 Margot Giocondo1
Margot Giocondo1 Belén Ponte2
Belén Ponte2 Sophie de Seigneux2
Sophie de Seigneux2 Samira M. Sadowski3
Samira M. Sadowski3 Benoît Bédat1
Benoît Bédat1 Frédéric Triponez1
Frédéric Triponez1 Marco Stefano Demarchi1*
Marco Stefano Demarchi1*- 1Department of Thoracic and Endocrine Surgery and Faculty of Medicine, University Hospitals of Geneva, Geneva, Switzerland
- 2Nephrology and Hypertension Division, Department of Medicine, University Hospitals of Geneva, Geneva, Switzerland
- 3Neuroendocrine Cancer Therapy Section, Surgical Oncology Program, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, United States
Background: Primary hyperparathyroidism (PHPT) is a condition recognized to include distinct biochemical phenotypes: hypercalcemic, normocalcemic, and normohormonal PHPT. This condition is characterized by inappropriately elevated parathyroid hormone (PTH) levels relative to serum calcium levels, leading to high bone turnover and decreased bone mineral density (BMD). Although BMD has been shown to improve following curative parathyroidectomy (PTX), there is limited data on the relationship between BMD changes after PTX and according to the clinical phenotypes of PHPT. This prospective study aims to identify the best candidates for surgery among these three phenotypes of PHPT by examining symptoms and comorbidities, biochemical results, and both pre- and post-operative DXA scans.
Methods: This is a prospective single-center study including 104 consecutive patients who underwent PTX for PHPT. Sociodemographic profiles and biochemical results were collected at both pre- and at 6 months post-surgery. All patients underwent dual-energy x-ray absorptiometry (DXA) scans at 1 and 6 months before surgery, and again between 12 and 18 months after surgery, to assess and compare changes in bone mineral density (BMD). Patients were categorized into three subgroups (normohormonal, hyperparathyroid normocalcemic and hyperparathyroid hypercalcemic) to assess differences in BMD improvement across these groups.
Results: According to predefined thresholds, 40.0% of patients experienced a significant BMD gain at the spine, 35.1% at the femur, 23.5% at the left hip, and 8.6% at the radius. Additionally, a greater postoperative drop in PTH was associated with larger BMD gains at the spine (SD 0.07; mean 0.03) and left femur bone (SD 0.06; mean 0.02). There was no significant change in T-score at the one-third radius. Higher preoperative urinary calcium level was associated with greater BMD and T-score improvement at the left hip. All PHPT phenotypes demonstrated similar postoperative BMD gains. No differences in BMD improvement were observed between males and females, nor was there any correlation between BMD gains and age.
Conclusions: Our findings suggest that BMD improves in all PHPT patients undergoing curative PTX, irrespective of clinical phenotype, age or sex. While patients with more severe biochemical profiles exhibited greater increases in BMD and T-scores, milder forms showed favorable trends that require confirmation in larger studies.
Introduction
Primary hyperparathyroidism (PHPT) is a common endocrine disorder characterized by parathyroid hormone (PTH) levels inappropriately elevated relative to serum calcium levels, typically due to overactivity in one or more parathyroid glands. Since the 1970s, advances in biochemical screening have expanded the understanding of PHPT from its classical presentation—associated with significant hypercalcemia, bone pain, kidney stones, and neuropsychiatric symptoms—to a spectrum of clinical phenotypes (1, 2). These include “asymptomatic” PHPT (3), where patients present with slightly elevated or upper-normal serum calcium levels but with no obvious clinical signs of PHPT, and normocalcemic PHPT (4–6), where patients have persistently elevated PTH levels with normal adjusted and ionized calcium in the absence of secondary causes.
One consequence of elevated PTH secretion in PHPT is increased bone turnover (7), which leads to decreased bone mineral density (BMD), particularly at cortical sites (8). This reduction in BMD can result in osteopenia or osteoporosis in the long run, thereby increasing the risk of fractures. Numerous studies have shown that patients with PHPT experience an increase in BMD following successful parathyroidectomy (PTX) (9–13). Several factors are thought to influence the extent of BMD improvement. Randomized clinical trials have documented BMD improvements in patients with mild, asymptomatic PHPT (14), yet a meta-analysis indicated that surgery offers similar benefits compared to surveillance (15, 16), albeit with the need for longer follow-up periods. Moreover, recent research has highlighted that even normocalcemic PHPT patients experience significant BMD gains post-PTX (17, 18). Additionally, differences in patients’ sociodemographic profiles, such as age, and biochemical characteristics, like hypercalciuria or lower baseline PTH, are predictors of better BMD improvement (19).
Although distinct phenotypes of PHPT have emerged, PTX remains the only curative treatment, with growing evidence supporting its efficacy in improving BMD in PHPT patients. PTX is recommended for all symptomatic and asymptomatic cases with serum calcium ≥1 mg/dl above the upper limit of normal, those with osteoporosis (T-score ≤−2.5) or vertebral fractures, those with eGFR <60 ml/min, severe hypercalciuria (>400 mg/day), increased risk of stones, evidence of nephrolithiasis, or nephrocalcinosis, and those under 50 years of age (3, 17). However, with the evolving definition of the disease and limited data on the different phenotypes, the question of which patients should undergo surgery remains. This study focuses on the predictors of increased postoperative BMD across different PHPT phenotypes.
Materials, methods and definition
Study design and population
We performed a prospective observational study including patients diagnosed with primary hyperparathyroidism (PHPT), who underwent parathyroidectomy at Geneva University Hospitals in Geneva, Switzerland, between November 2016 and May 2020.
Inclusion and exclusion criteria
Inclusion criteria: Patients aged 18 years or older diagnosed with primary hyperparathyroidism who provided written informed consent for participation in the study.
Exclusion criteria: Patients were excluded if they met any of the following conditions: (1) diagnosis of secondary or tertiary hyperparathyroidism, (2) absence of preoperative bone mineral density (BMD) measurements, or (3) failure to meet the inclusion criteria.
This study was conducted in accordance with the guidelines outlined in the Declaration of Helsinki. All procedures involving research participants were approved by the Ethics Committee, and informed consent was obtained from all subjects involved in the study.
Collected variables
Demographic and clinical data were collected during the initial preoperative visit: age, sex, height, weight, BMI and clinical symptoms like osteopenia and osteoporosis.
For the laboratory measures, serum and urinary calcium, parathyroid hormone (PTH), and phosphate levels were evaluated at multiple time points throughout the study. Preoperative measurements were taken during the initial visit (V1). Postoperative assessments were conducted on day 1 (V2) and day 10 (V3) following parathyroidectomy (PTX), with a final follow-up at 6 months post-surgery (V4). The analytical methods employed were specific to each biomarker. PTH was quantified using the Cobas 8000 ECLIA (Electrochemiluminescence immunoassay) method, with normal values ranging from 1.1 to 6.8 pmol/L. Both serum calcium and phosphate were analyzed using UV-visible absorption spectrometry. The reference range for serum calcium was established between 2.20 and 2.52 mmol/L, while phosphate levels were considered normal between 0.80 and 1.45 mmol/L.
Bone mineral density (BMD) was assessed using dual-energy x-ray absorptiometry (DXA) in g/cm2 at the same facility and with the same machine for all patients. Scans were performed by trained technicians. Measurements were conducted between 1 and 6 months prior to surgery and again between 12 and 18 months post-surgery. Bone density and T-scores were measured at spine, left femur, left hip and radius.
Regarding the preoperative imaging protocol, a comprehensive evaluation was performed using two complementary techniques: high-resolution neck ultrasound and technetium-99m sestamibi scintigraphy. This dual-modality approach was employed to accurately localize parathyroid adenomas and guide surgical planning.
Finally, we collected intraoperative data: identified parathyroid glands number, removed glands number and weight.
Definitions
The three biochemical profiles were defined based on lab values at the first visit (V1) as follows: the normohormonal (NH) group had normal PTH with elevated serum calcium, the hyperparathyroid normocalcemic (HC) group had elevated PTH with normal serum calcium, and the hyperparathyroid hypercalcemic (HH) group exhibited concomitantly elevated serum calcium and PTH. This classification was adopted based on previous studies (25) highlighting distinct biochemical patterns and potentially different pathophysiological mechanisms among these subtypes.
The changes in BMD and T-scores were determined by subtracting preoperative values from postoperative values. Declining in bone density is considered <0%, moderate improvement is considered between 0.1 and 5%, and significant improvement with more than 5% (20).
Statistical analysis
The distribution of demographic, preoperative characteristics, and symptom variables was analyzed to identify patterns and potential outliers. Histograms, box plots, and normality tests (e.g., Shapiro-Wilk test) were used to assess the shape of distributions. IBM SPSS software was used to perform all statistical analyses.
Comparative analyses were conducted to explore differences in preoperative characteristics and cross demographic subgroups, utilizing t-tests or ANOVA for continuous variables and chi-square tests for categorical variables. Pearson and Spearman correlation coefficients were calculated to assess the relationships between demographic variables, preoperative characteristics, symptoms, and the changes in BMD and T-scores from pre- to postoperative measurements.
Results
We initially included 123 patients, but only 111 completed the study and follow-up, from which 104 had BMD measures at the 2 time points. Therefore, for this study we analyzed 104 PHPT patients from whom 84 were females (80.7%) and 20 males (19.2%). Their baseline characteristics are reported in Table 1 and Table 2. They were divided into three categories according to serum calcium and PTH levels (see Table 3). A total of 5 (4.8%) were classified as normohormonal hypercalcemic (NH), 32 (30.8%) as hyperparathyroid normocalcemic (HC), and 67 (64.4%) as hyperparathyroid hypercalcemic (HH). According to Charlston Comorbidity Index, 19.2% had no comorbidities and 85.6% had one and more. Out of 104 patients, 44% had osteopenia and 37.5% had osteoporosis. By subgroup, osteopenia was present in 40% of NH, 40.6% of HC, and 46.2% of HH patients, while osteoporosis was found in 40%, 46.9%, and 32.8% respectively (see Table 2).
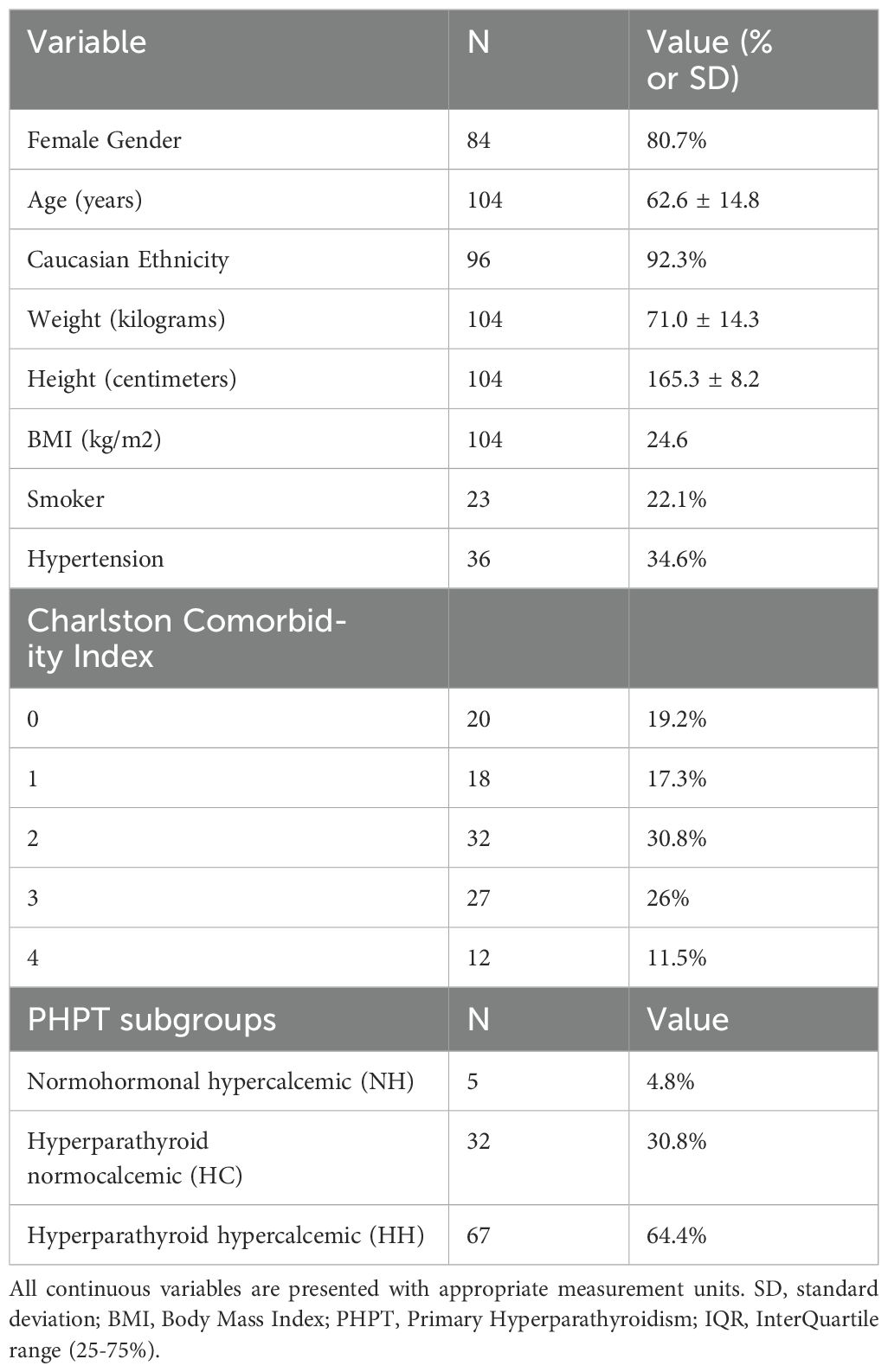
Table 1. clinical baseline characteristics of the patients included in the study.
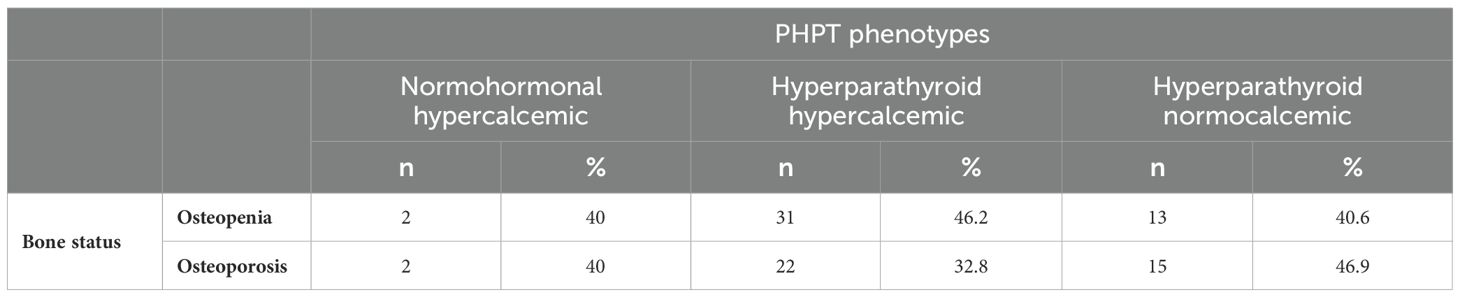
Table 2. Osteopenia and osteoporosis percentages in the three groups.

Table 3. Pre-operative calcium and PTH concentrations in the 3 subgroups (V1).
The median time interval between preoperative and postoperative bone density measurements was 1.67 years [IQR 1.23 - 2.10], and the median time interval between the last bone density measurement and surgery was 1.06 years [IQR 0.95 - 1.4].
Imaging
Considering imaging and surgical findings of patients, assessment of glands by cervical US showed that one gland was more prevalent in HH patients (p = 0.026), with median gland weight also significantly higher in this group (median = 0.82 [IQR 0.33 – 1.43] (p < 0.001), that is 4-fold higher than the other groups as well. This is also linked with histology findings that showed adenoma in 75% of the cases, double adenoma in 7.8%, and hyperplasia in 22.1% of the patients (Supplementary Table 1).
Surgical management
We identified discordant preoperative imaging results in 36.5% of patients, between high-resolution neck ultrasound and technetium-99m sestamibi scintigraphy. Bilateral surgical exploration was performed in 35.6% of patients. The majority of patients (80.8%) had one gland removed, while 17.3% had two and 6.7% had three glands removed (Supplementary Table 1).
Biological modifications after PTX
Analysis of total calcium and corrected calcium at V1 showed a significant difference in pre-operative calcium between the groups, with highest values, by definition, in the HH patients and lowest values in NH patients (p < 0.001). As expected, there were significant differences in preoperative PTH between NH, HC or HH groups. Preoperative (V1) total calcium was significantly different (p < 0.001) between HC and HH groups, with a median total calcium of 2.55 and 2.75 mmol/l, respectively (see Table 3).
BMD evolution after PTX
Post-operative BMD was performed at a median of 1.05 years after surgery. Pre- and post-operative DXA scans with resulting bone mineral density parameters and calculated T-scores of the patients summarized in Table 4. When comparing preoperative and post-operative BMD, PTX was associated with a significant increase in BMD at the spine (standard deviation (SD) 0.07; mean 0.03), left femur bone (SD 0.06; mean 0.02), and at the left hip bone (SD 0.06; mean 0.01), whereas no significant difference was found at the one-third radius (Table 5).
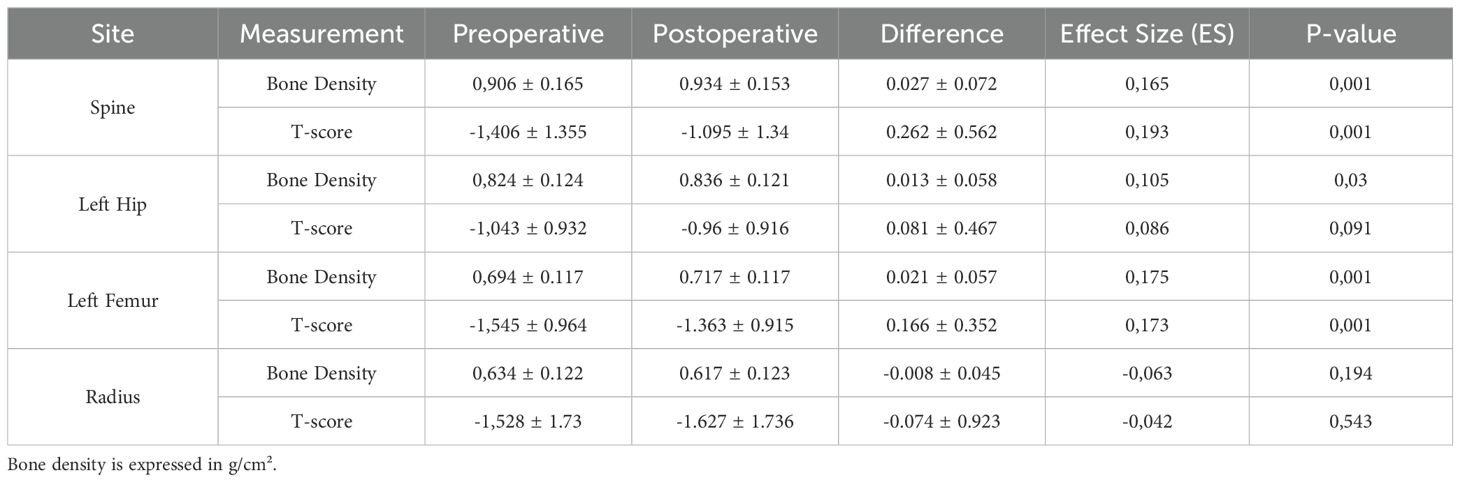
Table 4. Preoperative and postoperative bone density parameters of the patients included in the study.
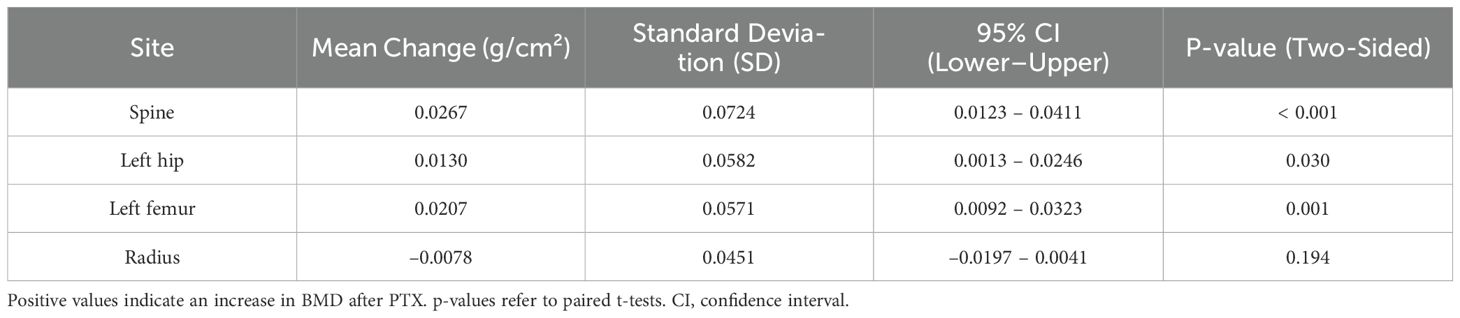
Table 5. Paired differences in BMD (g/cm²) between preoperative and postoperative measurements at four skeletal sites.
Figure 1 and its Supplementary Table 2 illustrate the 95% confidence intervals for changes in bone mineral density (BMD) and T-scores at the spine, left femur, left hip, and one-third radius. The spine showed the most significant and consistent gains in both BMD and T-score. Improvements at the left femur were also notable. At the left hip, changes were more modest, with confidence intervals crossing zero, indicating no statistical significance. No significant change was observed at the one-third radius, which also demonstrated the greatest variability—some patients experienced substantial gains, while others showed no improvement or even loss.
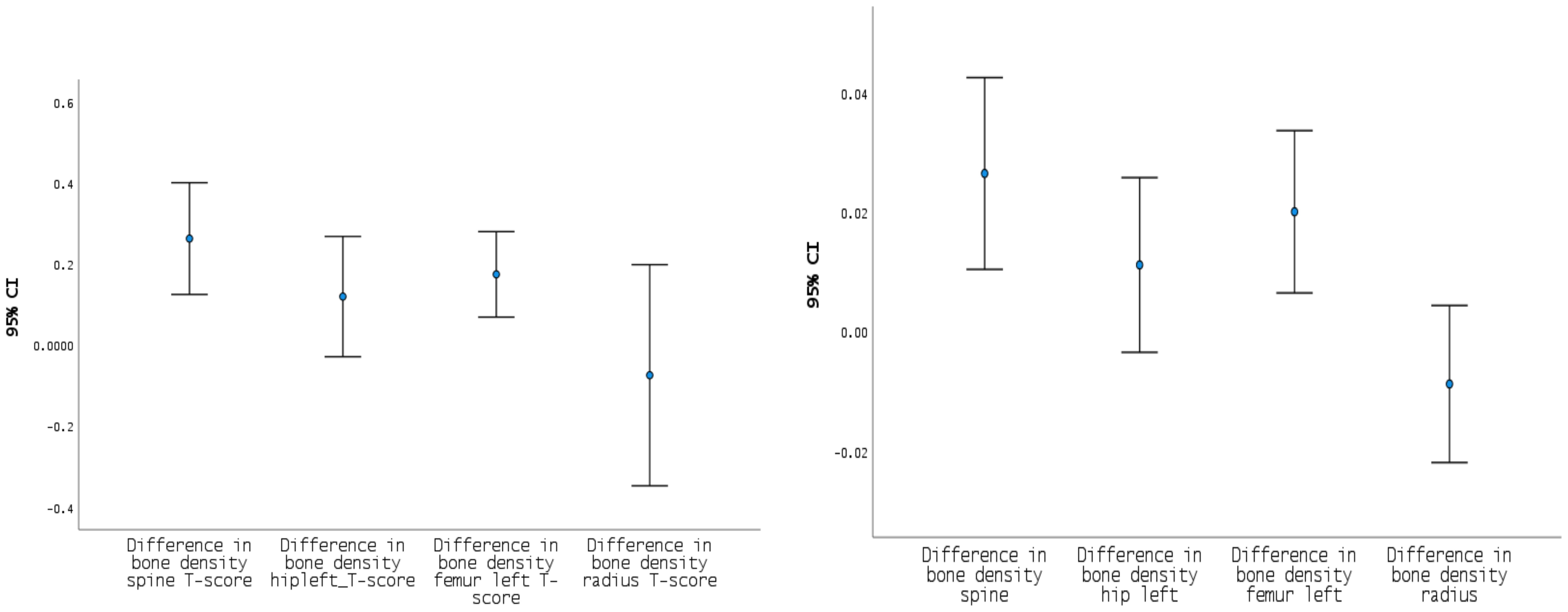
Figure 1. IC 95% difference in T-score and bone density for spine, left hip, left femur and radius. Mean changes in T-score (left) and BMD (right) at the spine, left hip, femur, and radius one year after parathyroidectomy. The most significant improvements were observed at the spine, while no significant change was detected at the radius. At the left hip, changes were more modest, with confidence intervals crossing zero, indicating weaker statistical significance.
In addition to statistical comparisons, individual-level changes in BMD were evaluated according to the predefined threshold of a >5% increase representing a significant improvement. As illustrated in Figure 2, which shows the distribution of percent BMD change at each anatomical site, a significant improvement (>5%) in BMD was observed in 40.0% of patients at the spine, 35.1% at the left femur, 23.5% at the left hip, and 8.6% at the radius. Moderate increases (0.1–5%) and decreases were also observed across all sites, highlighting the heterogeneity in individual responses to surgery.
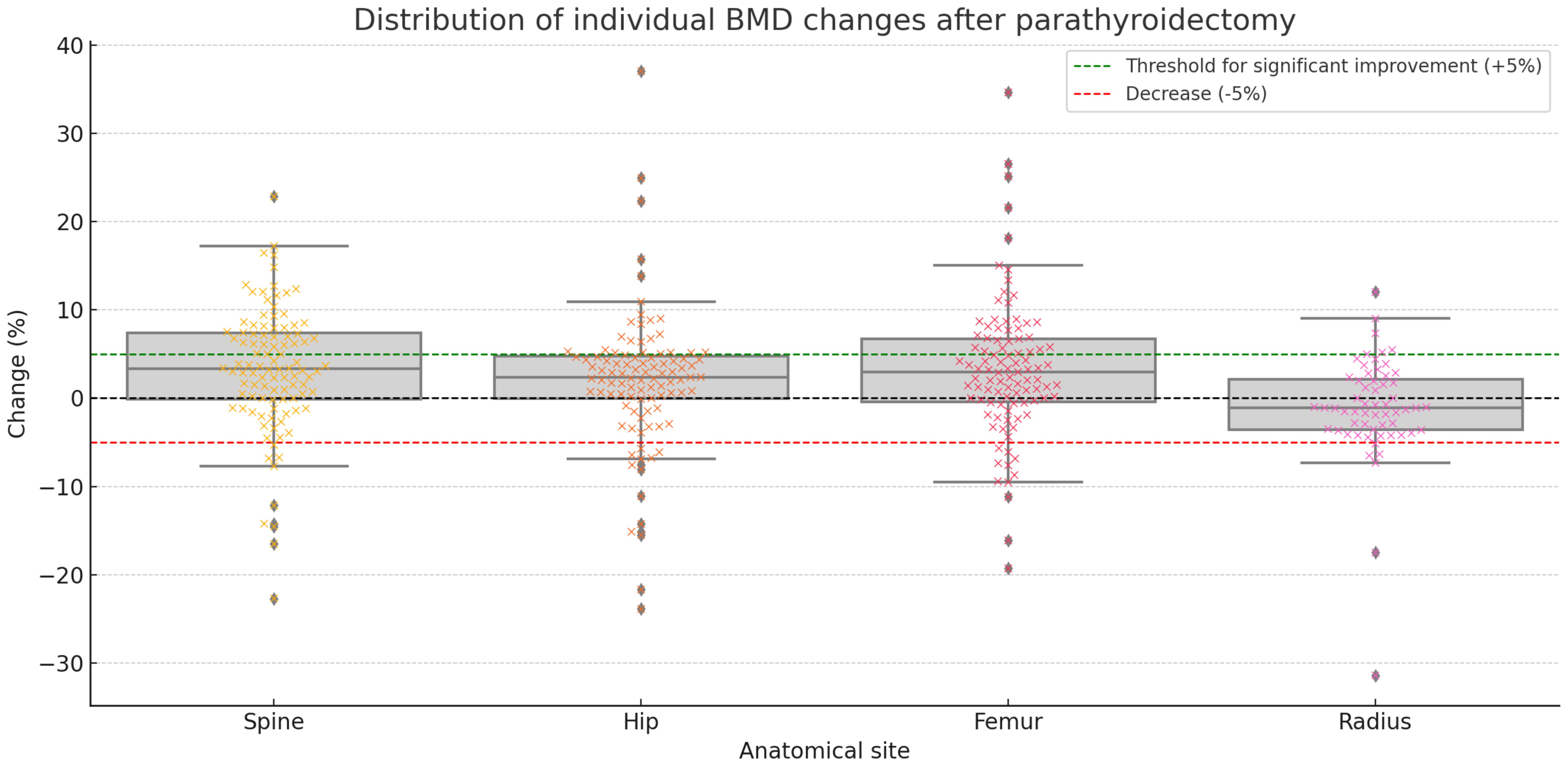
Figure 2. Distribution of individual changes in bone mineral density (BMD) for all patients at the spine, left hip, left femur, and radius after parathyroidectomy. Each dot represents an individual patient. Box plots show the distribution of percent changes. The green dashed line indicates the +5% threshold for significant improvement, while the red dashed line marks a 5% decrease. The black dashed line represents no change. For example, in the spine, 27.0% of patients showed a decrease, 33.0% had a moderate increase (0.1–5%), and 40.0% had a significant increase (>5%).
Table 6 presents the Spearman’s rho correlations between preoperative PTH levels (V1) and postoperative changes in BMD and T-scores at various anatomical sites. Our analysis showed modest but statistically significant associations between baseline PTH and BMD improvements, especially at the spine (ρ = 0.240, p = 0.017) and left femur (ρ = 0.335, p = 0.001), as well as their corresponding T-scores (spine: ρ = 0.241, p = 0.017; left femur: ρ = 0.220, p = 0.032). These associations suggest that patients with higher baseline PTH may exhibit greater postoperative gains in BMD at these sites. Higher preoperative urinary calcium levels were significantly associated with greater improvements in both BMD and T-score at the left hip, as shown in Table 7.
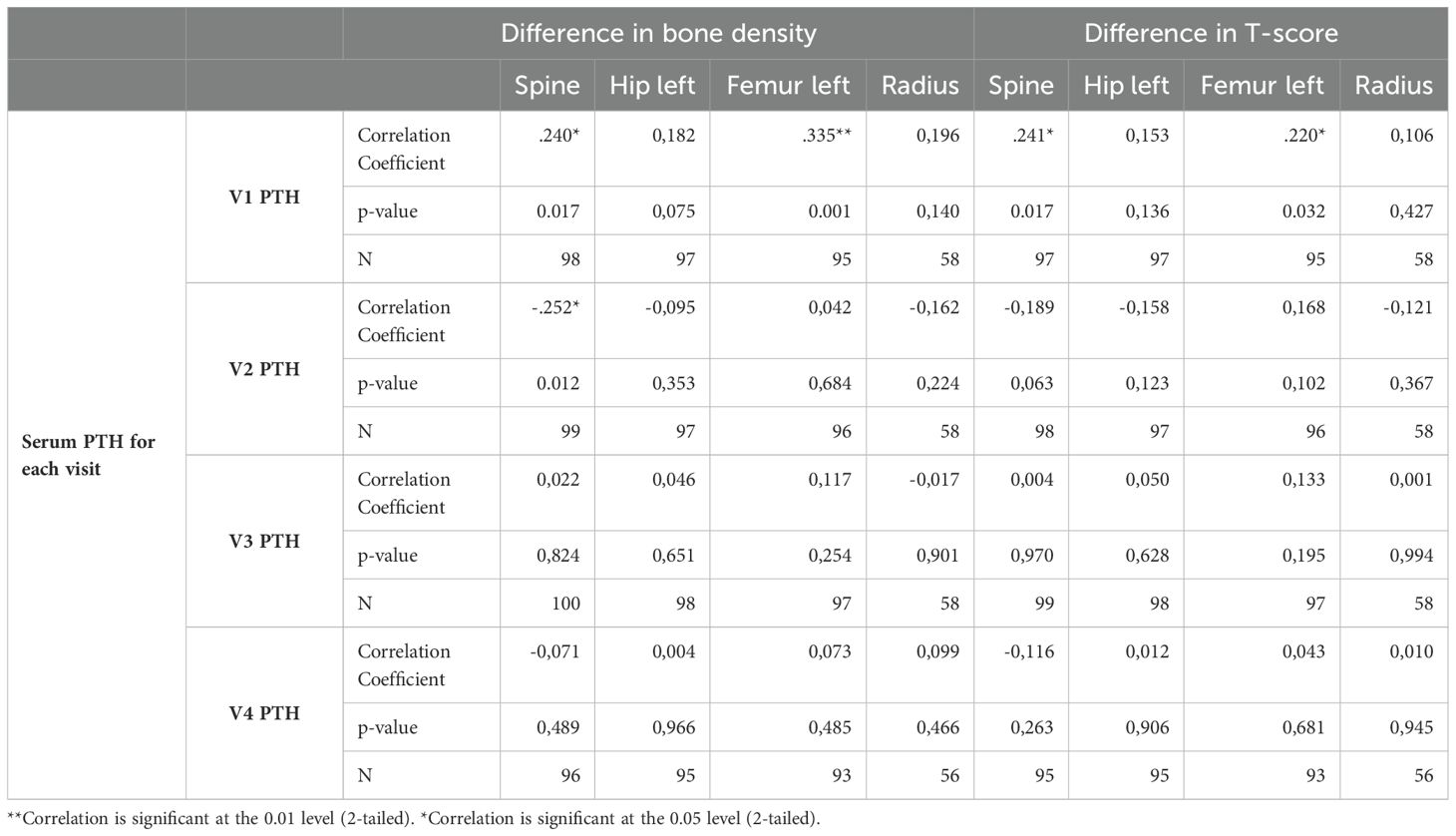
Table 6. Spearman’s rho correlation between PTH levels at V1 to V4 and BMD.

Table 7. Spearman’s rank correlation coefficients between urinary calcium levels at each visit and change in BMD at various skeletal sites.
When comparing variation in bone density by gender, no significant difference was found between males and females. We also found no significant differences in bone density levels between the three hormonal subgroups, which aligns with current literature. Figure 2 and Table 8 demonstrate that patients across all three phenotypes—hypercalcemic, normocalcemic, and normohormonal—experienced BMD improvements, with comparable proportions achieving moderate or significant gains.
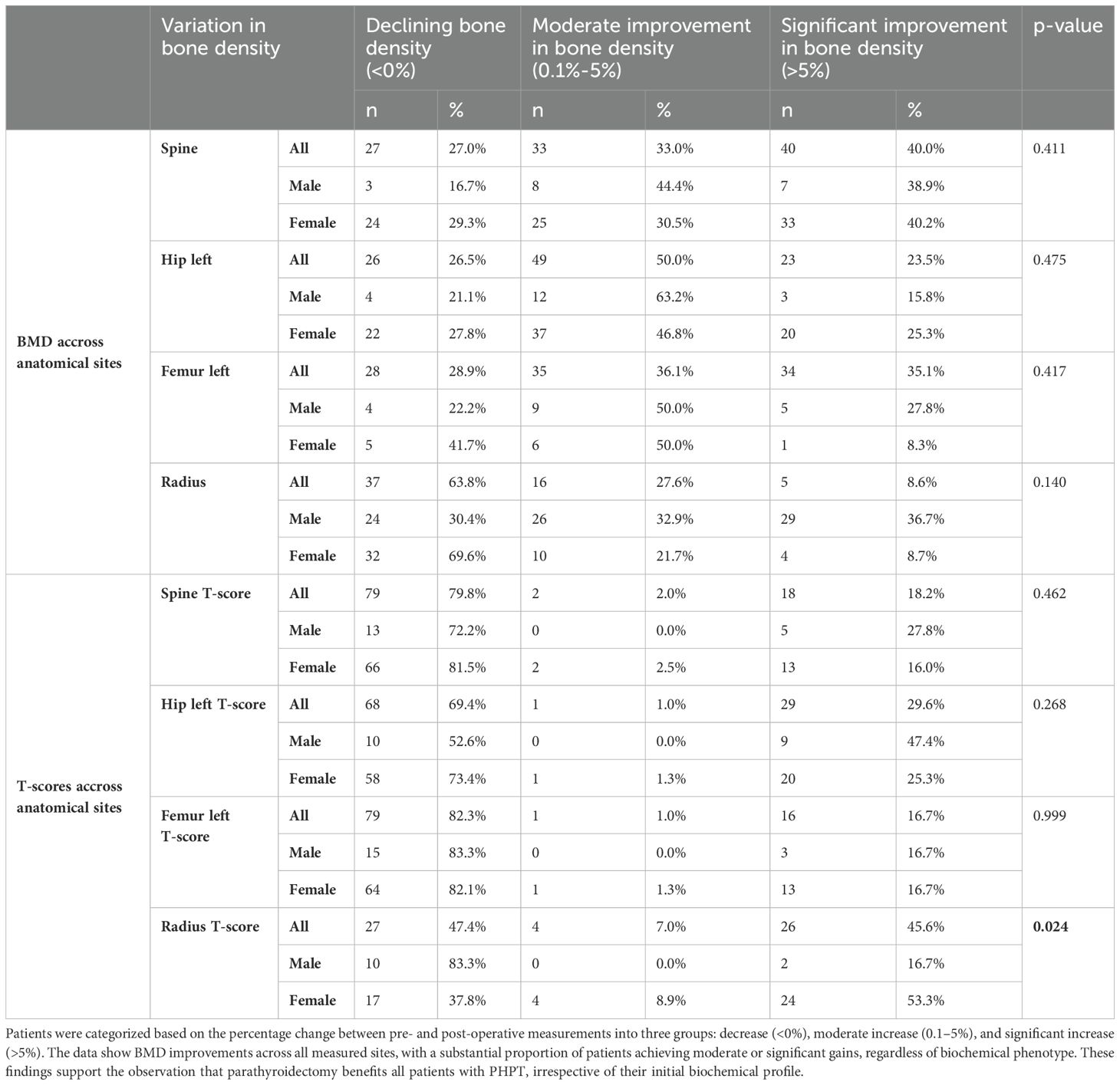
Table 8. Variation in bone density, overall, and by gender.
To further evaluate whether BMD changes differed across the three biochemical phenotypes of PHPT (hypercalcemic, normocalcemic, and normohormonal), we conducted ANOVA tests on preoperative, postoperative, and delta BMD values at all anatomical sites. As shown in Table 9, no statistically significant differences were found between the groups, either at baseline, after surgery, or in terms of BMD change. These findings confirm that the magnitude of bone mineral density improvement following parathyroidectomy is comparable across all three clinical phenotypes.
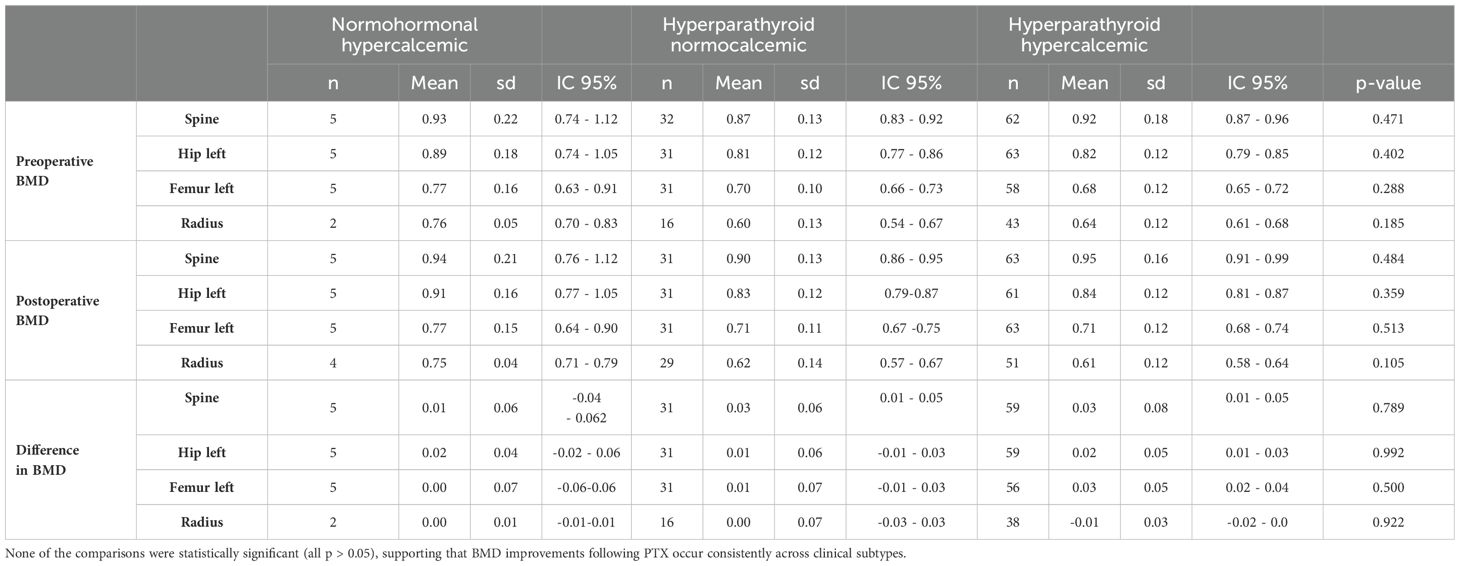
Table 9. Comparison of the 3 groups using ANOVA tests.
This consistent pattern supports our conclusion that parathyroidectomy is beneficial for PHPT patients regardless of their biochemical profile.
Discussion
This prospective study of 104 patients with primary hyperparathyroidism (PHPT) who underwent curative parathyroidectomy (PTX) at Geneva University Hospitals confirms and extends prior evidence that BMD improves after surgery. Notably, we demonstrate that this benefit applies consistently across the three major biochemical phenotypes of PHPT—hypercalcemic, normocalcemic, and normohormonal. A visual summary of our conclusions can be found on Figure 3.
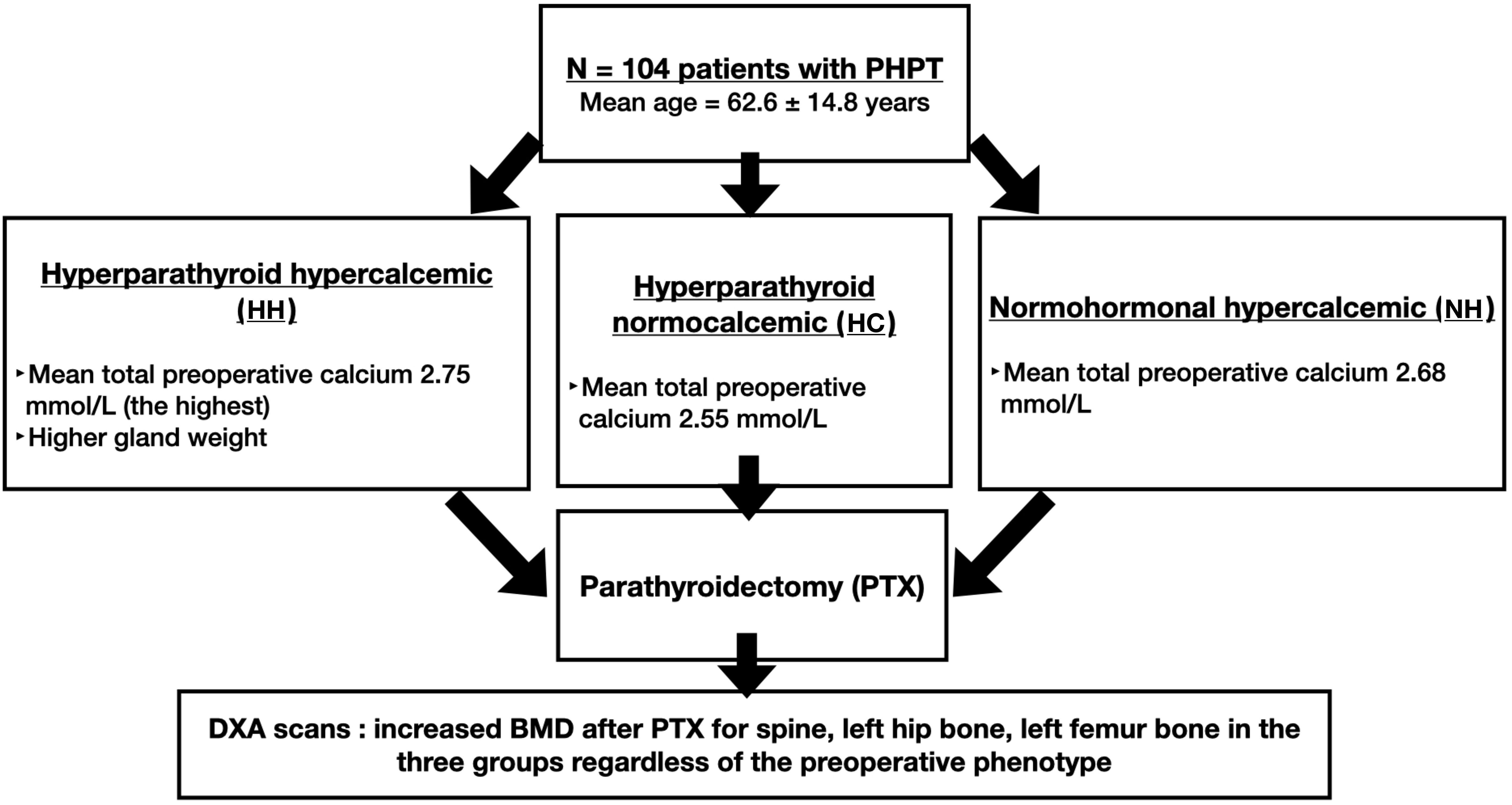
Figure 3. Findings’ summary of the comparison of the 3 groups. Patients from all three phenotypes—hypercalcemic, normocalcemic, and normohormonal—experienced postoperative BMD gains. These improvements were consistent across skeletal sites, with no significant differences between groups, supporting the role of PTX in all PHPT variants.
When comparing pre-operative and post-operative parathyroid hormone (PTH) levels, the greatest drop in PTH was linked to a greater rise in BMD and T-score both in the spine and left femur, as well as corresponding gains in T-scores (Table 6). As expected, no meaningful correlations were observed at later time points (V3 and V4), when both PTH and BMD had largely normalized. While this study focused on baseline PTH, future research could investigate the predictive value of the change in PTH (ΔPTH) as a dynamic marker of skeletal recovery following parathyroidectomy.
We acknowledge, however, that the strength of these associations varied across anatomical sites. While the correlations at the spine and left femur were statistically significant, the association at the left hip was not statistically significant, but demonstrated a trend suggestive of clinical relevance, and no correlation was observed at the one-third radius. The observed BMD improvement at these sites is consistent with observational and randomized studies (22, 23) and also reported in a recent study by Osorio-Silla et al. (11). In fact, differences between pre- and post-operative BMD showed the greatest variability at the radius; some patients showed an improvement in BMD whereas other patients showed a decline in BMD at this site. These findings are in line with the literature, with different studies reporting contrasting results; some studies report an increase (24), others no change (22) and others still report a decrease in BMD at the one-third radius (5, 13). This may highlight one of the limitations of our study: the follow-up period. With a median time interval between surgery and the last bone density measurement of 1.06 years [IQR 0.95 -1.4] this follow-up time is relatively short and may explain why we do not capture an improvement in BMD at this site. Longer-term data are likely needed to observe improvement or stabilization at the one-third radius after parathyroidectomy. However, extended follow-up remains logistically challenging in patients who are successfully cured of a benign disease.
An additional limitation with our study when assessing findings is the limited size of the normohormonal hypercalcemic group (n = 5), where we cannot exclude a type II error for differences observed in this group compared to the other two groups. We acknowledge that a subset of patients with hypercalcemic PHPT may present with inappropriately normal PTH levels, especially in mild cases. However, we chose to classify patients into three distinct phenotype since previous studies (25) have highlighted differences in biochemical profiles and potential underlying mechanisms among these groups. Even though the normohormonal group is small, we believe that presenting these patients separately provides transparency in our analysis and allows future studies to build on our findings.
While patients with more severe biochemical profiles exhibited the largest increases in BMD and T-scores, even asymptomatic individuals—particularly those in the normohormonal group—showed favorable trends following PTX. However, as previously noted, the small sample size in this subgroup (n = 5) limited statistical power, and most of the 95% confidence intervals for both the normohormonal and normocalcemic groups crossed zero (Table 9), precluding firm conclusions. This suggests that although the direction of change is encouraging, the magnitude of effect may not be clinically or statistically meaningful in all cases.
Higher preoperative urinary calcium was associated with a greater BMD and T-score gain in left hip (Table 7). This finding is in line with Lee et al. (13) who reported that the degree of elevation of preoperative calcium is associated with post-PTX change in BMD. Similarly, Benzon et al. (20) also found that patients with greater serum PTH and urinary calcium preoperatively benefited greater gains on BMD and T-score. As expected, high serum PTH and high calciuria are indicative of the more symptomatic form of PHPT.
In line with previous studies by Lee et al. (13)and Koumakis et al. (5, 21), our study also suggests that multiple nodules are more common in HC patients compared to the other two groups. Koumakis et al. (5) compared HC and HH patients and found that the former are more likely to have multinodular adenomas. In addition to gland number, analysis of gland weight in our study highlighted that whilst HH patients had fewer diseased glands (only one in nearly 90% of cases), gland weight was increased nearly fourfold compared to the other two groups. This finding suggests a positive correlation between PTH levels and gland size, with larger (heavier) glands secreting more PTH, as typically observed in more severe forms of the disease.
Taken together, our findings confirm that BMD improves significantly in PHPT patients undergoing PTX across biochemical phenotypes, age groups, and sexes. The absence of significant differences in BMD gains between subgroups (Table 8) supports the potential for broad surgical benefit. While our results must be interpreted in light of subgroup limitations, they support a more inclusive consideration of surgery for PHPT patients, including those with mild or atypical biochemical presentations. This prospective study provides compelling evidence that PTX offers skeletal benefits across the clinical spectrum of PHPT, reinforcing the need to revisit current surgical indications.
Conclusion
This prospective study provides evidence that parathyroidectomy enhances bone mineral density in patients with primary hyperparathyroidism (PHPT), including those with normocalcemic and normohormonal biochemical profiles. Nearly 40% of patients achieved a BMD gain exceeding 5%, a threshold considered clinically meaningful in DXA monitoring. While the most substantial gains were observed in patients with more severe biochemical profiles, even those with milder or asymptomatic forms of PHPT demonstrated favorable trends.
However, the magnitude of BMD improvement in normohormonal and normocalcemic patients was modest, and the associated confidence intervals often included zero. This highlights the need for cautious interpretation of subgroup results and underscores the importance of confirming these findings in larger cohorts.
Overall, our findings support extending surgical consideration to a broader population of PHPT patients. Future studies should aim to clarify the long-term skeletal outcomes in normocalcemic and normohormonal subtypes, and to further refine surgical indications across the full spectrum of PHPT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Service de la pharmacienne cantonaleCommission cantonale d’éthique de la recherche (CCER)Rue Adrien-Lachenal 8 1207 Genève. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MG: Writing – original draft, Writing – review & editing, Validation. BP: Writing – review & editing, Validation. SD: Writing – review & editing, Validation. SS: Writing – review & editing, Validation. BB: Writing – original draft, Writing – review & editing, Validation. FT: Conceptualization, Validation, Writing – review & editing. MD: Validation, Conceptualization, Methodology, Data curation, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript. The authors declare that AI tools (such as ChatGPT, developed by OpenAI) were used in this study solely for language editing purposes, including grammar correction, syntax refinement, and clarity enhancement of the manuscript text. No AI tools were used for data analysis, interpretation, or the generation of scientific content. All authors reviewed and approved the final version of the manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1562340/full#supplementary-material
Supplementary Table 1 | Imaging and surgical characteristics of the patients included in the study.
Supplementary Table 2 | IC 95% difference in T-score and bone density for spine, left hip, left femur and radius. Cohen's d uses the sample standard deviation of the mean difference adjusted by the correlation between measures. Hedges' correction uses the sample standard deviation of the mean difference adjusted by the correlation between measures, plus a correction factor.
References
1. Bilezikian JP, Bandeira L, Khan A, and Cusano NE. Hyperparathyroidism. Lancet. (2018) 391:168–78. doi: 10.1016/S0140-6736(17)31430-7
2. Bilezikian JP, Brandi ML, Cusano NE, Mannstadt M, Rejnmark L, Rizzoli R, et al. Management of hypoparathyroidism: Present and future. J Clin Endocrinol Metab. (2016) 101:2313–24. doi: 10.1210/jc.2015-3910
3. Wilhelm SM, Wang TS, Ruan DT, Lee JA, Asa SL, Duh Q-Y, et al. The american association of endocrine surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. (2016) 151:959. doi: 10.1001/jamasurg.2016.2310
4. Lui MS, Clemente-Gutierrez U, Vodopivec DM, Chang SL, Shirali AS, Huang BL, et al. Parathyroidectomy for normocalcemic primary hyperparathyroidism is associated with improved bone mineral density regardless of postoperative parathyroid hormone levels. World J Surg. (2022) 47:363–70. doi: 10.1007/s00268-022-06756-x
5. Koumakis E, Souberbielle J-C, Sarfati E, Meunier M, Maury E, Gallimard E, et al. Bone mineral density evolution after successful parathyroidectomy in patients with normocalcemic primary hyperparathyroidism. J Clin Endocrinol Metab. (2013) 98:3213–20. doi: 10.1210/jc.2013-1518
6. Šiprová H, Fryšák Z, and Souček M. Primary hyperparathyroidism, with A focus on management of the normocalcemic form: to treat or not to treat? Endocr Pract. (2016) 22:294–301. doi: 10.4158/EP15971.RA
7. Nakaoka D, Sugimoto T, Kobayashi T, Yamaguchi T, Kobayashi A, and Chihara K. Evaluation of changes in bone density and biochemical parameters after parathyroidectomy in primary hyperparathyroidism. Endocr J. (2000) 47:231–7. doi: 10.1507/endocrj.47.231
8. Lewiecki EM and Miller PD. Skeletal effects of primary hyperparathyroidism: bone mineral density and fracture risk. J Clin Densitom. (2013) 16:28–32. doi: 10.1016/j.jocd.2012.11.013
9. Pal R, Arya AK, Aggarwal A, Singh P, Dahiya D, Sood A, et al. Weight gain after curative parathyroidectomy predicts increase in bone mineral density in patients with symptomatic primary hyperparathyroidism. Clin Endocrinol (Oxf). (2020) 93:28–35. doi: 10.1111/cen.14195
10. Miguel G, Carranza F, Rodríguez J, Ramos M, Pablos D, Herrero E, et al. Trabecular bone score, bone mineral density and bone markers in patients with primary hyperparathyroidism 2 years after parathyroidectomy. Horm Metab Res. (2019) 51:186–90. doi: 10.1055/a-0850-8679
11. Osorio-Silla I, Gómez-Ramírez J, Valdazo-Gómez A, Salido Fernández S, Sánchez García C, and Pardo García R. What happens to the bone structure after normocalcemic primary hyperparathyroidism surgery? Surgery. (2022) 171:932–9. doi: 10.1016/j.surg.2021.08.047
12. Lu S, Gong M, Zha Y, Cui A, Chen C, Sun W, et al. Identification of independent factors affecting bone mineral density after successful parathyroidectomy for symptomatic hyperparathyroidism. BMC Endocr Disord. (2020) 20:141. doi: 10.1186/s12902-020-00622-4
13. Lee D, Walker MD, Chen HY, Chabot JA, Lee JA, and Kuo JH. Bone mineral density changes after parathyroidectomy are dependent on biochemical profile. Surgery. (2019) 165:107–13. doi: 10.1016/j.surg.2018.04.065
14. Rao DS, Phillips ER, Divine GW, and Talpos GB. Randomized controlled clinical trial of surgery versus no surgery in patients with mild asymptomatic primary hyperparathyroidism. J Clin Endocrinol Metab. (2004) 89:5415–22. doi: 10.1210/jc.2004-0028
15. Singh Ospina N, Maraka S, Rodriguez-Gutierrez R, Espinosa de Ycaza AE, Jasim S, Gionfriddo M, et al. Comparative efficacy of parathyroidectomy and active surveillance in patients with mild primary hyperparathyroidism: a systematic review and meta-analysis. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. (2016) 27:3395–407. doi: 10.1007/s00198-016-3715-3
16. Ye Z, Silverberg SJ, Sreekanta A, Tong K, Wang Y, Chang Y, et al. The efficacy and safety of medical and surgical therapy in patients with primary hyperparathyroidism: A systematic review and meta-analysis of randomized controlled trials. J Bone Miner Res Off J Am Soc Bone Miner Res. (2022) 37:2351–72. doi: 10.1002/jbmr.4685
17. Bilezikian JP, Khan AA, Silverberg SJ, El-Hajj Fuleihan G, Marcocci C, Minisola S, et al. Evaluation and management of primary hyperparathyroidism: summary statement and guidelines from the fifth international workshop. J Bone Miner Res. (2022) 37:2113–34. doi: 10.1002/jbmr.4677
18. Steinl GK, Yeh R, Walker MD, McManus C, Lee JA, and Kuo JH. Preoperative imaging predicts change in bone mineral density after parathyroidectomy for primary hyperparathyroidism. Bone. (2021) 145:115871. doi: 10.1016/j.bone.2021.115871
19. Okada M, Tominaga Y, Tomosugi T, Hiramitsu T, Ichimori T, and Sato T. Predictors of bone mineral density improvement after parathyroidectomy for secondary hyperparathyroidism: A retrospective single-center analysis. World J Surg. (2021) 45:2777–84. doi: 10.1007/s00268-021-06186-1
20. Dy BM, Grant CS, Wermers RA, Kearns AE, Huebner M, Harmsen WS, et al. Changes in bone mineral density after surgical intervention for primary hyperparathyroidism. Surgery. (2012) 152:1051–8. doi: 10.1016/j.surg.2012.08.015
21. Koumakis E, Souberbielle J-C, Payet J, Sarfati E, Borderie D, Kahan A, et al. Individual site-specific bone mineral density gain in normocalcemic primary hyperparathyroidism. Osteoporos Int. (2014) 25:1963–8. doi: 10.1007/s00198-014-2689-2
22. Silverberg SJ and Bilezikian JP. A 10-year prospective study of primary hyperparathyroidism with or without parathyroid surgery. N Engl J Med. (1999) 341:1249–55. doi: 10.1056/NEJM199910213411701
23. Bollerslev J, Jansson S, Mollerup CL, Nordenström J, Lundgren E, Tørring O, et al. Medical observation, compared with parathyroidectomy, for asymptomatic primary hyperparathyroidism: A prospective, randomized trial. J Clin Endocrinol Metab. (2007) 92:1687–92. doi: 10.1210/jc.2006-1836
24. Christiansen P, Steiniche T, Brixen K, Hessov I, Melsen F, Heickendorff L, et al. Primary hyperparathyroidism: effect of parathyroidectomy on regional bone mineral density in Danish patients: a three-year follow-up study. Bone. (1999) 25:589–95. doi: 10.1016/S8756-3282(99)00207-0
Keywords: primary hyperparathyroidism, bone mineral density, parathyroidectomy, dual-energy x-ray absorptiometry, normocalcemic hyperparathyroidism
Citation: Giocondo M, Ponte B, de Seigneux S, Sadowski SM, Bédat B, Triponez F and Demarchi MS (2025) Factors influencing bone mineral density in hyperparathyroidism phenotypes: a prospective study. Front. Endocrinol. 16:1562340. doi: 10.3389/fendo.2025.1562340
Received: 17 January 2025; Accepted: 05 May 2025;
Published: 28 May 2025.
Edited by:
Rimesh Pal, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaReviewed by:
Kyriakos Vamvakidis, Henry Dunant Hospital, GreeceZhixing Song, Tsinghua University, China
Copyright © 2025 Giocondo, Ponte, de Seigneux, Sadowski, Bédat, Triponez and Demarchi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Stefano Demarchi, cmRlaEBodWcuY2g=