 Kenana Hatab1
Kenana Hatab1 Fadila Serdarevic2,3,4
Fadila Serdarevic2,3,4 Aisha Yousuf5
Aisha Yousuf5 Sarah Al Ali1Khawla Eissa Ahmed M. Al Hajaj5,6Fatima Mohamed Abdulla Mohamed Almarzooqi7Leena Tawfiq Swaidan8Elsheikh Farah ElHassan8Mahra Nooruddin Abdulwahid Kazim9Hanan Hamza Ahmed Abdalla7Hanan Ali Al-Muhaureq7Salah Mohammed Thabit7Hassan Abdulla BaKhamis5
Sarah Al Ali1Khawla Eissa Ahmed M. Al Hajaj5,6Fatima Mohamed Abdulla Mohamed Almarzooqi7Leena Tawfiq Swaidan8Elsheikh Farah ElHassan8Mahra Nooruddin Abdulwahid Kazim9Hanan Hamza Ahmed Abdalla7Hanan Ali Al-Muhaureq7Salah Mohammed Thabit7Hassan Abdulla BaKhamis5 Sabina Semiz1,10*
Sabina Semiz1,10*- 1College of Medicine and Health Sciences, Khalifa University of Science and Technology, Abu Dhabi, United Arab Emirates
- 2Sarajevo School of Science and Technology, Sarajevo Medical School, Sarajevo, Bosnia and Herzegovina
- 3Erasmus Medical Center, Rotterdam, Netherlands
- 4Center for Epidemiology and Statistics ("EpiSTa"), Sarajevo, Bosnia and Herzegovina
- 5Za’abeel Health Center, Dubai Health, Dubai, United Arab Emirates
- 6Dubai Health Authority, Dubai, United Arab Emirates
- 7Almizhar Health Center, Dubai Health, Dubai, United Arab Emirates
- 8Al Towar Health Center, Dubai Health, Dubai, United Arab Emirates
- 9Al Barsha Health Center, Dubai Health, Dubai, United Arab Emirates
- 10Center for Biotechnology, Khalifa University of Science and Technology, Abu Dhabi, United Arab Emirates
Objectives: Given the increasing prevalence of type 2 diabetes (T2D) in the United Arab Emirates (UAE), in this cross-sectional study we analyzed the dietary habits, physical activity, as well as anthropometric, clinical, and laboratory parameters in patients with T2D and nondiabetic (ND) subjects from the UAE.
Subjects and Methods: This study included 344 UAE nationals, age 18 or older, who completed a questionnaire to assess their dietary habits and physical activity. The mean age of the recruited participants was 50.9 years (+/-14.1) and females presented 63.4% of the sample size. The linear regression analysis was applied to analyze all clinical parameters and dietary habits as outcomes, while a logistic regression analysis was used to determine the association of patient status with physical activity, as an outcome. All models were controlled for age, gender, and BMI.
Results: There was a difference in dietary habits between the groups (B=-3.7; CI -6.42, -0.92; p=0.009), where patients with T2D had a lower dietary score than ND subjects, indicating a healthier diet. Our results showed that 19% of T2D patients and 32% of nondiabetic individuals were concerned about their weight. Both groups considered dietary changes important, and more than 90% of participants expressed high or moderate confidence in making those changes. Furthermore, the male nondiabetic subjects demonstrated a 4 times higher level of physical activity versus their diabetic counterparts (OR=4.01, CI: 1.01, 15.9, p=0.04), while the difference in physical activity between female subjects with and without T2D was not demonstrated.
Conclusions: Our results showed that patients with T2D consumed a healthier diet than nondiabetic subjects, probably resulting in more favorable total cholesterol and LDL-cholesterol profiles. A gender difference in physical activity was also observed in this sample of UAE population. Our findings suggest that although patients with T2D in the UAE may adopt healthier dietary habits, there remains a significant need to address physical activity disparities, particularly among women, to improve overall health outcomes in this population. Addressing these habits through targeted clinical interventions and lifestyle medicine approach can optimize long-term management and prevention strategies for type 2 diabetes in this region.
Introduction
Diabetes is considered as one of the major pandemics of the 21st century, affecting 537 million people in 2021 (1). This chronic metabolic disorder, characterized by elevated blood glucose levels, is one of leading causes of morbidity and mortality, with its prevalence expected to increase significantly. It is estimated that by 2045 the number of diabetic patients will increase to 700 million worldwide, with the second highest expected increase (86%) reaching 136 million diabetic individuals in the Middle Eastern and North African (MENA) region (1). Furthermore, it is suggested that, in particular, the Gulf countries, located within this region, have high risk factors for type 2 diabetes (T2D) (2), with a prevalence of about 16% in the United Arab Emirates (UAE) (1), estimated to reach 21% by 2030 (3, 4).
The development of T2D is multifactorial, with a strong association to lifestyle factors such as obesity, unhealthy dietary habits, and a sedentary lifestyle. The global rise in obesity rates (5–7), which has been particularly noticeable in the Gulf countries (2, 8–10), is contributing to the escalating prevalence of T2D. Obesity, a major risk factor for insulin resistance and T2D, has reached alarming levels in the UAE (11). Based on the recent UAE national data, 74% of adults in the UAE are classified as overweight, with 37% of them being obese (12). Furthermore, childhood obesity is an increasing concern (13–16), with recent estimates indicating that 17% of children in the UAE are classified as overweight or obese (17). This is particularly worrying given that children who are overweight or obese face up to 80% risk of remaining obese later in adulthood, thus increasing their lifetime risk of developing T2D (18).
In addition to obesity, lifestyle factors such as physical inactivity and poor dietary habits play critical roles in the development of T2D. Previous studies performed in the UAE population showed that an accentuated exposure to sedentary lifestyle characterized by limited physical activity, combined with an increased consumption of calorie-dense food (19, 20) increase risk for obesity (7), insulin resistance (21), impaired glucose tolerance and onset of T2D (22). Despite these concerns, there remains a dearth of comprehensive studies examining the relationship between lifestyle habits and T2D-related traits in the UAE population.
Considering the growing burden of T2D in the region, the primary objective of this study is to investigate the dietary habits, physical activity levels, and their associations with T2D-related traits in individuals in the UAE. The secondary objectives aim to explore if participants’ gender may influence the relationship between lifestyle habits and diabetes-related traits in patients with T2D and in nondiabetic subjects, as well as to assess participants’ views and attitudes towards their weight and diet. Understanding these associations is crucial for developing targeted public health interventions and promoting lifestyle modifications that could reduce the growing incidence of diabetes and help guide preventive and clinical strategies tailored to the UAE and the broader region.
Subjects and methods
Subjects
We conducted a cross-sectional study involving 344 subjects, including 218 patients with type 2 diabetes and 126 nondiabetic subjects, who were recruited consecutively from March 2021 to September 2022 at Zabeel, Al Mizhar, Al Towar, and Al Barsha primary healthcare centers in Dubai, United Arab Emirates. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist was used as reporting tool (23). All participants met the major inclusion criteria, which included being a UAE national, 18 years old or older, and providing signed consent. Patients with chronic gastrointestinal diseases, including chronic liver disease, cholelithiasis, chronic pancreatitis, inflammatory bowel disease and gastroduodenal ulcer, chronic kidney disease, endocrine disorders, infection and hormonal therapy were excluded. Demographic data, anthropometric measurements, and biochemical parameters were obtained from the participant’s medical records.
The study was approved by the Research Ethics Committee of the Khalifa University, Department of Health Abu Dhabi and Dubai Scientific Research Ethics Committee, Dubai Health Authority.
Questionnaire
In order to assess the participants’ dietary habits and physical activity, the study participants completed a questionnaire including the selected questions from the UK Diabetes & Diet Questionnaire (UKDDQ) and the Nurse Health Studies II Physical Activity questionnaire (NHSPAQ). Sixteen out of the nineteen questions contributed to the overall dietary score, while the remaining three questions addressed weight concerns, the significance of dietary changes, and the participants’ confidence in making such changes. The interviewed subjects were also asked to specify how frequently they consumed various food items from different groups over the past month. They were given options to describe their consumption frequency, ranging from “never,” “very rarely or less than once a week,” “1–4 times a week,” and “5 times to every day in a week.” The total dietary score was obtained by summing the raw values of all UKDDQ items, with higher scores indicating less healthy dietary choices (24). The Nurse Health Studies II Physical Activity questionnaire included questions about the participants’ physical lifestyle habits, classifying them as physically active based on their exercise duration and work type (25). This questionnaire included inquiries about the frequency of the participants’ physical activity per week in the past year and their participation in recreational activities. Additionally, the nature of the participants’ occupations contributed to the final evaluation, mainly if they were engaged in physically demanding fields. The hours of physical activity were systematically calculated and subsequently categorized into two distinct groups based on WHO recommendation (World Health Organization, Guidelines on physical activity and sedentary behavior, 2020) (26). Patients who exercised for 150–300 minutes or more per week were classified as exhibiting a “physically active” status, whereas patients engaging in less exercise in one week were classified as demonstrating a “physically inactive” status.
Clinical and biochemical parameters
After obtaining consent, the study participants provided a blood sample for measuring various biochemical parameters, including but not limited to fasting glucose (FG), glycated hemoglobin (HbA1c), fasting insulin (FI), total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and C-reactive protein (CRP). The body mass index (BMI) was calculated by dividing the participant’s weight by their height in square meters. BMI categories were defined according to the World Health Organization (WHO) classifications as underweight (BMI < 18.8 m^2), average weight (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (≥ 30 kg/m2). Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) was calculated by using the equation HOMA-IR = [fasting insulin (pmol/l) x fasting glucose (mmol/l)]/156.26.
Statistical analysis
We estimated the differences between diabetic and nondiabetic participants regarding their physical activity by using the logistic regression analysis, as well as regarding their dietary habits and biochemical parameters by using the linear regression analysis. We adjusted all analysis for age, gender, and BMI. Statistical significance was considered when the two-tailed p-value was < 0.05. Laboratory data were standardized using z-scores.
Sensitivity analysis
We additionally adjusted all models for participants’ education.
Results
The characteristics of the study participants are presented in Table 1. Out of all participants with type 2 diabetes, 60.7% were females and 66.1% completed high school or less, while in the group of nondiabetic subjects, 69.7% were females and 44% completed high school or less. Patients with T2D had on average BMI 30.4 (SD=6.3) and nondiabetic subjects had on average BMI 29.1 (SD=6.1), and based on the WHO classification, were considered as obese and overweight, respectively.
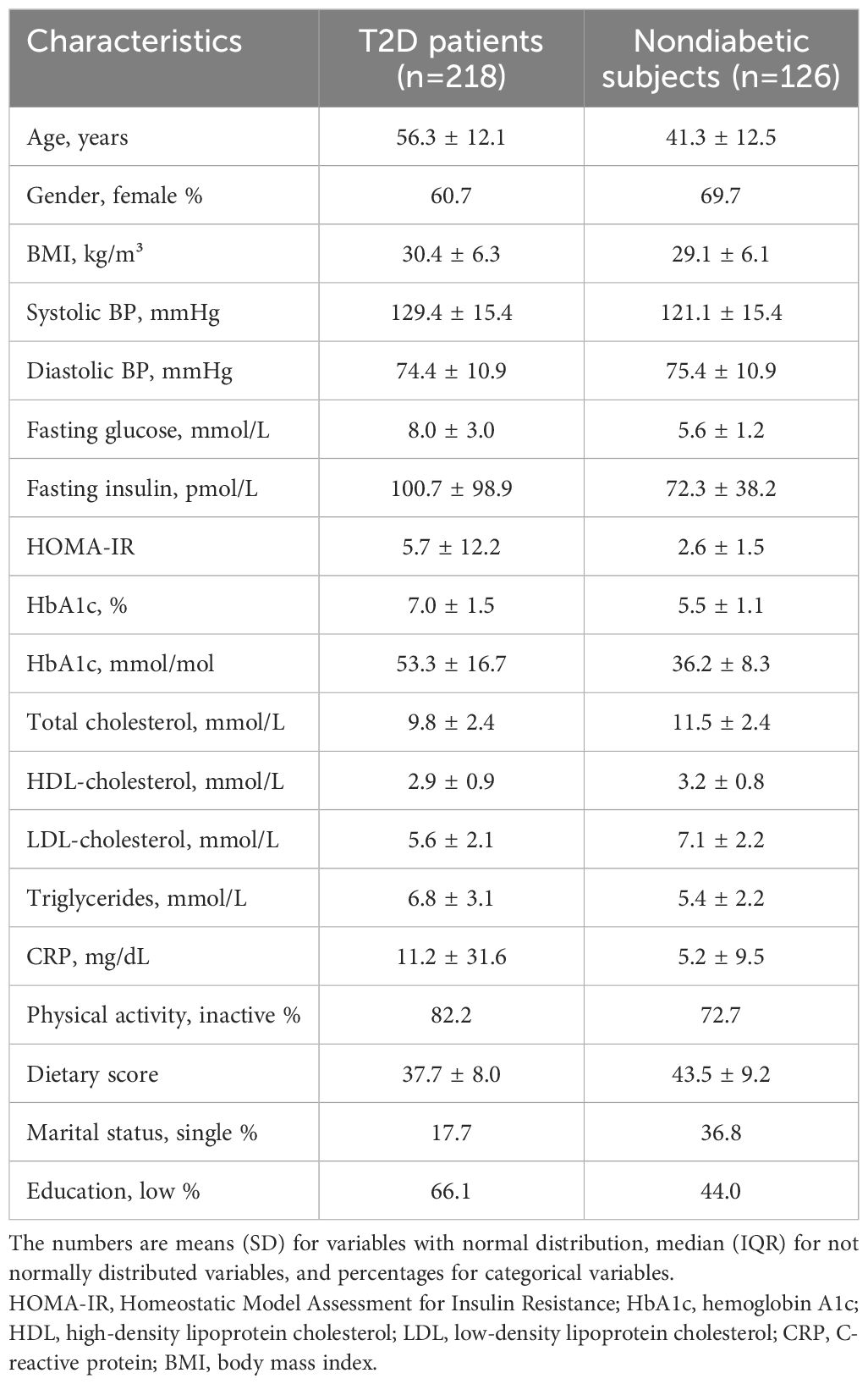
Table 1. Characteristics of patients with T2D and nondiabetic subjects participating in this study (n=344).
As expected, the levels of fasting glucose, fasting insulin, HbA1c, HOMA-IR, triglycerides, and CRP were increased in patients with T2D, as compared to nondiabetic subjects, after adjusting for age, gender, and BMI (Table 2). Furthermore, HDL-cholesterol levels were lower in T2D patients. The concentration of TC and LDL-cholesterol was also lower in diabetic patients than in nondiabetic subjects (Table 2).
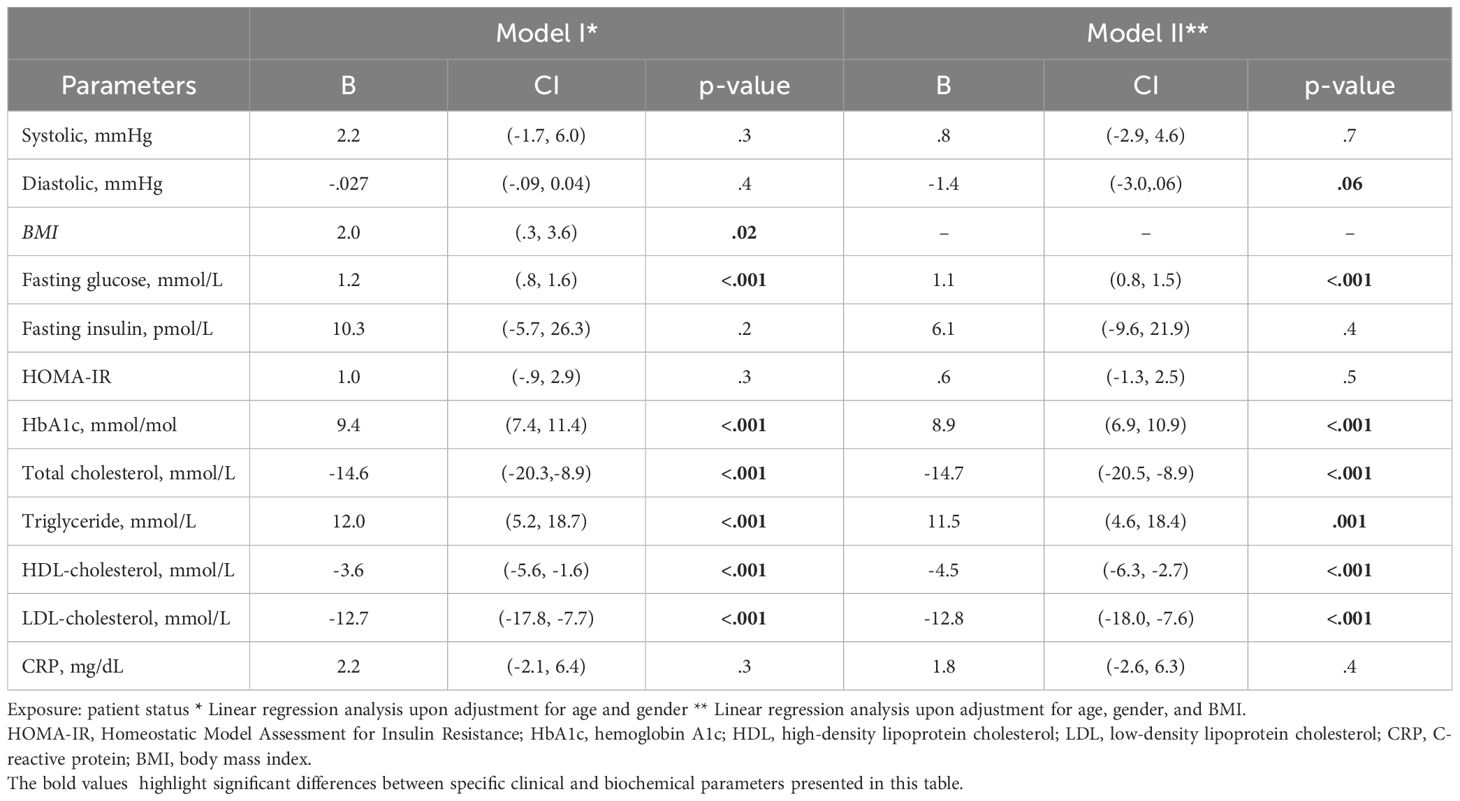
Table 2. The clinical and biochemical parameters in T2D patients and nondiabetic subjects.
Most of the participants with T2D (82.2%) and nondiabetic subjects (72.7%) reported to be physically inactive (Table 1). We did not observe a difference in physical activity between T2D patients and nondiabetic subjects (OR=1.0 CI: 0.48, 2.43, p=0.85). Furthermore, our results also showed that males exercised 3.1 times more than female subjects upon controlling for patient status, age and BMI (OR=3.1, CI:1.58, 6.09, p<.001). We did not observe a significant difference in physical activity between the two groups of female subjects. The male subjects with T2D demonstrated a 4 times lower level of physical activity versus their nondiabetic counterparts (OR=4.01, CI:1.01, 15.9, p=0.04).
We observed a significant difference in dietary habits between patients with T2D and nondiabetic subjects (B=-3.8; CI -6.03, -0.72; p=0.01), indicating healthier diet consumption by T2D patients. Patients with T2D were more likely to consume less fast food and sweets, and more fruits and vegetables when compared to nondiabetic individuals (B=-1.8; CI -3.4, -0.2; p=0.029). Female participants with diabetes have a lower mean dietary score, indicating healthier dietary habits as compared to female nondiabetic subjects (B=-3.7; CI -6.40, -0.94; p=0.009). A similar trend in dietary habits between male participants with and without type 2 diabetes was also observed, however this difference was not significant (B=-2.5; CI -8.61, 3.65; p=0.42).
Due to observed significant interactions of gender with BMI upon age adjustment (p=0.02) and a tendency of gender interaction with diastolic blood pressure (p=0.06) (Table 2), we analyzed the BMI separately in female and male participants. As shown in the Supplementary Table 1, there was no significant difference in BMI and blood pressure values between male subjects with T2D and nondiabetic males. However, our results demonstrated a difference in BMI between female diabetic patients and nondiabetic subjects upon age adjustment (B=2.25; CI: -8.61, -3.65, p = 0.04) (Supplementary Table 2).
The participants’ views regarding their weight and diet change are summarized in Table 3. These findings indicate that about 19% of T2D patients and 32% of nondiabetic subjects were moderately or very concerned about their weight. Changing their diet was shown to be of high or moderate importance to both of these study groups. Furthermore, both diabetic and nondiabetic subjects showed a self-confidence in diet change, with about 96% of T2D patients and 92% nondiabetic individuals demonstrating high or moderate confidence in changing their diet (Table 3). There was no significant difference in the participants’ views and attitudes towards their weight and diet between male and female subjects (Supplementary Tables 3, 4).
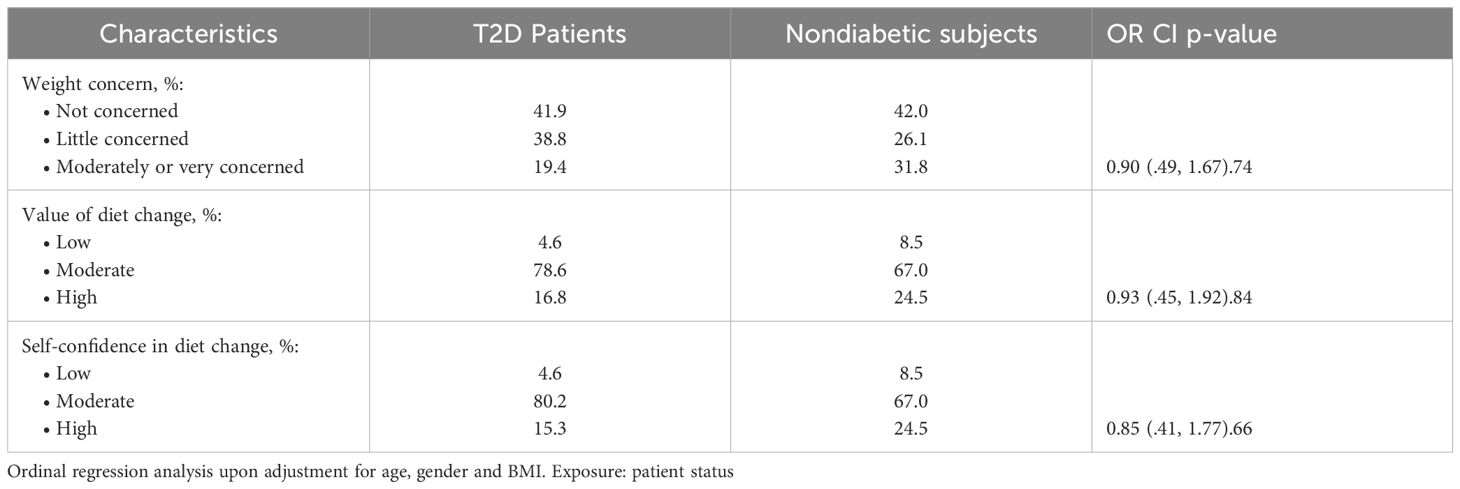
Table 3. Participants’ views and attitudes towards their weight and diet.
All results did not materially change upon additionally controlling for the participants’ educational status.
Discussion
This study offers crucial insights into the lifestyle factors that contribute to type 2 diabetes management and prevention within the UAE population. Given the rising prevalence of T2D in the UAE (1, 3, 4), understanding the role of dietary habits, physical activity, and their association with T2D traits is essential for optimizing healthcare interventions. Our finding that individuals with T2D reported healthier dietary habits than their nondiabetic counterparts is particularly noteworthy, as it suggests that diabetes may influence individuals to make healthier food choices, potentially contributing to improved lipid profiles and other metabolic markers. However, the study also highlights a significant disparity in physical activity levels between male diabetic and nondiabetic subjects, with nondiabetic men being significantly more active. This gender-specific difference in physical activity warrants further investigation, as it could have important implications for targeted health promotions and interventions aimed at increasing physical activity among individuals with T2D, particularly in female subjects.
This study was performed in the sample of the UAE nationals residing in Dubai. Although the participants were recruited randomly during the course of this study, the majority of them were overweight or obese, including the patients with T2D and nondiabetic subjects. Thus, these findings indicate an increased prevalence of overweight/obesity in this population sample, which aligns with previous studies demonstrating an increased prevalence of overweight/obesity in the UAE (7, 11, 12, 22), including the Emirate of Dubai (27). The cross-sectional survey performed in the Emirate of Dubai in 2019 (27) reported that the overall prevalence of overweight and obesity was about 40% and 18%, respectively, with the highest obesity rates being in UAE nationals (39.6%) as compared to the other ethnic groups living in this Emirate. It was shown that similar to Kuwait and Saudi Arabia, the UAE has one of the highest prevalence of overweight/obesity (2, 8) and type 2 diabetes (28) among the Gulf Cooperation Council (GCC) countries. Furthermore, a systematic review by Radwan et al. (11) reported a high prevalence rate of obesity and diabetes in the UAE, as well as noticed a 2 to 3-fold increase in the prevalence of overweight/obesity between 1989 and 2017.
A few studies performed in the UAE pointed out the role of gender in obesity risk, with the male individuals appearing to be more prone to being obese than females (17). Another recent study demonstrated an alarming high prevalence of extreme obesity in the UAE, especially among boys (29, 30). On the other hand, previous reports performed in the adult UAE population showed a high percentage of females being overweight (27%) and obese (16%), suggesting that adult females were more prone to be obese than adult males (31). This is in line with recent findings, which also demonstrated that women had a higher BMI across different countries in the Middle East, including the UAE (32). Furthermore, a recent cross-sectional survey performed in the Emirate of Dubai in 2019 reported a high obesity rate (21.6%), as well as a higher obesity risk in female than in male subjects (27). Our results did not show a significant difference in BMI between female and male subjects in this sample of the Emirati population. A reason for this discrepancy might be the smaller sample size in the current study. However, there was a difference in BMI between female diabetic and nondiabetic subjects upon age adjustment, while the significant difference in BMI between T2D and nondiabetic male individuals was not observed.
The risk for becoming overweight and obese has been linked with the urbanization and high socioeconomic status observed in Gulf countries, including Saudi Arabia and the UAE (33, 34). It appears that the influx of Western lifestyles led to changes in behavioral patterns and in the habits of food consumption in the UAE, through having an easy access to processed food and high-calorie beverages, as well as to a sedentary lifestyle (17, 28). It was shown that participants’ fast-food consumption and time spent watching TV were associated with an increased BMI (13), and that consuming less than five servings of fruits/vegetables per day and being physically inactive are the leading predictors of obesity (30). Furthermore, the suboptimal diet was found to be the primary risk factor for cardiometabolic disease mortality in the Middle East countries, accounting for 72% in the UAE (32). Our study showed that the average dietary score was higher in T2D patients than in nondiabetic subjects, suggesting that diabetic patients improved their diet following the diagnosis of diabetes by being more likely to consume less fast food and sweets, and more fruits and vegetables, as indicated by the questionnaire. These adopted changes in their diet probably had a beneficial effect on the lipid profile, including total cholesterol and LDL-cholesterol levels, which were lower in patients with T2D as compared to nondiabetic subjects in this sample of UAE population. Choosing to consume a healthier diet might be related to an increased awareness of diabetic patients participating in our study about the impact of changing their dietary habits on diabetes management. As demonstrated by the questionnaire, altering their diet appeared to be important to all study participants, with the apparent higher percentage of T2D patients considering moderate or high value of diet change vs nondiabetic subjects.
The global age-standardized prevalence of insufficient physical activity is reported to have reached 27.5% in 2016, with the prevalence of insufficient physical activity being particularly increased in the GCC, such as Kuwait (67%), Saudi Arabia (53%), and the UAE (41%) (35). Since most of these countries are based on the service sector, with a low number of physically demanding jobs, this is an additional factor contributing to decreased rates of physical activity observed in the GCC (36). Our results showed that most of the participants (78.8%) are physically inactive. We also demonstrated a trend of lower physical activity in patients with T2D as compared to nondiabetic subjects in this sample of the UAE population. Furthermore, our findings showed that the female participants had lower physical activity than their male counterparts. This is in line with the previous study that demonstrated lower physical activity in women than in men (35). These observations could be related to the cultural and social aspects in the UAE, where boys are found to be more educated about exercise, more encouraged to exercise, seem to have better access to exercise than girls, and appear to comply more with exercise guidelines than girls (28).
There are several limitations of this study. Since it included the adult population from Dubai, our results cannot be applied to the general UAE population. The study sample was restricted to UAE nationals, which means the results may not be applicable to non-UAE residents or other populations with different cultural or lifestyle characteristics. Furthermore, due to the cross-sectional design of this study, we could not establish causality between diabetes diagnosis and dietary habits. However, although we couldn’t establish causality, to the best of our knowledge, this is the first study exploring dietary knowledge, awareness and confidence in diet change in the UAE outpatient population. The study’s relevance to the UAE population is an important strength, as the country is experiencing a growing prevalence of type 2 diabetes, making these findings highly applicable for healthcare professionals and policymakers seeking to address this pressing health concern. Furthermore, this study employed rigorous statistical methods, including linear and logistic regression models, to analyze the data while controlling for important confounding variables such as age, gender, and BMI, ensuring that the findings are not biased by these factors. Another notable strength of the study is its focus on gender-specific analysis, which revealed important differences in physical activity levels between male and female participants and suggested that clinical interventions could be more effective if tailored according to gender. It would be pertinent to increase public health efforts to raise awareness about the role of physical activity in diabetes management, particularly for women, to reduce the overall disease burden and improve quality of life for individuals at risk of or living with T2D. This is in line with the National Nutrition Strategy 2022–2030 launched by the UAE’s Ministry of Health and Prevention (37) and the UAE’s 2021 vision, which pointed at the prevalence of diabetes and the prevalence of obesity in children among the primary national healthcare performance indicators in public healthcare interventions (38). Accordingly, it would be essential to increase awareness about healthy food choices and physical activity, along with developing effective policies and interventions for the nation’s healthy way of life.
Our findings underscore the importance of personalized care strategies that address not only dietary habits but also physical activity levels and gender-specific health behaviors. Healthcare providers in the UAE should further develop clinical and community care practices to enhance preventive measures and design more effective, culturally tailored programs to mitigate the growing burden of T2D. This is in line with the recently developed case management approach (39), where specialized nurses with specific skills in promoting lifestyle changes and managing chronic diseases contribute to the efforts of a multidisciplinary team of healthcare professionals to optimally manage T2D (40). In this particular context, the lifestyle medicine case manager nurse could play a crucial role in T2D management by assisting with their care and offering a tailored care plan, contributing to the overall enhancement of the patient’s clinical condition (41).
In conclusion, our findings demonstrated that majority of the participants in this sample of UAE nationals living in Dubai were obese or overweight. These results are in accordance with the previous studies indicating that the combination of persisting traditional cultural practices, modern cultural changes, and economic prosperity in the Gulf region, including the UAE, created an obesogenic environment that promotes unhealthy eating, sedentary lifestyles, and weight gain, that contributes to the rise in “lifestyle diseases,” such as obesity and T2D (42). Our results showed that the patients with T2D had a lower dietary score than nondiabetic subjects, indicating that they potentially improved their diet following diagnosis by being more likely to consume less fast food and sweets, and more fruits and vegetables. These adopted changes in their diet probably had a beneficial effect on the lipid profile, including total cholesterol and LDL-cholesterol levels, which were decreased in patients with T2D. Furthermore, we also observed a trend of lower physical activity in patients with T2D vs nondiabetic individuals, as well as decreased physical activity in female vs male participants. Understanding dietary habits, physical activity levels, and associated clinical parameters can guide healthcare providers in developing targeted, personalized interventions to improve management and prevention strategies for T2D. The findings suggest that although patients with T2D in the UAE may adopt healthier dietary habits, there remains a significant need to address physical activity disparities, particularly among women, to improve overall health outcomes in this population. Thus, further studies are needed to explore the long-term effects of dietary and physical activity interventions on the health outcomes of T2D patients in the UAE, with particular attention to gender differences and cultural factors influencing lifestyle behaviors.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the Khalifa University, Department of Health Abu Dhabi, and Dubai Scientific Research Ethics Committee, Dubai Health Authority. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KH: Data curation, Formal Analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. FS: Data curation, Formal Analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. AY: Investigation, Resources, Writing – original draft, Writing – review & editing. SA: Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. KH: Investigation, Resources, Writing – original draft, Writing – review & editing. FA: Investigation, Resources, Writing – original draft, Writing – review & editing. LS: Investigation, Resources, Writing – original draft, Writing – review & editing. EE: Investigation, Resources, Writing – original draft, Writing – review & editing. MK: Investigation, Resources, Writing – original draft, Writing – review & editing. HA: Investigation, Resources, Writing – original draft, Writing – review & editing. HA-M: Investigation, Resources, Writing – original draft, Writing – review & editing. ST: Investigation, Resources, Writing – original draft, Writing – review & editing. HB: Resources, Writing – original draft, Writing – review & editing, Investigation. SS: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Khalifa University research grant.
Acknowledgments
The authors thank all subjects who participated in the study, as well as medical doctors, nurses and other paramedical staff from the primary healthcare centers in Dubai, United Arab Emirates, who assisted in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1436536/full#supplementary-material
References
1. IDF. International diabetes federation. In: IDF diabetes atlas, 10th ed. Brussels, Belgium: International Diabetes Federation. (2021).
2. Ng SW, Zaghloul S, Ali HI, Harrison G, Popkin BM. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes Rev. (2011) 12:1–13. doi: 10.1111/j.1467-789X.2010.00750.x
3. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. (2010) 87:4–14. doi: 10.1016/j.diabres.2009.10.007
4. Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. (2011) 94:311–21. doi: 10.1016/j.diabres.2011.10.029
5. Collaboration N.C.D.R.F. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
6. Maggio CA, Pi-Sunyer FX. Obesity and type 2 diabetes. Endocrinol Metab Clin North Am. (2003) 32:805–22, viii. doi: 10.1016/S0889-8529(03)00071-9
7. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2014) 384:766–81. doi: 10.1016/S0140-6736(14)60460-8
8. DeNicola E, Aburizaiza OS, Siddique A, Khwaja H, Carpenter DO. Obesity and public health in the Kingdom of Saudi Arabia. Rev Environ Health. (2015) 30:191–205. doi: 10.1515/reveh-2015-0008
9. Meo SA, Usmani AM, Qalbani E. Prevalence of type 2 diabetes in the Arab world: impact of GDP and energy consumption. Eur Rev Med Pharmacol Sci. (2017) 21:1303–12.
10. Agarwal MM. Gestational diabetes in the arab gulf countries: sitting on a land-mine. Int J Environ Res Public Health. (2020) 17:9270–84. doi: 10.3390/ijerph17249270
11. Radwan H, Ballout RA, Hasan H, Lessan N, Karavetian M, Rizk R. The epidemiology and economic burden of obesity and related cardiometabolic disorders in the United Arab Emirates: A systematic review and qualitative synthesis. J Obes 2018. (2018) p:2185942. doi: 10.1155/2018/2185942
12. Sulaiman N, Elbadawi S, Hussein A, Abusnana S, Madani A, Mairghani M, et al. Prevalence of overweight and obesity in United Arab Emirates Expatriates: the UAE National Diabetes and Lifestyle Study. Diabetol Metab Syndr. (2017) 9:88. doi: 10.1186/s13098-017-0287-0
13. Abduelkarem AR, Sharif SI, Bankessli FG, Kamal SA, Kulhasan NM, Hamrouni AM. Obesity and its associated risk factors among school-aged children in Sharjah, UAE. PloS One. (2020) 15:e0234244. doi: 10.1371/journal.pone.0234244
14. Al Junaibi A, Abdulle A, Sabri S, Hag-Ali M, Nagelkerke N. The prevalence and potential determinants of obesity among school children and adolescents in Abu Dhabi, United Arab Emirates. Int J Obes (Lond). (2013) 37:68–74. doi: 10.1038/ijo.2012.131
15. Al-Haddad FH, Little BB, Abdul Ghafoor AG. Childhood obesity in United Arab Emirates schoolchildren: a national study. Ann Hum Biol. (2005) 32:72–9. doi: 10.1080/03014460400027425
16. Malik M, Bakir A. Prevalence of overweight and obesity among children in the United Arab Emirates. Obes Rev. (2007) 8:15–20. doi: 10.1111/j.1467-789X.2006.00290.x
17. Al Sabbah H, Assaf EA, Al-Jawaldeh A, AlSammach AS, Madi H, Khamis Al Ali N, et al. Nutrition situation analysis in the UAE: A review study. Nutrients. (2023) 15:363–83. doi: 10.3390/nu15020363
18. Awofeso N, Imam SA, Ahmed A. Content analysis of media coverage of childhood obesity topics in UAE newspapers and popular social media platforms, 2014-2017. Int J Health Policy Manag. (2019) 8:81–9. doi: 10.15171/ijhpm.2018.100
19. Khawaja AH, Qassim S, Hassan NA, Arafa EA. Added sugar: Nutritional knowledge and consumption pattern of a principal driver of obesity and diabetes among undergraduates in UAE. Diabetes Metab Syndr. (2019) 13:2579–84. doi: 10.1016/j.dsx.2019.06.031
20. Ng SW, Zaghloul S, Ali H, Harrison G, Yeatts K, El Sadig M, et al. Nutrition transition in the United Arab Emirates. Eur J Clin Nutr. (2011) 65:1328–37. doi: 10.1038/ejcn.2011.135
21. Pugh RN, Hossain MM, Malik M, El Mugamer IT, White MA. Arabian Peninsula men tend to insulin resistance and cardiovascular risk seen in South Asians. Trop Med Int Health. (1998) 3:89–94. doi: 10.1046/j.1365-3156.1998.00199.x
22. Malik M, Bakir A, Saab BA, King H. Glucose intolerance and associated factors in the multi-ethnic population of the United Arab Emirates: results of a national survey. Diabetes Res Clin Pract. (2005) 69:188–95. doi: 10.1016/j.diabres.2004.12.005
23. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PloS Med. (2007) 4:e296. doi: 10.1097/EDE.0b013e3181577654
24. England CY, Thompson JL, Jago R, Cooper AR, Andrews RC. Development of a brief, reliable and valid diet assessment tool for impaired glucose tolerance and diabetes: the UK Diabetes and Diet Questionnaire. Public Health Nutr. (2017) 20:191–9. doi: 10.1017/S1368980016002275
25. Quinn T, Bs MF, von Heideken J, Iannaccone C, Shadick NA, Weinblatt M, et al. Validity of the Nurses’ health study physical activity questionnaire in estimating physical activity in adults with rheumatoid arthritis. BMC Musculoskelet Disord. (2017) 18:234. doi: 10.1186/s12891-017-1589-y
26. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. WHO guidelines on physical activity and sedentary behaviour. Geneva: World Health Organization (2020).
27. Mamdouh H, Hussain HY, Ibrahim GM, Alawadi F, Hassanein M, Zarooni AA, et al. Prevalence and associated risk factors of overweight and obesity among adult population in Dubai: a population-based cross-sectional survey in Dubai, the United Arab Emirates. BMJ Open. (2023) 13:e062053. doi: 10.1136/bmjopen-2022-062053
28. Asma Deeb RAH, Attia S, ElFatih A, Afandi O, Nagelkerke N. Energy intake, dietary habits and life style in obese school children with dyslipidemia in the UAE. Int Arch Endocrinol Clin Res. (2015) 1:1–4. doi: 10.23937/2572-407X.1510001
29. AlBlooshi A, Shaban S, AlTunaiji M, Fares N, AlShehhi L, AlShehhi H, et al. Increasing obesity rates in school children in United Arab Emirates. Obes Sci Pract. (2016) 2:196–202. doi: 10.1002/osp4.v2.2
30. Baniissa W, Radwan H, Rossiter R, Fakhry R, Al-Yateem N, Al-Shujairi A, et al. Prevalence and determinants of overweight/obesity among school-aged adolescents in the United Arab Emirates: a cross-sectional study of private and public schools. BMJ Open. (2020) 10:e038667. doi: 10.1136/bmjopen-2020-038667
31. Sheikh-Ismail LI, Henry CJ, Lightowler HJ, Aldhaheri AS, Masuadi E, Al Hourani HM. Prevalence of overweight and obesity among adult females in the United Arab Emirates. Int J Food Sci Nutr. (2009) 60 Suppl 3:26–33. doi: 10.1080/09637480802331179
32. Afshin A, Micha R, Khatibzadeh S, Fahimi S, Shi P, Powles J, et al. The impact of dietary habits and metabolic risk factors on cardiovascular and diabetes mortality in countries of the Middle East and North Africa in 2010: a comparative risk assessment analysis. BMJ Open. (2015) 5:e006385. doi: 10.1136/bmjopen-2014-006385
33. Alfadda AA, Masood A. Now trending in Riyadh: Increased urbanization equals to more obesity in children and adolescents. Saudi J Gastroenterol. (2019) 25:207–9. doi: 10.4103/sjg.SJG_347_19
34. Abusnana S, Fargaly M, Alfardan SH, Al Hammadi FH, Bashier A, Kaddaha G, et al. Clinical practice recommendations for the management of obesity in the United Arab Emirates. Obes Facts. (2018) 11:413–28. doi: 10.1159/000491796
35. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health. (2018) 6:e1077–86. doi: 10.1016/S2214-109X(18)30357-7
36. Sherif S, Sumpio BE. Economic development and diabetes prevalence in MENA countries: Egypt and Saudi Arabia comparison. World J Diabetes. (2015) 6:304–11. doi: 10.4239/wjd.v6.i2.304
37. Prevention, U.A.E.M.o.H.a. National nutrition strategy 2022-2030. (2022). Available online at: https://u.ae/en/about-the-uae/strategies-initiatives-and-awards/strategies-plans-and-visions/health/national-nutrition-strategy-2030 (Accessed April 02, 2024).
38. Prevention, U.A.E.M.o.H.a. “Scope of Vision 2021”, in the UAE Government's official portal (u.ae) United Arab Emirates (UAE) Government. (2022).
39. Joo JY, Huber DL. An integrative review of case management for diabetes. Prof Case Manag. (2012) 17:72–85. doi: 10.1097/NCM.0b013e318243d473
40. O’Flynn S. Nurses’ role in diabetes management and prevention in community care. Br J Community Nurs. (2022) 27:374–6. doi: 10.12968/bjcn.2022.27.8.374
41. Cangelosi G, Grappasonni I, Pantanetti P, Scuri S, Garda G, Cuc Thi Thu N, et al. Nurse Case Manager Lifestyle Medicine (NCMLM) in the Type Two Diabetes patient concerning post COVID-19 Pandemic management: Integrated-Scoping literature review. Ann Ig. (2022) 34:585–602. doi: 10.7416/ai.2022.2500
Keywords: obesity, diabetes, diet, physical activity, gender
Citation: Hatab K, Serdarevic F, Yousuf A, Al Ali S, Al Hajaj KEAM, Almarzooqi FMAM, Swaidan LT, ElHassan EF, Kazim MNA, Abdalla HHA, Al-Muhaureq HA, Thabit SM, BaKhamis HA and Semiz S (2025) Lifestyle habits and type 2 diabetes traits in patients from healthcare centers in Dubai, United Arab Emirates: a cross-sectional study. Front. Endocrinol. 16:1436536. doi: 10.3389/fendo.2025.1436536
Received: 24 May 2024; Accepted: 14 April 2025;
Published: 06 May 2025.
Edited by:
Senthil Kumar Nachimuthu, Mizoram University, IndiaReviewed by:
Mustafa Kursat Sahin, Ondokuz Mayıs University, TürkiyeGiovanni Cangelosi, AST Fermo Marche Region Health System, Italy
Copyright © 2025 Hatab, Serdarevic, Yousuf, Al Ali, Al Hajaj, Almarzooqi, Swaidan, ElHassan, Kazim, Abdalla, Al-Muhaureq, Thabit, BaKhamis and Semiz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabina Semiz, c2FiaW5hLnNlbWl6QGt1LmFjLmFl; c2FiaW5hc2VtaXpAaG90bWFpbC5jb20=