 (0.38, 0.96) in Model 1 and Model 2 for females regarding dietary selenium with OP across quartile 4 relative to quartile 1; however, this association was not significant relative to quartile 1 for men. The highest quartiles of total selenium intake were not significantly related to the risk of osteoporosis in men.

Table 4 Association between selenium intake levels and BMD by sex.
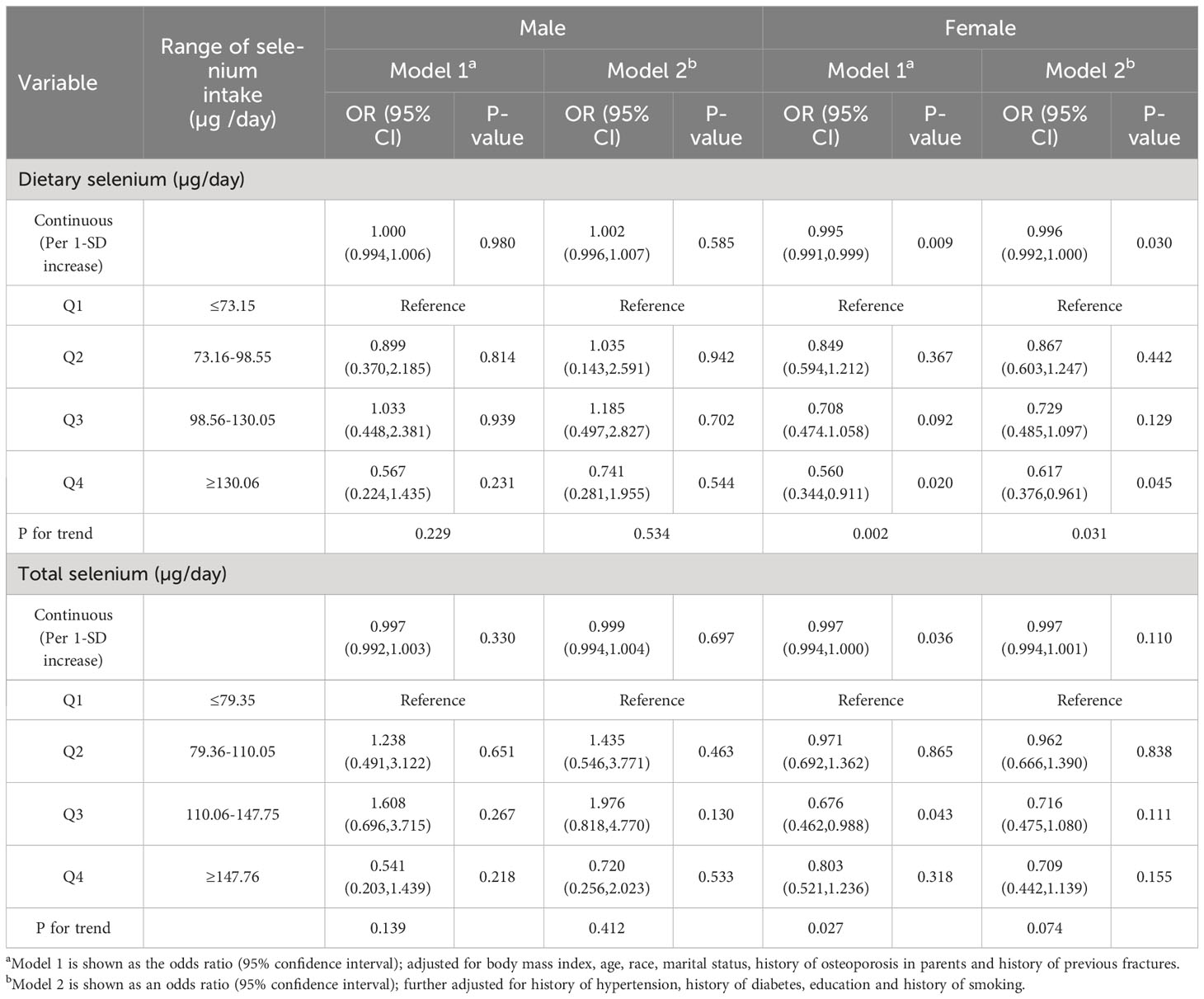
Table 5 Association between selenium intake levels and osteoporosis by sex.
Discussion
Few studies have investigated whether diet and total selenium intake are associated with bone health. Based on US adult samples from NHANES (2009–2010, 2013–2014, and 2017–2020) in this study, we found that selenium intake was independently related to a lower risk of OP, while a higher selenium intake was related to a higher total femur/femoral neck BMD. Additionally, higher Se intake among females was related to a higher total femur/femoral neck BMD in women, but not in men.
This is the first study to determine the correlation between selenium intake and factors such as BMD and the risk of osteoporosis in adults in the US based on large data. Although some studies have investigated the effects of dietary selenium intake on bone health, and those that have are limited by small sample sizes (19, 20, 24). In our study, we analyzed the relationship between selenium intake and bone health from 3 cycles of NHANES (2009-2010, 2013-2014, and 2017-2020) in middle-aged and older adults aged 50 years or older, overcoming the small amount of data described in previous studies. In addition, studies have investigated the relationship between selenium intake and BMD of adults in the US and other countries (19, 20, 24–26), but the results of their studies were different. For example, Wolf et al. suggested in their cross-sectional study that Se intake from the diet did not have any association with BMD in the US adults (24); Xue et al. showed that an increase in the dietary Se level can predict higher BMD levels in the femur, femur neck, intertrochanter, trochanter, and that dietary selenium intake had an inverted U-shaped relationship with bone mineral density in the US adults (20); Walsh et al. conducted a randomized double-blinded controlled study and found that Se intake at 200 µg/day did not significantly alter the musculoskeletal health of postmenopausal women in the UK (25); A cross-sectional study conducted with 6,267 participants found that a higher dietary intake of Se increased the BMD of individuals in a middle-aged and elderly Chinese population (19); Recently, Xie et al. showed that selenium was positively associated with BMD and inversely associated with OP by a meta-analysis of data from different countries (26); Thus, it is necessary to further clarify the relationship between dietary selenium and bone mineral density in the US adults. Furthermore, previous study (20) have only analyzed the relationship between dietary selenium intake and bone mineral density, and did not consider selenium intake from dietary supplements. In our study, in addition to analyzing the relationship between dietary selenium intake and bone mineral density, we also analyzed the relationship between total selenium intake (dietary selenium intake and supplement intake from dietary supplements) and bone mineral density, so our study is more comprehensive and detailed than previous studies. We results showed that selenium intake was positively associated with total femur/femoral neck BMD, which partially matched the findings of previous study, supporting the finding that selenium intake is positively related to BMD. Meanwhile, very few articles have investigated the relationship between the status of selenium and osteoporosis in the US population. Although Zhang et al. suggested that Se intake was negatively associated with the risk of osteoporotic hip fracture, those researchers focused on smokers (27). Xue et al. showed an inverted U-shaped relationship between dietary selenium intake and bone mineral density, but they did not assess the relationship between dietary selenium intake and osteoporosis risk due to limitations of the original data (26). This is the first analysis between the dietary and total intake of selenium and osteoporosis among US adults. Our results indicate that dietary and total selenium intake was negative with the risk of osteoporosis in US adults.
Selenium is an essential trace mineral element in the human body. It can regulate cellular processes, such as the Se-driven antioxidant enzyme component, which can scavenge ROS in cells (28–30). The mechanism by which selenium plays a role in the development of osteoporosis is not clear, but we hypothesized several mechanisms that link selenium and osteoporosis. First, ROS has a critical effect on the development of OP (16). Apoptosis of osteoblasts and osteocytes induced by ROS may promote the production of osteoclasts and inhibit osteogenesis and mineralization. However, excessive osteocyte apoptosis can result in oxidative stress, which can disrupt the generation of osteoclasts, increase bone loss, and result in remodeling (31, 32). Selenoproteins are transporters of Se in bones, and they are found in osteoclasts and osteoblasts. They have antioxidant activities and can scavenge the generated ROS (15, 16, 33). Second, selenium can also influence anti-inflammatory and immune processes. Since cytokines such as interleukin-6 (IL-6) are important for the pathogenic mechanism of OP. Selenium exerts an anti-inflammatory effect, partially regulated via the inhibition of cytokine activities; thus, Se regulates bone turnover to protect against OP (34, 35). Third, Se-mediated iodothyronine deiodinases help regulate thyroid hormone turnover, while Se-mediated glutathione peroxidases help in protecting the thyroid gland. Thus, Se might also affect bone health via the relationship between Se-mediated glutathione peroxidase activity and thyroid protection. A deficiency of Se might increase the blood thyroid hormone level, thus accelerating bone loss and osteoporosis (36, 37). Therefore, determining the relationship between selenium intake and OP is extremely important.
This study had some strengths. First, this study was conducted based on a nationwide survey, where BMD was determined using established approaches by expert scientists. Second, this was the first study to analyze the relationship between Se intake and parameters such as BMD and OP among adults in the US. Our results showed a potential role of appropriate dietary Se intake in preventing the development of OP. Additionally, after confounding factors were adjusted, a gender-stratified subgroup analysis was conducted to provide a reference to determine the relationship between selenium intake and changes in BMD and risk of osteoporosis. However, our study had certain limitations. First, this was a cross-sectional study, and residual confounding due to additional unmeasured factors was not eliminated, although certain covariates were adjusted. Second, we acquired dietary intake information from the NHANES based on 24-h dietary recall interviews, which might be associated with recall bias. Hence, our results should be confirmed by conducting larger, prospective studies.
To summarize, the level of dietary and total Se intake was positively associated with BMD and negatively associated with the risk of OP among adults in the US. However, larger prospective studies are needed to confirm our findings.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by the Institutional Review Board of the National Center for Health Statistics. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SP analyzed the data, and wrote the manuscript. GZ and DW designed the study and revised the manuscript. SP is the first author. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors acknowledge the data from the National Health and Nutrition Examination Survey (NHANES) and Dietary Reference Intakes: The Essential Guide to Nutrient Requirements (2006) (https://doi.org/10.17226/11537).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hendrickx G, Boudin E, Van Hul W. A look behind the scenes: the risk and pathogenesis of primary osteoporosis. Nat Rev Rheumatol (2015) 11(8):462–74. doi: 10.1038/nrrheum.2015.48
2. Kanis JA, McCloskey EV, Johansson H, Oden A, Melton LJ 3rd, Khaltaev N. A reference standard for the description of osteoporosis. Bone (2008) 42(3):467–75. doi: 10.1016/j.bone.2007.11.001
3. Duan W, Meng X, Sun Y, Jia C. Association between polycyclic aromatic hydrocarbons and osteoporosis: data from NHANES, 2005-2014. Arch Osteoporos (2018) 13(1):112. doi: 10.1007/s11657-018-0527-4
4. Cai S, Fan J, Zhu L, Ye J, Rao X, Fan C, et al. Bone mineral density and osteoporosis in relation to all-cause and cause-specific mortality in NHANES: A population-based cohort study. Bone (2020) 141:115597. doi: 10.1016/j.bone.2020.115597
5. Lorentzon M, Nilsson AG, Johansson H, Kanis JA, Mellstrom D, Sundh D. Extensive undertreatment of osteoporosis in older Swedish women. Osteoporos Int (2019) 30(6):1297–305. doi: 10.1007/s00198-019-04872-4
6. Lunde A, Tell GS, Pedersen AB, Scheike TH, Apalset EM, Ehrenstein V, et al. The role of comorbidity in mortality after hip fracture: A nationwide norwegian study of 38,126 women with hip fracture matched to a general-population comparison cohort. Am J Epidemiol (2019) 188(2):398–407. doi: 10.1093/aje/kwy251
7. Rizzoli R, Biver E, Brennan-Speranza TC. Nutritional intake and bone health. Lancet Diabetes Endocrinol (2021) 9(9):606–21. doi: 10.1016/S2213-8587(21)00119-4
8. Aaseth J, Boivin G, Andersen O. Osteoporosis and trace elements–an overview. J Trace Elem Med Biol (2012) 26(2-3):149–52. doi: 10.1016/j.jtemb.2012.03.017
9. Martiniakova M, Babikova M, Mondockova V, Blahova J, Kovacova V, Omelka R. The role of macronutrients, micronutrients and flavonoid polyphenols in the prevention and treatment of osteoporosis. Nutrients (2022) 14(3):523. doi: 10.3390/nu14030523
10. Ratajczak AE, Rychter AM, Zawada A, Dobrowolska A, Krela-Kazmierczak I. Do only calcium and vitamin D matter? Micronutrients in the diet of inflammatory bowel diseases patients and the risk of osteoporosis. Nutrients (2021) 13(2):525. doi: 10.3390/nu13020525
11. Zhang H, Wang A, Shen G, Wang X, Liu G, Yang F, et al. Hepcidin-induced reduction in iron content and PGC-1beta expression negatively regulates osteoclast differentiation to play a protective role in postmenopausal osteoporosis. Aging (Albany NY) (2021) 13(8):11296–314. doi: 10.18632/aging.202817
12. Ceylan MN, Akdas S, Yazihan N. Is zinc an important trace element on bone-related diseases and complications? A meta-analysis and systematic review from serum level, dietary intake, and supplementation aspects. Biol Trace Elem Res (2021) 199(2):535–49. doi: 10.1007/s12011-020-02193-w
13. Zhou H, Wang T, Li Q, Li D. Prevention of keshan disease by selenium supplementation: a systematic review and meta-analysis. Biol Trace Elem Res (2018) 186(1):98–105. doi: 10.1007/s12011-018-1302-5
14. Winther KH, Rayman MP, Bonnema SJ, Hegedus L. Selenium in thyroid disorders - essential knowledge for clinicians. Nat Rev Endocrinol (2020) 16(3):165–76. doi: 10.1038/s41574-019-0311-6
15. Pietschmann N, Rijntjes E, Hoeg A, Stoedter M, Schweizer U, Seemann P, et al. Selenoprotein P is the essential selenium transporter for bones. Metallomics (2014) 6(5):1043–9. doi: 10.1039/C4MT00003J
16. Manolagas SC. From estrogen-centric to aging and oxidative stress: a revised perspective of the pathogenesis of osteoporosis. Endocr Rev (2010) 31(3):266–300. doi: 10.1210/er.2009-0024
17. Hoeg A, Gogakos A, Murphy E, Mueller S, Kohrle J, Reid DM, et al. Bone turnover and bone mineral density are independently related to selenium status in healthy euthyroid postmenopausal women. J Clin Endocrinol Metab (2012) 97(11):4061–70. doi: 10.1210/jc.2012-2121
18. Galvez-Fernandez M, Grau-Perez M, Garcia-Barrera T, Ramirez-Acosta S, Gomez-Ariza JL, Perez-Gomez B, et al. Arsenic, cadmium, and selenium exposures and bone mineral density-related endpoints: The HORTEGA study. Free Radic Biol Med (2021) 162:392–400. doi: 10.1016/j.freeradbiomed.2020.10.318
19. Wang Y, Xie D, Li J, Long H, Wu J, Wu Z, et al. Association between dietary selenium intake and the prevalence of osteoporosis: a cross-sectional study. BMC Musculoskelet Disord (2019) 20(1):585. doi: 10.1186/s12891-019-2958-5
20. Xue G, Liu R. Association between dietary selenium intake and bone mineral density in the US general population. Ann Transl Med (2022) 10(16):869. doi: 10.21037/atm-22-3441
21. Willett WC, Howe GR, Kushi LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr (1997) 65(4 Suppl):1220S–8S; discussion 9S-31S. doi: 10.1093/ajcn/65.4.1220S
22. Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, et al. Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int (1998) 8(5):468–89. doi: 10.1007/s001980050093
23. Bass MA, Sharma A, Nahar VK, Chelf S, Zeller B, Pham L, et al. Bone mineral density among men and women aged 35 to 50 years. J Am Osteopath Assoc (2019) 119(6):357–63. doi: 10.7556/jaoa.2019.064
24. Wolf RL, Cauley JA, Pettinger M, Jackson R, Lacroix A, Leboff MS, et al. Lack of a relation between vitamin and mineral antioxidants and bone mineral density: results from the Women’s Health Initiative. Am J Clin Nutr (2005) 82(3):581–8. doi: 10.1093/ajcn/82.3.581
25. Walsh JS, Jacques RM, Schomburg L, Hill TR, Mathers JC, Williams GR, et al. Effect of selenium supplementation on musculoskeletal health in older women: a randomised, double-blind, placebo-controlled trial. Lancet Healthy Longev (2021) 2(4):e212–e21. doi: 10.1016/S2666-7568(21)00051-9
26. Xie H, Wang N, He H, Yang Z, Wu J, Yang T, et al. The association between selenium and bone health: a meta-analysis. Bone Joint Res (2023) 12(7):423–32. doi: 10.1302/2046-3758.127.BJR-2022-0420.R1
27. Zhang J, Munger RG, West NA, Cutler DR, Wengreen HJ, Corcoran CD. Antioxidant intake and risk of osteoporotic hip fracture in Utah: an effect modified by smoking status. Am J Epidemiol (2006) 163(1):9–17. doi: 10.1093/aje/kwj005
28. Allan CB, Lacourciere GM, Stadtman TC. Responsiveness of selenoproteins to dietary selenium. Annu Rev Nutr (1999) 19:1–16. doi: 10.1146/annurev.nutr.19.1.1
29. Lei XG, Cheng WH, McClung JP. Metabolic regulation and function of glutathione peroxidase-1. Annu Rev Nutr (2007) 27:41–61. doi: 10.1146/annurev.nutr.27.061406.093716
30. Sunde RA. Molecular biology of selenoproteins. Annu Rev Nutr (1990) 10:451–74. doi: 10.1146/annurev.nu.10.070190.002315
31. Domazetovic V, Marcucci G, Iantomasi T, Brandi ML, Vincenzini MT. Oxidative stress in bone remodeling: role of antioxidants. Clin cases Miner Bone Metab (2017) 14(2):209–16. doi: 10.11138/ccmbm/2017.14.1.209
32. Robling AG, Bonewald LF. The osteocyte: new insights. Annu Rev Physiol (2020) 82:485–506. doi: 10.1146/annurev-physiol-021119-034332
33. Jakob F, Becker K, Paar E, Ebert-Duemig R, Schutze N. Expression and regulation of thioredoxin reductases and other selenoproteins in bone. Methods Enzymol (2002) 347:168–79. doi: 10.1016/S0076-6879(02)47015-2
34. Heaney RP. Calcium, dairy products and osteoporosis. J Am Coll Nutr (2000) 19(2 Suppl):83S–99S. doi: 10.1080/07315724.2000.10718088
35. Duntas LH. Selenium and inflammation: underlying anti-inflammatory mechanisms. Horm Metab Res (2009) 41(6):443–7. doi: 10.1055/s-0029-1220724
36. Schomburg L, Kohrle J. On the importance of selenium and iodine metabolism for thyroid hormone biosynthesis and human health. Mol Nutr Food Res (2008) 52(11):1235–46. doi: 10.1002/mnfr.200700465
Keywords: selenium intake, bone mineral density (BMD), osteoporosis, NHANES, cross-sectional survey
Citation: Peng S, Zhang G and Wang D (2023) Association of selenium intake with bone mineral density and osteoporosis: the national health and nutrition examination survey. Front. Endocrinol. 14:1251838. doi: 10.3389/fendo.2023.1251838
Received: 02 July 2023; Accepted: 12 September 2023;
Published: 29 September 2023.
Edited by:
Alberto Falchetti, Italian Auxological Institute (IRCCS), ItalyReviewed by:
Francesco Grassi, Rizzoli Orthopedic Institute (IRCCS), ItalyJuliana Ebling Brondani, Federal University of Santa Maria, Brazil
Copyright © 2023 Peng, Zhang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gaoxiang Zhang, ejAxMDAyMDIwMjFAMTYzLmNvbQ==; Decheng Wang, V2RjMTM1MDExMzExMzVAMTYzLmNvbQ==