 Yu Hu1,2,3,4,5†
Yu Hu1,2,3,4,5† Chenlin Gao
Chenlin Gao Yong Xu
Yong Xu- 1Department of Endocrinology and Metabolism, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, China
- 2Southwest Medical University, Luzhou, Sichuan, China
- 3Cardiovascular and Metabolic Diseases Key Laboratory of Luzhou, Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, China
- 4Sichuan Clinical Research Center for Nephropathy, Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, China
- 5Metabolic Vascular Disease Key Laboratory of Sichuan Province, Luzhou, Sichuan, China
Background: While middle-aged and elderly individuals account for the majority of diabetes cases, recent years have witnessed a rising incidence of diabetes, particularly type 2 diabetes, among younger populations. This study aims to examine global trends in diabetes among children and adolescents (<20 years) across 204 countries and regions.
Methods: This study draws primarily from the 2021 GBD database, offering an in-depth analysis of trends in the incidence, mortality, and disability-adjusted life years (DALYs) of diabetes in children and adolescents from 1990 to 2021, with further subgroup analyses conducted by sex, age, and specific regions. Furthermore, we investigated the potential risk factors contributing to diabetes-related mortality in children and adolescents.
Results: Between 1990 and 2021, the global incidence of diabetes among children and adolescents exhibited a steady upward trend. By 2021, the incidence of diabetes had risen by approximately 94.0% compared to 1990, while both mortality and DALYs experienced a notable decline. Subgroup analyses region revealed that death rates were generally lower in regions with a high sociodemographic index (SDI) compared to those with a low SDI and low income. Additionally, high fasting blood glucose, along with extreme temperature conditions (both high and low), were identified as the three major risk factors contributing to diabetes-related mortality in children and adolescents.
Conclusions: While diabetes-related mortality in children and adolescents has declined over time, the sharp increase in incidence indicates that it is emerging as a major threat to global child and adolescent health.
Highlights
• Why did we undertake this study?
Although diabetes predominantly affects middle-aged and older adults, there has been a notable increase in the incidence of diabetes, especially type 2 diabetes, among younger populations in recent years.
• What is the specific question(s) we wanted to answer?
Global Epidemiological Trends of Diabetes Among Children and Adolescents from 1990 to 2021.
• What did we find?
The burden of diabetes among children and adolescents varies markedly by sex and geographic region. While the diabetes-related mortality rate among children and adolescents has declined over time, the incidence has risen sharply.
Elevated fasting blood glucose and high and low temperatures are the three principal risk factors for diabetes-related mortality.
• What are the implications of our findings?
Diabetes is emerging as a significant global health threat to children and adolescents. Consequently, healthcare institutions must devise more cost-effective and targeted strategies to alleviate the adverse effects of diabetes on children and adolescents.
1 Introduction
Diabetes is a severe chronic condition primarily characterized by elevated blood glucose levels, typically resulting from absolute or relative insulin deficiency. Estimates from the 2019 Global Burden of Disease (GBD) study indicate that diabetes has emerged as the eighth leading cause of death and disability, affecting approximately 460 million people worldwide in 2019 (1). Furthermore, the International Diabetes Federation (IDF) reported in the 2021 Diabetes Atlas that the global prevalence of diabetes reached 537 million individuals in 2021. Projections indicate that by 2030, the number of individuals with diabetes may increase to 643 million and escalate to an alarming 783 million by 2045, with global healthcare expenditures potentially surpassing $105.4 billion (2). This highlights the immense burden that diabetes imposes on healthcare systems (3–5). The Non-Communicable Diseases Risk Factor Collaboration (NCD-RisC) estimated in 2016 that the probability of achieving the global objective of halting the rise in diabetes prevalence by 2025 was less than 1% for females and even lower for males (6).
Although diabetes can be categorized into various subtypes based on its underlying pathological mechanisms, it is predominantly classified as type 1 and type 2 diabetes (7). Type 1 diabetes is commonly recognized as an autoimmune disorder mediated by T cells, usually emerging in childhood and reaching its peak incidence around 14 years of age (8, 9). Krolewski et al. (10) observed a secondary peak in incidence around age 50, though this accounts for only 7% of cases. Conversely, type 2 diabetes is influenced by a complex interplay of genetic, dietary, and lifestyle factors and typically manifests after the age of 40 (11). Recent studies have highlighted a rising incidence of diabetes among younger individuals, indicating that the condition is increasingly posing a significant threat to an expanding cohort of young people (12). Despite advancements in prevention strategies, including enhanced basic healthcare infrastructure and increased availability of insulin and antidiabetic medications, these measures have yet to effectively curb the rising incidence and the trend of earlier onset of diabetes (13). Consequently, this study utilizes the most recent data from GBD 2021 to examine the evolving epidemiological trends of diabetes among children and adolescents (<20 years) across 204 countries from 1990 to 2021. Additionally, it aims to analyze risk factors associated with diabetes-related mortality, thereby aiding relevant organizations in developing more effective prevention and treatment policies to counteract the trend of earlier onset diabetes.
2 Method
2.1 Data source
The GBD 2021 study examined over 370 diseases and injuries across 204 countries and regions, offering comprehensive data on incidence, mortality, and Disability-Adjusted Life Years (DALYs) (14, 15). All data are derived from reputable public databases and have undergone rigorous screening processes to ensure data integrity (16).
Deaths and mortality rates are primarily estimated using the cause-of-death ensemble model, whereas prevalence and incidence are assessed using the Bayesian meta-regression model. Disability weights are conceptualized as indicators of the severity of health loss or non-fatal disability, whereas DALYs represent the aggregate of years lost due to health impairment from onset to death (17).
The Socio-Demographic Index (SDI) is a composite metric that reflects a country’s developmental status, incorporating lag-distributed income per capita, the average educational attainment of individuals aged 15 and older, and the total fertility rate among those under 25. It has a significant association with health outcomes. SDI values span from 0 to 1, with 0 indicating the lowest level of development and 1 denoting the highest level (18). Based on SDI values, the 204 countries and regions are stratified into five categories: high SDI, high-middle SDI, middle SDI, low-middle SDI, and low SDI regions. Furthermore, patients are classified into five age subgroups: under 1 year, 2 – 4 years, 5 – 9 years, 10 – 14 years, and 15 – 19 years.
2.2 Estimation of risk factor
We identified 66 specific attributable risk factors for evaluation, including particulate pollution, high temperature, low temperature, lead exposure, smoking, secondhand smoke exposure, high consumption of red meat, high sodium intake, low fiber intake, low fruit consumption, low vegetable intake, and elevated fasting blood glucose, as defined by prior research (19). Ultimately, relevant data were available only for high temperature, low temperature, and elevated fasting blood glucose, leading the subsequent attribution analysis to concentrate on these three risk factors.
2.3 Definition of diabetes
In the 2021 Global Burden of Disease study, diabetes is classified based on the International Classification of Diseases, Tenth Revision (ICD - 10), specifically codes E10 and E11.
2.4 Statistical analyses
To examine the relationship between trends in incidence and mortality rates and levels of social development, we computed the Pearson correlation coefficient concerning SDI values. Statistical analyses, including t-tests and analysis of variance (ANOVA), were performed using GraphPad Prism (version 10.0.0 for Windows) to compare incidence rates, mortality rates, and DALYs across different genders, age groups, and regions. The Autoregressive Integrated Moving Average (ARIMA) model was constructed to predict the changing trends in the incidence and mortality rates of diabetes among children and adolescents worldwide over the next 15 years. Unlike conventional linear regression, the ARIMA model offers a more accurate computational method that captures the dynamics of time series while incorporating additional relevant information (20). All hypothesis tests were conducted with a two-sided approach, and a significance level was set at P < 0.05.
3 Result
3.1 Global trends and incidence of diabetes in children and adolescents
Globally, the incidence of diabetes among children and adolescents has demonstrated a significant annual increase over the past 32 years, rising from 25.77 per 100,000 in 1990 to 49.99 per 100,000 in 2021, reflecting an approximate 94.0% increase. The total number of diabetes cases escalated from 581,949 in 1990 to 1,317,669 in 2021. The prevalence of both type 1 and type 2 diabetes has increased, with type 2 diabetes rates surpassing those of type 1 diabetes (Supplementary Figure S1). Notably, although the absolute number of cases is higher in males, the incidence rate for females exceeded that of males before 2020 (Table 1, Figure 1A). At the SDI level, diabetes incidence trends upward across all five SDI regions. The Low SDI region exhibits the lowest burden, while the High-middle SDI region shows the highest burden, with an incidence rate of 61.3 (95% UI: 47.71 - 75.84) (Table 1, Figure 2A, Supplementary Figures S3, S4). Geographically, Oceania reports the highest incidence rates, increasing from 48.29 per 100,000 in 1990 to 101.00 per 100,000 in 2021. The North Africa and Middle East, as well as East Asia regions, experienced the most substantial increases in incidence rates (Table 2). At the national level, China and India report the highest numbers of diabetes cases, with figures rising from 177.6×103 and 93.2×103 in 1990 to 342.1×103 and 243.0×103 in 2021, respectively. Meanwhile, Pakistan’s number of cases increased from seventh place in 1990 (14.87×103) to third place in 2021 (53.7×103) (Figures 3A, 4A, Supplementary Tables S1, S2).
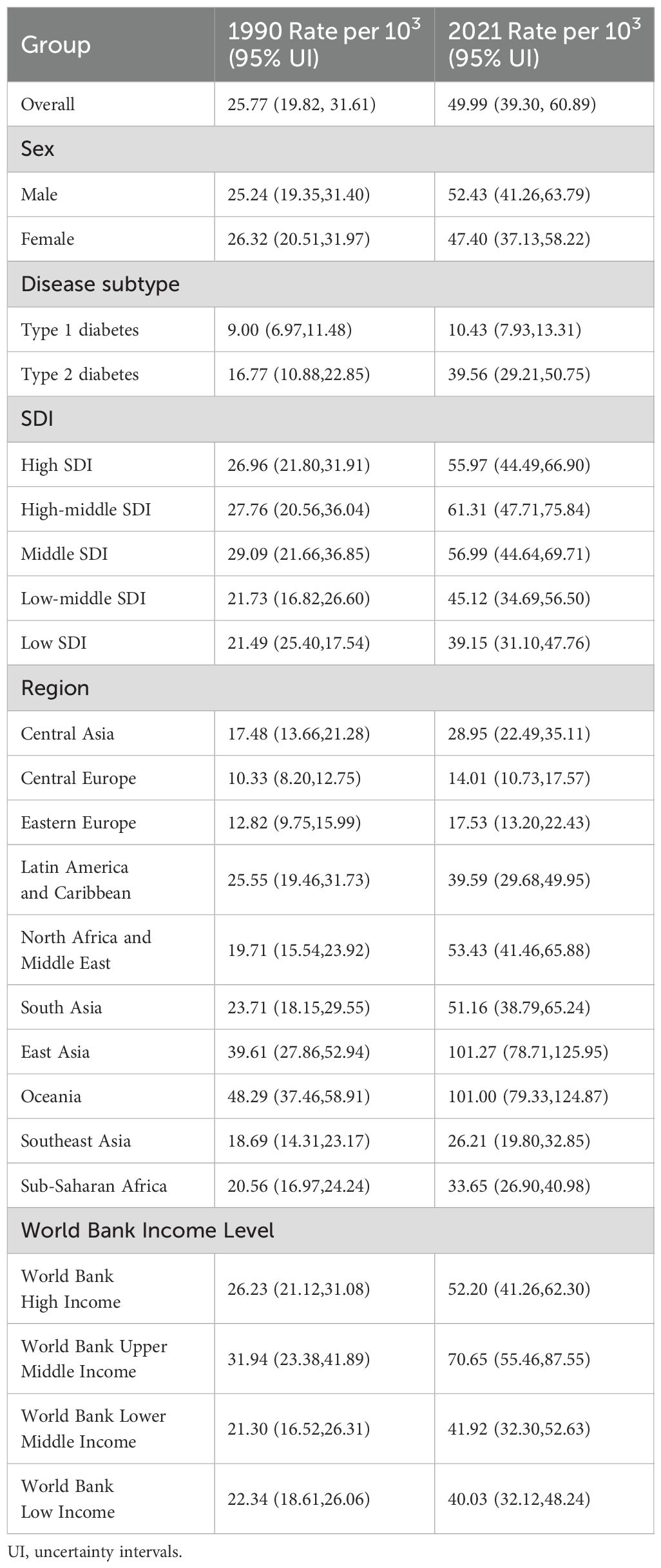
Table 1. The incidence rate of diabetes in 1990/2021.
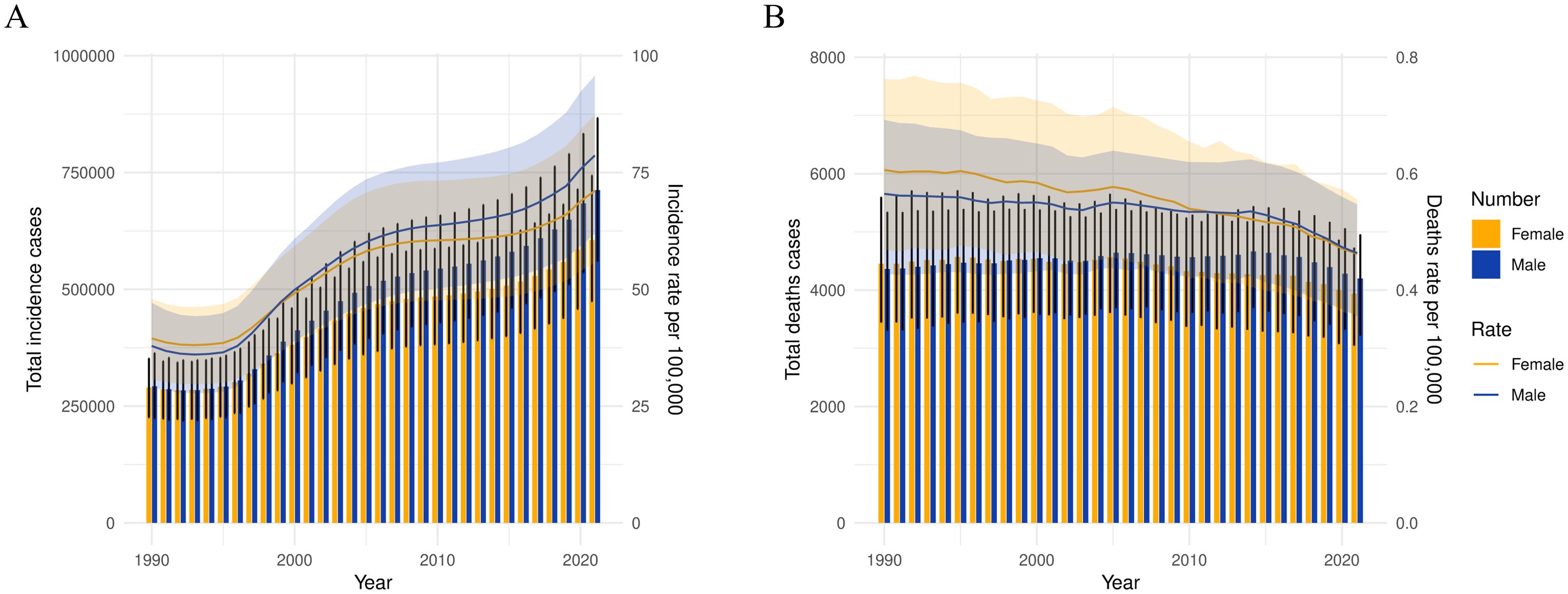
Figure 1. The change trends of diabetes’s incidence cases, and deaths from 1990 to 2021. (A) The change trends of incidences, (B) the change trends of deaths. Blue bars represent males and orange bars represent females.
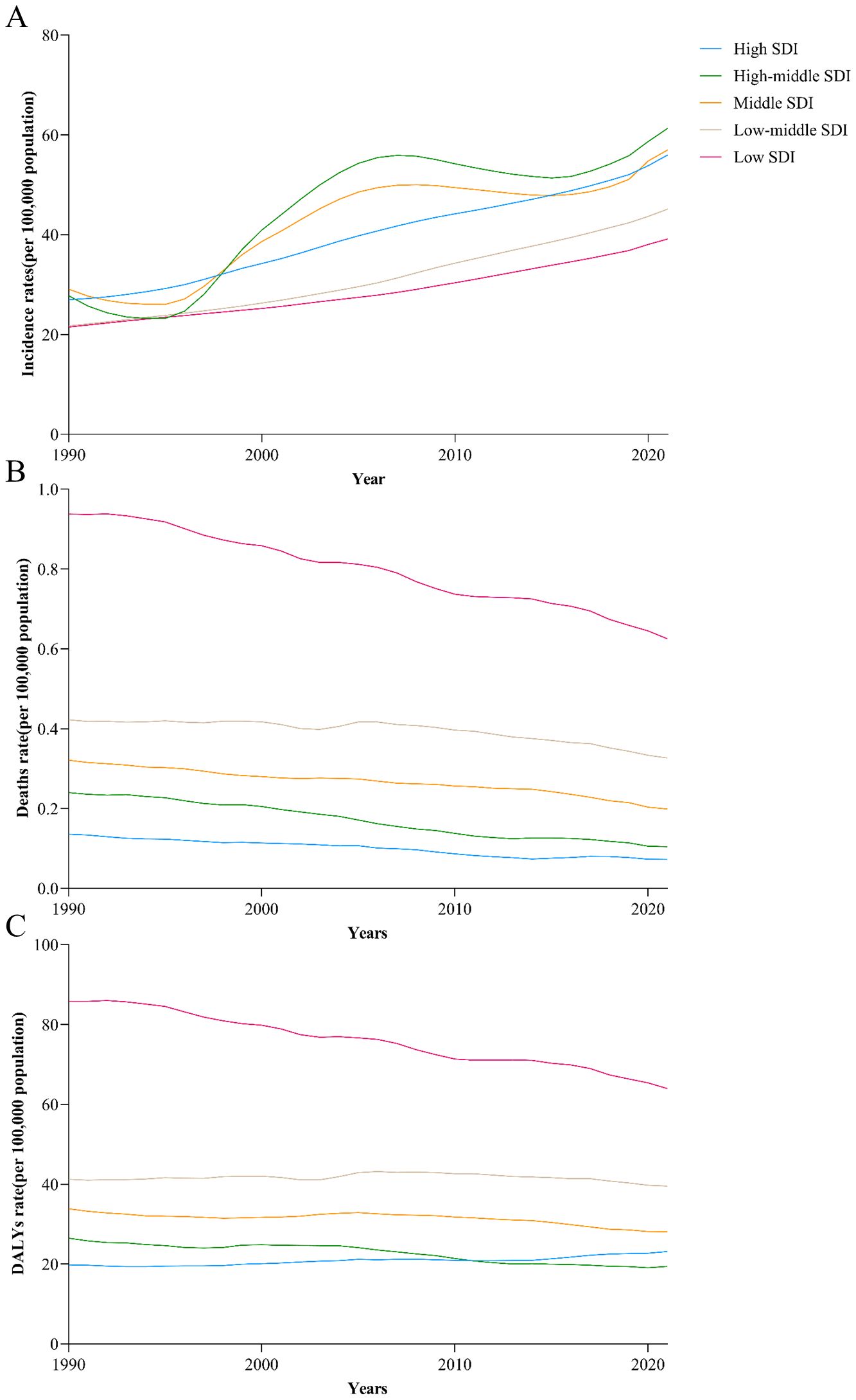
Figure 2. Trends from 1990 to 2021 in the death rate of diabetes in five SDI regions. (A) The change trends of incidences, (B) the change trends of deaths, (C) the change trends of DALYs.
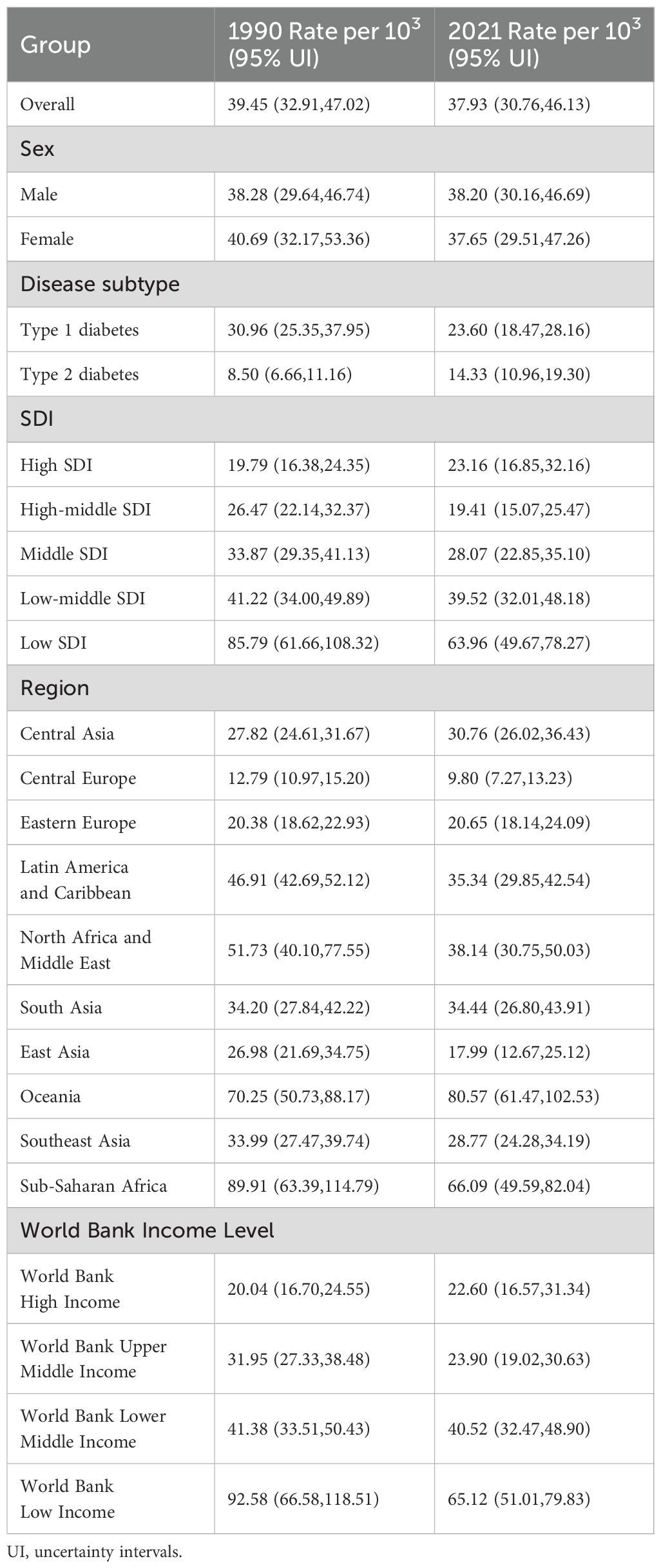
Table 2. The DALY of diabetes in 1990/2021.
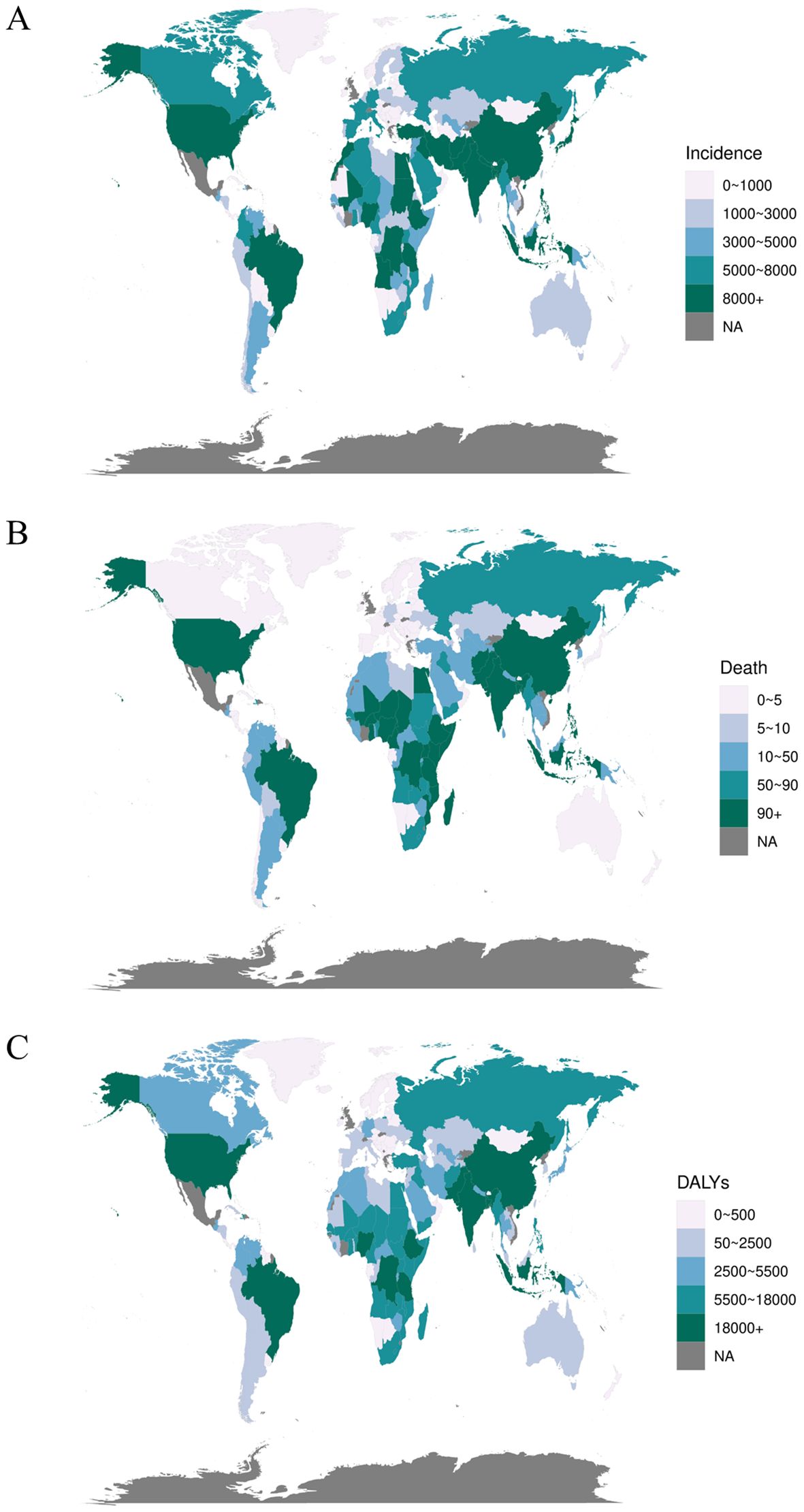
Figure 3. The global disease burden of diabetes in 204 countries or territories. (A) The incidence cases of 204 countries or territories in 2021, (B) the deaths of 204 countries or territories in 2021, and (C) the DALYs of 204 countries or territories in 2021.
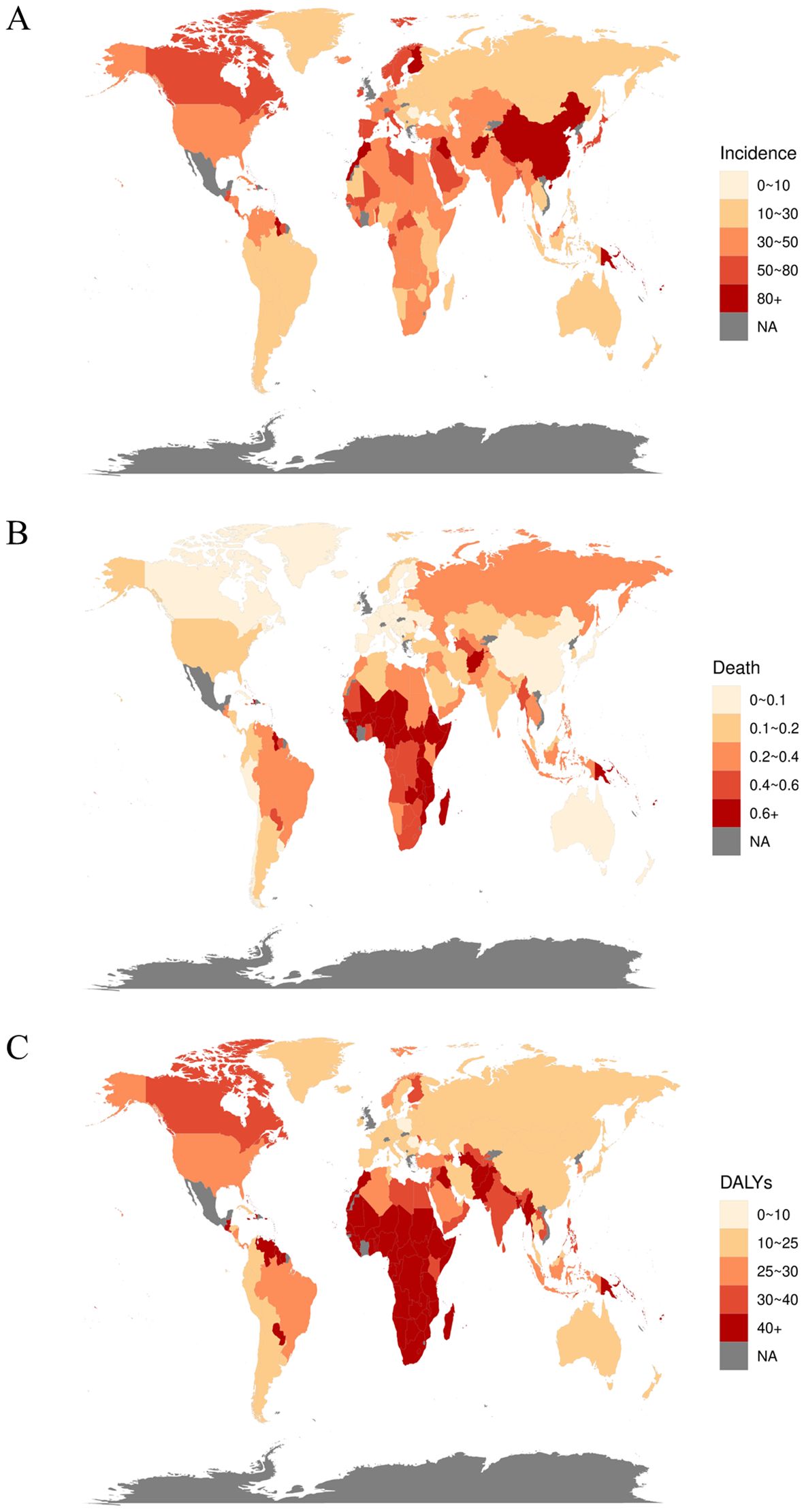
Figure 4. The rates of diabetes in 204 countries or territories. (A) The incidence rate of 204 countries or territories in 2021, (B) the death rate of 204 countries or territories in 2021, and (C) the DALY rate of 204 countries or territories in 2021.
3.2 Global trends and death of diabetes in children and adolescents
Among the global population of children and adolescents, the diabetes-related death rate has exhibited a general annual decline over the past 32 years, decreasing from 0.39 per 100,000 in 1990 to 0.31 per 100,000 in 2021. Correspondingly, the number of deaths has decreased from 8,813 to 8,134. Deaths associated with type 1 diabetes remain substantially higher than those associated with type 2 diabetes (Supplementary Figure S2); however, the death rate for type 2 diabetes has risen from 0.06 per 100,000 in 1990 to 0.08 per 100,000 in 2021. The diabetes death rate is comparable between males and females, both standing at 0.31 per 100,000 (Table 3, Figure 1B). At the SDI level, diabetes-related death rates across the five SDI regions demonstrate a generally decreasing trend. The death rate is lowest in the High SDI regions (0.07, 95% UI: 0.07 – 0.08) and highest in the Low SDI regions (0.63, 95% UI: 0.46 – 0.76) (Table 3, Figure 2B, Supplementary Figures S3, S4). Subgroup analysis by geographical region reveals that Oceania exhibits the highest death rate and an increasing trend, rising from 0.73 per 100,000 in 1990 to 0.77 per 100,000 in 2021. In contrast, East Asia has experienced the most significant reduction in death rate, decreasing by 74% relative to 1990 (Table 3). At the national level, India reports the highest number of diabetes-related deaths, with 1.32×10³ cases in 1990 and 0.96×10³ cases in 2021. Conversely, China’s diabetes-related deaths have decreased from the second highest in 1990 (1.02×10³ cases) to the ninth position in 2021 (0.19×10³ cases) (Figures 3B, 4B, Supplementary Tables S3, S4).
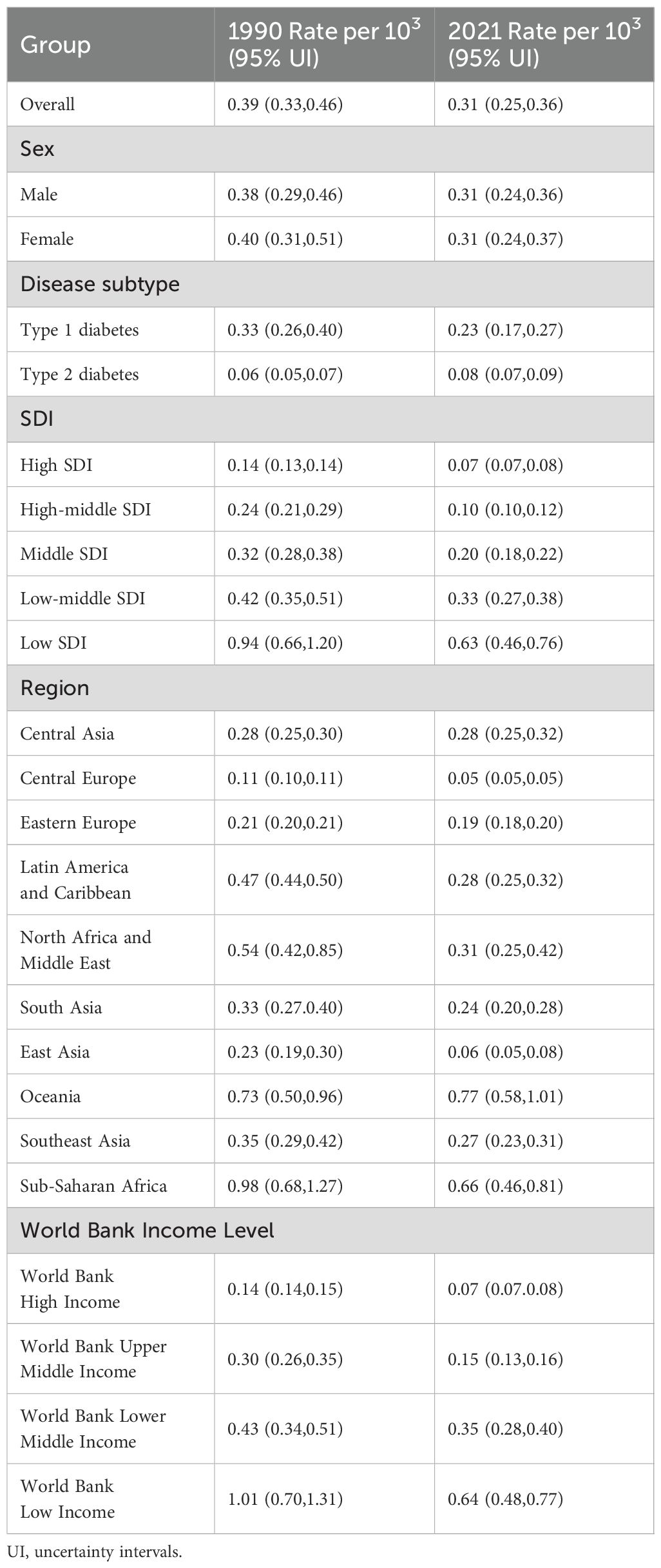
Table 3. The death of diabetes in 1990/2021.
3.3 Global trends and DALY of diabetes in children and adolescents
Among the global population of children and adolescents, the DALY rate has generally declined over the past 32 years, decreasing from 39.45 per 100,000 in 1990 to 37.83 per 100,000 in 2021. However, the total DALYs have risen from 891.1×10³ years to 999.9×10³ years. Compared to 1990, the DALY rate for type 1 diabetes decreased by 2021, whereas the DALY rate for type 2 diabetes increased. Nonetheless, the DALY rate for type 1 diabetes remains higher overall, at 23.60 per 100,000 compared to 14.33 per 100,000 for type 2 diabetes (Supplementary Figure S3). The DALY rate for males has remained relatively stable, whereas the DALY rate for females appears to be a significant factor in the overall decrease in the DALY rate, decreasing from 40.69 in 1990 to 37.65 in 2021. In 2021, the female DALY rate is lower than that of males (Table 2). At the SDI level, only the High SDI region has experienced an increase in the diabetes DALY rate, while the other four SDI regions have all shown a decline, with the Low SDI region exhibiting the most pronounced decrease (Table 2, Figure 2C, Supplementary Figures S3, S4). Subgroup analysis by geographical region indicates that Oceania has the highest DALY rate and displays an increasing trend, rising from 7,025 per 100,000 in 1990 to 80.57 per 100,000 in 2021 (Table 2). At the national level, India reports the highest total diabetes DALYs and an increasing trend, rising from 135.04×10³ years in 1990 to 150.73×10³ years in 2021. Conversely, China’s total diabetes DALYs have decreased, falling from the second highest in 1990 (119.81×10³ years) to the third highest in 2021 (59.29×10³ years) (Figures 3C, 4C, Supplementary Tables S5, S6).
3.4 Association between SDI and global incidence and death rates of diabetes in children and adolescents
We evaluated the association between trends in the SDI across 21 global regions from 1990 to 2021 and the incidence and death rates of diabetes in children and adolescents. The results reveal that both global and regional diabetes incidence rates are significantly positively associated with SDI (correlation coefficient = 0.10, P < 0.01), whereas diabetes-related death rates are significantly negatively associated with SDI (correlation coefficient = -0.74, P < 0.01) (Figure 5).
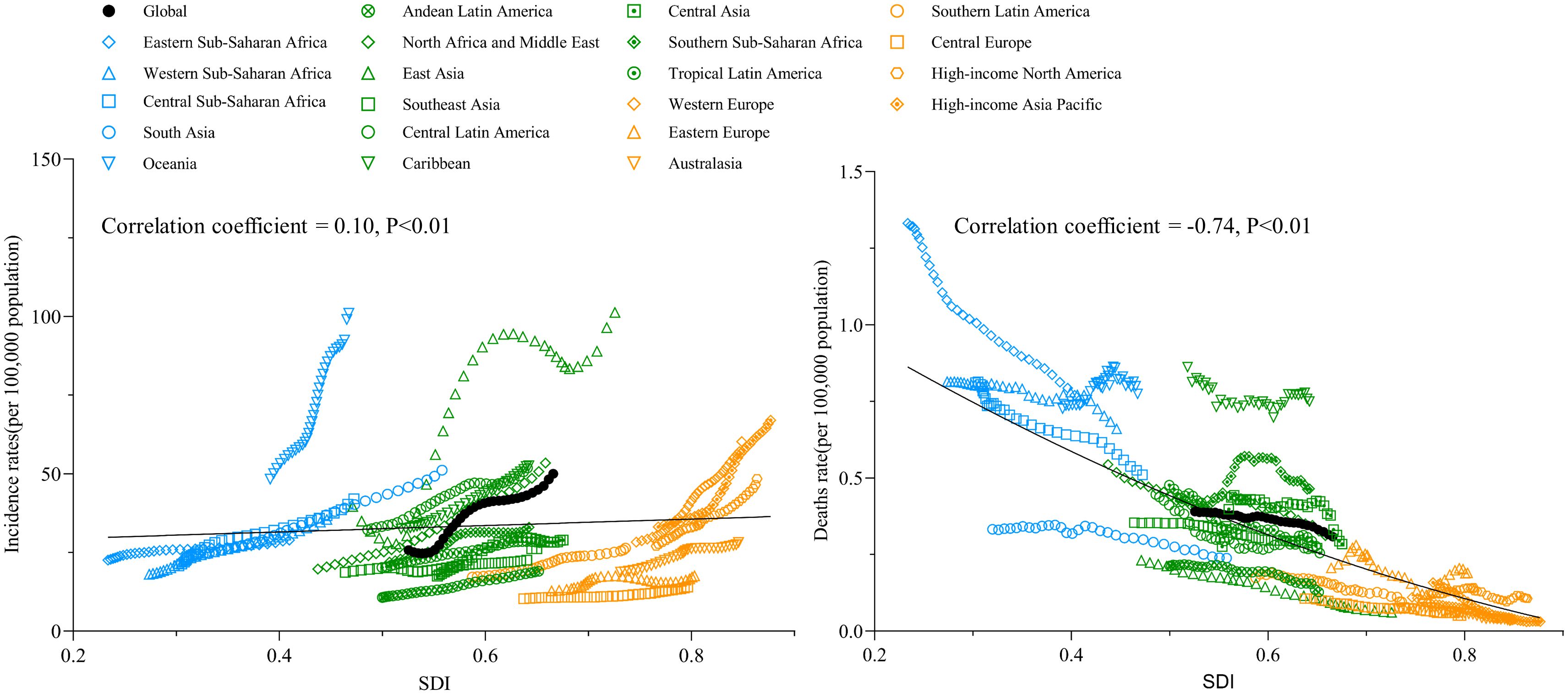
Figure 5. The change trends and correlation analyses of incidence rate and death rate with SDI from 1990 to 2021.
3.5 Age distribution of diabetes incidence among children and adolescents
We examined the incidence rates of diabetes across five distinct age groups (< 1 year, 2 to 4 years, 5 to 9 years, 10 to 14 years, and 15 to 19 years) both globally and within various regions from 1990 to 2021. The results reveal that both globally and across the five SDI regions, the highest incidence rate is observed in the 15 – 19 year age group, which demonstrates a significant upward trend in diabetes incidence (Figure 6, Supplementary Material 3). In addition, the mortality and DALY rates for type 1 diabetes patients under 1 year of age are significantly higher than those in other age groups, despite this group having the lowest incidence rate. The highest incidence is observed among adolescents aged 10 – 14 years (Supplementary Figure S6). Notably, due to the research framework adopted by the GBD, the incidence, mortality, and DALY rates for type 2 diabetes in patients under 15 years of age are all reported as zero (Supplementary Material 4).
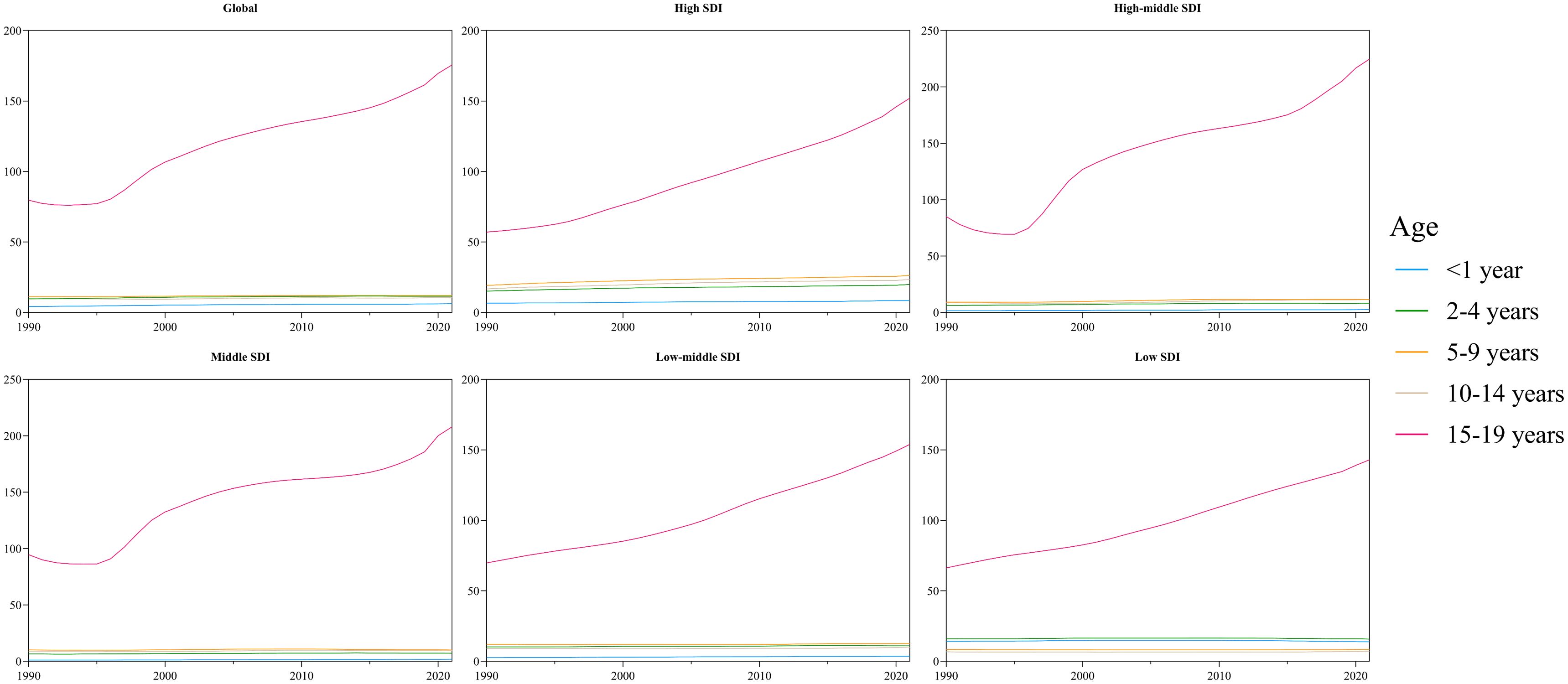
Figure 6. The incidence of cases of diabetes in different age groups from 1990 to 2021.
3.6 Risk factors contributing to diabetes-related death in children and adolescents worldwide
We identified three primary risk factors contributing to diabetes-related death and DALYs in children and adolescents: high fasting blood glucose, high temperatures, and low temperatures. Among these risk factors, elevated fasting blood glucose is the predominant contributor to diabetes-related death and DALYs in children and adolescents, both globally and across various regions from 1990 to 2021. In High SDI, High-middle SDI, and Middle SDI regions, low temperatures rank as the second most significant risk factor. In Low-middle SDI and Low SDI regions, high temperatures are identified as the second most significant risk factor (Figures 7A, B).
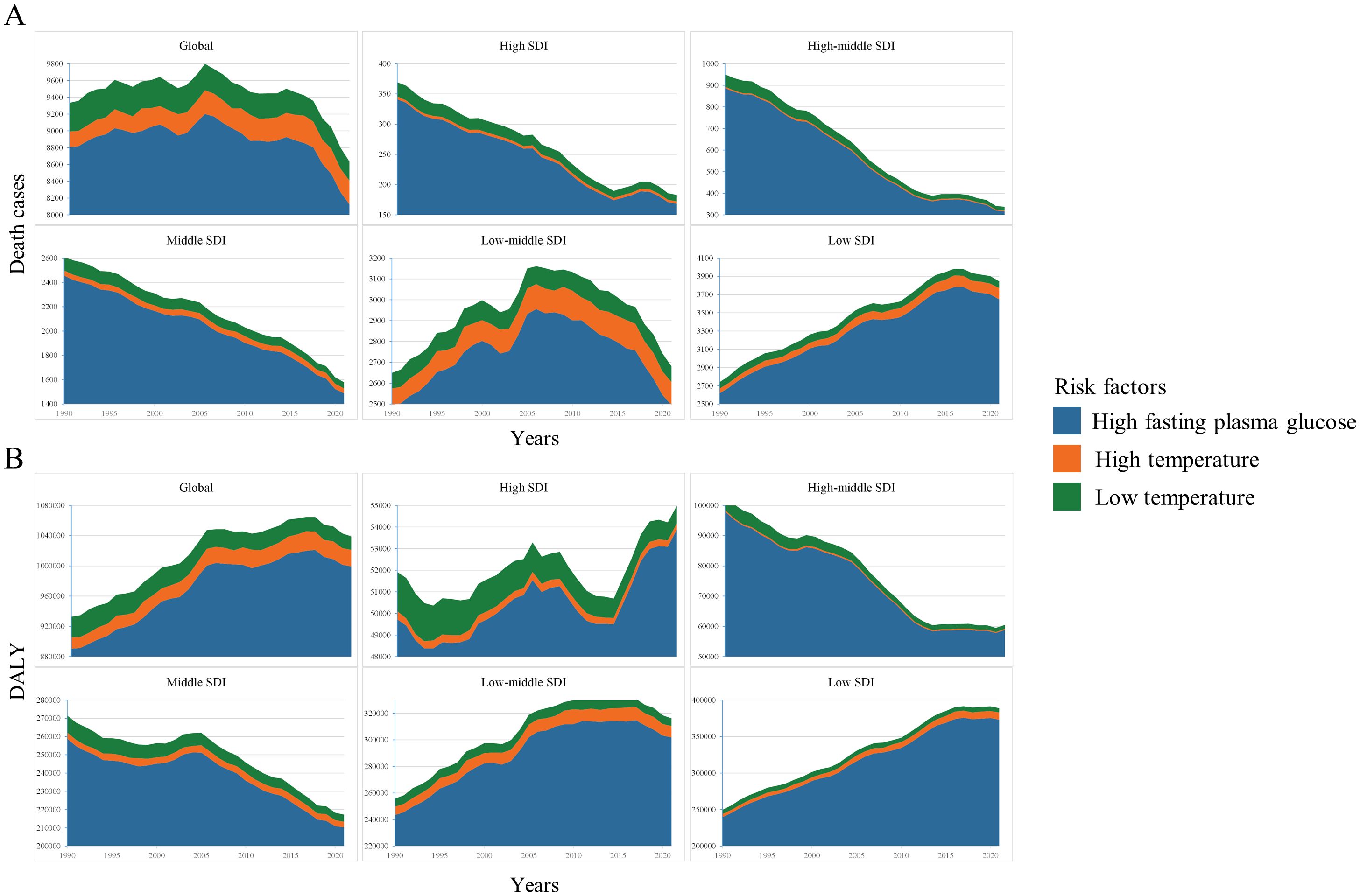
Figure 7. Risk factors contributing to diabetes-related death (A) and DALY (B).
3.7 Projecting trends in global childhood and adolescent diabetes incidence and mortality over the next 15 years with ARIMA models
As shown in Supplementary Figure S7 and Supplementary Figure S8, it is projected that the current trends in the incidence and mortality rates of diabetes in children and adolescents worldwide will persist over the next 15 years, with incidence increasing and mortality decreasing.
4 Discussion
This study presents the incidence, mortality, and DALY data for diabetes in children and adolescents, both globally and regionally, from 1990 to 2021, using the GBD 2021 database. Additionally, it examines the risk factors associated with diabetes-related mortality within this demographic. The findings indicate that between 1990 and 2021, there have been substantial changes in the burden and epidemiological trends of diabetes among children and adolescents, both globally and regionally. Notably, the global burden of diabetes within this age group has continued to rise.
Between 1990 and 2021, the incidence rate of diabetes among children and adolescents has exhibited a general increase, with a notable rise of 94.0% in global incidence over this period. Recent research attributes these trends to factors such as obesity, familial predisposition, and sedentary lifestyles (21). This increase may reflect broader trends including global population growth, demographic aging, dietary changes, and shifts in lifestyle over the past 32 years (22). Regions with higher Socio-Demographic Index (SDI) scores have demonstrated higher incidence rates compared to regions with lower SDI scores, showing a significant positive correlation between SDI and incidence rates. This pattern aligns with previous perspectives that classify diabetes as a “disease of affluence,” characterized by distinctive modern attributes. Residents of high SDI regions frequently encounter overnutrition and reduced physical activity, contributing to elevated obesity rates among children and adolescents, which is a well-established risk factor for diabetes (23–25). Additionally, this trend may be partly attributable to more advanced diabetes diagnosis and registration systems in high SDI regions (14).
It is encouraging to note that over the past 31 years, the mortality rate and DALYs associated with diabetes in children and adolescents have declined globally. In regions with high SDI scores, mortality rates, and DALYs are markedly lower than in regions with low SDI scores. Correlation analysis further reveals a significant negative correlation between SDI and mortality rates. This trend can be attributed to advancements in basic healthcare coverage globally and the superior medical services available in high SDI regions, which enable more effective and timely diagnosis and treatment of diabetes in children and adolescents (26).
Diabetes is acknowledged as a complex, multifactorial condition influenced by genetic, metabolic, and environmental factors. The precise pathogenesis of diabetes remains elusive, and the exact roles of these factors in the onset and progression of the disease in children and adolescents warrant further investigation (27). Elevated fasting blood glucose is unequivocally the principal risk factor for diabetes-related mortality among children and adolescents. Numerous studies have demonstrated that elevated blood glucose levels in diabetic patients are associated with an increased risk of complications, including coronary heart disease and stroke (28, 29). Diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome, both mediated by elevated blood glucose levels, are also major contributors to diabetes-related mortality (30, 31). Additionally, our analysis revealed that both high and low temperatures are risk factors for diabetes-related mortality in children and adolescents worldwide, with varying impacts depending on SDI regions. One study indicates that rising temperatures may lead to an accumulation of reactive substances due to chronic inflammation, thereby contributing to diabetes complications, with NADPH oxidase potentially playing a significant role (32). Furthermore, an observational study conducted in inland and coastal regions of China identified a significant correlation between environmental temperatures and diabetes mortality (33).
This study offers several significant advantages. Firstly, by leveraging the high-quality evidence and methodological framework provided by GBD 2021, we have accurately reported the incidence and mortality rates of diabetes among children and adolescents, both globally and regionally, from 1990 to 2021. Secondly, in comparison to existing research, our study provides an innovative analysis of the epidemiological status of diabetes in children and adolescents (under 20 years), grounded in current trends and utilizing the most recent data from GBD 2021, thus ensuring the timeliness of our conclusions.
Nevertheless, this study has several limitations. Firstly, the results are based on aggregated data from the GBD study, and the accuracy of this data is contingent upon the quality of data reported by different countries. Certain countries and regions may have a substantial number of undiagnosed cases of diabetes among children and adolescents, coupled with insufficient data on related risk factors, which can undermine the accuracy of the findings. Secondly, The aggregate-level data provided by the GBD prevent the use of conventional epidemiological methods, such as survival analysis or regression analysis, to explore potential associations between individual indicators and diseases, which may introduce bias. Thirdly, the study is limited by the absence of some critical data, which precluded the use of age standardization and thereby constrained our ability to comprehensively describe global epidemiological trends of diabetes in children and adolescents. This limitation may have diminished the overall completeness of the results.
5 Conclusions
Over the 32-year period from 1990 to 2021, the global burden of diabetes among children and adolescents remained substantial. Specifically, the incidence rates of both type 1 and type 2 diabetes exhibited an overall upward trend. Although global mortality and DALYs associated with diabetes have declined, this decrease has been primarily driven by improvements in type 1 diabetes outcomes. In contrast, both the mortality rate and DALYs related to type 2 diabetes have actually increased. This suggests that diabetes will continue to pose a serious threat to the health of children and adolescents worldwide. Therefore, healthcare institutions must develop more cost-effective and targeted strategies to alleviate the adverse impacts of diabetes on young populations and to reduce the associated socioeconomic burden.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
YH: Data curation, Methodology, Writing – original draft. TH: Data curation, Methodology, Writing – original draft. YZ: Data curation, Methodology, Writing – original draft. YL: Writing – review & editing. CG: Writing – review & editing. YX: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by the Sichuan Province cadre health research project (NO.ZH2022 - 1501) and SichuanScience and Technology Program (NO.2023YFS0471).
Acknowledgments
We extend our sincere gratitude to the GBD team for granting us access to their extensive database.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1587055/full#supplementary-material
Supplementary Material 1 | Top 20 countries or areas with the highest number of incidence, mortality and DALYs, 1990 or 2021.
Supplementary Material 2 | The global burden situation based on the grouping criterion of diabetes types and the ARIMA analysis results.
Supplementary Material 3 | The global burden of disease based on age groups.
Supplementary Material 4 | The global burden of disease based on age groups and diabetes groups.
References
1. Global burden of 369 diseases and injuries in 204 countries and territories, 1990 - 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Lond Engl. (2020) 396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan B, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
3. Squires E, Duber H, Campbell M, Cao J, Chapin A, Horst C, et al. Health care spending on diabetes in the U.S., 1996-2013. Diabetes Care. (2018) 41(7):1423–31. doi: 10.2337/dc17-1376
4. Afroz A, Alramadan MJ, Hossain MN, Romero L, Alam K, Magliano DJ, et al. Cost-of-illness of type 2 diabetes mellitus in low and lower-middle income countries: a systematic review. BMC Health Serv Res. (2018) 18(1):972. doi: 10.1186/s12913-018-3772-8
5. S T, A O, and S M. The economic costs of type 2 diabetes: A global systematic review. PharmacoEconomics. (2015) 33(8):811–31. doi: 10.1007/s40273-015-0268-9
6. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet Lond Engl. (2016) 387(10027):1513–30. doi: 10.1016/S0140-6736(16)00618-8
7. Organization WH. Classification of Diabetes Mellitus. Geneva: World Health Organization (2019). Available online at: https://iris.who.int/handle/10665/325182.
8. Diaz-Valencia PA, Bougnères P, and Valleron AJ. Global epidemiology of type 1 diabetes in young adults and adults: a systematic review. BMC Public Health. (2015) 15:255. doi: 10.1186/s12889-015-1591-y
9. P C, G L, D G, S G, O G, and S M. Diabetes in the young - a global view and worldwide estimates of numbers of children with type 1 diabetes. Diabetes Res Clin Pract. (2014) 103(2):161–75. doi: 10.1016/j.diabres.2013.11.005
10. K As, W Jh, R Li, and K Cr. Epidemiologic approach to the etiology of type I diabetes mellitus and its complications. N Engl J Med. (1987) 317(122):1390–8. doi: 10.1056/NEJM198711263172206
11. A E, L S, L R, W Dr, and D Mj. Type 2 diabetes. Lancet Lond Engl. (2022) 400:1803–20. doi: 10.1016/S0140-6736(22)01655-5
12. L N, B J, P H, B Ah, B Cj, and B S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. (2018) 6(1):69–80. doi: 10.1016/S2213-8587(17)30186-9
13. Bhutta ZA, Salam RA, Gomber A, Lewis-Watts L, Narang T, Mbanya JC, et al. A century past the discovery of insulin: global progress and challenges for type 1 diabetes among children and adolescents in low-income and middle-income countries. Lancet Lond Engl. (2021) 398(10313):1837–50. doi: 10.1016/S0140-6736(21)02247-9
14. Yi M, Li A, Zhou L, Chu Q, Song Y, and Wu K. The global burden and attributable risk factor analysis of acute myeloid leukemia in 195 countries and territories from 1990 to 2017: estimates based on the global burden of disease study 2017. J Hematol OncolJ Hematol Oncol. (2020) 13(1):72. doi: 10.1186/s13045-020-00908-z
15. Lv B, Lan JX, Si YF, Ren YF, Li MY, Guo FF, et al. Epidemiological trends of subarachnoid hemorrhage at global, regional, and national level: a trend analysis study from 1990 to 2021. Mil Med Res. (2024) 11(1):46. doi: 10.1186/s40779-024-00551-6
16. Collaborators G 2021 D. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Lond Engl. (2023) 402:203. doi: 10.1016/S0140-6736(23)01301-6
17. Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990 - 2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Lond Engl. (2019) 394(10204):1145–58. doi: 10.1016/S0140-6736(19)30427-1
18. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990 - 2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Lond Engl. (2024) 403(10440):2133–61. doi: 10.1016/S0140-6736(24)00757-8
19. GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990 - 2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Lond Engl. (2018) 392:1923–94. doi: 10.1016/S0140-6736(18)32225-6
20. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. (2022) 7:e105-25. doi: 10.1016/S2468-2667(21)00249-8
21. Zhang K, Kan C, Han F, Zhang J, Ding C, Guo Z, et al. Global, regional, and national epidemiology of diabetes in children from 1990 to 2019. JAMA Pediatr. (2023) 177:837. doi: 10.1001/jamapediatrics.2023.2029
22. W Eg, D Mj, Y T, B K, L Ig, and K K. Type 2 diabetes in younger adults: the emerging UK epidemic. Postgrad Med J. (2010) 86(1022):711–8. doi: 10.1136/pgmj.2010.100917
23. Hill-Briggs F, Adler NE, Berkowitz SA, Chin MH, Gary-Webb TL, Navas-Acien A, et al. Social determinants of health and diabetes: A scientific review. Diabetes Care. (2020) 44(1):258–79. doi: 10.2337/dci20-0053
24. Manne-Goehler J, Geldsetzer P, Agoudavi K, Andall-Brereton G, Aryal KK, Bicaba BW, et al. Health system performance for people with diabetes in 28 low- and middle-income countries: A cross-sectional study of nationally representative surveys. PloS Med. (2019) 16(3):e1002751. doi: 10.1371/journal.pmed.1002751
25. Flood D, Seiglie JA, Dunn M, Tschida S, Theilmann M, Marcus ME, et al. The state of diabetes treatment coverage in 55 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 680 – 102 adults. Lancet Healthy Longev. (2021) 2(6):e340-51. doi: 10.1016/s2666-7568(21)00089-1
26. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990 - 2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond Engl. (2015) 385(9963):117–71. doi: 10.1016/S0140-6736(14)61682-2
27. S Mm and R Ns. Genetic predisposition in type 2 diabetes: A promising approach toward a personalized management of diabetes. Clin Genet. (2020) 98(6):525–47. doi: 10.1111/cge.13772
28. C M, G Hc, W Y, and Y S. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care. (1999) 22(2):233–40. doi: 10.2337/diacare.22.2.233
29. Collaboration TERF. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. (2010) 375:2215. doi: 10.1016/S0140-6736(10)60484-9
30. N Ea and K Ae. The evolution of diabetic ketoacidosis: An update of its etiology, pathogenesis and management. Metabolism. (2016) 65(4):507–21. doi: 10.1016/j.metabol.2015.12.007
31. Sn L and Th S. Treatment of hyperglycaemic hyperosmolar non-ketotic syndrome. Drugs. (1989) 38(3):462–72. doi: 10.2165/00003495-198938030-00007
32. Tikhonova IV, Grinevich AA, Kosyakova NI, and Safronova VG. The effect of high temperature on kinetics of reactive species generation in patients with type 2 diabetes. Free Radic Biol Med. (2022) 192:235–45. doi: 10.1016/j.freeradbiomed.2022.09.031
Keywords: diabetes, children and adolescents, global burden of disease, risk factors, subgroup analysis
Citation: Hu Y, He T, Zhang Y, Long Y, Gao C and Xu Y (2025) Analysis of the global burden of diabetes and attributable risk factor in children and adolescents across 204 countries and regions from 1990 to 2021. Front. Endocrinol. 16:1587055. doi: 10.3389/fendo.2025.1587055
Received: 03 March 2025; Accepted: 19 August 2025;
Published: 08 September 2025.
Edited by:
Russell Kabir, Anglia Ruskin University, United KingdomReviewed by:
Subhodip Pramanik, Neotia Getwel Healthcare Center, IndiaMarta Carolina Ruiz-Grao, University of Castilla La Mancha, Spain
Copyright © 2025 Hu, He, Zhang, Long, Gao and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Xu, eHl3eWxsQHN3bXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship