 Edinson Dante Meregildo-Rodriguez
Edinson Dante Meregildo-Rodriguez Martha Genara Asmat-Rubio2
Martha Genara Asmat-Rubio2 Gustavo Adolfo Vásquez-Tirado
Gustavo Adolfo Vásquez-Tirado- 1Escuela de Medicina, Universidad César Vallejo, Trujillo, Peru
- 2Escuela de Posgrado, Universidad Privada Antenor Orrego, Trujillo, Peru
- 3Escuela de Medicina, Universidad Privada Antenor Orrego, Trujillo, Peru
Introduction: SGLT2 inhibitors (SGLT2Is) have demonstrated cardioprotective and nephroprotective effects in patients with and without diabetes. Recent studies suggest that SGLT2Is may reduce the risk of contrast-induced nephropathy (CIN) in patients with diabetes undergoing coronary arteriography (CAG) or percutaneous coronary interventions (PCI). However, the evidence is still inconclusive. We aimed to systematically review the evidence regarding the potential nephroprotective role of SGLT2Is in preventing CIN in this population.
Methods: We searched for studies in six databases published up to September 30, 2023, following a PECO/PICO strategy. Initially, we meta-analyzed five studies, but due to several reasons, mainly methodological concerns, we excluded one RCT. In our final meta-analysis, we included four observational studies.
Results: This meta-analysis comprised 2,572 patients with diabetes undergoing CAG or PCI, 512 patients treated with SGLT2Is, and 289 events of CIN. This is the first meta-analysis demonstrating that SGLT2Is may reduce the risk of developing CIN by up to 63% (RR 0.37; 95% CI 0.24–0.58) in patients with diabetes undergoing CAG or PCI, compared to not using SGLT2Is. Statistical heterogeneity was not significant (I2 = 0%, p = 0.91). We assessed the certainty of the evidence of this systematic review and meta-analysis, according to the GRADE criteria, as moderate.
Conclusion: SGLT2Is significantly reduce the risk of CIN by up to 63% in patients with diabetes undergoing CAG or PCI. Clinical trials are needed; several are already underway, which could confirm our findings and investigate other unresolved issues, such as the optimal dose, type, and duration of SGLT2 inhibitor therapy to prevent CIN.
Systematic Review: PROSPERO, identifier CRD42023412892.
1 Introduction
Diabetes mellitus and ischemic heart disease are growing public health problems worldwide (1–3). Contrast-induced nephropathy (CIN), also known as contrast-induced acute kidney injury (CI-AKI), is a common complication of coronary angiography (CAG) and percutaneous coronary intervention (PCI), especially in patients with diabetes. CIN is associated with high morbidity and mortality because it can lead to a significant decline in kidney function, and in severe cases, it can require dialysis. These complications also present with higher incidence in patients with type 2 diabetes mellitus (T2D) (4–6).
Sodium-glucose cotransporter-2 inhibitors (SGLT2Is) are a recent class of oral anti-diabetic agents (OADs) for treating patients with T2D (7). Currently, there exist four SGLT2Is approved by the Food and Drug Administration (FDA): empagliflozin, canagliflozin, dapagliflozin, and ertugliflozin (8). SGLT2Is act by inhibiting the renal reabsorption of glucose, enhancing renal glucose excretion, and decreasing serum glycemic levels (7). These medications reduce blood pressure, the risk of cardiovascular events (CVEs), and kidney disease in patients with and without diabetes (9–16). Two randomized controlled trials (RCTs), the DAPA-CKD (17) and the EMPA-Kidney (18) studies, showed that among patients with chronic kidney disease (CKD), regardless of the presence or absence of diabetes, gliflozins led to a lower risk of progression of CKD or death from renal o CVEs than placebo. Furthermore, the EMPEROR-Reduced trial showed that empagliflozin, compared to placebo, reduced deaths due to CVEs, heart failure (HF) hospitalizations, and the rate of decline in renal function in patients with and without T2D (19).
Likewise, the DAPA-HF trial found that patients with HF and a reduced ejection fraction treated with dapagliflozin had lower risks of worsening HF or death from CVEs than those who received a placebo, regardless of the presence or absence of diabetes; however, rates of worsening renal function was similar in both groups (20). In the DELIVER trial of patients with HF and mildly reduced or preserved ejection fraction, dapagliflozin reduced the risk of CV death or worsening HF regardless of baseline kidney function. Moreover, treatment with dapagliflozin slowed the rate of renal function decline, compared with placebo. Interestingly, this nephroprotective effect was more pronounced among patients with diabetes than those without (21).
Recent observational studies have suggested that SGLT2Is may prevent CIN in patients with diabetes undergoing coronary interventions such as CAG and PCI (22–26). However, observational studies showing discordant results also exist (27). A recent non-blinded open-labeled RCT failed to show a clear nephroprotective effect of SGLT2Is in patients undergoing PCI (28). Then, we aimed to conduct this systematic review and meta-analysis to evaluate the evidence on the effectiveness of SGLT2Is in preventing CIN in this patient population. The results of this study will provide important information on the potential role of SGLT2Is in the prevention of CIN in patients with diabetes undergoing coronary interventions.
2 Materials and methods
We conducted this systematic review according to the Cochrane Handbook for Systematic Reviews (29), PRISMA (30), and AMSTAR 2 (31) guidelines. We previously registered the protocol in PROSPERO (CRD42023412892).
We extensively searched MEDLINE (PubMed), Scopus, EMBASE, Web of Science, Google Scholar, and Cochrane Library. Each database was screened using thesaurus or controlled language terms (MeSH, Emtree, etc.), free terms, and their synonyms. These terms were combined using Boolean operators following our PECO/PICO strategy (Population: adult patients undergoing percutaneous coronary interventions or coronary artery bypass grafting; Exposure: treatment with any SGLT2I; Comparator: no use of SGLT2Is or other OADs; Outcome: Contrast-induced acute kidney injury OR Contrast-induced nephropathy).
The keywords included terms related to the exposure, such as “Sodium-Glucose Transporter 2 Inhibitors” OR “SLGT2 inhibitors” OR “Gliflozins”, and terms related to the outcome, such as “Contrast-induced nephropathy” OR “Contrast-induced acute kidney injury” OR “Contrast related acute kidney injury”. In addition, we conducted manual secondary screening of the references in primary and secondary studies. There were no restrictions on language or publication year. The search strategy is detailed in Supplementary Materials.
Our search included observational studies and randomized controlled trials (RCTs) published from inception until September 30, 2023. We excluded case reports, case series, and duplicated publications. All articles derived from the primary and secondary screenings were compiled using Zotero® 6.0.15. After duplicate removal, these documents were imported into the Rayyan® tool. Then, these records were screened and individually examined by two blinded and independent researchers (MGAR and GAVT). The studies were selected by consensus, and a third researcher acted as the arbitrator (EDMR) in case of discordance. All the articles collected were examined using the terms of the PECO/PICO strategy and the inclusion and exclusion criteria.
There is no consensus on the definition of CIN (32, 33). The criteria initially proposed by Barrett and Parfrey defined CIN as an absolute increase in serum creatinine levels by ≥0.5 mg/dL or a relative increase in serum creatinine by ≥25% from baseline within 72 hours after contrast exposure (34). In a recent meta-analysis, definitions of CIN based on serum creatinine levels ranged from 0.3 to 0.5 mg/dL for an absolute increase and 25 to 50% for a relative increase within 48-72 hours following intravenous contrast administration (35). Consequently, in this systematic review, we considered a patient to have CIN if they met any of the above definitions.
The selected papers were exported into a spreadsheet for a second full-text screening. The study selection process is detailed in Figure 1. For data extraction, the same two blinded and independent researchers performed the selection process, examined articles, and collected the relevant details of the study, such as the authors’ names, country and year of publication, the clinical and epidemiological characteristics of the population, the number of participants and cases, the measures of association, the confounding factors, and the outcomes. For the case of dichotomous and time-to-event variables, we compiled odds ratios (OR), relative risks (RR), and hazard ratios (HR) with 95% confidence intervals (95% CI). If critical data were missing, at least two emails were sent to the corresponding authors. Data from each paper were extracted and recorded in a spreadsheet. In case of a discrepancy, a third researcher (EDMR) solved it if necessary.
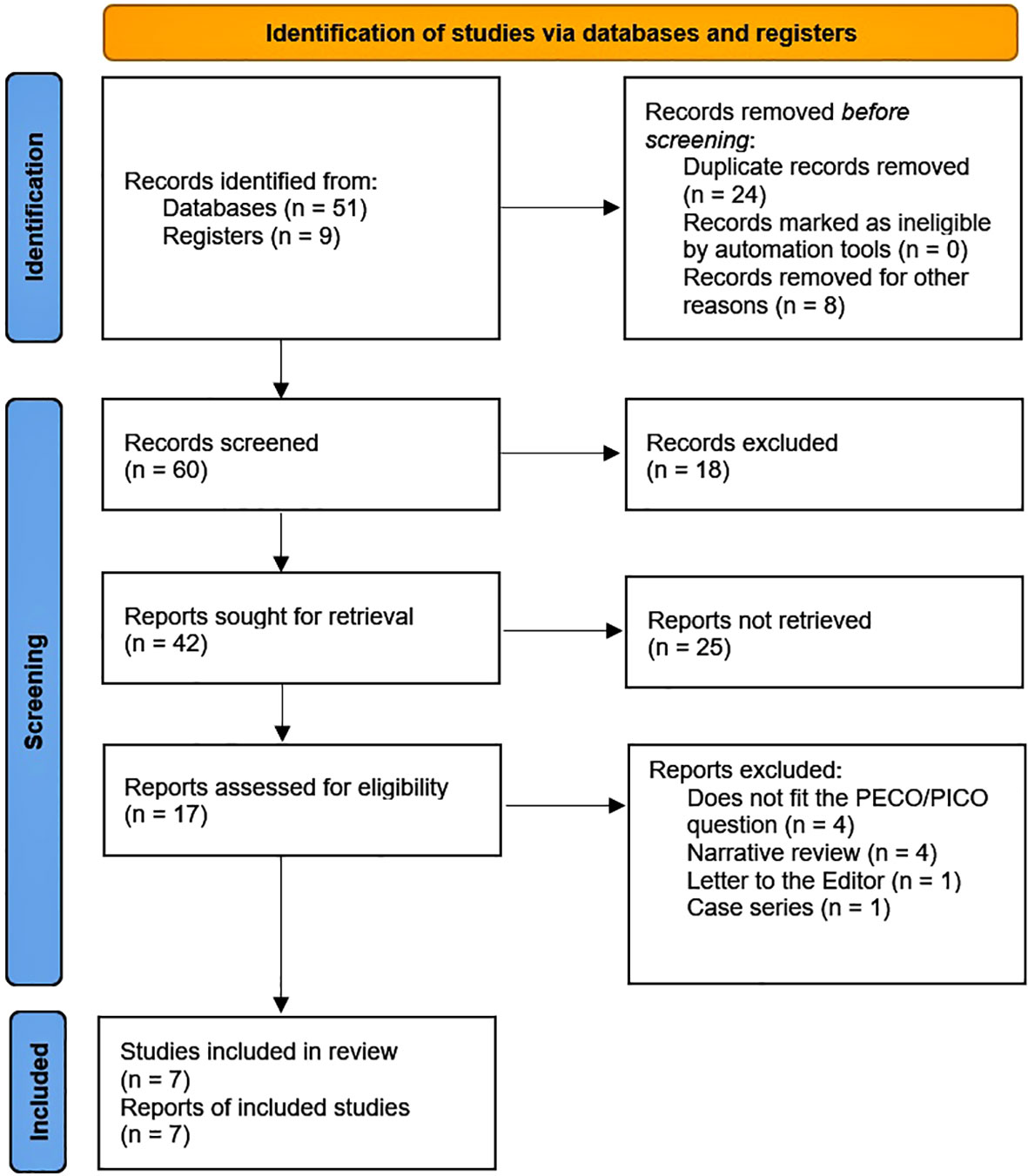
Figure 1 PRISMA 2020 flow diagram.
We pooled adjusted ORs, RRs, or HRs with 95% CIs using the generic inverse-variance method in the meta-analysis. We considered RRs equivalent to the ORs if the frequency of the event of interest was < 10% (36). We performed this meta-analysis using R® 4.2.226 software. We summarized the quantitative synthesis using forest plots using the library meta, function metagen, and inverse variance method with Restricted Maximum-Likelihood (REML) for tau2. Our protocol stated that we would examine heterogeneity among studies with Cochran’s Q test and Higgins I2 statistic, using a fixed effects model if heterogeneity were not statistically significant (p > 0.10, I2 statistics < 40%). On the other hand, we would use a random effects model (29). The potential subgroups to be analyzed were study type, continent of origin, class, and dose of SGLT2I. We conducted sensitivity and influence analysis using the function InfluenceAnalysis.
We assessed the risk of bias using the Newcastle–Ottawa scale (NOS) (37) and version 2 of the Cochrane risk-of-bias tool for randomized trials (ROB 2) (38). We examined the publication bias using a funnel plot.
Two researchers (MGAR and GAVT) independently assessed the certainty of the evidence (CoE) of the study outcomes for each study outcome based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria (39, 40). Any reviewer discrepancy was resolved by discussion with the leading researcher (EDMR).
3 Results
We identified 60 records, 51 of which were retrieved from databases and 9 from registers. Among the latter, all were clinical trials, of which one was already published, and 7 were in different phases of execution, and 1 was suspended. After record removal and exclusion, we found 17 reports for retrieval and for assessing eligibility. Of these studies, 10 were excluded for different reasons (Table S2, Supplementary Material). Finally, we had 7 studies (22–28) included in our review (Table 1). Notably, two papers (22, 23) reported their outcomes with some differences, but the population included was the same. Consequently, in our meta-analysis of these two papers, we only considered the one that reported renal outcomes with more detail (23). Subsequently, we excluded the studies conducted by Bernardini F et al. (27) and Feitosa MPM et al. (28) for the reasons we explain in this section’s second and fourth paragraphs.
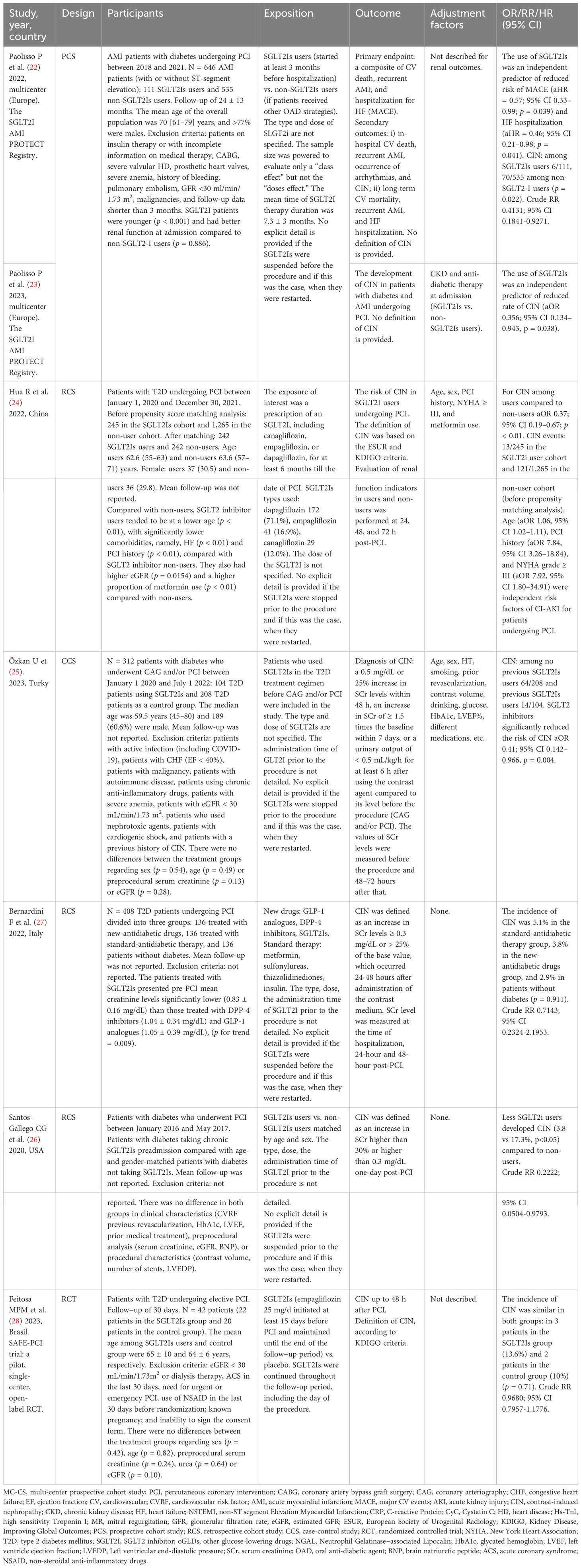
Table 1 General Characteristics of Included Studies.
Of the seven studies included in this systematic review, three were retrospective cohort studies (RCS) (24, 26, 27), two were prospective cohort studies (PCS) (22, 23), one was a case-control design (25), and one was an RCT (28). Three studies were conducted in Europe, two in Asia, and two in America. Of the seven studies included, only one reported the type, dose, and length of administration of the SGLT2I (28). One study reported the class but not the dose or length of the SGLT2I administered (24). Five studies did not report the type, dose, or duration of administration of the SGLT2I (22, 23, 25–27). At first, we excluded the study conducted by Bernardini F et al. (27) because this study compared a group of patients on “new-antidiabetic drugs” (including GLP-1 analogs, DPP-4 inhibitors, and SGLT2Is) vs. “standard therapy” (metformin, sulfonylureas, thiazolidinediones, and insulin) where the authors did not specify the number of patients on SGLT2Is neither specify the outcome of these group of patients.
This systematic review included 3,022 patients with type 2 diabetes mellitus undergoing CAG or PCI, 670 who received treatment with any SLGT2Is, and 306 CIN events. However, our meta-analysis included 2,572 patients, 512 of whom were treated with SGLTI2s and 289 acute renal failure events (Table 1). Most patients were in their sixties, with a minimum age of 45 and a maximum age of 80. The follow-up period varied from 1 to 24 months; however, four studies did not report the length of follow-up. Similarly, most studies did not report outcomes according to sex.
Initially, we conducted a meta-analysis, including five studies (fourth observational and one RCT), obtaining an overall estimate (RR 0.50; 95% CI 0.25–0.99) for the risk of CIN among users of SGLT2Is compared to non-users. Nonetheless, the heterogeneity (I2 = 74%, p < 0.01) was unacceptably high (Figure 2A). We did not conduct subgroup, heterogeneity, or meta-regression analyses due to the scarce number of studies included, which may influence the robustness and ability to obtain significant and reliable results with these methods (29, 41–43). In the sensitivity and influence analysis (Figure 2B), we found that the study by Feitosa MPM et al. (28) had extreme values (outliers) that significantly impacted the overall estimate. Consequently, we excluded this study from our final meta-analysis (Figure 2C).

Figure 2 (A) Forest plot of the effect of SGLT2Is on the risk of developing CIN in patients with diabetes undergoing CAG or PCI considering non-duplicated (RCTs and observational) studies. (B) Plot of the influence analysis considering non-duplicated (RCTs and observational) studies included in the initial meta-analysis. (C) Forest plot of the effect of SGLT2Is on the risk of developing CIN in patients with diabetes undergoing CAG or PCI considering only observational studies.
According to our results, SGLT2Is could reduce the risk of developing CIN by 63% (RR 0.37; 95% CI 0.24–0.58) in patients with diabetes undergoing CAG or PCI (Figure 2C), compared to those not using SGLT2Is. Statistical heterogeneity was not significant (I2 = 0%, p = 0.91).
Of the seven studies included in the systematic review, all six observational studies had a low risk of bias, according to the NOS tool. However, the only RCT included showed some concerns regarding the domain of “performance bias” due to the absence of blinding of participants and personnel and blinding of outcome assessment. Furthermore, the time of the patient’s exposure to SGLT2Is was short (30 days) (28).
GRADE assessment. We upgraded the level of CoE as all the studies included in the meta-analysis showed a low risk of bias (Table 2). Indirectness (the included studies compared similar interventions, similar populations, and similar outcomes), imprecision (this meta-analysis included 2,572 patients with diabetes undergoing CAG or PCI, 512 SGLT2Is users, and 289 events of CIN), publication bias, and inconsistency (I2 = 0) did not impact significantly the CoE. Nonetheless, the number of studies included was small. Then, we assessed the CoE according to GRADE criteria as moderate.
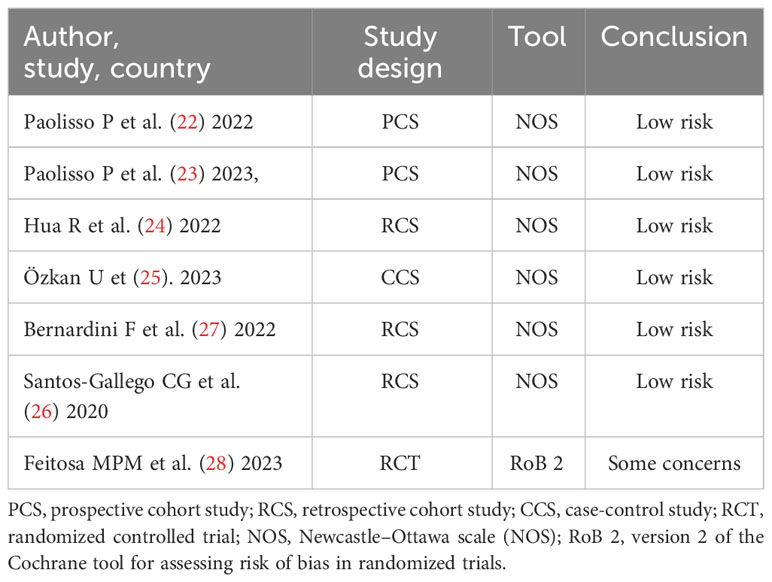
Table 2 Risk of bias of the included studies.
The funnel plot of the included studies in our final meta-analysis did not suggest a publication bias (Figure 3).
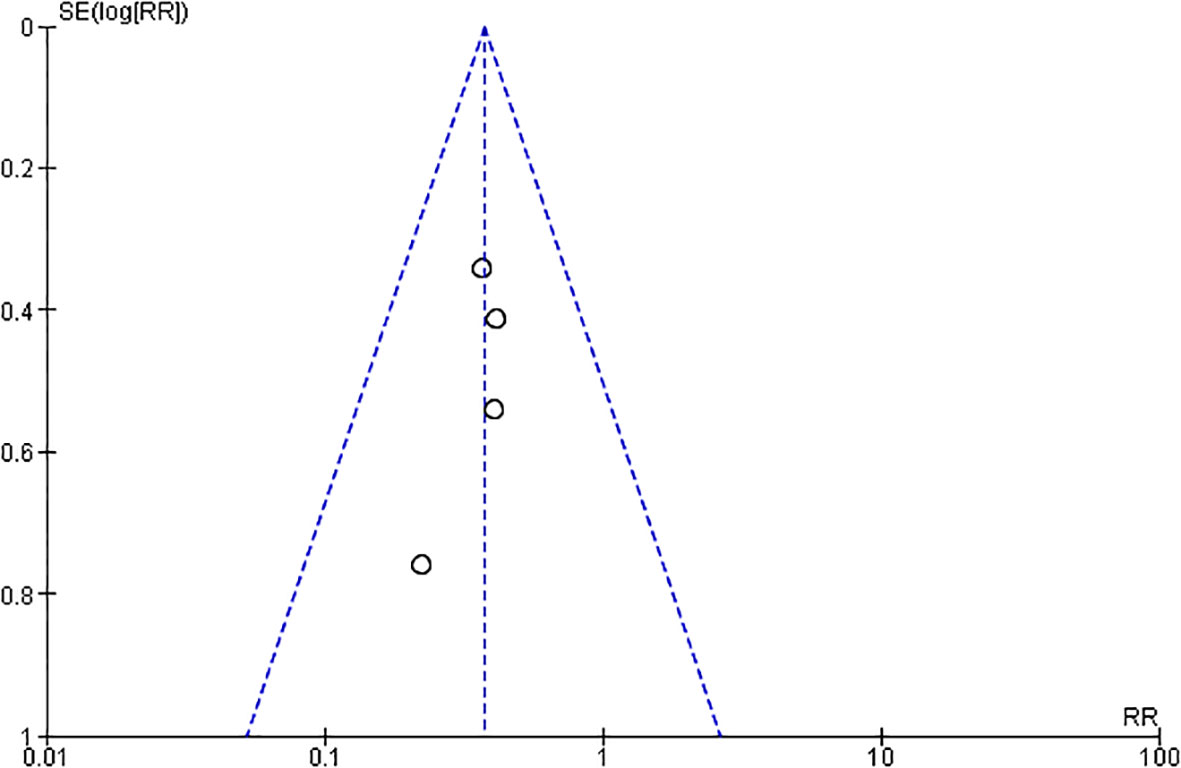
Figure 3 Funnel plot of the included studies in the meta-analysis on the effect of developing CIN in patients with diabetes undergoing CAG or PCI considering only observational studies.
4 Discussion
To our knowledge, this is the first systematic review and meta-analysis to investigate the effect of SGLT2Is on the risk of CIN in patients with diabetes undergoing CAG or PCI. Our findings suggest that SGLT2Is could reduce the risk of developing CIN by up to 63% (RR 0.37; 95% CI 0.24–0.58) in this population.
Since no previous systematic reviews have evaluated our PECO/PICO question, comparing our findings with similar studies is impossible. However, previous evidence derived from observational studies and RCTs is consistent with our results, which have shown that SGLT2Is reduce the risk of CIN in patients with diabetes undergoing invasive cardiac procedures with contrast administration (22–26).
The observational study conducted by Bernardini F et al. reported that patients with diabetes undergoing PCI and in treatment with new OADs (GLP-1 analogs, DPP-4 inhibitors, SGLT2Is) had a reduced incidence of CIN compared to patients with diabetes treated with traditional OADs (metformin, sulfonylureas, thiazolidinediones, insulin). Although this finding did not reach statistical significance (RR 0.7143; 95% CI 0.2324-2.1953), the authors concluded that their study underlined a possible protective role of new anti-diabetic drugs for preventing CIN (27).
Conversely, the only RCT assessing the effect of SGLT2Is on kidney function in patients with diabetes submitted to elective PCI was conducted in Brazil by Feitosa MPM et al. The SAFE−PCI trial was a prospective, open−label, randomized, single−center pilot study with a follow−up of 30 days. But, the objective of this study was quite different from the other studies included in our meta-analysis. They aimed to evaluate the safety of empagliflozin in these patients regarding kidney function. The researchers reported that the incidence of CIN, in the SGLT2Is group was 13.6% and 10.0% in the control group. However, this difference was not statistically significant (calculated RR 0.9680; 95% CI 0.7957-1.1776). They concluded that empagliflozin was safe regarding kidney function during elective PCI in patients with T2D compared with no SGLT2Is (28).
Even though the study by Feitosa MPM et al. was an RCT, we excluded it from our meta-analysis due to several reasons: 1) due to the heterogeneity caused when this study was included, 2) the small sample (22 patients in the intervention group and 20 patients in the control group), 3) concerns regarding the risk of bias due to the absence of blinding of participants, research staff, and outcome assessment, and 4) the short time of exposure to SGLT2Is i.e., “at least 15 days before PCI” (22). Indeed, several studies defined “exposure” to SGLT2Is as a cut-off value of six months because these drugs may render their cardiorenal beneficial effects for patients with T2D after this period (13, 24, 44).
Apart from the previously mentioned study, no other RCT has evaluated the nephroprotective effect of SGLT2Is in patients with diabetes after PCI or CAG. However, at least 8 RCTs are in different implementation stages aiming at answering this question (Supplementary Materials). Nevertheless, some RCTs have shown a renoprotective effect of SGLT2Is in patients with diabetes not undergoing contrast-enhanced coronary procedures. Two multi-center RCTs, the Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME) study and, subsequently, the CANagliflozin cardioVascular Assessment Study (CANVAS), demonstrated a decrease in the incidence of cardiovascular events and mortality with empagliflozin and canagliflozin, respectively (45, 46). Furthermore, these trials have shown that the use of Canagliflozin, Empagliflozin, or Dapagliflozin improved renal outcomes and is associated with slower progression of kidney disease and reduced the need for renal-replacement therapy in T2D (11, 14–16, 46–49).
Patients treated with SGLT2Is may have better kidney function than controls, reducing the baseline risk of CIN and inducing bias in the results of these studies. Of the five studies initially included in our meta-analysis, in the studies by Paoliso et al. (22, 23) and Hua R et al. (24), the patients in the group treated with SGLT2Is were younger. They also had better kidney function than the controls. But, there was no difference between the intervention groups in two other studies, Özkan U et al. (25) and Santos-Gallego CG et al. (26). Similarly, in the study by Feitosa MPM et al. (28), there were no differences in kidney function in both groups. In contrast, in the Bernardini F et al. (27) study, patients treated with SGKT2I had worse kidney function. As commented above, we excluded the last two studies from our final meta-analysis (27, 28).
Although the exact mechanisms by which SGLT2Is protect the kidneys are not fully understood, recent research has shown that these medications have numerous potential nephroprotective effects and traditional hypoglycemic effects. First, SGLT2Is cause osmotic diuresis, which leads to increased volume depletion. This volume depletion may help to protect the kidneys from contrast-induced injury. Second, SGLT2Is reduce renal medullary hypoxia, a significant risk factor for CIN. Third, SGLT2Is reduce glomerular hyperfiltration, decreasing excessive stress on the glomeruli and renal tubules, which could potentially lead to kidney damage over time. Fourth, these drugs have anti-inflammatory, antifibrosis, and antioxidant properties, which may also help to protect the kidneys from contrast-induced injury. Fifth, other proposed mechanisms are enhancing erythropoietin production, improving mitochondrial energy supply, inhibiting the sympathetic nervous system, protecting vascular endothelial cells, and reducing blood uric acid levels, among others (50, 51).
Our study has several strengths. First, we conducted a broad search strategy, including six important databases and registers of clinical trials. Second, we used a rigorous methodology to conduct our review and meta-analysis, including an exhaustive quality assessment of studies and a statistical analysis that accounted for heterogeneity. Third, the lack of statistical heterogeneity suggests that our findings are reliable and quite robust and that the results of individual studies are consistent.
Our study also has some limitations. First, a few completed studies have focused on explicitly answering our PECO/PICO question. Second, all the studies included in our meta-analysis were observational. Observational studies are more prone to bias than RCTs. Third, all the studies included in our meta-analysis were conducted in patients with type 2 diabetes. It is, therefore, possible that our findings may not be generalizable to patients with type 1 diabetes or patients without diabetes. Fourth, most studies included did not specify the type, dose, and duration of SGLT2Is administration. Consequently, performing subgroup analyses based on these factors was impossible.
5 Conclusions
Our findings indicate that SGLT2Is may significantly reduce the risk of CIN by up to 63% in patients with diabetes undergoing CAG or PCI. However, further RCTs are needed. Several RCTs are underway, aiming to confirm our findings and investigate other unresolved issues. These include determining whether SGLT2Is should be discontinued before CAG or PCI and identifying the optimal dose, type, and duration of SGLT2I therapy to prevent CIN, regardless of the presence or absence of diabetes or baseline kidney function.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
EM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MA: Data curation, Investigation, Validation, Visualization, Writing – review & editing. GV: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1307715/full#supplementary-material
References
1. Fan W. Epidemiology in diabetes mellitus and cardiovascular disease. Cardiovasc Endocrinol (2017) 6:8–16. doi: 10.1097/XCE.0000000000000116
2. Wang F, Yu Y, Mubarik S, Zhang Y, Liu X, Cheng Y, et al. Global burden of ischemic heart disease and attributable risk factors, 1990–2017: A secondary analysis based on the global burden of disease study 2017. Clin Epidemiol (2021) 13:859–70. doi: 10.2147/CLEP.S317787
3. Low Wang CC, Hess CN, Hiatt WR, Goldfine AB. Clinical update: cardiovascular disease in diabetes mellitus. Circulation (2016) 133:2459–502. doi: 10.1161/CIRCULATIONAHA.116.022194
4. Sany D, Refaat H, Elshahawy Y, Mohab A, Ezzat H. Frequency and risk factors of contrast-induced nephropathy after cardiac catheterization in type II diabetic patients: a study among Egyptian patients. Ren Fail (2014) 36:191–7. doi: 10.3109/0886022X.2013.843400
5. Zaytseva NV, Shamkhalova MS, Shestakova MV, Matskeplishvili ST, Tugeeva EF, Buziashvili UI, et al. Contrast-induced nephropathy in patients with type 2 diabetes during coronary angiography: Risk-factors and prognostic value. Diabetes Res Clin Pract (2009) 86:S63–9. doi: 10.1016/S0168-8227(09)70012-9
6. Yang J, Ran P, Chen J, He Y, Li L, Tan N, et al. Development of contrast-induced acute kidney injury after elective contrast media exposure in patients with type 2 diabetes mellitus: effect of albuminuria. PLoS One (2014) 9:e106454. doi: 10.1371/journal.pone.0106454
7. Nadkarni GN, Ferrandino R, Chang A, Surapaneni A, Chauhan K, Poojary P, et al. Acute kidney injury in patients on SGLT2 inhibitors: A propensity-matched analysis. Diabetes Care (2017) 40:1479–85. doi: 10.2337/dc17-1011
8. U.S. Food and Drug Administration. FDA warns about rare occurrences of serious infection in the genital area with SGLT2 inhibitors for diabetes. Silver Spring (MD): U.S. Food and Drug Administration; [published August 29, 2018]. Available at: https://www.fda.gov/drugs/drug-safety-and-availability/fda-warns-about-rare-occurrences-serious-infection-genital-area-sglt2-inhibitors-diabetes [Accessed October 24, 2023].
9. Agarwal R, Anker SD, Filippatos G, Pitt B, Rossing P, Ruilope LM, et al. Effects of canagliflozin versus finerenone on cardiorenal outcomes: exploratory post hoc analyses from FIDELIO-DKD compared to reported CREDENCE results. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc - Eur Ren Assoc (2022) 37:1261–9. doi: 10.1093/ndt/gfab336
10. Bazoukis G, Papadatos SS, Thomopoulos C, Tse G, Cheilidis S, Tsioufis K, et al. Impact of SGLT2 inhibitors on major clinical events and safety outcomes in heart failure patients: a meta-analysis of randomized clinical trials. J Geriatr Cardiol JGC (2021) 18:783–95. doi: 10.11909/j.issn.1671-5411.2021.10.003
11. Heerspink HJL, Kosiborod M, Inzucchi SE, Cherney DZI. Renoprotective effects of sodium-glucose cotransporter-2 inhibitors. Kidney Int (2018) 94:26–39. doi: 10.1016/j.kint.2017.12.027
12. Heerspink HJL, Perkins BA, Fitchett DH, Husain M, Cherney DZI. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation (2016) 134:752–72. doi: 10.1161/CIRCULATIONAHA.116.021887
13. Mosenzon O, Wiviott SD, Cahn A, Rozenberg A, Yanuv I, Goodrich EL, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol (2019) 7:606–17. doi: 10.1016/S2213-8587(19)30180-9
14. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med (2019) 380:347–57. doi: 10.1056/NEJMoa1812389
15. Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med (2016) 375:323–34. doi: 10.1056/NEJMoa1515920
16. Wanner C. EMPA-REG OUTCOME: the nephrologist’s point of view. Am J Med (2017) 130:S63–72. doi: 10.1016/j.amjmed.2017.04.007
17. Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou F-F, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med (2020) 383:1436–46. doi: 10.1056/NEJMoa2024816
18. The EMPA-KIDNEY Collaborative Group. Empagliflozin in patients with chronic kidney disease. N Engl J Med (2023) 388:117–27. doi: 10.1056/NEJMoa2204233
19. Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med (2020) 383:1413–24. doi: 10.1056/NEJMoa2022190
20. McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med (2019) 381:1995–2008. doi: 10.1056/NEJMoa1911303
21. Mc Causland FR, Claggett BL, Vaduganathan M, Desai AS, Jhund P, de Boer RA, et al. Dapagliflozin and kidney outcomes in patients with heart failure with mildly reduced or preserved ejection fraction: A prespecified analysis of the DELIVER randomized clinical trial. JAMA Cardiol (2023) 8:56–65. doi: 10.1001/jamacardio.2022.4210
22. Paolisso P, Bergamaschi L, Gragnano F, Gallinoro E, Cesaro A, Sardu C, et al. Outcomes in diabetic patients treated with SGLT2-Inhibitors with acute myocardial infarction undergoing PCI: The SGLT2-I AMI PROTECT Registry. Pharmacol Res (2023) 187:106597. doi: 10.1016/j.phrs.2022.106597
23. Paolisso P, Bergamaschi L, Cesaro A, Gallinoro E, Gragnano F, Sardu C, et al. Impact of SGLT2-inhibitors on contrast-induced acute kidney injury in diabetic patients with acute myocardial infarction with and without chronic kidney disease: Insight from SGLT2-I AMI PROTECT registry. Diabetes Res Clin Pract (2023) 202:110766. doi: 10.1016/j.diabres.2023.110766
24. Hua R, Ding N, Guo H, Wu Y, Yuan Z, Li T. Contrast-induced acute kidney injury in patients on SGLT2 inhibitors undergoing percutaneous coronary interventions: A propensity-matched analysis. Front Cardiovasc Med (2022) 9:918167. doi: 10.3389/fcvm.2022.918167
25. Özkan U, Gürdoğan M. The effect of SGLT2 inhibitors on the development of contrast-induced nephropathy in diabetic patients with non-ST segment elevation myocardial infarction. Med Kaunas Lith (2023) 59:505. doi: 10.3390/medicina59030505
26. Santos-Gallego C, Palamara G, Requena-Ibanez J, Vargas A, Mohebi R, Abascal V, et al. Pretreatment with SGLT2 inhibitors ameliorates contrast-induced nephropathy. J Am Coll Cardiol (2020) 75:1405–5.
27. Bernardini F, Nusca A, Giannone S, Mangiacapra F, Melfi R, Ricottini E, et al. Role of new antidiabetic drugs in the prevention of contrast induced nephropathy in diabetic patients undergoing percutaneous coronary intervention. Eur Heart J Suppl (2022) 24:K179. doi: 10.1093/eurheartjsupp/suac121.499
28. Feitosa MPM, Lima EG, Abizaid AAC, Mehran R, Lopes NHM, de Assis Fischer Ramos T, et al. The safety of SGLT-2 inhibitors in diabetic patients submitted to elective percutaneous coronary intervention regarding kidney function: SAFE-PCI pilot study. Diabetol Metab Syndr (2023) 15:138. doi: 10.1186/s13098-023-01107-9
29. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane (2023). Available at: www.training.cochrane.org/handbook.
30. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
31. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (2017) 358:j4008. doi: 10.1136/bmj.j4008
32. Modi K, Padala SA, Gupta M. Contrast-Induced Nephropathy. Treasure Island (FL: StatPearls Publishing (2023). Available at: http://www.ncbi.nlm.nih.gov/books/NBK448066/.
33. Meinel FG, De Cecco CN, Schoepf UJ, Katzberg R. Contrast-induced acute kidney injury: definition, epidemiology, and outcome. BioMed Res Int (2014) 2014:859328. doi: 10.1155/2014/859328
34. Barrett BJ, Parfrey PS. Prevention of nephrotoxicity induced by radiocontrast agents. N Engl J Med (1994) 331:1449–50. doi: 10.1056/NEJM199411243312111
35. Moro AB, Strauch JGN, Groto AD, Toregeani JF. Creatinine level variation in patients subjected to contrast-enhanced tomography: a meta-analysis. J Vasc Bras (2021) 20:e20200161. doi: 10.1590/1677-5449.200161
36. McKenzie DP, Thomas C. Relative risks and odds ratios: Simple rules on when and how to use them. Eur J Clin Invest (2020) 50. doi: 10.1111/eci.13249
37. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute. Available at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp [Accessed October 30, 2023].
38. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ (2019) 366:l4898. doi: 10.1136/bmj.l4898
39. Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Syst Rev (2014) 3:82. doi: 10.1186/2046-4053-3-82.
40. Granholm A, Alhazzani W, Møller MH. Use of the GRADE approach in systematic reviews and guidelines. Br J Anaesth (2019) 123:554–9. doi: 10.1016/j.bja.2019.08.015
41. Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods (2006) 11:193–206. doi: 10.1037/1082-989X.11.2.193
42. Higgins JPT. Measuring inconsistency in meta-analyses. BMJ (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
43. Geissbühler M, Hincapié CA, Aghlmandi S, Zwahlen M, Jüni P, da Costa BR. Most published meta-regression analyses based on aggregate data suffer from methodological pitfalls: a meta-epidemiological study. BMC Med Res Methodol (2021) 21:123. doi: 10.1186/s12874-021-01310-0
44. Verma S, Mazer CD, Yan AT, Mason T, Garg V, Teoh H, et al. Effect of empagliflozin on left ventricular mass in patients with type 2 diabetes mellitus and coronary artery disease. Circulation (2019) 140:1693–702. doi: 10.1161/CIRCULATIONAHA.119.042375
45. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med (2015) 373:2117–28. doi: 10.1056/NEJMoa1504720
46. Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med (2017) 377:644–57. doi: 10.1056/NEJMoa1611925
47. de Vos LC, Hettige TS, Cooper ME. New glucose-lowering agents for diabetic kidney disease. Adv Chronic Kidney Dis (2018) 25:149–57. doi: 10.1053/j.ackd.2018.01.002
48. Satirapoj B. Sodium-glucose cotransporter 2 inhibitors with renoprotective effects. Kidney Dis Basel Switz (2017) 3:24–32. doi: 10.1159/000471765
49. Vallon V, Thomson SC. Targeting renal glucose reabsorption to treat hyperglycaemia: the pleiotropic effects of SGLT2 inhibition. Diabetologia (2017) 60:215–25. doi: 10.1007/s00125-016-4157-3
50. Chu C, Lu Y-P, Yin L, Hocher B. The SGLT2 inhibitor empagliflozin might be a new approach for the prevention of acute kidney injury. Kidney Blood Press Res (2019) 44:149–57. doi: 10.1159/000498963
Keywords: sodium-glucose transporter 2 inhibitors, SGLT2 inhibitors, acute kidney injury, contrast-induced nephropathy, systematic review, meta-analysis
Citation: Meregildo-Rodriguez ED, Asmat-Rubio MG and Vásquez-Tirado GA (2023) SGLT-2 inhibitors and prevention of contrast-induced nephropathy in patients with diabetes undergoing coronary angiography and percutaneous coronary interventions: systematic review and meta-analysis. Front. Endocrinol. 14:1307715. doi: 10.3389/fendo.2023.1307715
Received: 05 October 2023; Accepted: 05 December 2023;
Published: 20 December 2023.
Edited by:
Manoocher Soleimani, University of New Mexico, United StatesReviewed by:
Peter Fasching, Vienna Health Association, AustriaMahmoud Nassar, University at Buffalo, United States
Copyright © 2023 Meregildo-Rodriguez, Asmat-Rubio and Vásquez-Tirado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Edinson Dante Meregildo-Rodriguez, ZWRtZXJlZ2lsZG9AdWN2dmlydHVhbC5lZHUucGU=